Embed Size (px)
Citation preview

Depressione e BPSD, terapie non farmacologiche e
farmacologiche: il punto
Dipartimento di Medicina e Chirurgia, Università Milano-Bicocca, Milano; UO Geriatria, AO S Gerardo, Monza;
Società Italiana di Gerontologia e Geriatria (SIGG)Associazione Italiana di Psicogeriatria (AIP);
Giuseppe Bellelli
1 dicembre 2016

Depressione e BPSD, terapie non farmacologiche e
farmacologiche nel paziente affetto da demenza: il punto
Dipartimento di Medicina e Chirurgia, Università Milano-Bicocca; UO Geriatria, AO S Gerardo, Monza;
Società Italiana di Gerontologia e Geriatria (SIGG)Associazione Italiana di Psicogeriatria (AIP);
Giuseppe Bellelli
1 dicembre 2016

Jost BC, Grossberg GT. J Am Geriatr Soc. 1996
Socially Unacceptable
100
80
60
40
20
0
–40 –30 –20 –10 0 10 20 30
Mesi prima della Diagnosi Mesi dopo la Diagnosi
Pre
vale
nza
(% d
i paz
ien
ti) Agitation
Diurnal Rhythm
Irritability
Wandering Aggression
HallucinationsMood Change
DelusionsSexually Inappropriate
AccusatorySuicidalIdeation
Paranoia
Depression
Anxiety
Social Withdrawal
BPSD occurrence in Alzheimer’s disease

