-
8/2/2019 dor fisiopat
1/12
94 Revista Brasileira de AnestesiologiaVol. 57, No 1,
Janeiro-Fevereiro, 2007
Rev Bras Anestesiol ARTIGO DE REVISO2007; 57: 1: 94-105 REVIEW
ARTICLE
RESUMORocha APC, Kraychete DC,Lemonica L, Carvalho LR, Barros
GAM,Garcia JBS, Sakata RK Dor: Aspectos Atuais da
SensibilizaoPerifrica e Central.
JUSTIFICATIVA E OBJETIVOS:As pesquisas recentes tm foca-lizado a
plasticidade bioqumica e estrutural do sistema nervoso
decorrente da leso tissular. Os mecanismos envolvidos na
tran-
sio da dor aguda para crnica so complexos e envolvem a
interao de sistemas receptores e o fluxo de ons
intracelulares,
sistemas de segundo mensageiro e novas conexes sinpticas. O
objetivo deste artigo foi discutir os novos mecanismos que
envol-
vem a sensibilizao perifrica e central.
CONTEDO:A leso tissular provoca aumento na resposta
dosnociceptores, chamada de sensibilizao ou facilitao. Esses
fe-
nmenos iniciam-se aps a liberao local de mediadores infla-
matrios e a ativao de clulas do sistema imune ou de
receptores
especficos no sistema nervoso perifrico e central.
CONCLUSES:As leses do tecido e dos neurnios resultam
emsensibilizao de nociceptores e facilitao da conduo nervo-
sa central e perifrica.
Unitermos: DOR: mecanismos, sensibilizao perifrica,
sen-sibilizao central.
SUMMARYRocha APC, Kraychete DC, Lemonica L, Carvalho LR, Barros
GAM,Garcia JBS, Sakata RK Pain: Current Aspects on Peripheral
andCentral Sensitization.
BACKGROUND AND OBJECTIVES:Current research has focusedon the
biochemical and structural plasticity of the nervous system
secondary to tissue injury. The mechanisms involved in the
tran-
sition from acute to chronic pain are complex and involve
the
interaction of receptor systems and the flow of intracellular
ions,
second messenger systems, and new synaptic connections. The
aim of this article was to discuss the new mechanisms
concerning
peripheral and central sensitization.
CONTENTS:Tissue injury increases the response of
nociceptors,known as sensitization or facilitation. These phenomena
begin after
the local release of inflammatory mediators and the activation
of the
cells of the immune system or specific receptors in the
peripheral
and central nervous system.
CONCLUSIONS:Tissue and neuronal lesions result in sensitiza-tion
of the nociceptors and facilitation of the central and
peripheral
nervous conduction.
Key Words: PAIN: mechanisms, peripheral sensitization,
centralsensitization.
INTRODUO
Apesar de a Associao Internacional para o Estudo daDor (IASP)
ter definido a dor como uma sensao sub-jet iva relacionada com uma
leso tissular, h evidnciasque essa associao possa no ocorrer. A
cefalia e a dorplvica crnica, por exemplo, parecem existir sem leso
tis-sular detectvel pelos mtodos diagnsticos disponveis naprtica
clnica atual, favorecendo a hiptese de que pode haveralteraes
neurofuncionais restritas ao mbito biomolecular,cuja interao pouco
conhecida entre neuromediadores,neurotransmissores e transdutores
de sinais, em uma rede
de bilhes de sinapses, o que dificulta a compreenso daetiologia
da dor 1. Por outro lado, o trauma e a estimulaodo sistema nervoso
perifrico ou central tambm podem al-terar as respostas imunes. Como
conseqncia, observa-sea ativao de peptdeos e receptores, com
posterior traduodo sinal para o meio intracelular. Nesse contexto,
o avanono conhecimento da neuroanatomia das vias de conduo,da
neurofarmacologia e da fisiopatologia da dor facilita
odesenvolvimento de pesquisas visando a novas modalidadesde
tratamento. Assim, a analgesia efetiva para as sndro-mes dolorosas
ainda um grande desafio.
Dor: Aspectos Atuais da Sensibilizao Perifrica e Central*Pain:
Current Aspects on Peripheral and Central Sensitization
Anita Perptua Carvalho Rocha1, Durval Campos Kraychete,
TSA2,Lino Lemonica, TSA3, Ldia Raquel de Carvalho4,
Guilherme Antnio Moreira de Barros, TSA5, Joo Batista dos Santos
Garcia, TSA6, Rioko Kimiko Sakata, TSA7
*Recebido do (Received from) CET/SBA da Faculdade de Medicina de
Botu-catu da Universidade Estadual de So Paulo (FMB UNESP),
Botucatu, SP
1. Mestre em Anestesiologia pela FMB UNESP; Coordenadora do
Servio
de Dor Aguda do Hospital da Sagrada Famlia
2. Professor Doutor, Disciplina de Anestesiologia da UFBA;
Coordenador do
Ambulatrio de Dor da UFBA
3. Professor Doutor do Departamento de Anestesiologia da FMB
UNESP;
Responsvel pelo Servio de Terapia Antlgica e Cuidados
Paliativos
4. Professor Doutor do Departamento de Bioestatstica do
Instituto de
Biocincias, UNESP
5. Professor Doutor do Departamento de Anestesiologia da FMB
UNESP
6. Professor Doutor da Disciplina de Anes tesiologia,
Universidade Federal do
Maranho; Presidente do Comit de Dor da Sociedade Brasileira
de
Anestesiologia7. Professor Doutor da Disciplina de
Anestesiologia da Universidade Federal
de So Paulo. Coordenador do Setor DOR da UNIFESP
Apresentado (Submitted) em 12 de janeiro de 2006Aceito
(Accepted) para publicao em 07 de setembro de 2006
Endereo para correspondncia (Correspondence to):Dra. Anita
Perptua Carvalho Rocha
Rua Pacfico Pereira, 457/404
Garcia
40100170 - Salvador-BA
E-mail: [email protected]
Sociedade Brasileira de Anestesiologia, 2007
-
8/2/2019 dor fisiopat
2/12
Revista Brasileira de Anestesiologia 95Vol. 57, No 1,
Janeiro-Fevereiro, 2007
No Brasil 2 e em outros pases 3,4, 10% a 50% dos indivdu-os
procuram clnicas-gerais por causa da dor 5-8. A dor estpresente em
mais de 70% dos pacientes que buscam osconsultrios brasileiros por
motivos diversos, sendo a razode consultas mdicas em um tero dos
casos. Esse argu-mento enfatiza a importncia da busca de elementos
que
permitam uma melhor abordagem da dor aguda e crnica.O objetivo
desta reviso foi discutir a fisiopatologia da dor,enfatizando os
mecanismos perifricos e centrais da trans-misso dolorosa.
