Embed Size (px)
Citation preview

DopplersonographieWer
WannWie oft
Susanne Fröhlich
praenatal.de
Symposion 18.11.2017
Dopplersonographiewer ! wann ! wie oft
Entscheidung über
Entbindung KontrolleEinsatz von
Kortikosteroiden
Ziel: Vermeidung von Azidämie/Asphyxie und intrauterinem Tod
DopplersonographieIndikationen
fetomaternal
maternal anamnestischfetal
DopplersonographieIndikationen
! V.a. Wachstumsrestriktion/ SGA
! Auffälligkeiten der fetalen Herzfrequenz
! V.a. Fehlbildung oder fetale Erkrankung
! Mehrlingsschwangerschaften
fetal
DopplersonographieIndikationen
maternal anamnestisch
! Nierenerkrankungen
! Hypertonie/SIH
! Diabetes mellitus
! Kollagenosen und Autoimmunerkrankungen
! Thrombophilien(Antiphospholipidsyndrom)
! Präeklampsie/Eklampsie
! Z.n. Präeklampsie/ Eklampsie
! Z.n. Mangelgeburt/ intrauterinem Tod
DopplersonographieIndikationen
! Plazentationsstörungen (AIP, Plazenta praevia ect.)
! Insertio velamentosa
! Auffälligkeiten der Plazentamorphologie („jelly like“)
fetomaternal
Dopplersonographie
Arterielle GefäßeAa. uterinaeA. umbilicalisAorta/ AortenisthmusA. cerebri media
Venöse GefäßeDuctus venosusV. umbilicalis
Beurteilung:Indizes RI (resistance index) u.PI (pulsatility index), GeschwindigkeitenFlussprofil: Notching, ARED-flow (absent or reversedenddiastolic flow)
DopplersonographieAa. uterinae
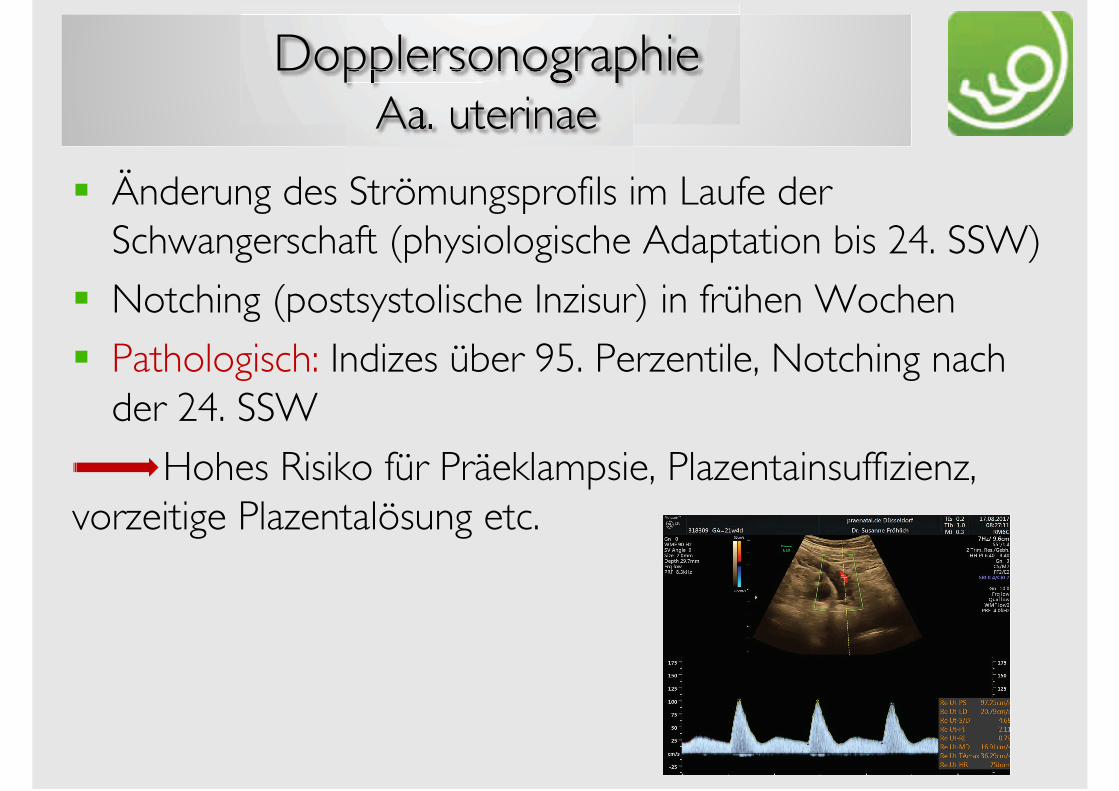
! Änderung des Strömungsprofils im Laufe der Schwangerschaft (physiologische Adaptation bis 24. SSW)
! Notching (postsystolische Inzisur) in frühen Wochen
! Pathologisch: Indizes über 95. Perzentile, Notching nach der 24. SSW
Hohes Risiko für Präeklampsie, Plazentainsuffizienz, vorzeitige Plazentalösung etc.
DopplersonographieA.umbilicalis
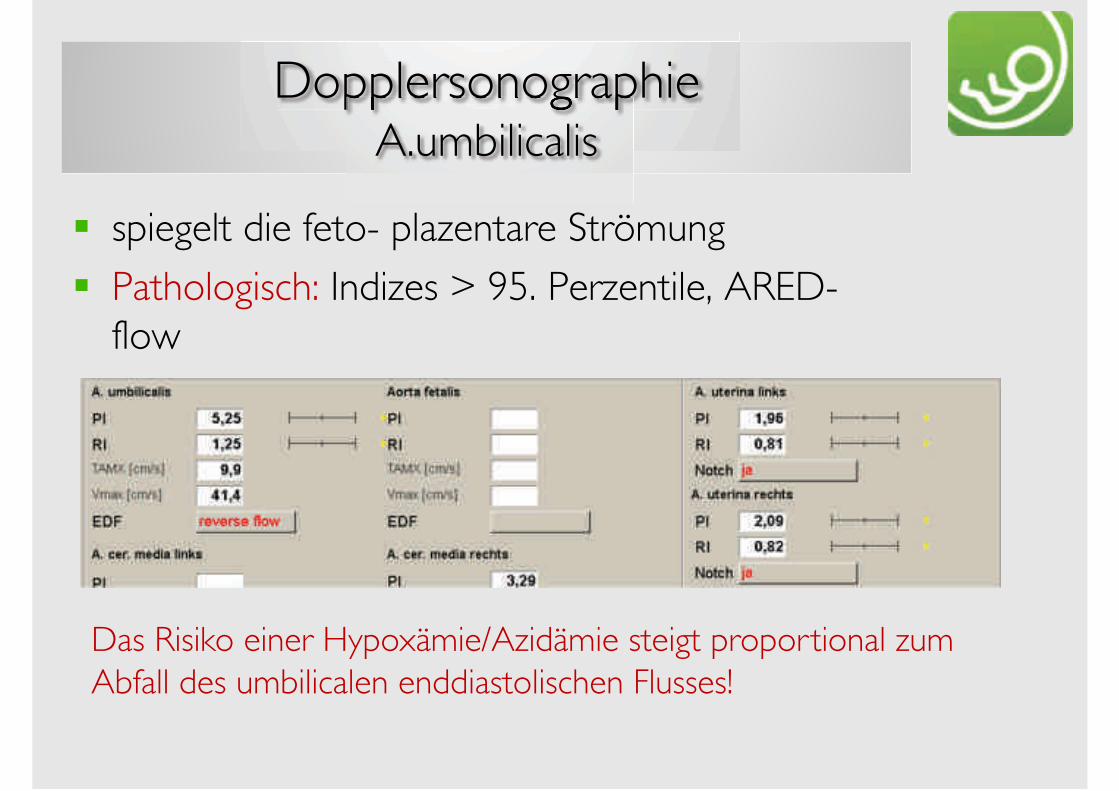
! spiegelt die feto- plazentare Strömung
! Pathologisch: Indizes > 95. Perzentile, ARED-flow
Das Risiko einer Hypoxämie/Azidämie steigt proportional zum Abfall des umbilicalen enddiastolischen Flusses!

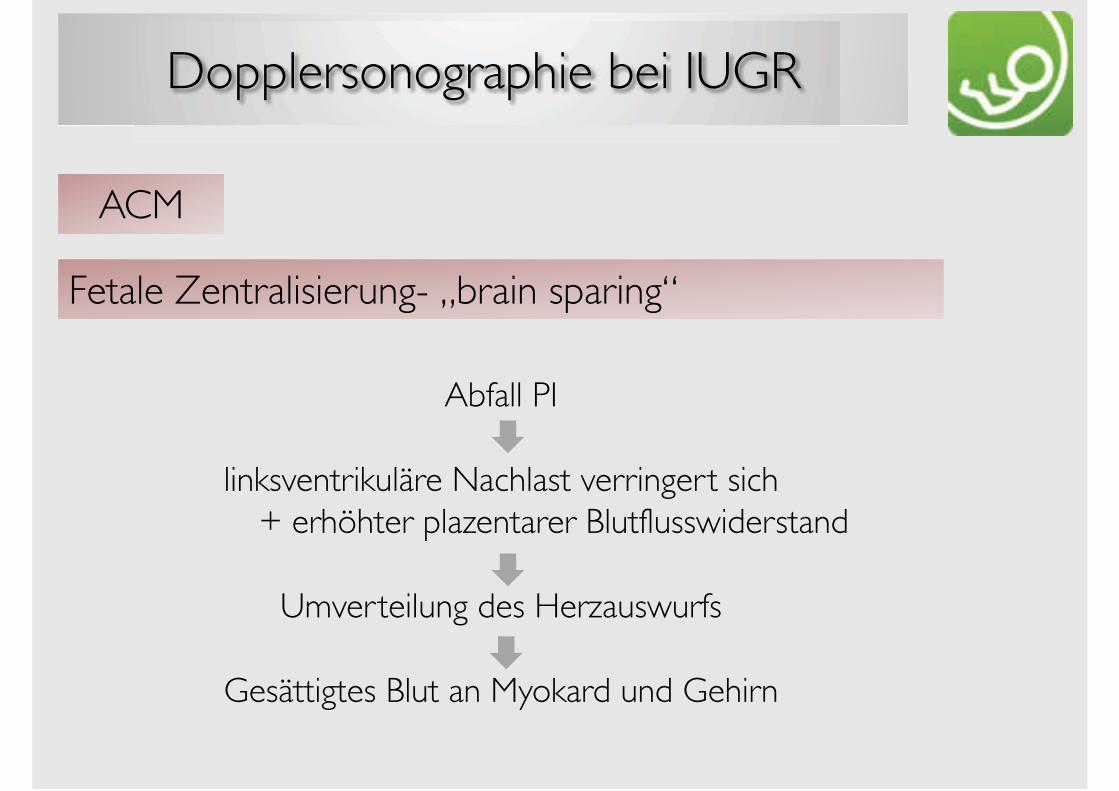
DopplersonographieA. cerebri media
! Physiologisch: hoher Gefäßwiderstand
! Terminnähe: Abnahme der Impedanz + Zunahme der Geschwindigkeit nach der 36. SSW
! Pathologisch: RI/PI > 5.-10. Perzentile „brain sparing“
Diagnostik der fetalen Anämie!
