Embed Size (px)
DESCRIPTION
asistensi cpr
Citation preview

C
Deit
GGa
b
c
d
e
f
a
ARRA
KORDC
i
L
0h
Resuscitation 85 (2014) 49–52
Contents lists available at ScienceDirect
Resuscitation
journa l homepage: www.e lsev ier .com/ locate / resusc i ta t ion
linical paper
ispatch-assisted CPR: Where are the hold-ups during calls tomergency dispatchers? A preliminary analysis of caller–dispatchernteractions during out-of-hospital cardiac arrest using a novel callranscription technique�
areth R. Clegga,b, Richard M. Lyona,c,∗, Scott Jamesa, Holly P. Branigand, Ellen G. Barde,erry J. Eganf
Emergency Medicine Research Group, Edinburgh, United KingdomQueen’s Medical Research Institute, The University of Edinburgh, Little France Crescent, Edinburgh EH16 4SA, United KingdomEmergency Department, Royal Infirmary of Edinburgh, Little France Crescent, Edinburgh EH16 4SA, United KingdomDepartment of Psychology, University of Edinburgh, United KingdomDepartment of Linguistics and English Language, University of Edinburgh, United KingdomScottish Ambulance Service, United Kingdom
r t i c l e i n f o
rticle history:eceived 3 June 2013eceived in revised form 5 August 2013ccepted 21 August 2013
eywords:ut-of-hospital cardiac arrestesuscitationispatchardiopulmonary resuscitation
a b s t r a c t
Background: Survival from out-of-hospital cardiac arrest (OHCA) is dependent on the chain of survival.Early recognition of cardiac arrest and provision of bystander cardiopulmonary resuscitation (CPR) arekey determinants of OHCA survival. Emergency medical dispatchers play a key role in cardiac arrestrecognition and giving telephone CPR advice. The interaction between caller and dispatcher can influencethe time to bystander CPR and quality of resuscitation. We sought to pilot the use of emergency calltranscription to audit and evaluate the holdups in performing dispatch-assisted CPR.Methods: A retrospective case selection of 50 consecutive suspected OHCA was performed. Audio recor-dings of calls were downloaded from the emergency medical dispatch centre computer database. All callswere transcribed using proprietary software and voice dialogue was compared with the correspondingstage on the Medical Priority Dispatch System (MPDS). Time to progress through each stage and numberof caller–dispatcher interactions were calculated.Results: Of the 50 downloaded calls, 47 were confirmed cases of OHCA. Call transcription was successfullycompleted for all OHCA calls. Bystander CPR was performed in 39 (83%) of these. In the remaining cases,the caller decided the patient was beyond help (n = 7) or the caller said that they were physically unableto perform CPR (n = 1). MPDS stages varied substantially in time to completion. Stage 9 (determining ifthe patient is breathing through airway instructions) took the longest time to complete (median = 59 s,IQR 22–82 s). Stage 11 (giving CPR instructions) also took a relatively longer time to complete comparedto the other stages (median = 46 s, IQR 37–75 s). Stage 5 (establishing the patient’s age) took the shortest
time to complete (median = 5.5 s, IQR 3–9 s).Conclusion: Transcription of OHCA emergency calls and caller–dispatcher interaction compared to MPDSstage is feasible. Confirming whether a patient is breathing and completing CPR instructions requiredthe longest time and most interactions between caller and dispatcher. Use of call transcription has thepotential to identify key factors in caller–dispatcher interaction that could improve time to CPR andfurther research is warranted in this area.� A Spanish translated version of the summary of this article appears as Appendixn the final online version at http://dx.doi.org/10.1016/j.resuscitation.2013.08.018.∗ Corresponding author at: Emergency Department, Royal Infirmary of Edinburgh,ittle France Crescent, Edinburgh EH16 4SA, United Kingdom.
E-mail address: [email protected] (R.M. Lyon).
