Embed Size (px)
Citation preview
- 116 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
Introduction
Dentigerous cyst (DC) is a common oral
lesion formed by fluid accumulation between the
fully formed tooth crown and the reduced enamel
epithelium. It is considered a developmental
abnormality arising from the reduced enamel
epithelium around the crown of an unerupted
tooth. The predilection site of DC is the
mandibular third molar. Other frequent sites
include maxillary canines, maxillary third molars,
and mandibular second premolar. It is always
associated with any unerupted teeth, usually
attached to the tooth at the cemento-enamel
junction. But rarely involves unerupted deciduous
teeth1.
Radiographically, the DC typically shows a
unilocular radiolucent shadow with a well-defined
sclerotic border associated with the crown of an
unerupted tooth, but an infected cyst will show
ill-defined borders2. Here, we will describe a case
of DC arising from right maxillary third molar and
involving the maxillary sinus with sinusitis.
Dentigerous Cyst Over Maxillary Sinus : A Case Report and Literature Review
Chih-Jen Wang*, Po-Hsien Huang, Yin-Lai Wang,
Yih-Chung Shyng, Wen-Bin Kao#
* Division of Oral and Maxillofacial Surgery, Department of Dentistry, Kaohsiung Armed
Forces General Hospital, Kaohsiung, Taiwan# School of Dentistry, National Defense Medical Center
Abstract
Dentigerous cyst (DC) is a common odontogenic cyst developed abnormally around unerupted maxillary or mandibular teeth. It is often asymptomatic and can be found incidentally on dental radiography with delayed eruption of teeth. However, it can be large and cause symptoms related to expansion and impingement on contiguous structures. Pain and swelling may be the major complains of patients. However, DC seldom caused head and neck inflammation or infection. Here, we described a 20-year-old male, who was found of a DC arising from right maxillary third molar involved the maxillary sinus and with sinusitis. We also reviewed articles to discuss the differential diagnosis of DC from other odontogenic cysts or odontogenic tumors.
Key words: dentigerous cyst, sinusitis, maxilla.
Taiwan J Oral Maxillofac Surg20: 116-124, June 2009 台灣口外誌

- 117 -
台灣口外誌 Dentigerous Cyst over Maxillary Sinus : A Case Report and Literature Review
Case report
A 20-year-old young male soldier was
referred to the Division of Oral and Maxillofacial
Surgery, Kaohsiung Armed Force General
Hospital with a history of painful sensation and
swelling over right maxilla. He was also suffered
with yellow-green pus discharges from nasal
cavity. On physical examination, pus discharged
from right maxillary second molar distal gingival
crevice area was noted. The right maxillary third
molar cannot be seen. The patient had recurrent
sinusitis for six years with medical treatment but
in vain. He had no systemic disease or drug and
food allergy history. Family history did not show
any contribution.
The panoramic radiography showed a well-
defined radiolucent lesion with sclerotic margin.
The lesion pushed the impacted maxillary third
molar upward to the roof of the maxillary sinus.
The right maxillary sinus was not clear in the
radiography. Root resorption of upper right
second molar was also noted (Fig. 1). Computed
Tomography revealed an expansive mass in
the right maxillary sinus associated with the
radioactive intensity similar to soft tissue. There
is no bone destruction (Fig. 2).
The patient was arranged to receive opera-
tion under general anesthesia. Cyst enucleation
was done with Caldwell-Luc’s procedure. Full
thickness mucoperiosteal flap was reflected at
the right mucobuccal fold from right fist premolar
to second molar. A bony window was made to
approach the maxillary sinus (Fig. 3). The cyst
was totally removed and the surrounding bony
structures about 1 to 2 mm thickness were
also shaved by Stryker. The lesion was about
4 × 3 × 2 cm in size with firm in consistency.
The impacted tooth was also removed. Delayed
closure of the wound was done. The opening was
packed with sterilized petrolatum gauze. Oozy
discharges were found on the following 2 days.
On the third day, the mucoperiostum was sutured
with 4-0 silk. Postoperative antibiotics were
prescribed for 7 days.
