Embed Size (px)
Citation preview
PONTIFÍCIA UNIVERSIDADE CATÓLICA DE MINAS GERAIS
Programa de Pós-graduação em Odontologia
DETECÇÃO DE FRATURA RADICULAR EM DENTES COM PINO
METÁLICO POR MEIO DE RADIOGRAFIA PERIAPICAL E
TOMOGRAFIA COMPUTADORIZADA
PRISCILA DIAS PEYNEAU
Belo Horizonte
2011

Priscila Dias Peyneau
DETECÇÃO DE FRATURA RADICULAR EM DENTES COM PINO
METÁLICO POR MEIO DE RADIOGRAFIA PERIAPICAL E
TOMOGRAFIA COMPUTADORIZADA
Dissertação apresentada ao Programa de Pós-graduação em Odontologia da Pontifícia Universidade Católica de Minas Gerais, como requisito parcial para obtenção do título de Mestre em Odontologia, área de concentração em Clínicas Odontológicas - Ênfase: Radiologia Odontológica e Imaginologia
Orientador: Prof. Dr. Flávio Ricardo Manzi
Belo Horizonte
2011
FICHA CATALOGRÁFICA Elaborada pela Biblioteca da Pontifícia Universidade Católica de Minas Gerais
Peyneau, Priscila Dias P515d Detecção de fratura radicular em dentes com pino metálico por meio de
radiografia periapical e tomografia computadorizada / Priscila Dias Peyneau. Belo Horizonte, 2011.
51f. : il. Orientador: Flávio Ricardo Manzi Dissertação (Mestrado) – Pontifícia Universidade Católica de Minas Gerais.
Programa de Pós-Graduação em Odontologia. 1. Fraturas de dentes - Diagnóstico. 2. Radiografia dentária digital. 3.
Tomografia computadorizada. I. Manzi, Flávio Ricardo. II. Pontifícia Universidade Católica de Minas Gerais. Programa de Pós-Graduação em Odontologia. III. Título.
CDU: 616.314-001.5

FOLHA DE APROVAÇÃO
AGRADECIMENTOS
À Deus por iluminar o meu caminho e me conceder sabedoria.
Aos meus pais, Hermes Peyneau e Mariza Rubim Dias Peyneau , pelo incentivo,
amor e dedicação nesta longa jornada da vida. Vocês foram fundamentais para mais
esta conquista.
Aos meus irmãos e cunhados , amigos e familiares, pelo apoio e carinho.
Às amigas, Adriana Maria de Andrade e Morgana Neves , pela amizade e pelo
carinho com que me acolheram.
Aos amigos da VIII turma do Mestrado Acadêmico em Odontologia da Pontifícia
Universidade Católica de Minas Gerais, pelos momentos alegres, intensos e difíceis
que passamos neste período de convivência. Hoje podemos dizer: vencemos!
Às minhas companheiras da Radiologia, Claudia Sgliano Valério e Andréia Cruz
Pires Ribeiro de Sousa , não tenho palavras para descrever o carinho com que me
receberam! Obrigada pela amizade, compreensão, simpatia e disponibilidade.
Aos Professores do Programa de Mestrado em Odontologia da Pontifícia
Universidade Católica de Minas Gerais, pelo conhecimento transmitido.
Ao Prof. Dr. Rogério A. Azeredo , pela amizade e pelo incentivo à pesquisa.
Em especial, ao meu orientador, Prof. Dr. Flávio Ricardo Manzi , pela dedicação,
confiança, amizade e incentivo à carreira acadêmica.
Á Axial Centro de Imagens , Axial Odonto , Digiface, Radiscan , Radiodonto , e ao
Prof. Arnaldo Horácio Pereira pela colaboração no meu crescimento profissional.
EPÍGRAFE
Bem-aventurado o homem que acha sabedoria, e o homem
que adquire conhecimento; Porque é melhor a sua
mercadoria do que artigos de prata, e maior o seu lucro
que o ouro mais fino. Mais preciosa é do que os rubis, e
tudo o que mais possas desejar não se pode comparar a
ela. (Provérbios 3:13-15).
RESUMO
O objetivo deste trabalho foi comparar o diagnóstico de fraturas radiculares em
dentes com pino metálico intra-canal através de radiografias periapicais
convencionais, radiografias periapicais digitais através do sensor CCD (charge-
coupled device) e placa de fósforo (PSP), além de tomografia computadorizada
multislice (TC multislice) e tomografia computadorizada cone beam (TCCB). Trinta
dentes extraídos, unirradiculares, tratados endodonticamente e com pino metálico
intra-canal foram utilizados como amostra. Na primeira fase de aquisição das
imagens estes dentes não apresentavam fratura. Em um segundo momento, os
mesmos dentes foram fraturados com a pressão de uma cunha e a aquisição das
imagens foi realizada mais uma vez. Três especialistas em radiologia odontológica,
com experiência em tomografia computadorizada e imagem digital avaliaram as
imagens. A sensibilidade (90%) e a especificidade (95%) foram calculadas usando a
curva ROC e os melhores resultados encontrados foram para as imagens realizadas
com PSP e que puderam ser manipuladas. As imagens obtidas com as radiografias
digitais sem manipulação, nos dois sistemas, e as imagens tomográficas obtidas nos
dois tomógrafos, não apresentaram diferença estatisticamente significante entre si
(CCD: 0,467-0,729, PSP: 0,5388-0,8112, TCCB: 0,5445-0,8155, TC multislice:
0,5544-0,8202), entretanto apresentaram diferença estatisticamente significante
quando comparadas com as radiografias periapicais convencionais e digitais com
manipulação (convencional: 0,7248-0,9352, CCD: 0,7442 -0,9458, PSP: 0,8541-
0,9959). Sendo assim, as imagens tomográficas não são adequadas para verificar a
ausência da fratura, pois o artefato do metal causado pelo núcleo metálico faz o
avaliador perceber fraturas em raízes hígidas (falso positivo). Para avaliação da
presença de fraturas radiculares em dentes com pino metálico intra-canal, indica-se
a utilização das imagens radiográficas digitais. Os sistemas digitais (CCD e PSP)
obtiveram os maiores valores de sensibilidade, especificidade e acurácia para esta
condição.
Palavras-chave : Diagnóstico. Fraturas dos dentes. Radiografia dentária digital.
Tomografia computadorizada por raios X.
ABSTRACT
The purpose of this study was to compare the diagnosis of root fractures in teeth with
intracanal metallic posts by means of conventional periapical, digital charge-coupled
device (CCD) and phosphor plate (PSP), and multislice CT and cone beam (CBCT).
Sample consisted of 30 extracted single-rooted, endodontically treated teeth and
intracanal metallic posts. In the first phase of image acquisition, these teeth showed
no fracture. In a second step, the same teeth were fractured by wedge pressure and
image acquisition was performed again. Three dental radiology experts with
experience in digital imaging and computed tomography evaluated the images. The
sensitivity (90%) and specificity (95%) was calculated using the ROC curve and the
best results were obtained for images acquired by PSP, which could be manipulated.
Images obtained with digital radiography without manipulation, in both systems, and
tomographic images obtained in the two scanners showed no statistically significant
differences between them (CCD: 0.467-0.729, PSP: 0.5388-0.8112, CBCT: 0.5445-
0,8155, CT multislice: 0.5544-0.8202), however there were statistically significant
differences when they were compared with conventional periapical radiographs and
digital manipulation (conventional:0.7248-0.9352, CCD:0.7442-0.9458, PSP:0.8541-
0.9959). Therefore, CT imaging is not adequate for verifying the absence of fracture,
since the metal artifact caused by a metallic post makes the evaluator see fractures
in healthy roots (false positive). To evaluate the presence of root fractures in teeth
with intracanal metallic posts, the use of digital radiographic images is indicated.
Digital systems (CCD and PSP) showed the highest sensitivity, specificity and
accuracy for this condition.
Keywords: Diagnosis. Digital dental radiography. Fracture of the teeth. X-ray
computed tomography.
LISTA DE ABREVIATURAS
CCD - Charge-coupled device
PSP – Placa de fósforo
TCCB - Tomografia computadorizada cone beam
TC – Tomografia computadorizada
SUMÁRIO
1. INTRODUÇÃO ...............................................................................................................................9
2. OBJETIVOS ................................................................................................................................ 12
3. MATERIAIS E MÉTODOS ........................................................................................................ 13
3.1 Preparação da amostra ............................................................................................................ 13
3.2 Aquisição das imagens ............................................................................................................ 14
3.2.1 Radiografia periapical ........................................................................................................... 14
3.2.2 Tomografia Computadorizada ............................................................................................ 15
3.3 Preparação da amostra (após a aquisição das ima gens) ............................................... 17
3.4 Avaliação das imagens ............................................................................................................ 17
ARTIGOS ............................................................................................................................................ 21
REFERÊNCIAS .................................................................................................................................. 50
9
1 INTRODUÇÃO
O diagnóstico da fratura radicular representa um desafio para o cirurgião-
dentista, e é um procedimento importante para avaliar o prognóstico e determinar o
tratamento adequado para o dente. Este tipo de lesão do órgão dentário
compreende entre 0,5 a 7% dos traumatismos que afetam os dentes permanentes
(ANDREASEN, 1981). Dentre alguns fatores etiológicos que podem causar as
fraturas, pode-se citar: o trauma físico, o trauma oclusal, os hábitos parafuncionais
repetitivos de estresse mastigatório, a reabsorção patológica induzindo uma fratura
radicular, além de iatrogenias que ocorrem durante e após o tratamento
endodôntico, como por exemplo, a instalação de pinos metálicos ou a pressão para
adaptá-los (YOUSSEFZADEH et al., 1999; MORA et al. 2007; KAMBUROGLU et al.,
2010).
A radiografia periapical é utilizada como exame inicial no diagnóstico de
fraturas radiculares e ideal para avaliar o órgão dental no que diz respeito à coroa,
raiz e suas estruturas adjacentes. Dentre as características radiográficas para o
diagnóstico de fraturas, pode-se notar uma linha radiolúcida entre os fragmentos ou
a separação dos mesmos, além do aumento do espaço do ligamento periodontal e
da perda óssea localizada. Porém, esta técnica radiográfica possui limitações, como
por exemplo, a sobreposição de estruturas adjacentes. Além disso, o feixe central de
raios X tem que passar paralelamente a linha de fratura para que a mesma seja
identificada (MORA et al., 2007; BERNARDES et al., 2009; HASSAN et al., 2009;
IIKUBO et al., 2009; KAMBUROGLU; CEBECI; GRONDAHL, 2009). Devido a isto,
muitas vezes é necessário que sejam feitas várias radiografias em ângulos
diferentes para conclusão da hipótese diagnóstica (BRANDINI et al., 2009;
KAMBUROGLU; CEBECI; GRONDAHL, 2009).
A radiografia convencional vem sendo substituída pelo sistema digital, que
também fornece imagem bidimensional e sobreposição de estruturas adjacentes.
Porém, a radiografia digital possui a vantagem de ser visualizada em tempo real,
economizando tempo e eliminando o uso de produtos químicos (reveladores e
fixadores) que são prejudiciais ao meio ambiente, e também permite a manipulação
(ampliação e alteração de brilho e contraste), armazenamento e envio das imagens
10
para outros profissionais (KOSITBOWORNCHAI et al., 2003; KAMBUROGLU;
CEBECI; GRONDAHL, 2009).
Com a descoberta da Tomografia Computadorizada em 1972 por Hounsfield e
Cormack, houve uma revolução na área médica em relação aos diagnósticos por
imagem. Muitas gerações de tomógrafos foram utilizadas até chegar ao tomógrafo
multislice, no qual o gantry possui várias fileiras de sensores permitindo rápida
aquisição de imagem. Através de reconstruções em terceira dimensão, visualização
de tecidos mole e duro, também possui a vantagem da obtenção de imagens com
alta acurácia e precisão e com recurso de manipulação favorecendo um diagnóstico
mais eficaz.
Ainda no final do século XX, em 1997, a tecnolgia da Tomografia
Computadorizada Cone Beam começou a ser utilizada na área odontológica por Arai
e colaboradores, principalmente devido ao porte físico reduzido do aparelho, menor
custo e menor dose de radiação, quando comparado com o equipamento de
tomografia utilizado em clínicas médicas. No tomógrafo Cone Beam a fonte de raios
X e o detector fazem um giro de 180° a 360° mantend o o volume selecionado no
centro de rotação, desta maneira uma série de dados é adquirida e então ocorre a
reconstrução das imagens através de algoritmos de computador.
Recentemente, a tecnologia da Tomografia Computadorizada começou a ser
utilizada na área odontológica oferecendo segurança para o profissional e para o
paciente com o intuito de obter planejamento e tratamento mais eficazes através de
reconstruções em terceira dimensão da maxila e da mandíbula. Este exame também
fornece informações mais detalhadas sobre os dentes e as estruturas adjacentes,
proporcionando precisão na detecção de fraturas radiculares quando comparadas
com as radiografias periapicais convencionais ou digitais de acordo com os estudos
de Mora et al (2007), Hassan et al (2009), Ilguy et al (2009), Wenzel et al (2009),
Kamburoglu et al (2010). Esta superioridade é devido à visualização da imagem em
três dimensões onde a linha de fratura é vizualizada entre os fragmentos, em dentes
sem núcleos metálicos. Entretanto em vários casos, a fratura fica mascarada no
exame radiográfico periapical principalmente se o ângulo de projeção do feixe de
raios X não estiver paralelo à fratura (WENZEL et al., 2009; HASSAN et al., 2010).
Porém, deve-se considerar também, que na tomografia, a colimação, o tamanho do
voxel, o número de aquisições e os artefatos possuem influência significativa na
qualidade da imagem (YOUSSEFZADEH et al., 1999). Além disso, cada tipo de
11
aparelho varia na qualidade da imagem e na capacidade de visualizar as estruturas
anatômicas em relação ao tamanho do FOV (Field Of View).
Mesmo diante de vários métodos de diagnóstico por imagem, as fraturas
radiculares, ainda são difíceis se serem detectadas principalmente em dentes que
possuem pino metálico intracanal. O uso de núcleo metálico em dentes tratados
endodonticamente é um procedimento frequente nos consultórios odontológicos, e
consequentemente as fraturas associadas a esta condição tem sido um dos maiores
problemas para o clínico. Estes artefatos podem aparecer como zonas escuras ou
listras em torno do material endodôntico e do núcleo semelhante às fraturas
radiculares, e assim levar a falsas leituras em dentes hígidos (falso-positivos)
(KAMBUROGLU et al., 2010). Desta maneira, existe a necessidade de um minucioso
exame clínico e de um diagnóstico por imagem confiável para a detecção de fraturas
radiculares em dentes com núcleo metálico.
12
2 OBJETIVOS
O presente trabalho teve como objetivo comparar a precisão no diagnóstico
de fraturas radiculares associadas a pinos intracanal com imagens de radiografias
periapicais convencionais e digitais (sistema CCD e fósforo - PSP), além de
tomografias computadorizadas (multislice e cone beam).