MECANISMOS PERIFRICOS DA DOR
O primeiro passo na seqncia dos eventos que originamo fenmeno
doloroso a transformao dos estmulos agres-sivos em potenciais de ao
que, das fibras nervosas peri-fricas, so transferidos para o
sistema nervoso central 9.Os receptores especficos para a dor esto
localizados nas
terminaes de fibras nervosas A e C
10,11
e, quando ati-vados, sofrem alteraes na sua membrana, permitindo
adeflagrao de potenciais de ao.As terminaes nervosas das fibras
nociceptivas A e C (no-ciceptores) so capazes de traduzir um
estmulo agressivode natureza trmica, qumica ou mecnica, em estmulo
el-trico que ser transmitido at o sistema nervoso central
einterpretado no crtex cerebral como dor. As fibras A
somielinizadas e as fibras C no so mielinizadas e possuema
capacidade de transmitir estmulos dolorosos em diferen-tes
velocidades. As fibras A, em funo da presena da bai-nha de mielina,
transmitem o estmulo doloroso de formarpida, enquanto as fibras C
so responsveis pela trans-
misso lenta da dor. Ambas so classificadas em subtiposA1, A2, C1
e C2 (Tabela I). O tipo de fibra nociceptiva pa-rece estar
envolvido com alteraes perifricas distintas nas
diversas sndromes dolorosas, e poder, no futuro, contri-buir
para o tratamento mais eficaz da dor.Os nociceptores, ento, so
sensibilizados pela ao desubstncias qumicas, denominadas
algiognicas, presentesno ambiente tissular 12: acetilcolina,
bradicinina, histamina,serotonina, leucotrieno, substncia P, fator
de ativao
plaquetrio, radicais cidos, ons potssio,
prostaglandinas,tromboxana, interleucinas, fator de necrose tumoral
(TNF),fator de crescimento nervoso (NGF) e monofosfato cclico
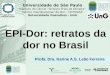
deadenosina (AMPc) 13-15 (Figura 1).Quando o estmulo provoca a leso
tecidual, h o desenca-deamento de processo inflamatrio seguido de
reparao.As clulas lesadas liberam enzimas de seu interior, que
noambiente extracelular degradam cidos graxos de cadeialonga e
atuam sobre os cininognios, dando origem for-mao de cininas. As
cininas so pequenos polipeptdeosda
2-calicrena presente no plasma ou nos lquidos org-
nicos. A calicrena uma enzima proteoltica que ativada
pela inflamao e outros efeitos qumicos ou fsicos sobreo sangue
ou os tecidos. Ao ser ativada, a calicrena atuaimediatamente sobre
a 2-globulina, liberando a cinina de-nominada calidina, que ,
assim, convertida em bradicininapor enzimas teciduais. Uma vez
formada, a bradicinina pro-voca intensa dilatao arteriolar e
aumento da permea-bilidade capilar, contribuindo para a propagao da
reaoinflamatria 16.Tambm, a ao da fosfolipase A na membrana celular
pro-voca a liberao de cido araquidnico. Este metabolizadopor trs
sistemas enzimticos principais: a cicloxigenase,de cuja atuao
obtm-se as prostaglandinas, os trom-boxanos e as prostaciclinas; a
lipoxigenase, que provoca a
produo de leucotrienos e lipoxinas; e o citocromo P-450,que
origina os denominados produtos da via da epoxige-
Tabela I Subtipos das Fibras Nervosas A e C
Tipo de Fibra Caractersticas
Fibras A tipo I Respondem a tem peratura em torno de52C, so
insensveis a capsaicina epossuem resposta mediada pelosreceptores
VRL-1
Fibras A tipo II So sensveis a temperatura em torno de
43C, a capsaicina e ativam, via receptoresVR1, canais catinicos
no-seletivospermeveis ao clcio
Fibras C tipo I Contm substncia P e CGRP e expressamreceptores
tirocinase A, para o fator decrescimento nervoso. So responsivas
acapsaicina e a prtons
Fibras C tipo II Expressam receptores purinrgicos P2X3
para adenosina e um grupo de carboidratosde superfcie, a
-D-galactose, capaz dese ligar a lecitina IB-4,
sensveisseletivamente a prtons
Membranacelular
Bradicinina
Leso
Acetilcolina
HistaminaEnzimasH+
TNF-K+
Substncia PSerotonina
ProstaglandinasSubstnciasalgiognicas
Figura 1 Liberao de Substncias Algiognicas aps a
LesoTecidual
DOR: ASPECTOS ATUAIS DA SENSIBILIZAO PERIFRICA E CENTRAL
-
8/2/2019 dor fisiopat
3/12
96 Revista Brasileira de AnestesiologiaVol. 57, No 1,
Janeiro-Fevereiro, 2007
nase. Essas substncias, sobretudo as prostaglandinas E2
(PGE2), promovem diminuio do limiar de excitabilidadedos
nociceptores 17.Do mesmo modo, clulas inflamatrias, macrfagos e
leu-ccitos liberam citocinas que vo contribuir para a migraode
novas clulas para o local da leso. H produo e libe-
rao de interleucina-1 e 6, fator de necrose tumoral, selec-tina,
fatores quimiotticos, xido ntrico e substnciasoxidantes. Novos
receptores, ento, so recrutados e pas-sam a fazer parte do processo
inflamatrio. A substncia Pe a neurocinina A produzem vasodilatao e
aumento dapermeabilidade vascular, contribuindo tambm para a
ma-nuteno do processo inflamatrio 18.A bradicinina, a
prostaglandina E2, o fator de crescimento ner-voso (NGF) e as
interleucinas, contudo, parecem exercer pa-pel fundamental na
nocicepo perifrica. A prostaglandinae a bradicinina causam alteraes
em receptores especfi-cos (TRPV1) acoplados a canais inicos
ligante-dependentevia ativao do AMPc, e das protenas cinases A
(PKA) e C(PKC), reduzindo o tempo ps-hiperpolarizao da membra-na
neural, causando reduo do limiar para disparo da fibranervosa.As
neurotrofinas aumentam a sntese, o transporte axonalantergrado e
quantidade de SP e CGRP nas fibras C tipo 1e reduzem a atividade do
cido gama-aminobutrico (GABA),tanto nas terminaes nervosas
perifricas quanto nas cen-trais. Ao lado disso, provocam mudanas
nos receptoresvanilides (VR1) de fibras A acoplados a canais inicos
ligan-te-dependente e acionam as protenas cinases ativadas
pormitgenos (MAPK) que podem fosforilar o AMPc e iniciar atranscrio
gentica responsvel por alteraes fenotpicas, as
quais contribuem para a amplificao da eficcia sinptica.A
persistncia da agresso causa modificaes no sistemanervoso perifrico
e sensibilizao de fibras nervosas, comconseqente hiperalgesia e
aumento dos nveis de AMPc eclcio nos nociceptores. Esse fenmeno
ocorre por aodos mediadores inflamatrios e conseqente atividade
es-pontnea dos neurnios, aumento da resposta a
estmulossupraliminares e diminuio do limiar de ativao dos
noci-ceptores 18-20. Um tipo particular de nociceptor referidocomo
nociceptor silente, o qual ativado aps inflamaoou depois de ter
ocorrido leso tissular. As estimativas sode que 40% das fibras C e
30% das fibras A contribuemcom nociceptores silentes. Aps a liberao
dos produtosqumicos da leso, esses receptores previamente
silencio-sos so ativados por estmulos trmicos e mecnicos e
de-senvolvem descargas espontneas, tornando-se capazesde responder
de maneira intensa a estmulos nociceptivose no-nociceptivos 21-22
(Figura 2).Em resumo, a agresso tecidual resulta na acumulao
demetablitos do cido araquidnico. A produo de prosta-glandinas e de
leucotrienos leva a degranulao de mas-tcitos e a ativao direta de
fibras nervosas, macrfagos elinfcitos. H liberao de mediadores,
como potssio,serotonina, substncia P, histamina e cininas. Ocorrem
al-
teraes na permeabilidade vascular, no fluxo sangneolocal e
produo dos sinais clssicos inflamatrios de ru-bor, calor, dor,
tumor e impotncia funcional. Tem incio o pro-cesso de sensibilizao
perifrica com conseqenteexacerbao da resposta ao estmulo doloroso
20-22.Os neuromediadores perifricos levam a despolarizao damembrana
neural por tempo prolongado, com conseqenteaumento da condutividade
dos canais de sdio e clcio e re-duo do influxo de potssio e cloro
para o meio intracelular.
Os canais de sdio esto envolvidos na gnese da
hiperex-citabilidade neuronal e podem estar e podem ser
classifi-cados em dois grandes grupos: os sensveis
tetrodotoxina(TTXs), que esto presentes nas fibras A, em todo
sistemanervoso e no gnglio da raiz dorsal; e os resistentes
tetro-dotoxina (TTXr), que so encontrados especialmente nas fi-bras
C do gnglio da raiz dorsal 23.Apesar de a leso perifrica da fibra
nervosa tipo C provo-car reduo no corno dorsal da medula espinhal
de SP, deneurotrofinas (BDNF), de receptores (VR1 e P2X3), de
canaisde clcio tipo N de alta voltagem, h regulao ascendentede
canais TTXs tipo III e existe a translocao do corpo ce-lular para o
neuroma de canais de sdio (TTXr), facilitandoo aumento da
excitabilidade nervosa 24. O exposto aconte-ce caso a fibra nervosa
esteja intacta (inflamao), ou seja,existe um aumento de
neuromediadores excitatrios no cor-no dorsal da medula espinhal e
uma maior expresso decanais de sdio (TTXr), fato que facilita a
hiperexcitabilidadeneuronal e dificulta a resposta ao tratamento
com anest-sicos locais 24.Tambm pode haver em ambas as situaes
descritas, so-bretudo na leso de fibras C, aumento de SP e BDNF
nasfibras A (mecanorreceptores de baixo limiar), assim
comobrotamento dessas no local das conexes aferentes das fi-
Figura 2 Processo de Sensibilizao Perifrica
EstmuloLiberao deSubstnciaAlgognica
DOR- Reduo do limiar paraa dor dos nociceptores
j ativos- Ativao de nocicepto-res silentes
ROCHA, KRAYCHETE, LEMONICA E COL.
