Embed Size (px)
Citation preview
Dott.ssa Maria Cappello
UOC Gastroenterologia ed Epatologia
Azienda Ospedaliera Universitaria Policlinico Palermo
Vecchi e nuovi biologici nelle MICI: criteri di scelta oggi
Disclosures
• Lecture fees: MSD, AbbVie, Takeda, Janssen, Chiesi, Pharmanutra
• Advisory Board Member: MSD, AbbVie, Takeda, Janssen, Shire,
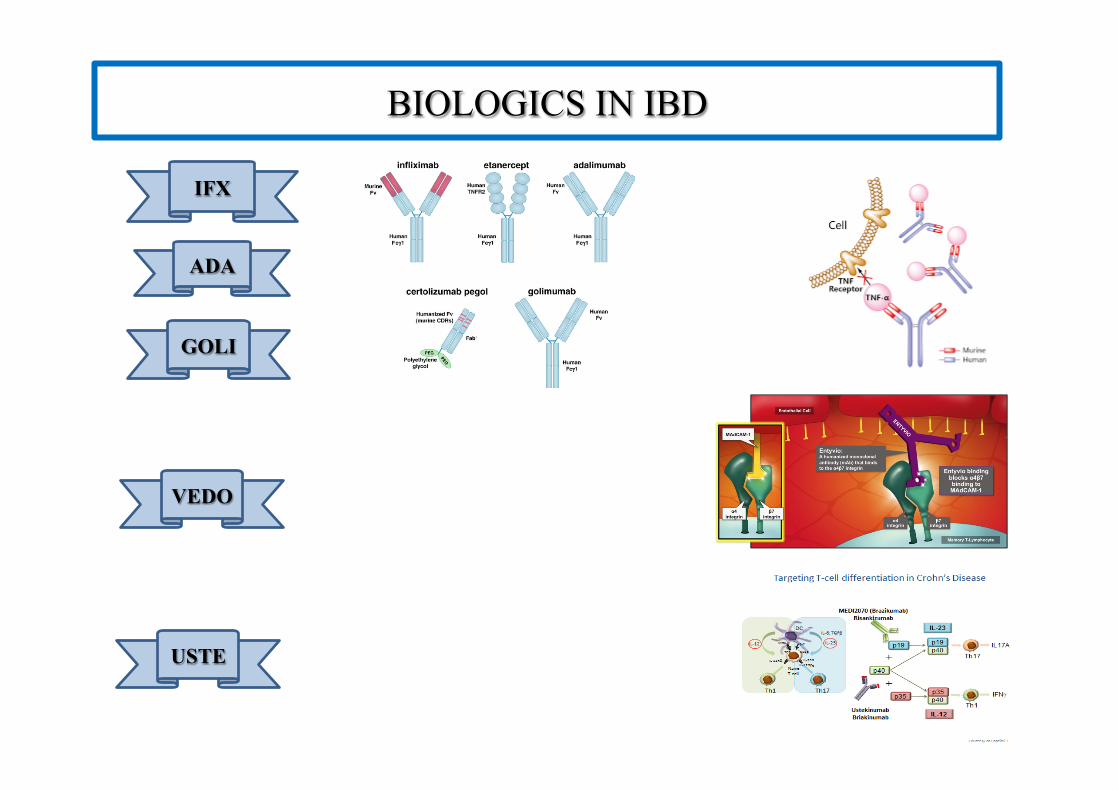
BIOLOGICS IN IBD
IFX
ADA
GOLI
VEDO
USTE
• Targetingleukocytetrafficking
anti-MAdCAM1,etrolizumab-anti-β7,CCR9antagonist,antiIP-10,
S1P1receptormodulator
• TargetingT-celldifferentiation(antiIL23p19)
• TargetingJAK-STATpathway(tofacitinibanti-JAK1/3,anti-JAK1)
• Cell-basedtherapy(autologusHSCtransplantation,MSC
transplantation,tolerogenicimmunecells)
Future perspectives
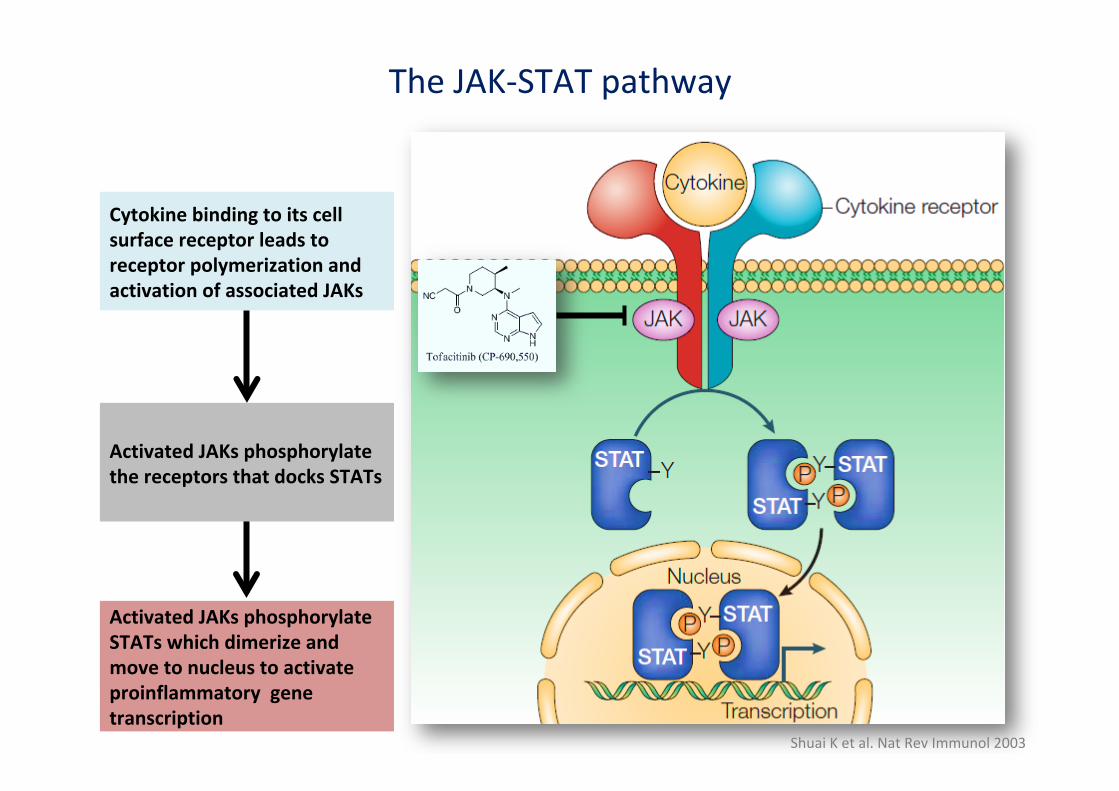
TheJAK-STATpathway
ShuaiKetal.NatRevImmunol2003
CytokinebindingtoitscellsurfacereceptorleadstoreceptorpolymerizationandactivationofassociatedJAKs
ActivatedJAKsphosphorylatethereceptorsthatdocksSTATs
ActivatedJAKsphosphorylateSTATswhichdimerizeandmovetonucleustoactivateproinflammatorygenetranscription
How to choose a biologic: the sources
• Pivotal RCTs • Guidelines • SMPC • Pharmacoeconomic studies • Indirect comparison studies Ø Network metaanalyses Ø Real-world experiences • Direct comparison: head-to-head RCTs
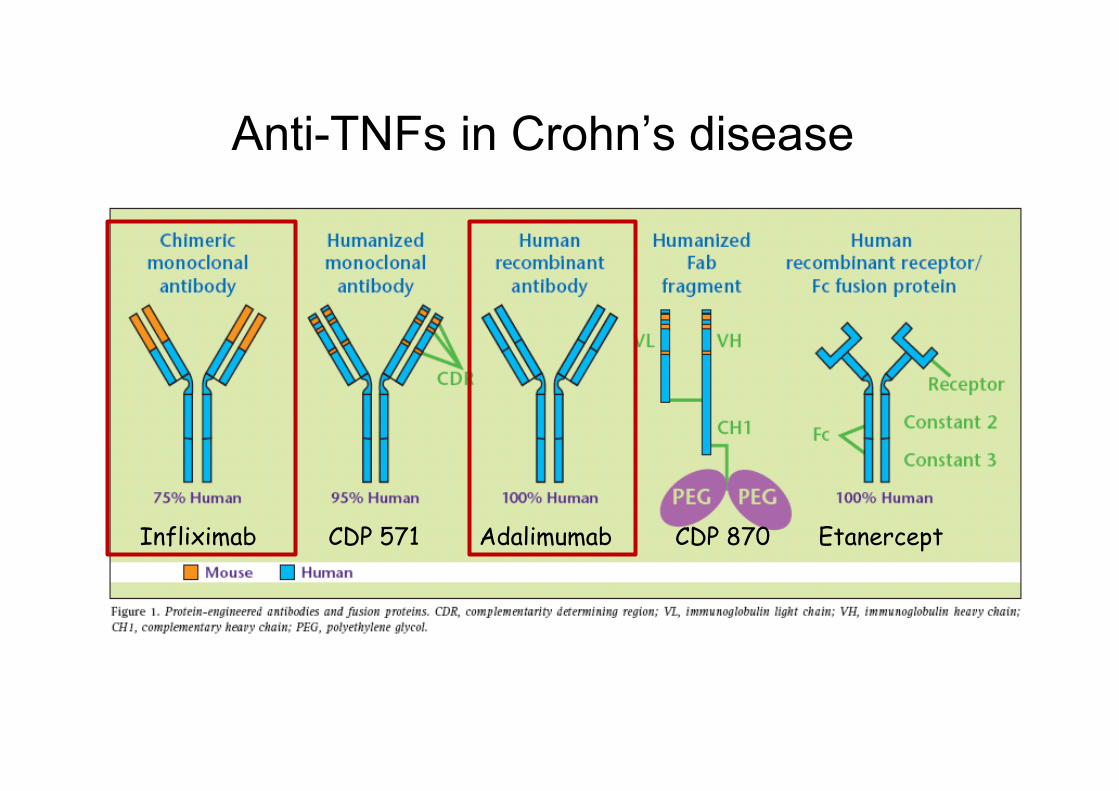
Infliximab CDP 571 Adalimumab CDP 870 Etanercept
Anti-TNFs in Crohn’s disease