13
3 MATERIAIS E MÉTODOS
O trabalho teve início após a aprovação pelo Comitê de Ética em Pesquisa da
Pontifícia Universidade Católica de Minas Gerais sob o protocolo 0271.0.213.000-10.
3.1 Preparação da amostra
O grupo do experimento consistiu de 30 dentes extraídos humanos, primeiro e
segundo pré-molares inferiores unirradiculares, com rizogênese completa, sem
fratura, lesão periapical, reabsorção radicular ou anomalia.
Foi realizada a abertura coronária em todos os elementos dentários,
impulsionado por um motor de alta rotação (300 000rpm), utilizando broca
diamantada. Para alargar a porção coronal dos condutos radiculares foi utilizada as
brocas Gates-Glidden números 2 e 3 (Dentsply Maillefer, Ballaigues, Suiça)
(MONAGHAN et al., 1993; MIREKU et al., 2010; COSTA et al., 2011). A seguir, os
condutos radiculares foram instrumentados através da técnica telescópica com limas
de aço inoxidável Kerr, e a cada mudança na instrumentação, os condutos
radiculares foram irrigados com hipoclorito de sódio a 2% (KAMBUROGLU et al.,
2010).
Em seguida, os canais foram preenchidos com guta-percha através da técnica
de condensação lateral. O cimento utilizado foi o Endofill (Malleifer, Dentsply,
Petrópolis, RJ, Brasil) manipulado de acordo com as instruções do fabricante. Após
esta fase, foi utilizado o calcador modelo Paiva aquecido na lamparina para remover
parte do material obturador deixando apenas 3 a 5mm da guta-percha preenchendo
o ápice da raiz afim de deixar o conduto radicular preparado para receber o núcleo
metálico.
Para a confecção do núcleo metálico, foi utilizada a técnica direta, onde a
resina acrílica (Duralay) faz uma cópia idêntica do conduto radicular, e em seguida é
enviada ao laboratório protético para a fundição. Os núcleos foram posicionados em
cada um dos dentes e fixados com cera utilidade para que não houvesse
movimentação dos mesmos. Os dentes foram colocados no alvéolo vazio de uma
14
mandíbula humana seca, e cada um deles foi fixado em um bloco de resina acrílica
para permanecerem na mesma posição durante a aquisição das imagens e para
permitir o reposiocinamento (Figura 1).
Figura 1 – Dentes fixados em resina acrílica posicionados na mandíbula seca.
3.2 Aquisição das imagens
3.2.1 Radiografia periapical
As radiografias periapicais foram realizadas com aparelho KODAK 2200
Intraoral X-Ray System® (Kodak Eastman Company, USA), operando a 60 kV, 10
mA, com a distância foco-receptor de 25 cm e 1.5 mm de filtração e tempo de
exposição de 0,35s para as imagens convencionais e 0,23s para as imagens
digitais. Para simular o corpo do paciente, foi utilizada uma placa de acrílico com
10mm de espessura (SOGUR; BAKS; GRONDAHL, 2007; CALDAS et al, 2010).
Para a realização das radiografias convencionais, foi utilizado filme F Speed (3 x
4cm Kodak Insight films; Eastman Kodak Company, Rochester, NY, USA) e o feixe
central de raios X foi direcionado perpendicularmente ao longo eixo do dente
(técnica do paralelismo) através de um suporte personalizado. Os filmes utilizados
foram processados em uma máquina processadora automática (AP 200 Processor;
PLH Medical, Watford, England).
15
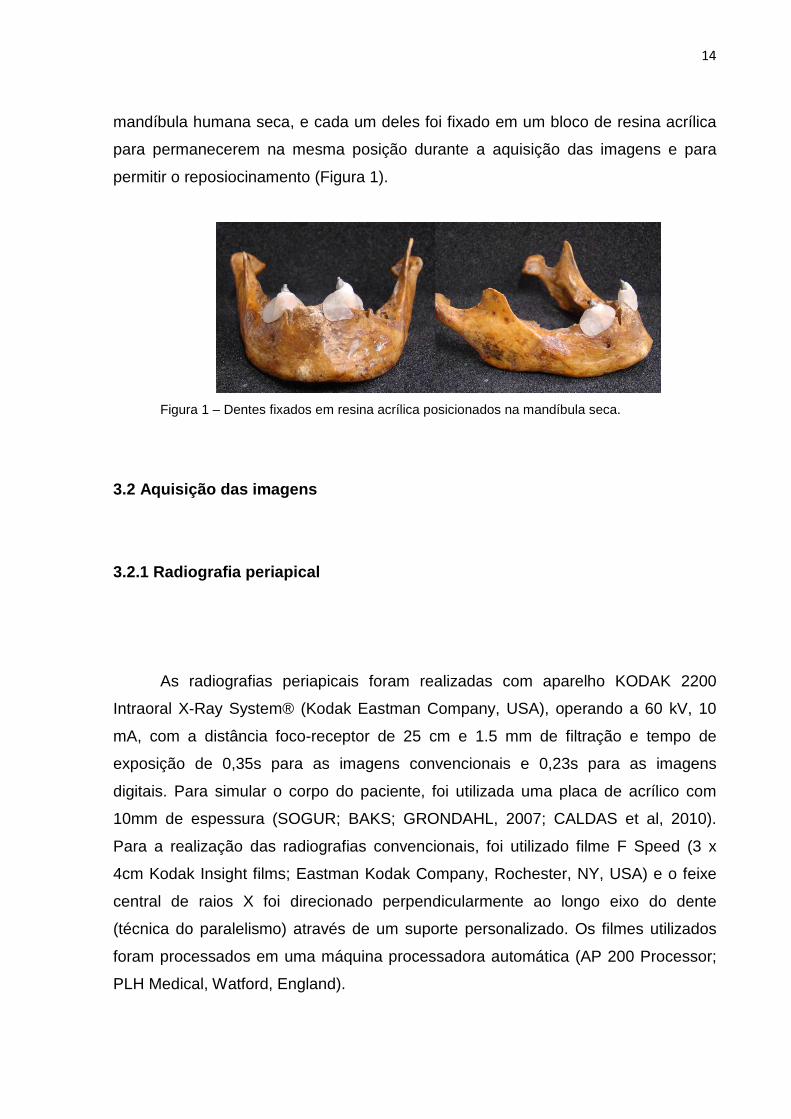
Para as radiografias digitais, dois sensores foram utilizados: CCD, RVG 5.0
(Trophy, Marne la Valle, France), sensor tamanho 2, com 10pl/mm de resolução
espacial e placa de fósforo (PSP) CR 7400 (Trophy, Marne la Valle, France),
com10pl/mm de resolução espacial e com 10,2s de tempo de leitura (Figura 2).
Como nas imagens convencionais, o feixe central de raios X foi direcionado
perpendicularmente ao longo eixo do dente (técnica do paralelismo) através de um
suporte personalizado. As placas de fósforo foram escaneadas imediatamente após
a exposição.
Figura 2 – Posicionamento do sensor CCD (A) e da placa de fósforo (B).
3.2.2 Tomografia Computadorizada
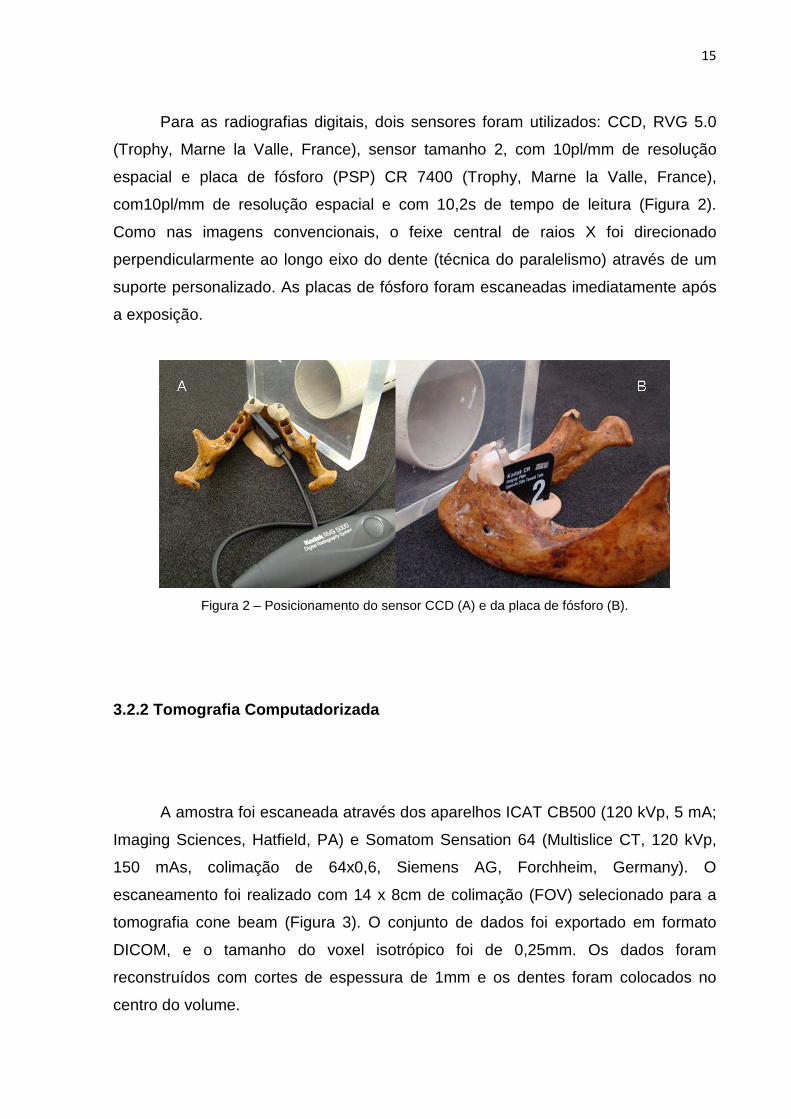
A amostra foi escaneada através dos aparelhos ICAT CB500 (120 kVp, 5 mA;
Imaging Sciences, Hatfield, PA) e Somatom Sensation 64 (Multislice CT, 120 kVp,
150 mAs, colimação de 64x0,6, Siemens AG, Forchheim, Germany). O
escaneamento foi realizado com 14 x 8cm de colimação (FOV) selecionado para a
tomografia cone beam (Figura 3). O conjunto de dados foi exportado em formato
DICOM, e o tamanho do voxel isotrópico foi de 0,25mm. Os dados foram
reconstruídos com cortes de espessura de 1mm e os dentes foram colocados no
centro do volume.
16
Figura 3 – Mandíbula posicionada no aparelho ICat CB500 (A e B) e no Somatom Sensation 64 (B).
Para TC Multislice, a direção do escanemaento foi cranio-caudal, começando
da base da mandibular e estendendo a crista alveolar (Figura 4). A espessura do
corte na imagem foi ajustada para 1mm com intervalo também de 1mm. Após a
aquisição das imagens axiais, as mesmas foram processadas através do programa
de reformatação Tomografia Computadorizada Dental (DCT). As reconstruções
multiplanares foram baseadas no protocolo do DCT e as panorâmicas pelo software
dental (Syngo Dental CT 2006 A-W VB20B-W) na workstation. Os cortes foram
reformatados para colocar o dente na posição vertical.
Figura 4 – Mandíbula posicionada no aparelho Somatom Sensation 64 (A).
17
3.3 Preparação da amostra (após a aquisição das ima gens)
As fraturas radiculares foram induzidas por força mecânica no plano vertical
descritas por Nair et al (2001), sendo que alguns traços de fratura se fizeram no
sentido vertical e outros no sentido horizontal, de acordo com a força incidida no
dente. Ambos os fragmentos foram montados e colados sem deslocamento. O pino
metálico intracanal foi reposicionado no conduto radicular e fixado com cera
utilidade, e os dentes foram submetidos a uma nova etapa de radiografias e
tomografias.
3.4 Avaliação das imagens
Três especialistas em radiologia odontológica, com experiência em tomografia
computadorizada e imagem digital, analisaram separadamente todas as radiografias
e tomografias de maneira independente. Estes avaliadores desconheciam os
procedimentos, os métodos, e as condições das raízes dos dentes. As radiografias
intraorais convencionais foram observadas em um negatoscópio, as imagens digitais
CCD e PSP foram avaliadas em um computador Dell PWS 670 (Dell Inc., Round
Rock, TX, USA), processador Intel® Core™ i5-2500K (6M Cache, 3.30 GHz) e
monitor Dell (22 polegadas), com e sem o uso de ferramentas do software (brilho,
contraste, zoom, negativo e colorização). Os dados volumétricos obtidos usando
TCCB e TC multislice foram exportados como DICOM e importados para um
software especialmente desenhado para visualizar imagens (Dental Slice; Bioparts,
Brasília, Brazil). As imagens transversais, coronais e perpendiculares às linhas de
fratura foram reconstruídas a partir dos dados exportados. Os observadores foram
livres para usar as opções de ferramentas de imagem disponíveis (densidade,
contraste, ampliação) em um monitor de 22 polegadas em tela plana (Figuras 4 e 5).
18
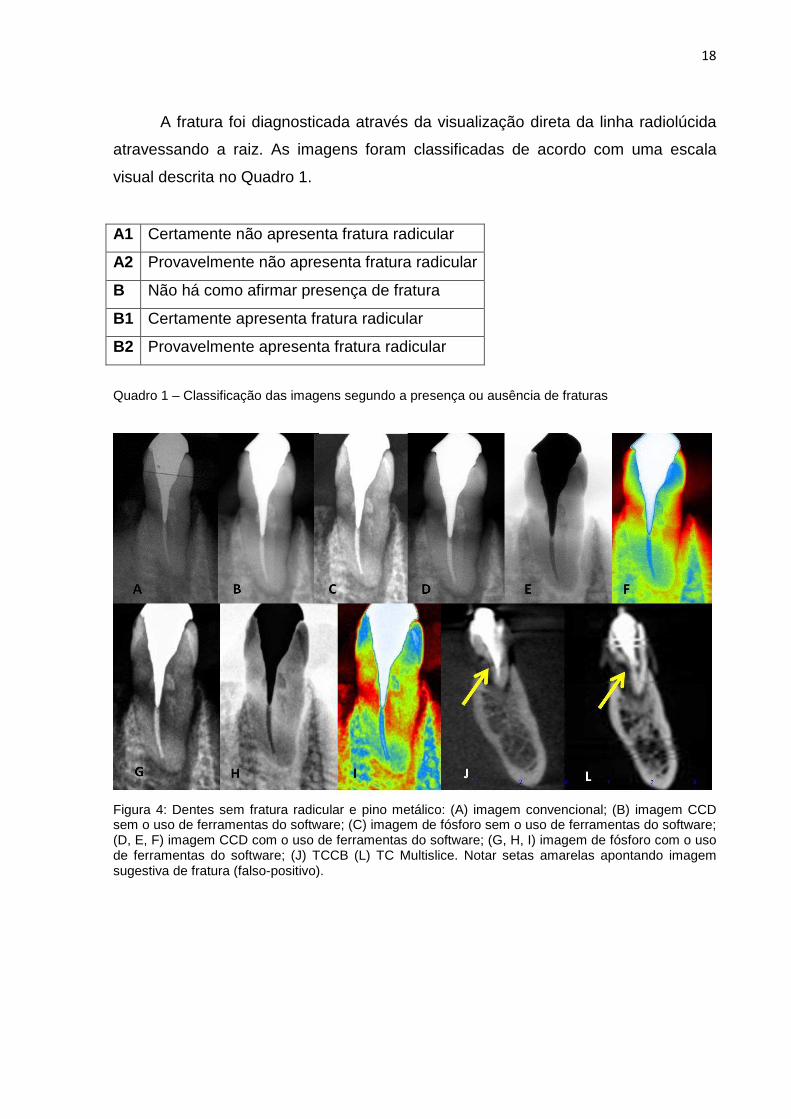
A fratura foi diagnosticada através da visualização direta da linha radiolúcida
atravessando a raiz. As imagens foram classificadas de acordo com uma escala
visual descrita no Quadro 1.