-
8/2/2019 dor fisiopat
4/12
Revista Brasileira de Anestesiologia 97Vol. 57, No 1,
Janeiro-Fevereiro, 2007
bras C (lmina II), ampliando o campo receptivo do neurnioe
facilitando a interpretao de estmulos mecnicos peri-fricos incuos
como agressivos 25. Isso explica, por exemplo,a alodinia mecnica
que acontece na neuralgia ps-herp-tica 26. Outra possibilidade
seria a do brotamento de axnionoradrenrgico simptico no gnglio da
raiz dorsal, ao re-
dor de neurnios de dimetro largo (fibras A), sugerindo ahiptese
da ativao de fibras aferentes sensitivas aps aestimulao simptica
27. Alm disso, pode existir algumadesproporo entre as vias
excitatrias e as de supressoda dor, com reduo da atividade
inibitria da glicina, daGABA e dos opiides 24.
MECANISMOS CENTRAIS DA DOR
A transmisso dos estmulos nocivos atravs da medulaespinhal no um
processo passivo. Os circuitos intrame-dulares tm a capacidade de
alterar o estmulo e a conse-qente resposta dolorosa. A interao
entre esses circuitosmedulares determinar as mensagens que atingiro
ocrtex cerebral 21.Estudos clnicos e experimentais tm demonstrado
que es-tmulos nocivos provocam alteraes no sistema nervosocentral,
modificando os mecanismos desencadeados pelosestmulos aferentes. A
estimulao persistente de nocicep-tores provoca dor espontnea, reduo
do limiar de sensi-bilidade e hiperalgesia. Esta pode ser
classificada comohiperalgesia primria e secundria. A hiperalgesia
primria conceituada como sendo o aumento da resposta ao est-mulo
doloroso no local da leso, enquanto a hiperalgesiasecundria aquela
que se estende para reas adjacentes.
A presena de todos esses elementos sugere que a sen-sibilizao
perifrica no o nico fenmeno responsvelpor todas essas mudanas e que
deve haver envolvimentodo sistema nervoso central neste processo
21,28,29.A sensibilizao central implica alteraes dos
impulsosperifricos, com adaptaes positivas ou negativas.
Ocorrereduo do limiar ou aumento da resposta aos impulsosaferentes,
descargas persistentes aps estmulos repetidose ampliao dos campos
receptivos de neurnios do cornodorsal.Impulsos repetidos em fibras
C amplificam sinais sensoriaisem neurnios espinhais, enviando
mensagens para o en-cfalo 13. Leses perifricas induzem plasticidade
em estru-turas supra-espinhais por meio de mecanismos queenvolvem
tipos especficos de receptores para o glutamato.Aps a agresso
tecidual h liberao de neurotransmis-sores, como substncia P,
somatotastina, peptdeo gene-ticamente relacionado com a
calcitonina, neurocinina-A,glutamato e aspartato. Essas substncias
esto relacionadascom a ativao de potenciais ps-sinpticos
excitatrios edos receptores N-metil-D-aspartato (NMDA) e
no-NMDA.Estmulos freqentes dos aferentes geram a somao
dospotenciais de ao e conseqente despolarizao ps-sinpticas
cumulativa. Depois da ativao de receptores
NMDA pelo glutamato h remoo do on magnsio do in-terior do
receptor e o influxo de clcio para a clula, do queresulta a
amplificao e o prolongamento da resposta aoimpulso doloroso 30,31.O
aumento do clcio tem como conseqncia a ativao daenzima xido
ntrico-sintetase e a estimulao da transcri-
o de protoncogenes. Estes so genes localizados no sis-tema
nervoso central e esto envolvidos na formao dedinorfinas e
encefalinas. As encefalinas tm ao antinoci-ceptiva e esto
envolvidas no processo de reduo da neu-roplasticidade e
hiperalgesia. Entretanto, as dinorfinas tmum efeito complexo, j que
possuem ao algognica eantinociceptiva 32,33.Estudos recentes tm
sugerido que a ativao do c-fose c-junpromove a transcrio de RNA
mensageiro responsvelpela sntese de protenas fundamentais, as quais
esto en-volvidas na alterao da expresso fenotpica e,
conseqen-temente, na perpetuao da hipersensibilidade neuronal
28,33
(Figura 3).A sensibilizao do corno dorsal da medula espinhal
podeser de diferentes modalidades: wind up, sensibilizao sinp-tica
clssica, potencializao de longo termo, fase tardia dapotenciao de
longo termo e facilitao de longo termo 34.A sensibilizao sinptica
clssica causada por uma se-qncia sincronizada de estmulos
perifricos nociceptivosrepetidos por uma nica estimulao nociceptiva
assncrona,aumentando a resposta de aferentes de fibras A e C
(poten-cializao homossinptica) e de aferentes de fibras A
no-es-timulados (potenciao heterossinptica). Isto conseqnciada
liberao de aminocidos excitatrios, peptdeos e deneurotrofinas no
corno dorsal da medula espinhal 35.
Os aminocidos excitatrios so representados pelo gluta-mato e
pelo aspartato e se ligam a receptores especficosdo tipo ionotrpico
ou metabotrpico. Os receptores ionotr-picos, ou receptores rpidos,
so aqueles nos quais o lo-cal de ligao do neurotransmissor parte
integrante deum canal inico, enquanto os receptores metabotrpicos
oureceptores lentos so ligados protena G. Dentre os recep-tores
para os aminocidos excitatrios destacam-se oAMPA, o cainato e o
N-metil-D-aspartato (NMDA), que soionotrpicos, e o receptor Mrglu,
que tem a sua ao me-diada pela protena G, sendo portanto um
receptor metabo-trpico. Os peptdeos, a substncia P e o
peptdeogeneticamente relacionado com a calcitonica (CGRP) ligam-se
as neurocininas do tipo NK-1 e NK-2, enquanto asneurotrofinas
possuem como receptores as tirocinases tipoA e B (trkA, trkB).Aps a
liberao de aminocidos excitatrios, peptdeos eneurotrofinas e sua
interao com receptores especficos,h a ativao de segundos
mensageiros, do tipo AMPc, PKA,PKC, fosfotidilinositol, fosfolipase
C, fosfolipase A2.. Isto pro-move a abertura de canais de clcio, e,
conseqentemen-te, a produo de prostaglandinas e xido ntrico.
Estesmigram do intracelular em direo fenda sinptica e cau-sam a
liberao de glutamato, aspartato, substncia P e
DOR: ASPECTOS ATUAIS DA SENSIBILIZAO PERIFRICA E CENTRAL
-
8/2/2019 dor fisiopat
5/12
98 Revista Brasileira de AnestesiologiaVol. 57, No 1,
Janeiro-Fevereiro, 2007
CGRP, contribuindo para a ampliao do processo lgico 34.O wind up
o resultado da somao de potenciais sinp-ticos lentos aps estimulao
aferente repetida de baixafreqncia, inferior a 5 Hz, e por tempo
prolongado. Isto es-timula a liberao de neurotransmissores
excitatrios,glutamato e aspartato, no corno dorsal da medula
espinhale produz a despolarizao relacionada com a remoo dobloqueio
voltagem-dependente exercido pelo magnsio nosreceptores NMDA.
Ocorre, ento, aumento da condutividadeao clcio e a resposta dor, a
cada estmulo repetido e damesma intensidade 36.
