Embed Size (px)
Citation preview
1/9/2014
1
Diabetic Retinopathy: An Update for Diabetes
Educators
A. Paul Chous, M.A., O.D., F.A.A.O.
Private Practice -Tacoma, WA
Specializing in Diabetes Eye Care & Education
A. Paul Chous, MA, OD, FAAO
Author of Diabetic Eye Disease: Lessons
From a Diabetic Eye Doctor (Fairwood
Press, 2003)
Web columnist for www.dLife.com and
www.diabetesincontrol.com
Optometric representative to the National
Diabetes Education Program of the NIH
Winner of American Diabetes Association’s
Distinguished Public Service Award in 1998
T1DM x 45 years
Disclosures
I am or have been a consultant for, been on
advisory boards of, or spoken on behalf of:
Bausch & Lomb, Freedom
Meditech, GlaxoSmithKline,
Kestrel, Kowa, LifeMed Media,
Prodigy Diabetes Care, Risk
Medical Solutions, Vision
Service Plan, ZeaVision
None of these affiliations
have affected the content of
this presentation
Diabetes-Related Eye
Diseases
“Diabetic Eye Disease” refers to ocular
pathologies more commonly seen in
patients with diabetes
All of these conditions are attributable, at
least in part, to chronic hyperglycemia
Ocular Diseases Associated With Ocular Diseases Associated With
DiabetesDiabetes
CataractCataract
KeratopathyKeratopathy
Efferent Cranial NeuropathyEfferent Cranial Neuropathy
GlaucomaGlaucoma
Ischemic Optic NeuropathyIschemic Optic Neuropathy
Retinal Vascular OcclusionRetinal Vascular Occlusion
Diabetic RetinopathyDiabetic Retinopathy
Cataract
Corneal Disease
CN VI Palsy
1/9/2014
2
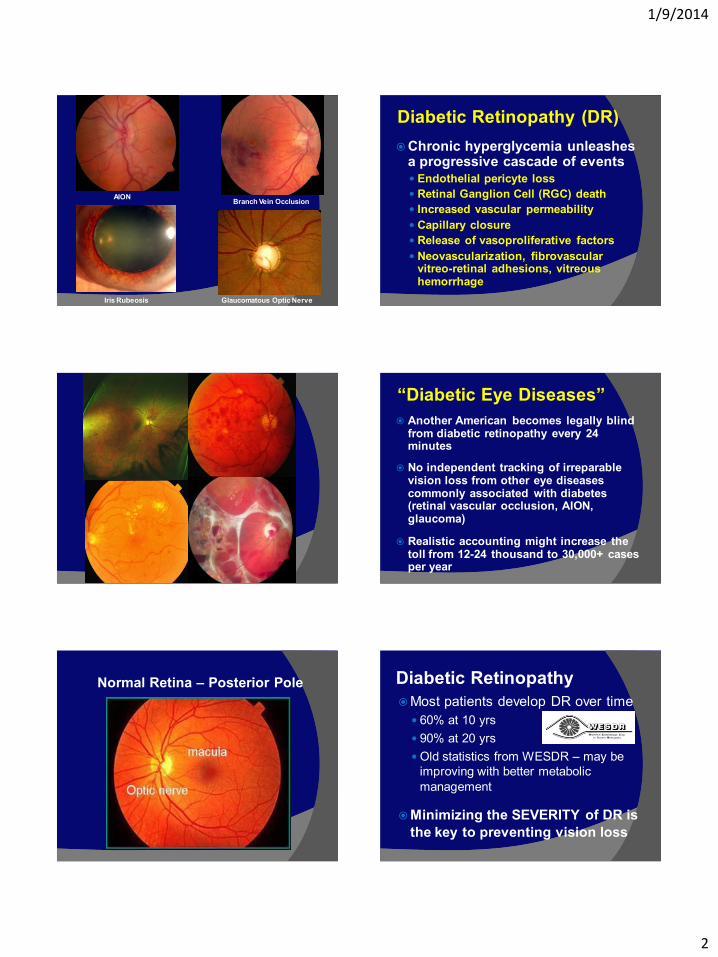
AION Branch Vein Occlusion
Iris Rubeosis Glaucomatous Optic Nerve
Diabetic Retinopathy (DR)
Chronic hyperglycemia unleashes a progressive cascade of events
Endothelial pericyte loss
Retinal Ganglion Cell (RGC) death
Increased vascular permeability
