Embed Size (px)
Citation preview
DES or maybe BMS ?
Prof. Dr. Helmut Schühlen, FESC, FACC
Vivantes Auguste-Viktoria-Klinikum
Berlin, Germany
Conflict of Interest Statement
Prof. Dr. Helmut Schühlen, FESC, FACC
Research support, speaker‘s or consulting honoraria from:
Astra Zeneca Abbott
Bayer Biotronik
Boehringer Ingelheim Bristol Myers-Squibb
Correvio Daiichi-Sankyo
Lilly Novartis
Prof. Dr. Helmut Schühlen, FESC, FACC
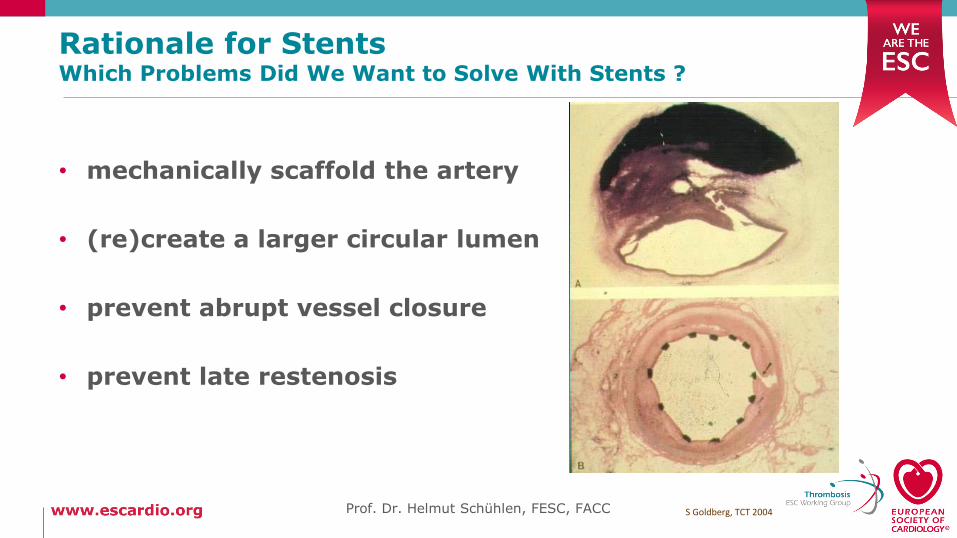
Rationale for StentsWhich Problems Did We Want to Solve With Stents ?
• mechanically scaffold the artery
• (re)create a larger circular lumen
• prevent abrupt vessel closure
• prevent late restenosis
S Goldberg, TCT 2004Prof. Dr. Helmut Schühlen, FESC, FACC
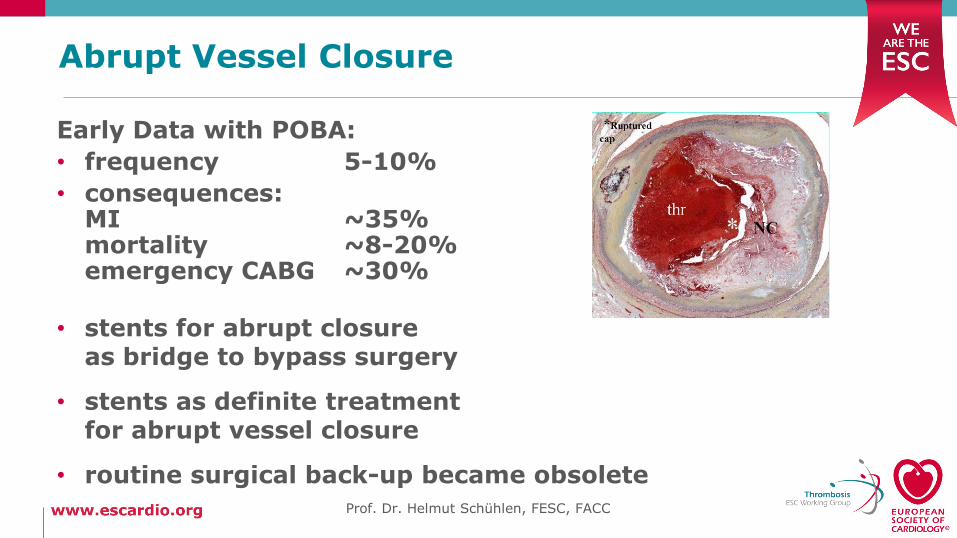
Abrupt Vessel Closure
Early Data with POBA:
• frequency 5-10%
• consequences:MI ~35%mortality ~8-20%emergency CABG ~30%
• stents for abrupt closureas bridge to bypass surgery