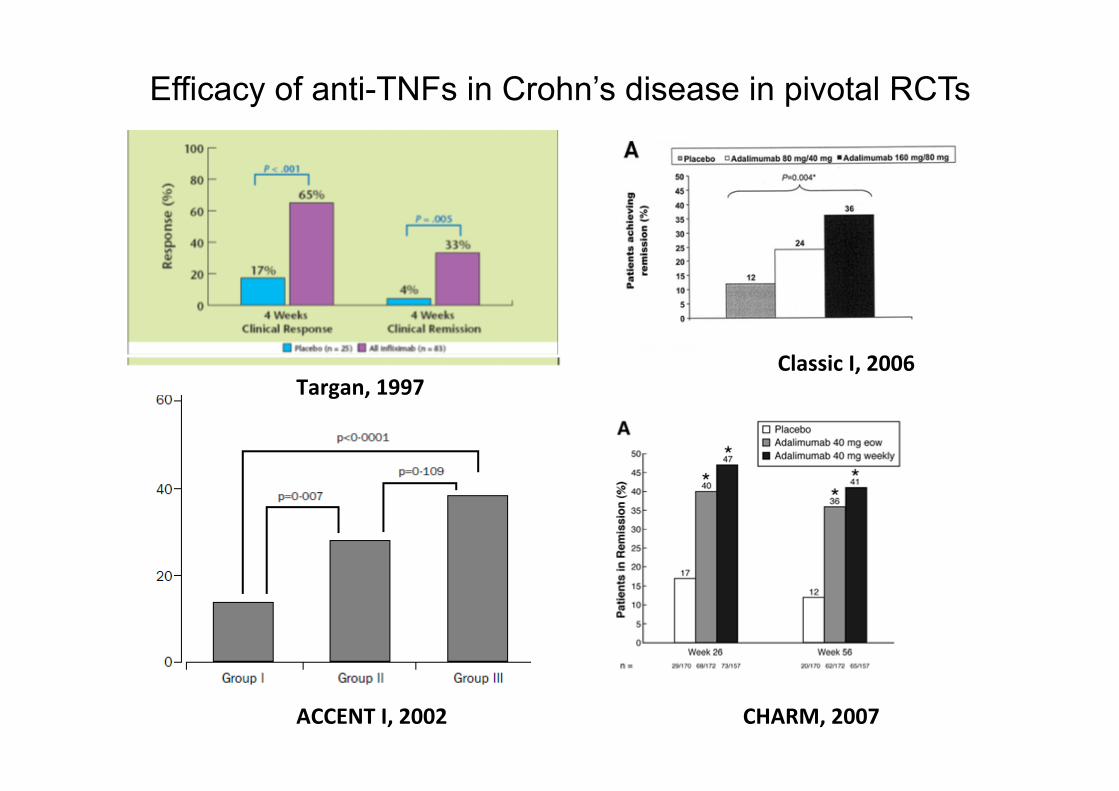
ACCENTI,2002 CHARM,2007
Efficacy of anti-TNFs in Crohn’s disease in pivotal RCTs
ClassicI,2006Targan,1997
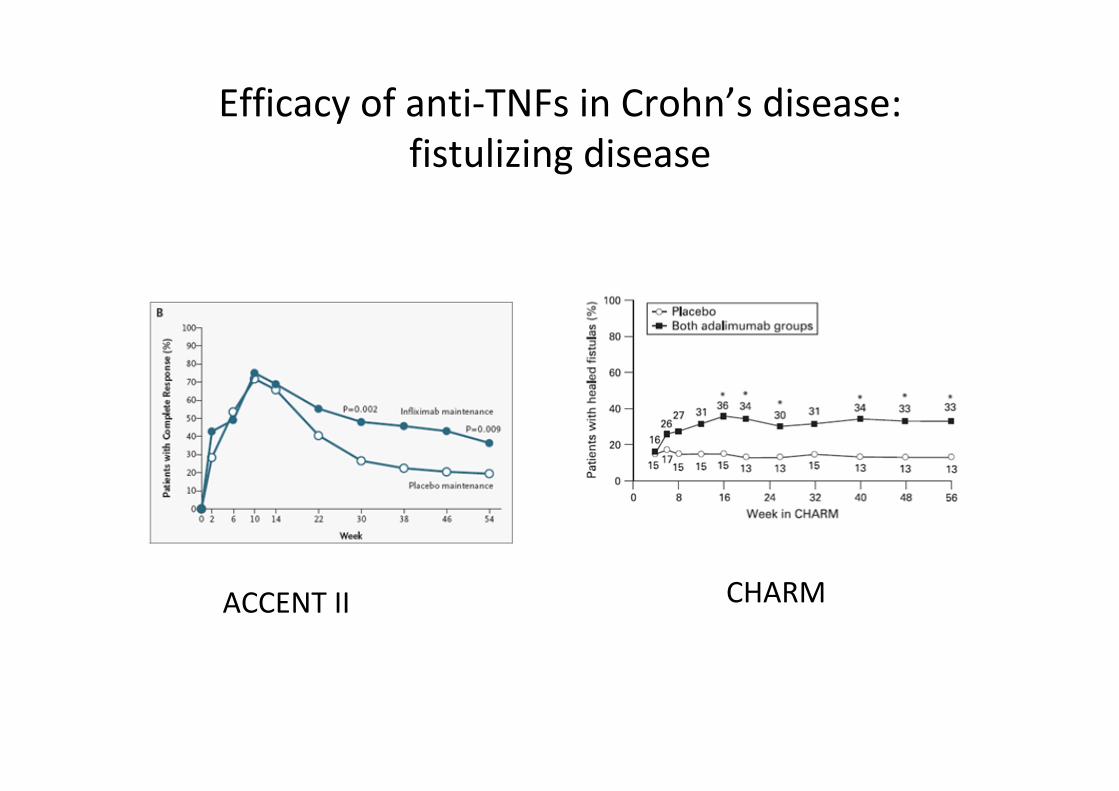
Efficacyofanti-TNFsinCrohn’sdisease:fistulizingdisease
ACCENTII CHARM

GUT,2011 Gastroenterology2012
Efficacy of anti-TNFs in UC in pivotal RCTs
NEJMed,2005
ACT1&2NEnglJMed2005)
ULTRA2ULTRA1
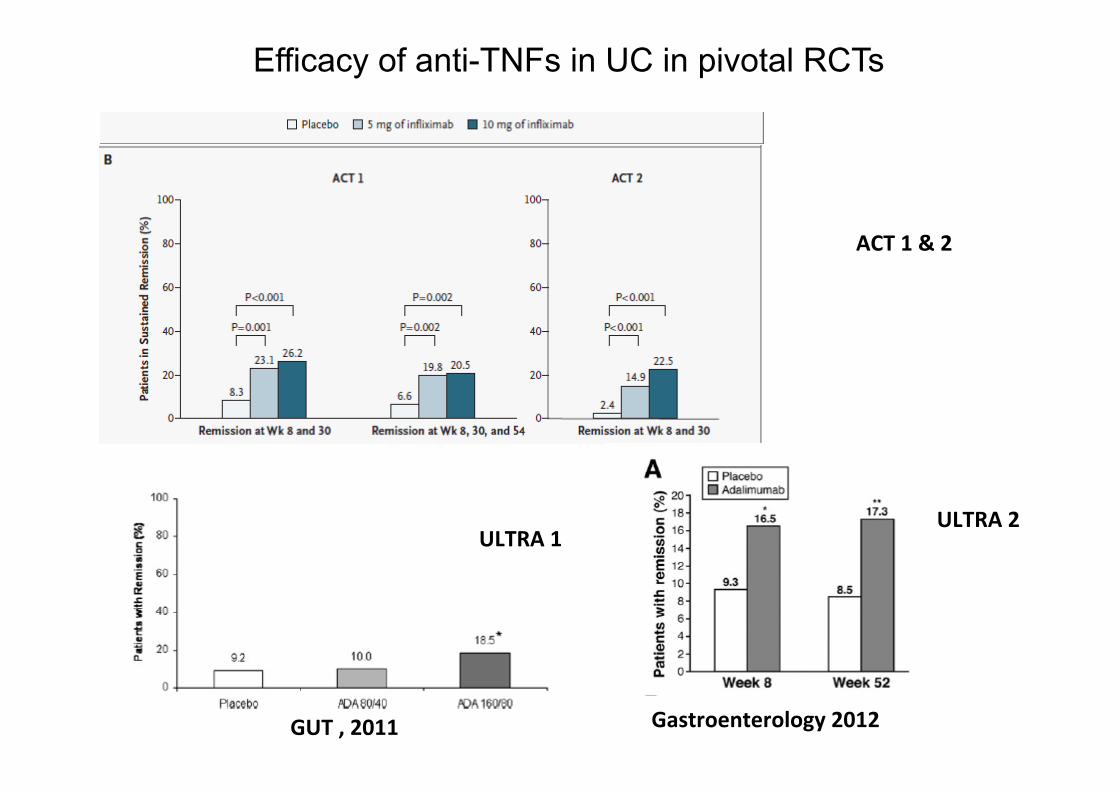
GUT,2011 Gastroenterology2012
Efficacy of anti-TNFs in UC in pivotal RCTs
NEJMed,2005
ACT1&2
ULTRA2ULTRA1
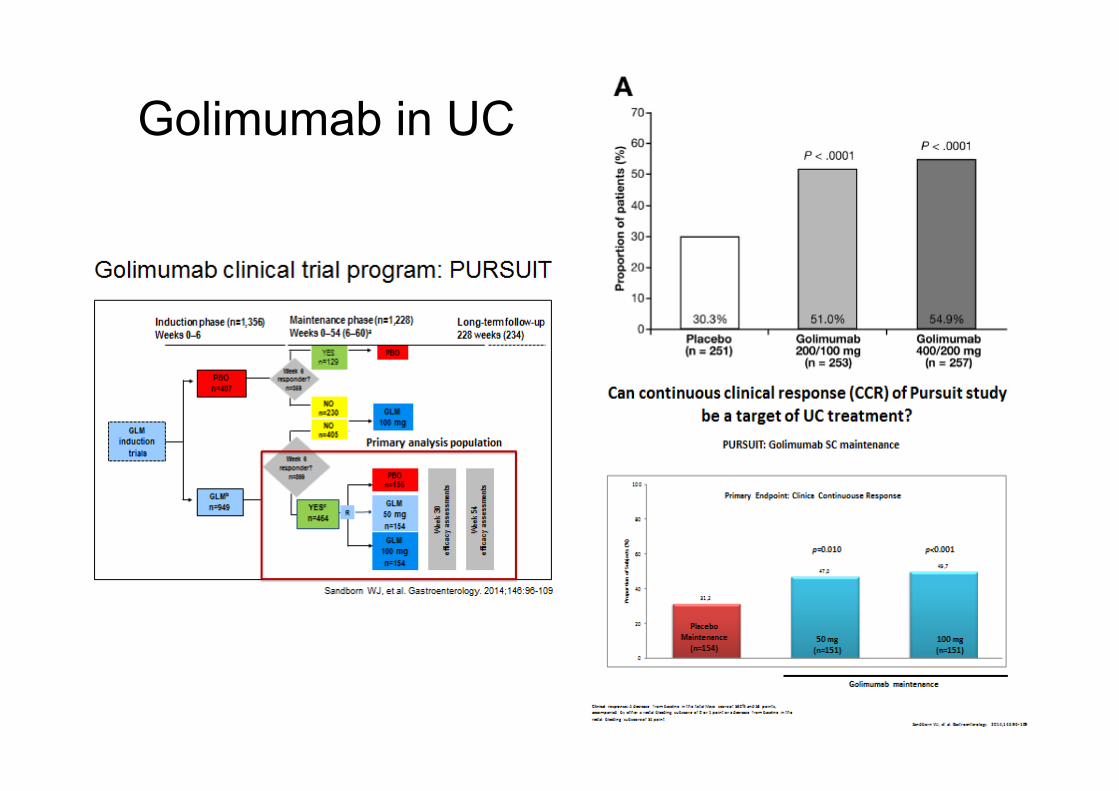
Golimumab in UC
Anti-TNF biosimilars § Infliximab Biosimilars:
§ Remsima or Inflectra (CT-P13, Celltrion) § Flixabi (SB2, Samsung Bioepis) § Zessly (L04AB02, Sandoz) positive CHMP opinion in March
2018
§ Adalimumab Biosimilars: § ABP-501 (Amgevita, Amgen) FDA approval in Sept 2016 § Amgevita and Solymbic (Amgen) positive CHMP opinion in
Jan 2017 § Imraldi (Samsung Bioepis) positive CHMP opinion in Aug
2017 § Cyltezo (Boehringer Ingelheim) FDA approval in Sept 2017
*DaneseS,etal,NatRevGastroenterolHepatol.2016Oct12.doi:10.1038/nrgastro.2016.155.
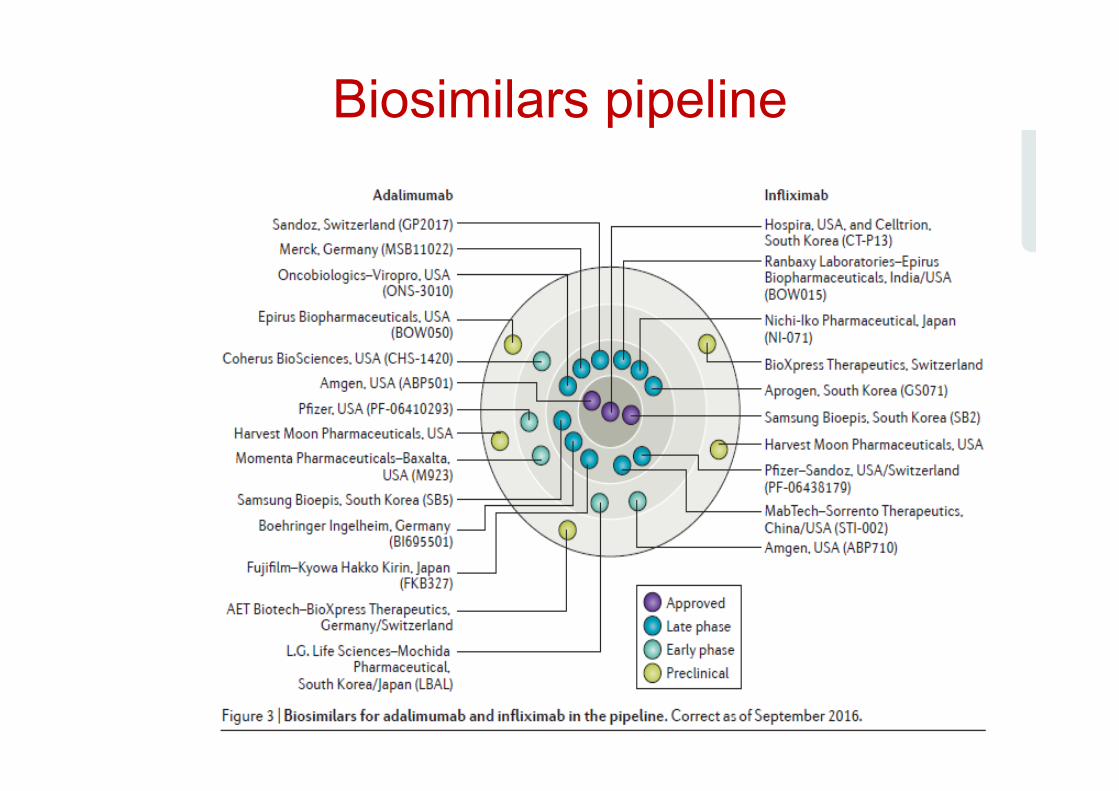
Biosimilars pipeline
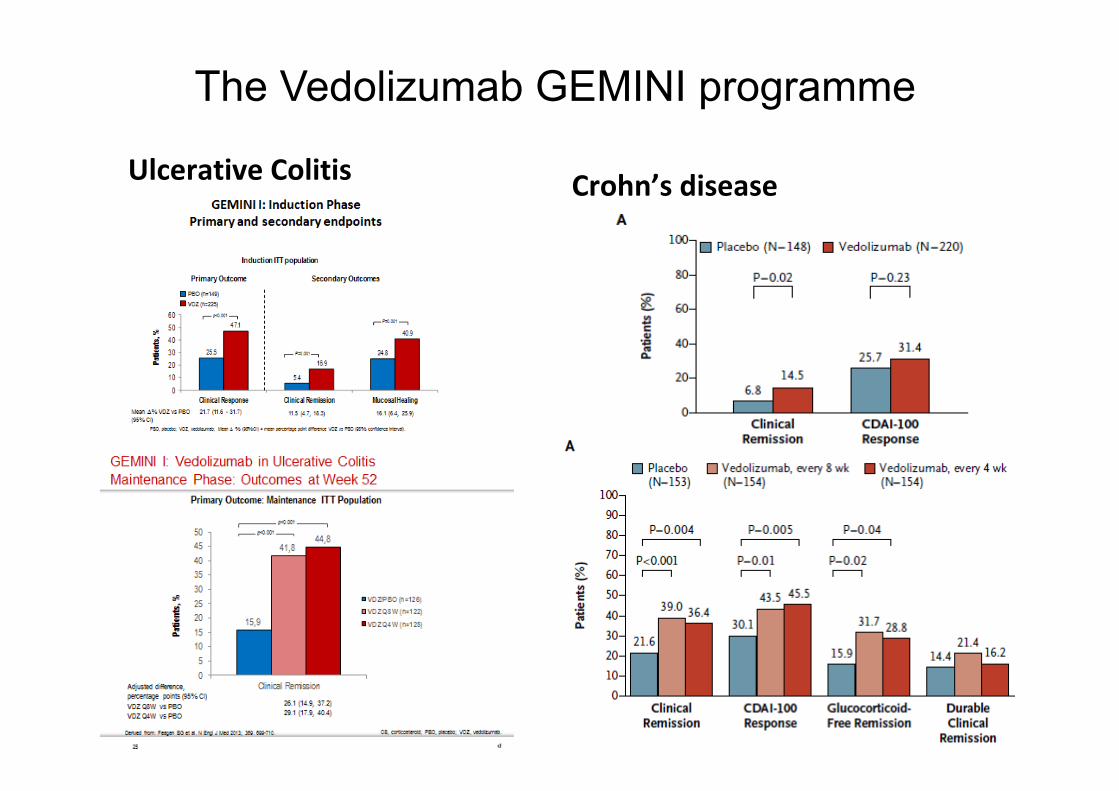
The Vedolizumab GEMINI programme
UlcerativeColitis Crohn’sdisease
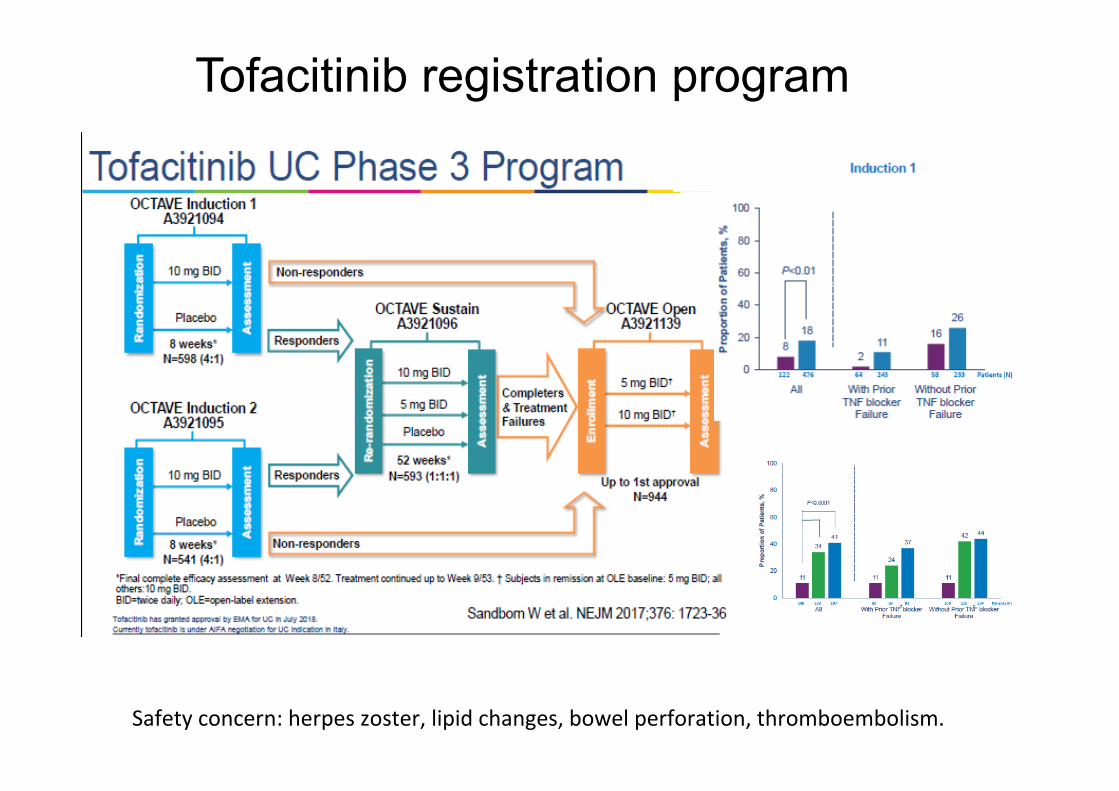
Tofacitinib registration program
Safetyconcern:herpeszoster,lipidchanges,bowelperforation,thromboembolism.