Capillary closure
Release of vasoproliferative factors
Neovascularization, fibrovascular vitreo-retinal adhesions, vitreous hemorrhage
“Diabetic Eye Diseases”
Another American becomes legally blind from diabetic retinopathy every 24 minutes
No independent tracking of irreparable vision loss from other eye diseases commonly associated with diabetes (retinal vascular occlusion, AION, glaucoma)
Realistic accounting might increase the toll from 12-24 thousand to 30,000+ cases per year
Normal Retina – Posterior Pole Diabetic Retinopathy
Most patients develop DR over time
60% at 10 yrs
90% at 20 yrs
Old statistics from WESDR – may be
improving with better metabolic
management
Minimizing the SEVERITY of DR is
the key to preventing vision loss
1/9/2014
3
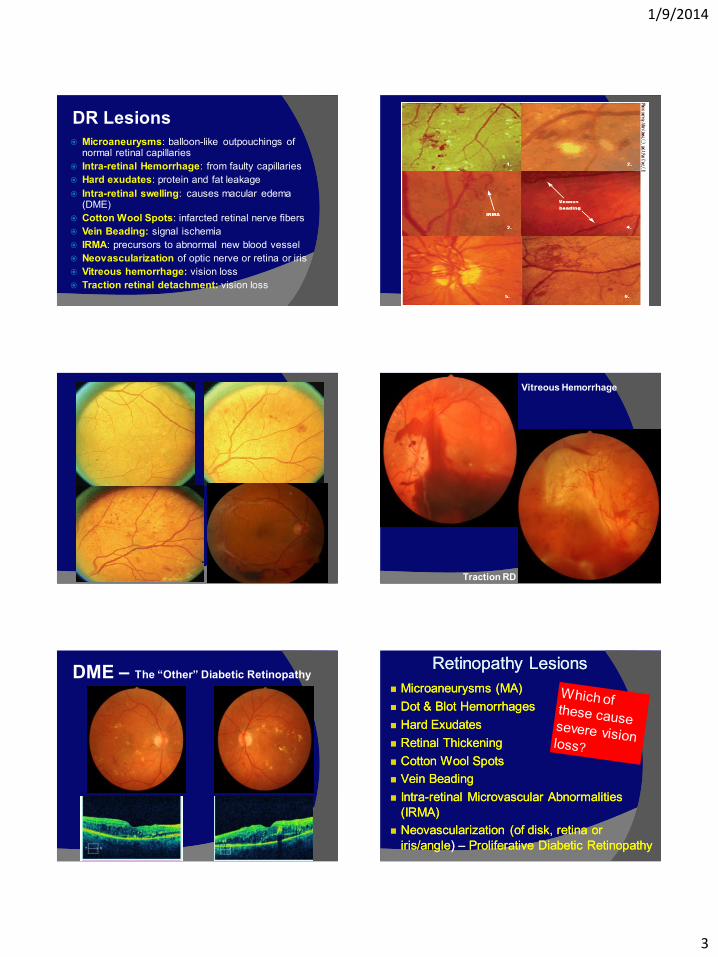
DR Lesions
Microaneurysms: balloon-like outpouchings of normal retinal capillaries
Intra-retinal Hemorrhage: from faulty capillaries
Hard exudates: protein and fat leakage
Intra-retinal swelling: causes macular edema (DME)
Cotton Wool Spots: infarcted retinal nerve fibers
Vein Beading: signal ischemia
IRMA: precursors to abnormal new blood vessel
Neovascularization of optic nerve or retina or iris
Vitreous hemorrhage: vision loss
Traction retinal detachment: vision loss
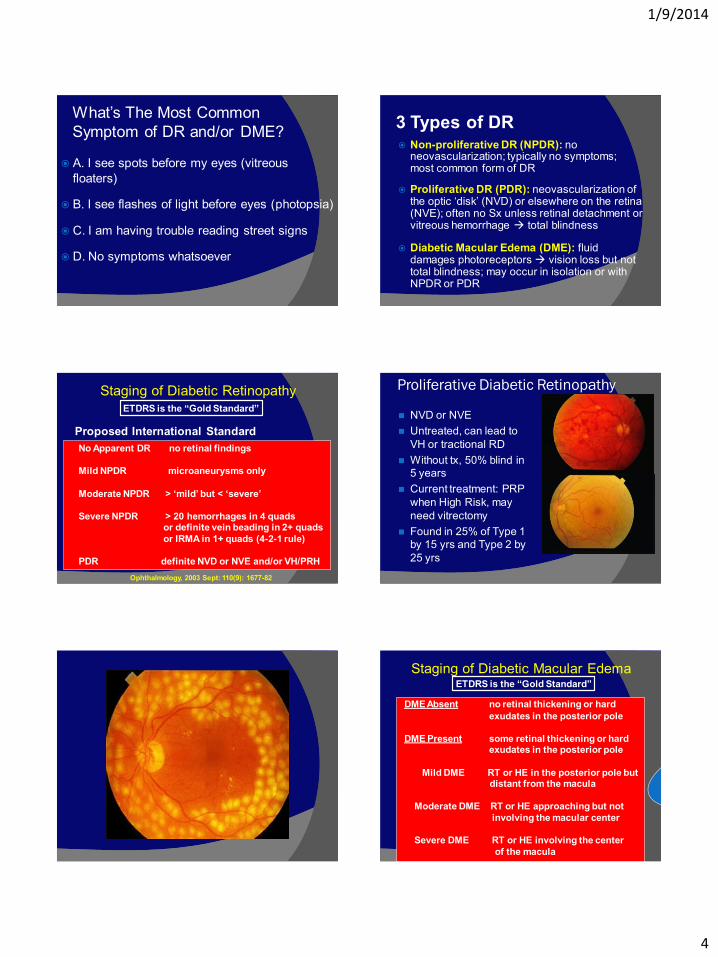
Vitreous Hemorrhage
Traction RD
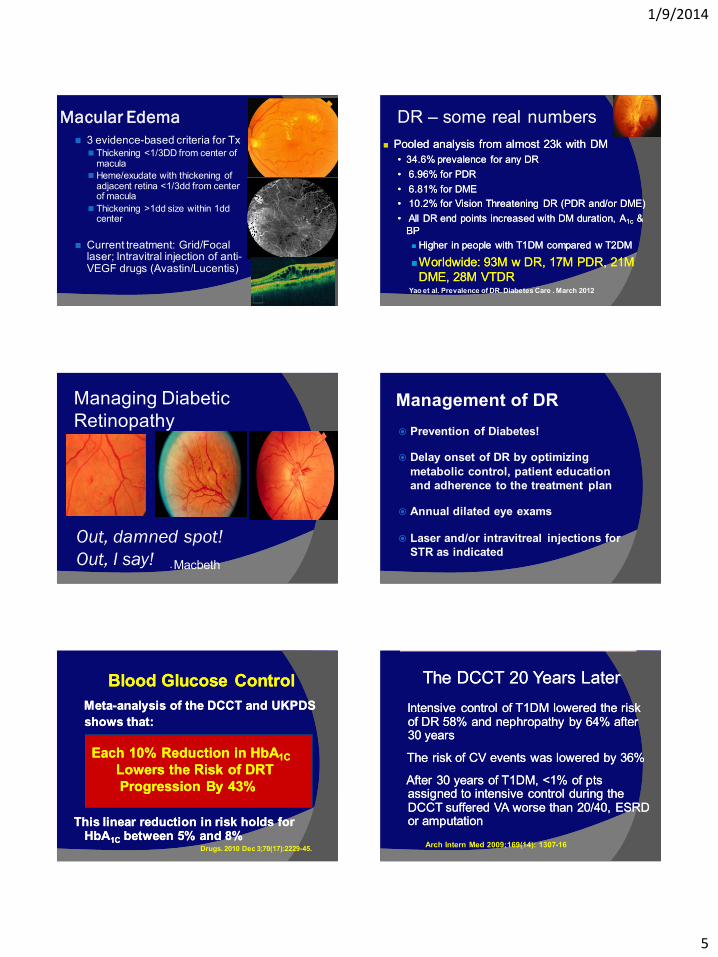
DME – The “Other” Diabetic Retinopathy Retinopathy LesionsRetinopathy Lesions
MicroaneurysmsMicroaneurysms (MA)(MA)
Dot & Blot HemorrhagesDot & Blot Hemorrhages
Hard ExudatesHard Exudates
Retinal ThickeningRetinal Thickening
Cotton Wool SpotsCotton Wool Spots
Vein BeadingVein Beading
IntraIntra--retinal retinal MicrovascularMicrovascular Abnormalities Abnormalities
(IRMA)(IRMA)