Irritabilità Opposività
Aggressività fisica
Aggressività verbale
‘Aggressività’
AllucinazioniDeliri
Misidentificazioni‘Psicosi’
Ritiro socialePerdita di interessi
‘Apatia’
Adapted from McShane R: Int Psychogeriatr 2000; 12: 147–54Finkel SI et al.: Am J Geriatr Psychiatry 1998; 6: 97–100
Alessi C et al.: J Am Geriatr Soc 1999; 47: 784–91
BPSD “Clusters"
TristezzaPianto
Perdita di speranzaBassa autosima
AnsiaColpa
‘Depressione’
‘Agitazione’
WanderingInquietudine
Vestirsi-svestirsiInsonnia
Sundowning
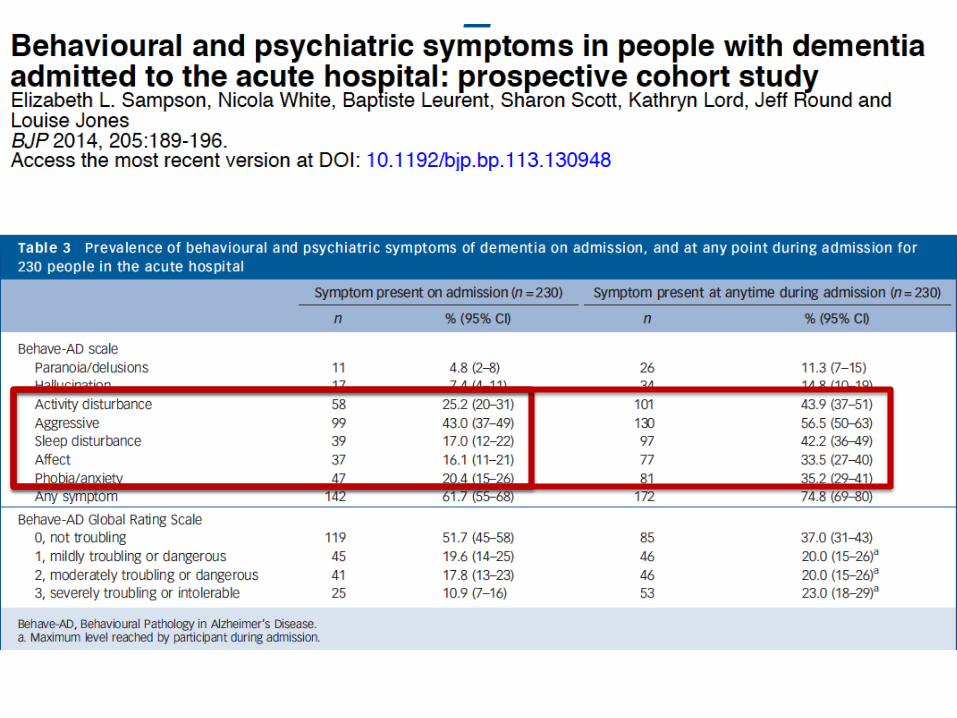
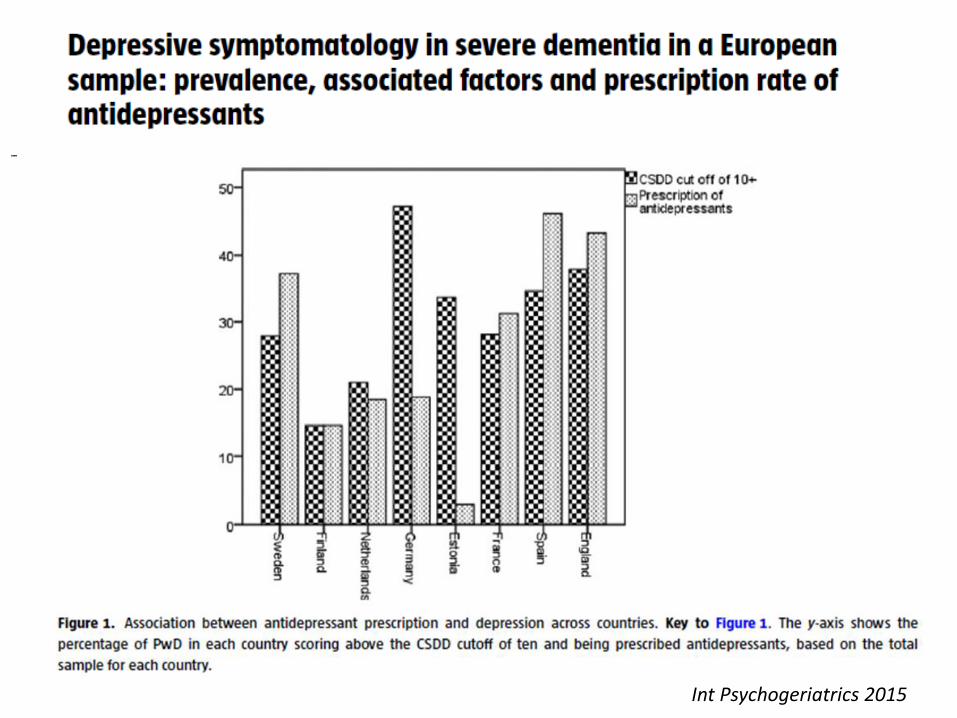
Int Psychogeriatrics 2015

Trattamento farmacologico dei BPSD
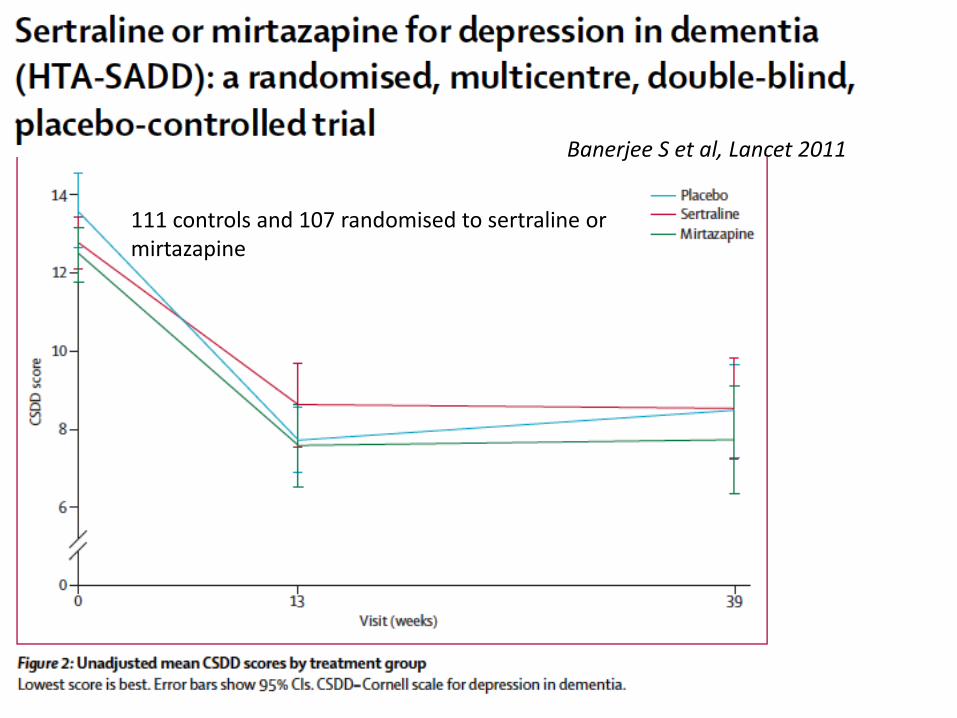
111 controls and 107 randomised to sertraline or mirtazapine
Banerjee S et al, Lancet 2011