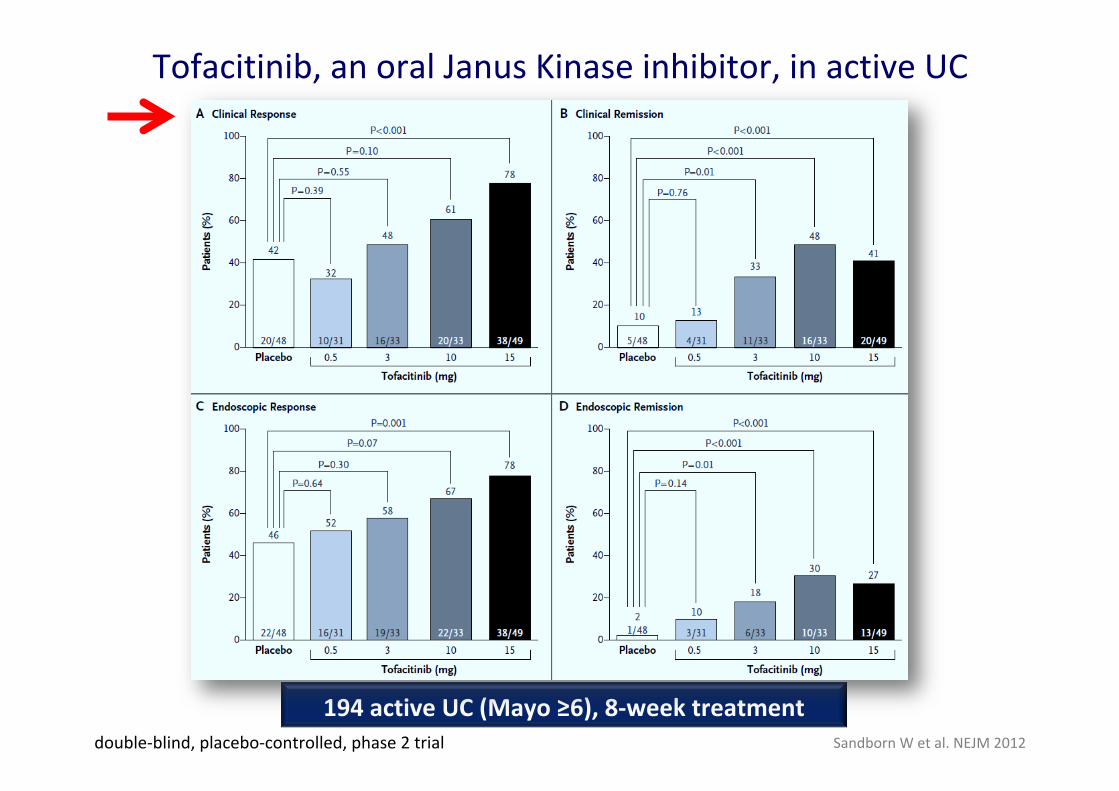
Tofacitinib,anoralJanusKinaseinhibitor,inactiveUC
SandbornWetal.NEJM2012
194activeUC(Mayo≥6),8-weektreatmentdouble-blind,placebo-controlled,phase2trial
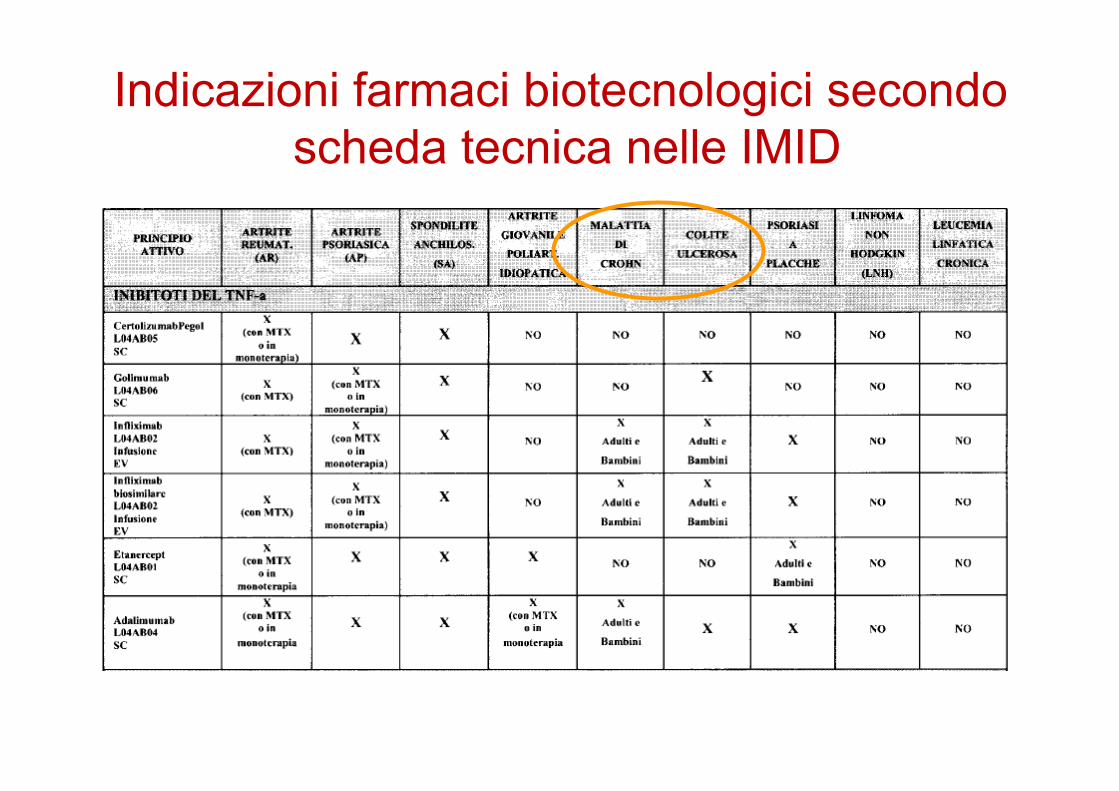
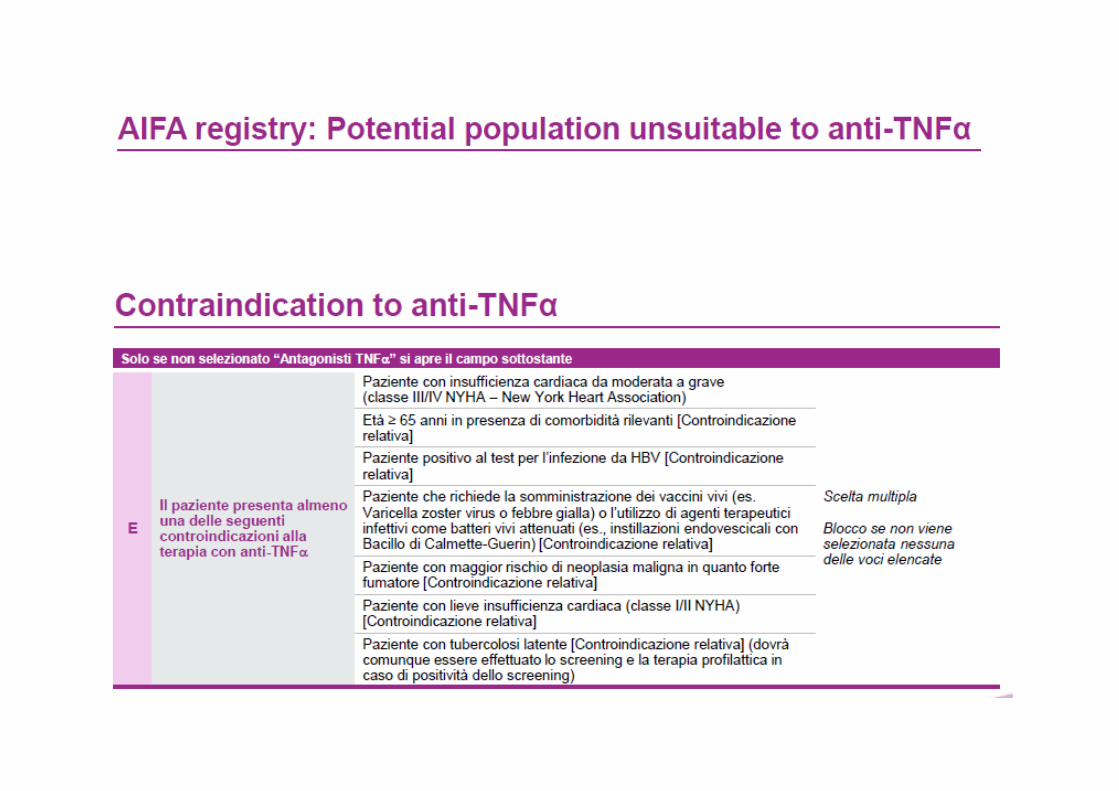
Indicazioni farmaci biotecnologici secondo scheda tecnica nelle IMID
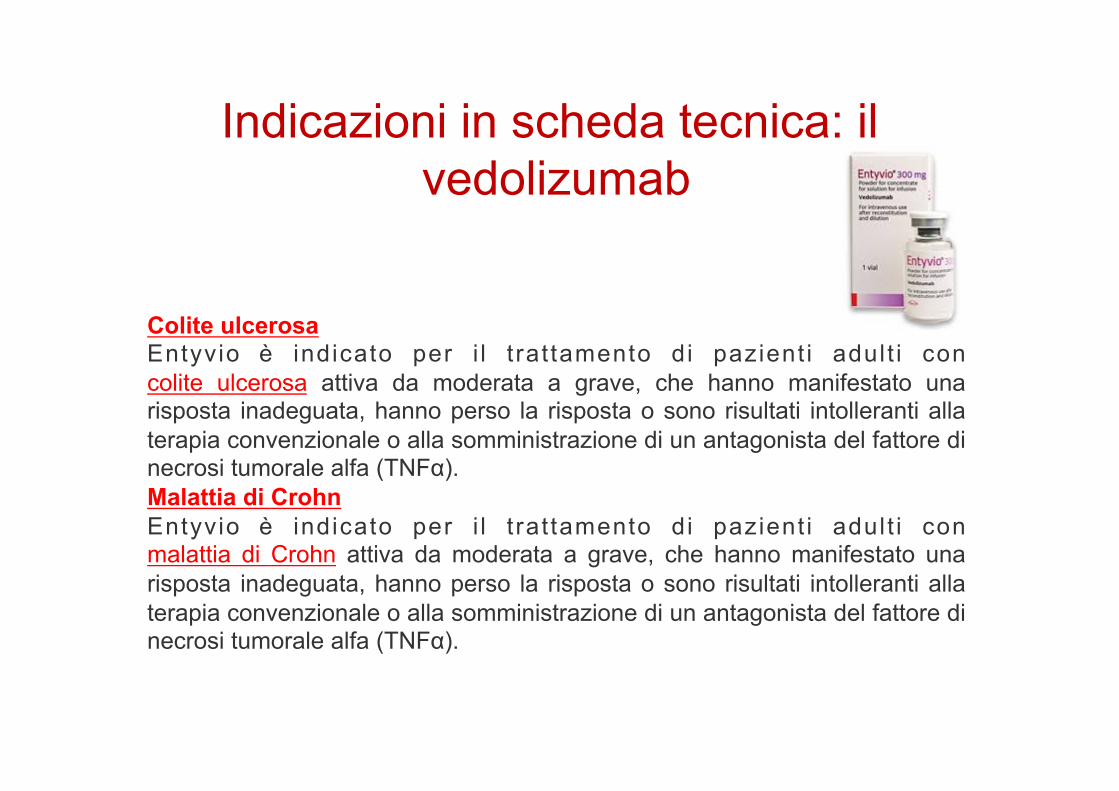
Indicazioni in scheda tecnica: il vedolizumab
Colite ulcerosa Entyvio è indicato per i l t rat tamento di pazient i adult i con colite ulcerosa attiva da moderata a grave, che hanno manifestato una risposta inadeguata, hanno perso la risposta o sono risultati intolleranti alla terapia convenzionale o alla somministrazione di un antagonista del fattore di necrosi tumorale alfa (TNFα). Malattia di Crohn Entyvio è indicato per i l t rat tamento di pazient i adult i con malattia di Crohn attiva da moderata a grave, che hanno manifestato una risposta inadeguata, hanno perso la risposta o sono risultati intolleranti alla terapia convenzionale o alla somministrazione di un antagonista del fattore di necrosi tumorale alfa (TNFα).