Quadro 1 – Classificação das imagens segundo a presença ou ausência de fraturas
Figura 4: Dentes sem fratura radicular e pino metálico: (A) imagem convencional; (B) imagem CCD sem o uso de ferramentas do software; (C) imagem de fósforo sem o uso de ferramentas do software; (D, E, F) imagem CCD com o uso de ferramentas do software; (G, H, I) imagem de fósforo com o uso de ferramentas do software; (J) TCCB (L) TC Multislice. Notar setas amarelas apontando imagem sugestiva de fratura (falso-positivo).
A1 Certamente não apresenta fratura radicular
A2 Provavelmente não apresenta fratura radicular
B Não há como afirmar presença de fratura
B1 Certamente apresenta fratura radicular
B2 Provavelmente apresenta fratura radicular

19
Figura 5: Dentes com fratura radicular e pino metálico: (A) imagem convencional; (B) imagem CCD sem o uso de ferramentas do software; (C) imagem de fósforo sem o uso de ferramentas do software; (D, E, F) imagem CCD com o uso de ferramentas do software; (G, H, I) imagem de fósforo com o uso de ferramentas do software; (J) TCCB; (L) TC Multislice.
O coeficiente Kappa foi calculado para avaliar a concordância intra e
interobservadores para cada conjunto de imagens. A classificação obtida com as
imagens convencionais, digitais e tomografias computadorizadas foram comparadas
com o padrão-ouro usando a curva ROC (receiver operating characteristic) através
da análise para avaliar a capacidade do observador em diferenciar entre os dentes
com ou sem fratura.
As áreas da curva ROC (valores Az) foram calculados utilizando o software
BioEstat 5.0 (Belém, Brasil) para cada tipo de imagem. Estas áreas foram
comparadas com o teste Q de Cochran com nível de significância de p=0,05.
Verdadeiro negativo (correta identificação de raízes não fraturadas), verdadeiro
positivo (correta identificação da fratura em raiz fraturada), falso positivo (presença
de fratura em raízes não fraturadas), falso negativo (ausência de fratura em raízes
fraturadas) e acurácia foram calculados.
As imagens radiográficas e tomográficas de cada modalidade de aquisição
(convencional, CCD sem manipulação, CCD com manipulação, PSP sem
manipulação, PSP com manipulação, tomografia computadorizada cone beam e
tomografia computadorizada mulstislice) foram comparadas. Sequencialmente, os
20
gráficos apresentam as curvas ROC para os conjuntos de imagens produzidas a
partir desta pesquisa. Nos gráficos ROC, as curvas são diferenciadas pelas áreas.
No gráfico ROC, o eixo das ordenadas representa a sensibilidade e o eixo
das abscissas, o inverso da especificidade. O cálculo do balanço entre os índices de
verdadeiro-positivos e falso-positivos é obtido pela determinação da área sob a
curva ROC, que representa uma expressão do poder discriminativo global que um
teste de diagnóstico possui e constitui uma boa medida sumária de exatidão
(HANLEY; MCNEIL, 1982; WENZEL; VERDONSCHOT, 1994). O valor mínimo da
área sob a curva ROC é de 0,50, sendo a representação gráfica de uma reta em 45o.
Isso acontece se as capacidades de previsão da modalidade não forem superiores
ao puro acaso, ou seja, quando o método não possui qualquer capacidade
discriminativa. Então, o índice de verdadeiro-positivos é igual ao índice de falso-
positivos. O valor máximo é igual a 1 nas situações em que se obtêm 100% de
verdadeiro-positivos e 0% de falso-positivos. A melhor performance é indicada por
uma curva que é mais elevada e voltada para a esquerda, no espaço ROC
(HANLEY; MCNEIL, 1982).
21
ARTIGOS
Artigo 1
Artigo publicado pela Revista Odontológica do Brasil Central
Rev Odontol Bras Central 2011;20(53):172-5.
DETECÇÃO DE FRATURA LONGITUDINAL POR MEIO DE TOMOGR AFIA
COMPUTADORIZADA CONE BEAM: RELATO DE DOIS CASOS CLÍ NICOS
DETECTION OF LONGITUDINAL FRACTURE THROUGH CONE BEAM
COMPUTED TOMOGRAPHY: REPORT OF TWO CLINICAL CASES
AUTORES
Priscila Dias Peyneau1
Claudia Scigliano Valerio2
Andréia Cruz Pires Ribeiro de Sousa3
Daniela Dazzi4
Flávio Ricardo Manzi5
1Especialista em Radiologia – Unigranrio. Mestranda em Clínicas Odontológicas –
Ênfase Radiologia – PUC Minas. 2Especialista em Ortodontia e Ortopedia Facial – PUC Minas. Especialista em
Odontopediatria- USP. Mestranda em Clínicas Odontológicas – Ênfase Radiologia –
PUC Minas. 3Especialista em Ortodontia – CEO-Ipsemg. Mestranda em Clínicas Odontológicas –
Ênfase Radiologia – PUC Minas. 4Especialista em Radiologia – ABO MG. 5Professor Adjunto de Radiologia e coordenador do mestrado em clínicas
odontológica ênfase de Radiologia do Mestrado em Clínicas Odontológicas da PUC
Minas.
22
Endereço para correspondência:
Prof. Dr. Flávio Ricardo Manzi
Av. Dom José Gaspar, Prédio 45 – Clínica de Radiologia
Coração Eucarístico, Belo Horizonte – MG
CEP: 30535-901
Fones: 31 – 3319-4591 // 31 – 8895-7033
RESUMO
Objetivo: O presente trabalho tem como objetivo mostrar a importância do uso de
técnicas avançadas por imagem, para diagnóstico preciso de fratura radicular
longitudinal. A tomografia computadorizada por feixe cônico através de
reconstruções em terceira dimensão e visualização da região de interesse nos
planos axial, sagital e coronal, veio revolucionar o diagnóstico por imagem
fornecendo acurácia e precisão.
Relato dos casos clínicos: O diagnóstico de fraturas radiculares longitudinais por
meio da tomografia computadorizada por feixe cônico será descrito através de dois
casos clínicos. Em ambos os casos, os pacientes foram encaminhados a centro de
diagnóstico devido sintomatologia dolorosa e a fratura foi detectada.
Conclusão: O diagnóstico de fratura radicular é muito difícil. O cirurgião dentista
deve realizar um exame clínico minucioso e lançar mão das novas tecnologias de
diagnóstico por imagem, como a tomografia computadorizada por feixe cônico, para
que seja feito um planejamento adequado e que o paciente tenha um bom
prognóstico.
PALVAVRAS-CHAVE: Fraturas dos dentes, diagnóstico, Tomografia
Computadorizada por raios X.
ABSTRACT
Objective: This study aims to show the importance of using advanced imaging
techniques for accurate diagnosis of longitudinal root fracture. The cone beam
computed tomography using three-dimensional reconstruction and visualization of
23
the region of interest in axial, sagittal and coronal, has revolutionized diagnostic
imaging provides accurate and precise.
Report of clinical cases: Diagnosis of longitudinal root fractures using the cone
beam computed tomography is described by two clinical cases. In both cases, the
patients were referred for diagnostic center because of painful symptoms and the
fracture was detected.
Conclusion: The diagnosis of root fracture is very difficult. The dentist should
perform a clinical exam and use the new technologies of diagnostic imaging such as
cone beam computed tomography, to have done adequate planning and the patient
has a good prognosis.
KEYWORDS: Tooth Fractures, diagnostic, X-Ray Computed Tomography.
INTRODUÇÃO
A fratura radicular longitudinal é caracterizada por uma linha na superfície
externa da raiz que possivelmente teve seu início na parede interna do canal na
região apical do dente, podendo envolver ambos os lados da raiz. Esta linha pode
originar-se na coroa em direção ao ápice e vice-versa, de acordo com Mora10 (2007)
e Mireku9 (2010). O prognóstico de um dente com fratura longitudinal é ruim e em
muitos casos a extração é a única opção de tratamento. Fuss3 (1999), Tamse14
(1999) e Youssefzadeh18 (1999) encontraram a prevalência de 2 e 5% na população,
sendo os dentes posteriores os mais afetados.
Dentre os fatores etiológicos que podem levar a fratura radicular longitudinal,
pode-se citar o trauma físico, o trauma oclusal, os hábitos parafuncionais repetitivos
de estresse mastigatório ou a reabsorção patológica induzindo uma fratura radicular.
Acredita-se que a causa mais comum para este tipo de fratura ocorre durante ou
após o tratamento endodôntico, quando as iatrogenias podem acontecer. Dentre
alguns exemplos pode-se citar a instalação de pinos ou a pressão para adaptá-los, e
também a condensação da guta percha no canal radicular durante a obturação, de
acordo com os estudos de Meister8 (1980). Além disso, o acesso endodôntico amplo
e o alargamento exagerado do canal contribuem para uma remoção exagerada da
dentina, tornando a raiz mais frágil, podendo ficar predisposta às fraturas
24
longitudinais, como foi pesquisado por Fuss4 (2001), Cohen e Hargreaves2 (2007) e
Mireku9 (2009).
Os sinais e sintomas clínicos da presença de fratura podem variar de acordo
com a localização, dente envolvido, tempo que a fratura está presente, condição
periodontal do dente e arquitetura óssea adjacente à fratura. Os dentes com fratura
longitudinal apresentam longa história de dor durante a mastigação associada com
infecção crônica. A dor normalmente é de moderada a intensa, segundo Moule11
(1999). Além disso, pode-se observar bolsa periodontal adjacente a fratura, fístula,
mobilidade dental, sensibilidade a percussão e palpação de acordo com Tamse15
(2006).
Dentre as características radiográficas para diagnóstico de fraturas
radiculares pode-se notar uma linha radiolúcida entre os fragmentos ou a separação
deles, aumento do espaço do ligamento periodontal e perda óssea localizada.
Segundo Mora10 (2007), os sinais radiográficos podem estar ausentes quando a
orientação do feixe de raios X não encontra-se paralelo ao plano da fratura. As
radiografias periapicais são adequadas para avaliar a coroa do dente, a raiz, e as
estruturas adjacentes, porém para o diagnóstico de fratura radicular existem
algumas limitações devido à sobreposição de estruturas e a natureza bidimensional
da imagem. Desta maneira, a tomografia computadorizada por meio de
reconstruções em terceira dimensão e visualização da região de interesse nos
planos axial, sagital e coronal, veio revolucionar o diagnóstico por imagem
fornecendo acurácia e precisão, além da rápida aquisição, alta resolução e baixa
dose de radiação, como mostram os trabalhos de Mora10 (2007), Hassan6 (2010) e
Kamburoglu7 (2010).
O objetivo do presente trabalho é mostrar a importância do uso de exames
por imagem como a tomografia computadorizada para diagnóstico preciso de fratura
radicular longitudinal, por meio da descrição de dois casos clínicos.
CASO CLÍNICO 1
Paciente com 42 anos de idade, gênero masculino, foi encaminhado ao centro
de diagnóstico por imagem em odontologia para exame do dente 15 tratado
endodonticamente por motivo de dor durante a mastigação. Foi realizada uma
tomografia computadorizada Cone Beam com o aparelho GXCB-500 Powered by i-
25
CAT® (Imaging Sciences, Hatfield, USA). Após a reconstrução da imagem original,
foram realizadas as reconstruções nos planos axiais, coronais, sagitais e oblíquos.
