-
344 DIABETES CARE, VOLUME 24, NUMBER 2, FEBRUARY 2001
Functional abnormalities of the micro-circulation have gained
significantattention in recent years for theirpotential pathogenic
role in the develop-ment of diabetic complications,
particularlydiabetic neuropathy and diabetic foot prob-
lems (15). The microvascular tone is reg-ulated by several
humoral and neural fac-tors. The vascular endothelium has
animportant role in controlling the microvas-cular tone by
releasing several vasodilatorsubstances such as nitric oxide,
prostacyclin
and endothelium-derived hyperpolarizingfactor, and
vasoconstrictor substances suchas prostaglandins and endothelin
(6). Nitricoxide is the most important vasodilatorsubstance
responsible for endothelium-dependent vasodilation. After its
secretionfrom the endothelium, it diffuses to theadjacent smooth
muscle cells and stimu-lates the guanylate cyclase enzyme to
pro-duce cyclic guanosine 3,5-monophos-phate, which, in turn, leads
to smoothmuscle relaxation and vasodilation (7).
The normal neurovascular responseconducted through the C
nociceptive nervefibers is another important mechanism forthe
regulation of the microcirculation.Stimulation of the C nociceptive
nervefibers leads to antidromic stimulation of theadjacent C
fibers, which secrete vasodilat-ing substances such as substance P
andbradykinin, causing vasodilation at theinjured or inflamed skin
areas. This vasodi-lating response, also known as the
Lewistriple-flare response, is decreased in thepresence of diabetic
neuropathy. Reductionof local blood flow increases the
vulnera-bility of the neuropathic limb to severe dia-betic foot
problems (8,9). It has beenpostulated that the abnormality in the
neu-rovascular response in the neuropathiclimb further aggravates
the abnormalities inthe microcirculation, and a vicious cyclemay
ensue (10).
Several recent studies (1013) havedemonstrated reduced
endothelium-dependent vasodilation in patients witheither type 1 or
type 2 diabetes. However,little information is available regarding
thecontribution of nerve-axon reflex-relatedvasodilatation to
maximal skin vasodila-tion in such patients (8,9). The
recentdevelopment of noninvasive techniquesthat can reliably
quantify blood flow in theskin microcirculation has made it
possibleto study changes in microvascular functionin patients with
diabetes (14,15). In thepresent study, we have examined the
con-tributing role of the nerve-axon reflex-related vasodilation
response to the totalskin vasodilation at both the forearm and
From the Clinical Research Center (O.H., K.A.-E., E.S.H.),
Joslin Diabetes Center, Department of Medicine,and the JoslinBeth
Israel Deaconess Foot Center and Microcirculation Laboratory
(F.W.L., A.V.), Departmentof Surgery, Beth Israel Deaconess Medical
Center, Harvard Medical School, Boston, Massachusetts.
Address correspondence and reprint requests to Aristidis Veves,
MD, Microcirculation Laboratory, Palmer317, West Campus, Beth
Israel Deaconess Medical Center, One Deaconess Road, Boston, MA
02215. E-mail:[email protected].
Received for publication 6 July 2000 and accepted in revised
form 19 October 2000.Abbreviations: CV, coefficient of variation.A
table elsewhere in this issue shows conventional and Systme
International (SI) units and conversion
factors for many substances.
Contribution of Nerve-Axon Reflex-Related Vasodilation to the
TotalSkin Vasodilation in Diabetic PatientsWith and Without
Neuropathy
O R I G I N A L A R T I C L E
OBJECTIVE To examine the contribution of nerve-axon
reflex-related vasodilation tototal acetylcholine-induced
vasodilation in the skin of normal and diabetic subjects.
RESEARCH DESIGN AND METHODS The skin microcirculation was
evaluated atthe forearm level in 69 healthy subjects and 42
nonneuropathic diabetic patients and at the footlevel in 27 healthy
subjects and 101 diabetic patients (33 with neuropathy, 23 with
Charcotarthropathy, 32 with peripheral vascular disease and
neuropathy, and 13 without complications).Two single-point laser
probes were used to measure total and neurovascular
vasodilationresponse to the iontophoresis of 1% acetylcholine, 1%
sodium nitroprusside, and deionized water.