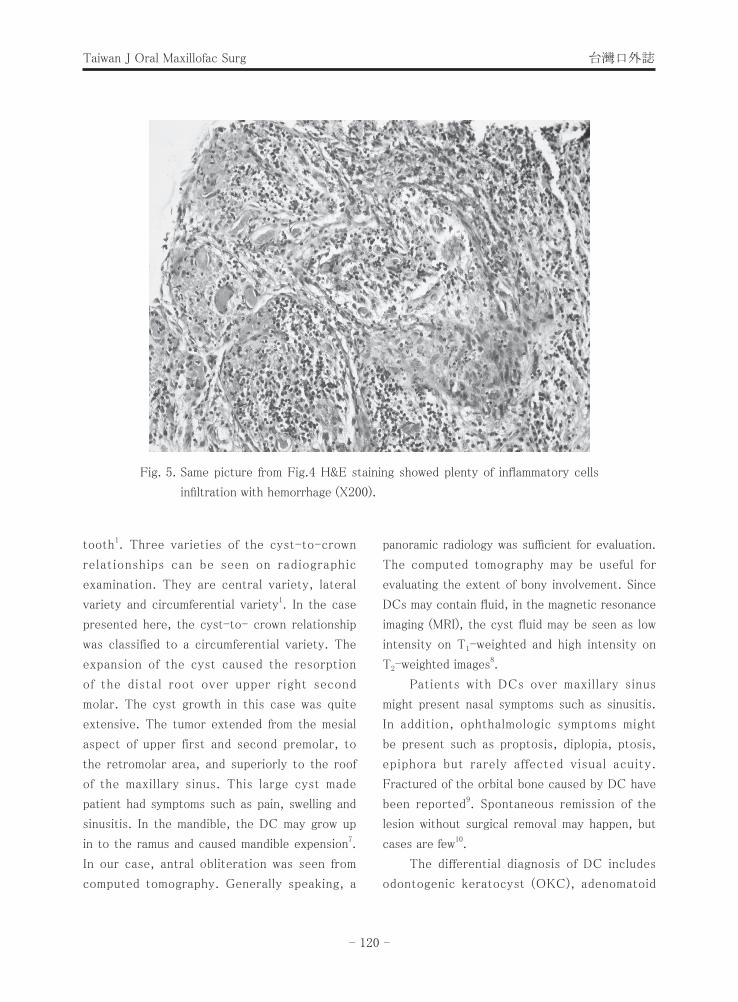
Microscopically, the epithelium was composed
of non-keratinizing stratified squamous epithelium
with plenty chronic inflammatory cells infiltration
(Fig 4, 5). There is no evidence of malignant
change or other odontogenic cysts differentiation.
A dentigerous cyst was confirmed.
One month latter, the patient was free from
sinusitis after receiving cyst enucleation. No cyst
recurrence was noted after an 18-months follow
up.
Discussion
The DC is the second most common
odontogenic cyst, with periapical cyst being
found more commonly. It presents mostly in the
second or third decade of life in the maxillary
or mandibular third molar or maxillary canine
regions3. It can originate from any tooth,
including supernumerary tooth4. The DCs are
mostly asymptomatic and may be found on
routine dental radiographic check-up. They may
also cause symptoms like pain or swelling with the
enlargement of the cyst size1. Several researchers