Neovascularization (of disk, retina or Neovascularization (of disk, retina or
iris/angleiris/angle) ) –– Proliferative Diabetic RetinopathyProliferative Diabetic Retinopathy
1/9/2014
4
What’s The Most Common
Symptom of DR and/or DME?
A. I see spots before my eyes (vitreous
floaters)
B. I see flashes of light before eyes (photopsia)
C. I am having trouble reading street signs
D. No symptoms whatsoever
3 Types of DR Non-proliferative DR (NPDR): no
neovascularization; typically no symptoms; most common form of DR
Proliferative DR (PDR): neovascularization of the optic ‘disk’ (NVD) or elsewhere on the retina (NVE); often no Sx unless retinal detachment or vitreous hemorrhage total blindness
Diabetic Macular Edema (DME): fluid damages photoreceptors vision loss but not total blindness; may occur in isolation or with NPDR or PDR
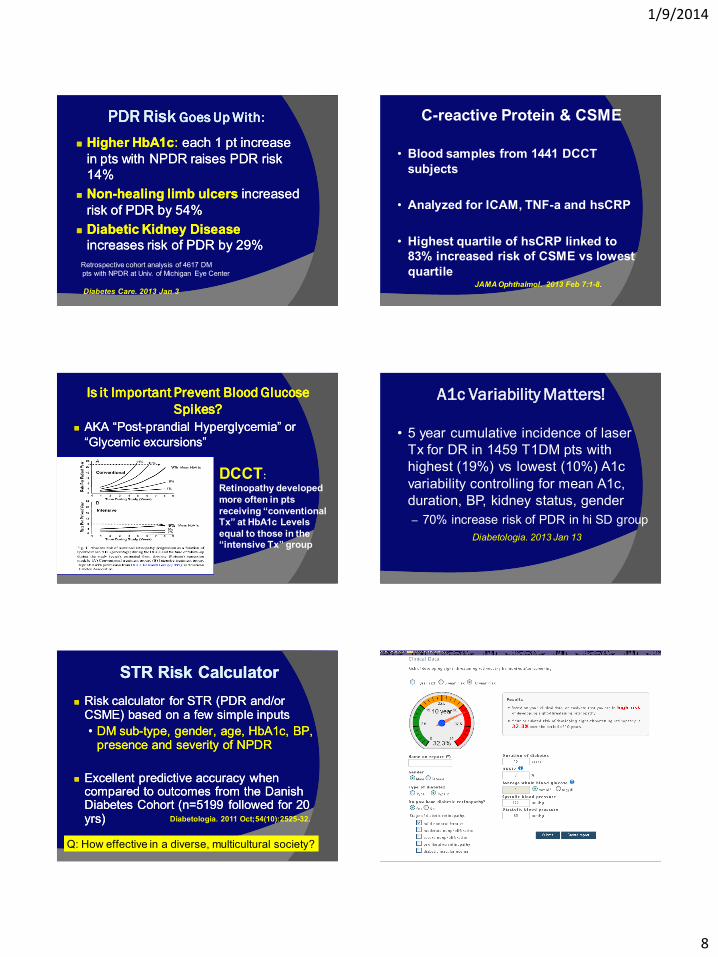
Staging of Diabetic Retinopathy
Proposed International Standard
No Apparent DR no retinal findings
Mild NPDR microaneurysms only
Moderate NPDR > ‘mild’ but < ‘severe’
Severe NPDR > 20 hemorrhages in 4 quads or definite vein beading in 2+ quads
or IRMA in 1+ quads (4-2-1 rule)
PDR definite NVD or NVE and/or VH/PRH
Ophthalmology, 2003 Sept: 110(9): 1677-82
ETDRS is the “Gold Standard”
Proliferative Diabetic Retinopathy
NVD or NVE
Untreated, can lead to
VH or tractional RD
Without tx, 50% blind in
5 years
Current treatment: PRP
when High Risk, may
need vitrectomy
Found in 25% of Type 1
by 15 yrs and Type 2 by
25 yrs
Staging of Diabetic Macular Edema
DME Absent no retinal thickening or hard
exudates in the posterior pole
DME Present some retinal thickening or hard exudates in the posterior pole
Mild DME RT or HE in the posterior pole but distant from the macula
Moderate DME RT or HE approaching but not
involving the macular center