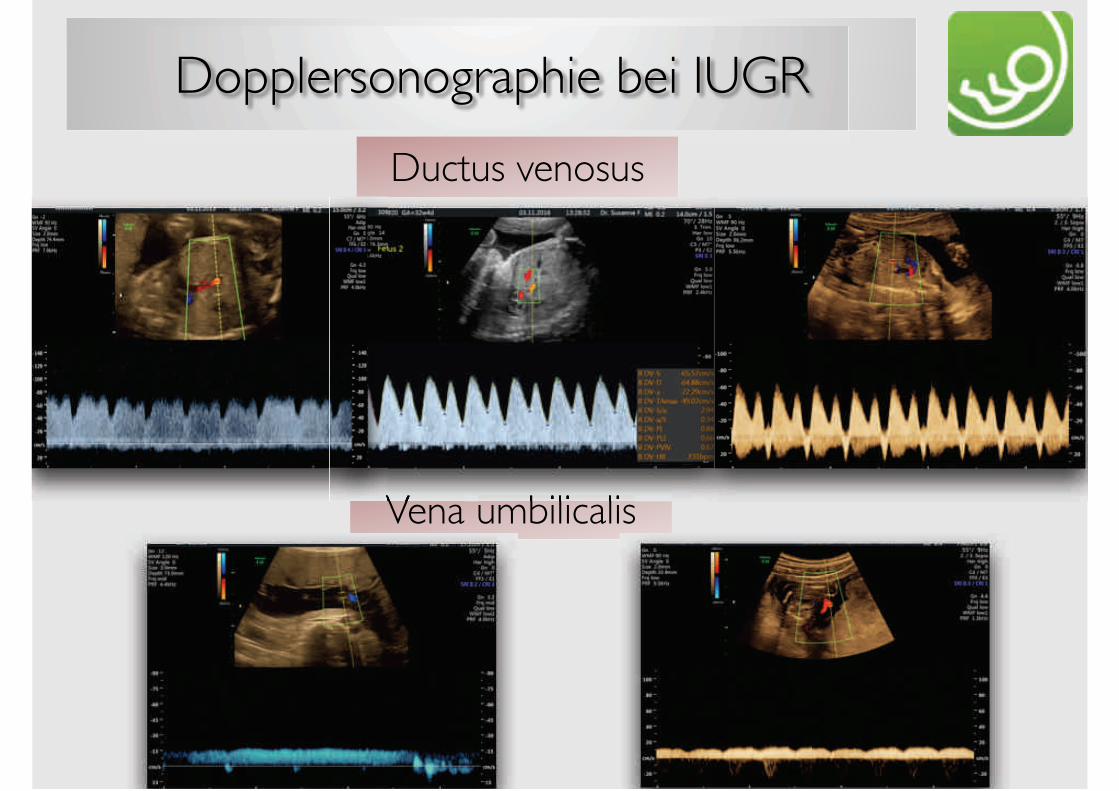
DopplersonographieDuctus venosus
Physiologisch: Zunahme der Flussgeschwindigkeit + Abnahme der Pulsatilität
Pathologisch: Zunahme der Pulsatilität + retrograder Fluss (reverse flow)
Pathologischer DV:! Schwer zentralisierte Feten! Kardiale Vitien! Herzrhythmusstörungen! Zwerchfellhernie! Erhöhtes Risiko für eine Aneuploidie (1.Trimenon!)
DopplersonographieV.umbilicalis
Strömung von Plazenta zu Fet
Kontinuierlicher Fluss: II. Schwangerschaftshälfte
Pulsationen: physiologisch im I. Trimenonpathologisch im II. + III. Trimenon
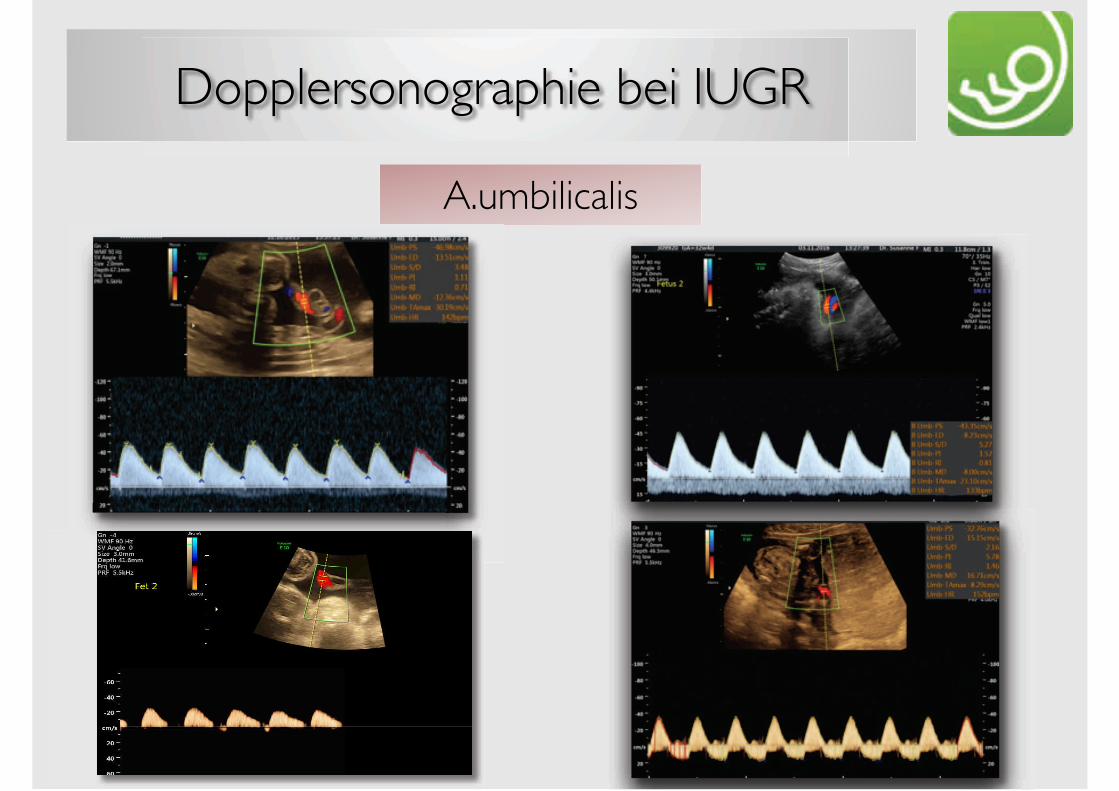
Dopplersonographie bei IUGR
A.umbilicalis
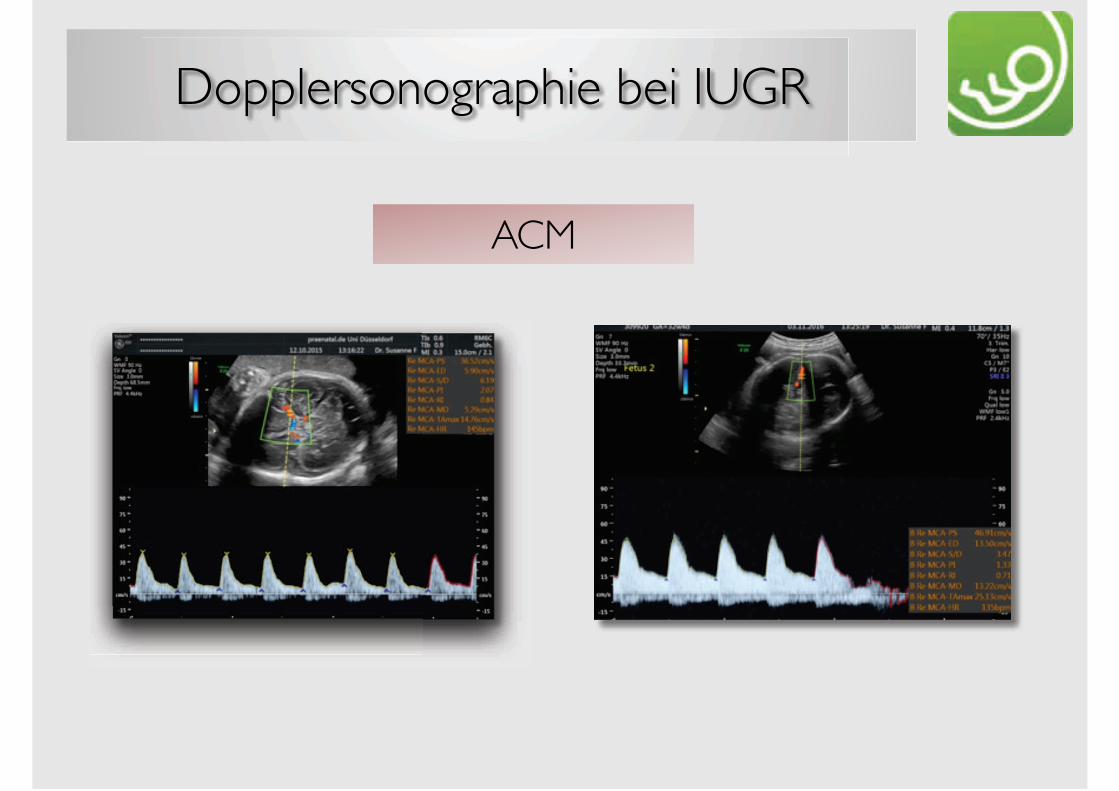
Dopplersonographie bei IUGR
ACM
Dopplersonographie bei IUGR
Ductus venosus
Vena umbilicalis
Dopplersonographie bei IUGR
ACM
Fetale Zentralisierung- „brain sparing“
Abfall PI
linksventrikuläre Nachlast verringert sich+ erhöhter plazentarer Blutflusswiderstand
Umverteilung des Herzauswurfs
Gesättigtes Blut an Myokard und Gehirn
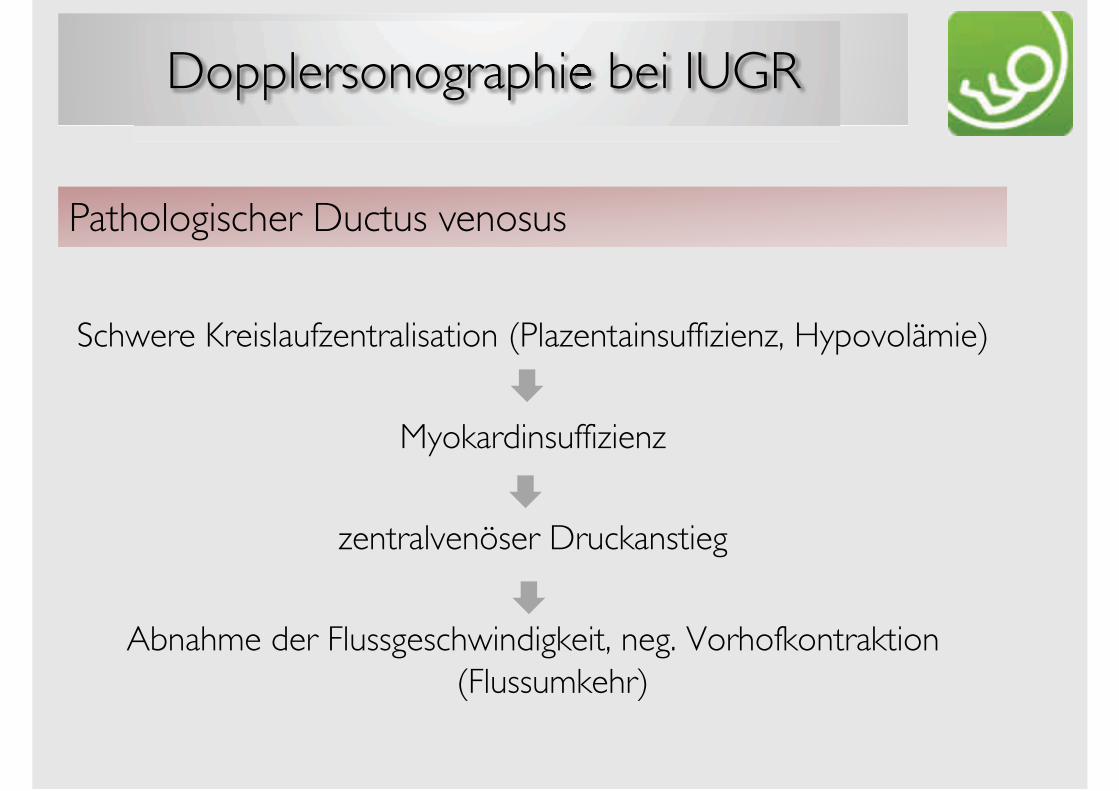
Dopplersonographie bei IUGR
Schwere Kreislaufzentralisation (Plazentainsuffizienz, Hypovolämie)
Myokardinsuffizienz
zentralvenöser Druckanstieg
Abnahme der Flussgeschwindigkeit, neg. Vorhofkontraktion (Flussumkehr)