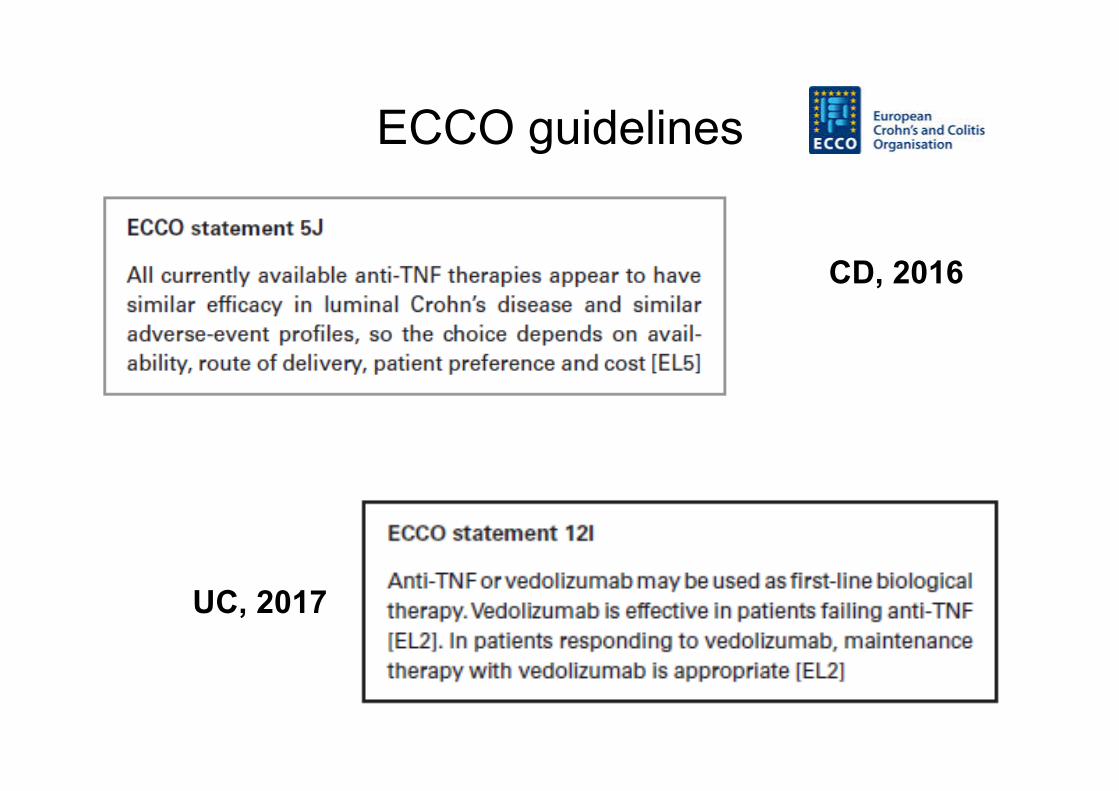
ECCO guidelines
UC, 2017
CD, 2016
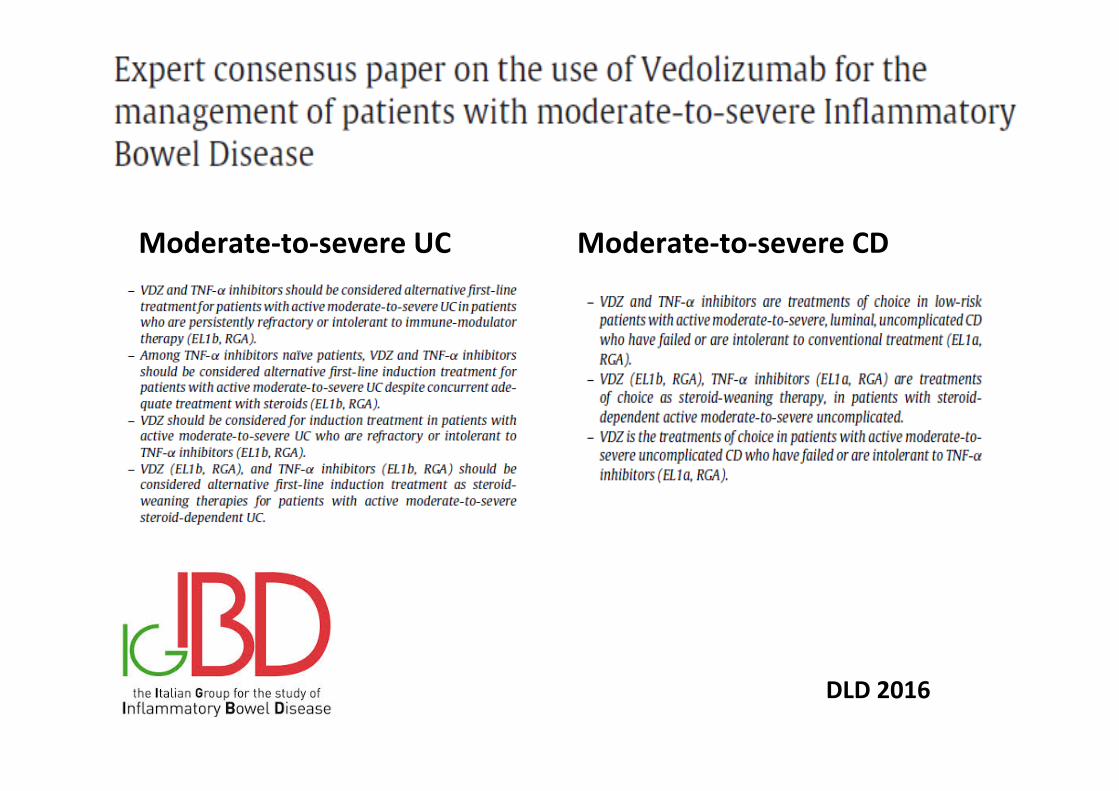
Moderate-to-severeUC Moderate-to-severeCD
DLD2016
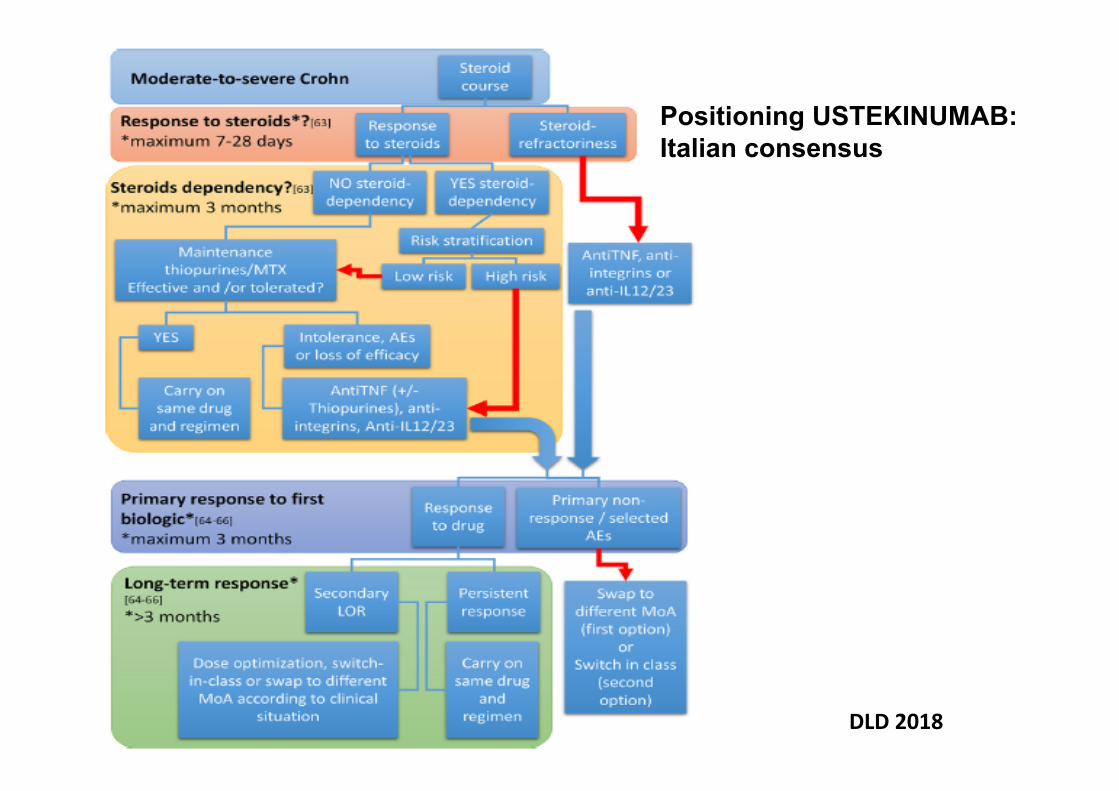
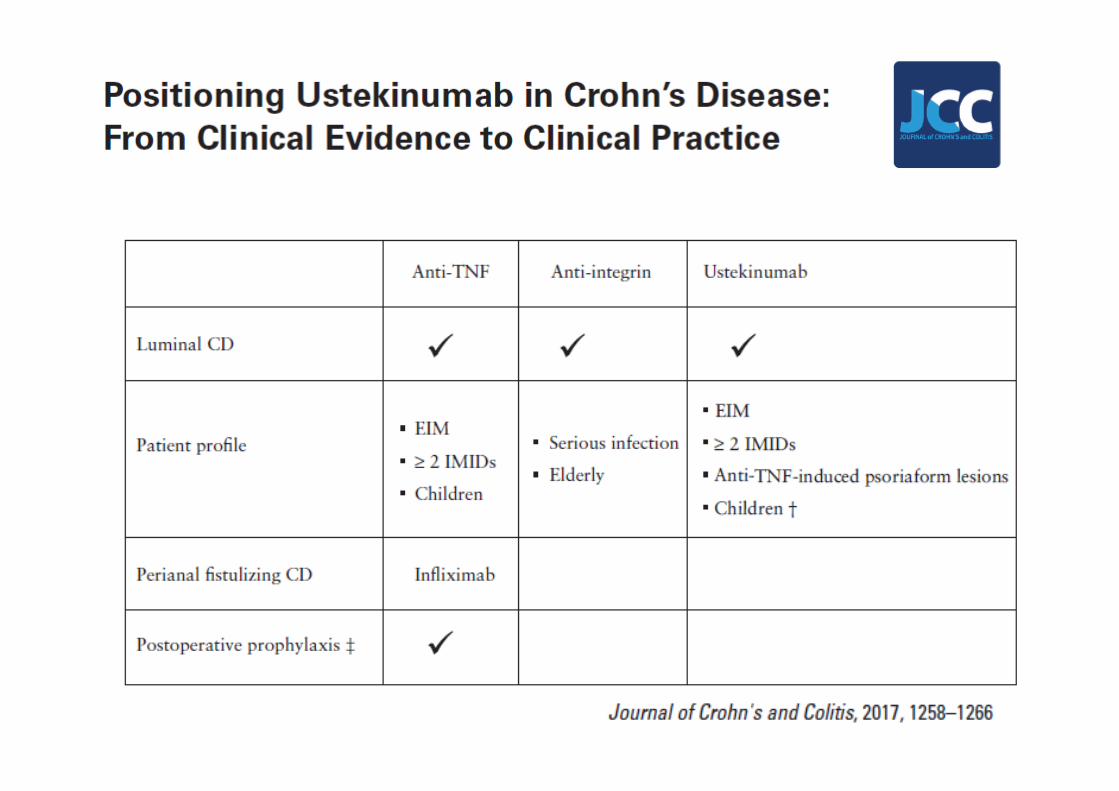
Positioning USTEKINUMAB: Italian consensus
DLD2018
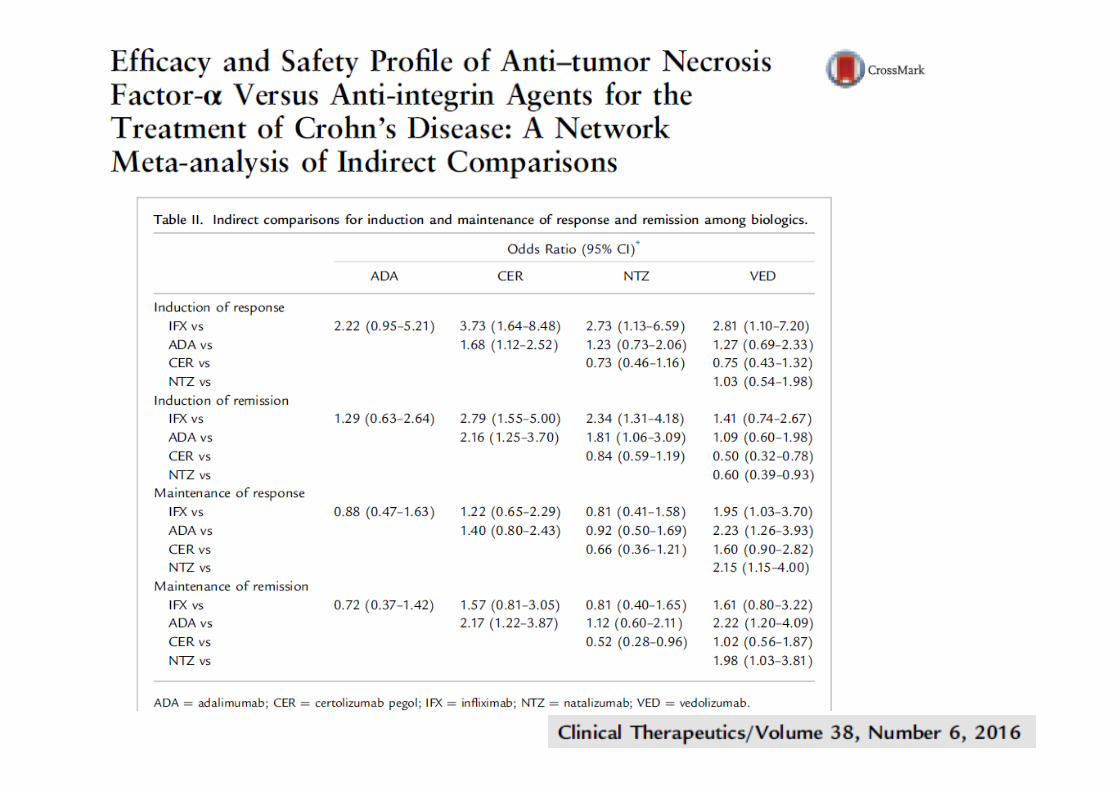
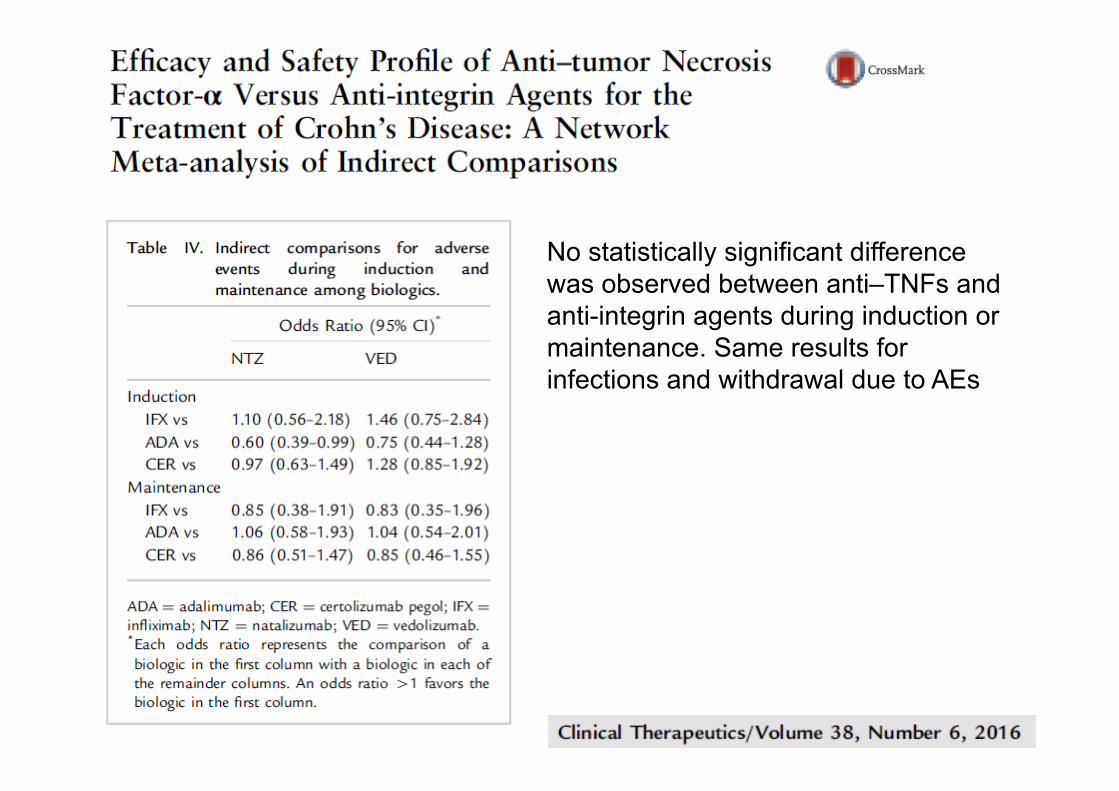
No statistically significant difference was observed between anti–TNFs and anti-integrin agents during induction or maintenance. Same results for infections and withdrawal due to AEs
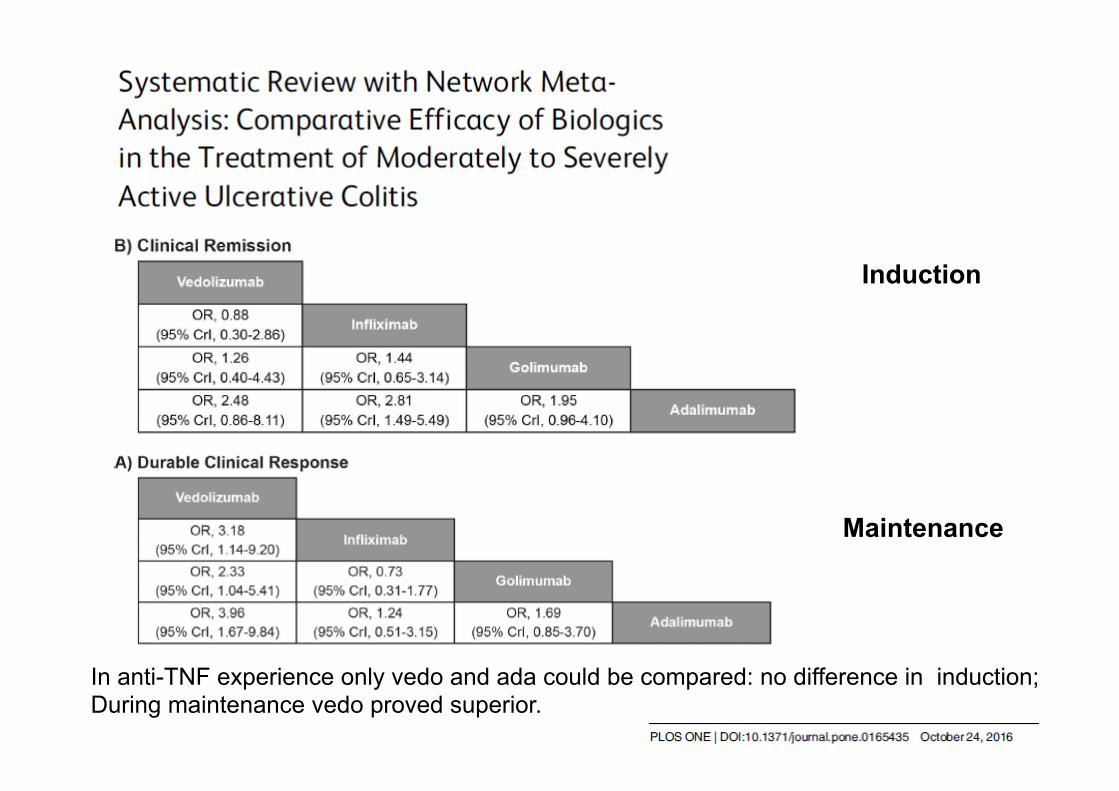
Induction
Maintenance