• stents as definite treatmentfor abrupt vessel closure
• routine surgical back-up became obsolete
Prof. Dr. Helmut Schühlen, FESC, FACC
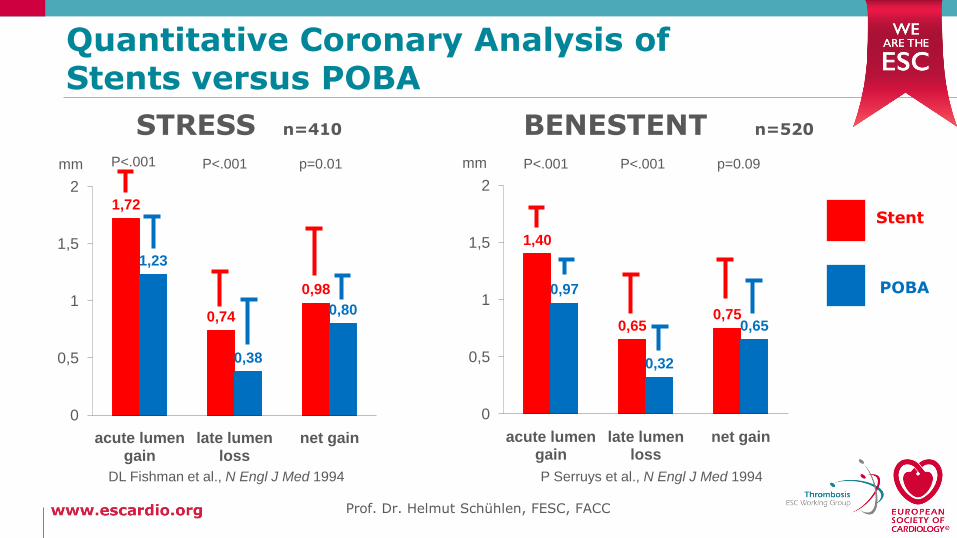
Quantitative Coronary Analysis ofStents versus POBA
STRESS n=410 BENESTENT n=520
P Serruys et al., N Engl J Med 1994
1,72
0,74
0,98
1,23
0,38
0,80
0
0,5
1
1,5
2
acute lumen gain
late lumen loss
net gain
mm P<.001
DL Fishman et al., N Engl J Med 1994
P<.001 p=0.01
1,40
0,650,75
0,97
0,32
0,65
0
0,5
1
1,5
2
acute lumen gain
late lumen loss
net gain
mm P<.001 P<.001 p=0.09
POBA
Stent
Prof. Dr. Helmut Schühlen, FESC, FACC
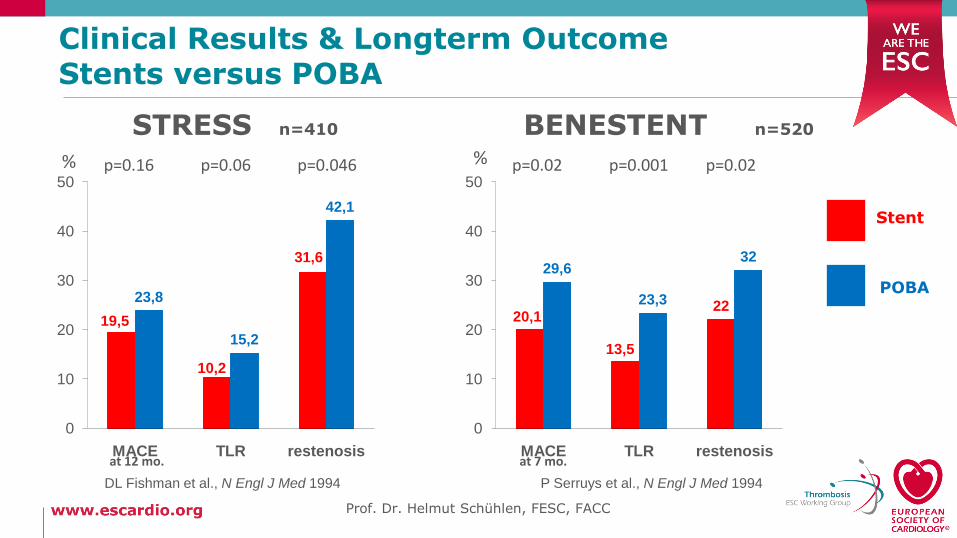
Clinical Results & Longterm OutcomeStents versus POBA
19,5
10,2
31,6
23,8
15,2
42,1
0
10
20
30
40
50
MACE TLR restenosis
% p=0.16 p=0.06 p=0.046
20,1
13,5
22
29,6
23,3
32
0
10
20
30
40
50
MACE TLR restenosisat 12 mo. at 7 mo.
p=0.02 p=0.001 p=0.02%
STRESS n=410 BENESTENT n=520
P Serruys et al., N Engl J Med 1994DL Fishman et al., N Engl J Med 1994