Porsteinsson AP et al, JAMA 2014
Worsening ofcognition (−1.05 points; 95%CI, −1.97 to −0.13; P = .03) and QT intervalprolongation (18.1 ms; 95%CI, 6.1-30.1; P = .01) in the citalopram group.

10
All causes
Intolerability
Schneider L et al. N Engl J Med. 2006 Oct 12;355(15):1525-38
Lack of efficacy
100
90
80
70
60
50
40
30
20
10
00 4 8 12 16 20 24 28 32 36 40
Time to discontinuation of treatment (wk)
Dis
con
tin
uat
ion
for
any
reas
on
(%
)
100
90
80
70
60
50
40
30
20
10
00 4 8 12 16 20 24 28 32 36 40
Time to discontinuation of treatment (wk)
Dis
con
tin
uat
ion
bec
ause
of
Into
rela
bili
ty,
Ad
vers
e Ev
ents
, or
Dea
th(%
)
Antipsychotics in dementia CATIE-time to discontinuation
100
90
80
70
60
50
40
30
20
10
00 4 8 12 16 20 24 28 32 36 40
Time to discontinuation of treatment (wk)
Dis
con
tin
uat
ion
bec
ause
of
Lack
of
Effi
cacy
(%
)
Olanzapine (N=99)
Quetiapine (N=94)
Risperidone (N=84)
Placebo (N=139)

11
Antipsychotics – marked sensitivity and mortality
• FDA: 1.7-fold increase in mortality
• Schneider JAMA2005: 1.5-fold increased mortality risk
Aarsland D, et al. J Clin Psychiatry 2005;66:633–7; Schneider LS, et al. JAMA 2005;294:1934–43; http://www.fda.gov/medwatch/safety/2006/Sep_PIs/Symbyax_PI.pdf
53
39
27
10
10
20
30
40
50
60
% p
atients
with s
eve
re n
euro
leptic
sensi
tivi
ty r
eact
ion
*75–80% diagnosed by autopsy
p = 0.006
DLB(n = 15*)
PDD(n = 36)
PD(n = 26)
AD(n = 17*)