RESULTS The neurovascular response to acetylcholine was
significantly higher than theresponse to sodium nitroprusside and
deionized water (P 0.01). At the forearm level, thecontribution of
neurovascular response to the total response to acetylcholine was
35% in dia-betic patients and 31% in control subjects. At the foot
level, the contribution was 29% in dia-betic patients without
neuropathy and 36% in control subjects, while it was
significantlydiminished in the three neuropathic groups. A
significantly lower nonspecific nerve-axonrelated vasodilation was
observed during the iontophoresis of sodium nitroprusside,which
does not specifically stimulate the C nociceptive fibers.
CONCLUSIONS Neurovascular vasodilation accounts for
approximately one-third of thetotal acetylcholine-induced
vasodilation at both the forearm and foot levels. The presence
ofdiabetic neuropathy results in reduction of both the total
vasodilatory response to acetylcholineand the percentage
contribution of neurovascular vasodilation to the total response.
Acetyl-choline and sodium nitroprusside cause vasodilation in the
skin microcirculation through dif-ferent pathways.
Diabetes Care 24:344349, 2001
OSAMA HAMDY, MDKARIM ABOU-ELENIN, MDFRANK W. LOGERFO, MD
EDWARD S. HORTON, MDARISTIDIS VEVES, MD
P a t h o p h y s i o l o g y / C o m p l i c a t i o n s
-
DIABETES CARE, VOLUME 24, NUMBER 2, FEBRUARY 2001 345
Hamdy and Associates
foot levels of neuropathic and nonneuro-pathic diabetic
patients.
RESEARCH DESIGN AND METHODS
PatientsWe studied the skin microcirculation at theforearm level
in 69 healthy subjects and 42nonneuropathic diabetic subjects. The
fol-lowing exclusion criteria were applied tosubjects in all
groups: smoking anyamount of cigarettes during the previous
6months, subjects with diagnosed cardio-vascular disease (coronary
artery disease,arrhythmia, congestive heart failure),stroke or
transient ischemic attack, periph-eral vascular disease (symptoms
of claudi-cation and/or absence of peripheralpulses), chronic renal
disease, severe dys-lipidemia (triglycerides 600 mg/dl
orcholesterol 300 mg/dl), or any other seri-ous chronic disease
requiring active treat-ment. Subjects were also excluded if
theywere on any of the following medications:any type of
antihypertensive drugs, lipid-lowering agents, glucocorticoids,
antineo-plastic agents, psychoactive agents, orbronchodilators. In
addition, diabeticpatients with proliferative
retinopathy,peripheral somatic neuropathy, macroal-buminuria
(expressed as albumin-to-crea-tinine ratio 300 g/mg), and/or
oninsulin or troglitazone were excluded fromthe study.
We also evaluated the skin microvascu-lar reactivity at the foot
level in 27 healthysubjects and 101 diabetic patients who
weredivided into four groups. The first groupconsisted of 33
diabetic neuropathicpatients with a history of foot ulceration
butno peripheral vascular disease, the second
group of 23 diabetic patients with Charcotarthropathy, the third
group of 32 diabeticpatients with peripheral vascular diseaseand
neuropathy, and the fourth group of 13diabetic patients without any
complications.
All healthy subjects were free of any ill-ness and did not take
any medications. Spe-cial emphasis was given to exclude anyonewith
a history of hypertension, diabetes,hypercholesterolemia, active
tobacco use,history of any systemic illness, or the use ofany
antihypertensive, cardiac, or hormonalmedication. Patients with
either type 1 ortype 2 diabetes were included. Patients
withnephropathy (creatinine 2 mg/l), severeheart failure, or any
other serious illnesswere excluded from the study.
Further details of the characteristics ofthe study population
are shown in Tables 1and 2. The study was approved by
theinstitutional review board, and consent wasobtained from all
participants.
MethodsA history, physical examination, and fastingplasma
glucose measurement were per-formed on all patients. Diabetic
neuropathywas diagnosed according to the San Anto-nio Consensus
Statement criteria (16). Thesymptoms were evaluated by using a
neu-ropathy symptom score, and the clinicalsigns were evaluated by
using a neuropathydisability score (17). Quantitative
sensorytesting included the assessment of vibrationperception
threshold using a Biothesiome-ter and cutaneous perception
thresholdusing Semmes-Weinstein monofilaments(18,19). The diagnosis
of Charcot neu-roarthropathy was made when grossdestruction of the
joints of the mid-footthat resulted in significant foot
deformitywas present. Patients were characterized ashaving
peripheral vascular disease based onthe presence of one or more of
the follow-ing clinical features: claudication, absentfoot pulses,
and/or abnormal invasive andabnormal noninvasive vascular
tests.