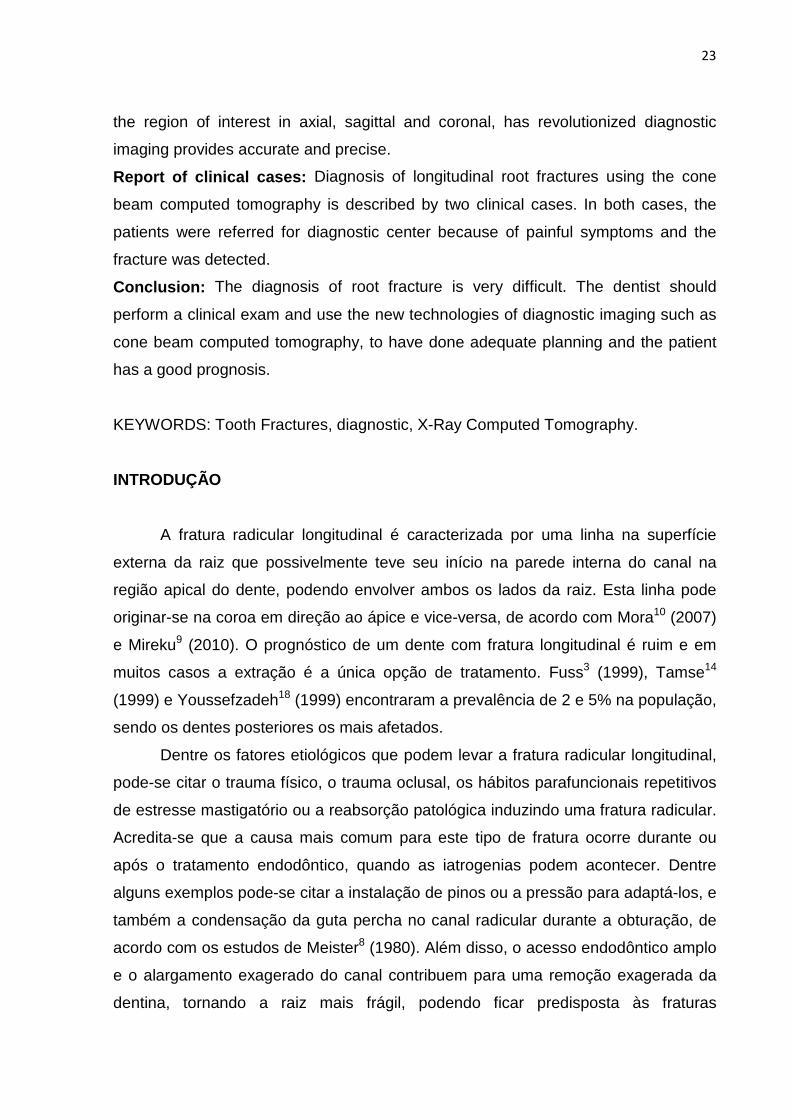
Por meio da imagem da reconstrução panorâmica, nota-se a presença de
rarefação óssea no periápice do dente 15. Nas reconstruções oblíquas também se
observa a rarefação periapical, linha hipodensa compatível de fratura, além da perda
de parte da tábua óssea vestibular e perda de crista óssea alveolar no sentido
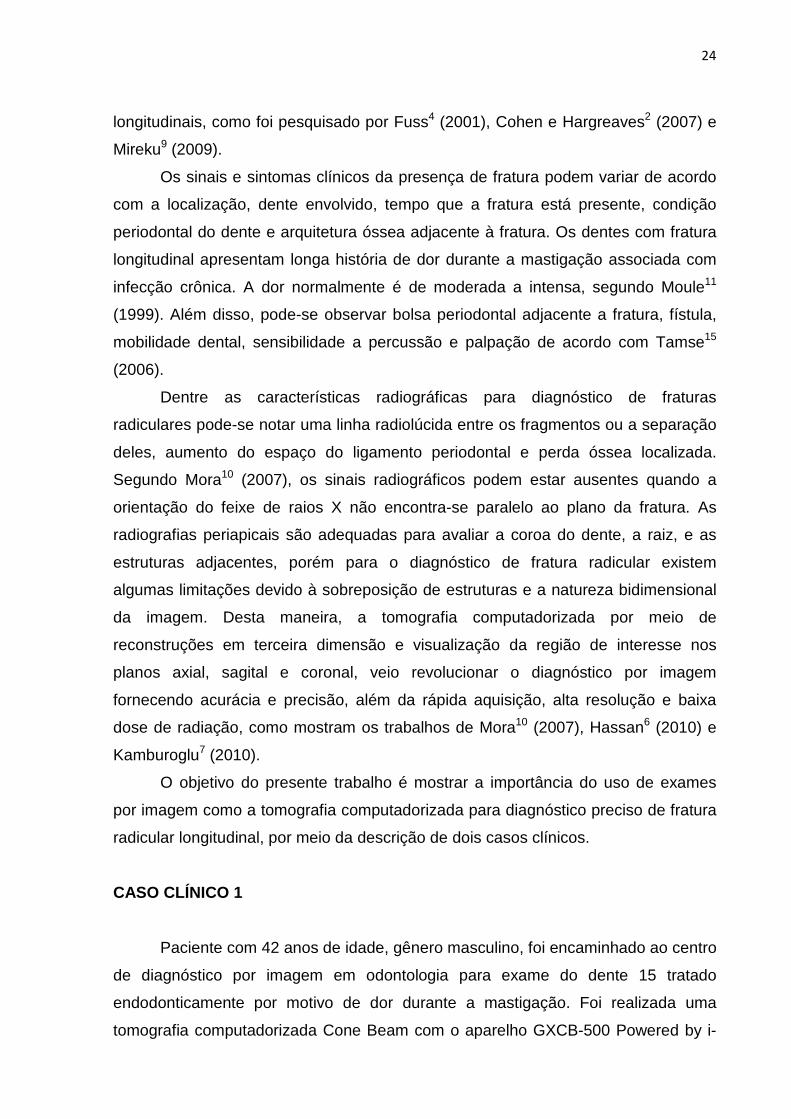
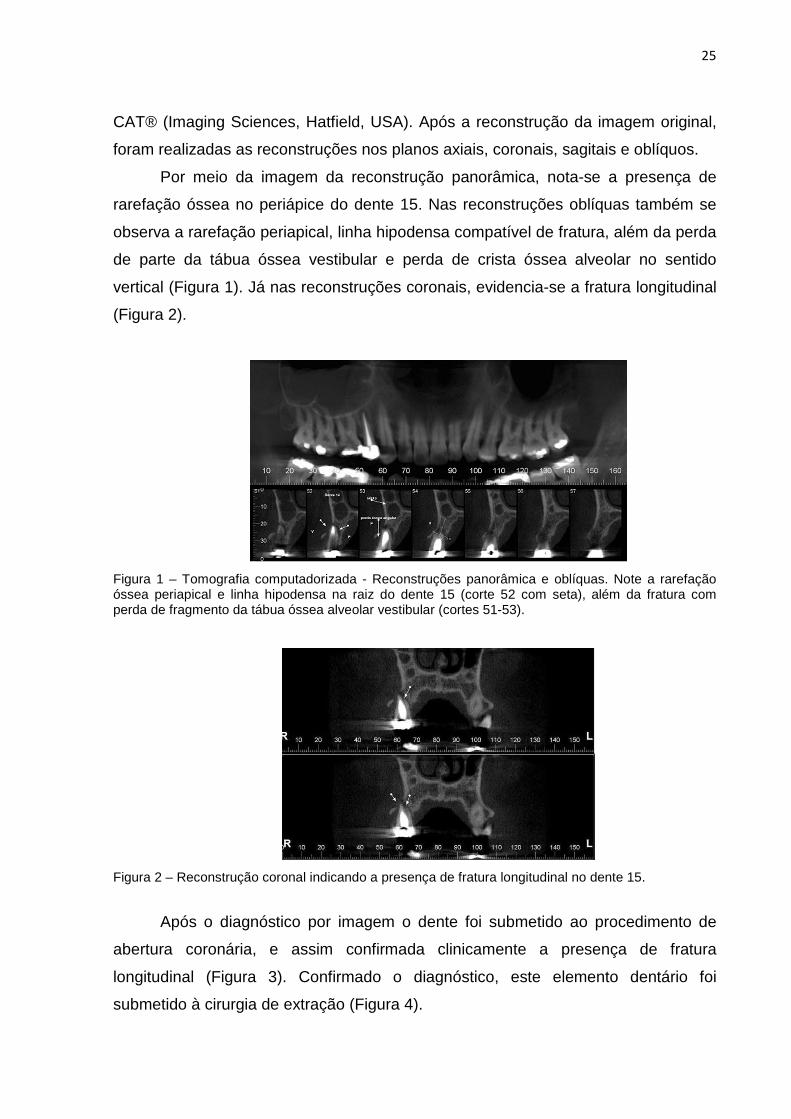
vertical (Figura 1). Já nas reconstruções coronais, evidencia-se a fratura longitudinal
(Figura 2).
Figura 1 – Tomografia computadorizada - Reconstruções panorâmica e oblíquas. Note a rarefação óssea periapical e linha hipodensa na raiz do dente 15 (corte 52 com seta), além da fratura com perda de fragmento da tábua óssea alveolar vestibular (cortes 51-53).
Figura 2 – Reconstrução coronal indicando a presença de fratura longitudinal no dente 15.
Após o diagnóstico por imagem o dente foi submetido ao procedimento de
abertura coronária, e assim confirmada clinicamente a presença de fratura
longitudinal (Figura 3). Confirmado o diagnóstico, este elemento dentário foi
submetido à cirurgia de extração (Figura 4).
26
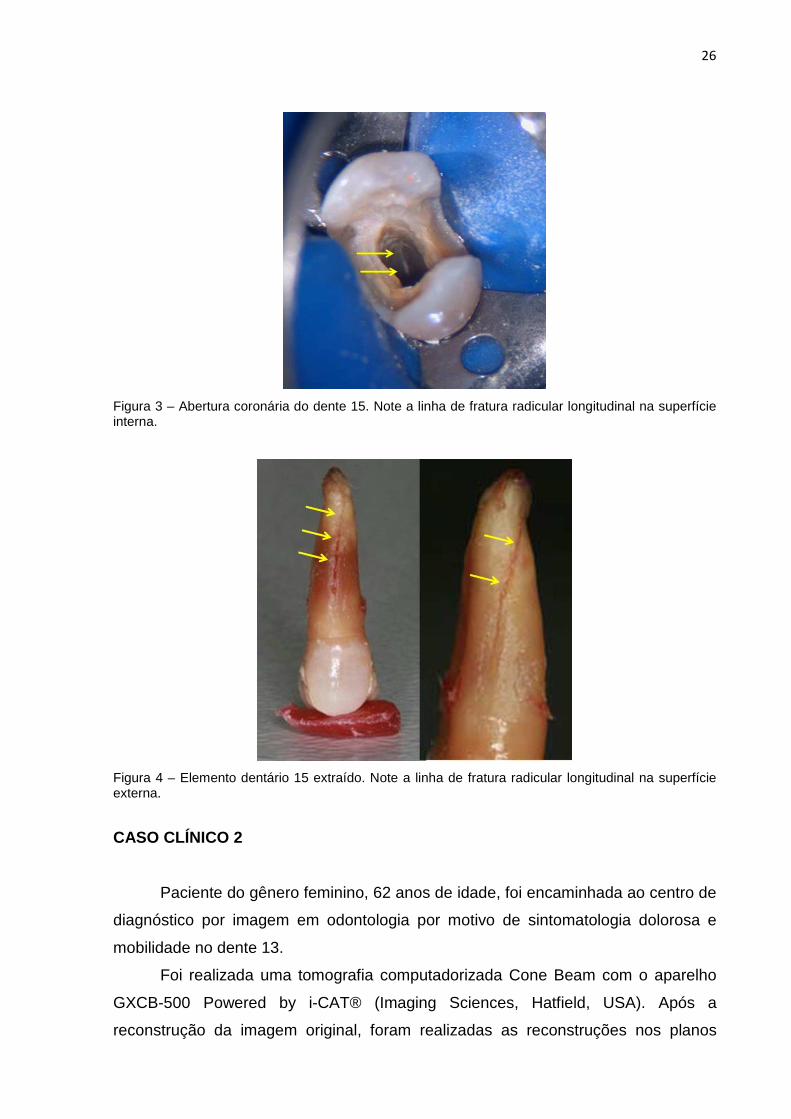
Figura 3 – Abertura coronária do dente 15. Note a linha de fratura radicular longitudinal na superfície interna.
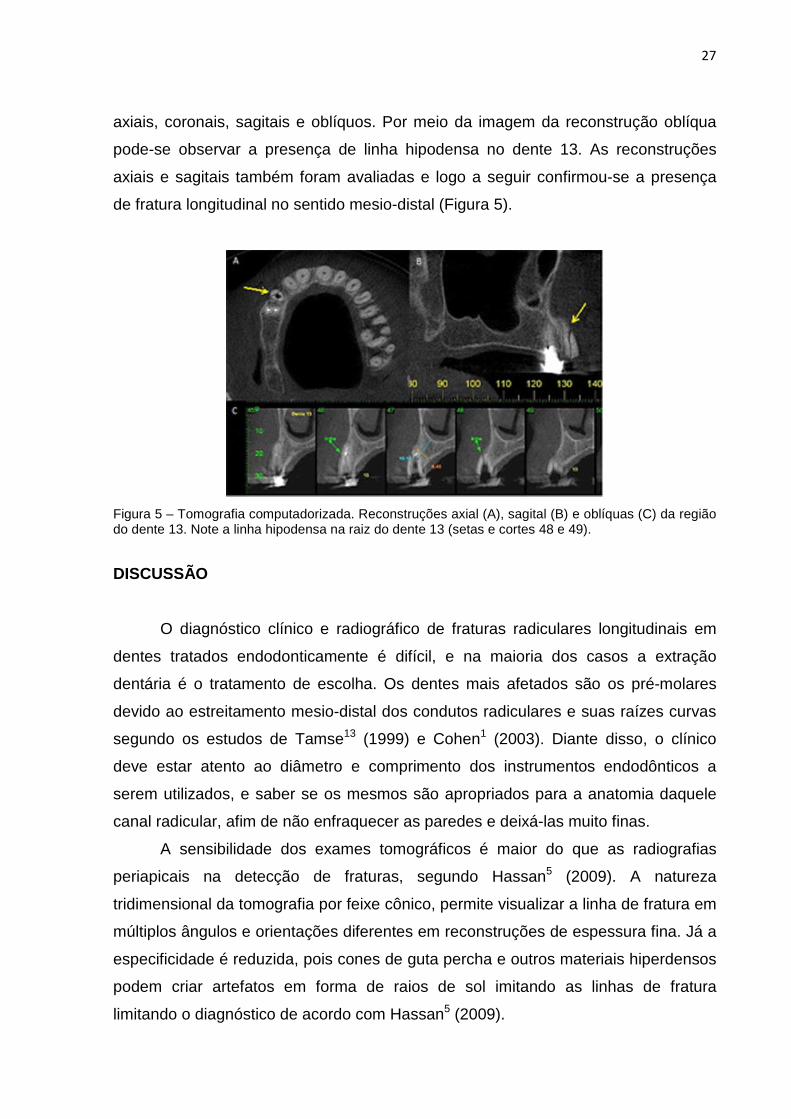
Figura 4 – Elemento dentário 15 extraído. Note a linha de fratura radicular longitudinal na superfície externa.
CASO CLÍNICO 2
Paciente do gênero feminino, 62 anos de idade, foi encaminhada ao centro de
diagnóstico por imagem em odontologia por motivo de sintomatologia dolorosa e
mobilidade no dente 13.
Foi realizada uma tomografia computadorizada Cone Beam com o aparelho
GXCB-500 Powered by i-CAT® (Imaging Sciences, Hatfield, USA). Após a
reconstrução da imagem original, foram realizadas as reconstruções nos planos
27
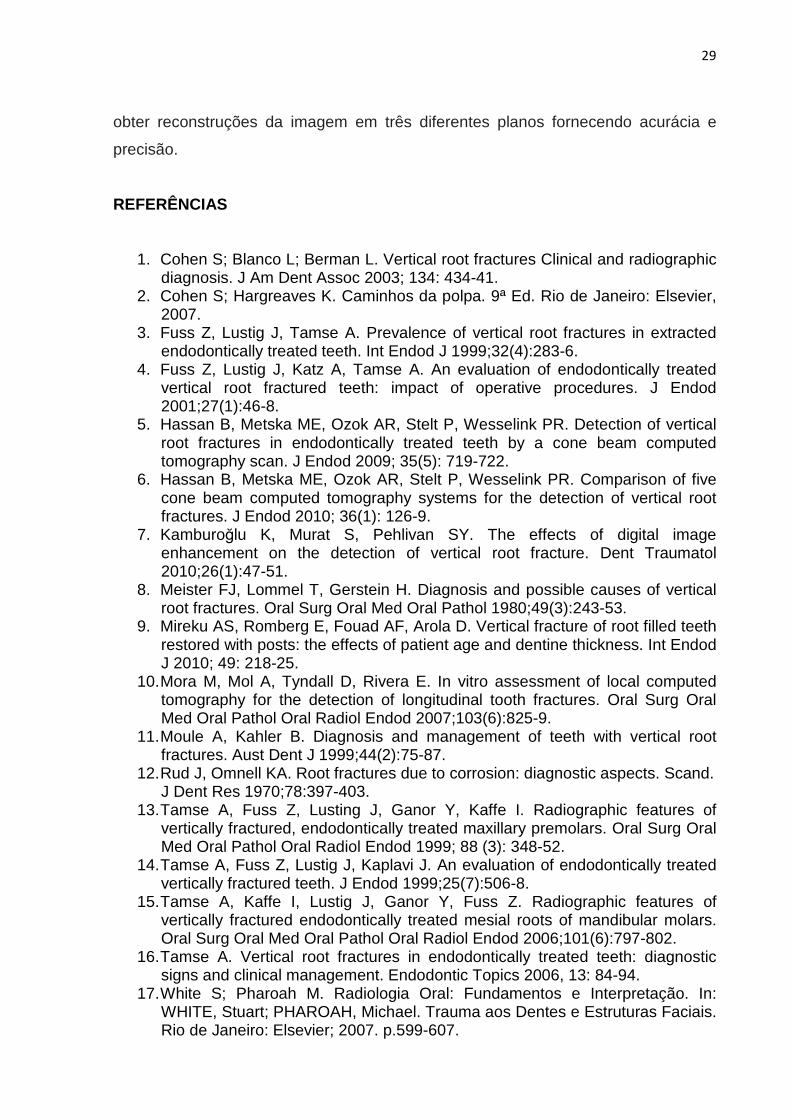
axiais, coronais, sagitais e oblíquos. Por meio da imagem da reconstrução oblíqua
pode-se observar a presença de linha hipodensa no dente 13. As reconstruções
axiais e sagitais também foram avaliadas e logo a seguir confirmou-se a presença
de fratura longitudinal no sentido mesio-distal (Figura 5).