A potencializao de longo termo, embora mais estudada nohipocampo
e nas reas corticais, pode ser decorrente de se-qncia de estmulos
nociceptivos breves e de alta freqn-cia. Isso provocaria a ativao
de receptores AMPA e NK1 e decanais de clcio, ocorrendo resposta
ps-sinptica prolonga-da e excitatria, sobretudo em neurnios da
lmina I 37.Os mecanismos que contribuem para o aumento da efic-cia
da transmisso sinptica seriam decorrentes da fosfo-rilao dos
receptores de membrana e das alteraes dotempo de abertura dos
canais inicos, ou da formao e dotransporte de substncias
excitatrias do interior da clula
Figura 3 Seqncia de Eventos que Levam a Sensibilizao dos
Neurnios do Corno Dorsal aps Estimulao Nociceptiva Intensa
eContinuada. Ativao intensa de neurnios aferentes primrios estimula
a liberao de glutamato (Glu) e substncia P (SP). O receptorNMDA, em
funo do papel do magnsio (Mg2+), inicialmente no-responsivo ao Glu;
mas seguindo a despolarizao do receptor AMPApelo Glu no receptor
metabotrpico estimula a ativao de fosfolipase C (PLC) mediada pela
protena G, levando a hidrlise e transformaodo 4,5-bifosfato de
fosfatidilinositol (PIP
2) em trifosfato de inositol (IP
3) e diacilglicerol (DAG). O DAG estimula a produo de protena
cinase
C (PKC), a qual ativada na presena de elevados nveis de clcio
(Ca 2+) intracelular. IP3estimula a liberao de clcio intracelular
de
estoques intracelulares no retculo sarcoplasmtico. PKC aumentada
induz o sustentado aumento da permeabilidade da membrana e,
emconjuno com o aumento do Ca2+ intracelular, leva ao aumento da
expresso de protoncogenes, como c-fose c-jun. As protenasproduzidas
por esses protoncogenes codificam neuropeptdeos como as encefalinas
(EKN), dinorfinas (DYN) e taquicininas (TK). Esseaumento tambm leva
a ativao de fosfolipase A
2(PLA
2) e a ativao da sntese de xido ntrico (NOS) por um mecanismo
clcio-
calmodulina dependente. PLA2
catalisa a converso de fosfatidilcolina (PC) para prostaglandina
(PG), tromboxano (TX) e pela lipoxigenase(LO) para produzir
leucotrienos (LT). NOS catalisa a produo de protena cinase e
alteraes na expresso gentica. NO difunde-sedo interior da clula
para o terminal do aferente primrio, onde aumenta a liberao de
glutamato.
Interneurnioinibitrio (?)
Efeitosextracelulares (?)
GC
NO cGMP
SP SP Glu
GluGluSP
NK1 NMDA AMPANa
K+
Na
K+
Metabotrpico
PLCPIP2PLA2A A
PC
CO LO
LTTX, PG
CAM
CAM
PK
NOS
NO
Efeitos
intracelulares (?)
GC-cGMP
L-CI
L-Arg
Ca++
c-fosc-jun
DINENC
IP3
Ca++
Retculo endoplasmtico
IP3DAG
PKC
O2
ROCHA, KRAYCHETE, LEMONICA E COL.
-
8/2/2019 dor fisiopat
6/12
Revista Brasileira de Anestesiologia 99Vol. 57, No 1,
Janeiro-Fevereiro, 2007
para a fenda sinptica. Alm disso, no corno dorsal da me-dula
espinhal, as proteinocinases ativadas por mitgenos(MAPK) modulam a
fosforilao dos receptores NMDA eAMPA, amplificando a resposta
nociceptiva 38.A facilitao de longo termo envolve a ativao de
fatores detranscrio e alteraes na transcrio. Os fatores de
trans-
crio modulam a relao entre o complexo receptor-neuromediador e
as alteraes na expresso gnica 39.O estmulo nociceptivo aciona a
mesma cascata de recepto-res e segundo mensageiros descritos para a
sensibilizaosinptica clssica; contudo, tambm provoca a expresso
degenes de formao imediata c-fos (B,C,D), c-jun, de enzimasCOX-2 e
de genes de resposta lenta que codificam a pr-dinorfina, o receptor
NK1 e a trkB no corno dorsal da medu-la espinhal. Ocorre regulao
ascendente das vias parasntese de citocinas, quimiocinas e molculas
de adeso.Assim, h mudana fenotpica no gnglio da raiz dorsal 40.
RESPOSTAS SEGMENTARES E SUPRA-SEGMENTARES DOR
As fibras nociceptivas cruzam a linha mdia no nvel do
cornodorsal da medula espinhal e ascendem pelos tratos
espi-notalmicos, espinorreticular, espinomesenceflico, colunadorsal
ps-sinptica e sistema espinopontoamigdaliano.Algumas dessas fibras
terminam no ncleo talmicoventroposteromedial (VPM) e depois
ascendem para o crtexcerebral somestsico (S1 e S2), crtex insular e
cingularanterior. Outros neurnios projetam axnios para o
hipot-lamo, formao reticular, substncia cinzenta
periaquedutal,ncleo medial e intratalmico, e estruturas enceflicas
an-
teriores que so responsveis pelas respostas neuroen-dcrinas e
emocionais a dor 41.A ativao de fibras nociceptivas perifricas
provoca migra-o retrgrada de fator de crescimento nervoso (NGF)
paraa medula espinhal e induz resposta segmentar reflexa,
comtransporte antergrado de substncia P para a
periferia,ocasionando vasodilatao, aumento da
permeabilidadevascular, atrao de clulas do sistema imune para o
localda leso e degranulao de mastcitos com liberao dediversos
neuromediadores. Desse modo, a substncia Pajuda na manuteno e na
expanso do processo inflama-trio para o campo receptivo de fibras
nervosas adjacentes rea lesada, constituindo a hiperalgesia
secundria 42.Por outro lado, as fibras adrenrgicas, alm de
contriburemcom o processo supracitado, aumentam a sensibilidade
defibras nociceptivas ao de bradicinina. Potencializam es-ses
efeitos, o vasoespasmo e o espasmo muscular, reflexosque
proporcionam liberao de radicais cidos e, conse-qentemente, a reduo
do limiar para disparos da fibranociceptiva 43.Do ponto de vista da
resposta supra-segmentar, a pessoacom dor crnica parece apresentar
possvel inabilidade deaumentar a secreo de hormnios do eixo
hipotlamo-hipofisrio e adrenal ou amplificando a resposta
simptica
ao lidar com o estresse fsico e emocional. Isso repercutenos
nveis de secreo do cortisol, da adrenalina, da nora-drenalina, do
hormnio do crescimento (GH), dos tireoidianose dos gonadais,
tornando o sistema de defesa hipoativo.Esse modelo tenta explicar a
fibromialgia ou a dor miofascial;nessas doenas, possvel que acontea
aumento da se-
creo hipotalmica de CRH com regulao descendentedos receptores na
hipfise, nveis elevados de ACTH e bai-xos de cortisol, e resistncia
perifrica a ao do cortisol 44.O eixo hipotlamo-hipofisrio parece
interagir, ento, com oprocesso doloroso em vrios nveis ou estgios.
A ausn-cia de glicocorticide pode: 1) diminuir a converso
doglutamato, neurotransmissor excitatrio, para glutamina,aumentando
a neurotoxicidade do glutamato no sistemanervoso central; 2)
aumentar a produo de fator de cresci-mento nervoso (NGF) e da
substncia P; e 3) aumento daproduo de citocinas e, conseqentemente,
de NGF 45.A leso do tecido e do neurnio resulta em sensibilizao
de nociceptores e facilitao da conduo nervosa perifri-ca e
central. O estudo desses mecanismos poder elucidarem um futuro
prximo meios para o diagnstico e o trata-mento de sndromes
dolorosas agudas e crnicas.
Pain: Current Aspects on Peripheraland Central Sensitization
Anita Perptua Carvalho Rocha, M.D.; Durval CamposKraychete, TSA,
M.D.;Lino Lemonica, TSA, M.D.; Ldia Raquelde Carvalho, M.D.;
Guilherme Antnio Moreira de Barros,TSA, M.D.; Joo Batista dos
Santos Garcia, TSA, M.D.; RiokoKimiko Sakata, TSA, M.D.
INTRODUCTION
Although the International Association for the Study of
Pain(IASP) defined pain as a subjective sensation related totissue
injury, there is evidence that this association mightnot occur.