POBA
Stent
Prof. Dr. Helmut Schühlen, FESC, FACC
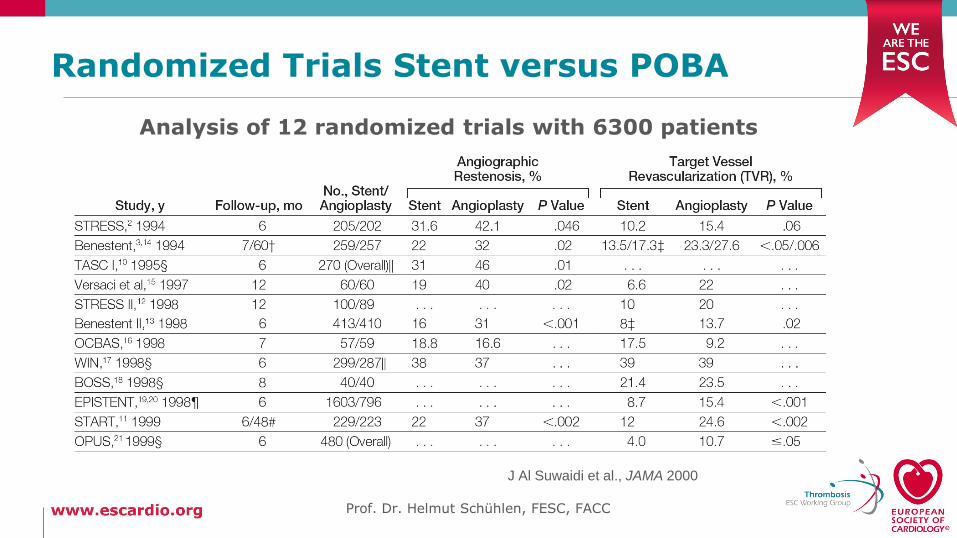
Randomized Trials Stent versus POBA
Prof. Dr. Helmut Schühlen, FESC, FACC
J Al Suwaidi et al., JAMA 2000
Analysis of 12 randomized trials with 6300 patients
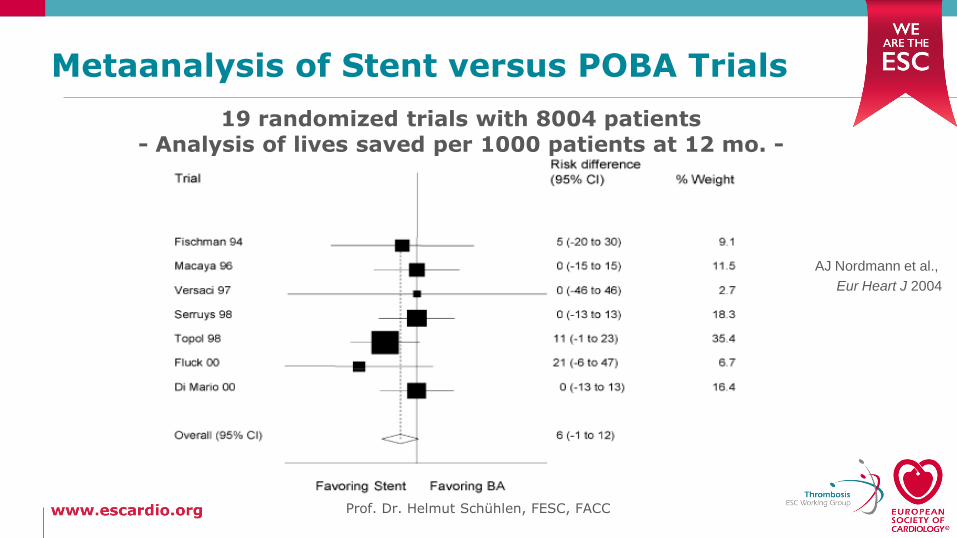
Metaanalysis of Stent versus POBA Trials
AJ Nordmann et al.,
Eur Heart J 2004
19 randomized trials with 8004 patients- Analysis of lives saved per 1000 patients at 12 mo. -
Prof. Dr. Helmut Schühlen, FESC, FACC
Initial Experience with DES
Prof. Dr. Helmut Schühlen, FESC, FACC
JE Sousa et al., Circulation 2001
The real target isnot BMS vs. DES,
it‘s surgery.
Interview at ACC 2003, www.theheart.org
Prof. Dr. Helmut Schühlen, FESC, FACC
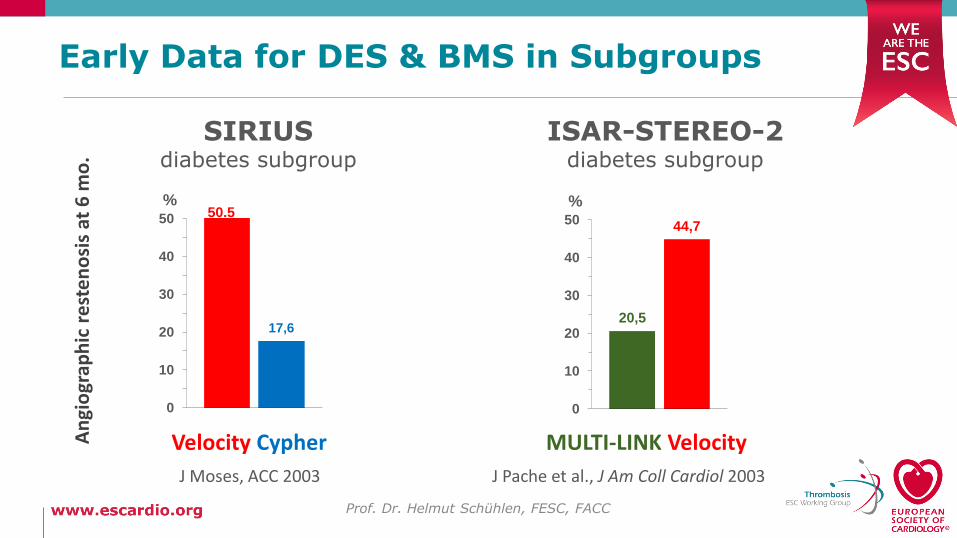
Early Data for DES & BMS in Subgroups
17,6
0
10
20
30
40
50
%50.5
SIRIUSdiabetes subgroup
Velocity CypherAn
gio
grap
hic
rest
en
osi
sat
6 m
o.