Figura 5 – Tomografia computadorizada. Reconstruções axial (A), sagital (B) e oblíquas (C) da região do dente 13. Note a linha hipodensa na raiz do dente 13 (setas e cortes 48 e 49).
DISCUSSÃO
O diagnóstico clínico e radiográfico de fraturas radiculares longitudinais em
dentes tratados endodonticamente é difícil, e na maioria dos casos a extração
dentária é o tratamento de escolha. Os dentes mais afetados são os pré-molares
devido ao estreitamento mesio-distal dos condutos radiculares e suas raízes curvas
segundo os estudos de Tamse13 (1999) e Cohen1 (2003). Diante disso, o clínico
deve estar atento ao diâmetro e comprimento dos instrumentos endodônticos a
serem utilizados, e saber se os mesmos são apropriados para a anatomia daquele
canal radicular, afim de não enfraquecer as paredes e deixá-las muito finas.
A sensibilidade dos exames tomográficos é maior do que as radiografias
periapicais na detecção de fraturas, segundo Hassan5 (2009). A natureza
tridimensional da tomografia por feixe cônico, permite visualizar a linha de fratura em
múltiplos ângulos e orientações diferentes em reconstruções de espessura fina. Já a
especificidade é reduzida, pois cones de guta percha e outros materiais hiperdensos
podem criar artefatos em forma de raios de sol imitando as linhas de fratura
limitando o diagnóstico de acordo com Hassan5 (2009).

28
De acordo com o trabalho de Rud e Omnell12 (1970), 75% das fraturas
radiculares aconteceram na maxila, sendo 62% em pré-molares. Tamse13 (1999) em
seu estudo concluiu que 40% das fraturas ocorreram neste mesmo grupo de dentes.
O primeiro caso clínico avaliado também se refere à extração de pré-molar superior
devido à fratura longitudinal em sua raiz. O diagnóstico foi realizado por meio do
exame clínico e sintomatologia dolorosa, sendo confirmado com a tomografia
computadorizada por feixe cônico. A tomografia se difundiu devido a sua dose de
radiação reduzida, excelente qualidade de imagem, especificidade, sensibilidade e
agilidade no diagnóstico dento-maxilo-facial.
Youssefzadeh et al. 18 (1999), descreveram que as fraturas radiculares
longitudinais ocorrem em 3,69% dos dentes tratados endodonticamente e possuem
dificuldade de diagnóstico. Normalmente a linha de fratura é observada em 35,7%
das radiografias periapicais. O estudo usou a tomografia computadorizada para
investigar a fratura radicular vertical e comparou com os achados clínicos e com a
radiografia periapical. Notou-se que o corte axial da tomografia é ideal para o
diagnóstico de fratura longitudinal, porque o plano é perpendicular à linha da fratura.
Concluiu-se que este exame é superior a radiografia periapical na detecção de
fratura radicular vertical. No segundo caso clínico apresentado pode-se observar a
definição da fratura através da reconstrução axial.
Os estudos de Mora et al. 10 (2007) tiveram como objetivo testar a acurácia da
tomografia computadorizada na detecção de fraturas longitudinais em comparação
com a radiografia periapical. Para este estudo foram utilizados 60 dentes humanos
extraídos, sendo que em 30 deles foram induzidos à fratura radicular longitudinal
através de uma cunha introduzida no canal radicular. Os dentes foram submetidos à
radiografia periapical convencional e tomografia computadorizada cone beam e
concluíram que a tomografia foi melhor para detectar fraturas longitudinais.
CONCLUSÃO
O diagnóstico das fraturas radiculares representa um desafio para o clínico,
pois em muitas vezes é difícil. Sendo assim, devem-se associar dados do exame
clínico e exames por imagem como a tomografia computadorizada. Esta técnica é
considerada um método seguro para avaliação de fraturas radiculares, podendo-se
29
obter reconstruções da imagem em três diferentes planos fornecendo acurácia e
precisão.
REFERÊNCIAS
1. Cohen S; Blanco L; Berman L. Vertical root fractures Clinical and radiographic diagnosis. J Am Dent Assoc 2003; 134: 434-41.
2. Cohen S; Hargreaves K. Caminhos da polpa. 9ª Ed. Rio de Janeiro: Elsevier, 2007.
3. Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted endodontically treated teeth. Int Endod J 1999;32(4):283-6.
4. Fuss Z, Lustig J, Katz A, Tamse A. An evaluation of endodontically treated vertical root fractured teeth: impact of operative procedures. J Endod 2001;27(1):46-8.
5. Hassan B, Metska ME, Ozok AR, Stelt P, Wesselink PR. Detection of vertical root fractures in endodontically treated teeth by a cone beam computed tomography scan. J Endod 2009; 35(5): 719-722.
6. Hassan B, Metska ME, Ozok AR, Stelt P, Wesselink PR. Comparison of five cone beam computed tomography systems for the detection of vertical root fractures. J Endod 2010; 36(1): 126-9.
7. Kamburoğlu K, Murat S, Pehlivan SY. The effects of digital image enhancement on the detection of vertical root fracture. Dent Traumatol 2010;26(1):47-51.
8. Meister FJ, Lommel T, Gerstein H. Diagnosis and possible causes of vertical root fractures. Oral Surg Oral Med Oral Pathol 1980;49(3):243-53.
9. Mireku AS, Romberg E, Fouad AF, Arola D. Vertical fracture of root filled teeth restored with posts: the effects of patient age and dentine thickness. Int Endod J 2010; 49: 218-25.
10. Mora M, Mol A, Tyndall D, Rivera E. In vitro assessment of local computed tomography for the detection of longitudinal tooth fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103(6):825-9.
11. Moule A, Kahler B. Diagnosis and management of teeth with vertical root fractures. Aust Dent J 1999;44(2):75-87.
12. Rud J, Omnell KA. Root fractures due to corrosion: diagnostic aspects. Scand. J Dent Res 1970;78:397-403.
13. Tamse A, Fuss Z, Lusting J, Ganor Y, Kaffe I. Radiographic features of vertically fractured, endodontically treated maxillary premolars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88 (3): 348-52.
14. Tamse A, Fuss Z, Lustig J, Kaplavi J. An evaluation of endodontically treated vertically fractured teeth. J Endod 1999;25(7):506-8.
15. Tamse A, Kaffe I, Lustig J, Ganor Y, Fuss Z. Radiographic features of vertically fractured endodontically treated mesial roots of mandibular molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101(6):797-802.
16. Tamse A. Vertical root fractures in endodontically treated teeth: diagnostic signs and clinical management. Endodontic Topics 2006, 13: 84-94.
17. White S; Pharoah M. Radiologia Oral: Fundamentos e Interpretação. In: WHITE, Stuart; PHAROAH, Michael. Trauma aos Dentes e Estruturas Faciais. Rio de Janeiro: Elsevier; 2007. p.599-607.

30
18. Youssefzadeh S, Gahleitner A, Dorffner R, Bernhart T, Kainberger F. Dental vertical root fractures: value of CT in detection. Radiology 1999;210(2):545-9.
31
Artigo 2
Artigo será submetido ao Journal of Endodontics
COMPUTED TOMOGRAPHY IN THE DIAGNOSIS OF ROOT PERFORATION
AUTHORS
Priscila Dias Peyneau
Claudia Scigliano Valerio
Andréia Cruz Pires Ribeiro de Sousa
Flávio Ricardo Manzi
Department of Oral Maxillofacial Radiology, Pontificial Catholic University of Minas
Gerais, Belo Horizonte, MG, Brazil
Address for Correspondence:
Prof. Dr. Flávio Ricardo Manzi
Av. Dom José Gaspar, Prédio 45 – Clínica de Radiologia
Coração Eucarístico, Belo Horizonte – MG
CEP: 30535-901
Phones: +55 31 – 3319-4591 // 31 – 8895-7033
ABSTRACT
Perforation is defined as communication between the root canal and the external
tooth surface, normally occurs during endodontic treatment and is induced by
iatrogenic causes. There are some conditions that favor the perforations, among
others the irregular morphology of root canals, root dilaceration, error during pulp
chamber preparation, excessive wear of root canal walls, and inadequate preparation
for intraradicular post placement. The definitive diagnosis of this type of iatrogenic
condition is very difficult due the limitation periapical radiography, as it offers a two-
dimensional image and superimposition of structures. For this reason, imaging
32
methods, such as Computerized tomography, which allows all the root faces to be
evaluated should be used, in order to diagnose and inform the location of root
perforations with greater precision. Thus, the aim of the present study is to
demonstrate the importance of Cone Beam Computerized Tomography in the
diagnosis of root perforation in three clinical cases.
Keyword: Tooth root, X-Ray Computed Tomography, Diagnosis, Root canal therapy,
Root perforation.
INTRODUCTION
Perforation is one of the most frustrating complications of endodontic
treatment. Over the last few years, the incidence has rise due to negligence,
imprudence and inexperience of new professional. An artificial communication in the
root caused by iatrogenic conditions or pathological resorptions that result in an
intimate relationship between the pulp cavity and periodontal tissues may be
considered a perforation. Iatrogenic perforations are caused by different factors,
such as irregular morphology of root canals, high incidence of root dilaceration, error
during pulp chamber preparation, excessive wear of root canal walls, calcifications,
and perforations resulting from inadequate preparations for intraradicular posts (1 –
6).
Among the clinical aspects of perforation, one could mention pain, sensitivity
to palpation, presence of fistula and/or periodontal pocket. The radiographic
characteristics include increase in the periodontal ligament space and bone
rarification adjacent to the region of the perforation, in addition to visualization of the
perforation when it occurs on the mesial and distal surfaces (2, 3).
Periapical radiography is the first exam requested in cases of perforation, as it
offers information about the condition and morphology of the root and root canal.
However, there is the limitation of the vestibular-lingual plane, as the image is two-
dimensional, and anatomic repairs may be confused with pathological lesions (1, 5,
7). Therefore, advanced imaging methods, such as Computerized Tomography
should be used, which allow visualization and evaluation of the root and alveolar
bone, location and extension of the pulp chamber and a tridimensional view of the
33
root (1, 8). Thus, tridimensional images are valuable in the diagnosis and treatment
of dental problems (7).
The prognosis for teeth with root perforation depends mainly on prevention
and the use of biocompatible material in the repair to provide the best possible
sealing against bacterial penetration and limit periodontal inflammation (6), in
addition to the experience and skill of the professional, location of the perforation,
quality of endodontic treatment, periodontal conditions and size of the perforation.
Therefore, the greatest complication resulting from perforation is the potential for a
secondary inflammation in the periodontal ligament causing loss of bone insertion,
and consequently leading to loss of the tooth (4 - 6).
The aim of this study is to demonstrate the importance of Computerized
Tomography in locating and diagnosing root perforation, by means of three clinical
case reports.
CLINICAL CASE 1
The patient J. F. G., 43 years of age, was referred for evaluation of the
maxillary right first molar that presented painful symptoms after root canal
preparation for intraradicular post fabrication. By means of the clinical exam, probing,
negative palpation and sensitivity to vertical and horizontal percussion, the presence
of fistula was identified in the region of the tooth in question.
The patient was submitted to Multislice Computerized Tomography, using the
SOMATOM Sensation 64® appliance (Siemens, Erlangen, Germany) involving the
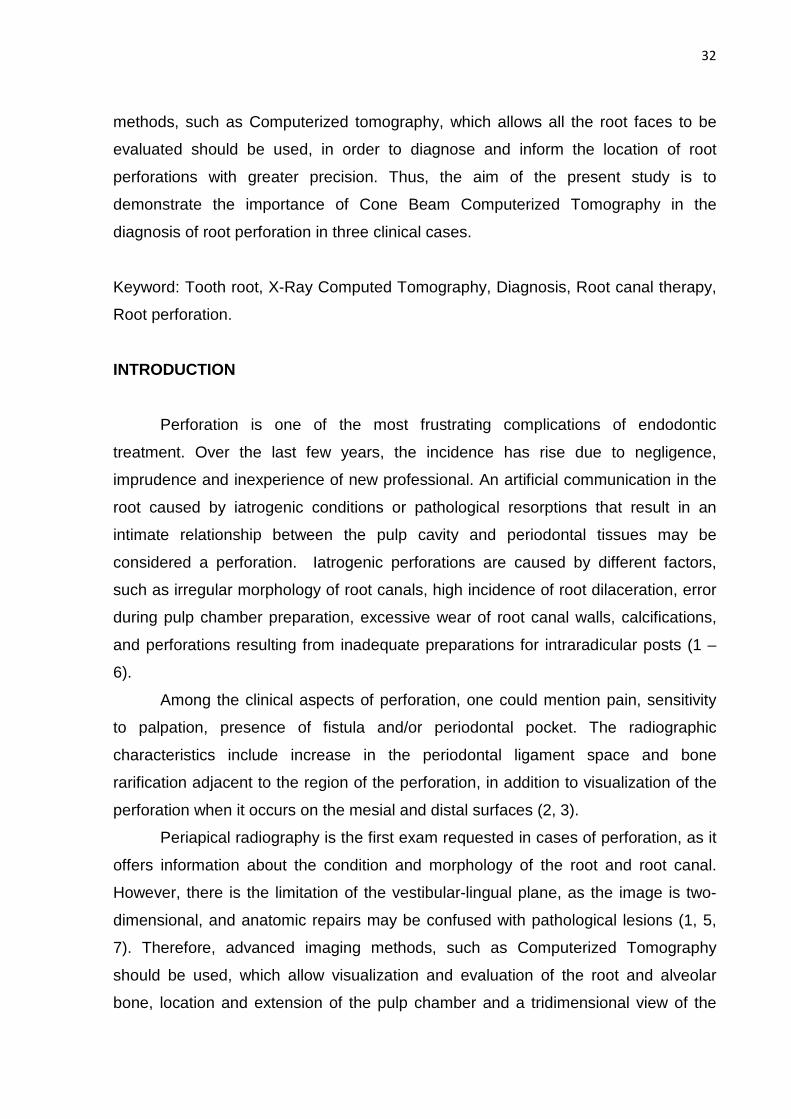
region of interest. In the panoramic reconstruction, a lesion was observed in the
furca, and in the oblique reconstructions the presence of perforation and periapical
radiolucency in the palatine root of the maxillary right first molar (Figure 1). In this
case, due to the compromised furca as and perforation confirmed clinically, the
prognosis was not favorable and the tooth was extracted.