Headache and chronic pelvic pain, for example,seem to exist without
tissue damage that can be detected bythe diagnostic methods
currently available, favoring thehypothesis that there can be
neurofunctional changes res-
tricted to the biomolecular level, with the little known
inte-raction among neuromediators, neurotransmitters, andsignal
transducers in a network of billion of synapses, ma-king it
difficult to understand the etiology of pain 1. On theother hand,
trauma and stimulation of the peripheral or cen-tral nervous system
can also change immune responses. Asa consequence, peptides and
receptors are activated,followed by the translation of the signal
to the intracellularenvironment. In this context, advances in the
knowledge ofthe neuranatomy of conduction pathways,
neuropharma-cology, and pathophysiology of pain facilitate the
development
PAIN: CURRENT ASPECTS ON PERIPHERAL AND CENTRAL
SENSITIZATION
-
8/2/2019 dor fisiopat
7/12
100 Revista Brasileira de AnestesiologiaVol. 57, No 1,
Janeiro-Fevereiro, 2007
of research on new treatment modalities. Thus,
effectiveanalgesia for painful syndromes is still a great
challenge.In Brazil 2 and in other countries 3,4, 10% to 50% of the
peopleseek clinics to treat their pain 5-8. In Brazil, pain is
present inover 70% of the patients who seek medical attention
forseveral reasons, and is the main reason for the medical
visit
in one third of the cases. This argument stresses the
impor-tance of searching for elements that could lead to a
betterapproach of acute and chronic pain.The aim of this review was
to discuss the pathophysiologyof pain, emphasizing the peripheral
and central mechanismsof pain transmission.
PERIPHERAL PAIN MECHANISMS
The first step on the sequence of events that originate
thepainful phenomenon is the transformation of aggressivestimuli in
action potentials that are transmitted from the
peripheral nerve fibers to the central nervous system9
.Specific pain receptors are located at the nerve endings ofA
and C nerve fibers 10,11 and, when they are activated, thereare
changes in their membranes, allowing the deflagrationof the action
potentials.Nerve endings of nociceptive A and C fibers
(nociceptors)are capable to translate an aggressive thermic,
chemical, ormechanical stimulus into an electrical stimulus that
will betransmitted to the central nervous system and interpreted
inthe cerebral cortex as pain. The A fibers are myelinated whileC
fibers are non-myelinated; therefore, they are capable
oftransmitting painful stimuli at different speeds. Due to
thepresence of the myelin shaft, A fibers transmit the painful
stimulus fast, while C fibers are responsible for the
slowtransmission of pain. Both are classified as subtypes A1,A2,
C1, and C2 (Table I). The type of nociceptive fiber seems
to be related to distinct peripheral changes on the
differentpainful syndromes and could, in the future, contribute for
amore effective pain treatment.The nociceptors are then sensitized
by the action of chemicalsubstances, known as angiogenic, present
in the tissue envi-ronment 12: acetylcholine, bradykinin,
histamine, serotonin,
leukotriene, substance P, platelet activating factor, acid
ra-dicals, potassium ions, prostaglandins, thromboxane,
inter-leukins, tumor necrosis factor (TNF), nerve growth
factor(NGF), and cyclic adenosine monophosphate (cAMP) 13-15
(Fi-gure 1).When the stimulus causes tissue injury, the
inflammatoryprocess is triggered, which is followed by repair.
Damagedcells release their enzymes that, once in the
extracellularenvironment, degrade long chain fatty acids and act on
kini-nogens, originating the kinins. Kinins are small
polypeptidesof
2-calicrein present in the plasma or body fluids. Kallikrein
is a proteolytic enzyme activated by inflammation and other
chemical or physical effects on blood or tissues. Onceactivated,
kallikrein works immediately on the 2-globulin,
liberating the kinin called kallidin that is then converted
inbradykinin by tissue enzymes. Once formed, bradykinin cau-ses
intense dilation of the arterioles and increases
capillarypermeability, contributing to the dissemination of
inflam-mattion 16.The action of phospholipase A on the cell
membrane causesthe release of arachidonic acid, which is
metabolized bythree enzymatic systems: cyclooxigenase that
originatesprostaglandins, thromboxanes, and prostacyclins;
lipoxige-nase that induces the production of leukotrienes and
lipoxins;and P-450 cytochrome that originates the products of
the
epoxigenase pathway. These substances, especially
pros-taglandins E
2(PGE
2), decrease the excitability threshold of
nociceptors 17. Inflammatory cells, macrophages, and leu-
Table I Subtypes of A and C Fibers
Fiber Type Characteristics
Type I A fibers Respond to temperatures of about 52C,they are
not sensitive to capsaicin andtheir response is modulated by
VRL-1receptors
Type II A f ibers Sensit ive to temperatures of about 43C,
activated by capsaicin, and activate,through VR1 receptors,
non-selectivecationic channels permeable to calcium
Type I C fibers Con ta in substance P and CGRP andexpress
thyrokinase A receptors for thenerve growth factor. They respond
tocapsaicin and protons
Type II C fibers E xpr es s p ur ine rgi c P 2X3
receptor foradenosine and a group of surfacecarbohydrates,
-D-galactose, capable ofbinding lectin IB-4, and have
selectivesensitivity to protons
Cellularmembrane
Bradykinin
Lesion
Acetylcholine
HistamineEnzymes
H+
TNF-K+
Substance PSerotonin
ProstaglandinsAlgogenic
substances
Figure 1 Release of Algogenic Substances After Tissue Injury
ROCHA, KRAYCHETE, LEMONICA ET AL.
-
8/2/2019 dor fisiopat
8/12
Revista Brasileira de Anestesiologia 101Vol. 57, No 1,
Janeiro-Fevereiro, 2007
cocytes release cytokines that contribute to the migration ofnew
cells to the site of injury. There is production and relea-se of
interleukins 1 and 6, tumor necrosis factor, selectin,chemotactic
factors, nitric oxide, and oxidizing substances.New receptors are
then recruited, and participate in theinflammatory process.
Substance P and neurokinin A cause
vasodilation and increase vascular permeability, which alsofor
maintaining the inflammatory process 18.However, bradikinin,
prostaglandin E2, nerve growth factor(NGF), and interleukins seem
to be fundamental in periphe-ral nociception. Prostaglandin and
bradykinin cause changesin specific receptors (TRPV1) attached to
ligand-dependention channels through the activation of cAMP and
proteinkinases A (PKA) and C (PKC), reducing the
post-hyperpo-larization time of the neural membrane, and decreasing
thetriggering threshold of the nervous fiber.Neurotrophins increase
the synthesis, anterograde axonaltransport, and the amount of SP
and CGRP in type 1 C fibers,and reduce the activity of
gamma-aminobutyric acid (GABA),both in peripheral and central nerve
endings. They alsocause changes in the vanilloid receptors (VR1) of
A fibersattached to ligand-dependent ion channels and trigger
pro-tein kinases activated by mitogens (MAPK) that can
phospho-rilate cAMP and initiate the genetic transcription
responsiblefor phenotypic changes that contribute to the increase
insynaptic efficacy.If the aggression is persistent, it leads to
changes in theperipheral nervous system and sensitizes nerve
fibers, withconsequent hyperalgia and increase in the levels of
cAMPand calcium in the nociceptors. This phenomenon is secon-dary
to the action of inflammatory mediators and consequent
spontaneous activity of neurons, increase in the response
tosuprathreshold stimuli, and reduction of the activationthreshold
of nociceptors 18-20. An especial type of nociceptor,known as
silent nociceptor, is activated after inflammation orafter tissue
injury. It is estimated that 40% of C fibers and30% of A fibers
contribute with silent nociceptors. After therelease of chemical
products in the lesion, these receptors,previously silent, are
activated by thermal and mechanicalstimuli, developing spontaneous
discharges, being capableof an intense response to nociceptive and
non-nociceptivestimuli 21-22 (Figure 2).In short, tissue injury
results in accumulation of arachidonicacid metabolites. The
production of prostaglandins and leuko-trienes leads to the
degranulation of mast cells and directactivation of nerve fibers,
macrophages and lymphocytes.Mediators, such as potassium,
serotonin, substance P,histamine, and kinins are released. There
are changes invascular permeability, local blood flow, resulting in
theclassical signs of inflammation, like erythema,
increasedtemperature, edema, and functional impotence. The
processof peripheral sensitization is initiated with the
consequentexacerbation of the response to the painful stimulus
20-22.Peripheral neuromediators prolong the depolarization of
theneural membrane, with the consequent increase of sodium
and calcium channels conductivity, and a decrease in theinflux
of potassium and chloride.Sodium channels are involved in the
genesis of neuronalhyperexcitability and can be classified in two
large groups:those sensitive to tetrodotoxin (TTXs), present in A
fibers, inthe entire nervous system, and in the dorsal root
ganglion;and those resistant to tetrodotoxin (TTXr), found
especially inC fibers of the dorsal root ganglion 23. Although the
peripherallesion of C fiber decreases SP, neurotrophins (BDNF),
receptors (VR1 and P2X3), and high-voltage type N
calciumchannels in the dorsal horn of the spinal cord, there
isupregulation of type III TTXs channels, and sodium channels(TTXr)
are translocated from the cell body to the neuroma,facilitating the
increase in nervous excitability 24. Thishappens if the nerve fiber
is intact (inflammation), i.e., thereis an increase in excitatory
neuromediators in the dorsalhorn of the spinal cord and greater
expression of sodiumchannels (TTXr), which facilitates neuronal
hyperexcitabilityand hinders the response to the treatment with
localanesthetics 24.In both situations described, especially in the
lesion of Cfibers, there can also be an increase in SP and BDNF in
Afibers (low threshold mechanoreceptors), as well as buddingof
those at the connections of afferent C fibers (lamina
II),increasing the receptive field of the neuron and facilitating
theinterpretation of harmless stimuli as aggressive 25.