Each participant was studied after a 20-min acclimatization
period in a warm envi-ronment (room temperature 2324C). Weused two
single-point laser probes and aDRT4 Laser Doppler Blood Flow
Monitor
Table 1Characteristics of the forearm study subjects
Diabetic nonneuropathic patients Control subjects
n 42 69Age (years) 54 9 49 9Men/women 21/21 33/36Type 2 diabetes
42 Diabetes duration (years) 4 5 BMI (kg/m2)* 32.3 6.3 27.3
4.3HbA1c (%)* 8.0 1.6 5.6 0.4Albumin-to-creatinine ratio 30 50
Neuropathy symptom score* 1.43 2.27 0.02 0.13Neuropathy disability
score* 0.8 1.45 0.15 0.62Vibration perception threshold* 15.86 9.5
10.69 6.39
Data are means SD. *P 0.001.
Table 2Characteristics of the foot study subjects
Charcot Neuropathy and Diabetic patients ControlNeuropathy
arthropathy peripheral vascular without subjects
(DN) (DA) disease (DI) complications (D) (C)
n 33 23 32 13 27Age (years)* 56 9 57 9 60 8 39 10 52 13Men/women
24/9 13/10 23/9 9/4 13/14Type of diabetes (1/2) 12/21 5/18 16/16
8/5 Diabetes duration 21 12 17 11 25 13 17 7 BMI (kg/m2) 30.3 6.8
29.5 4.8 27.8 4.5 26.8 4.5 27.5 4.9HbA1c (%) 8.7 2.7 8.7 2.0 8.9
0.9 9.9 4.3 Creatinine (mg/dl) 1.03 0.3 1.01 0.4 1.05 0.031 1.02
0.03 Neuropathy 3.2 2.9 2.9 2.5 3.5 2.8 0.5 1.1 0.1 0.4symptom
score
Neuropathy 19.3 6.1 21.8 3.9 18.7 6.7 0.5 1.2 0.4 1.2disability
score
Vibration perception 48 5 50 3.4 47 8 11 5 12 6threshold
Semmes-Weinstein 6.6 0.7 6.9 0.4 6.6 0.5 4 0.5 4
0.5monofilaments
Data are means SD. *DN, DA, and DI vs. D, P 0.001; DN, DA, and
DI vs. D and C, P 0.001.
-
346 DIABETES CARE, VOLUME 24, NUMBER 2, FEBRUARY 2001
Nerve-axon reflex and skin vasodilation
(Moor Instruments, Millwey, Devon, U.K.)to evaluate the skin
microcirculation. Fore-arm microcirculatory flow was measuredover
the flexor surface of the forearm, andfoot microcirculatory flow
was measuredover the dorsum of the foot. The blood flowresponse was
measured in response to ion-tophoresis of each of three substances:
1%acetylcholine chloride solution (a substancethat elicits both a
neurovascular responseand endothelium-dependent vasodilation),1%
sodium nitroprusside (a substance thatdoes not elicit a
neurovascular response,but induces
endothelium-independentvasodilation), and deionized water (used asa
control during iontophoresis to measurethe vasodilation caused by
the direct effectof a constant current flow) (10). Deionizedwater
was iontophoresed in both anodalmode (the same mode in which the
ion-tophoresis of acetylcholine is performed)and cathodal mode (the
mode that the ion-tophoresis of sodium nitroprusside is
per-formed). The difference in these two modesis the polarity of
the iontophoresis chamber:the chamber serves as the anode for
ion-tophoresis of acetylcholine, which has anegative electrical
charge, and as the cath-ode for the iontophoresis of sodium
nitro-prusside, which has a positive electricalcharge. Therefore,
the constant current hasan opposite direction when the polarity
ofthe chamber is changed.