reported the pathologic fracture of the mandible
caused by the huge of DC4,5. The outgrowth
of the cyst may also cause the resorption of
adjacent tooth. According to Eliasson’s report,
roughly 1% of impacted maxillary third molars will
subsequently become involved with a DC6.
Radiographically, the typical DC showed a
well-defined radiolucency with sclerotic border
associated with the crown of an unerupted
- 118 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
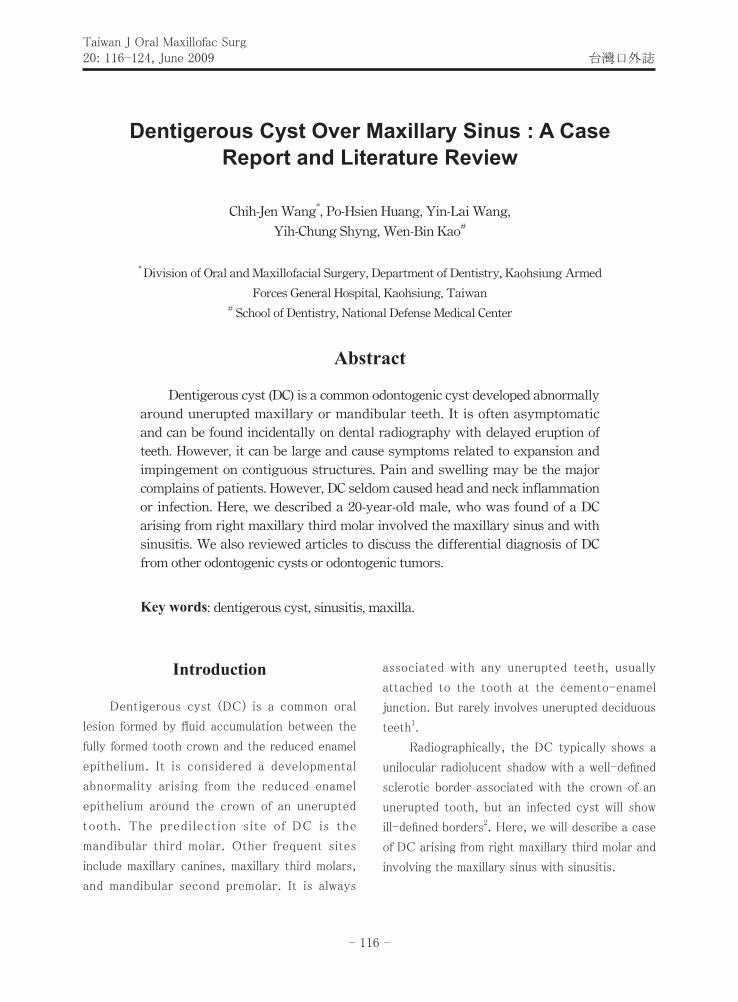
Fig. 1. Unclear sinus image with distal root resorption of upper right 2nd molar were seen. The impacted
tooth was pushed to the roof of maxillary sinus by the cyst. The cyst extended from upper right
premolar to retromolar area and maxillary sinus roof.
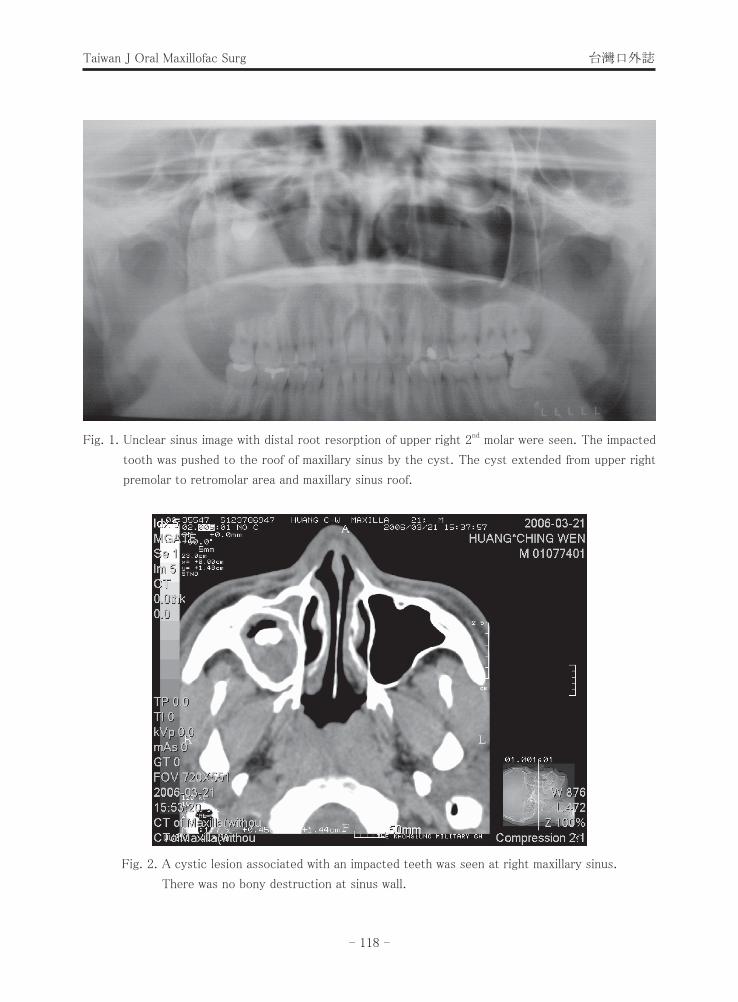
Fig. 2. A cystic lesion associated with an impacted teeth was seen at right maxillary sinus.
There was no bony destruction at sinus wall.