J Moses, ACC 2003
20,5
44,7
0
10
20
30
40
50
%
VelocityMULTI-LINK
ISAR-STEREO-2diabetes subgroup
J Pache et al., J Am Coll Cardiol 2003
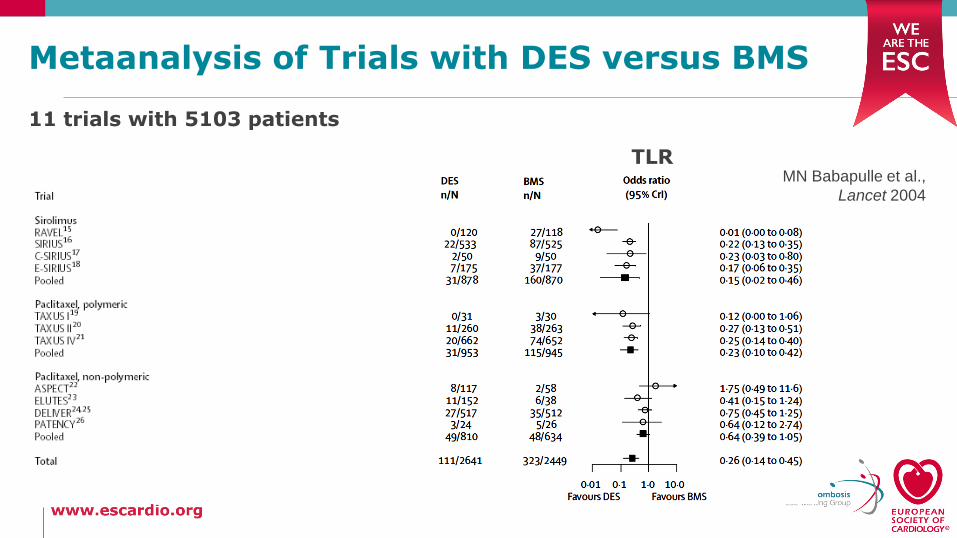
Metaanalysis of Trials with DES versus BMS
11 trials with 5103 patients
mortality TLRMN Babapulle et al.,
Lancet 2004
The Debate at ESC 2006
Prof. Dr. Helmut Schühlen, FESC, FACC
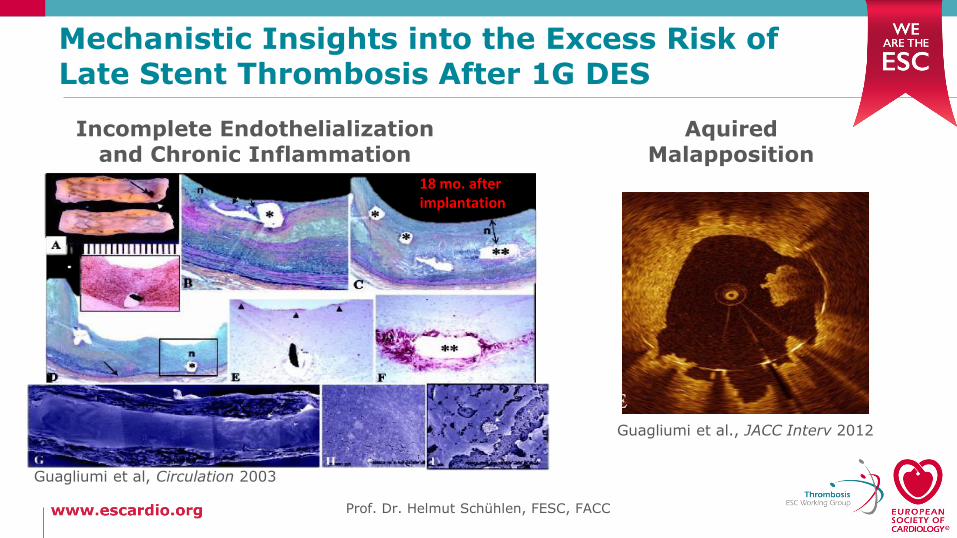
Mechanistic Insights into the Excess Risk ofLate Stent Thrombosis After 1G DES
AquiredMalapposition
Incomplete Endothelializationand Chronic Inflammation
Guagliumi et al., JACC Interv 2012
Guagliumi et al, Circulation 2003
18 mo. after implantation
Prof. Dr. Helmut Schühlen, FESC, FACC