The iontophoresis instrument (MIC1iontophoresis system; Moor
Instruments)consists of an iontophoresis delivery vehicledevice
that sticks firmly to the skin with thehelp of adhesive tape. The
device containstwo chambers that accommodate two sin-gle-point
laser probes. One probe is placed
within the chamber containing the ion-tophoresis solution (thus
measuring thedirect response to acetylcholine or
sodiumnitroprusside iontophoresis), while the sec-ond probe is
placed outside but withinproximity (within 5 mm) to the
ion-tophoresis solution chamber, thus meas-uring the indirect
nerve-axonrelatedresponse that results from stimulation of theC
nociceptive nerve fibers. A small amount(1 ml) of test solution was
applied to theiontophoresis chamber. Subsequently, aconstant
current of 200 A for 60 s wasapplied, achieving a dose of 6
mC/cm2
between the iontophoresis chamber and asecond nonactive
electrode placed 1015cm proximal to the chamber. The two
laserprobes recorded changes in skin blood flow.Measurements were
obtained for 40 sbefore the iontophoresis, during the
ion-tophoresis, and 90 s after it (10,11). Theday-to-day
reproducibility of the techniquewas evaluated in five healthy
subjects (fourmen and one woman, ages 2339 years)who were
repeatedly tested at their footand forearm for 10 consecutive
workingdays. With use of a single-point laser probe,the coefficient
of variation (CV) for the base-line blood flow before iontophoresis
ofacetylcholine was 60.6% and for the maxi-mal hyperemic response
was 35.2% afterthe iontophoresis of acetylcholine.
Statistical analysisThe results were recorded and
tabulatedbefore revealing the patient category assig-nations.
Changes in microvascular bloodflow were expressed as the percentage
ofincrease over baseline, where median, firstquartile, and third
quartile values are used
for comparisons. Parametric data wereexpressed as means SD.
Statistical analysiswas performed using the Minitab
computersoftware (State College, PA), using bothparametric and
nonparametric tests. All testswere two-tailed, with significance
taken asP 0.05. For between-group comparisons,we used paired t test
for parametric data andKruskal-Wallis test for nonparametric
data.
RESULTS
Forearm levelThe results of the iontophoresis are shownin Table
3. To evaluate the degree of vasodi-lation that is specific to the
neurovascularresponse, we measured the capillary bloodflow in a
skin area in direct contact withacetylcholine and in an adjacent
skin areanot in direct contact with it. The latter rep-resents the
nerve-axonrelated portion ofthe total response. The percentage
contri-bution of the nerve-axonrelated responseto the total
response was similar betweennonneuropathic diabetic patients and
thecontrol group after the iontophoresis ofacetylcholine (35 and
31%, respectively,NS). In both the nonneuropathic diabeticpatients
and control group, the percentagecontribution of the
nerve-axonrelatedresponse to the total response was signifi-cantly
less after the iontophoresis of eithersodium nitroprusside (13 and
10%, respec-tively, P 0.01) or deionized water (16and 17%,
respectively, P 0.01). No sig-nificant difference was seen between
thepercentage contribution of the nerve-axonrelated reflex to the
total response tosodium nitroprusside and to deionizedwater both in
anodal and cathodal mode in
Table 3The contribution of nerve-axon reflex-related
vasodilation to the total response to acetylcholine, sodium
nitroprusside, and deionized waterat the forearm level
Nonneuropathic diabetic patients Control subjects
Total response to Ach 835 (2891476) 1,181
(5472,299)Nerve-axonrelated response to Ach 365 (120513) 338
(207706)The % contribution of nerve-axon response to the total
response to Ach 35 (1683)* 31 (1760)*Total response to SNP 525
(307974) 880 (4452,178)Nerve-axonrelated response to SNP 77 (22230)
118 (40769)The contribution of nerve-axon response to the total
response to SNP 13 (634) 10 (322)Total response to W, anodal mode
83 (15400) 300 (65897)Nerve-axonrelated response to W 14 (160) 35
(8141)The % contribution of nerve-axon response to the total
response to W 16 (254) 17 (440)Total response to W, cathodal mode
111 (45315) 108 (20252)Nerve-axonrelated response to W 11 (160) 35
(022)The % contribution of nerve-axon response to the total
response to W 5 (135) 6 (027)
Data are medians (25th75th quartiles). Ach, acetylcholine; SNP,
sodium nitroprusside; W, deionized water. *Ach vs. SNP and W, P
0.01.
-
DIABETES CARE, VOLUME 24, NUMBER 2, FEBRUARY 2001 347
Hamdy and Associates
both the nonneuropathic diabetic patientsand control group (NS).
This is consistentwith the fact that acetylcholine
specificallystimulates C nociceptive fibers and
thenerve-axonrelated reflex, whereas sodiumnitroprusside and
deionized water do not.The contribution of the
neurovascularresponse to the total response to acetyl-choline is
approximately one-third of thetotal response and is not compromised
bydiabetes at the forearm level.