- 119 -
台灣口外誌 Dentigerous Cyst over Maxillary Sinus : A Case Report and Literature Review
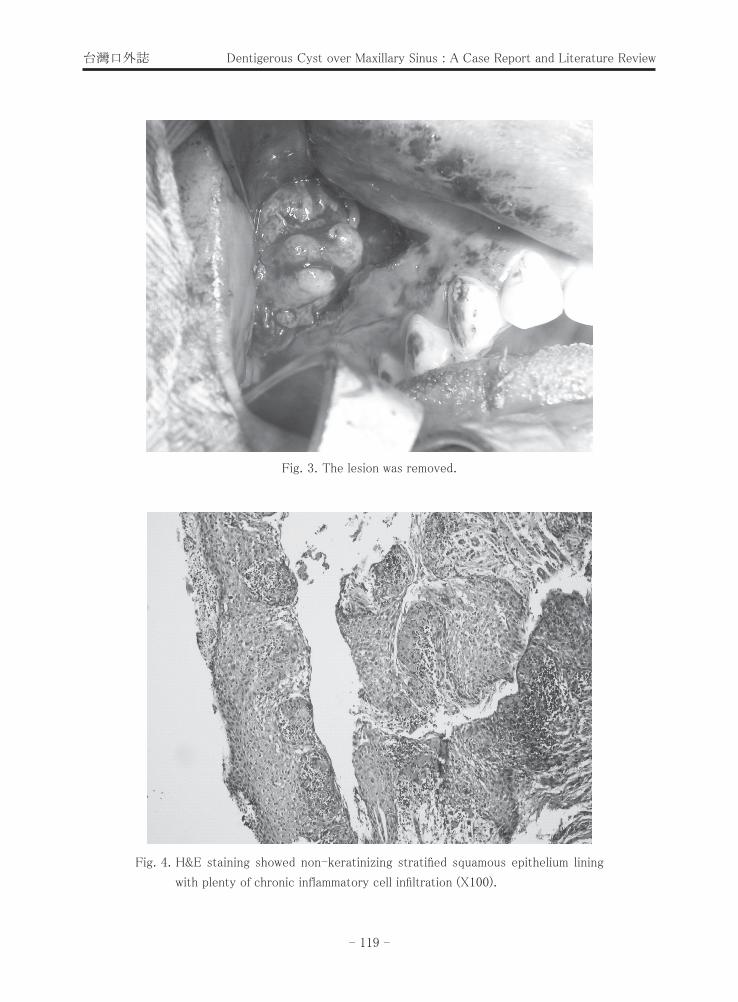
Fig. 3. The lesion was removed.
Fig. 4. H&E staining showed non-keratinizing stratified squamous epithelium lining
with plenty of chronic inflammatory cell infiltration (X100).
- 120 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
Fig. 5. Same picture from Fig.4 H&E staining showed plenty of inflammatory cells
infiltration with hemorrhage (X200).
tooth1. Three varieties of the cyst-to-crown
relationships can be seen on radiographic
examination. They are central variety, lateral
variety and circumferential variety1. In the case
presented here, the cyst-to- crown relationship
was classified to a circumferential variety. The
expansion of the cyst caused the resorption
of the distal root over upper right second
molar. The cyst growth in this case was quite
extensive. The tumor extended from the mesial
aspect of upper first and second premolar, to
the retromolar area, and superiorly to the roof
of the maxillary sinus. This large cyst made
patient had symptoms such as pain, swelling and
sinusitis. In the mandible, the DC may grow up
in to the ramus and caused mandible expension7.
In our case, antral obliteration was seen from
computed tomography. Generally speaking, a
panoramic radiology was sufficient for evaluation.
The computed tomography may be useful for
evaluating the extent of bony involvement. Since
DCs may contain fluid, in the magnetic resonance
imaging (MRI), the cyst fluid may be seen as low
intensity on T1-weighted and high intensity on
T2-weighted images8.
Patients with DCs over maxillary sinus
might present nasal symptoms such as sinusitis.
In addition, ophthalmologic symptoms might
be present such as proptosis, diplopia, ptosis,
epiphora but rarely affected visual acuity.
Fractured of the orbital bone caused by DC have
been reported9. Spontaneous remission of the
lesion without surgical removal may happen, but
cases are few10.
The differential diagnosis of DC includes
odontogenic keratocyst (OKC), adenomatoid

- 121 -
台灣口外誌 Dentigerous Cyst over Maxillary Sinus : A Case Report and Literature Review
odontogenic tumor (AOT), calcifying epithelial
odontogenic cyst (COC), calcifying epithelial
odontogenic tumor (CEOT), and unicystic
ameloblastoma (UAs). In addition to the histo-
pathologic differences between the feature of
the epithelium of OKC and DC, the differential
diagnosis can also include the development
and the recurrence tendency of these cysts.