Severe DME RT or HE involving the center
of the macula
ETDRS is the “Gold Standard”
1/9/2014
5
Macular Edema
3 evidence-based criteria for Tx Thickening <1/3DD from center of
macula
Heme/exudate with thickening of adjacent retina <1/3dd from center of macula
Thickening >1dd size within 1dd center
Current treatment: Grid/Focal laser; Intravitral injection of anti- VEGF drugs (Avastin/Lucentis)
DR – some real numbers
Pooled analysis from almost 23k Pooled analysis from almost 23k with with DMDM
•• 34.6% prevalence for any DR34.6% prevalence for any DR
•• 6.96% for PDR6.96% for PDR
•• 6.81% for DME6.81% for DME
•• 10.2% for 10.2% for Vision Threatening DR (PDR and/or DME)Vision Threatening DR (PDR and/or DME)
•• All DR end points increased with DM duration, AAll DR end points increased with DM duration, A1c1c & &
BPBP
Higher in people with T1DM compared w T2DM Higher in people with T1DM compared w T2DM
Worldwide: 93M w DR, 17M PDR, 21M Worldwide: 93M w DR, 17M PDR, 21M
DME, 28M VTDRDME, 28M VTDR Yao et al. Prevalence of DR. Diabetes Care . March 2012
Managing Diabetic
Retinopathy
Out, damned spot!
Out, I say! - Macbeth
Management of DR
Prevention of Diabetes!
Delay onset of DR by optimizing
metabolic control, patient education
and adherence to the treatment plan
Annual dilated eye exams
Laser and/or intravitreal injections for
STR as indicated
Blood Glucose ControlBlood Glucose Control
MetaMeta--analysis of the DCCT and UKPDS analysis of the DCCT and UKPDS
shows that:shows that:
This linear reduction in risk holds for This linear reduction in risk holds for
HbAHbA1C1C between 5% and 8%between 5% and 8%
Each 10% Reduction in HbAEach 10% Reduction in HbA1C1C
Lowers the Risk of DRT Lowers the Risk of DRT
Progression By 43%Progression By 43%
Drugs. 2010 Dec 3;70(17):2229-45.