Thisexplains, for example, the mechanical allodynia that occursin
post-herpetic neuralgia 26. Other possibility would be thebudding
of sympathetic noradrenergic axons at the dorsalroot ganglion,
around large diameter neurons (A fibers),suggesting the hypothesis
of activation of afferent sensitivefibers after the sympathetic
stimulation 27. Besides, there canalso be a disproportion between
excitatory and pain sup-
Figure 2 Process of Peripheral Sensitization
StimulusRelease ofAlgogenicSubstance
PAIN- Reduction of the painthreshold in the activenociceptors-
Activation of silent no-ciceptors
PAIN: CURRENT ASPECTS ON PERIPHERAL AND CENTRAL
SENSITIZATION
-
8/2/2019 dor fisiopat
9/12
102 Revista Brasileira de AnestesiologiaVol. 57, No 1,
Janeiro-Fevereiro, 2007
pressing pathways, with a decrease in the inhibitory activityof
glycine, GABA, and opioids 24.
CENTRAL PAIN MECHANISMS
The transmission of noxious stimuli in the spinal cord is
not
a passive process. Intraspinal circuits have a capacity tochange
both the stimulus and painful response. The inte-raction among the
intramedullary circuits determines whichmessages will reach the
cerebral cortex 21.Clinical and experimental studies have
demonstrated thatnoxious stimuli cause changes in the central
nervoussystem, which modify the mechanisms triggered by
afferentstimuli. Persistent stimulation of nociceptors causes
spon-taneous pain, reduces the sensitivity threshold, and
causeshyperalgesia. This can be divided in primary and
secondaryhyperalgesia. Primary hyperalgesia is defined as the
in-creased response to the painful stimulus at the site of
injury,while secondary hyperalgesia is the extension of that
res-ponse to adjacent areas. The presence of all of those ele-ments
suggests that peripheral sensitization is not the onlyphenomena
responsible for them, and that the central ner-vous system must be
involved in this process 21,28,29.Central sensitization implies
changes in peripheral impul-ses, with positive or negative
adaptations. There is a reductionin the threshold or an increase in
the response to afferentimpulses, persistent discharges after
repeated stimuli, andwidening of the receptive fields of dorsal
horn neurons.Repeated impulses in C fibers amplify sensorial
signals inspinal neurons, sending messages to the brain 13.
Periphe-ral lesions induce plasticity in supraspinal structures
through
mechanisms that encompass specific types of gluatamatereceptors.
Neurotransmitters, such as substance P, soma-tostatin, peptide
genetically linked to calcitonin, neurokinin A,glutamate, and
aspartate are released after tissue injury.These substances are
connected to the activation of exci-tatory post-synaptic
potentials, and of N-methyl-D-aspartate(NMDA) and non-NMDA
receptors. Frequent stimulation ofafferent fibers generates a
summation of action potentialsand the consequent cumulative
pos-synaptic depolarization.After activation of NMDA receptors by
glutamate, the ionmagnesium is removed from the receptor, leading
to theinflux of calcium into the cell, amplifying and prolonging
theresponse to the painful stimulus 30,31.The increase in calcium
concentration leads to activation ofnitrous oxide synthase and
stimulation of the transcription ofprotooncogenes. These genes are
located in the centralnervous system, being involved in the
formation of dinorphinsand enkephalins. Enkephalins are
antinociceptive andconnected to the reduction of neuroplasticity
and hyperal-gia 32,33. However, dinorphins have a complex mechanism
ofaction, since they have algogenic and antinociceptvie
actions.Recent studies have suggested that the activation of
f-fosand c-junpromotes the transcription of the messenger
RNAresponsible for the synthesis of fundamental proteins invol-
ved in changing the phenotypic expression, and the conse-quent
perpetuation of neuronal hypersensitivity 28,33 (Figure 3).The
sensitization of the dorsal horn of the spinal cord can beof
several modalities: wind up, classical synaptic sensiti-zation,
long-term potentiation, late phase of the long-termpotentiation,
and long-term facilitation 34.
The classical synaptic sensitization is caused by a
synchro-nized sequency of repeated peripheral nociceptive stimuli
forone asynchronous nociceptive stimulus, increasing theafferent
response of A and C fibers (homosynaptic potentia-tion) and the
afferent response of non-stimulated A fibers(heterosynaptic
potentiation). This is a consequence of therelease of excitatory
amino acids, peptides, and neurotro-phins in the dorsal horn of the
spinal cord 35.Excitatory amino acids, represented by glutamate and
as-partate, bind to specific ionotropic or metabotropic
receptors.In ionotropic, or fast, receptors the neurotransmitter
bindingsite is an integral part of an ion channel, while
metabotropic,or slow, receptors are bound to protein G. Among the
recep-tors for excitatory amino acids, we should mention
AMPA,cainate, and N-methyl-D-aspartate (NMDA), that are
ionotro-pic, and the Mrglu receptor, whose action is mediated
byprotein G, making it a metabotropic receptor. Peptides,
subs-tance P, and calcitonin gene-related peptide (CGRP) bind
toneurokinins type NK-1 and NK-2, while neurotrophins bindto
thyrokinases types A and B (trkA and trkB) receptors.After the
release of excitatory amino acids, peptides, andneurotrophins and
their binding to specific receptors, thereis activation of second
messengers, such as cAMP, PKA,PKC, phosphatidylinositol,
phospholipase C, and phospho-lipase A2. This opens the calcium
channels and, conse-
quently, the production of prostaglandins and nitrous
oxide,which migrate from the intracellular environment to the
sy-naptic cleft and cause the release of glutamate,
aspartate,substance P, and CGRP, contributing to the amplification
ofthe painful process 34.Wind up is the summation of slow synaptic
potentials afterrepeated low frequency, below 5 Hz, stimulation of
theafferent fibers for a prolonged time. This triggers the
releaseof excitatory neurotransmitters, glutamate, and aspartate
inthe dorsal horn of the spinal cord and produces depola-rization
secondary to the removal of the voltage-dependentblockade caused by
the presence of magnesium in NMDAreceptors. There is an increase in
calcium conductivity andresponse to pain to each repeated stimulus
of the sameintensity 36.Although long-term potentiation is better
known in the hippo-campus and cortical areas, it may be the result
of a sequenceof short, high frequency nociceptive stimuli. This
wouldactivate AMPA and NK1 receptors and calcium channels,leading
to the prolonged, excitatory post-synaptic response,especially in
the neurons in lamina I 37.The mechanisms that contribute to the
increased efficacy ofsynaptic transmission would be the result of
phosphorylationof membrane receptors and changes in the opening
time of
ROCHA, KRAYCHETE, LEMONICA ET AL.