About 40% unilocular OKC contain impacted
tooth. The OKC is more aggressive with higher
recurrence risk than DC and may be associated
with nevoid basal cell carcinoma syndrome.
Recently, researches showed mutation of PTCH
gene and overactivated of Shh signaling may be
associated with the clinicopathological expression
of OKCs11. BMP-4 may be a useful biochemical
marker to differentiation of OKC and DC. BMP-4
is expressed more intensive in OKC compared
with DC, and is more intensively expressed
in the recurred cases12. The AOT and COC
generally are more frequently seen in maxillary
anterior area with some degree of calcification
within the cyst cavity, which may be observed
from radiography7,13. Histopathologically, the
COC may present keratinized epithelial cell
so-called ghost cells in the cavity. The AOT
different from the DC, its predilection in female
with epithelial cells syncytially arranged in
rosettes or duct-like structure. The CEOT may
be differentiated from DC by its honeycomb
pattern radiolucency with foci of radiopacity
in radiographs. Microscopically, it shows large
polygonal epithelial cells with variation in size and
shape with amyloid materials, which contained
concentric calcified deposits (Liesegan rings)13.
Although the unicystic ameloblastoma is rare,
its clinical expression and microscopic feature
can be deceptive and may be confused with DC.
The UAs is more locally aggressive than DC with
several immunohistochemical markers enhanced,
such as Bcl-2, Bcl-xL,FGF, MMPs, Ki-67 and
PCNA14,15. Recently, calretinin was suggested to
be a specific immunohistochemical biomarker for
neoplastic ameloblastic epithelium and may serve
as a diagnostic tool for differentiating cystic
odontogenic lesions from ameloblastoma16.
The best treatment of the UAs is radical
though enucleation is sufficient in subtype 1
and 217,18,21-23. Considering the similarity of UAs
and DC clinically, we enucleated the lesion and
also trimmed the surrounding bony structures
to about 1 to 2 mm in thickness. Hopefully, the
histopathological report confirmed the diagnosis
of DC.
The DC may cause head and neck infection
with a prevalence of 2.1%24. The cyst can undergo
carcinomatous transformation into ameloblastoma
or squamous cell carcinoma but is rare25-28. In
cases where mucous cells are present in the
epithelium, the intraosseous mucoepidermoid
carcinoma may be ruled out1. Enucleation of the
cyst contents with extraction of the associated
tooth is sufficient for DC. For extremely large
lesions, or in cases when the involved tooth is
desired to keep in the arch, marsupialization may
be done. With decompression, the involved tooth
may erupt spontaneously by orthodontically into
occlusion. When other odontogenic tumors are
highly suspected, radical removal of the lesions
or removal of the cyst with surrounding bony
structures is suggested.
References
1. Neville BW, Damm DD, Allen CM, Bouquot
JE. Oral& Maxillofacial Pathology. 2nd ed.
Philadelphia: WB Saunders. 2002: 590-3.
2. Wood NK, Goaz PW. Differential Diagnosis of

- 122 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
Oral Lesions. 5th ed. St. Louis Mosby 1997:
283-8.
3. Regezi JA, Sciubba JJ, Jodan R.C.K. Oral
pathology, clinical pathologic correlations.
4th ed. St. Louis: WB Saunders. 2003: 246-
88.
4. Som PM, Shangold LM, Biller HF. A palatal
dentigerous cyst arising from a mesiodente.
Am H Neuroradiol 1992; 13: 212-4.
5. Maroo SV. Clinico-radiological aspects of
dentigerous cysts. East Afr Med J 1991; 68:
249-54.
6. Eliasson S, Heimdahl A, Nordenram A.
Pathological changes related to long-
term impaction of third molars. Int J Oral
Maxillofac Surg 1989: 210-25.
7. Goaz PW, White SC. Oral radiology, principles
and interpretation. 2nd ed. St. Louis: Mosby.
1987: 486-9, 426-692.
8. SOM PM, Shugar JMA, Cohen BA, Biller HF.
The nonspecificity of the antral bowing sign
in maxillary sinus pathology. J Comput Assist
Tomogr 1981; 5: 350-2.
9. Omer K, Onder B. A misdiagnosed giant
dentigerous cyst involving the maxillary
antrum and affecting the orbit. Case report.
Aust Dent J 1994; 39: 165-7.
10. Freedman GL. A disappearing dentigerous
cyst:Report of a case. J Oral Maxillofac Surg
1988; 46: 885-6.