The DCCT 20 Years LaterThe DCCT 20 Years Later
Intensive control of T1DM lowered the risk Intensive control of T1DM lowered the risk of DR 58% and nephropathy by 64% after of DR 58% and nephropathy by 64% after 30 years30 years
The risk of CV events was lowered by 36%The risk of CV events was lowered by 36%
After 30 years of T1DM, <1% of pts After 30 years of T1DM, <1% of pts assigned to intensive control during the assigned to intensive control during the DCCT suffered VA worse than 20/40, ESRD DCCT suffered VA worse than 20/40, ESRD or amputationor amputation
Arch Intern Med 2009;169(14): 1307-16

1/9/2014
6
Highlights from The ‘Big’ DR Studies
PRP reduces risk of severe vision loss (< 20/800) from PDR by 50-65% (DRS/ETDRS)
Focal laser reduces risk of doubling the visual angle by 50% in CSME (ETDRS)
Aspirin has no effect on PDR/VH (ETDRS)
Vitrectomy is indicated for non-clearing vitreous hemorrhage and tractional RD of the macula (DRVS)
Invest Ophthalmol Vis Sci 1981 : 210-226
Arch Ophthalmol 1985 Dec;103(12):1796-806
Arch Ophthalmol 1990;108: 958-964
RESTORE & READRESTORE & READ
LucentisLucentis versus Laser for Vision loss from versus Laser for Vision loss from
CSME (20/40 to 20/200 BCVA)CSME (20/40 to 20/200 BCVA)
Percent Percent achieving achieving >> 20/40 ETDRS acuity 20/40 ETDRS acuity
at 12 months:at 12 months:
LucentisLucentis –– 53%53%
LucentisLucentis + Laser + Laser –– 44.9%44.9%
Laser alone Laser alone –– 26.3%26.3%
Benefit of Benefit of LucentisLucentis maintained at 3 yearsmaintained at 3 years
No increased MI or CVA with No increased MI or CVA with LucentisLucentis Ophthalmology. 2011 Apr;118(4):615-25.
JAMA Ophthalmol. 2013 Feb;131(2):139-45
What’s Best for DMEWhat’s Best for DME??
antianti--VEGF treatments are VEGF treatments are
superior to macular laser for superior to macular laser for
VA and VA and retinal thickening retinal thickening
BUT…need repeat injections &
costs more money
Bevacizumab (AvastinTM) + Laser
most cost-effective comparing laser, steroid,
Lucentis, Avastin or any combination
Ophthalmology. 2013 May 1. epub
A Few Important
Considerations Regarding
Systemic Management of
Diabetes and DR
ACEIs/ARBs & Retinopathy
Vasotec® (enalapril) and Cozaar® (losartan)
reduced the risk of DR progression by 65%
and 70% in T1DM NEJM 2009;361: 40-51
Captopril reduces DR progression 40% and DME 30%
in T2DM
Should these agents become standard
treatment of DR?
-prils and –sartans may
lower DR Risk of Progression
Chin Med J (Engl) 2012 Jan;125(2):287-92

1/9/2014
7
Lipid Agents & Retinopathy
Simvistatin + Fenofibrate therapy lowers the risk of DR progression by 35% (and need for laser by 31%) compared to simvistatin alone in pts with T2DM and high cardiovascular risk (n = 2856)
Consistent with FIELD Study showing reduced progression of DR and need for laser Tx Lancet 2007 370(9600):687-97
ACCORD Eye Study, N Engl J Med. 2010 Jul 15;363(3):233-44
Add-on Fenofibrate lowers risk of DR progression in T2DM
TZDs & DME Retrospective cohort study of 103K+
T2DM patients suggests use of
rosiglitazone or pioglitazone more
than doubled the risk of DME (3x risk
with concomitant insulin use –
attenuated by ASA and especially
ACEI use)
Probably wise to avoid or D/C
glitazones in patients with DME
Arch Intern Med. 2012 Jul 9;172(13):1005-11
More to Retinopathy than Retinopathy
Retinopathy predicts CV mortality and
coronary heart disease (CHD)1
PDR>NPDR>no retinopathy in likely CVD and CHD
mortality, and women>men, especially in NPR
In women, PDR yields nearly 5x risk of CHD death!
Independent of smoking, HTN, Cholesterol, HDL,
duration or control of DM or proteinuria
Retinopathy predicts stroke rate2
Those with DR have 2.34x risk for ischemic stroke
Independent of smoking, cholesterol, insulin use,
HTN
1. Diabetes Care. Feb. 2007;30:292-99. 2. Cheung et al. Stroke. Feb 2007
Can We Predict Who is Going to
Develop Sight-threatening
Diabetic Retinopathy?
Risk Factors For Diabetic
Retinopathy Established
Disease duration
HbA1c
Disease sub-type
Gender
HTN
Microalbuminuria
Emerging
Obesity
Sleep apnea
Vitamin D insufficiency
Vit B12 deficiency
Carotenoid imbalance
Invest Ophthalmol Vis Sci. 2011 Jun 22;52(7):4416-21
Diabet Med. 2010 Apr;27(4):423-30
Endocr Pract. 2012 Mar-Apr;18(2):185-93
PLoS One. 2011;6(11):e26747
Obstructive Sleep Apnea Syndrome
OSAS is independently associated with risk of
DR and its progression
Br J Ophthalmol. 2012 Dec;96(12):1535 Retina. 2012 Oct;32(9):1791-8.