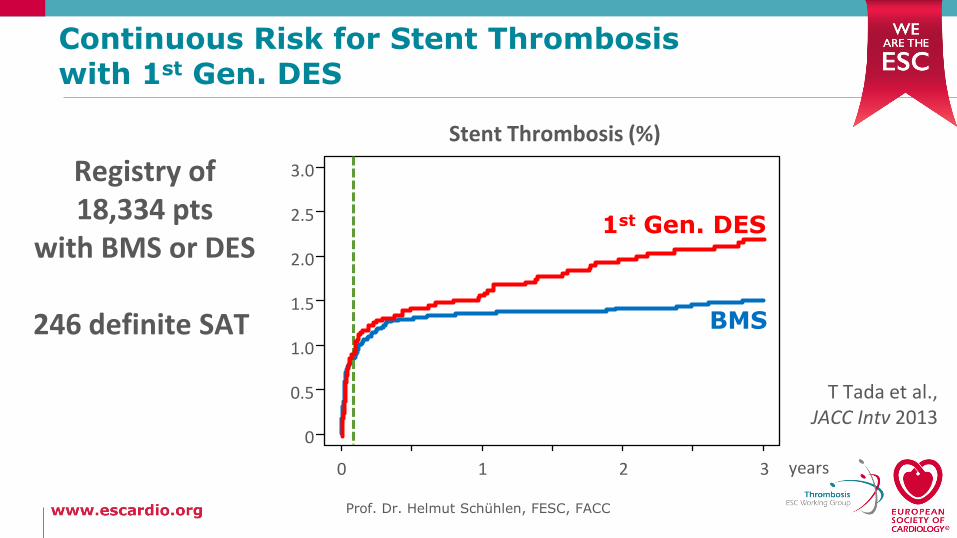
Continuous Risk for Stent Thrombosis with 1st Gen. DES
Stent Thrombosis (%)
Registry of18,334 pts
with BMS or DES
246 definite SAT
T Tada et al., JACC Intv 2013
years
0
0.5
1.0
2.0
3.0
0 1 2 3
1.5
2.5
BMS
1st Gen. DES
Prof. Dr. Helmut Schühlen, FESC, FACC
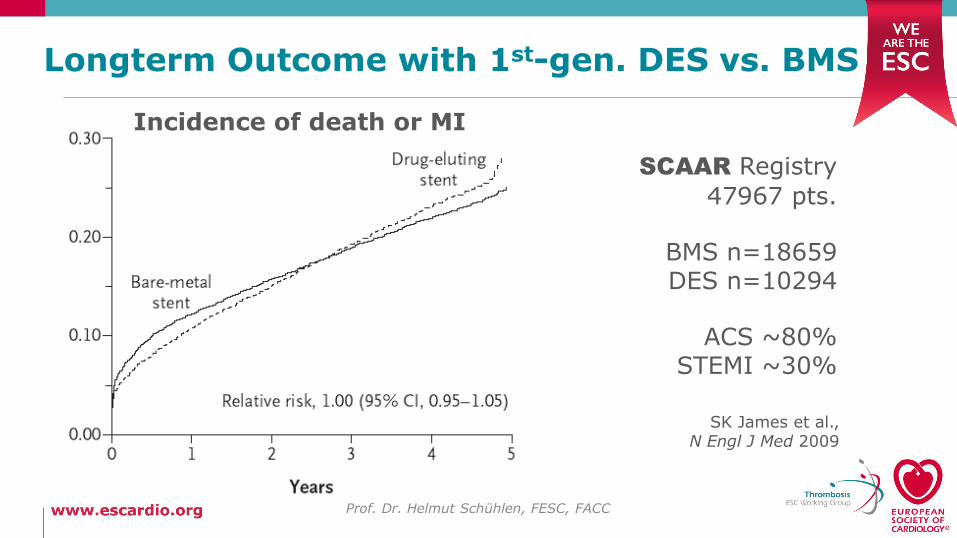
Longterm Outcome with 1st-gen. DES vs. BMS
Prof. Dr. Helmut Schühlen, FESC, FACC
SK James et al., N Engl J Med 2009
Incidence of death or MI
SCAAR Registry
47967 pts.
BMS n=18659DES n=10294
ACS ~80%STEMI ~30%
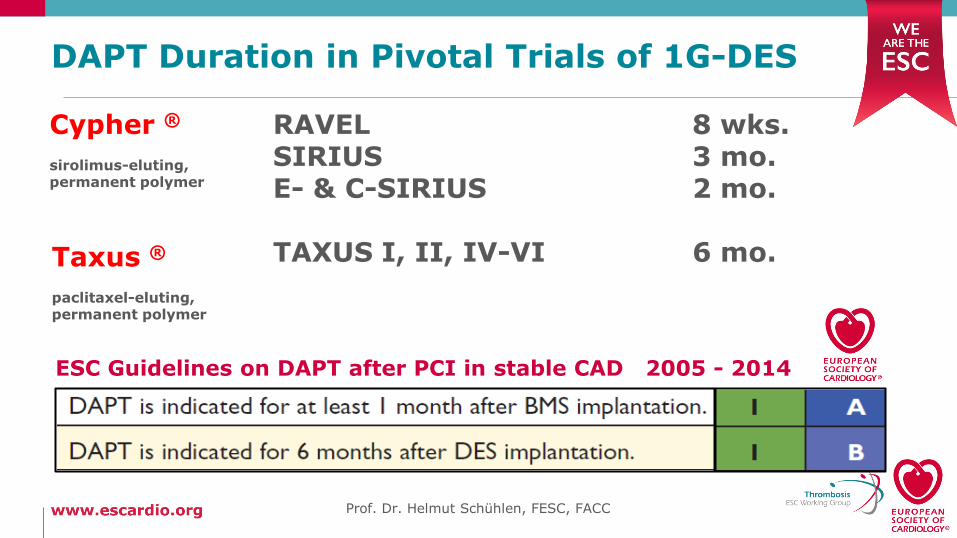
DAPT Duration in Pivotal Trials of 1G-DES
RAVEL 8 wks.SIRIUS 3 mo.E- & C-SIRIUS 2 mo.
TAXUS I, II, IV-VI 6 mo.