JAMA Psychiatry 2015
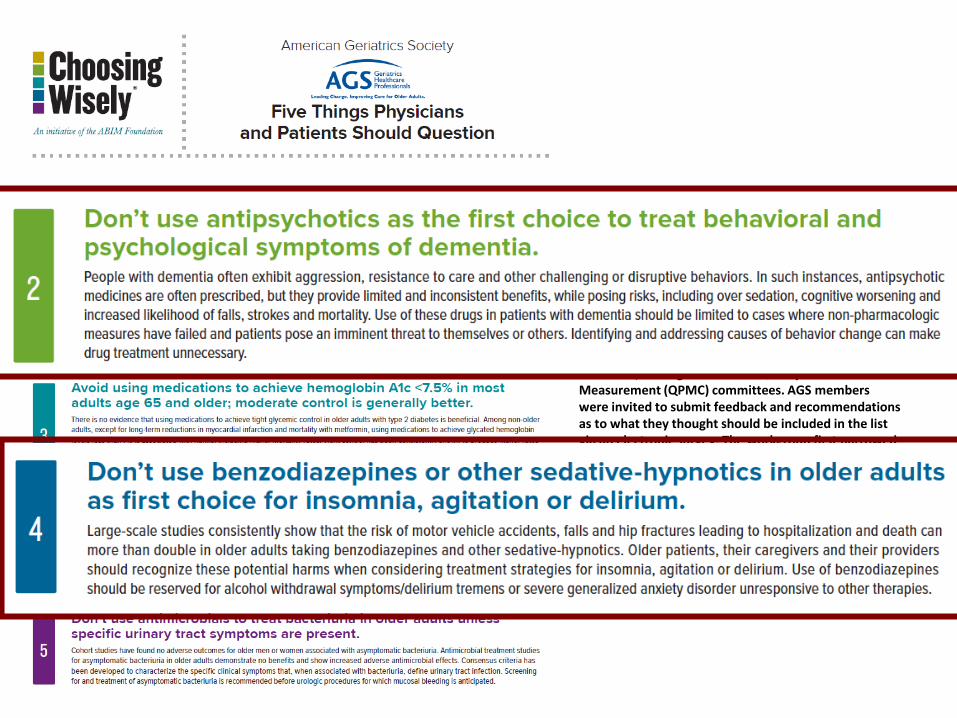
How This List Was CreatedThe American Geriatrics Society (AGS) established a work group chaired by the Vice Chair of Clinical Practice and Models of Care Committee (CPMC). Work groupmembers were drawn from that committee, as well as the Ethics, Ethnogeriatrics and Quality and Performance Measurement (QPMC) committees. AGS memberswere invited to submit feedback and recommendations as to what they thought should be included in the list via an electronic survey. The workgroup first narrowedthe list down to the top 10 potential tests or procedures. The workgroup then reviewed the evidence and sought expert advice to further refine the list to fiverecommendations, which were then reviewed and approved by the AGS Executive Committee and the Chairs/Vice Chairs of CPMC, Ethics and QPMC.


…e i trattamenti non farmacologici?

16
Special care units for BPSD management
Mean + SD
at baseline
Mean + SD
at 3 months
Mean + SD
at 6 months
P* P**
MMSE 6.1 +5.0 6.8 +6.1 6.2 +6.8 n.s. n.s.
Barthel Index 36.2 +26.3 39.7 +27.0 41.6 +28.2 n.s. n.s.
NPI 38.2 +16.5 29.2 +15.7 25.6 +16.7 .001 <.0005
Psychotropicdrugs
1.5 +.9 1.1 +.8 .8 +.8 <.0005 <.0005
Physicalrestraints
20 (36.4 %) -- 16 (29.0 %) -- .002
Bellelli G et al, Gerontologist, 1998
18
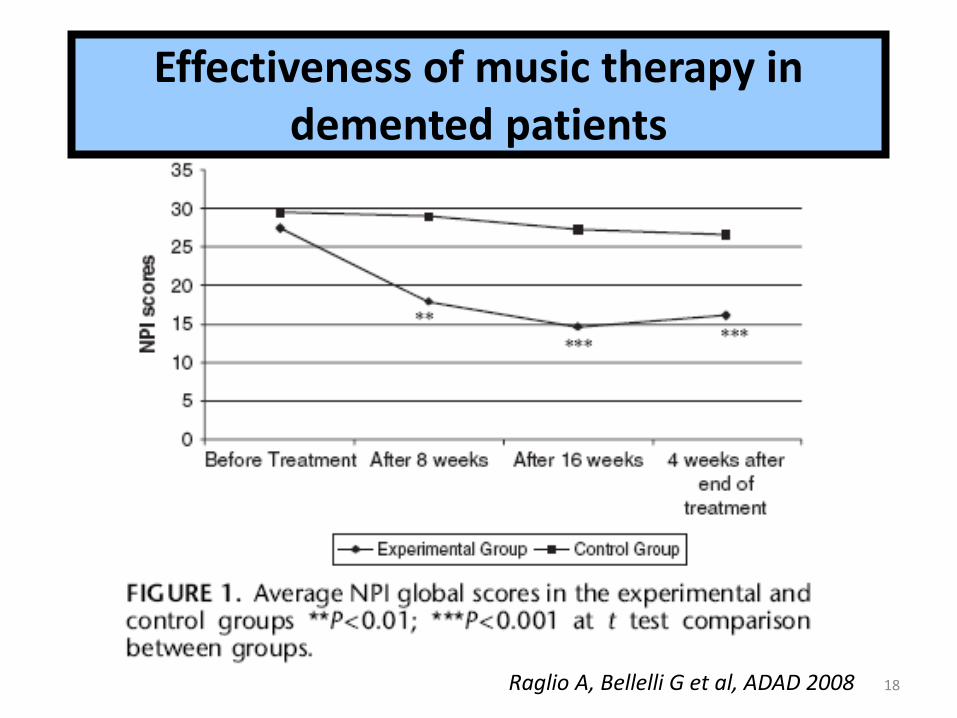
Effectiveness of music therapy in demented patients
Raglio A, Bellelli G et al, ADAD 2008