Pathologischer Ductus venosus
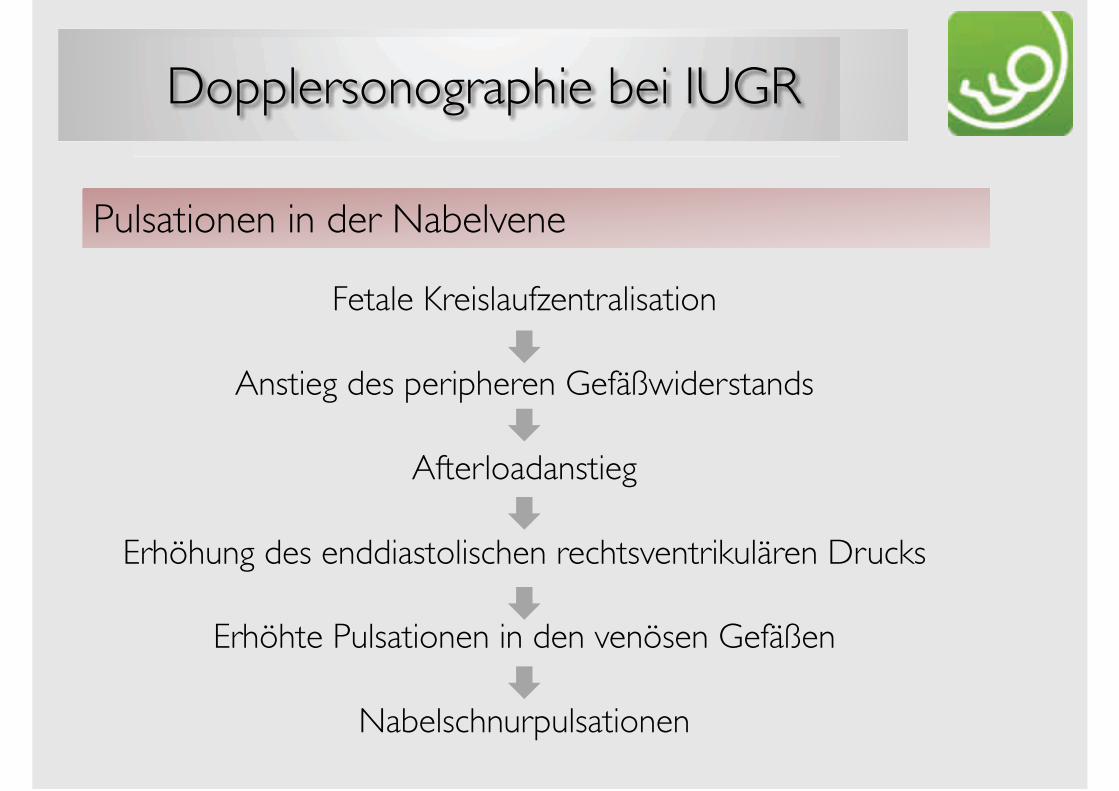
Dopplersonographie bei IUGR
Fetale Kreislaufzentralisation
Anstieg des peripheren Gefäßwiderstands
Afterloadanstieg
Erhöhung des enddiastolischen rechtsventrikulären Drucks
Erhöhte Pulsationen in den venösen Gefäßen
Nabelschnurpulsationen
Pulsationen in der Nabelvene
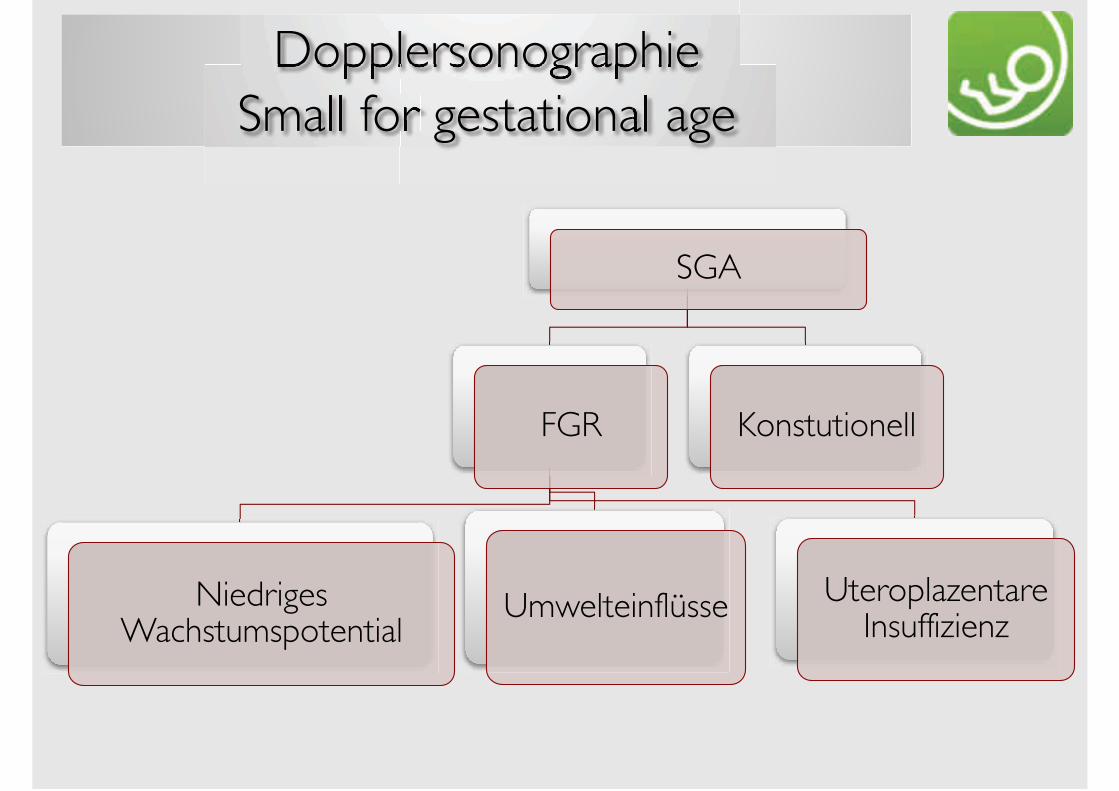
DopplersonographieSmall for gestational age
SGA
FGR
Niedriges Wachstumspotential
Umwelteinflüsse UteroplazentareInsuffizienz
Konstutionell
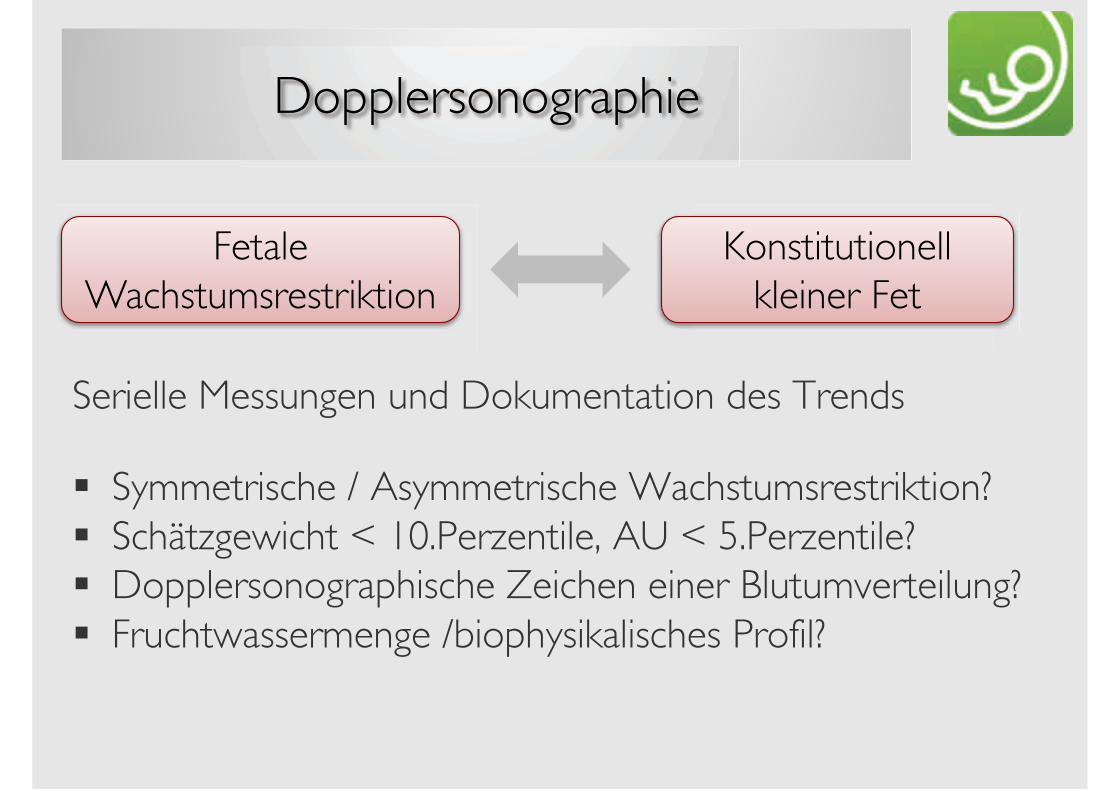
Dopplersonographie
Serielle Messungen und Dokumentation des Trends
! Symmetrische / Asymmetrische Wachstumsrestriktion?! Schätzgewicht < 10.Perzentile, AU < 5.Perzentile?! Dopplersonographische Zeichen einer Blutumverteilung?! Fruchtwassermenge /biophysikalisches Profil?
Fetale Wachstumsrestriktion
Konstitutionell kleiner Fet
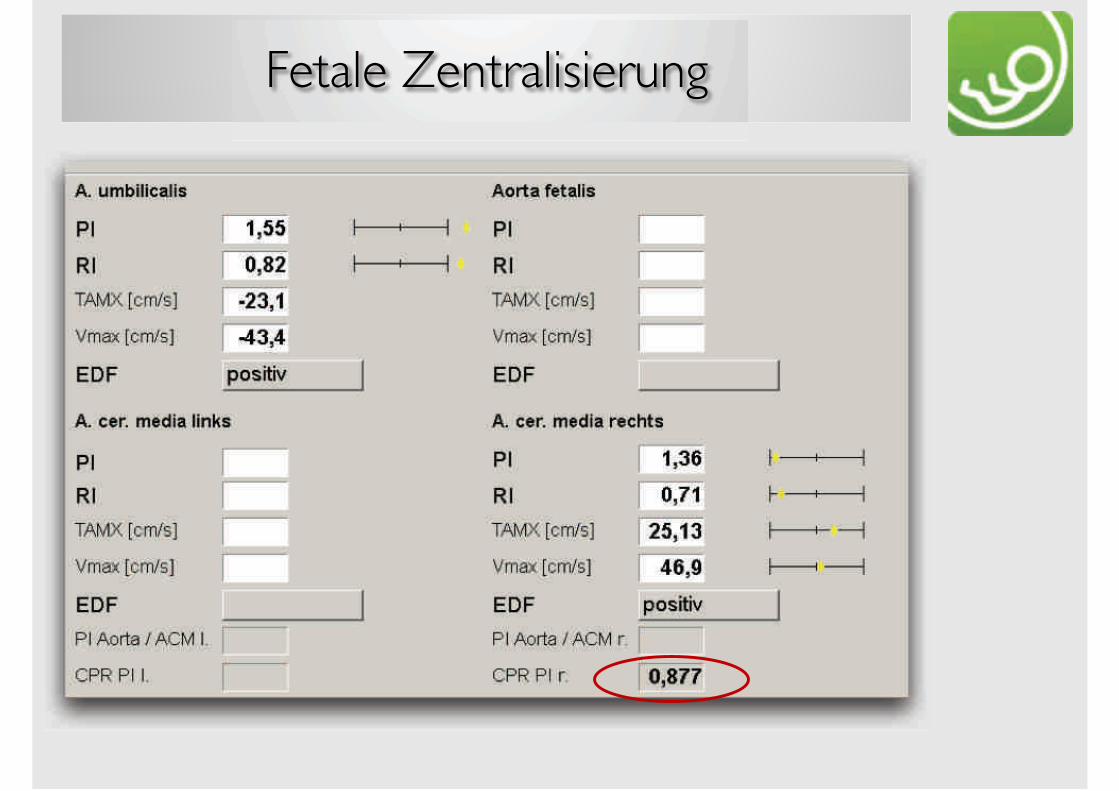
Fetale Zentralisierung
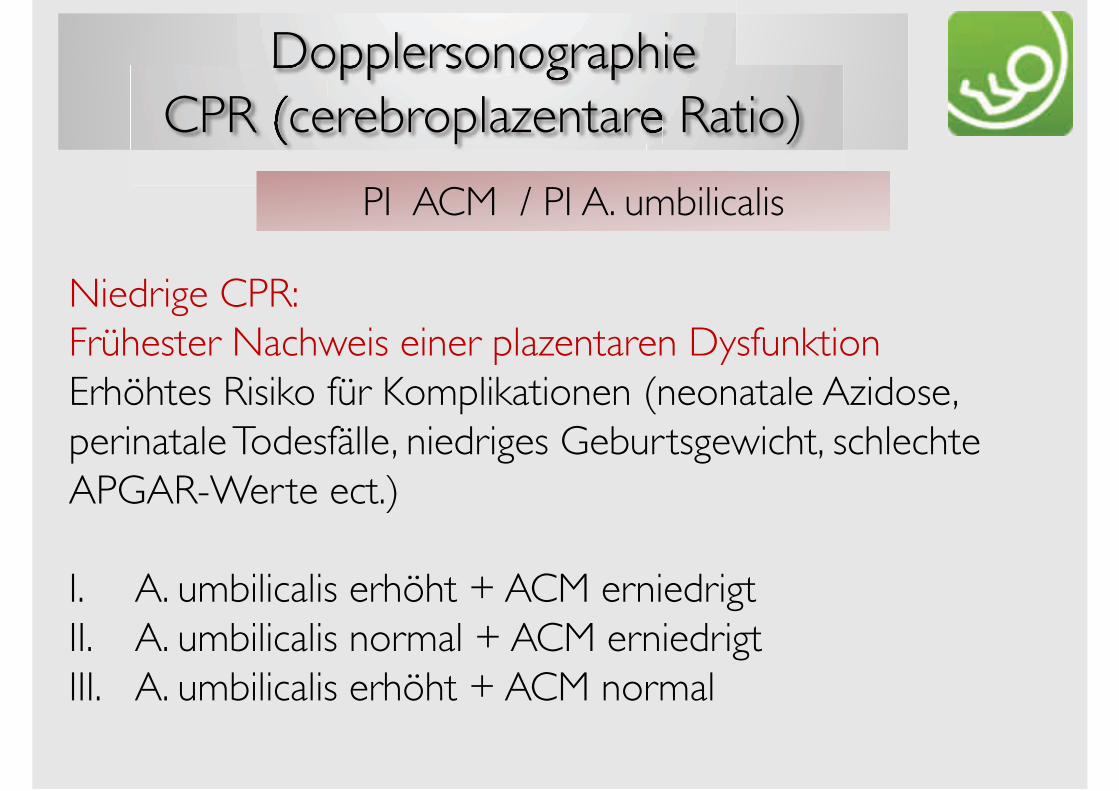
DopplersonographieCPR (cerebroplazentare Ratio)
Niedrige CPR:Frühester Nachweis einer plazentaren DysfunktionErhöhtes Risiko für Komplikationen (neonatale Azidose, perinatale Todesfälle, niedriges Geburtsgewicht, schlechte APGAR-Werte ect.)