In anti-TNF experience only vedo and ada could be compared: no difference in induction; During maintenance vedo proved superior.
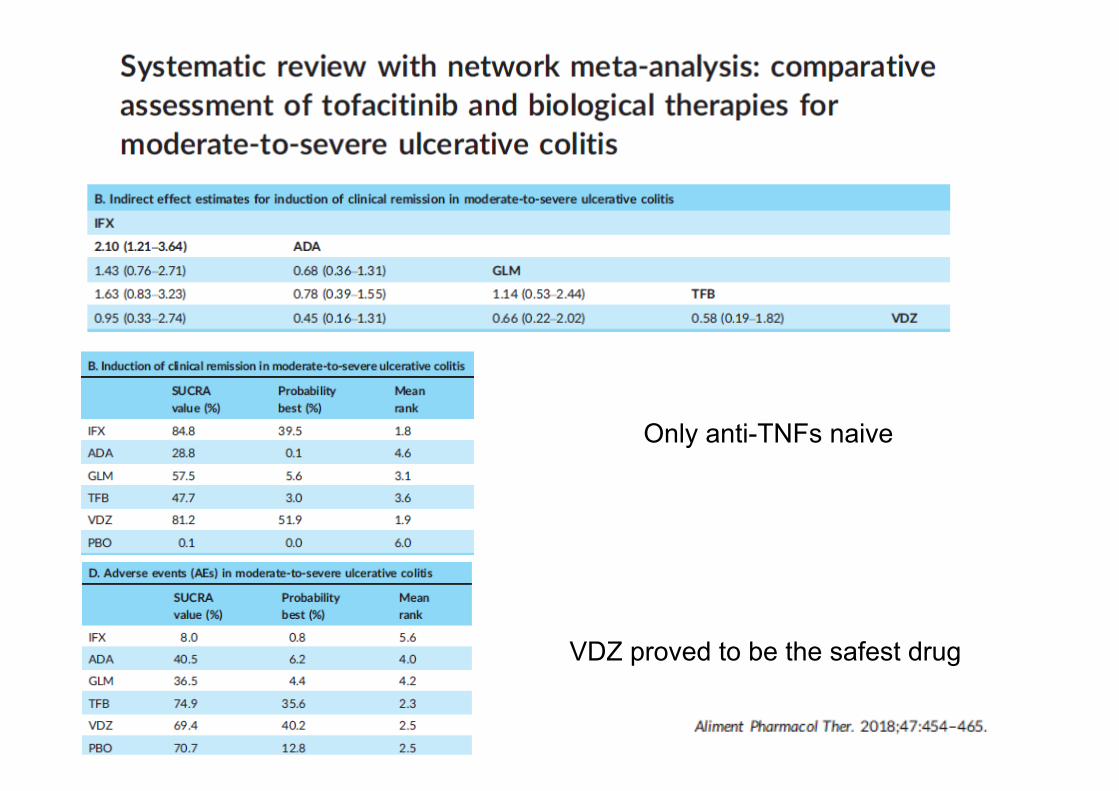
Only anti-TNFs naive
VDZ proved to be the safest drug
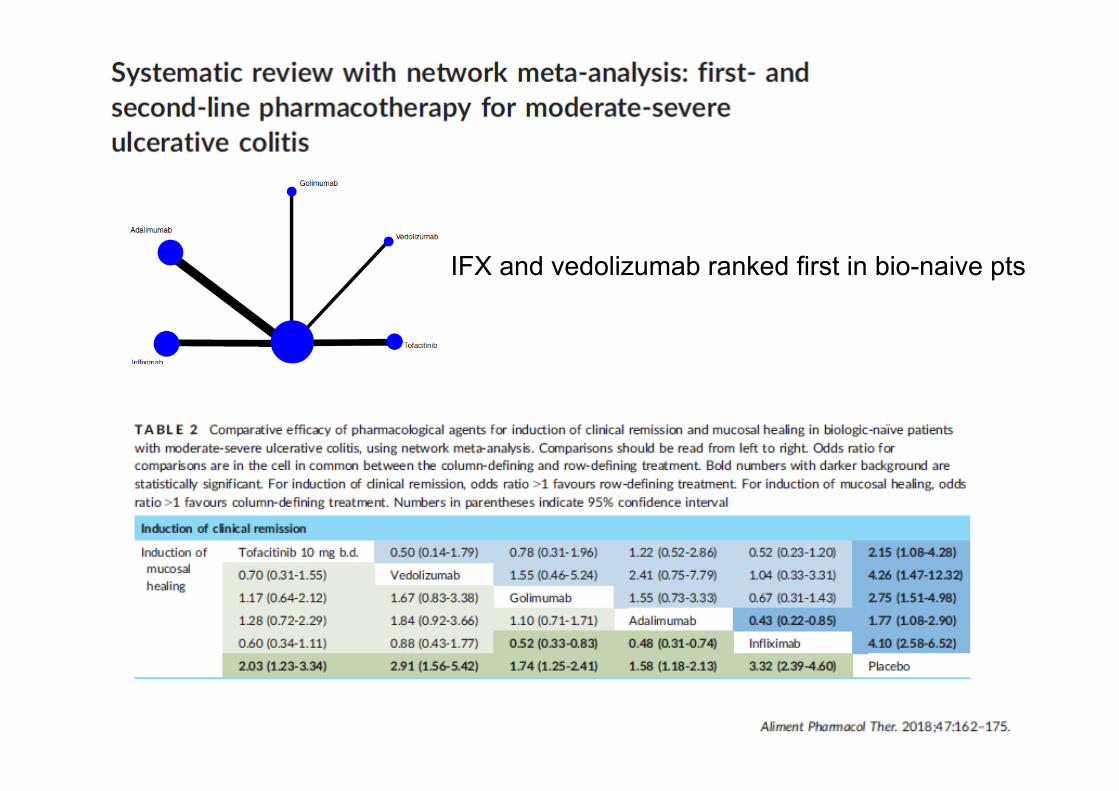
IFX and vedolizumab ranked first in bio-naive pts
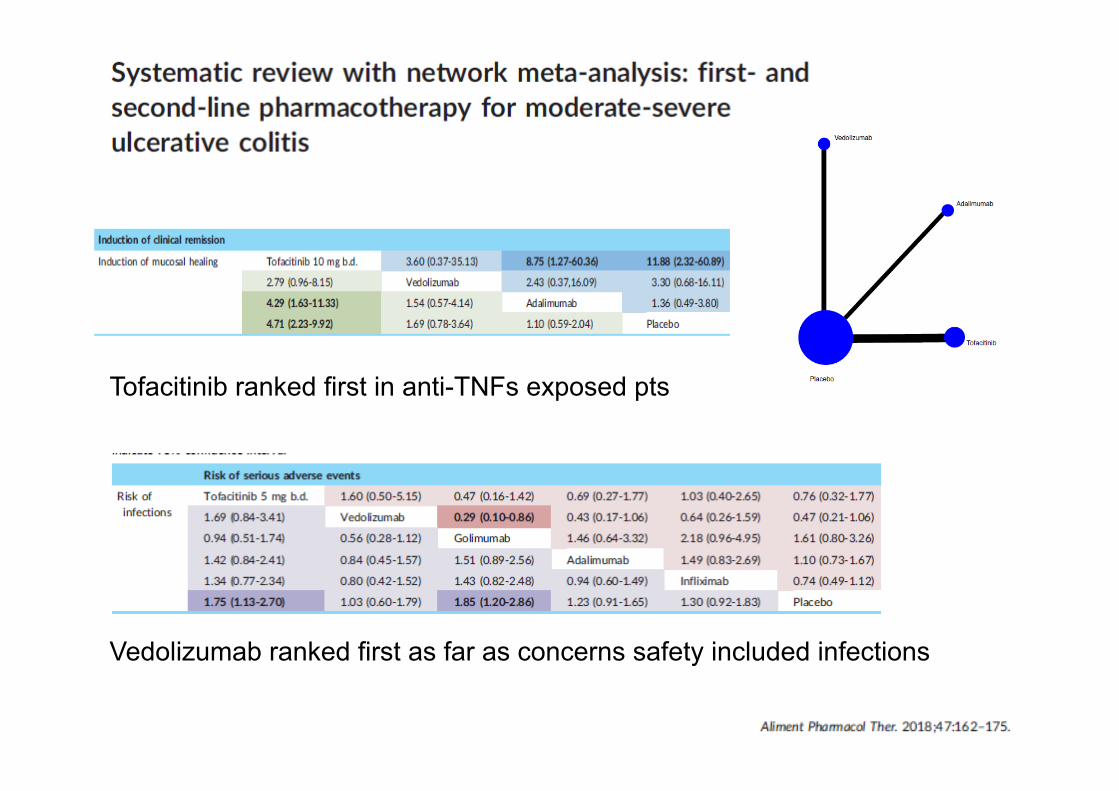
Vedolizumab ranked first as far as concerns safety included infections
Tofacitinib ranked first in anti-TNFs exposed pts
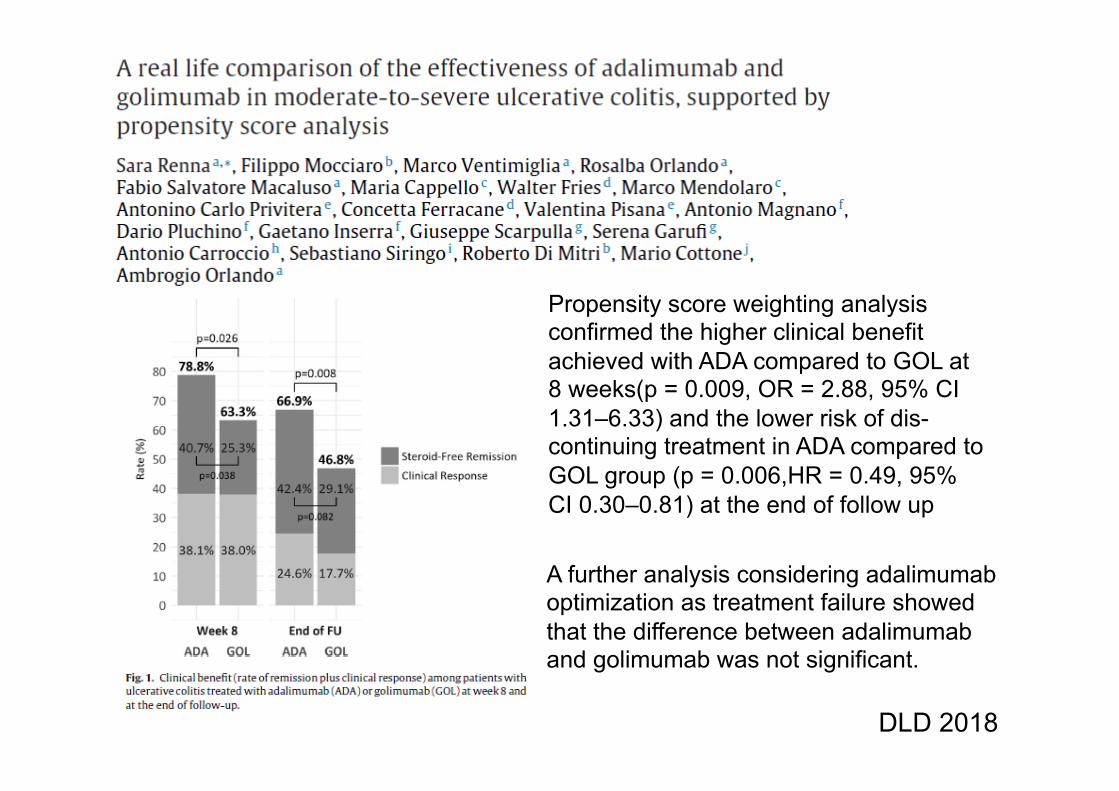
DLD 2018
A further analysis considering adalimumab optimization as treatment failure showed that the difference between adalimumab and golimumab was not significant.