300-9572/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.resuscitation.2013.08.018
© 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Out-of-hospital cardiac arrest (OHCA) is a significant cause ofmortality and serious neurological morbidity with over 275,000
OHCA occurring in Europe annually.1 Survival-to-discharge ratesafter OHCA continue to vary significantly. Early bystander car-diopulmonary resuscitation (CPR) has been shown to significantlyimprove survival from OHCA.2,3
5 scitat
fCcti
hpfiabwC
CgaiCDt
bsfecacitc
mii
2
2
b(auq
2
fib5ftwutc
ist
0 G.R. Clegg et al. / Resu
Emergency medical dispatchers can give instructions on per-orming CPR. The introduction of a protocol for dispatch-assistedPR has been shown to improve rates of bystander CPR and out-ome from OHCA.4 Emergency medical dispatch is the first link inhe chain of survival and dispatch-assisted CPR plays a key role innitiating early basic life support.
Rates of dispatch-assisted CPR are variable. Previous studiesave reported highly variable bystander CPR rates when the dis-atcher offers CPR instructions. The most frequently cited reasonor not performing dispatch-assisted CPR is refusal to follow thenstructions given by the dispatcher. The interaction between callernd dispatcher is a key to determining whether bystander CPR wille performed. Identifying factors that would improve complianceith dispatch-assisted CPR has the potential to increase bystanderPR rates and potentially to save lives.
Call processing by dispatchers is important for dispatch-assistedPR.5,6 Confirmation of cardiac arrest and establishing the geo-raphical location of the incident both need to be undertakenccurately and rapidly. The dispatcher needs to provide clearnstructions to the caller to perform CPR. Any delay in commencingPR could have an adverse effect on patient outcome from OHCA.ispatch research has been designated a key area of research by
he European Resuscitation Council.7
The interactions between caller and dispatcher influenceystander CPR. Dispatch–caller interaction can determine thepeed and accuracy of identification of cardiac arrest and canacilitate timely initiation of bystander-CPR.4 Audio recordings ofmergency calls have previously been used in an attempt to analysealler–dispatcher interaction as part of emergency dispatch qualityssurance. Many emergency dispatch systems use standard proto-ols, such as Medical Priority Dispatch System (MPDS), to guide callnterrogation and advice. Audio transcription with mapping ontohe dispatch algorithm is a novel method of objectively analysingaller–dispatcher interaction.
We sought to pilot the use of audio call transcription as a novelethod of caller–dispatcher audit and analyse caller–dispatch
nteractions during OHCA emergency calls to identify factors affect-ng the likelihood of bystanders performing dispatch-guided CPR.
. Methods
.1. Population
The regional Emergency Medical Dispatch Centre (EMDC),ased in Edinburgh, serves the population of south-east Scotlandapproximately 1.5 million population). Edinburgh EMDC handlespproximately 3000 calls per day. Emergency medical call handlersndergo an 8-week training program and do not require any formalualifications to undertake the role.
.2. Cardiac arrest calls
All emergency calls taken by EMDC are recorded as digital audioles. Audio files from 50 consecutive OHCA calls were selectedy MPDS classification from all OHCA calls between 2/3/2011 an/4/2011. Ethical permission for analyzing the calls was gainedrom the University of Edinburgh. Calls were downloaded fromhe EMDC system and stored on a secure computer systemithin Edinburgh University. These recordings were transcribedsing ChannelTrans software (University of California, Berkeley)o delineate the exact timing and content of the caller–dispatcheronversation throughout the call.
All emergency calls are handled by EMDC adhering closely to andentical protocol. The dispatcher is directed through a pre-definederies of questions to identify the nature of the call and priori-ise an appropriate ambulance response. The triage system used by
ion 85 (2014) 49–52
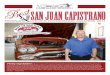
Scottish EMDCs is MPDS. The sequence of questions used in the caseof suspected cardiac arrest is summarised as a series of key stages inFig. 1. This sequence is rigidly adhered to by call-handlers. Calls aresystematically audited to check compliance with MPDS protocols.
Following transcription, timestamps were inserted to indicatethe move from one stage to the next. These timings formed a ‘callmap’ for each of the 50 audio files and determination of the exactamount of time spent moving through each stage of the call. Thenumber of ‘turns’ was also determined for each stage. A turn isdefined as one person’s speech between stretches of speech by theother person. A ‘turn’ might ask one or more questions or provideinstruction, information, or feedback.