Foot levelThe results of the iontophoresis are shown inTable 4.
In response to iontophoresis ofacetylcholine, the percentage
contribution ofthe nerve-axonrelated response was similarto that
seen at the forearm level in both thediabetic patients without
complications andthe healthy control subjects (29 and
36%,respectively, NS). The diabetic neuropathicpatients had a
significantly lower medianincrease of capillary blood flow over
baselinein response to acetylcholine compared withthe diabetic
patients without complicationsand the control group (P 0.01) (Fig.
1).The neurovascular response was markedlydecreased in all three
neuropathic groupswhen compared with diabetic patients with-out
complications and the control group.The contribution of the
nerve-axonrelatedresponse to the total response was 8% indiabetic
patients with neuropathy (P 0.01), 5% in diabetic patients with
Charcot
arthropathy (P 0.01), and 20% in diabeticpatients with
neuropathy and peripheralvascular disease (P 0.01). The
nerve-axonrelated response to sodium nitro-prusside and to the
anodal and cathodaliontophoresis of deionized water was simi-
lar to the response observed in the upperextremity.
CONCLUSIONS In the presentstudy, we have shown that in healthy
sub-jects and in nonneuropathic diabetic
Table 4Contribution of nerve-axon reflex-related vasodilation to
the total response to acetylcholine, sodium nitroprusside, and
deionized waterat the foot level
Charcot Neuropathy and Diabetic patients ControlNeuropathy
arthropathy peripheral vascular without subjects
(DN) (DA) disease (DI) complications (D) (C)
Total response to Ach 90 (15378) 227 (86554) 74 (1212) 578
(1521,858) 411 (148541)Nerve-axonrelated response to Ach 4 (026) 13
(152) 5 (052) 118 (19304) 153 (60264)The % contribution of
nerve-axon response to the total 8 (031)* 5 (027) 20 (070) 29 (752)
36 (1888)response to Ach
Total response to SNP 89 (31227) 80 (74400) 86 (7239) 234
(141520) 234 (129590)Nerve-axonrelated response to SNP 10 (024) 2
(032) 1 (012) 27 (887) 48 (16108)The % contribution of nerve-axon
response to the total 8 (031) 10 (029) 2 (018) 12 (235) 9
(476)response to SNP
Total response to W, Anodal mode 8 (040) 12 (150) 19 (031) 238
(35427) 33 (11107)Nerve-axonrelated response to W 0 (013) 6 (012) 3
(010) 23 (728) 12 (025)The % contribution of nerve-axon response to
the total 11 (0100) 43 (6106) 26 (081) 13 (248) 18 (6111)response
to W
Total response to W, Cathodal mode 4 (014) 12 (038) 18 (042) 28
(10109) 25 (843)Nerve-axonrelated response to W 0 (09) 1 (012) 0
(015) 11 (142) 3 (011)The % contribution of nerve-axon response to
the total 35 (0100) 18 (6106) 4 (081) 41 (248) 0 (6111)response to
W
Data are medians (25th75th quartiles). Ach, acetylcholine; SNP,
sodium nitroprusside; W, deionized water. *DN vs. D and C, P 0.01;
DA vs. D and C, P 0.01;DI vs. D and C, P 0.01; Ach vs. SNP and W, P
0.01.
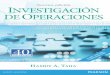
Figure 1Total and neurovascular (N) change in skin blood flow in
response to acetylcholine at thefoot level. The median, first
quartile, and third quartile and the range are shown. The total
response issignificantly lower in neuropathic diabetic patients
than it is in control subjects and diabetic patientswithout
neuropathy (P 0.01). The percentage contribution of neurovascular
response to the totalresponse is also significantly lower in
neuropathic diabetic patients than in control subjects and
diabeticpatients without neuropathy (P 0.01).
-
348 DIABETES CARE, VOLUME 24, NUMBER 2, FEBRUARY 2001
Nerve-axon reflex and skin vasodilation
patients, at both the forearm and foot lev-els, the
microvascular vasodilation that isrelated to the neurovascular
responseaccounts for approximately one-third ofthe total
vasodilation that is observed afterthe iontophoresis of
acetylcholine. Thisportion is markedly decreased in the pres-ence
of diabetic neuropathy.