Do caregivers management strategies influence patient behavior in dementia?
De Vugt ME, Int J Geriatr Psych 2004
99 pazienti con demenza e caregiver informali seguiti per un annoSenso di competenza misurato con SSCQ e BPSD con NPI

Di Rosa M et al., Geriatr Gerontol Int 2016
• 928 patients not taking antipsychotics at admission in seven acute care wards of geriatric medicine in Italy (mean age 80.8 ± 7.2 years, 54.9%women).
• The outcome of the study was defined as receiving an antipsychotic prescription at discharge.
• Patients were grouped according to their living conditions as follows: (i) living alone; (ii) living only with care worker; (iii) living with care worker and family members; and (iv) living only with family members.

• Community-dwelling patients aged 65 years or older, with mild-to-moderate dementia, and their informal caregivers (135 couples of patients with their caregivers) randomly assigned to 10 sessions of occupational therapy over 5 weeks or no intervention.
• Outcome measures: patients’ and caregivers’ quality of life (Dementia Quality of Life Instrument, Dqol), patients’ mood (Cornell Scale for Depression, CSD), caregivers’ mood (Center for Epidemiologic Studies Depression Scale, CES-D)
Graff MJ et al., J Gerontol Biol Med Sci, 2007
Nuove prospettive terapeutiche
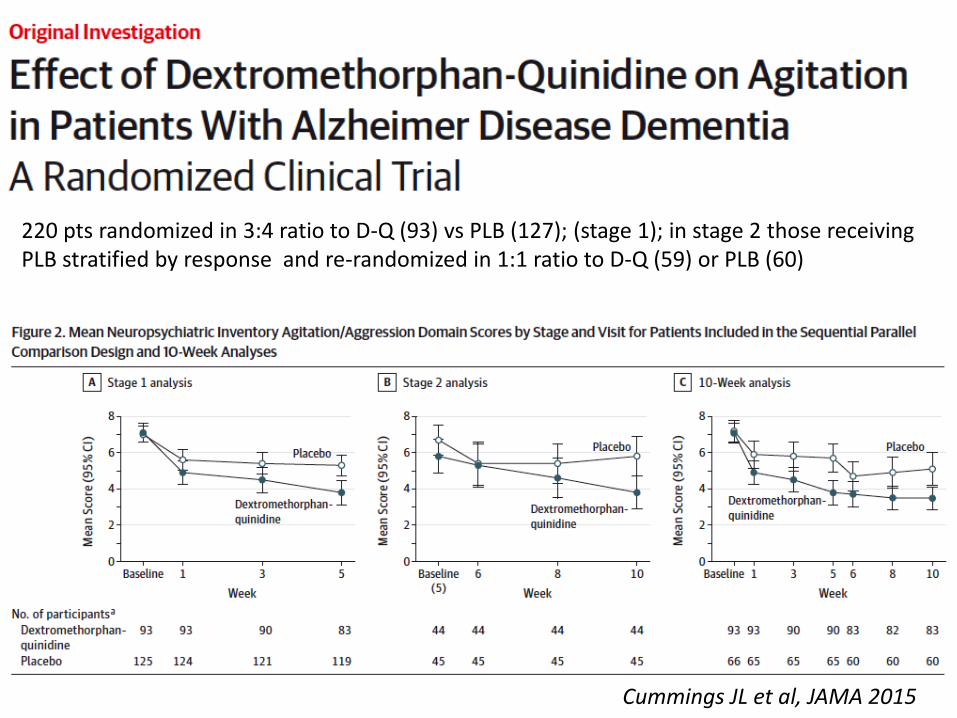
Cummings JL et al, JAMA 2015
220 pts randomized in 3:4 ratio to D-Q (93) vs PLB (127); (stage 1); in stage 2 those receiving PLB stratified by response and re-randomized in 1:1 ratio to D-Q (59) or PLB (60)
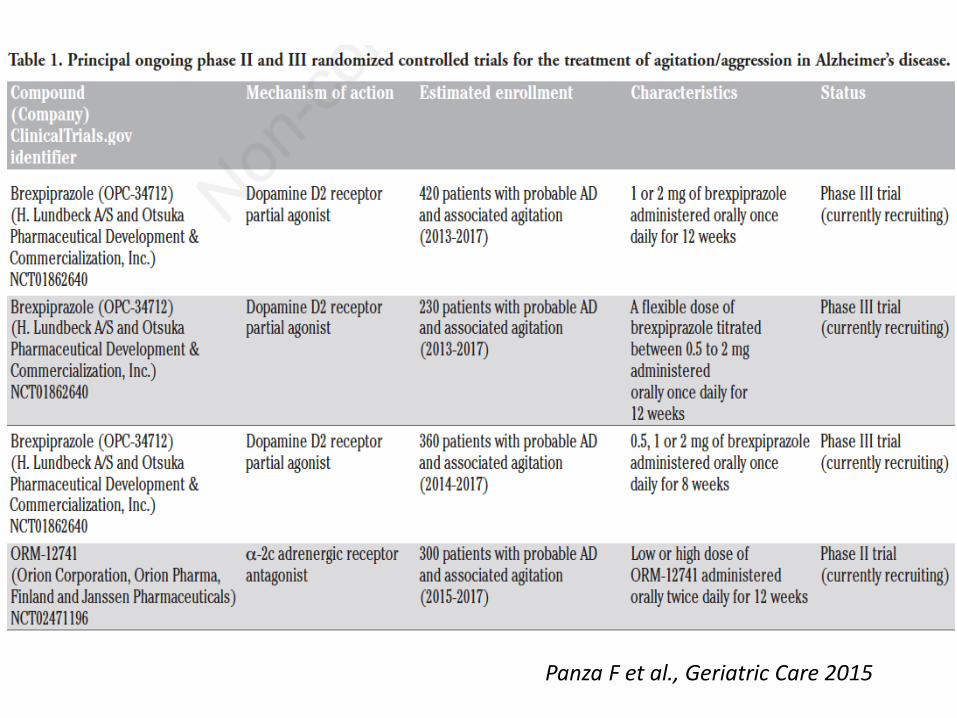
Panza F et al., Geriatric Care 2015

e nel frattempo?