34
Figure 1 – A) Note tooth 16 in the panoramic reconstruction (yellow arrow). B) Oblique reconstruction - note the white arrow indicating the presence of root perforation in tooth 16 (cut 25).
CLINICAL CASE 2:
The patient, M. J. G., 34 years of age presented at the dental clinic with slight
painful symptoms and swelling in the apical region of tooth 21 seven months after the
conclusion of endodontic treatment in this tooth.
Cone Beam Computerized Tomography was performed with the appliance
GXCB-500 Powered by i-CAT® (Imaging Sciences, Hatfield, USA). In the panoramic
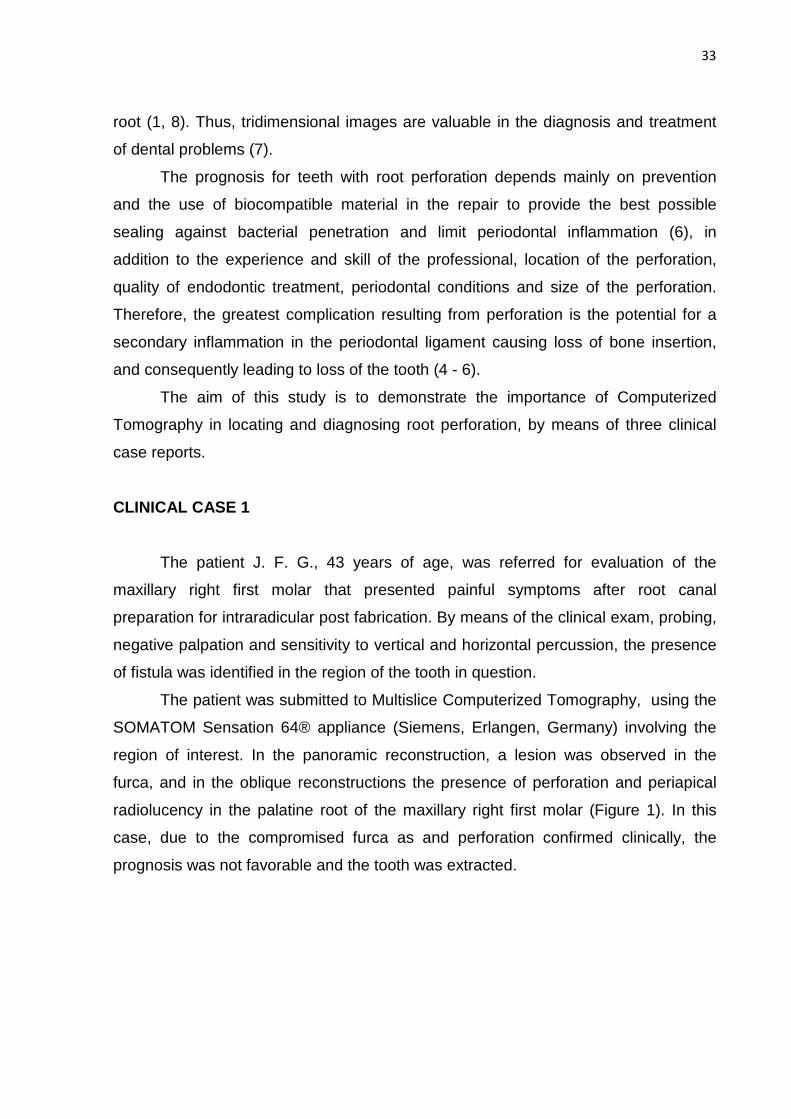
reconstruction, only periapical radiolucency was observed in the apex of the tooth 21.
In the oblique reconstructions, the presence of perforation can be identified (Figure
2). After clinical confirmation, the perforation was sealed with mineral trioxide
aggregate (MTA), as it is a biocompatible material that prevents leakage promotes
tissue regeneration.
35
Figure 2 – A) Panoramic Reconstruction – note the radiolucent image at the apex of tooth 21. (Arrow yellow). B) 3D Reconstruction. C) Oblique Reconstruction oblique – note the root perforation in cut 28.
CLINICAL CASE 3
The patient B. D. R, 27 years of age, was referred for evaluation of the right
central incisor which presented pain and recurrent fistula. During the clinical exam,
swelling and sensitivity to touch were verified in the region in question. The patient
was submitted to a Cone Beam Computerized Tomography exam of the maxilla,
performed with the appliance GXCB-500 Powered by i-CAT® (Imaging Sciences,
Hatfield, USA).
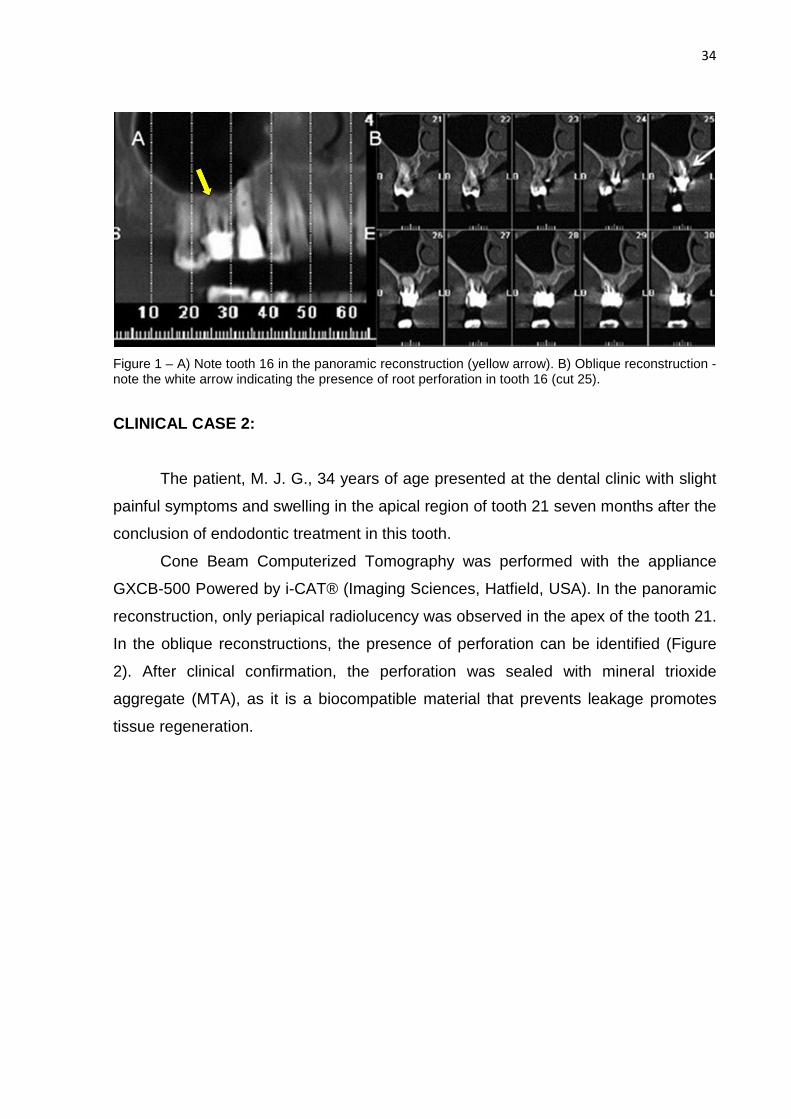
Periapical radiolucency was observed at the apex of the tooth 11 and a slightly
hyperdense image on the mesial face of the root. In the sagittal cut of tooth 11, the
presence of perforation was identified, in addition to extravasation of the filling
material in the middle third of the root (Figure 3). After clinical confirmation, the tooth
was extracted and the patient was referred for oral rehabilitation by means of an
implant in the region.
36
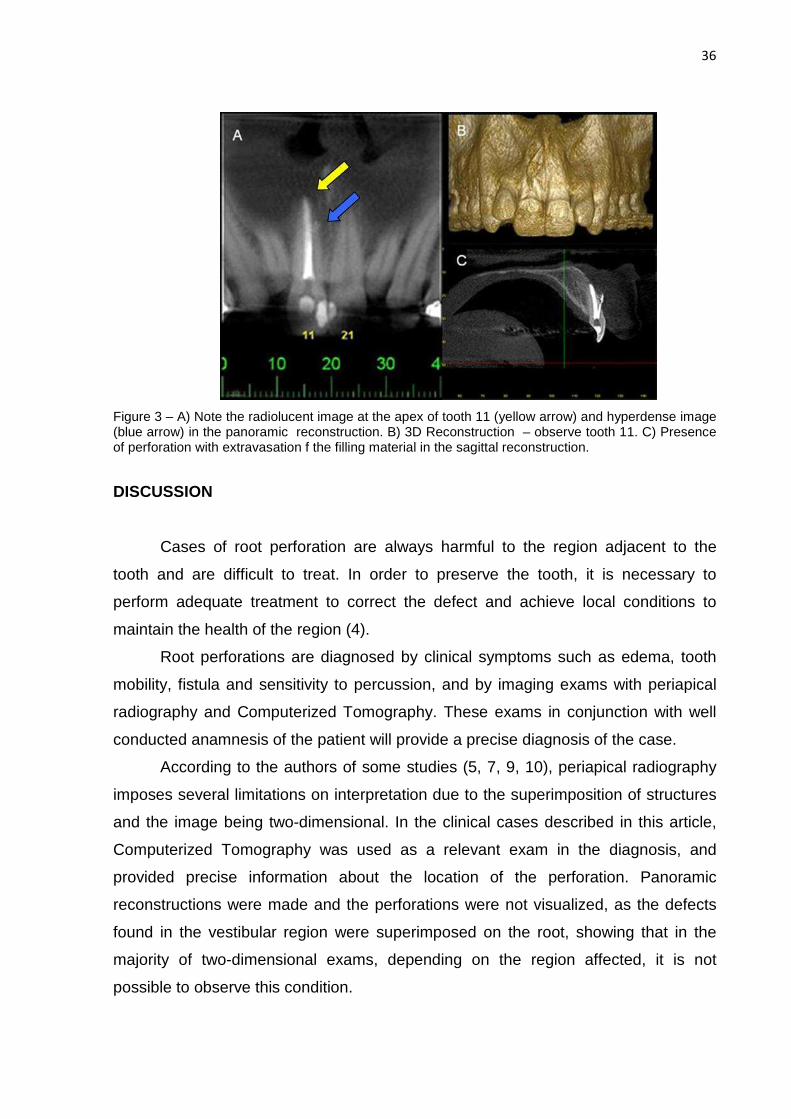
Figure 3 – A) Note the radiolucent image at the apex of tooth 11 (yellow arrow) and hyperdense image (blue arrow) in the panoramic reconstruction. B) 3D Reconstruction – observe tooth 11. C) Presence of perforation with extravasation f the filling material in the sagittal reconstruction.
DISCUSSION
Cases of root perforation are always harmful to the region adjacent to the
tooth and are difficult to treat. In order to preserve the tooth, it is necessary to
perform adequate treatment to correct the defect and achieve local conditions to
maintain the health of the region (4).
Root perforations are diagnosed by clinical symptoms such as edema, tooth
mobility, fistula and sensitivity to percussion, and by imaging exams with periapical
radiography and Computerized Tomography. These exams in conjunction with well
conducted anamnesis of the patient will provide a precise diagnosis of the case.
According to the authors of some studies (5, 7, 9, 10), periapical radiography
imposes several limitations on interpretation due to the superimposition of structures
and the image being two-dimensional. In the clinical cases described in this article,
Computerized Tomography was used as a relevant exam in the diagnosis, and
provided precise information about the location of the perforation. Panoramic
reconstructions were made and the perforations were not visualized, as the defects
found in the vestibular region were superimposed on the root, showing that in the
majority of two-dimensional exams, depending on the region affected, it is not
possible to observe this condition.
37
In 1981, Metzger, mentioned that the shape and direction of the alveolar bone
in relation to the root of the tooth and the shape of the root canal are essential
characteristics for successful endodontic treatment. Therefore, Computerized
Tomography can be mentioned as an important diagnostic imaging that provides
information about the anatomic structures, helping with planning and performing
endodontic treatment.
In 2011, D’Addazio et al, conducted a study to diagnose different endodontic
defects. As regards root perforations, periapical radiographs did not identify any
signs of perforation in 80% of the images evaluated and provided imprecise
diagnoses in 20% of the cases. With Cone Beam Computerized Tomography all the
alterations were identified, and 20% were precise. The tomographic exam offered
greater accuracy than periapical radiographs.
In their studies, in 2011, Bueno et al presented some considerations with
regard to false interpretations of images obtained by means of Cone Beam
Computerized Tomography due to metal artifacts. These may simulate endodontic
defects and confuse the diagnosis of root perforation. The artifacts appear as dark
strips producing errors of interpretation and may lead to disagreeable consequences
in endodontic therapy. However, correct handling of images may minimize errors in
diagnosis. Coronal, axial and sagittal images 0.2mm thick should be used, as was
done in the clinical cases reported, as they provide precise information on the exact
location of the point of communication between the root canals and periodontal
space, frequently associated with hypodense areas, suggesting root perforation. This
method overcomes the limitations of periapical radiography, with the possibility of
navigating the image, showing a dynamic visualization of images that previously
were static. In the cases reported in this study, it was verified that computerized
tomography enabled the diagnosis of root perforations in addition to helping with the
preparation of clinical planning.
CONCLUSION
To make a definitive diagnosis of perforations is challenging, particularly due
to the absence of pathognomonic clinical signs and the limited capacity of periapical
radiography to enable visualization of these perforations. Therefore, Computerized
Tomography is a technology that is useful to the endodontist in the diagnosis and
38
treatment of complex endodontic problems, as it allows tridimensional visualization of
structures in different planes. Nevertheless, it is important to remember that the final
diagnosis and choice of clinical therapy for root perforations must always be made in
conjunction with the clinical findings.
REFERENCES
1. Metzger Z, Shperling I. Iatrogenic perforation of the roots of restoration-
covered teeth. J Endod 1981; 7: 232-233. 2. Biggs JT, Benenati FW, Sabala CL. Treatment of iatrogenic root perforations
with associated osseus lesions. J Endod 1988; 14: 620-624. 3. Behnia A, Strassler HE, Campbell R. Repairing iatrogenic root perforations.
JADA 2000; 131: 196-201. 4. Alves DF, Gomes FB, Sayão SM, Mourato AP. Surgical clinical treatment of
perforation of the root channel with MTA-clinical report. Int J Dent 2005; 4: 37-40.
5. Eleftheriadis GI, Lambrianidis TP. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J, 2005;38: 725–734.
6. Young GR. Contemporary management of lateral root perforation diagnosed with the aid of dental computed tomography. Aust Endod J 2007; 33: 112–118.