Propensity score weighting analysis confirmed the higher clinical benefit achieved with ADA compared to GOL at 8 weeks(p = 0.009, OR = 2.88, 95% CI 1.31–6.33) and the lower risk of dis-continuing treatment in ADA compared to GOL group (p = 0.006,HR = 0.49, 95% CI 0.30–0.81) at the end of follow up
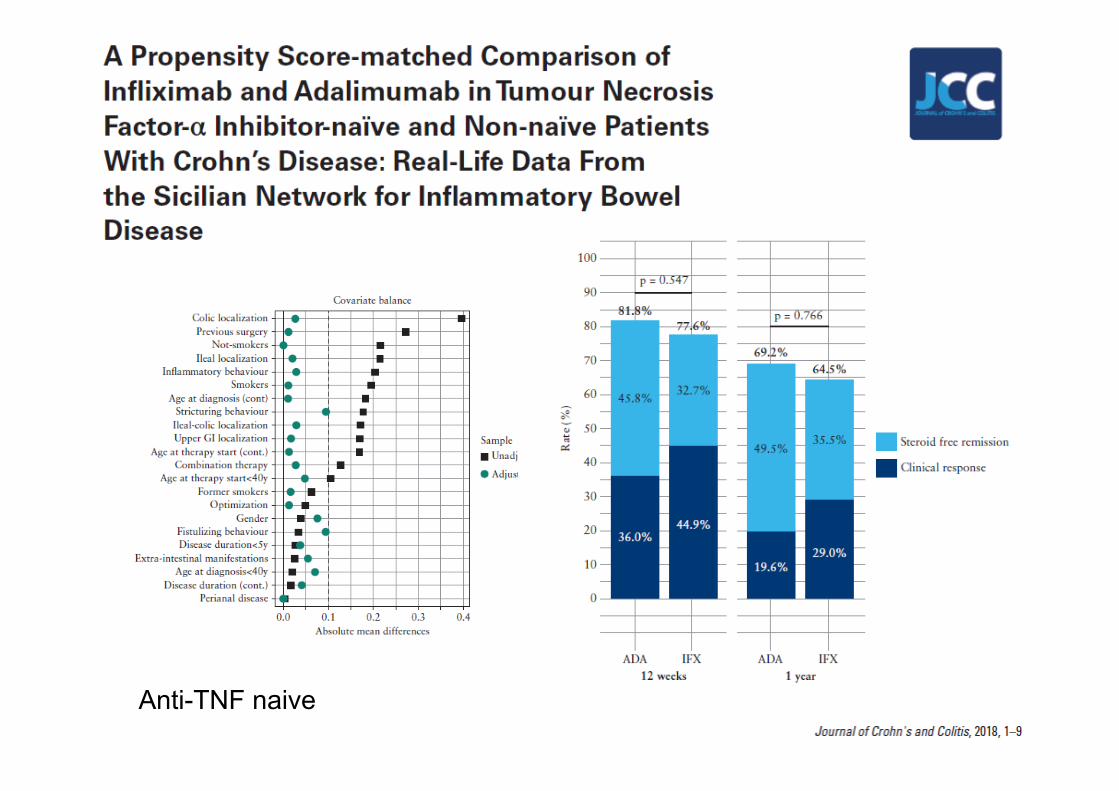
Anti-TNF naive
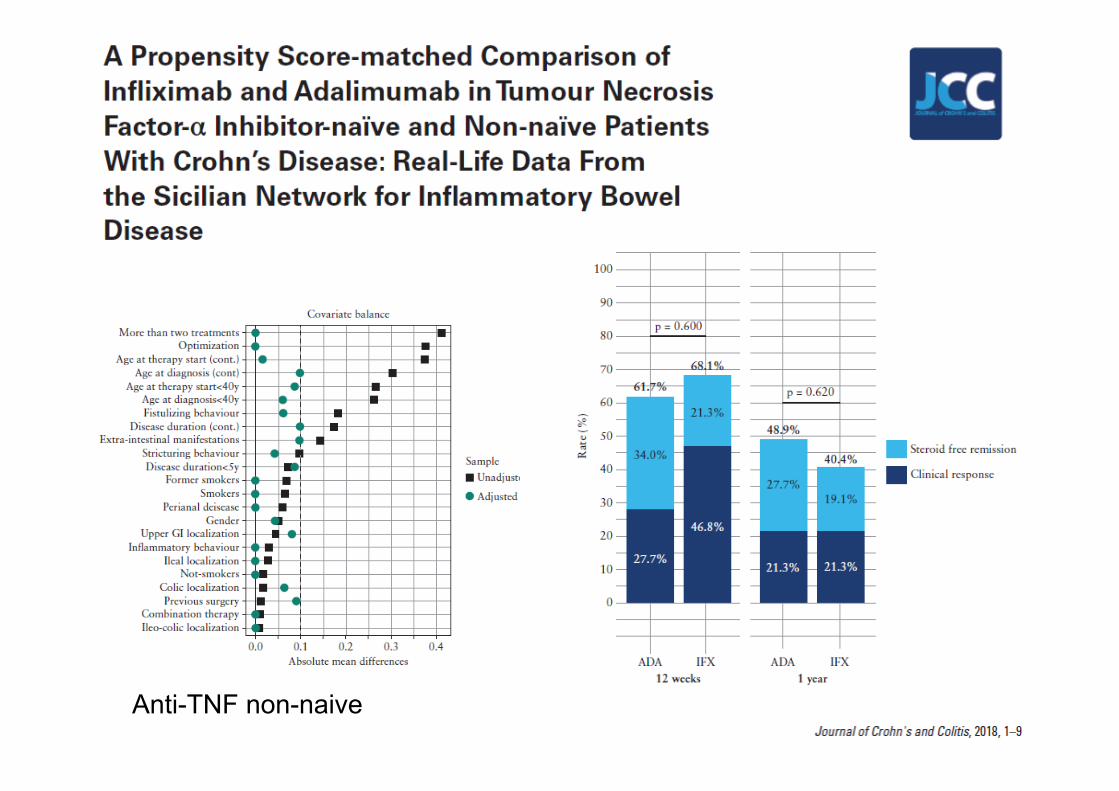
Anti-TNF non-naive

M.Bohmetal.-ECCO2018–OP025
12months
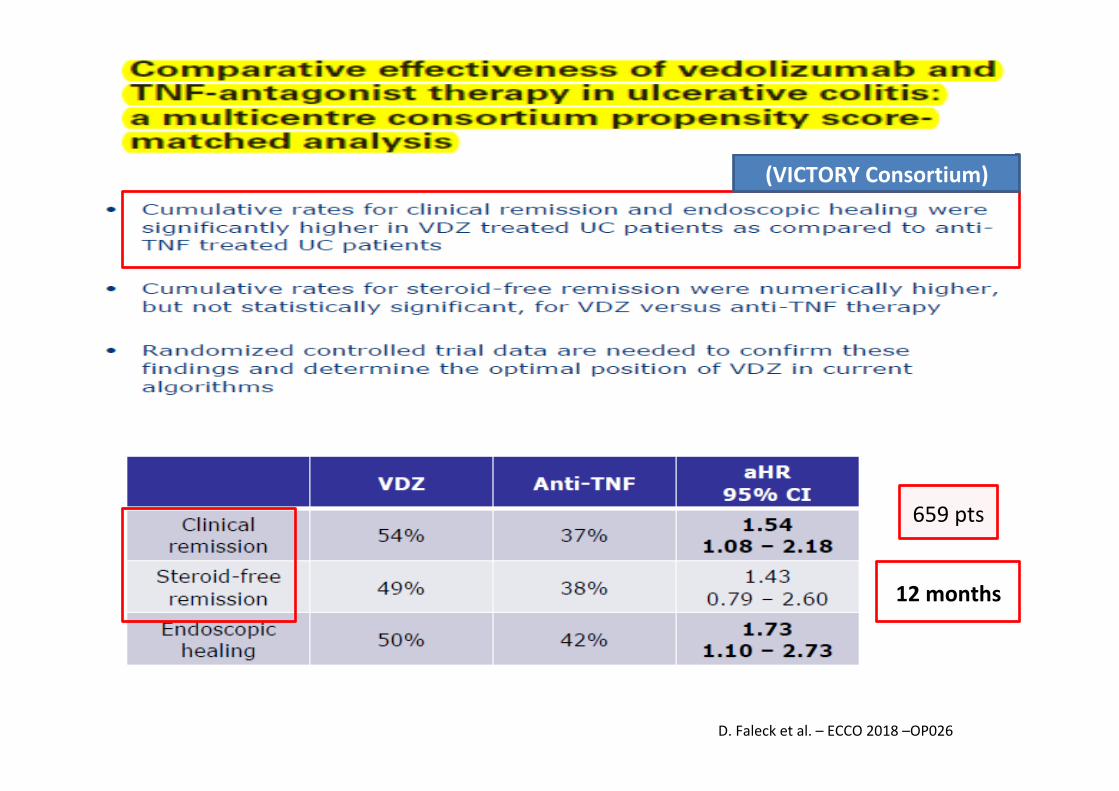
(VICTORYConsortium)
538pts
12months
D.Falecketal.–ECCO2018–OP026
(VICTORYConsortium)
659pts
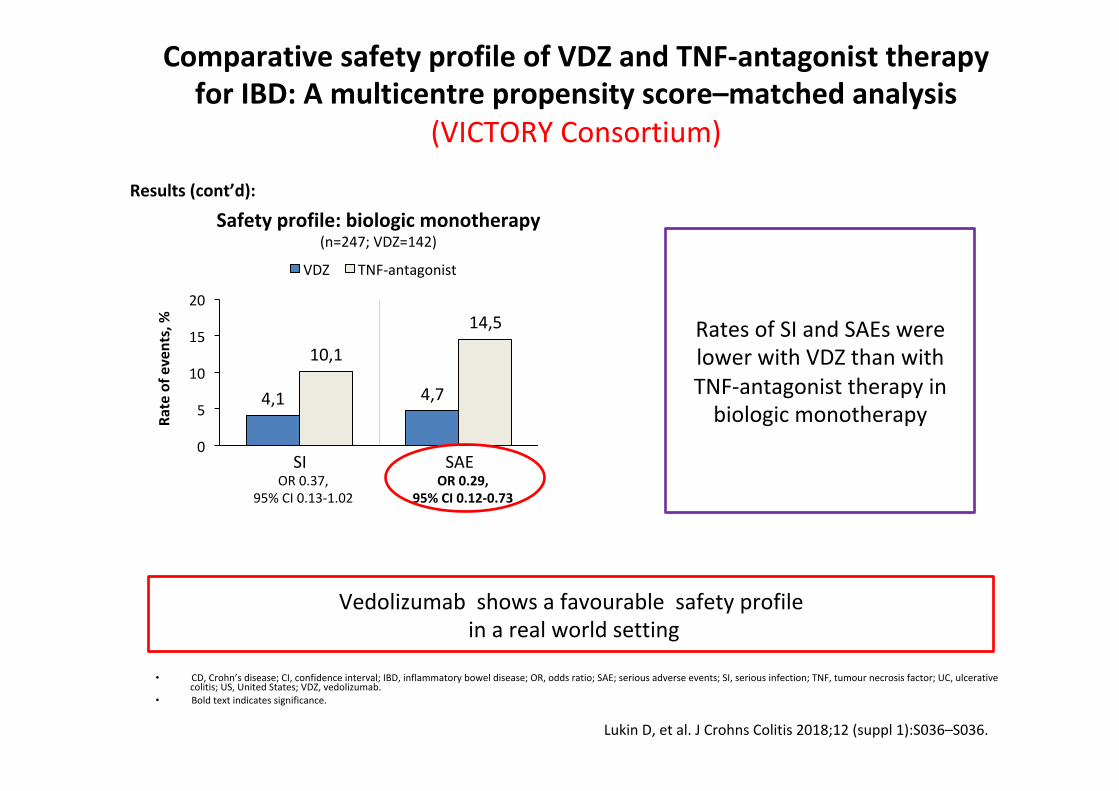
ComparativesafetyprofileofVDZandTNF-antagonisttherapyforIBD:Amulticentrepropensityscore–matchedanalysis
(VICTORYConsortium)
• CD,Crohn’sdisease;CI,confidenceinterval;IBD,inflammatoryboweldisease;OR,oddsratio;SAE;seriousadverseevents;SI,seriousinfection;TNF,tumournecrosisfactor;UC,ulcerativecolitis;US,UnitedStates;VDZ,vedolizumab.