The total microvascular vasodilation inresponse to acetylcholine
is currently con-sidered to represent the sum of direct
stim-ulation of the endothelium by acetylcholineand of the
vasodilation that is related to thenerve-axon reflex (20). However,
the mag-nitude of the contribution of each of thesetwo factors to
the total vasodilation has notbeen adequately studied, and the
currentlyavailable data are conflicting. Thus, althoughsome studies
have suggested a considerablyhigher contribution of the
neurovascularresponse, the techniques used did not allowthe precise
quantification of this contribu-tion (8,21). On the other hand,
anotherstudy has shown that local sensory inhibi-tion by topical
application of lignocaine andprilocaine did not have an effect on
the totalvasodilatory response to the iontophoresis ofacetylcholine
(22). The main problem ininterpreting these data, though, lies in
thefact that there is no evidence that topicalapplication of
lignocaine abolishes thenerve-axon reflex, since it may cause
localanesthesia via mechanisms that are notaffecting the antidromic
stimulation of localC nociceptive fibers. This is further
empha-sized by the findings of a previous studythat showed that
deep subcutaneous injec-tion of lignocaine does inhibit the
nerve-axonrelated vasodilation in response to theiontophoresis of
acetylcholine (23).
In the present study, we have used achamber that can accommodate
two single-point laser probes that can measure the totaland the
nerve-axon reflex-related vasodila-tion. This technique can
satisfactorily mea-sure the two responses separately, making
itpossible to evaluate the relative contributionof the
neurovascular response to the totalresponse with an adequate
reliability. Fur-thermore, we have studied subjects withand without
peripheral neuropathy ratherthan testing with local anesthesia,
which, asmentioned previously, has questionableeffects on the
nerve-axon reflex. Finally, itshould be remembered that under
condi-tions of stress (such as injury or inflamma-tion), hyperemia
is necessary not only in theinjured area alone but in a
considerablylarger area that surrounds the injured site.Because
this response depends mainly on a
normal nerve-axon reflex, our findings makethe point that this
response, under normalconditions, is one-third of the
maximalachievable vasodilation and that this isdrastically reduced
in the presence of dia-betic neuropathy.
Single-point laser probe measurementsare known to have a
considerably high CV,whereas the use of laser scanners reducesthis
variability (10,16). However, with laserscanners, one cannot
evaluate the nerve-axon response, a measurement that can bedone
only with use of the single-point lasertechnique. The large number
of subjects ineach studied group compensates for thehigh
variability and does not affect the valid-ity of the conclusions
regarding the contri-bution of nerve-axon response to
totalvasodilation. On the other hand, the highvariability does not
allow the direct com-parison of the vasodilatory response amongthe
various studied groups, which makesthis study prone to type 2
statistical error.Therefore, it is recommended that for reli-able
data regarding these questions, thereader is directed to studies
that have specif-ically addressed this question and used
theappropriate techniques, including the use ofa Laser Scanner
Imager (10,11,2426).
In contrast to acetylcholine, sodiumnitroprusside causes
vasodilation bydirectly stimulating the vascular smoothmuscle cell
and does not specifically stim-ulate the C nociceptive fibers. This
resultcan be seen in the present study by thesmall
nerve-axonrelated vasodilationachieved with sodium nitroprusside,
simi-lar to that achieved by deionized water,which can be
attributed to a nonspecificgalvanic effect of the constant current
thatis used for the iontophoresis (27). There-fore, we believe that
the presented dataalso provide further evidence of
differentpathways through which acetylcholine andsodium
nitroprusside cause vasodilation inthe skin microcirculation.
The iontophoresis of deionized water inthe same polarity with
that of acetylcholine(i.e., with an anodal constant current)
hasbeen previously shown to lead to a smallnonspecific galvanic
effect (20,21). In con-trast, iontophoresis with a cathodal
current,as used for the iontophoresis of sodiumnitroprusside, has
been reported in onestudy to result in a significant
nonspecificvasodilatory response (22). In the presentstudy, we have
not found such an exagger-ated response, and both anodal and
cathodalmodes elicited very similar responses. Themain differences
between previous studies
and the present study that may explain thisdiscrepancy are the
duration and amplitudeof the current used for iontophoresis.
Thus,in our unit, we apply 200 A for 60 s. Thisproduces maximal
specific vasodilation witha minimal nonspecific vasodilation. This
isin sharp contrast with a previous study inwhich three rather
small pulses of ion-tophoresis were performed over a period of10
min, raising the question as to whethermaximal vasodilation was
achieved.