I. A. umbilicalis erhöht + ACM erniedrigtII. A. umbilicalis normal + ACM erniedrigtIII. A. umbilicalis erhöht + ACM normal
PI ACM / PI A. umbilicalis
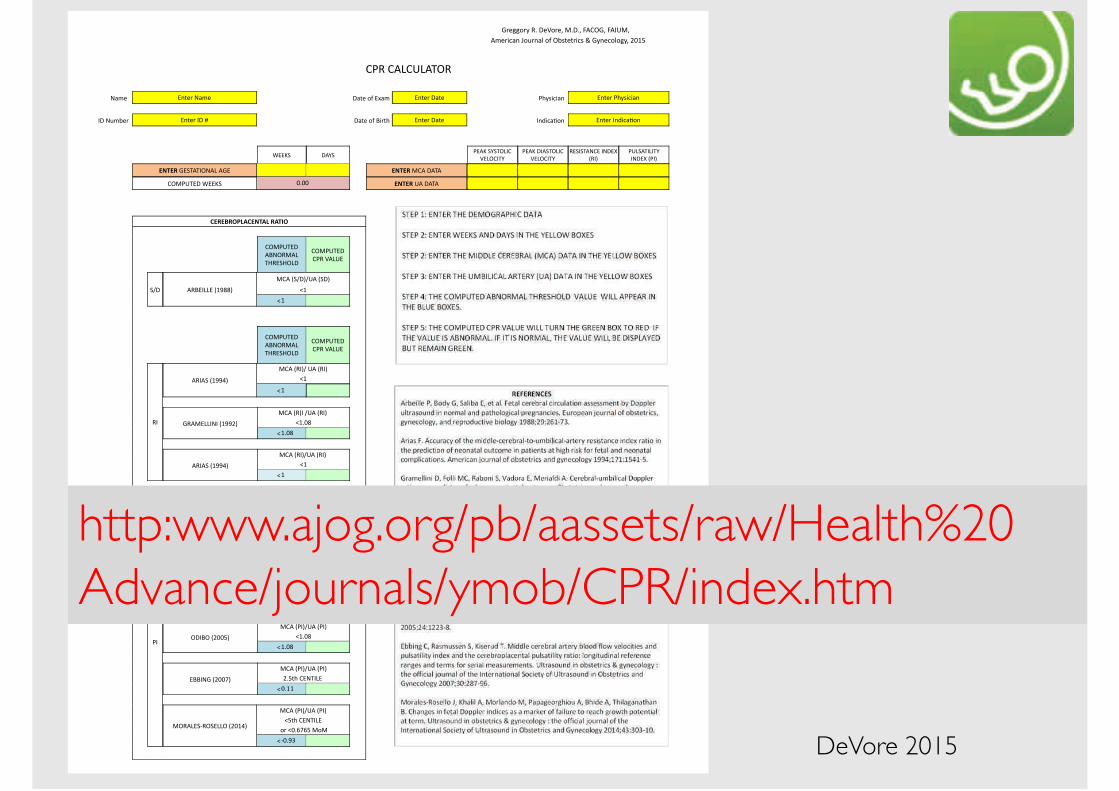
!"#$$%"&'()'*#+%"#,'-)*),'./01!,'./23-,'''
/4#"5678'9%:"87;'%<'1=>?#?"56>'@'!&8#6%;%$&,'ABCD
' ' ' ' ' ' '
0E('0/F03F/G1(
' ' ' ' ' '
' ' ' ' ' ' ' ' ' ' ' ' '
' ' ' ' ' ' ' ' ' ' ' ' '
H74#''' I8?#"'H74# ' ' *7?#'%<'IJ74' I8?#"'*7?# ' EK&>56578'' I8?#"'EK&>56578 '
2*'H:4=#"'' I8?#"'2*'L ' ' *7?#'%<'M5"?K' I8?#"'*7?# ' 28N567O%8'' I8?#"'28N567O%8 '
' ' 'PIIQR */SR
' ' '
EI/Q'RSRG1F20
+IF102GS
EI/Q'*2/RG1F20
+IF102GS
(IR2RG/H0I'2H*IT
U(2V
E3FR/G2F2GS
2H*IT'UE2V '
' !"#!$'!IRG/G21H/F'/!I ' !"#!$'-0/'*/G/ '
' 01-E3GI*'PIIQR B)BB ' !"#!$'3/'*/G/ '
' ' ' '
' '
' ' ' ' ' ' ' ' '
%!$!&$'()*%!"#*)+$*#,'
' ' ' '
01-E3GI*
/MH1(-/F
GW(IRW1F*
01-E3GI*
0E('+/F3I' ' ' ' ' ' ' '
' '
RX* /(MI2FFI'UCYZZV
-0/'URX*VX3/'UR*V ' ' ' ' ' ' ' '
[C
[C
' ' ' '
01-E3GI*
/MH1(-/F
GW(IRW1F*
01-E3GI*
0E('+/F3I' ' ' ' ' ' ' '
(2
/(2/R'UCYY\V
-0/'U(2VX'3/'U(2V
[C
' ' [C ' ' ' ' ' ' '
!(/-IFF2H2'UCYYAV
-0/'U(V2'X3/'U(2V'
[C)BZ
[C)BZ
/(2/R'UCYY\V
-0/'U(2VX3/'U(2V'
[C
[C
' ' ' '01-E3GI*
/MH1(-/F
GW(IRW1F*
01-E3GI*
0E('+/F3I' ' ' ' ' ' ' '
E2
M/W/*1]R2H!W'UCYYYV
-0/'UE2VX3/'UE2V
[B)D'%<'?K#'-%-
[]C)DD
M/R0W/G'UABB^V
-0/'UE2VX3/'UE2V
[D?K'0IHG2FI'
[]A)YD
1*2M1'UABBDV
-0/'UE2VX3/'UE2V
[C)BZ
[C)BZ
IMM2H!'UABB_V
-0/'UE2VX3/'UE2V
A)D?K'0IHG2FI'
[!"##
-1(/FIR](1RIFF1'UABC\V
-0/'UE2VX3/'UE2V
[D?K'0IHG2FI
'%"'[B)`_`D'-%-
[]B)Y^
' ' ' ' ' ' ' ' ' ' ' ' ' ' ' '
http:www.ajog.org/pb/aassets/raw/Health%20Advance/journals/ymob/CPR/index.htm
DeVore 2015
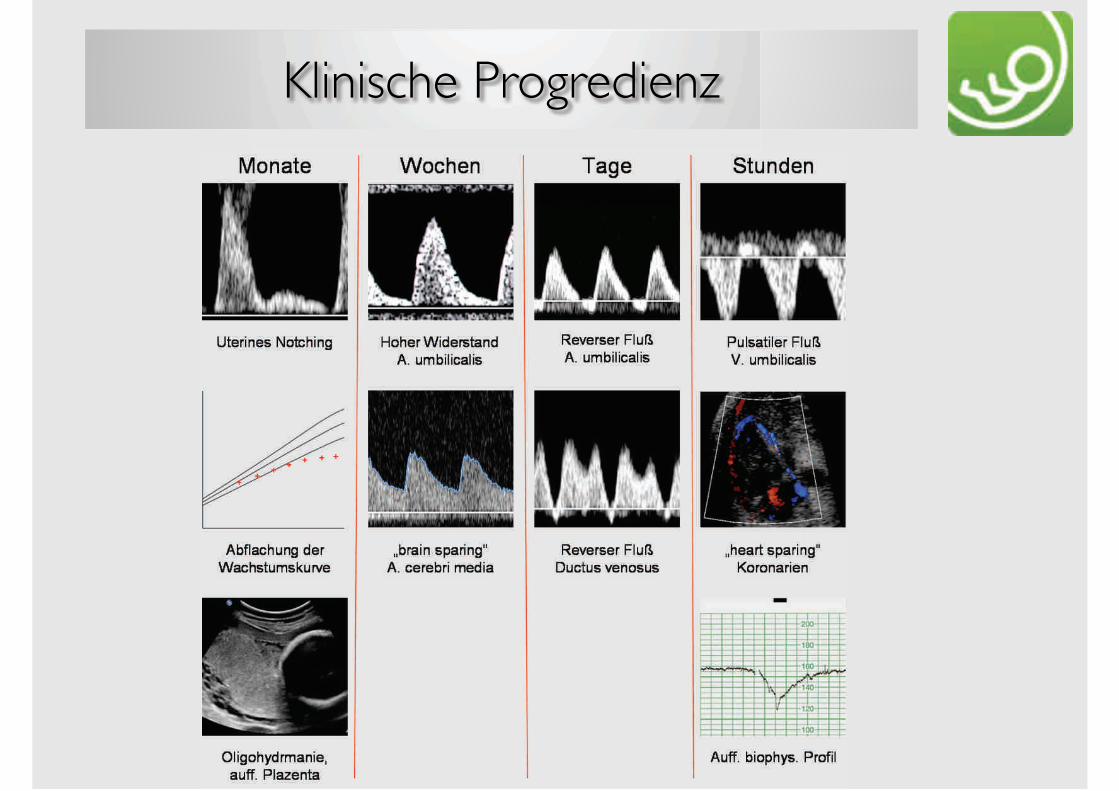
Klinische Progredienz
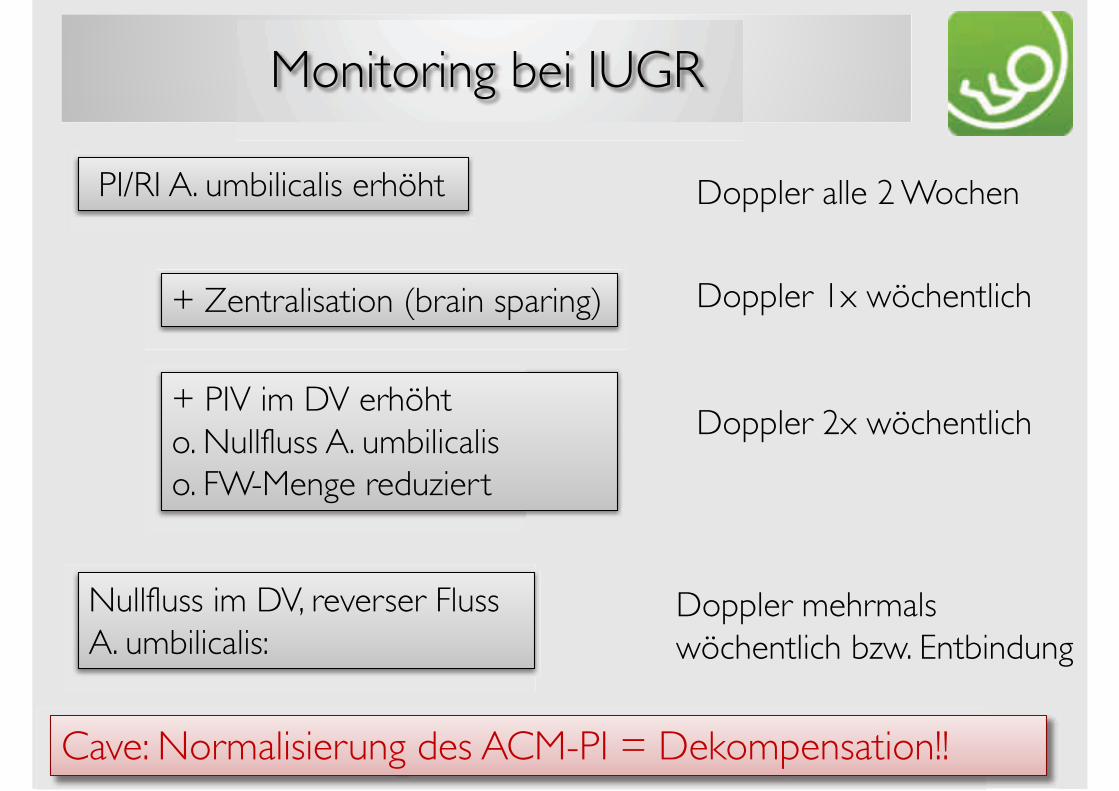
Monitoring bei IUGR
PI/RI A. umbilicalis erhöht Doppler alle 2 Wochen
Doppler 1x wöchentlich
Doppler 2x wöchentlich
Doppler mehrmals wöchentlich bzw. Entbindung
+ Zentralisation (brain sparing)
+ PIV im DV erhöhto. Nullfluss A. umbilicaliso. FW-Menge reduziert
Nullfluss im DV, reverser Fluss A. umbilicalis:
Cave: Normalisierung des ACM-PI = Dekompensation!!