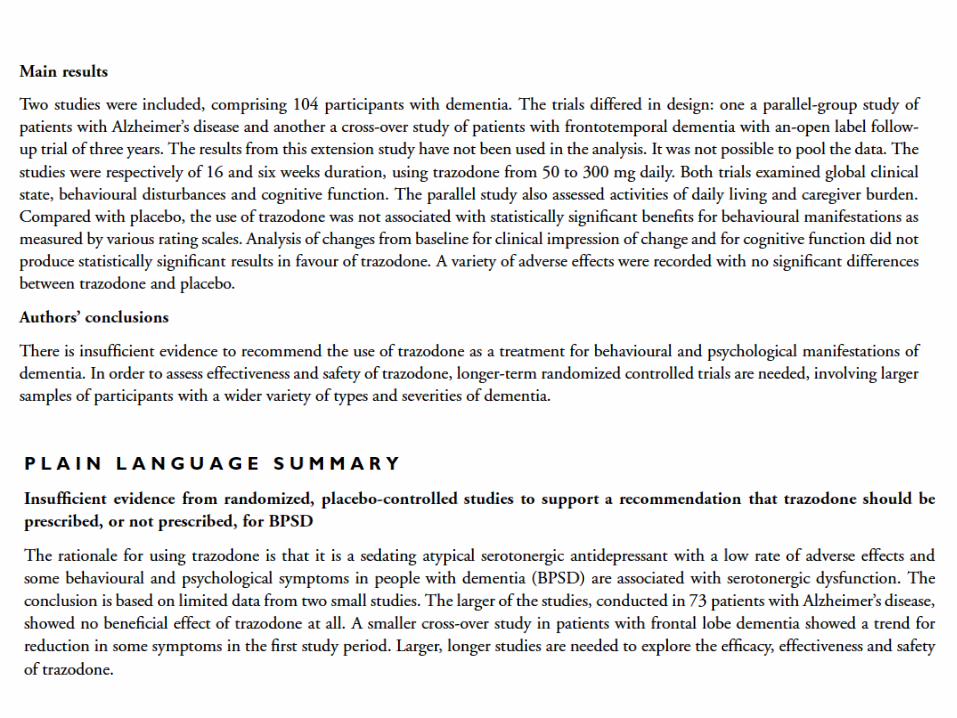
Trazodone e i bassi dosaggi
A basse dosi (25-150 mg):-blocco 5-HT2A,-arruolamento progressivo di α1 adrenergici e H1 istaminergici
Miglioramento del profilo sedativo-ipnotico
≤150mg

• Design: Randomized, double-blind, parallel-group, 9-week treatment trial.
• Setting: Inpatient geropsychiatry unit.
• Intervention: Haloperidol 1 to 5 mg/day or trazodone 50 to 250 mg/day.
• Measurements: CMAI and delusions (through subscale of BEHAVE-AD)
J Am Geriatr Soc 2001
Serotonergic mechanisms may improve aggression with atypical antipsychotic treatment

Trazodone Improves Sleep Parameters in Alzheimer Disease Patients: A Randomized, Double-Blind, and Placebo-Controlled
Study
• Design: double-blind, RCT during periods of 7–9 days at baseline and 2 weeks of treatment.
• Setting: Geriatric medical center.• Participants: 30 individuals with probable AD and SD assigned
to either the active treatment group (N = 15) or the placebo group (N = 15).
• Intervention: 50 mg of trazodone once daily at 10:00 P.M. or placebo in a 1:1 ratio for 2 weeks.
• Measurements: actigraphy and structured scales before and after intervention.
• Results: Trazodone users slept 42.5 more minutes per night and had their nighttime percent sleep increased 8.5 percentage points according to actigraphic data post-treatment.
Camargos E, Am J Geriatr Psych 2014

Conclusioni
• La depressione nell’anziano affetto da demenza è un fenomeno biologico probabilmente diverso da quello dell’anziano cognitivamente integro– I farmaci sono inefficaci
• I neurolettici e le benzodiazepine sono farmaci pericolosi per la salute e inefficaci sui BPSD (non dovrebbero essere usati)
• L’approccio non farmacologico va sempre ricercato– Terapista occupazionale/educazione caregiver?
• Se insonnia/agitazione/affaccendamento afinalistico usa farmaci maneggevoli e sicuri (es trazodone) (25-75 RP, eventualmente con l’aggiunta di equivalenti melatonina)
• …..in attesa di destrometorfano/chinidina e brexpiprazolo





