3. Results
All of the audio files provided by the Scottish Ambulance Servicefor the audit, all were of sufficient quality to allow for completetranscription and further analysis of the caller/dispatcher interac-tions. Version 12 MDPS was used without any changes for localdialect or language. A single researcher transcribed all the callsafter minimal familiarisation with the ChannelTrans software. Ofthe total 50 calls provided, three were excluded because the callwas not deemed to be an actual cardiac arrest by the investigators(n = 3). Of the remaining 47 calls, CPR was performed in 39 (83%).Reasons for not performing CPR included the caller’s judgementthat the patient was beyond help (n = 6) and the caller reportingthat they were physically unable to perform CPR (n = 1). In one caseCPR was already on going when the emergency call was made andthis case was excluded. 46 (98%) calls were placed by individualsknown to the patient and only one call was placed by a passer-bywho was a stranger to the patient.
The timestamp data and number of ‘turns’ at each stage of thecall were recorded and plotted. Turns versus time were plottedfor each of the ten primary MPDS stages shown in Fig. 1. Therewas a positive correlation between the time taken to completestage 9 (determining if the patient is breathing through airwayinstructions) and the number of ‘turns’ in the caller–call handlerinteraction (r2 = 0.871). There was no relationship between timetaken and number of turns on the remaining stages.
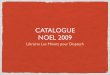
The time spent on each individual MPDS stage is the shown inFig. 2. The plot shows the progress of the call through the MPDSprotocol. Several stages took a relatively long time to complete.Stage 9 (determining if the patient is breathing by moving patientto floor and airway instructions) took the longest (median = 59 s,IQR 22–82 s). Stage 11 (giving CPR instructions) was also longerrelative to the other stages (median = 46 s, IQR 37–75 s). Stage 5(establishing the patient’s age) took the shortest time to complete(median = 5.5 s, IQR 3–9 s).
The number of turns plotted against MPDS stage is shown inFig. 3. Stage 9 (determining if the patient is breathing by movingpatient to the floor and airway instructions) took the most numberof turns to complete and had the widest range of turns (median = 6,IQR 3–11). Stage 7 (asking if the patient is breathing) also had awide range of turns (median = 2, IQR 1–5).
Both analyses by time and number of turns identified stages 7(asking if patient is breathing) and 9 (determining if the patientis breathing by moving patient to floor and airway instructions)as steps on the MPDS protocol that could be targeted to improvetime to bystander CPR. In our sample the time spent transitioningthrough stage 9 (airway instructions and placing patient flat onground) did not significantly affect the time to starting CPR, butthere was a significant relationship between the number of turns
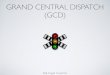
on stage 9 and the number of turns before CPR instructions weregiven (p = 0.0005 CI 95%).The time elements for each stage are shown in cumulative inFig. 4. The cumulative mean time to identification of cardiac arrest

G.R. Clegg et al. / Resuscitation 85 (2014) 49–52 51
DS cal
w(
4
wskitett
Fig. 1. Summary of the key stages in the MP
as 03:39 (range 00:33–09:40) and first chest compression 04:45range 00:24–10:47).
. Discussion
OHCA call download, transcription and analysis are possibleith a high degree of data accuracy. Comparison of the call tran-
cript to ambulance dispatch protocols such as MPDS can identifyey stages in the call that delay bystander CPR. Accurately identify-ng whether a patient is breathing and giving CPR instructions takehe longest time and most turns, possibly reflecting the difficulties
ncountered in getting the bystander to complete the requestedasks. These stages could be specifically targeted during dispatcherraining and could be the focus of future dispatch research.Fig. 2. Stage vs. time for all calls (n = 47).
l protocol for out-of-hospital cardiac arrest.
The number of turns taken to complete each MPDS stage maygive an indication of the clarity of the dispatch instructions. Stageswith a high number of turns may indicate areas where communica-tion is poor. This will of course be affected by factors unique to thecallers and call-handlers themselves (e.g. hearing acuity, level ofcognitive function, etc.), but where difficulties occur in a majorityof calls, or where the range of timings and turn taking is large, thedistribution of stage durations may indicate factors in the EMDCsystem itself which may be improved.