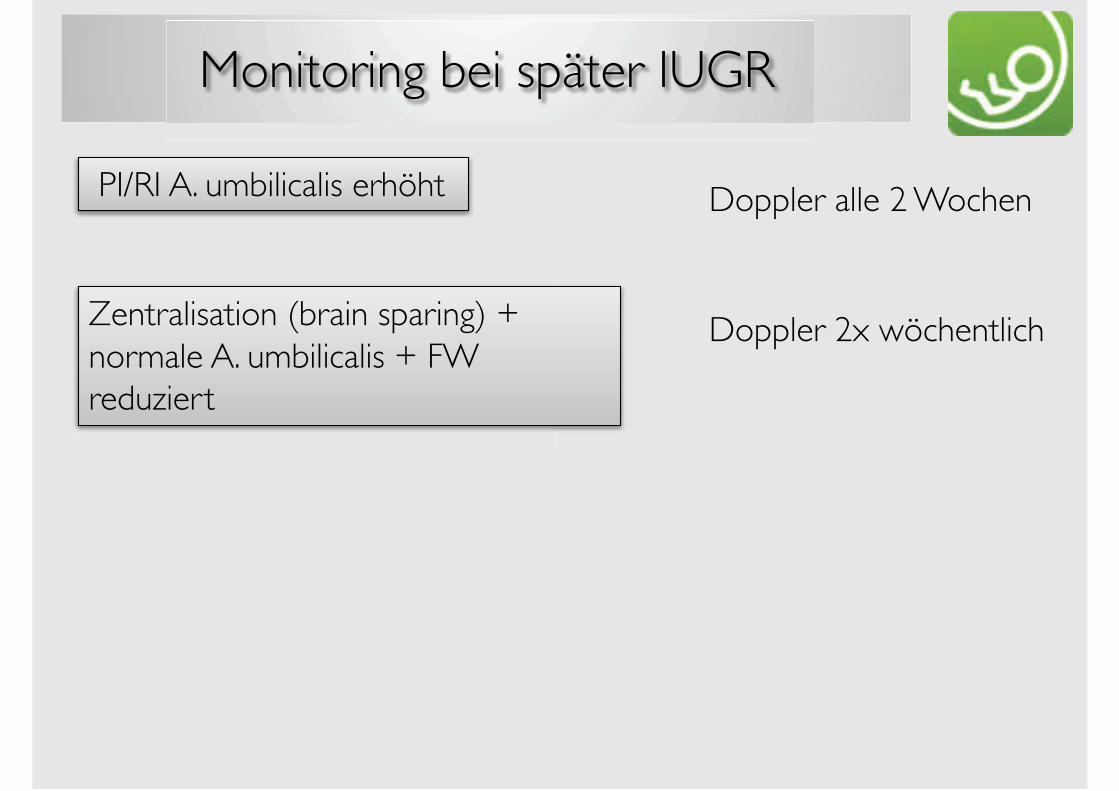
Monitoring bei später IUGR
PI/RI A. umbilicalis erhöht Doppler alle 2 Wochen
Doppler 2x wöchentlichZentralisation (brain sparing) + normale A. umbilicalis + FW reduziert
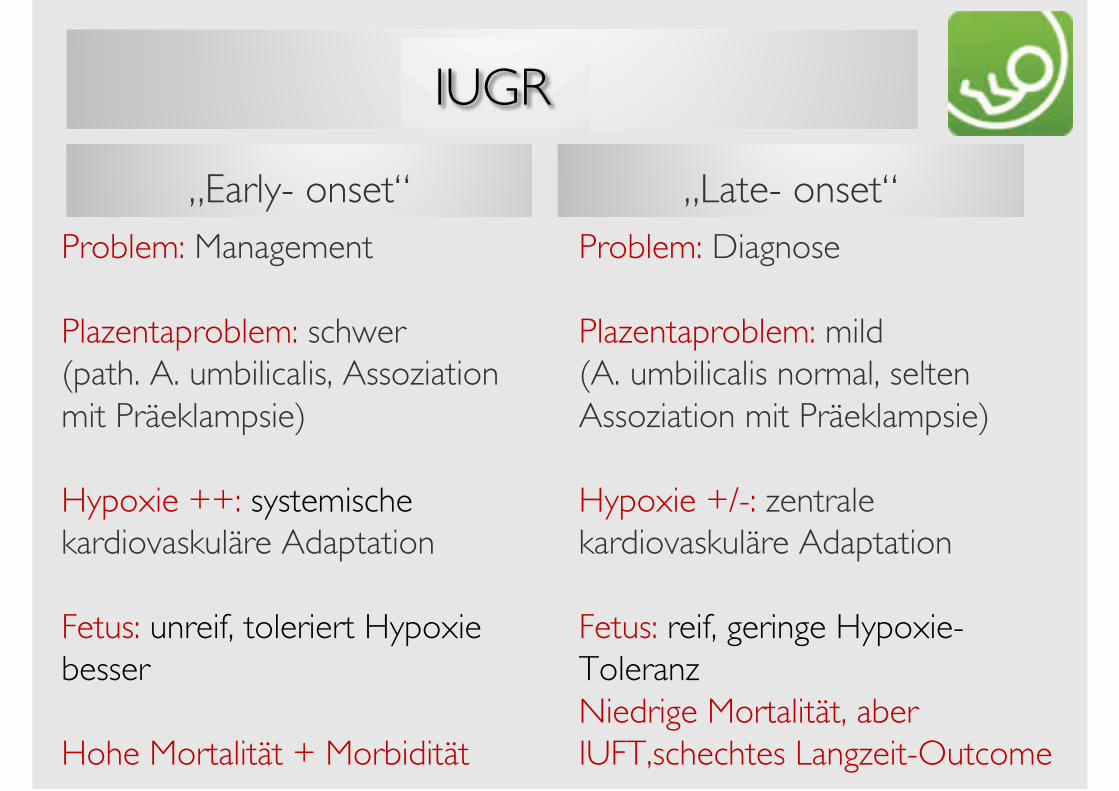
IUGR
„Early- onset“
Problem: Management
Plazentaproblem: schwer (path. A. umbilicalis, Assoziation mit Präeklampsie)
Hypoxie ++: systemische kardiovaskuläre Adaptation
Fetus: unreif, toleriert Hypoxie besser
Hohe Mortalität + Morbidität
„Late- onset“
Problem: Diagnose
Plazentaproblem: mild (A. umbilicalis normal, selten Assoziation mit Präeklampsie)
Hypoxie +/-: zentrale kardiovaskuläre Adaptation
Fetus: reif, geringe Hypoxie-ToleranzNiedrige Mortalität, aber IUFT,schechtes Langzeit-Outcome
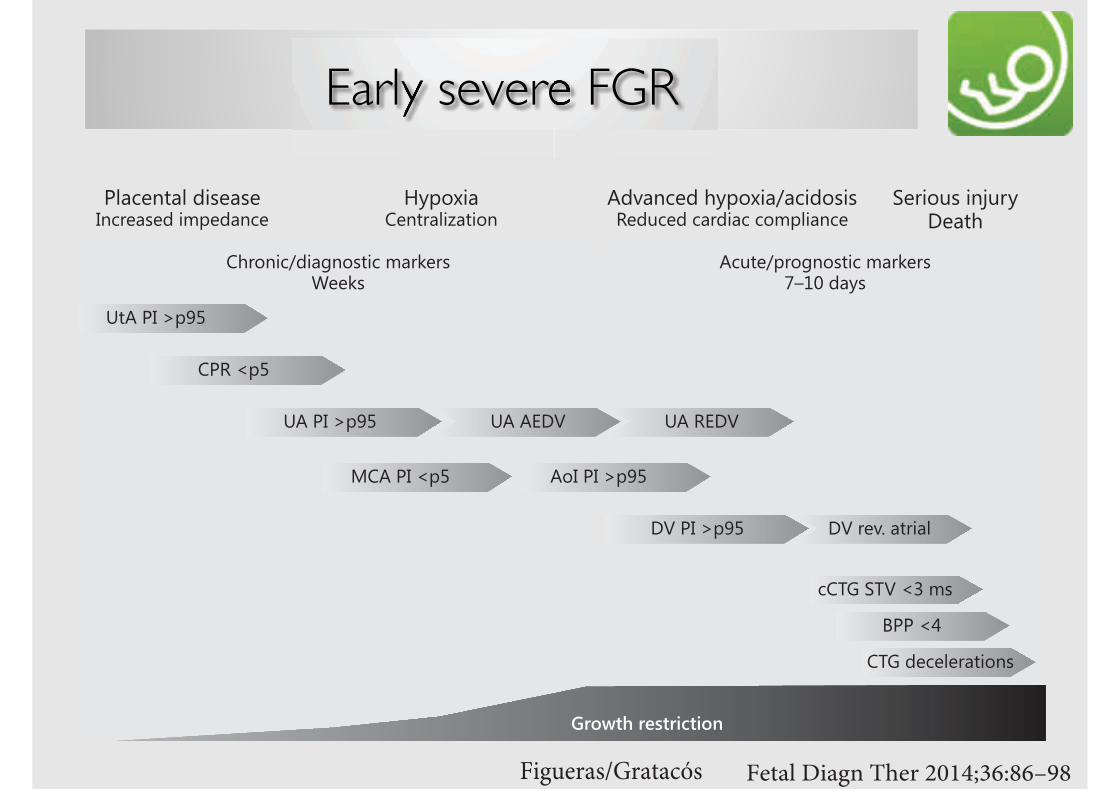
Early severe FGR
!"#$%&'"()%"*+%*#,
!"#$%#&'()
*+#$%#&'()
+,%#$%#&'()-.+#$%#/')
.$0#/')
*1+#$%#&'()
2.34#53"#/6#78
9$$#/:
.34#;<2<=<>?1@,A8
5<>@,B8#@ACB>D!<?1E
+;F?A2<;#ED',G@?H?2@;,8@80<;B2<;#2?>;@?2#2,7'=@?A2<
ID',G@?.<A1>?=@J?1@,A
$=?2<A1?=#;@8<?8<%A2><?8<;#@7'<;?A2<
!"#><FK#?1>@?=
*+#0L!"