Cypher ®
sirolimus-eluting, permanent polymer
Taxus ®
paclitaxel-eluting, permanent polymer
Prof. Dr. Helmut Schühlen, FESC, FACC
ESC Guidelines on DAPT after PCI in stable CAD 2005 - 2014
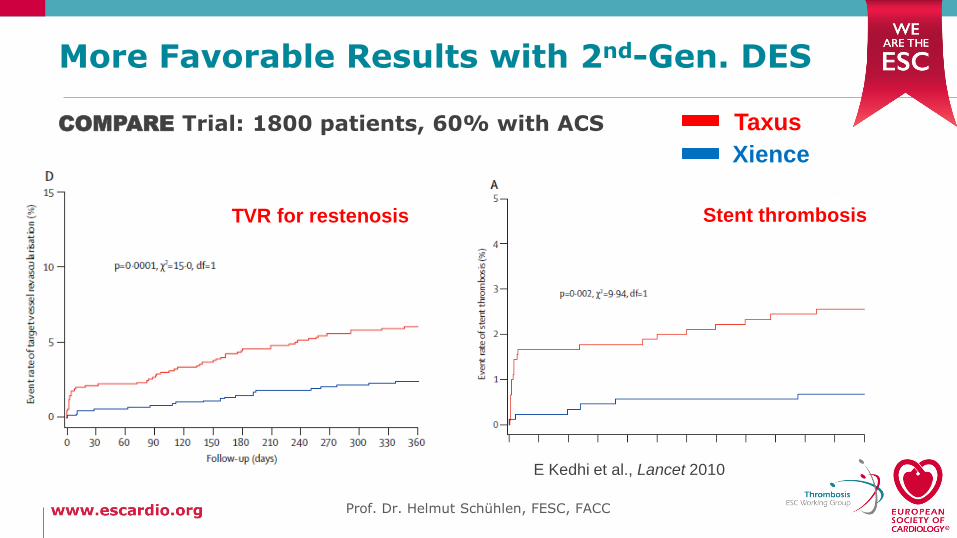
E Kedhi et al., Lancet 2010
Taxus
Stent thrombosis
Xience
TVR for restenosis
COMPARE Trial: 1800 patients, 60% with ACS
More Favorable Results with 2nd-Gen. DES
Prof. Dr. Helmut Schühlen, FESC, FACC
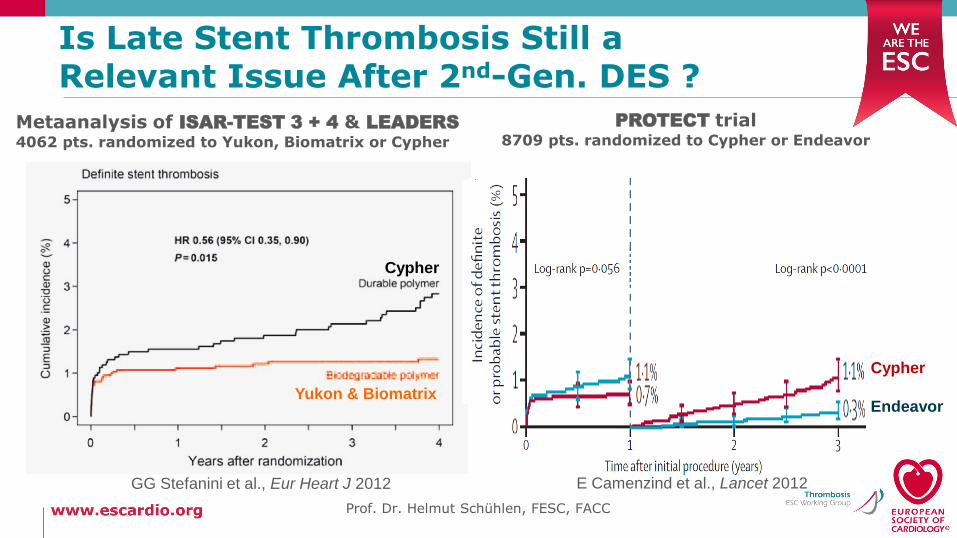
Is Late Stent Thrombosis Still a Relevant Issue After 2nd-Gen. DES ?
GG Stefanini et al., Eur Heart J 2012
Metaanalysis of ISAR-TEST 3 + 4 & LEADERS
4062 pts. randomized to Yukon, Biomatrix or Cypher
Endeavor
PROTECT trial 8709 pts. randomized to Cypher or Endeavor
Cypher
Yukon & Biomatrix
Cypher
E Camenzind et al., Lancet 2012
Prof. Dr. Helmut Schühlen, FESC, FACC
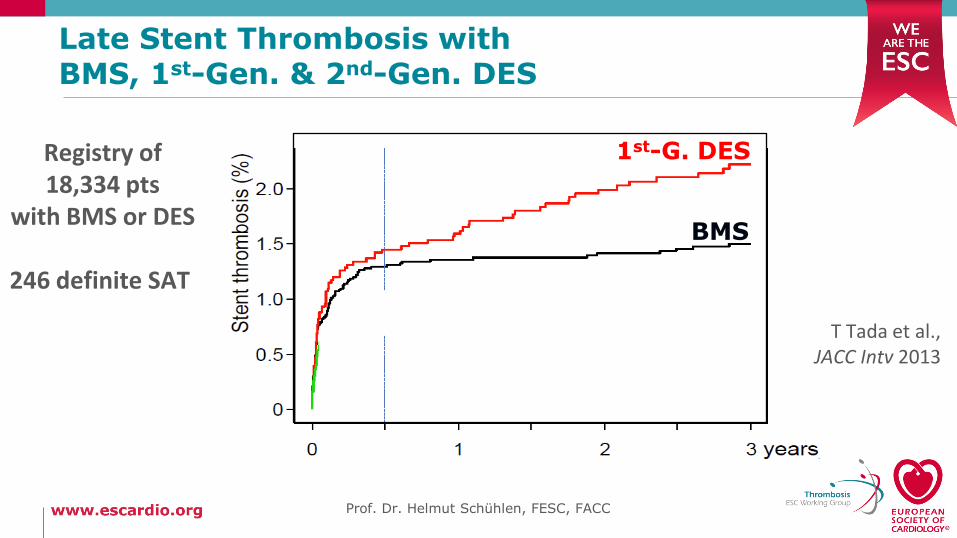
Late Stent Thrombosis with BMS, 1st-Gen. & 2nd-Gen. DES
1st-G. DES
BMS
2nd-G. DES