7. D’Addazio PSS, Campos CN, Ozcan M, Teixeira HGC, Passoni RM, Carvalho ACP. A comparative study between cone-beam computed tomography and periapical radiographs in the diagnosis of simulated endodontic complications. Int Endod J, 2011; 44: 218–224.
8. Patel S, Dawood A, Pitt Ford T, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J, 2007; 40: 818-830.
9. Bueno MR, Estrela C, Figueiredo JAP, Azevedo BC. Map-reading Strategy to Diagnose Root Perforations Near Metallic Intracanal Posts by Using Cone Beam Computed Tomography. J Endod 2011; 37: 85-90.
10. Shemesh H, Cristescu RC, Wesselink PR, Wu MK. The Use of Cone-beam Computed Tomography and Digital Periapical Radiographs to Diagnose Root Perforations. J Endod 2011; 37: 515-516.
39
Artigo 3
Artigo será submetido ao Journal of Endodontics
DETECTION OF ROOT FRACTURE IN TEETH WITH METALLIC P OST BY
MEANS OF PERIAPICAL RADIOGRAPHS AND COMPUTED TOMOGR APHY
Priscila Dias Peyneau
Flávio Ricardo Manzi
Department of Oral Maxillofacial Radiology, Pontificial Catholic University of Minas
Gerais, Belo Horizonte, MG, Brazil
Address for Correspondence:
Prof. Dr. Flávio Ricardo Manzi
Av. Dom José Gaspar, Prédio 45 – Clínica de Radiologia
Coração Eucarístico, Belo Horizonte – MG
CEP: 30535-901
Phones: +55 31 – 3319-4591 // 31 – 8895-7033
ABSTRACT
Objectives : The purpose of this study was to compare the diagnosis of root fractures
in teeth with intracanal metallic posts by means of conventional periapical, digital
charge-coupled device (CCD) and phosphor plate (PSP), and multislice CT and cone
beam (CBCT). Methods : Sample consisted of 30 extracted single-rooted,
endodontically treated teeth and intracanal metallic posts. In the first phase of image
acquisition, these teeth showed no fracture. In a second step, the same teeth were
fractured by wedge pressure and image acquisition was performed again. Three
dental radiology experts evaluated the images. Results : The sensitivity (90%) and
specificity (95%) was calculated using the ROC curve and the best results were
40
obtained for images acquired by PSP, which could be manipulated. Images obtained
with digital radiography without manipulation, in both systems, and tomographic
images obtained in the two scanners showed no statistically significant differences
between them (CCD: 0.467-0.729, PSP: 0.5388-0.8112, CBCT: 0.5445-0,8155, CT
multislice: 0.5544-0.8202), however there were statistically significant differences
when they were compared with conventional periapical radiographs and digital
manipulation (conventional:0.7248-0.9352, CCD:0.7442-0.9458, PSP:0.8541-
0.9959). Conclusions : To evaluate the presence of root fractures in teeth with
intracanal metallic posts, the use of digital radiographic images is indicated. Digital
systems (CCD and PSP) showed the highest sensitivity, specificity and accuracy for
this condition.
Keywords: Diagnosis, Digital Dental Radiography, Fracture of the teeth, X-ray
Computed Tomography.
INTRODUCTION
The diagnosis of root fractures poses a challenge to dentists and is an
important procedure to evaluate the prognosis and determine the appropriate
treatment for the tooth. This type of lesion in teeth represents between 0.5% and 7%
of all injuries affecting permanent teeth (1). Among some of the etiological factors
involved in the occurrence of fractures, the following may be mentioned: physical
trauma, occlusal trauma, masticatory stress induced by repetitive parafunctional
habits, pathological resorption inducing root fracture, in addition to iatrogenic injuries
occurring during and after endodontic treatment, such as post placements or the
pressure applied to adapt them (2-4).
Conventional radiography is increasingly being replaced by the digital system,
as it provides two-dimensional images subject to resulting in superimposition of
overlapping adjacent structures (5-6). Recently, computed tomography technology
began to be used in dentistry, offering both the dentist and the patient assurance of
more effective planning and treatment by means of three-dimensional reconstruction
of the maxilla and mandible (2,3,4,7,8,9).
Even when one relies on the resources of several diagnostic imaging
methods, root fractures are still difficult to detect, particularly in teeth with intra-canal

41
metal posts. In dental clinics, the use of posts in endodontically treated teeth is a
frequent procedure, and consequently, fractures associated with this condition have
represented a major problem for dentists. In computed tomography, the root canal
filling material and the metal post impair fracture diagnosis, as these materials cause
imaging artifacts. Artifacts may be seen as obscured zones or stripes around the
endodontic material and the nucleus, similar to root fractures, and may lead to false-
positive readings (4). Thus, careful clinical examination and reliable imaging
diagnosis are required for the detection of root fractures.
The aim of the present study was to compare the accuracy of conventional
and digital periapical radiography and computed tomography (multislice and cone
beam) in the diagnosis of root fractures associated with intra-canal posts.
MATERIALS AND METHODS
Sample Preparation – Before Imaging procedures
The experimental group consisted of 30 extracted human mandibular first or
second premolars with complete root development, without fractures, periapical
pathologies or root resorption.
All root canals were filled with gutta-percha by the lateral condensation
technique. Next, part of the filling material was removed, leaving only 3 to 5 mm of
gutta-percha filling the root apex, in order to prepare the root canal to receive the
metal post.
Image Acquisition
Periapical Radiography:
Periapical radiographic images were acquired with a 60 kV, 10 mA KODAK
2200 Intraoral X-Ray System® (Kodak Eastman Company, USA ), operating with a
focus-receptor distance of 25 cm and 1.5 mm equivalent filtration and with an
exposure time of 0.35s for conventional images, and 0.23s for digital images. A 10
mm thick acrylic phantom was used to simulate the patient’s body (10-11). The
conventional periapical radiographic images were acquired with F Speed films (3 x 4
42
cm Kodak Insight films; Eastman Kodak Company, Rochester, NY, USA), using a
custom film holder, with the central X-ray beam positioned perpendicularly to the long
axis of the tooth (paralleling technique). The films were used and processed in an
automatic processor (AP 200, PLH Medical, Watford, England).
Two digital sensors were used for the digital periapical radiographs: CCD,
RVG 5.0 (Trophy, Marne la Valle, France), sensor size 2, with 10 lp/mm spatial
resolution and a photostimulable phosphor plate (PSP) CR 7400 (Trophy, Marne la
Valle, France), offering 10 lp/mm spatial resolution with 10.2s readout time. In the
same way as in the acquisition of the conventional images. The phosphor plates
were scanned immediately after exposure.
Computed Tomography
Tomographic images of the samples were obtained using i-CAT CBCT
(Imaging Sciences, Hatfield, PA, USA), operated at 120 kVp, 5 mA and a Somatom
Sensation 64 Multislice CT (Siemens AG, Forchheim, Germany), operated at 120
kVp, 150 mAs, and collimation 64x0.6. The scans were performed with a 14 X 8 cm
field of view (FOV) selection for cone beam computed tomography (CBCT). The
datasets were exported in DICOM file format, and the size of the isotropic voxel was
0.25 mm. The data were reconstructed with cuts of 1mm thick and the teeth were
placed in the center of the volume.
For Multislice CT, craniocaudal scanning was performed from the mandibular
base extending up to the alveolar crest. The slice thickness was adjusted to 1 mm at
1 mm intervals. Axial images were acquired and subsequently processed by means
of the dental computed tomography (DCT) reformatting program. Multiplanar image
reconstruction based on the DCT protocol was obtained in the orthoradial panoramic
plane on a workstation running a dental software package (Syngo Dental CT 2006 A-
W VB20B-W). The sections were reformatted to place the teeth in a vertical position.
Sample Preparation - After Image Acquisition
Root fractures were mechanically induced in the vertical plane, as described
by Nair et al (12), and some fracture lines were made vertically and some
horizontally, according to force falling on the tooth. The two fragments were then
43
assembled and glued without displacement. The intraradicular posts were
repositioned within the root canals and fixed with utility wax, and then the teeth were
submitted to a new series of radiography and CT scans.
Image Evaluation
All the radiographic and tomographic images were individually analyzed by
three oral and maxillofacial radiology specialists who were blind to procedures,
methods, and the conditions of the tooth roots. The conventional intraoral
radiographs were observed on a light box, the CCD and PSP images were analyzed
on a Dell PWS 670 Workstation (Dell Inc., Round Rock, TX, USA) with Intel® Core™
i5-2500K Processor (6M Cache, 3.30 GHz) and a 22-inch Dell-monitor, with and
without the aid of software tools (brightness, contrast, zoom, negative and color).
Volumetric data obtained with CBCT and Multislice CT were exported as DICOM files
and imported into a specially designed DICOM viewer software program (Dental
Slice; Bioparts, Brasília, Brazil). The exported data were reconstructed, yielding
cross-sectional coronal images perpendicular to the fracture lines. The observers
were free to use the available image-enhancement options (density, contrast and
magnification).
The fractures were diagnosed by means of direct visualization of a radiolucent
line traversing the root. The images were classified according to a visual scale: A1-
Root fracture definitely not present; A2-Root fracture probably not present; B-
Unsure; B1-Root fracture definitely present; B2-Root fracture probably present (3,
13).
The Kappa index was calculated to assess intra- and inter-observer
agreement for each image set. The rating assigned to conventional, digital images
and CT images were compared with the gold standard using receiver operating
characteristic (ROC curves) to evaluate the observer’s ability to differentiate between
teeth with and without root fracture.
The areas under the ROC curves (Az values) were calculated using the
BioEstat 5.0 software (Belem, Brazil) and these Az values for each image type were
compared using the Cochran's Q test with a significance level set at p=0.05. The
rates of true negative (correct identification of a nonfractured root), true positive
44
(fracture in a fractured root), false positive (fracture in a nonfractured root), false
negative (nonfracture in a fractured root) and accuracy were calculated.
Radiographic and CT images for each acquisition modality (conventional, CCD
without manipulation, CCD with manipulation, PSP without manipulation, cone beam
computed tomography and multislice computed tomography) were compared.
Sequentially, the graphs present the ROC curves for the image sets produced in the
present study, and the curves are differentiated by the areas (14-15).
RESULTS
The digital images without manipulation present a smaller graph area (the
vertex of the graph of the digital images without manipulation (B) are closer to the 45°
straight line). However, the digital images with use of manipulation presented larger
areas, particularly in the phosphor system (PSP). When the images from the two
digital systems (CCD and PSP) with manipulation by the system software were
compared, it was verified that the phosphor system presented a larger area, while the
CCD system presented an area very similar to that of the conventional radiographic
image. Conventional radiographic and computed tomography (cone beam and
Multislice) images were compared, the conventional radiographic images presented
a much larger area compared with the CT images. When the tomographic images
were compared, the areas were very similar to each other. And finally, digital
radiographic with manipulation images present larger areas than the tomographic
images (Figure 1).
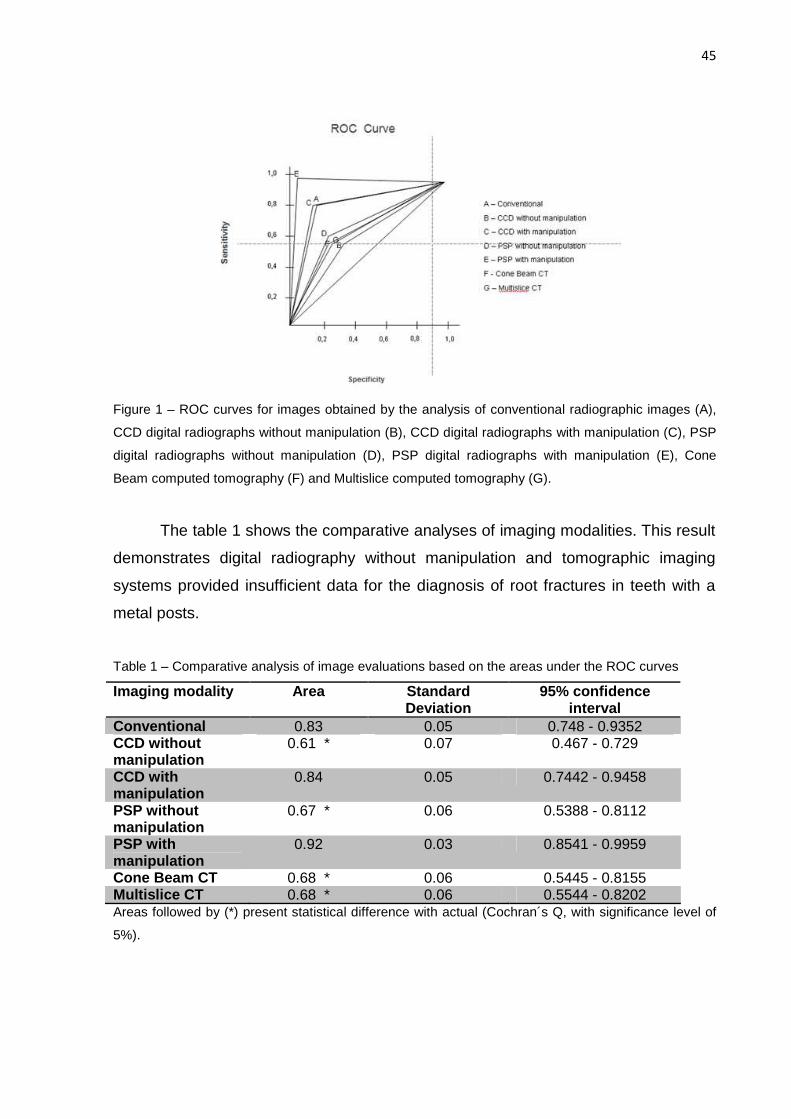
45
Figure 1 – ROC curves for images obtained by the analysis of conventional radiographic images (A),
CCD digital radiographs without manipulation (B), CCD digital radiographs with manipulation (C), PSP
digital radiographs without manipulation (D), PSP digital radiographs with manipulation (E), Cone
Beam computed tomography (F) and Multislice computed tomography (G).
The table 1 shows the comparative analyses of imaging modalities. This result
demonstrates digital radiography without manipulation and tomographic imaging
systems provided insufficient data for the diagnosis of root fractures in teeth with a
metal posts.
Table 1 – Comparative analysis of image evaluations based on the areas under the ROC curves
Imaging modality Area Standard Deviation
95% confidence interval
Conventional 0.83 0.05 0.748 - 0.9352 CCD without manipulation
0.61 * 0.07 0.467 - 0.729
CCD with manipulation
0.84 0.05 0.7442 - 0.9458
PSP without manipulation
0.67 * 0.06 0.5388 - 0.8112
PSP with manipulation
0.92 0.03 0.8541 - 0.9959
Cone Beam CT 0.68 * 0.06 0.5445 - 0.8155 Multislice CT 0.68 * 0.06 0.5544 - 0.8202 Areas followed by (*) present statistical difference with actual (Cochran´s Q, with significance level of
5%).