Jpn J Ophthalmol. 2011 Nov;55(6):638-42
Am J Ophthalmol. 2011 Apr;151(4):604-9
Mil Med. 2010 Nov;175(11):913-6 Diabet Med. 2010 Apr;27(4):423-30
Am J Ophthalmol. 2009 Jun;147(6):1017-21
1/9/2014
8
PDR Risk PDR Risk Goes Up WithGoes Up With::
Higher HbA1cHigher HbA1c: : each 1 pt increase each 1 pt increase
in pts with NPDR raises PDR risk in pts with NPDR raises PDR risk
14%14%
NonNon--healing limb ulcers healing limb ulcers increased increased
risk of PDR by 54%risk of PDR by 54%
Diabetic Kidney Disease Diabetic Kidney Disease
increases risk of PDR by 29%increases risk of PDR by 29%
Retrospective cohort analysis of 4617 DM
pts with NPDR at Univ. of Michigan Eye Center
Diabetes Care. 2013 Jan 3
C-reactive Protein & CSME
• Blood samples from 1441 DCCT
subjects
• Analyzed for ICAM, TNF-a and hsCRP
• Highest quartile of hsCRP linked to
83% increased risk of CSME vs lowest
quartile JAMA Ophthalmol. 2013 Feb 7:1-8.
Is it Important Prevent Is it Important Prevent Blood Glucose Blood Glucose
Spikes?Spikes?
AKA “PostAKA “Post--prandialprandial Hyperglycemia” or Hyperglycemia” or
““GlycemicGlycemic excursions”excursions”
DCCT:
Retinopathy developed
more often in pts
receiving “conventional Tx” at HbA1c Levels
equal to those in the “intensive Tx” group
A1c Variability Matters!
• 5 year cumulative incidence of laser
Tx for DR in 1459 T1DM pts with
highest (19%) vs lowest (10%) A1c
variability controlling for mean A1c,
duration, BP, kidney status, gender
– 70% increase risk of PDR in hi SD group
Diabetologia. 2013 Jan 13
STR STR Risk CalculatorRisk Calculator
Risk calculator for STR (PDR and/or Risk calculator for STR (PDR and/or CSME) based on a few simple inputsCSME) based on a few simple inputs
•• DM subDM sub--type, gender, age, HbA1c, BP, type, gender, age, HbA1c, BP, presence and severity of NPDRpresence and severity of NPDR
Excellent predictive accuracy when Excellent predictive accuracy when compared to outcomes from the Danish compared to outcomes from the Danish Diabetes Cohort (n=5199 followed for 20 Diabetes Cohort (n=5199 followed for 20 yrs)yrs) Diabetologia. 2011 Oct;54(10):2525-32.
Q: How effective in a diverse, multicultural society?

1/9/2014
9
If our patient can reduce HbA1c to the AACE Target of 6.5%
the 10 year risk of developing sight-threatening
retinopathy drops to 19.8%, or by 39%
www.Retinarisk.com
Gold MedalistsGold Medalists
Time/Metabolic Control Time/Metabolic Control may not be may not be
the only the only enemyenemy……
“Medalists”: h/o T1DM x 50yrs “Medalists”: h/o T1DM x 50yrs
42.642.6% did not have PDR, and those % did not have PDR, and those
without had little progression of DR without had little progression of DR
after after first first 17yrs17yrs
With little to no correspondence to A1cWith little to no correspondence to A1c Diabetes Care. 2011 Apr;34(4):968-74
Key Message
Most blindness and severe visual
impairment caused by diabetic
retinopathy is preventable with
good diabetes self-management,
regular dilated eye examinations
and timely treatment
Diabetes & DR Affect Visual
Function
Snellen visual acuity is a 150+ yr old
test that does not always reflect real
world visual function
DM/DR also impair: color perception,
contrast sensitivity, visual field sensitivity
Graefes Arch Clin Exp Ophthalmol. 2012 Dec;250(12):
Diabet Med. 2011 Jul;28(7):865-71
Acta Opthalmol 2005; 82(5):574-80
Graefes Arch Clin Exp Ophthalmol. 2001 Sep;239(9):643-8 BJO 1996;80: 209-13
IOVS 1997; 38(9): 1819-24
Diabetes Care 1992; 15(5):620-25
Graefes Arch Clin Exp Ophthalmol. 1996 May;234(5):300-5
1/9/2014
10
Vision in The Real World
It may be time to develop, test and educate ECPs, PCPs & the public
about an AREDS-2 type multi-component supplement for patients
with diabetes and diabetic retinopathy
Beyond AREDS: is there a place for antioxidant therapy in
the prevention/treatment of eye disease?
Kowluru RA, Zhong Q.