• Boldtextindicatessignificance.
LukinD,etal.JCrohnsColitis2018;12(suppl1):S036–S036.
4,1 4,7
10,1
14,5
0
5
10
15
20
SI SAE
VDZ TNF-antagonist
Results(cont’d):Ra
teofe
vents,%
Safetyprofile:biologicmonotherapy(n=247;VDZ=142)
SIOR0.37,
95%CI0.13-1.02OR0.29,
95%CI0.12-0.73
SAE
RatesofSIandSAEswerelowerwithVDZthanwithTNF-antagonisttherapyinbiologicmonotherapy
Vedolizumabshowsafavourablesafetyprofileinarealworldsetting
ECCO2019-OP34
Thefirsttrialhead-to-headinIBD
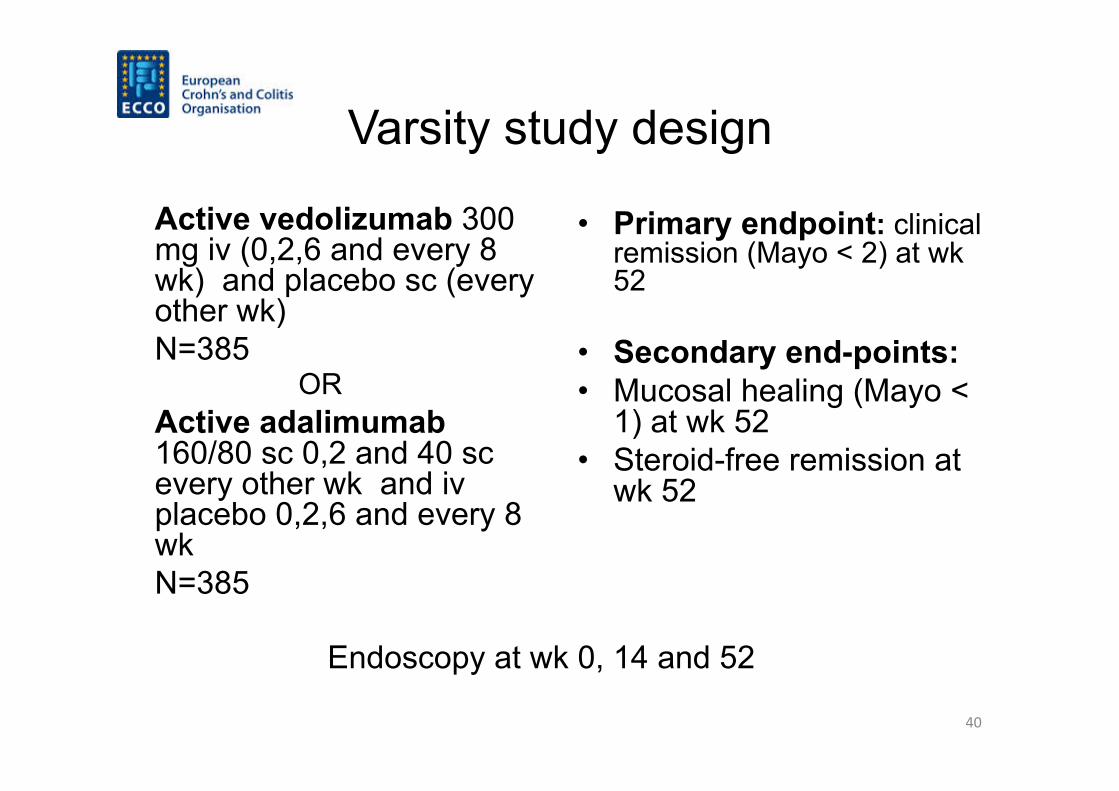
Varsity study design
Active vedolizumab 300 mg iv (0,2,6 and every 8 wk) and placebo sc (every other wk) N=385
OR Active adalimumab 160/80 sc 0,2 and 40 sc every other wk and iv placebo 0,2,6 and every 8 wk N=385
• Primary endpoint: clinical remission (Mayo < 2) at wk 52
• Secondary end-points: • Mucosal healing (Mayo <
1) at wk 52 • Steroid-free remission at
wk 52
Endoscopy at wk 0, 14 and 52
40
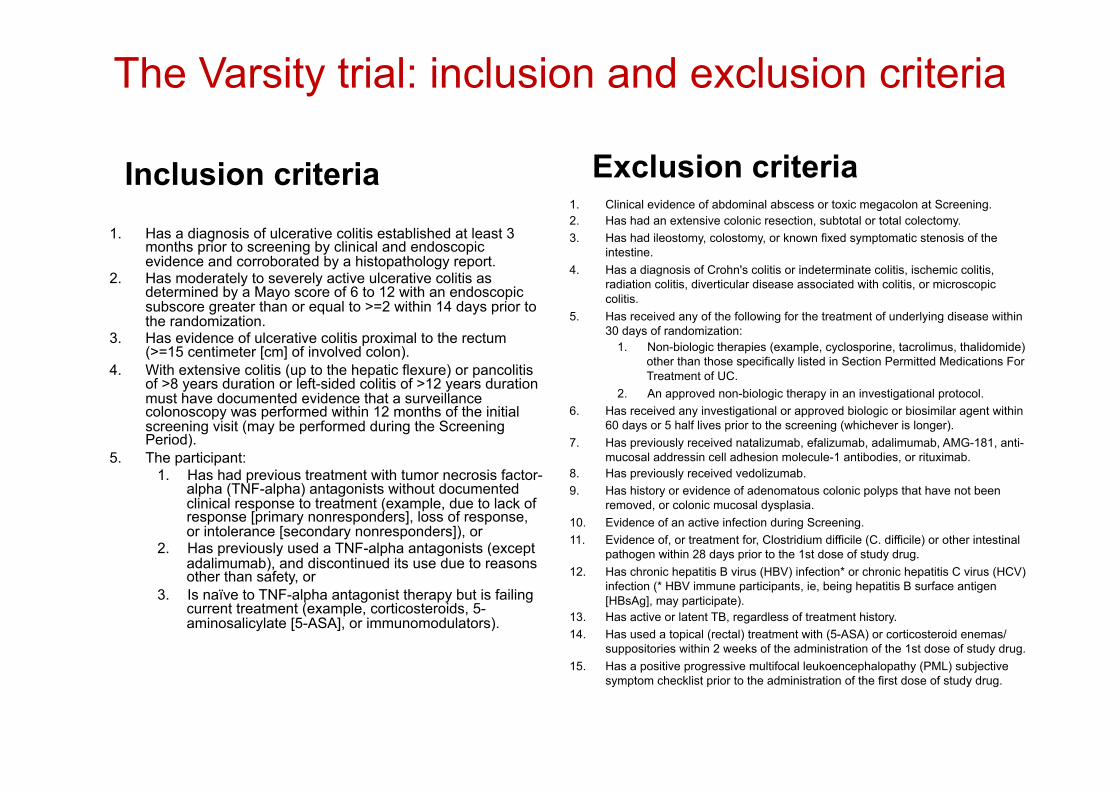
The Varsity trial: inclusion and exclusion criteria
Inclusion criteria 1. Has a diagnosis of ulcerative colitis established at least 3
months prior to screening by clinical and endoscopic evidence and corroborated by a histopathology report.
2. Has moderately to severely active ulcerative colitis as determined by a Mayo score of 6 to 12 with an endoscopic subscore greater than or equal to >=2 within 14 days prior to the randomization.
3. Has evidence of ulcerative colitis proximal to the rectum (>=15 centimeter [cm] of involved colon).
4. With extensive colitis (up to the hepatic flexure) or pancolitis of >8 years duration or left-sided colitis of >12 years duration must have documented evidence that a surveillance colonoscopy was performed within 12 months of the initial screening visit (may be performed during the Screening Period).
5. The participant: 1. Has had previous treatment with tumor necrosis factor-
alpha (TNF-alpha) antagonists without documented clinical response to treatment (example, due to lack of response [primary nonresponders], loss of response, or intolerance [secondary nonresponders]), or
2. Has previously used a TNF-alpha antagonists (except adalimumab), and discontinued its use due to reasons other than safety, or
3. Is naïve to TNF-alpha antagonist therapy but is failing current treatment (example, corticosteroids, 5-aminosalicylate [5-ASA], or immunomodulators).
Exclusion criteria 1. Clinical evidence of abdominal abscess or toxic megacolon at Screening. 2. Has had an extensive colonic resection, subtotal or total colectomy. 3. Has had ileostomy, colostomy, or known fixed symptomatic stenosis of the
intestine. 4. Has a diagnosis of Crohn's colitis or indeterminate colitis, ischemic colitis,
radiation colitis, diverticular disease associated with colitis, or microscopic colitis.
5. Has received any of the following for the treatment of underlying disease within 30 days of randomization:
1. Non-biologic therapies (example, cyclosporine, tacrolimus, thalidomide) other than those specifically listed in Section Permitted Medications For Treatment of UC.
2. An approved non-biologic therapy in an investigational protocol. 6. Has received any investigational or approved biologic or biosimilar agent within
60 days or 5 half lives prior to the screening (whichever is longer). 7. Has previously received natalizumab, efalizumab, adalimumab, AMG-181, anti-
mucosal addressin cell adhesion molecule-1 antibodies, or rituximab. 8. Has previously received vedolizumab. 9. Has history or evidence of adenomatous colonic polyps that have not been
removed, or colonic mucosal dysplasia. 10. Evidence of an active infection during Screening. 11. Evidence of, or treatment for, Clostridium difficile (C. difficile) or other intestinal
pathogen within 28 days prior to the 1st dose of study drug. 12. Has chronic hepatitis B virus (HBV) infection* or chronic hepatitis C virus (HCV)
infection (* HBV immune participants, ie, being hepatitis B surface antigen [HBsAg], may participate).
13. Has active or latent TB, regardless of treatment history. 14. Has used a topical (rectal) treatment with (5-ASA) or corticosteroid enemas/
suppositories within 2 weeks of the administration of the 1st dose of study drug. 15. Has a positive progressive multifocal leukoencephalopathy (PML) subjective
symptom checklist prior to the administration of the first dose of study drug.