46
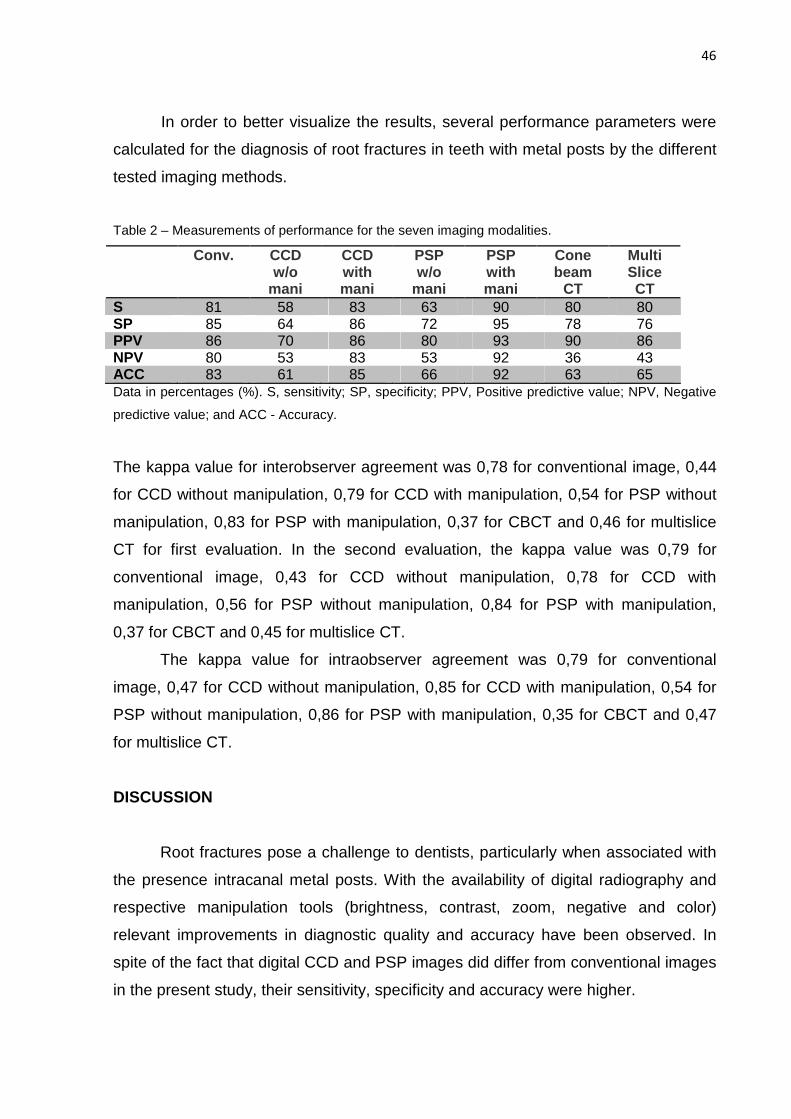
In order to better visualize the results, several performance parameters were
calculated for the diagnosis of root fractures in teeth with metal posts by the different
tested imaging methods.
Table 2 – Measurements of performance for the seven imaging modalities.
Conv. CCD w/o
mani
CCD with mani
PSP w/o
mani
PSP with mani
Cone beam
CT
Multi Slice CT
S 81 58 83 63 90 80 80 SP 85 64 86 72 95 78 76 PPV 86 70 86 80 93 90 86 NPV 80 53 83 53 92 36 43 ACC 83 61 85 66 92 63 65 Data in percentages (%). S, sensitivity; SP, specificity; PPV, Positive predictive value; NPV, Negative
predictive value; and ACC - Accuracy.
The kappa value for interobserver agreement was 0,78 for conventional image, 0,44
for CCD without manipulation, 0,79 for CCD with manipulation, 0,54 for PSP without
manipulation, 0,83 for PSP with manipulation, 0,37 for CBCT and 0,46 for multislice
CT for first evaluation. In the second evaluation, the kappa value was 0,79 for
conventional image, 0,43 for CCD without manipulation, 0,78 for CCD with
manipulation, 0,56 for PSP without manipulation, 0,84 for PSP with manipulation,
0,37 for CBCT and 0,45 for multislice CT.
The kappa value for intraobserver agreement was 0,79 for conventional
image, 0,47 for CCD without manipulation, 0,85 for CCD with manipulation, 0,54 for
PSP without manipulation, 0,86 for PSP with manipulation, 0,35 for CBCT and 0,47
for multislice CT.
DISCUSSION
Root fractures pose a challenge to dentists, particularly when associated with
the presence intracanal metal posts. With the availability of digital radiography and
respective manipulation tools (brightness, contrast, zoom, negative and color)
relevant improvements in diagnostic quality and accuracy have been observed. In
spite of the fact that digital CCD and PSP images did differ from conventional images
in the present study, their sensitivity, specificity and accuracy were higher.
47
Most studies (3,4,5,13,16,17) comparing radiographic and tomographic
imaging techniques in the diagnosis of root fractures were limited to teeth without the
presence of intracanal metal posts, or with the fracture already present. However, the
results of the present study demonstrated that tomographic images presented the
worst results, particularly as regards false-positive results and method specificity.
Tomographic images are not appropriate for demonstrating the absence of root
fracture in teeth with metal posts, as the imaging artifact produced by the metal post
leads the observer to seeing fractures in healthy roots (false positive). It is important
to highlight that computed tomography is highly effective in the diagnosis of other
endodontic conditions (18-19), but the use of intracanal metal posts is a limiting
factor for the diagnosis of root fracture, as demonstrated by the present study. This
hypothesis is supported by studies (2,5,20) reporting the detection of false negative
results because of the presence of imaging artifacts caused by root canal filling
material and intracanal posts. In a recent study (20), the CBCT presented high
accuracy in the detection of horizontal fractures without metal posts. However, the
presence of metal posts causes significant decrease in sensitivity and specificity of
CBCT.
The radiation dose is a factor that should be taken into consideration in order to
protect the patient from unnecessary exposure. The digital system delivers a lower
radiation dose when compared with conventional periapical radiography and
particularly, tomography (19, 21-23). The results of the present study demonstrate
that conventional radiography and digital CCD and PST digital systems obtained
better results in comparison with computed tomography; therefore it is possible to
conclude that a small radiation dose will be used in patients for the diagnosis of root
fracture with intracanal metal post.
CONCLUSION
Digital radiography is indicated for detecting the presence of root fractures in
teeth with intracanal metal posts. The digital systems (PSP and CCD) presented the
highest sensitivity, specificity and accuracy levels for this condition.
48
REFERENCES
1. Andreasen JO. Traumatic injuries of the teeth. 2nd ed. WB Saunders: Philadelphia, 1981.
2. Youssefzadeh S, Gahleitner A, Dorffner R, Bernhart T, Kainberger F. Dental vertical root fractures: value of CT in detection. Radiology 1999;210(2):545-9.
3. Mora M, Mol A, Tyndall D, Rivera E. In vitro assessment of local computed tomography for the detection of longitudinal tooth fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103(6):825-9.
4. Kamburoglu K, Murat S, Yuksel SP, Cebeci AR, Horasan S. Detection of vertical root fracture using cone-beam computerized tomography: an in vitro assessment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109(2):e74–81.
5. Kamburoglu K; Cebeci I; Grondahl H. Effectiveness of limited cone-beam computed tomograph in the detection of horizontal root fracture. Dent Traumatol 2009; 25(3):256-261.
6. Kositbowornchai S, Sikram S, Nuansakul R, Thinkhamrop B. Root fracture detection on digital images: effect of the zoom function. Dent Traumatol 2003;19(3):154-159.
7. Hassan B, Metska ME, Ozok AR, Stelt P, Wesselink PR. Detection of vertical root fractures in endodontically treated teeth by a cone beam computed tomography scan. J Endod 2009; 35(5): 719-722.
8. Ilguy D, Ilguy M, Fisekcioglu E, Bayirli G. Detection of jaw and root fractures using cone beam computed tomography: a case report. Dentomaxillofac Radiol 2009;38: 169–173.
9. Wenzel A, Haiter-Neto F, Frydenberg M, Kirkevang LL. Variable-resolution cone-beam computerized tomography with enhancement filtration compared with intraoral photostimulable phosphor radiography in detection of transverse root fractures in an in vitro model. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:939–45.
10. Caldas MP, Ramos-Perez FM, de Almeida SM, Haiter-Neto F. Comparative evaluation among different materials to replace soft tissue in oral radiology studies J Appl Oral 2010;18(3):264-7.
11. Sogur E, Baks BG, Grondahl HG. Imaging of root canal fillings: a comparison of subjective image quality between limited conebeam CT, storage phosphor and film radiography. Int Endod J 2007;40(3):179–185.
12. Nair MK, Nair UDP, Grondahl HG, Webber RL, Wallace JA. Detection of artificially induced vertical radicular fractures using Tuned Aperture Computed Tomography. Eur J Oral Sci 2001;109(6):375-9, Set 2001.
13. Bernardes RA; Moraes IG; Duarte MAH; Azevedo BC; Azevedo JR; Bramante CM. Use of cone-beam volumetric tomography in the diagnosis of root fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108(2):270-277.
14. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1): 29-36.
15. Wenzel A, Verdonschot EH. Some considerations in the evaluation of diagnostic tests in Dentistry. Dentomaxillofac Radiol. 1994; 23(4):179-82.
16. Iikubo, Masahiro. et al. Accuracy of intraoral radiography, multidetector helical CT, and limited cone-beam CT for the detection of horizontal tooth root
49
fracture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108(5): e70-4.
17. Wang P, Yan XB, Lui DG, Zhang WL, Zhang Y and Ma XC. Detection of dental root fractures by using cone-beam computed Tomography Dentomaxillofac Radiol 2011;40(5):290–298.
18. Scarfe, WC. Use of cone-beam computed tomography in endodontics. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(2):234-7.
19. Nair MK, Nair UP. Digital an advanced imaging in endodontics: a review. J Endod 2007;33(1):1-6.
20. Costa FF, Gaia BF, Umetsubo OS, Cavalcanti MGP. Detection of Horizontal Root Fracture with Small-volume Cone-Beam Computed Tomography in the Presence and Absence of Intracanal Metallic Post. J Endod 2011;37(10):1456-9.
21. Bueno MK, Estrela C, Azevedo BC. Tomografia computadorizada cone beam: revolução na odontologia. Rev Assoc Paul Cir Dent 2007;61(5):354-63.
22. Roberts JA, Drage NA, Davies J, Thomas DW. Effective dose from cone beam CT examinations in dentistry. Br J Radiol 2009;82(973):35-40.
23. Sakurai T et al. Relationship between radiation dose reduction and image quality change in photostimulable phosphor luminescence X-ray imaging systems. Dentomaxillofac Radiol 2010;39(4):207-215.
50
REFERÊNCIAS
ANDREASEN, JO. Traumatic injuries of the teeth . 2nd ed. WB Saunders: Philadelphia, 1981. ARAI, Y. et al. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofacacial Radiology , v. 28, n. 4, p. 245-8, Jul 1999. BERNARDES, Ricardo Affonso.et al. Use of cone-beam volumetric tomography in the diagnosis of root fractures. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology , v. 108, n. 2, p. 270-77, Aug 2009. BRANDINI, Daniela. et al. Integrated treatment to resolve a horizontal root fracture. Dental Traumatology , v. 25, n. 2, p. 16-20, Apr 2009. CALDAS, Maria de Paula. et al. Comparative evaluation among different materials to replace soft tissue in oral radiology studies Journal of Applied Oral Science , v. 18, n. 3, p. 264-7, May-Jun 2010. COSTA, Felipe Ferreira. et al. Detection of Horizontal Root Fracture with Small-volume Cone-Beam Computed Tomography in the Presence and Absence of Intracanal Metallic Post. Journal of Endodontics , v. 37, n. 10, p. 1456-9, Oct 2011. HASSAN, Bassam. et al. Detection of vertical root fractures in endodontically treated teeth by a cone beam computed tomography scan. Journal of Endodontics , v. 35, n. 5, p. 719-22, May 2009. HASSAN, Bassam. et al. Comparison of five cone beam computed tomography systems for the detection of vertical root fractures. Journal of Endodontics , v. 36, n. 1, p. 126-9, Jan 2010. HANLEY JA, MCNEIL BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology , v. 143, n. 1, p. 29-36, Apr 1982. IIKUBO, Masahiro. et al. Accuracy of intraoral radiography, multidetector helical CT, and limited cone-beam CT for the detection of horizontal tooth root fracture. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology , v. 108, n. 5, p. e70-4, Nov 2009. ILGUY D, ILGUY M, FISEKCIOGLU E, BAYIRLI G. Detection of jaw and root fractures using cone beam computed tomography: a case report. Dentomaxillofacial Radiology , v. 38, n. 3, p. 169-173,Mar 2009. KAMBUROGLU, Kivanç. et al. Effectiveness of limited cone-beam computed tomograph in the detection of horizontal root fracture. Dental Traumatology , v. 25, n. 3, p. 256-61, Jun 2009. KAMBUROGLU, Kivanç. et al. Detection of vertical root fracture using cone-beam computerized tomography: an in vitro assessment. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology , v. 109, n. 2, p. e74-81, Feb 2010.
51
KOSITBOWORNCHAI, Suwadee. et al. Root fracture detection on digital images: effect of the zoom function. Dental Traumatology , v. 19, n. 3, p. 154-59, Jun 2003. MIREKU, AS. et al. Vertical fracture of root filled teeth restored with posts: the effect of patient age and dentine thickness. International Endodontic Journal , v. 43, n. 3, p. 218-225, Mar 2010. MONAGHAN, Peter. et al. A method for producing experimental simple vertical root fractures in dog teeth. Journal of Endodontics , v. 19, n. 10, p. 512-15, Oct 1993. MORA, Maria. et al. In vitro assessment of local computed tomography for the detection of longitudinal tooth fractures. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology , v. 103, n. 6, p. 825-9, Jun 2007. NAIR, Madhu et al. Detection of artificially induced vertical radicular fractures using Tuned Aperture Computed Tomography. European Journal of Oral Sciences , v. 109, n. 6, p. 375-9, Dec 2001. SOGUR, E; BAKS, BG; GRONDAHL, HG. Imaging of root canal fillings: a comparison of subjective image quality between limited conebeam CT, storage phosphor and film radiography. International Endodontic Journal , v. 40, v. 3, p. 179–185, Mar 2007. YOUSSEFZADEH, Soraya. et al. Dental vertical root fractures: value of CT in detection. Radiology , v. 210, n. 2, p. 545-9, Feb 1999. WENZEL, Ann; VERDONSCHOT EH. Some considerations in the evaluation of diagnostic tests in dentistry. Dentomaxillofacial Radiology , v. 23, n. 4, p. 179-82, Nov 1994. WENZEL, Ann. et al. Variable-resolution cone-beam computerized tomography with enhancement filtration compared with intraoral photostimulable phosphor radiography in detection of transverse root fractures in an in vitro model. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology , v. 108, n. 6, p. 939–45, Dec 2009.





