Invest Ophthalmol Vis Sci. 2011 Nov 7;52(12):8665-71
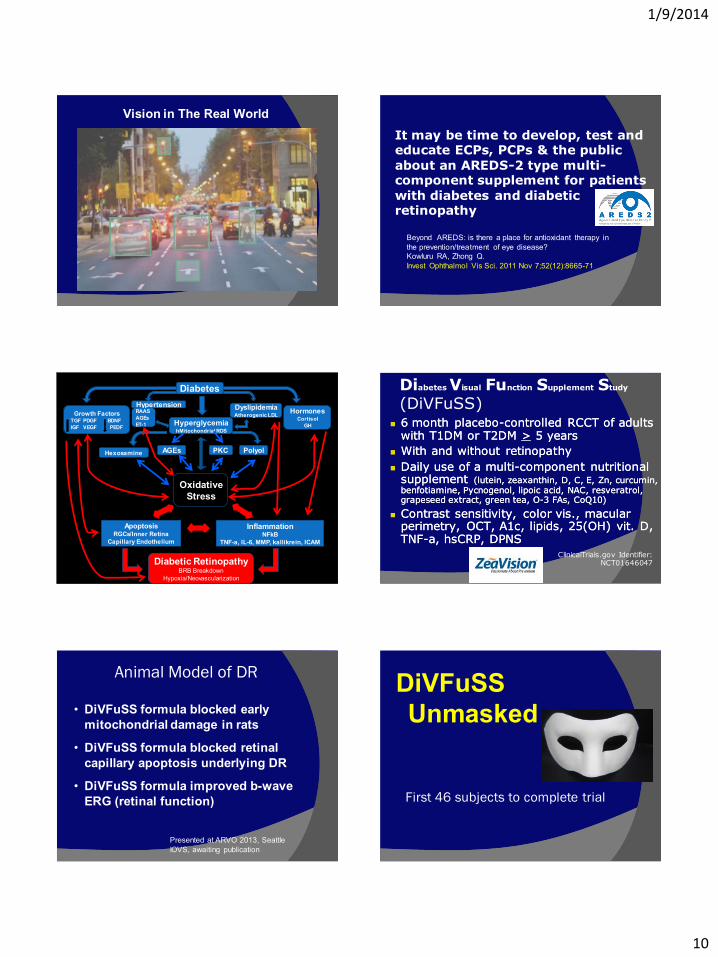
Diabetes
Growth Factors TGF PDGF BDNF
IGF VEGF PEDF
Hypertension
Hyperglycemia hMitochondrial ROS
Dyslipidemia Atherogenic LDL
Hormones Cortisol
GH
RAAS
AGEs
ET-1
AGEs Hexosamine PKC Polyol
Oxidative
Stress
Apoptosis RGCs/Inner Retina
Capillary Endothelium
Inflammation NFkB
TNF-a, IL-6, MMP, kallikrein, ICAM
Diabetic Retinopathy BRB Breakdown
Hypoxia/Neovascularization
6 month placebo6 month placebo--controlled RCCT of adults controlled RCCT of adults with T1DM or T2DM with T1DM or T2DM >> 5 years5 years
With and without retinopathyWith and without retinopathy
Daily use of a multiDaily use of a multi--component nutritional component nutritional supplement supplement ((luteinlutein, , zeaxanthinzeaxanthin, D, C, , D, C, E, Zn, E, Zn, curcumincurcumin, , benfotiaminebenfotiamine, Pycnogenol, , Pycnogenol, lipoiclipoic acid, NAC, acid, NAC, resveratrolresveratrol, , grapeseedgrapeseed extract, green tea, extract, green tea, OO--3 FAs, CoQ10)3 FAs, CoQ10)
Contrast sensitivity, Contrast sensitivity, color vis., macular color vis., macular perimetryperimetry, OCT, A1c, lipids, 25(OH) , OCT, A1c, lipids, 25(OH) vitvit. D, . D, TNFTNF--a, a, hsCRPhsCRP, DPNS, DPNS
Diabetes Visual Function Supplement Study
(DiVFuSS)
ClinicalTrials.gov Identifier: NCT01646047
Animal Model of DR
• DiVFuSS formula blocked early
mitochondrial damage in rats
• DiVFuSS formula blocked retinal
capillary apoptosis underlying DR
• DiVFuSS formula improved b-wave
ERG (retinal function)
Presented at ARVO 2013, Seattle
IOVS, awaiting publication
First 46 subjects to complete trial
DiVFuSS
Unmasked
1/9/2014
11
Subject Characteristics (n = 46)
31-79 yo (mean = 56 yrs)
25 with NPDR & 21 with no DR
18 T1DM & 28 T2DM
HbA1c range 5.8 to 9.3% (mean 7.4%)
Mean A1c in those with DR = 7.8%
Mean A1c in those with no DR = 7.1%
Diabetes duration 5-52 years (mean 21.2 yrs)
Mean 23.4 years in those with DR
Mean 14.7 years in those with no DR
DiVFuSS Unmasked Data Δ from baseline Supplement versus Placebo
Contrast: +31% -20%
Color Error Score: -50% -2%
5-2 MD: +1.1 dB +0.17 dB
hsCRP: -72% +10%
HbA1c: -4% +2.5%
OCT mean NFL: unchanged in both groups
For contrast, color, visual field, hsCRP, p < 0.02
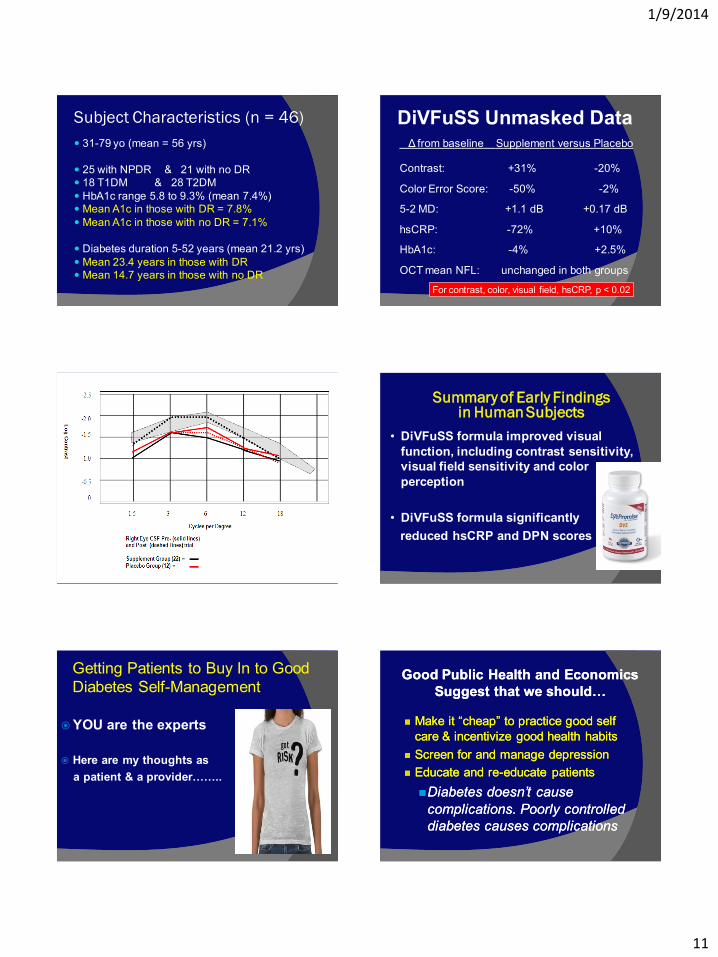
Mean Contrast For S and P Groups Pre- and Post Trial
Summary of Early Findings in Human Subjects
• DiVFuSS formula improved visual
function, including contrast sensitivity,
visual field sensitivity and color
perception
• DiVFuSS formula significantly
reduced hsCRP and DPN scores
Getting Patients to Buy In to Good
Diabetes Self-Management
YOU are the experts