In a previous study, we showed thatdiabetes impairs the total
endothelium-dependent and endothelium-independentvasodilation at
the forearm level, a skinarea that is rarely affected by diabetic
neu-ropathy (11). In addition, the presentstudy shows that this
reduction is inde-pendent of the nerve-axonrelatedresponse. A
direct effect of diabetes onendothelium function or smooth
musclecells should therefore be considered as themain cause of the
observed impairedvasodilation in response to acetylcholineand
sodium nitroprusside. We have previ-ously shown that differences
exist betweenthe forearm and foot microcirculationbeds, with the
foot vasodilatory responsebeing approximately half that of
theresponse at the forearm level (11). Similarresults were observed
in the present study.
Neuropathy has been shown to reducethe vasodilatory response at
the foot level,irrespectively of the presence or absence
ofperipheral vascular disease (10,11). In thepresent study, the
nerve-axonrelatedresponse in diabetic patients during
specificstimulation of the C fibers with acetylcholinewas markedly
decreased, being similar tothat observed with sodium
nitroprusside.Thus, this is another indication that neu-ropathy
renders the diabetic foot function-ally ischemic, as blood flow
fails to increaseunder conditions of stress.
In summary, we have shown in thepresent study that the
neurovascular vasodi-lation response accounts for
approximatelyone-third of the total
acetylcholine-inducedvasodilation response at both the forearmand
foot levels of healthy subjects and non-neuropathic diabetic
patients. The presenceof diabetic neuropathy at the lower
extrem-ity results in a significant reduction in thetotal
vasodilatory response to acetylcholineand to an even more
pronounced reductionin the percentage contribution of the
neu-rovascular response to the total skinvasodilatory response to
acetylcholine.Acetylcholine and sodium nitroprussidecause
vasodilation in the skin microcircula-
-
DIABETES CARE, VOLUME 24, NUMBER 2, FEBRUARY 2001 349
Hamdy and Associates
tion through different pathways. Finally, thetechnique used in
this study may be partic-ularly helpful in developing new
methodsthat can objectively evaluate the efficacy ofnew treatments
on small-fiber function.
References1. Malik RA, Tesfaye S, Thompson SD, Veves
A, Sharma AK, Boulton AJM, Ward JD:Endothelial localization of
microvasculardamage in human diabetic neuropathy.Diabetologia
36:454459, 1993
2. Tesfaye S, Harris N, Jakubowski JJ, ModyC, Wilson RM, Rennie
IG, Ward JD:Impaired blood flow and arterio-venousshunting in human
diabetic neuropathy: anovel technique of nerve photography
andfluorescein angiography. Diabetologia 36:12261274, 1993
3. Stevens MJ, Dananberg J, Feldman EL,Lattmir SA, Kamijo M,
Thomas TP, ShindoH, Sima AA, Greene DA: The linked roles ofnitric
oxide, aldose reductase and (Na,K)-ATPase in the slowing of nerve
con-duction in the streptozotocin diabetic rat. JClin Invest
64:853919, 1994
4. Stevens MJ, Feldman EL, Greene DA: Theetiology of diabetic
neuropathy: the com-bined roles of metabolic and vasculardefects.
Diabet Med 12:566579, 1995
5. Tesfaye S, Malik R, Ward JD: Vascular fac-tors in diabetic
neuropathy. Diabetologia 37:847854, 1994
6. Vane JR, Anggard EE, Botting RM: Mecha-nisms of disease:
regulatory functions ofendothelium. N Engl J Med 323:2736, 1990
7. Palmer RMJ, Ashton DS, Moncada S: Vas-cular endothelial cells
synthesize nitricoxide from L-arginine. Nature 333:664666, 1988
8. Parkhouse N, LeQuesne PM: Impairedneurogenic vascular
response in patientswith diabetes and neuropathic foot lesions.N
Engl J Med 318:13061309, 1988
9. Walmsley D, Wiles PG: Early loss of neu-rogenic inflammation
in the human dia-betic foot. Clin Sci 80:605610, 1991
10. Veves A, Akbari CA, Primavera J, Don-aghue VM, Zacharoulis
D, Chrzan JS,
DeGirolami U, LoGerfo FW, Freeman R:Endothelial dysfunction and
the expres-sion of endothelial nitric oxide synthetasein diabetic
neuropathy, vascular disease,and foot ulceration. Diabetes
47:457463,1998
11. Arora S, Smakowski P, Frykberg RG, Sime-one LS, Freeman R,
LoGerfo FW, Veves A:Differences in foot and forearm skin
micro-circulation in diabetic patients with andwithout neuropathy.