+2B1<H'>,MA,81@2#7?>N<>8OPQR#;?D8
.E>,A@2H;@?MA,81@2#7?>N<>8S<<N8
*+#+L!"
Figueras/Gratacós Fetal Diagn Ther 2014;36:86–98DOI: 10.1159/000357592
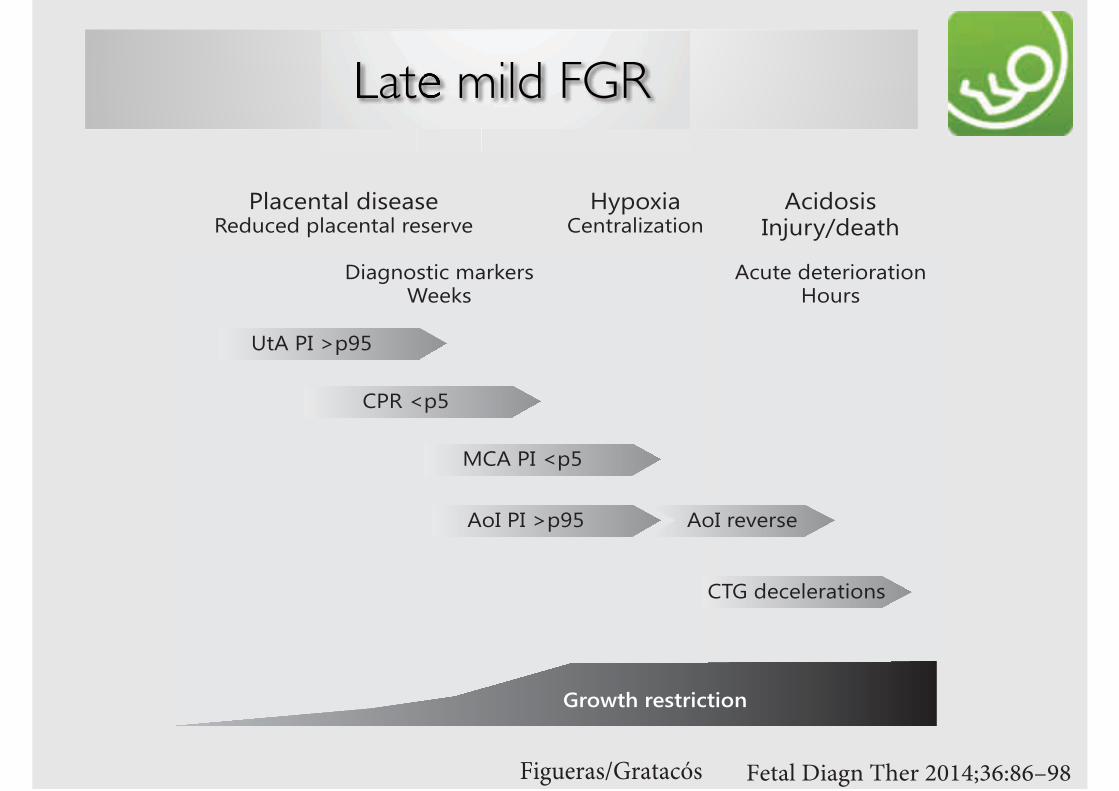
Late mild FGR
Figueras/Gratacós Fetal Diagn Ther 2014;36:86–98DOI: 10.1159/000357592
!"#$%&'"()%"*+%*#,
!"#$%&$'()
#*&$%&$+(,)
"%-$'()
./#$%&$+(,)
"01$23435367/8*9:
#482*:8:&9;<6=>237/?
@=(*A87"39/6758B7/8*9
%57439/75$28:37:3-32<432$(57439/75$63:36C3
#4</3$23/368*67/8*9@*<6:
D87E9*:/84$F76G36:H33G:
#*&$63C36:3
DopplersonographieCTG
! Abnormer Doppler geht in 90% der Fälle den CTG-Veränderungen voraus
! Zeitintervall zwischen Nullfluss in der A. umbilicalis und späten Dezelerationen ca. 12 Tage
! Zeitintervall in höheren Schwangerschaftswochen und bei hypertensiven Erkrankungen kürzer
DopplersonographieIUGR
Ein wachstumsrestringierter Fet im chronischen Hungern während des späten II. und des frühen III.Trimenons toleriert eine chronische Hypoxämie deutlich länger als ein gut ernährter Fet im III. Trimenon mit hohem Energieverbrauch!
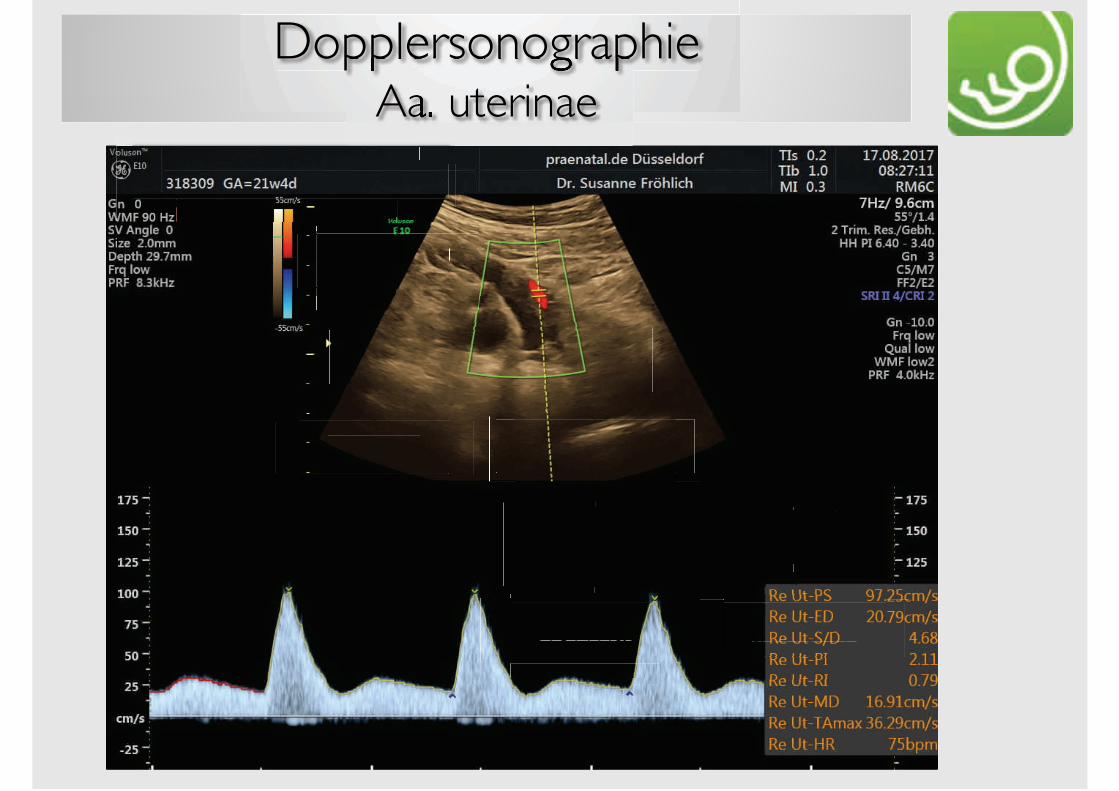
DopplersonographieAa. uterinae
Doppler 20.-24.SSW
abnorm
Doppler 28.-30.SSW
normal abnorm
Doppler 34.SSW
normal abnorm
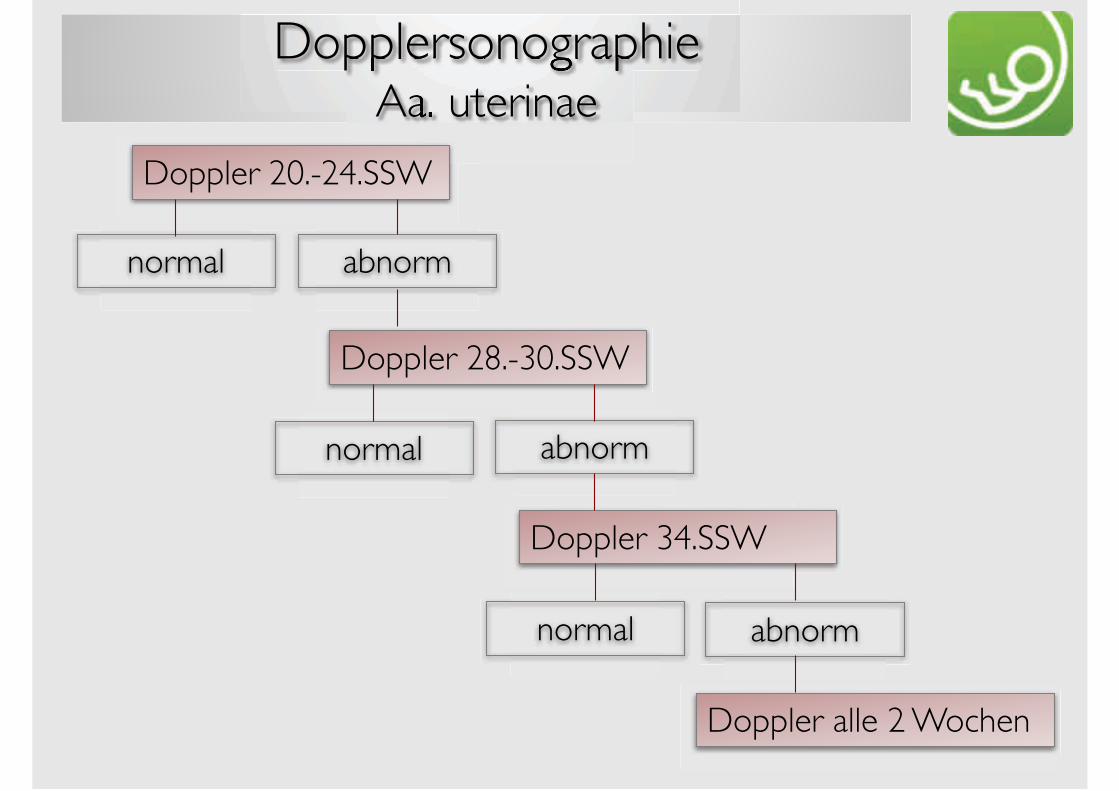
DopplersonographieAa. uterinae
Doppler 20.-24.SSW
normal abnorm
Doppler 28.-30.SSW
normal abnorm
Doppler 34.SSW
normal abnorm
Doppler alle 2 Wochen
DopplersonographieAa. uterinae
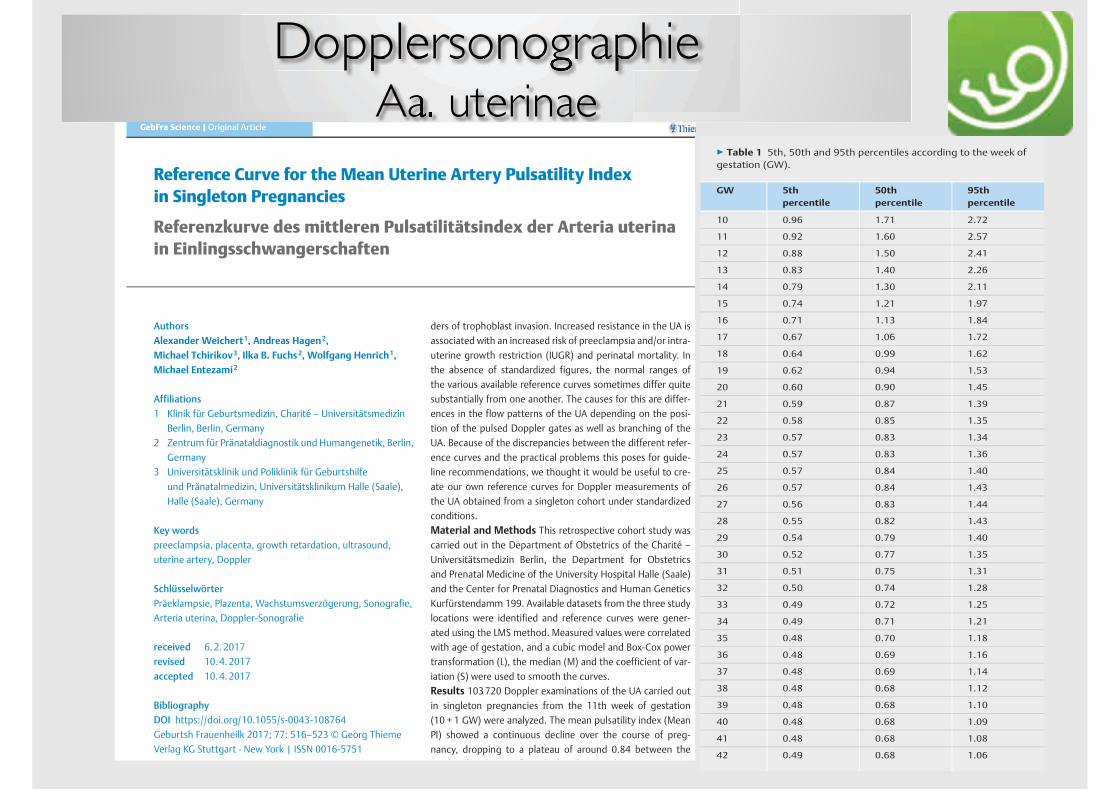
Reference Curve for the Mean Uterine Artery Pulsatility Index
in Singleton Pregnancies
Referenzkurve des mittleren Pulsatilitätsindex der Arteria uterina
in Einlingsschwangerschaften
Authors
Alexander Weichert1, Andreas Hagen2,
Michael Tchirikov3, Ilka B. Fuchs2, Wolfgang Henrich1,
Michael Entezami2
Affiliations
1 Klinik für Geburtsmedizin, Charité – Universitätsmedizin
Berlin, Berlin, Germany
2 Zentrum für Pränataldiagnostik und Humangenetik, Berlin,
Germany
3 Universitätsklinik und Poliklinik für Geburtshilfe
und Pränatalmedizin, Universitätsklinikum Halle (Saale),
Halle (Saale), Germany
Key words
preeclampsia, placenta, growth retardation, ultrasound,
uterine artery, Doppler
Schlüsselwörter
Präeklampsie, Plazenta, Wachstumsverzögerung, Sonografie,
Arteria uterina, Doppler‑Sonografie
received 6.2.2017
revised 10.4.2017
accepted 10.4.2017
Bibliography
DOI https://doi.org/10.1055/s-0043-108764
Geburtsh Frauenheilk 2017; 77: 516–523 © Georg Thieme
Verlag KG Stuttgart · New York | ISSN 0016‑5751
ders of trophoblast invasion. Increased resistance in the UA is
associated with an increased risk of preeclampsia and/or intra-
uterine growth restriction (IUGR) and perinatal mortality. In
the absence of standardized figures, the normal ranges of
the various available reference curves sometimes differ quite
substantially from one another. The causes for this are differ-
ences in the flow patterns of the UA depending on the posi-
tion of the pulsed Doppler gates as well as branching of the
UA. Because of the discrepancies between the different refer-
ence curves and the practical problems this poses for guide-
line recommendations, we thought it would be useful to cre-
ate our own reference curves for Doppler measurements of
the UA obtained from a singleton cohort under standardized
conditions.