Here are my thoughts as
a patient & a provider……..
Good Public Health and Economics Good Public Health and Economics
Suggest that we should…Suggest that we should…
Make it “cheap” to practice good self Make it “cheap” to practice good self
care & incentivize good health habitscare & incentivize good health habits
Screen for and manage depressionScreen for and manage depression
Educate and reEducate and re--educate patientseducate patients
Diabetes doesn’t cause Diabetes doesn’t cause
complications. Poorly controlled complications. Poorly controlled
diabetes causes complications diabetes causes complications
1/9/2014
12
My ExperienceMy Experience
Scare tactics generally Scare tactics generally
don’t don’t work, if at all, until patients work, if at all, until patients
have lost somethinghave lost something
Scare tactics and threats aren’t Scare tactics and threats aren’t
conducive to good relationshipsconducive to good relationships
Building a relationship worksBuilding a relationship works
“If you want to tell
someone the truth,
first make them laugh.
Otherwise they will
kill you.”
- Oscar Wilde
Getting Patients To Buy In
Use humor
Tell patients about your personal or family
experiences with diabetes
Criticize behaviors, not the person
Use patient Handouts & Digital Imaging
Conference with the patient & family
As a last resort for men, the risk of
impotence can be a very strong motivator
Various research indicates that men think about sex Q 6-8 seconds
The Most Important Message A
Health Care Professional Can
Convey To Patients Living With
Chronic Disease, Including
Diabetes:
“I Am On
Your Side”
The Most Important Message A
Health Care Professional Can
Convey To Other Members of
the Diabetes Care Team…
“The only way to keep your health
is to eat what you don't want, drink
what you don't like, and do what
you'd rather not.”
“Get your facts first, then you
can distort them as you please”
1/9/2014
13
Thank You!Thank You!
A. Paul A. Paul ChousChous, MA, OD, FAAO, MA, OD, FAAO
[email protected]@diabeticeyes.com








![[2015 KAGGLE CHALLENGE CASE II - CANCEL] Diabetic Retinopathy …neohan.org/wp-content/uploads/2015/07/캐글-프로젝트... · 2015-07-29 · 2015_kaggle_diabetic retinopathy 문제](https://img.pdfslide.tips/doc/110x75/5e3ed349955a8e530e0e641a/2015-kaggle-challenge-case-ii-cancel-diabetic-retinopathy-e-eoe.jpg)



![Community Pharmacy Centered Rural Mobile Diabetic ... · Diabetic Retinopathy (DR) is considered one of the leading global causes of blindness [1]. It is a common complication of](https://img.pdfslide.tips/doc/110x75/5e3ed00cf9c32e41ea6578ad/community-pharmacy-centered-rural-mobile-diabetic-diabetic-retinopathy-dr.jpg)