Diabetes Care 21:13391344, 1998
12. Johnstone MT, Creager SJ, Scales KM,Casco JA, Lee BK,
Creager MA: Impairedendothelium-dependent vasodilation inpatients
with insulin-dependent diabetesmellitus. Circulation 88:25102516,
1993
13. Williams SB, Cusco JA, Roddy M, John-stone MT, Creager MA:
Impaired nitricoxide-mediated vasodilatation in patientswith
non-insulin-dependent diabetes mel-litus. J Am Coll Cardiol
27:567574, 1996
14. Celermajer DS, Sorensen KE, Gooch VM,Spiegelhalter DJ,
Miller OI, Sullivan ID,Lloyd JK, Deanfield JE: Non-invasive
detec-tion of endothelial dysfunction in childrenand adults at risk
of atherosclerosis. Lancet340:11111115, 1992
15. Tooke JE: Methodologies used in the studyof the
microcirculation in diabetes mellitus.Diabetes Metab Rev 9:5770,
1993
16. American Diabetes Association: Report andrecommendations of
the San Antonio Con-ference on Diabetic Neuropathy (Consen-sus
Statement). Diabetes 37:10001004,1988
17. Veves A, Uccioli L, Manes C, Van Acker K,Komninou H,
Philippides P, Kat-SilambrosN, De Leeuw I, Menzinger G, Boulton
AJM:Comparisons of risk factors for foot prob-lems in diabetic
patients attending teachinghospitals out-patient clinics in four
differ-ent European states. Diabet Med 11:709713, 1994
18. Wiles PG, Pearce SM, Rice PJS, MitchellJMO: Vibration
perception threshold: influ-ence of age, height, sex, and smoking
andcalculation of accurate centile values. Dia-bet Med 8:157161,
1991
19. Kumar S, Fernando DJS, Veves A, Knowles
EA, Young MJ, Boulton AJM: Semmes-Weinstein monofilaments: a
simple, effec-tive and inexpensive screening device foridentifying
diabetic patients at risk of footulceration. Diabetes Res Clin
Pract 13:6367, 1991
20. Pham H, Economides PA, Veves A: Therole of endothelial
function on the footmicrocirculation and wound healing in dia-betic
patients. Clin Podiatr Med Surg 15:8594, 1998
21. Forst T, Pfutzner A, Kunt T, Pohlmann T,Schenk U, Bauersachs
R, Kustner E, BeyerJ: Skin microcirculation in patients withtype I
diabetes with and without neuropa-thy after neurovascular
stimulation. ClinSci 94:255261, 1998
22. Morris SJ, Shore AC: Skin blood flowresponses to the
iontophoresis of acetyl-choline and sodium nitroprusside in
man:possible mechanisms. J Physiol 496:531542, 1996
23. Parkhouse N, Le Quesne PM: Quantitativeobjective assessment
of peripheral noci-ceptive C fibre function. J Neurol
NeurosurgPsychiatry 51:2834, 1988
24. Morris SJ, Shore AC, Tooke JE: Responsesof the skin
microcirculation to acetyl-choline and sodium nitroprusside
inpatients with NIDDM. Diabetologia 38:13371344, 1995
25. Caballero AE, Arora S, Saouaf R, Lim SC,Smakowski P, Park
JY, King GL, LoGerfoFW, Horton ES, Veves A: Microvascularand
macrovascular reactivity is reduced insubjects at risk for type 2
diabetes. Diabetes48:18561862, 1999
26. Lim SC, Caballero AE, Arora S, SmakowskiP, Bashoft E, Brown
F, LoGerfo FW, HortonES, Veves A: The effect of gender and
hor-monal replacement therapy on the vascularreactivity of healthy
individuals and indi-viduals with type 2 diabetes. J ClinEndocrinol
Metab 84:41594164, 1999
27. Noon JP, Walker BR, Hand MF, Webb DJ:Studies with
iontophoretic administrationof drugs to human dermal vessels in
vivo:cholinergic vasodilatation is mediated bydilator prostanoids
rather than nitric oxide.Br J Clin Pharmacol 45:545550, 1998