Material and Methods This retrospective cohort study was
carried out in the Department of Obstetrics of the Charité –
Universitätsmedizin Berlin, the Department for Obstetrics
and Prenatal Medicine of the University Hospital Halle (Saale)
and the Center for Prenatal Diagnostics and Human Genetics
Kurfürstendamm 199. Available datasets from the three study
locations were identified and reference curves were gener-
ated using the LMS method. Measured values were correlated
with age of gestation, and a cubic model and Box-Cox power
transformation (L), the median (M) and the coefficient of var-
iation (S) were used to smooth the curves.
Results 103720 Doppler examinations of the UA carried out
in singleton pregnancies from the 11th week of gestation
(10 + 1 GW) were analyzed. The mean pulsatility index (Mean
PI) showed a continuous decline over the course of preg-
nancy, dropping to a plateau of around 0.84 between the
23rd and 27th GW, after which it decreased again.
GebFra Science |Original Article
▶ Table 1 5th, 50th and 95th percentiles according to the week of
gestation (GW).
GW 5th
percentile
50th
percentile
95th
percentile
10 0.96 1.71 2.72
11 0.92 1.60 2.57
12 0.88 1.50 2.41
13 0.83 1.40 2.26
14 0.79 1.30 2.11
15 0.74 1.21 1.97
16 0.71 1.13 1.84
17 0.67 1.06 1.72
18 0.64 0.99 1.62
19 0.62 0.94 1.53
20 0.60 0.90 1.45
21 0.59 0.87 1.39
22 0.58 0.85 1.35
23 0.57 0.83 1.34
24 0.57 0.83 1.36
25 0.57 0.84 1.40
26 0.57 0.84 1.43
27 0.56 0.83 1.44
28 0.55 0.82 1.43
29 0.54 0.79 1.40
30 0.52 0.77 1.35
31 0.51 0.75 1.31
32 0.50 0.74 1.28
33 0.49 0.72 1.25
34 0.49 0.71 1.21
35 0.48 0.70 1.18
36 0.48 0.69 1.16
37 0.48 0.69 1.14
38 0.48 0.68 1.12
39 0.48 0.68 1.10
40 0.48 0.68 1.09
41 0.48 0.68 1.08
42 0.49 0.68 1.06
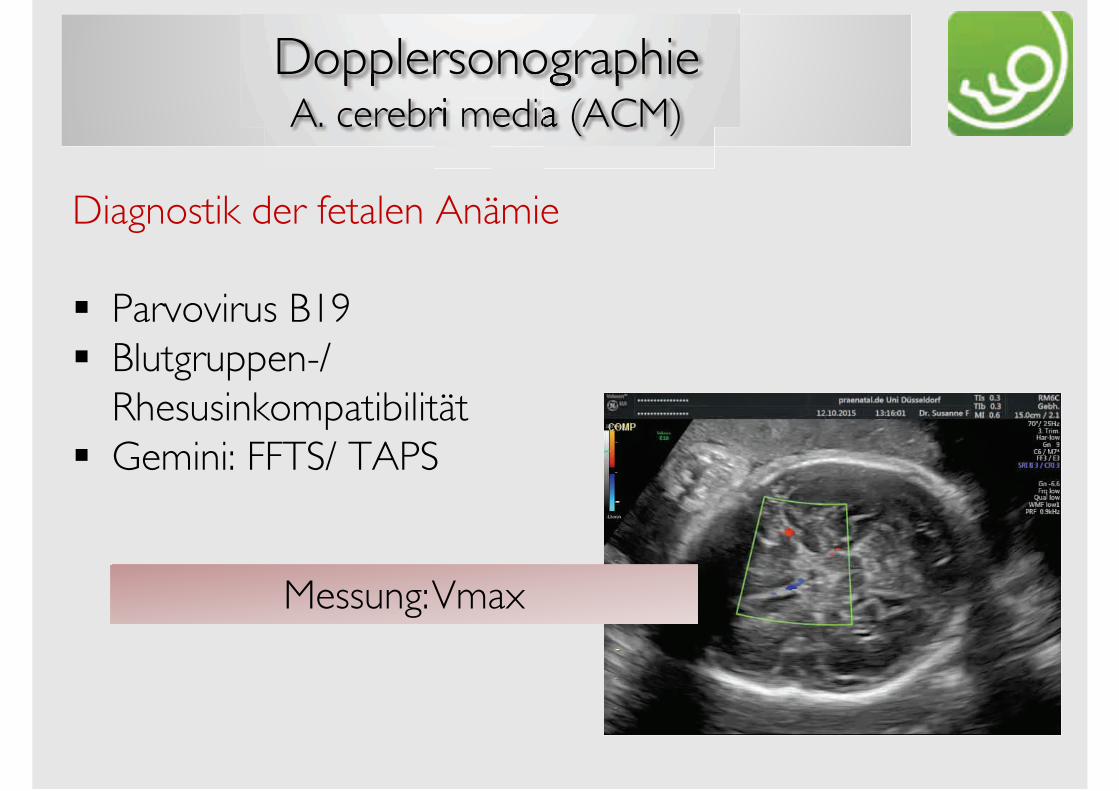
DopplersonographieA. cerebri media (ACM)
Diagnostik der fetalen Anämie
! Parvovirus B19! Blutgruppen-/
Rhesusinkompatibilität! Gemini: FFTS/ TAPS
Messung: Vmax
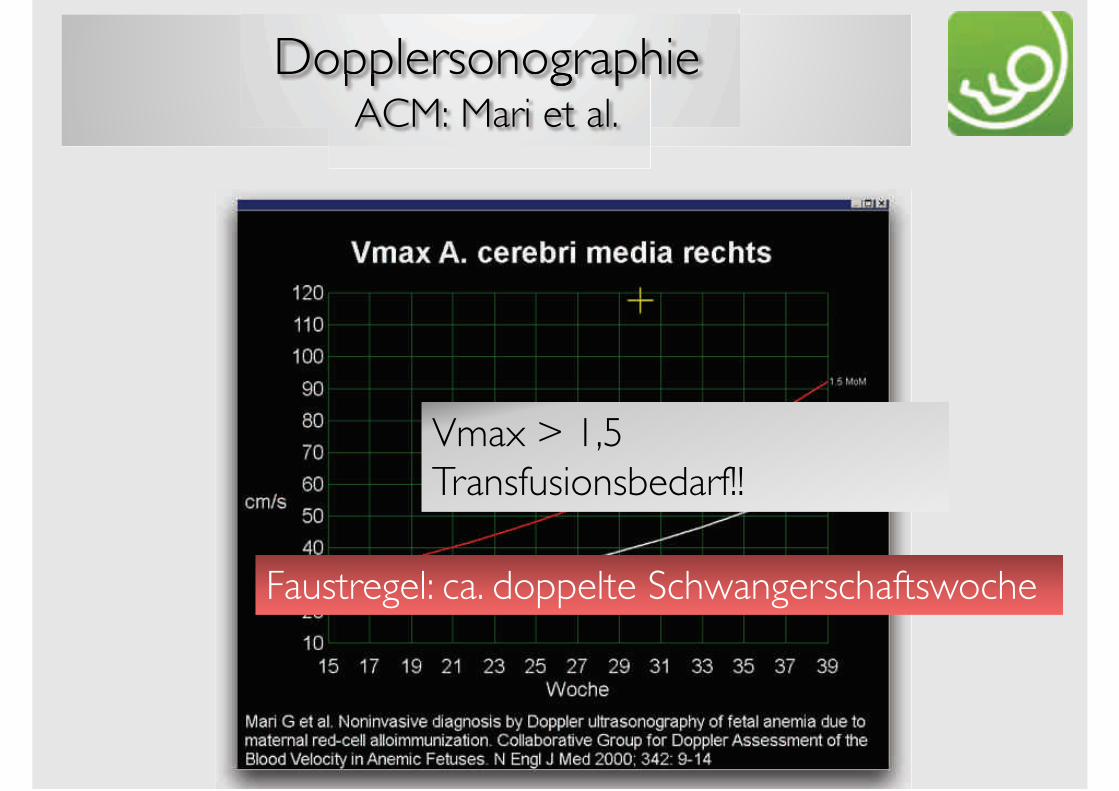
DopplersonographieACM: Mari et al.
Vmax > 1,5 Transfusionsbedarf!!