11. Koyama E, Yamaai T, Isseki S, Ohuchi H,
Nohno T, Yoshiola H, Hayash Y, Leatherman
JL, Golden EBm Noji S, Pacifici M. Polarizing
activity, Sonic hedgehog, and tooth develop-
ment in embryonic and postnatal mouse. Dev
Dyn 1996; 206: 59-72.
12. Kim SG, Yang BE, Oh SH, Min SK, Hong SP,
Choi JY. The differential expression pattern
of BMP-4 between the dentigerous cyst and
the odontogenic keratocyst. J Oral Pathol
Med 2005; 34: 178-83.
13. Regezi JA, Sciubba JJ, Jodan RCK. Oral
pathology, clinical pathologic correlations.
4th ed. St Louis: WB Saunders. 2003: 274-
76.
14. Kumamoto H, Ooya L. Immunohistochemical
analysis of Bcl-2 family proteins in benign and
malignant ameloblastomas. J Oral Pathol Med
1999; 28: 343-9.
15. Li TJ, Brown RM, Matthews JB. Expression
of proliferating cell nuclear antigen (PCNA)
and Ki-67 in unicystic ameloblastoma.
Histopathol 1955; 26: 219-28.
16. Coleman H, Altini M, Ali H, Doflioni C,
Favia G, Maiorano E. Use of calretinin
in the differential diagnosis of unicystic
ameloblastomas. Histopathol 2001; 38: 312-
7.
17. Gardner D. Plexiform unicystic ameloblas-
toma: a diagnostic problem in dentigerous
cyst. Cancer 1981; 47: 1358-63.
18. Ackermann GL, Altini M, Shear M. The
unicystic ameloblastoma: a clinicopathological
study of 57 cases. J Oral Pathol 1988; 17:
541-6.
19. Philipsen HP, reichart PA. Unicystic amelo-
blastoma. A review of 193 cases from the
literature. Oral Oncol 1998; 34: 317-25.
21. Shear M. Cysts of the Oral Regions, 3rd ed.
Oxfort: Wright. 1992; 75-98
22. Robinson L, Martinez MG. Unicystic amelo-
blastoma: a prognostically distinct entity.
Cancer 1977; 40: 2278-85.
23. Li TJ, Wu YT, Yu SF, Yu GY. Unicystic
ameloblastoma: a clinicopathologic study of
33 Chinese patients. Am J Surg Pathol 2000;
24: 1385-92.
24. Smith JL, Kellman RM. Dentigerous cysts

- 123 -
台灣口外誌 Dentigerous Cyst over Maxillary Sinus : A Case Report and Literature Review
presenting as head and neck infections.
Otolaryngol Head Neck Surg 2005; 133: 715-
20.
25. Kramer IRH, Pindborg JJ, Shear M. Histo-
logical Typing of Odontogenic Tumors.
Berlin: Springer 1992: 11-4.
26. Yaacob HB, Ling KC. Ameloblastomatous
changes in dentigerous cyst. Aust Dent J
1982; 27: 365-7.
27. Rafael M: Ameloblastoma developing from a
dentigerous cyst. Oral Surg Oral Med Oral
Pathol 1960; 13: 781-6.
28. McMillan MD, Millie AC. Ameloblastomas
associated with dentigerous cysts. J Oral
Pathol Med 1981; 51: 489-96.
- 124 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
Received: March 28, 2009Accepted: May 31, 2009Reprint requests to: Dr. Wen-Bin Kao, Division of Oral and Maxillofacial Surgery, Department of
Dentistry, Kaohsiung Armed Forces General Hospital.
上顎竇之含牙囊腫:病例報告與文獻回顧
王峙仁* 黃寶賢 王銀來 邢憶春 高文斌#
* 國軍高雄總醫院牙科部口腔顎面外科
# 國防醫學院牙醫學系
摘 要
含牙囊腫是一種常見於上下顎阻生齒周圍發育異常的齒源性囊腫。由於
通常並無症狀,故患者常因為牙齒延遲萌發,於接受放射檢查時而發現。然
而,此囊腫若持續擴大,侵犯擠壓到鄰近組織,便可能產生不適。腫大與疼
痛是大多數病人的主要抱怨的症狀,但含牙囊腫鮮少引起頭頸部發炎或感
染。本文提出一位20歲男性因右上顎第三大臼齒侵犯上顎竇導致鼻竇炎的個
案報告,同時藉由回顧文獻,討論對於含牙囊腫與其他齒源性囊腫的鑑別診
斷。
關鍵詞:含牙囊腫,鼻竇炎,上顎。