-
8/2/2019 dor fisiopat
10/12
Revista Brasileira de Anestesiologia 103Vol. 57, No 1,
Janeiro-Fevereiro, 2007
ion channels, or the formation and transport of
excitatorysubstances from the cell to the synaptic cleft. Besides,
pro-teinokinases activated by mitogens (MAPK) in the dorsalhorn of
the spinal cord modulate the phosphorylation ofNMDA and AMPA
receptors, amplifying the nociceptive res-ponse 38.Long-term
facilitation involves the activation of transcriptionfactors and
changes in transcription. Transcription factorsmodulate the
relationship between the receptor-neurome-diator complex and
changes in gene expression 39.
The nociceptive stimulus triggers the same receptor cascadeand
second messengers described previously for the clas-sical synaptic
sensitization, but it also triggers the expres-sion of immediate
early genes c-fos (B, C, D), c-jun, COX-2enzymes, and slow response
genes that encode pro-dinorphin, NK1 receptor, and trkB in the
dorsal horn of thespinal cord. There is upregulation of the
pathways for thesynthesis of cytokines, chemokines, and adhesion
mole-cules. This causes phenotypic changes in the dorsal
rootganglion 40.
Figure 3 Sequence of Events that Lead to Sensitization of the
Neurons in the Dorsal Horn After Intense and Continuous Nociceptive
Stimulation.The intense activation of primary afferent neurons
triggers the release of glutamate (Glu) and substance P (SP). Due
to the role ofmagnesium (Mg+2), the NMDA receptor is not responsive
to Glu initially; but the depolarization of AMPA receptors by the
presence of Gluin the metabotropic receptor activates phospholipase
C (PLC), which is mediated by protein G, causing hydrolysis and
transformation ofphosphatidyilinositol 4,5-biphosphate (PIP
2) in inositol triphosphate (IP
3) and diacylgyicerol (DAG). Diacylglycerol stimulates the
production
of protein kinase C (PKC), which is activated in the presence of
elevated intracellular calcium (Ca +2) levels. Inositol
triphosphate stimulatesthe release of calcium from intracellular
storage sites in the sarcoplasmic reticulum. The increase in PKC
induces the sustained increasein membrane permeability and, along
with an increase in intracellular Ca+2, increases the expression of
protooncogenes, such as c-fosand c-jun. The proteins produced by
these protooncogens encode neuropeptides, such as enkephalins
(EKN), dinorphins (DYN), andtachykinin (TK). This increase also
leads to the activation of phospholipase A
2(PLA
2) and activation of the nitric oxide synthetase (NOS)
by a calmodulin-dependent mechanism. Phospholipase A2
catalyzes the conversion of phosphatidilcholine (PC) to
prostaglandin (PG), andthromboxane (TX) and to produce leukotrienes
(LT) by lypoxigenase (LO). Nitric oxide synthetase catalyzes the
production of protein kinaseand leads to changes in the genetic
expression. Nitric oxide diffuses from the intracellular
environment to the terminal of the primary afferentwhere it
increases the release of glutamate
Inhibitoryinterneuron (?)
Extracellulareffects (?)
GC
NO cGMP
SP SP Glu
GluGluSP
NK1 NMDA AMPANa
K+
Na
K+
Metabotropics
PLCPIP2PLA2A A
PC
CO LO
LTTX, PG
CAM
CAM
PK
NOS
NO
Intracellular
effects (?)
GC-cGMP
L-CI
L-Arg
Ca++
c-fosc-jun
DINENC
IP3
Ca++
Endoplasmic reticulum
IP3DAG
PKC
O2
PAIN: CURRENT ASPECTS ON PERIPHERAL AND CENTRAL
SENSITIZATION
-
8/2/2019 dor fisiopat
11/12
104 Revista Brasileira de AnestesiologiaVol. 57, No 1,
Janeiro-Fevereiro, 2007
SEGMENTAR AND SUPRA-SEGMETAR RESPONSESTO PAIN
Nociceptive fibers cross the midline at the level of dorsalhorn
of the spinal cord and ascend through the spinotha-lamic,
spinoreticular, and spinomesencephalic tracts, post-
synaptic posterior column, and spino-ponto-amigdalasystem. Some
of those fibers end at the ventroposteromedialthalamic nucleus
(VPM) and ascend posteriorly to the so-mesthesic (S1 and S2)
cerebral cortex, insular cortex, andposterior cingular cortex.
Other neurons project their axonsto the hypothalamus, reticular
formation, periaqueductal graymatter, medial and intrathalamic
nucleus, and anterior brainstructures responsible for the
neuroendocrine and emotionalresponses to pain 41.The activation of
peripheral nociceptive fibers leads to re-trograde migration of
nerve growth factor (NGF) to the spinalcord and induces reflex
segmental response with antero-grade transport of substance P to
the periphery, causingvasodilation, increase in vascular
permeability, attraction ofcells of the immune system to the site
of injury, and degra-nulation of mast cells and the release of
several neuro me-diators. Thus, substance P helps the maintenance
andexpansion of the inflammatory process to the receptive fieldof
nerve fibers adjacent to the site of injury, constituting
thesecondary hyperalgia 42.On the other hand, adrenergic fibers
contribute not only tothe process described above but also increase
the sensi-tivity of nociceptive fibers to bradykinin. Vasospasm,
muscu-lar spasm, reflexes that trigger the release of acid
radicalsand, consequently, reduce the discharge threshold for
noci-
ceptive fibers, potentiate those effects 43.In supra-segmental
response, the individual with chronicpain seems to have a possible
inability to increase thesecretion of the
hypothalamus-pituitary-adrenal axis hormo-nes or increase the
sympathetic response when dealing withphysical and emotional
stress. This is reflected on the in-creased levels of cortisol,
adrenaline, noradrenaline, growthhormone (GH), and thyroid and
gonadal hormones, decrea-sing the activity of the defense system.
This model tries toexplain fibromyalgia or myofascial pain; it is
possible thatthere is an increase in the hypothalamic secretion of
CRHwith down regulation of receptors in the pituitary,
increasedlevels of ACTH and low levels of cortisol, and
peripheralresistance to cortisol 44.The hypothalamus-pituitary axis
seems to interact with thepainful process in several levels or
stages. The absence ofglucocorticoids can: 1) decrease the
conversion of glutama-te, an excitatory neurotransmitter, to
glutamine, increasing theneurotoxicity of glutamate in the central
nervous system; 2)increase the production of nerve growth factor
(NGF) andsubstance P; and 3) increase the production of
cytokinesand, consequently, of NGF 45.Tissue and neuronal injury
result in sensitization of noci-ceptors and facilitate peripheral
and central nervous systems
conduction. The study of those mechanisms may, in the fu-ture,
elucidate ways to diagnose and treat acute and chronicpain
syndromes.
REFERNCIAS REFERENCES
01. Lacerte M, Shah RV - Interventions in chronic pain
management.1. Pain concepts, assessment, and medicolegal issues.
ArchPhys Med Rehabil, 2003;84:S35-S38.
02. Turk DC, Melzack R - The Measurement of Pain and the
Assess-ment of People Experiencing Pain. Handbook of Pain
Assessment.New York, Guildford, 1992;3-12.
03. Jacobsson L, Lindgarde F, Manthorpe R - The commonest
rheu-matic complaints of over six week duration in a
twelve-monthperiod in a defined Swedish population. Prevalences and
rela-tionships. Scand J Rheumatol, 1989;18:353-360.
04. James FR, Large RG, Bushnell JA et al - Epidemiology of pain
inNew Zealand. Pain, 1991;44:279-283.
05. Bonica JJ - Treatment of Cancer Pain: Current Status and
FutureNeeds, em: Dubner R, Cervero F - Advances in Pain
Research
and Therapy, 1985;589-616.06. Bovim G, Schrader H, Sand T - Neck
pain in the general popu-
lation. Spine, 1994;19:1307-1309.07. Brattberg G -
Epidemiological studies of pain. Acta Universitatis
Upsaliensis, Comprehensive Summaries of Upsala Dissertationsfrom
the Faculty of Medicine, 1989;196:52.
08. Walco GA, Oberlander TM - Musculoskeletal Pain Syndromes
inChildren, em: Schechter NL, Berde CB, Yaster M - Pain in
Infants,Children, and Adolescents. Baltimore, Williams &
Williams1996;459-472.
09. Besson P, Perl ER - Responses of cutaneous sensory units
withunmyelinated fibers to noxious stimuli. J Neurophysiol,
1969;32:1025-1043.