Registry of18,334 pts
with BMS or DES
246 definite SAT
T Tada et al., JACC Intv 2013
Prof. Dr. Helmut Schühlen, FESC, FACC
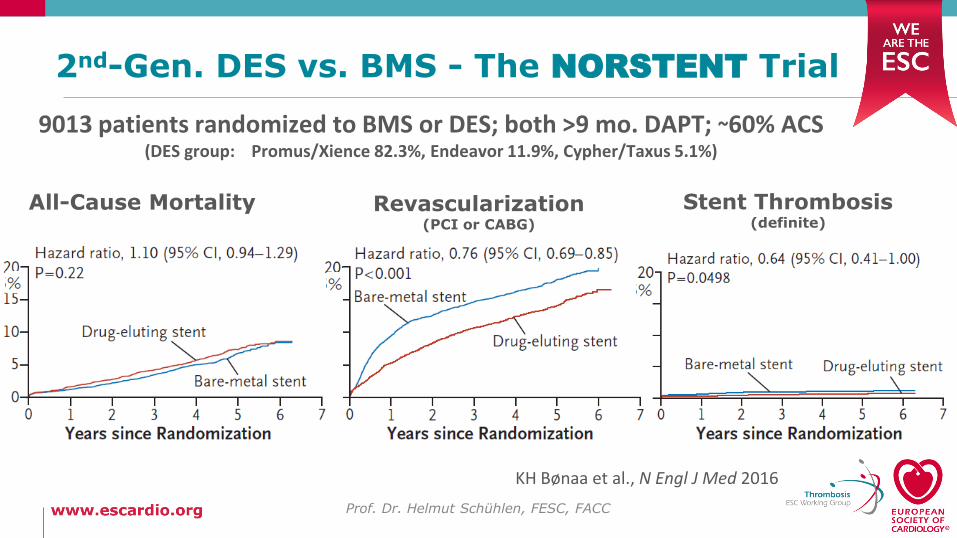
2nd-Gen. DES vs. BMS - The NORSTENT Trial
Prof. Dr. Helmut Schühlen, FESC, FACC
KH Bønaa et al., N Engl J Med 2016
9013 patients randomized to BMS or DES; both >9 mo. DAPT; ~60% ACS (DES group: Promus/Xience 82.3%, Endeavor 11.9%, Cypher/Taxus 5.1%)
All-Cause Mortality Revascularization(PCI or CABG)
Stent Thrombosis(definite)
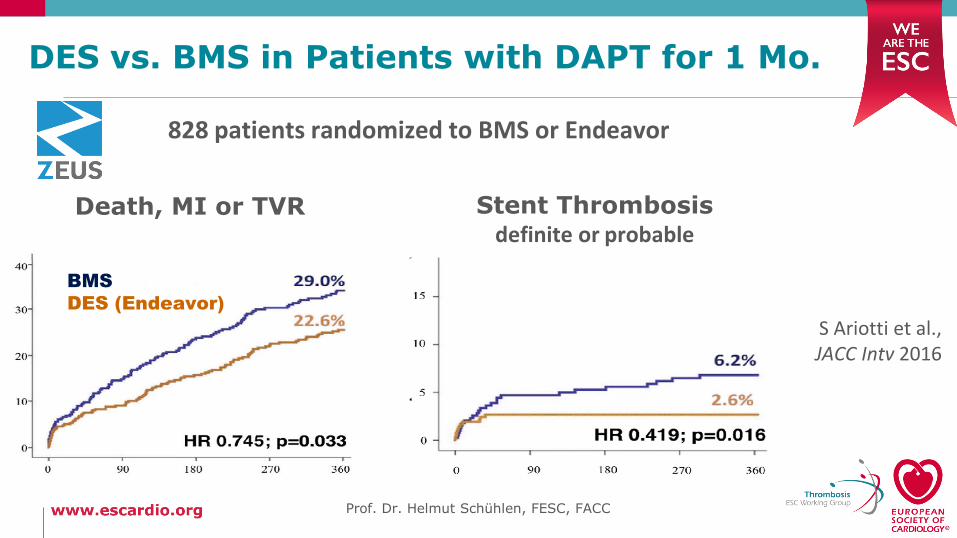
DES vs. BMS in Patients with DAPT for 1 Mo.
Stent Thrombosisdefinite or probable
Death, MI or TVR
BMS
DES (Endeavor)
828 patients randomized to BMS or Endeavor
S Ariotti et al.,JACC Intv 2016
Prof. Dr. Helmut Schühlen, FESC, FACC
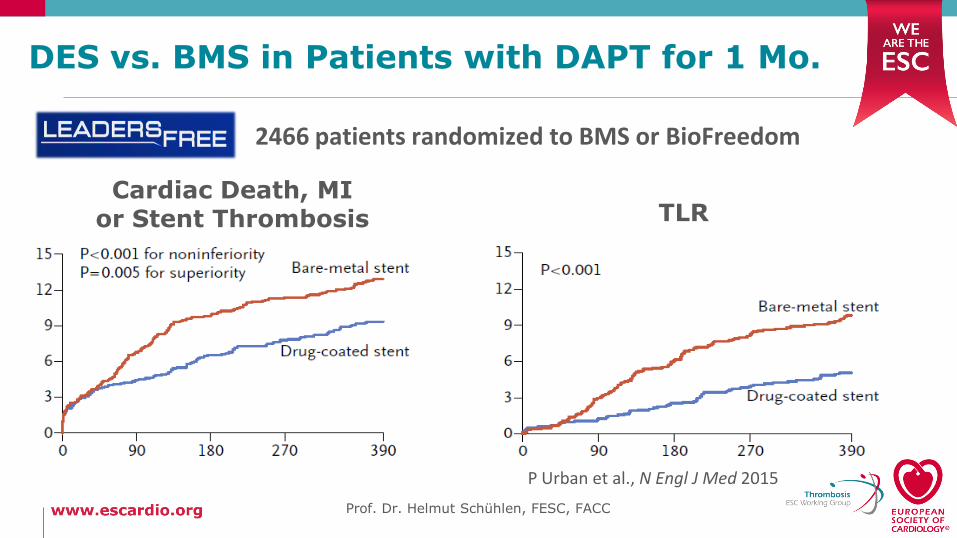
Cardiac Death, MI or Stent Thrombosis TLR
P Urban et al., N Engl J Med 2015
Prof. Dr. Helmut Schühlen, FESC, FACC
DES vs. BMS in Patients with DAPT for 1 Mo.