Undertaking dispatch analysis by this means ensures account-ability. The call taking process is not routinely audited in great detailbut is a crucially important step in the chain of survival. Pre-ROSCelements in the chain of survival are critically time-dependent andtheir duration is likely to be of disproportionate importance when
compared with other subsequent links. Dispatch analysis of thistime is manpower intensive and further research is warranted onusing technology to automate some of this process.Fig. 3. Stage vs. turns for all calls (n = 47).

52 G.R. Clegg et al. / Resuscitation 85 (2014) 49–52
to CPR
Odpdnciesp
lwcn
atfisaitbst
5
i
1
2
3
4
5
6
Fig. 4. Cumula times
Previous studies have demonstrated an improved outcome fromHCA when the initial emergency call is handled by an experiencedispatcher.8 This is consistent with our results as experienced dis-atchers may be able to negotiate the problematic stages, such asetermining whether the patient is breathing, more rapidly. Weoted that relatives of OHCA victims placed a high proportion ofalls, and may be prone to a higher degree of emotional stress dur-ng the emergency call than unrelated bystanders. It is possible thatxperienced or talented dispatchers may succeed in dealing withuch distress more effectively and ensure that bystander CPR iserformed in timely fashion.
This study has several limitations. The number of calls ana-ysed was relatively small and may not be representative of the
ider OHCA population. However, call transcription was accuratelyompleted in all calls, affirming the usefulness of this research tech-ique for dispatch analysis.
Further investigation is warranted in this field. Transcribing andnalysing a larger number of OHCA calls would confirm call stageshat require improvement. Comparing calls where an accurate con-rmation of cardiac arrest is achieved and dispatch-assisted CPRtarted promptly to calls where diagnosis and CPR are delayed mayllow dispatch factors to be identified for targeted training andmprovement. Identifying factors in the language, tone and mannerhe dispatcher uses may be important. Further analysis of discourseetween caller and dispatcher may identify ways to enhance andtreamline communication to aid diagnosis of OHCA and decreaseime to CPR.
. Conclusion
Transcription of OHCA emergency calls and caller–dispatchernteraction by MPDS stage is feasible. Confirming whether a patient
7
8
by stage for 47 calls.
is breathing and completing CPR instructions required the longesttime and most interactions between caller and dispatcher. Useof call transcription has the potential to identify key factors incaller–dispatcher interaction that could improve time to CPR andfurther research is warranted in this area.
Funding
This project was supported by the University of Edinburgh.
Conflict of interest statement
None to declare.
References
. Atwood C, Eisenberg MS, Herlitz J, et al. Incidence of EMS-treated out-of-hospitalcardiac arrest in Europe. Resuscitation 2005;67:75–80.
. Bardy GH. A critic’s assessment of our approach to cardiac arrest. N Engl J Med2011;364:374–5.
. Sasson C, Rogers MAM, Dahl J, et al. Predictors of survival from out-of-hospitalcardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Out-comes 2010;3:63–81.
. Nurmi J, Pettilä V, Biber B, et al. Effect of protocol compliance to cardiacarrest identification by emergency medical dispatchers. Resuscitation 2006;70:463–9.
. Castrén M, Bohm K, Kvam AM, et al. Reporting of data from out-of-hospitalcardiac arrest has to involve emergency medical dispatching – taking the rec-ommendations on reporting OHCA the Utstein style a step further. Resuscitation2011;82:1496–500.
. Svensson L, Bohm K, Castren M, et al. Compression-only CPR or standard CPR inout-of-hospital cardiac arrest. N Engl J Med 2010;363:434–42.
. Nolan JP, Soar J. Dispatcher-assisted bystander CPR: a KISS for a kiss. Lancet2010;376:1522–4.
. Kuisma M, Boyd J, Väyrynen T, et al. Emergency call processing andsurvival from out-of-hospital ventricular fibrillation. Resuscitation 2005;67:89–93.