10. Levine JD, Taiwo Y - Inflammatory Pain, em: Wall PD, Melzack
R,Bonica JJ - Textbook of Pain. 3rd ed., Edinburgh, Scothand,
Chur-
chill Livingstone, 1994;45-56.11. Loewenstein WR -
Mechano-Electric Transduction in the Paci-
nian Corpuscle: Initiation of Sensory Impulses in
Mechanore-ceptors, em: Autrum H - Handbook of Sensory Physiology.
Berlin.Springer-Verlag, 1971;267-290.
12. Webster KE - Somaesthetic pathways. Br Med Bull,
1977;33:113-120.
13. Bedbrook GM - Injuries of the Thoracolumbar Spine with
Neu-rological Symptoms, em: Vinken PJ, Bruyn GW - Handbook
ofClinical Neurology Amsterdam. 25th ed., North-Holland,
1976;437-466.
14. Campbell JN, Raja SN, Cohen RH et al - Peripheral
NeuralMechanisms of Nociception, em: Wall PD, Melzack R -
Textbookof Pain. Edimburgh, Scotland, Churchill Livingstone,
1989;22-45.
15. Piotrowski W, Foreman JC - Some effects of calcitonin
gene-related peptide in human skin and on histamine release. Br
JDermatol, 1986;114:37-46.
16. Guyton AC, Hall JE - Controle Local do Fluxo Sanguneo
pelosTecidos, em: Guyton AC, Hall JE - Tratado de Fisiologia
Mdica.Rio de Janeiro, Guanabara Koogan, 2002;166-173.
17. OBanion MK - Cyclooxygenase-2: molecular biology,
pharma-cology, and neurobiology. Crit Rev Neurobiol,
1999;13:45-82.
18. Ferreira SH - Hiperalgesia inflamatrial, xido ntrico y
controlperifrico del dolor. Rev Latino Americana de Dolor,
1995;12:6-17.
19. Fletcher D, Kayser V, Guilbaud G - Influence of timing of
admi-nistration on the analgesic effect of bupivacaine infiltration
incarrageenin-injected rats. Anesthesiology, 1996;84:1129-1137.
ROCHA, KRAYCHETE, LEMONICA ET AL.
-
8/2/2019 dor fisiopat
12/12
Revista Brasileira de Anestesiologia 105Vol. 57, No 1,
Janeiro-Fevereiro, 2007
20. Aida S, Baba H, Yamakura T et al - The effectiveness
ofpreemptive analgesia varies according to the type of surgery:
arandomized, double-blind study. Anesth Analg, 1999;89:711-716.
21. Woolf CJ - Recent advances in the pathophysiology of
acutepain. Br J Anaesth, 1989;63:139-146.
22. Woolf CJ, Chong MS - Preemptive analgesia treating
postope-rative pain by prevention the establishment of central
sensi-
tization. Anesth Analg, 1993;77:362-379.23. Lai J, Gold MS, Kim
CS et al - Inhibition of neuropathic pain bydecreased expression of
the tetrodotoxin-resistant sodiumchannel, Nav1.8. Pain,
2002;95:143-152.
24. McMahon SB - Neuropathic Pain Mechanisms, em:
GiamberardinoMA Pain 2002 an Updated Review: Refresher
CourseSyllabuss. Seattle, IASP, 2002;155-161.
25. Mannion RJ, Doubell TP, Coggeshall RE et al - Collateral
sproutingof uninjured primary afferent A-fibers into the
superficial dorsalhorn of the adult rat spinal cord after topical
capsaicin treatmentto the sciatic nerve. J Neurosci,
1996;16:5189-5195.
26. Rowbotham MC, Fields HL - The relationship of pain,
allodyniaand thermal sensation in post-herpetic neuralgia. Brain,
1996;119:347-354.
27. Choi B, Rowbotham MC - Effect of adrenergic receptor
acti-
vation on post-herpetic neuralgia pain and sensory
disturbances.Pain, 1997;69:55-63.28. Alan NS - Controle da dor no
perodo perioperatrio. Clin Cirurg
Am Norte, 1999;79:197-211.29. Dickenson AH, Sullivan AF -
Subcutaneous formalin-induced
activity of dorsal horn neurons in the rat: differential
responseto an intrathecal opiate administered pre or pos formalin.
Pain,1987; 30:349-360.
30. Woolf CJ - Somatic pain pathogenesis and prevention. Br
JAnaesth, 1995;75:169-176.
31. Dickenson AH - Recent advances in the physiology and
phar-macology of pain: plasticity and its implications for clinical
anal-gesia. J Psychopharm, 1991;5:342-351.
32. Coderre TJ, Vaccarino AL, Melzack R - Central nervous
systemplasticity in the tonic pain response to subcutaneous
formalin
injection. Brain Res, 1990;535:155-158.33. Malmberg AB, Yaksh TL
- Hyperalgesia mediated by spinalglutamate or substance P receptor
blocked by spinal cyclooxy-genase inhibition. Science,
1992;257:1276-1279.
34. Ji RR, Kohno T, Moore KA et al - Central sensitization and
LTP:do pain and memory share similar mechanisms? Trends
Neurosci,2003;26:696-705.
35. Woolf CJ, Salter MW - Neuronal plasticity: increasing the
gain inpain. Science, 2000;288:1765-1769.
36. Li J, Simone DA, Larson AA - Windup leads to characteristics
ofcentral sensitization. Pain, 1999;79:75-82.
37. Randic M, Jiang MC, Cerne R - Long-term potentiation and
long-term depression of primary afferent neurotransmission in the
ratspinal cord. J Neurosci, 1993;13:5228-5241.
38. Ji RR, Samad TA, Jin SX et al - p38 MAPK activation by NGF
inprimary sensory neurons after inflammation increases TRPV1levels
and maintains heat hyperalgesia. Neuron, 2002;36:57-68.
39. Sandkuhler J - Learning and memory in pain pathways.
Pain,2000;88:113-118.
40. Hunt SP, Pini A, Evan G - Induction of c-fos-like protein in
spinalcord neurons following sensory stimulation. Nature, 1987;
328:
632-634.41. Basbaum A, Bushnell MA - Pain: Basic Mechanisms,
em:Giamberardino MA Pain 2002 an updated Review: RefresherCourse
Syllabuss. 1st ed., Seattle, IASP, 2002;3-7.
42. Otten U, Goedert M, Mayer N et al - Requirement of nerve
growthfactor for development of substance P-containing
sensoryneurones. Nature, 1980;287:158-159.
43. Basbaum AI - Distinct neurochemical features of acute
andpersistent pain. Proc Natl Acad Sci, 1999;96:7739-7743.
44. Neeck G - Pathogenic mechanisms of fibromyalgia. Ageing
ResRev, 2002;1:243-255.
45. Dessein PH, Shipton EA, Stanwix AE et al -
Neuroendocrinedeficiency-mediated development and persistence of
pain infibromyalgia: a promising paradigm? Pain,
2000;86:213-215.
RESUMENRocha APC, Kraychete DC,Lemonica L, Carvalho LR, Barros
GAM,Garcia JBS, Sakata RK Dolor: Aspectos Actuales de la
Sensibili-zacin Perifrica y Central.
JUSTIFICATIVA Y OBJETIVOS:Las recientes investigaciones sehan
centrado en la plasticidad bioqumica y estructural del sistema
nervioso proveniente de la lesin tisular. Los mecanismos
involu-
crados en transicin del dolor agudo para crnico son
complejos
e involucran la interaccin de sistemas receptores y el flujo de
iones
intracelulares, sistemas de segundo mensajero y nuevas cone-
xiones sinpticas. El objetivo de este artculo fue discutir los
nuevos
mecanismos que envuelven la sensibilizacin perifrica y
central.
CONTENIDO:La lesin tisular provoca un aumento en la respuestade
los nociceptores, llamada sensibilizacin o facilitacin. Esos
fen-
menos empiezan despus de la liberacin local de mediadores
inflamatorios y de la activacin de clulas del sistema inmune o
de
receptores especficos en el sistema nervioso perifrico y
central.
CONCLUSIONES:Las lesiones del tejido y de las neuronasresultan
en una sensibilizacin de nociceptores y en la facilitacin
de la conduccin nerviosa central y perifrica.
PAIN: CURRENT ASPECTS ON PERIPHERAL AND CENTRAL
SENSITIZATION