2466 patients randomized to BMS or BioFreedom
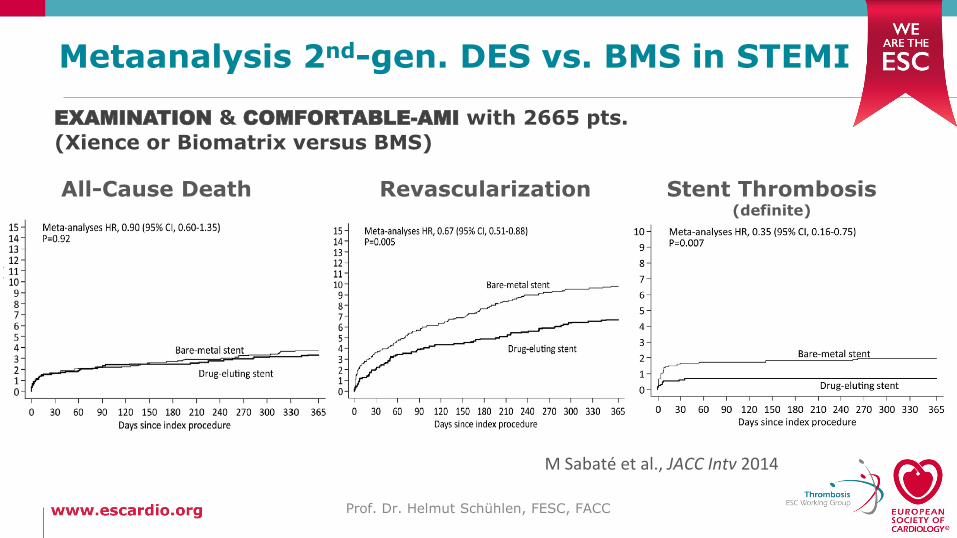
Metaanalysis 2nd-gen. DES vs. BMS in STEMI
Prof. Dr. Helmut Schühlen, FESC, FACC
M Sabaté et al., JACC Intv 2014
EXAMINATION & COMFORTABLE-AMI with 2665 pts.
(Xience or Biomatrix versus BMS)
All-Cause Death Revascularization Stent Thrombosis(definite)
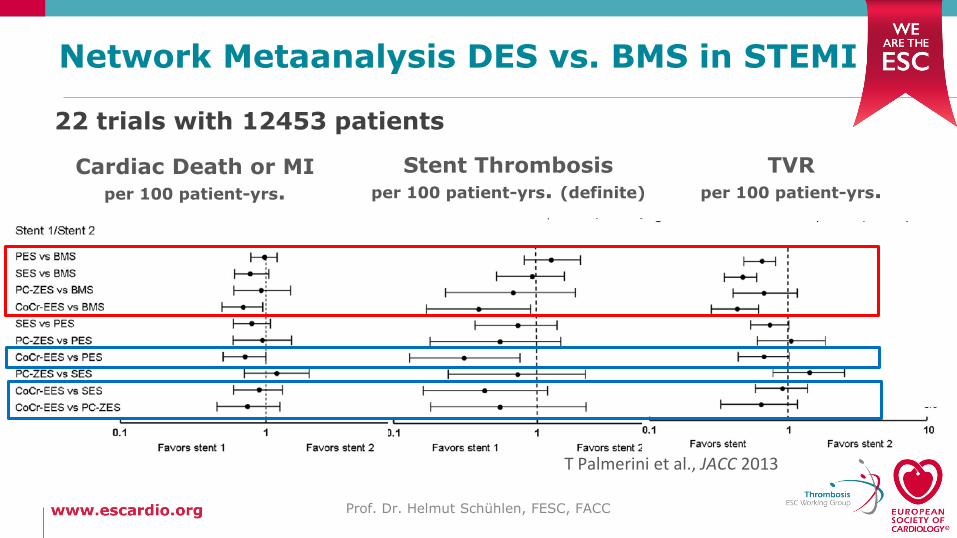
Network Metaanalysis DES vs. BMS in STEMI
Prof. Dr. Helmut Schühlen, FESC, FACC
T Palmerini et al., JACC 2013
22 trials with 12453 patients
Cardiac Death or MI per 100 patient-yrs.
Stent Thrombosisper 100 patient-yrs. (definite)
TVRper 100 patient-yrs.
Summary
Mortality is better perceived as the target for themandatory & well-established longterm medical therapy.
Stents have revolutionized & simplified PCI.
Stents (BMS) increase the proliferative response to PTCA.
1st-gen. DES diminished this proliferative response at thecost of deficient healing & a continuous thrombotic risk.
“3rd“gen. DES are safer than BMS, even with 1 mo. DAPT.
Prof. Dr. Helmut Schühlen, FESC, FACC
Prof. Dr. Helmut Schühlen, FESC, FACC
Our opinion of these data is that there is a clearbenefit from DES… and that this benefit is inde-pendent of the clinical indication. …In 2016 implantation of BMS is no longer justified. We suggest that BMS should be honourably retiredand added to the history books that document theevolution of interventional therapies.

Prof. Dr. Helmut Schühlen, FESC, FACC





