Faustregel: ca. doppelte Schwangerschaftswoche
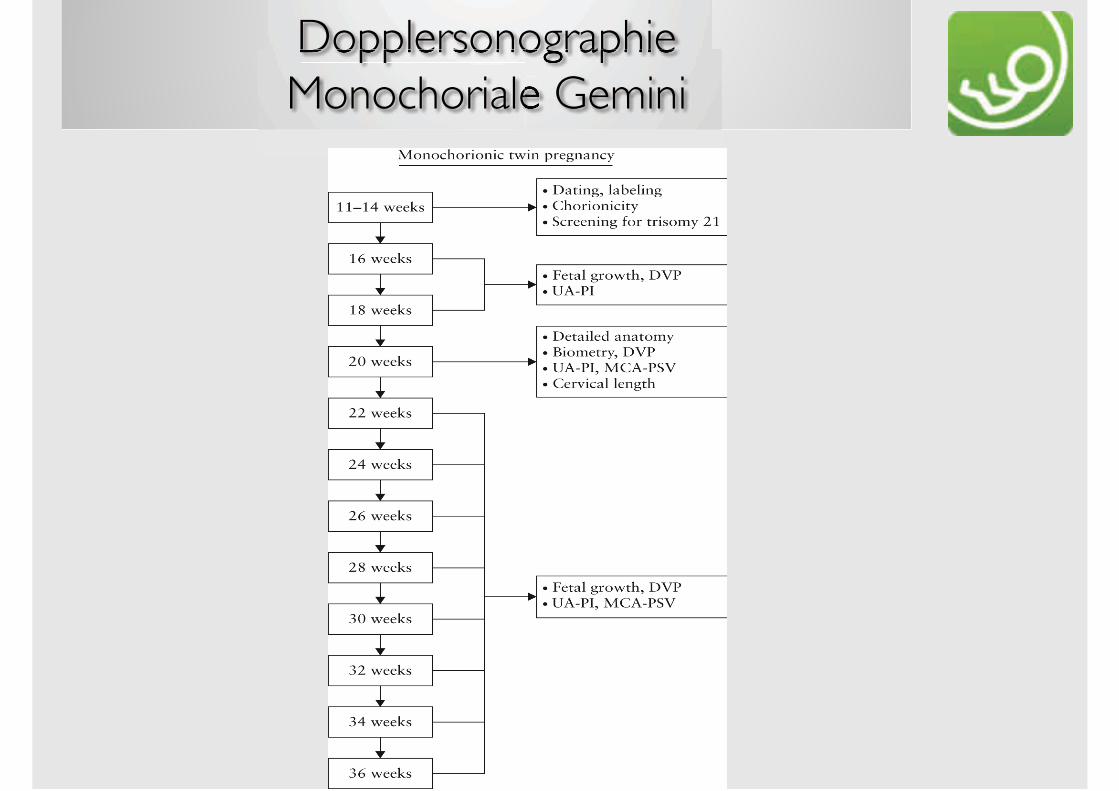
DopplersonographieMonochoriale Gemini
DopplersonographieMonochoriale Gemini
! selektive Wachstumsrestriktion
! Feto-fetale Transfusionssyndrom (TTTS)Rezipient: path.DV, kardiale Dekompensation
Donor: path. A.umbilicalis
! Anämie-Polyzythämie-Sequenz (TAPS)ACM (Anämiediagnostik)
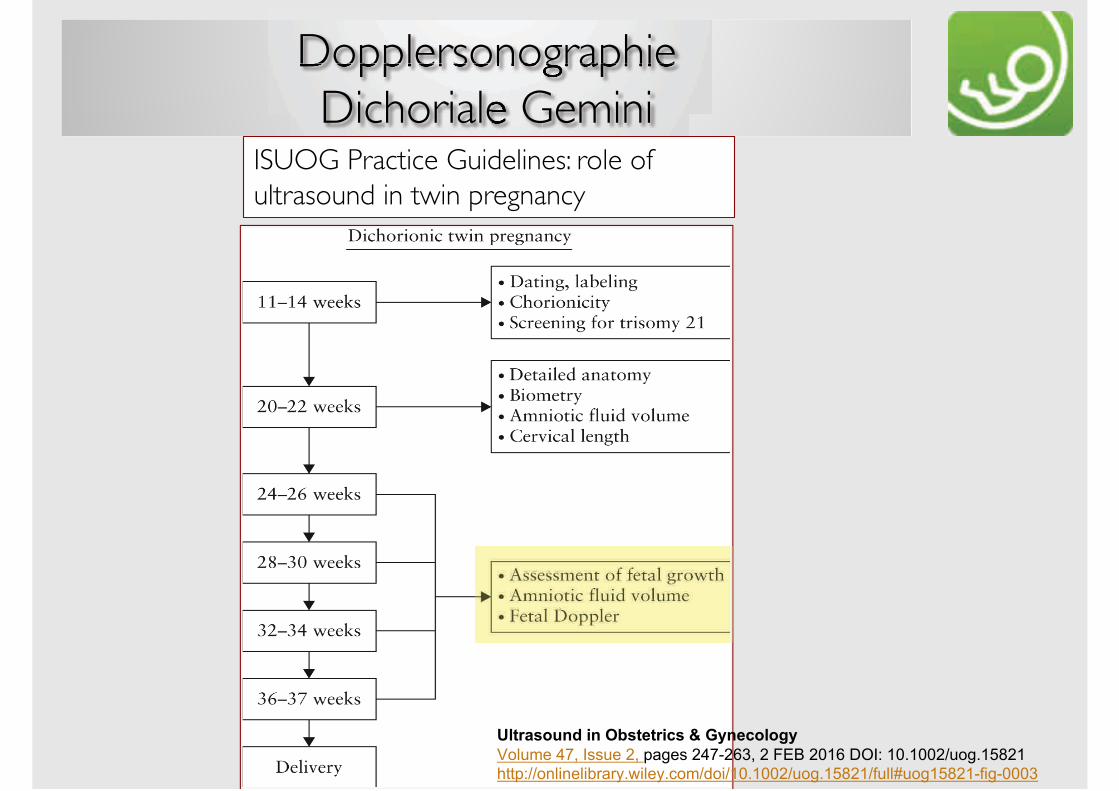
DopplersonographieDichoriale Gemini
ISUOG Practice Guidelines: role ofultrasound in twin pregnancy
!"#$%&'()*+,)+-.&#/#$,0&+1+23)/0'"'43
!"#$%&'()*'+,,$&'-*'./0&,'-()1-23*'-'456'-782'9:+;'87<877-=$"0<8>?-8
@AA.;=="B#CB&#CDE/EF<GC#&F<H"%=I"C=87<877-=$"0<8>?-8=J$##K$"08>?-81JC017773
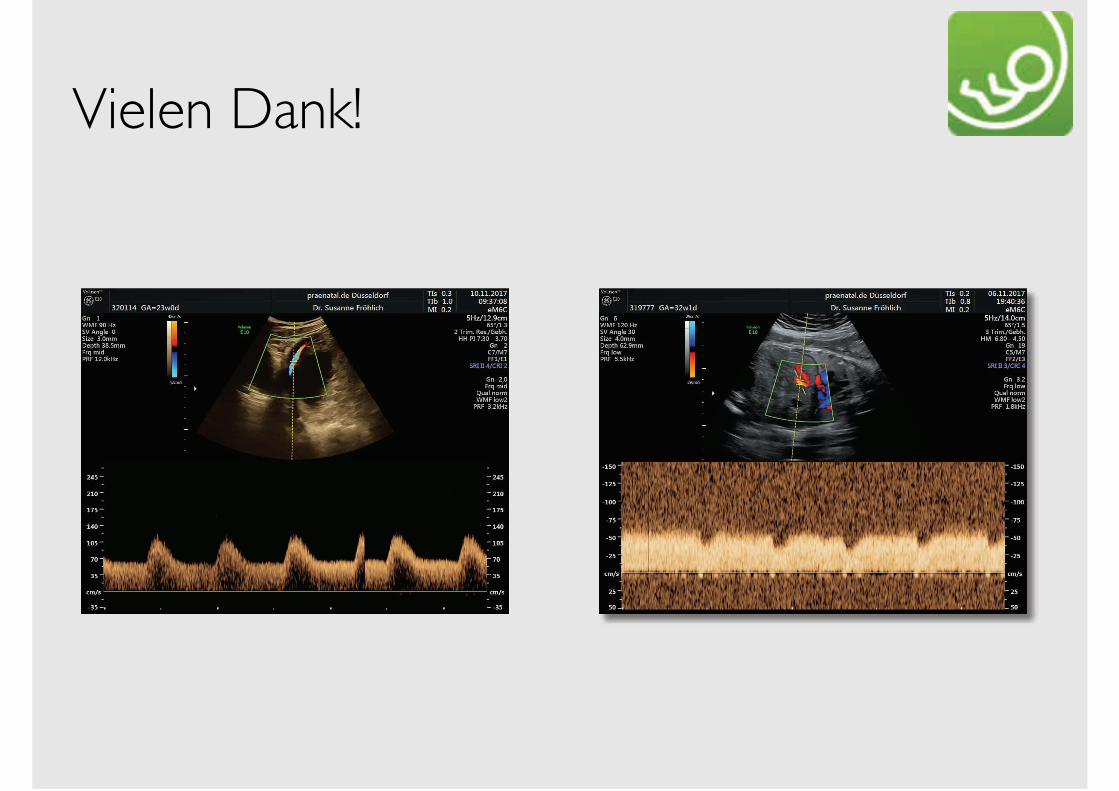
Vielen Dank!
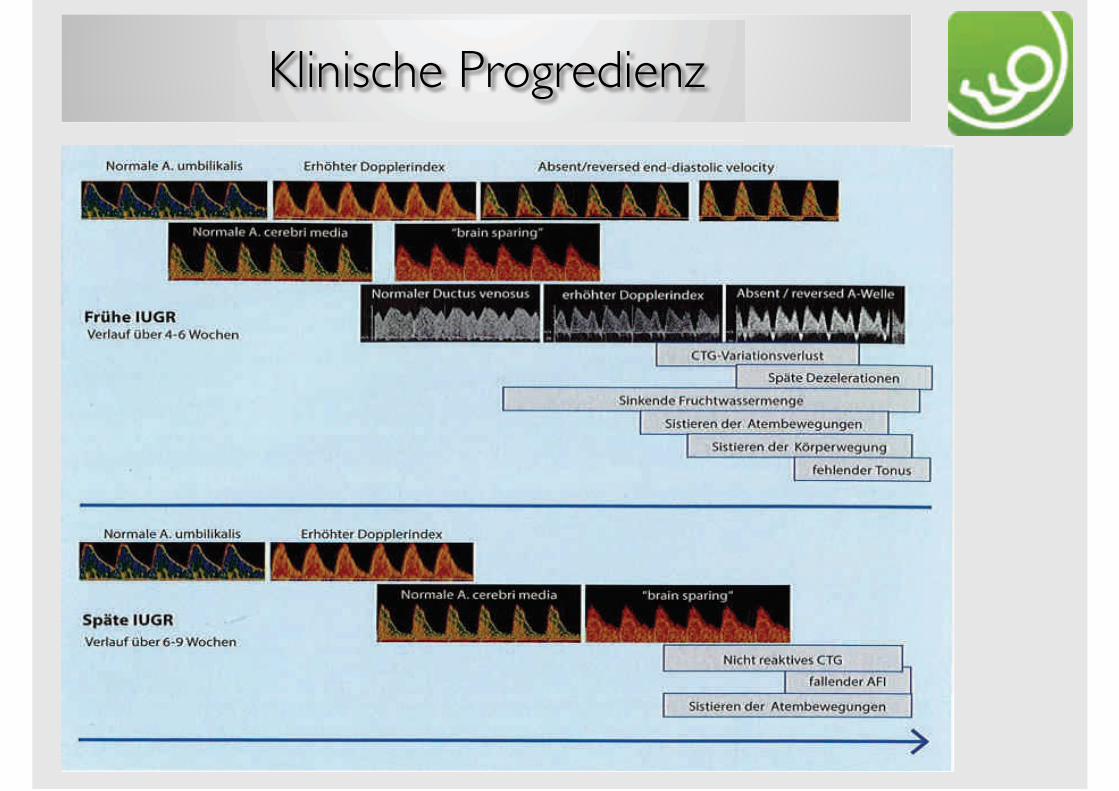
Klinische Progredienz












![V.A. Obrucev - Plutonia [1956]](https://img.pdfslide.tips/doc/110x75/5571fb3249795991699435c7/va-obrucev-plutonia-1956.jpg)









![ExercÃ-cios [2ª V.A.]](https://img.pdfslide.tips/doc/110x75/55cf8ec3550346703b956371/exerca-cios-2aa-va.jpg)

![Exercícios [2ª V.A.] - 2013](https://img.pdfslide.tips/doc/110x75/55cf9b0d550346d033a48ab8/exercicios-2a-va-2013.jpg)


![ExercÃ-cios [1ª V.A.]](https://img.pdfslide.tips/doc/110x75/55cf921e550346f57b93c458/exerca-cios-1aa-va.jpg)