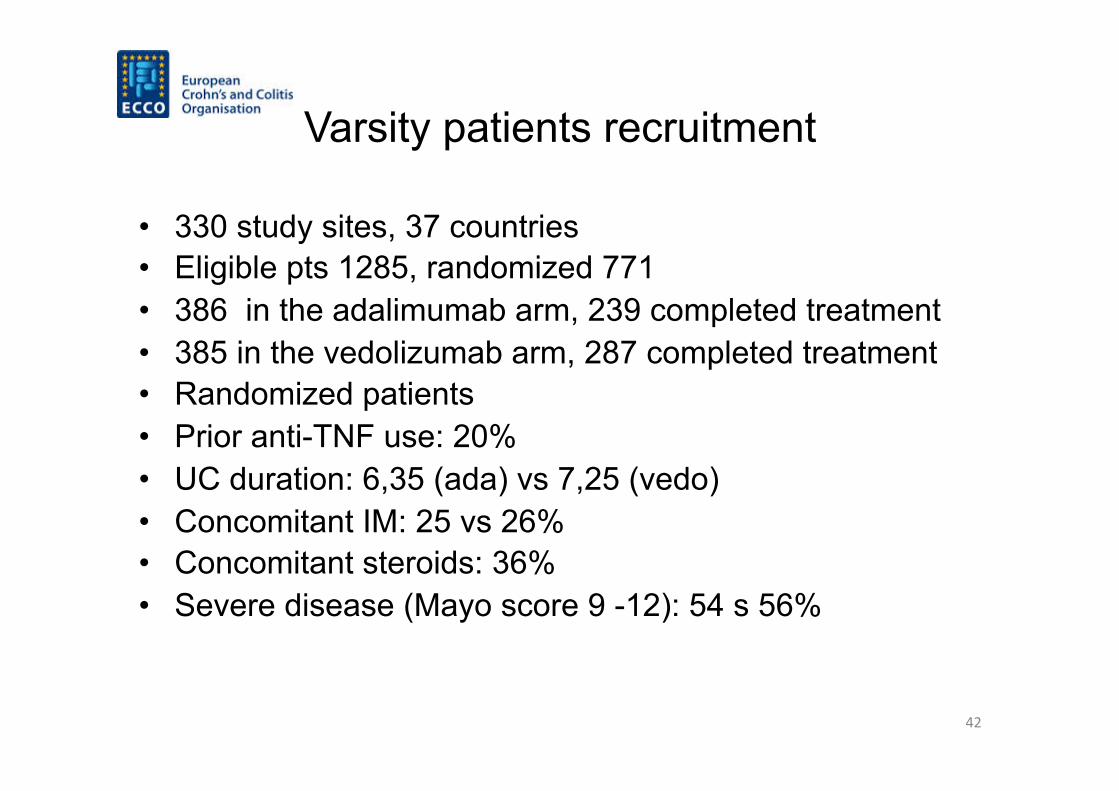
Varsity patients recruitment
• 330 study sites, 37 countries • Eligible pts 1285, randomized 771 • 386 in the adalimumab arm, 239 completed treatment • 385 in the vedolizumab arm, 287 completed treatment • Randomized patients • Prior anti-TNF use: 20% • UC duration: 6,35 (ada) vs 7,25 (vedo) • Concomitant IM: 25 vs 26% • Concomitant steroids: 36% • Severe disease (Mayo score 9 -12): 54 s 56%
42
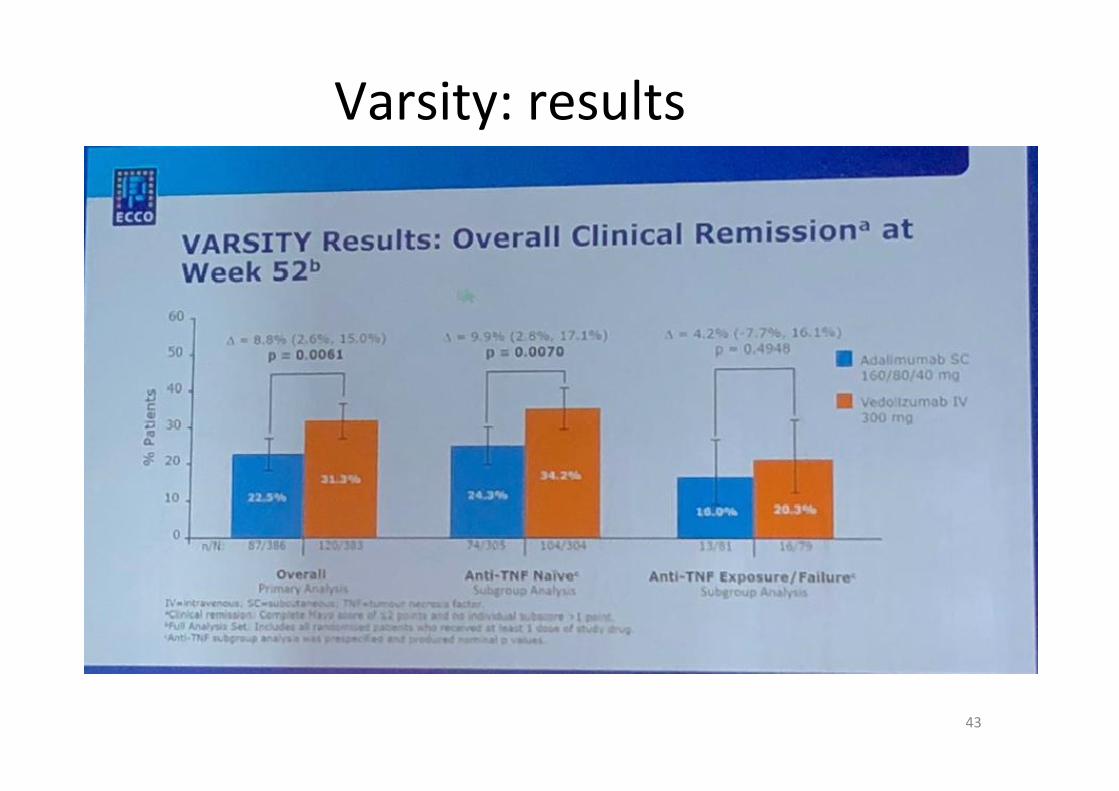
Varsity:results
43
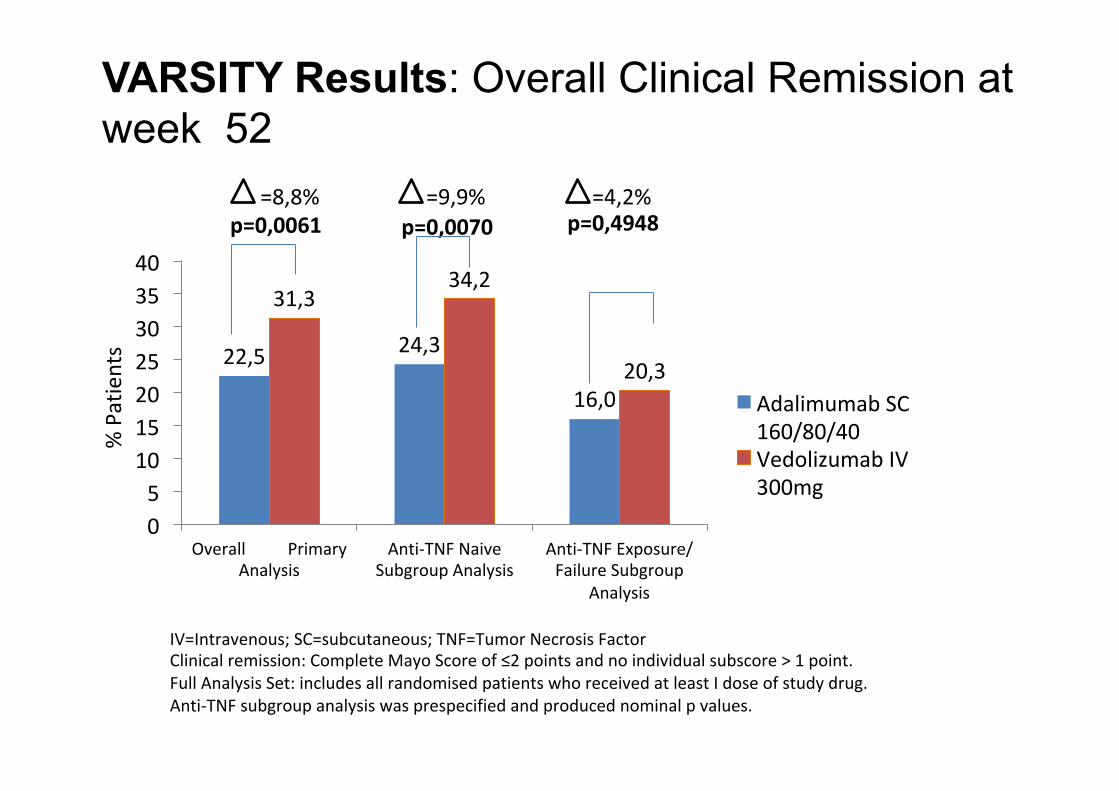
VARSITY Results: Overall Clinical Remission at week 52
22,5 24,3
16,0
31,334,2
20,3
05
10152025303540
OverallPrimaryAnalysis
Anti-TNFNaiveSubgroupAnalysis
Anti-TNFExposure/FailureSubgroup
Analysis
AdalimumabSC160/80/40VedolizumabIV300mg
=8,8%p=0,0061
=9,9% =4,2%p=0,0070 p=0,4948
%Patients
IV=Intravenous;SC=subcutaneous;TNF=TumorNecrosisFactorClinicalremission:CompleteMayoScoreof≤2pointsandnoindividualsubscore>1point.FullAnalysisSet:includesallrandomisedpatientswhoreceivedatleastIdoseofstudydrug.Anti-TNFsubgroupanalysiswasprespecifiedandproducednominalpvalues.
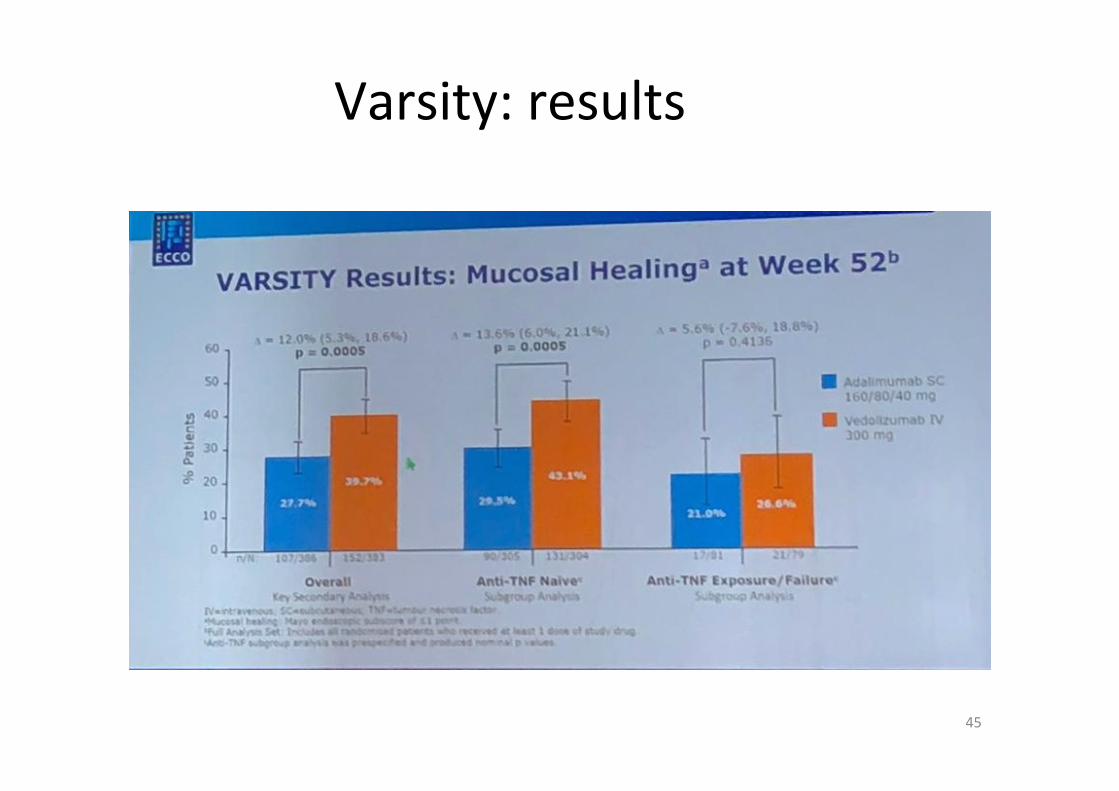
Varsity:results
45
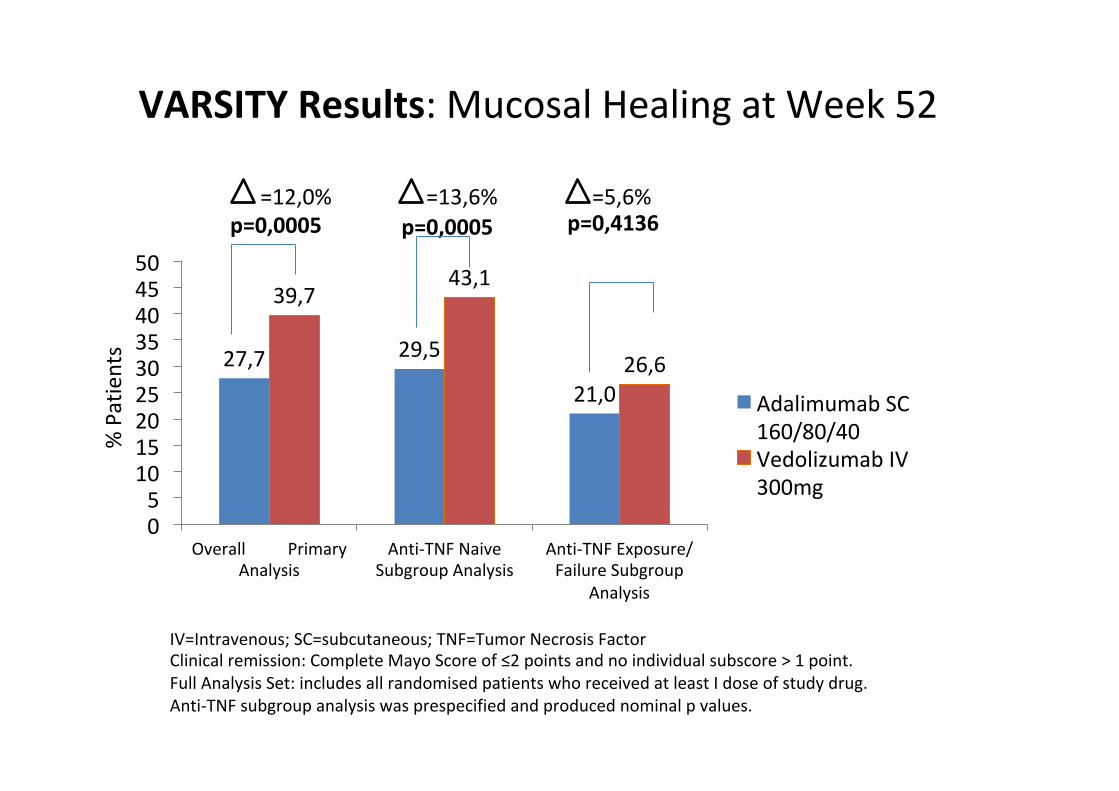
VARSITYResults:MucosalHealingatWeek52
27,7 29,5
21,0
39,743,1
26,6
05
101520253035404550
OverallPrimaryAnalysis
Anti-TNFNaiveSubgroupAnalysis
Anti-TNFExposure/FailureSubgroup
Analysis
AdalimumabSC160/80/40VedolizumabIV300mg
=12,0%p=0,0005
=13,6% =5,6%p=0,0005 p=0,4136
%Patients
IV=Intravenous;SC=subcutaneous;TNF=TumorNecrosisFactorClinicalremission:CompleteMayoScoreof≤2pointsandnoindividualsubscore>1point.FullAnalysisSet:includesallrandomisedpatientswhoreceivedatleastIdoseofstudydrug.Anti-TNFsubgroupanalysiswasprespecifiedandproducednominalpvalues.
Varsity study conclusions
• Superiority of vedo vs ada both in terms of clinical remission and mucosal healing
• Superiority of vedo most pronounced in naive to anti-TNFs
• Treatment differences emerge between wk 6 and 14
• Both drugs safe and well tolerated; serious infections rate higher (NS) in the ADA group
• Results support the use of vedo before anti-TNFs
Biologics in IBD: factors influencing therapeutic choices
Diseasesiteandactivity
Comorbidities
Druginteractions
Age
Adherence
Previoussurgery
EIM
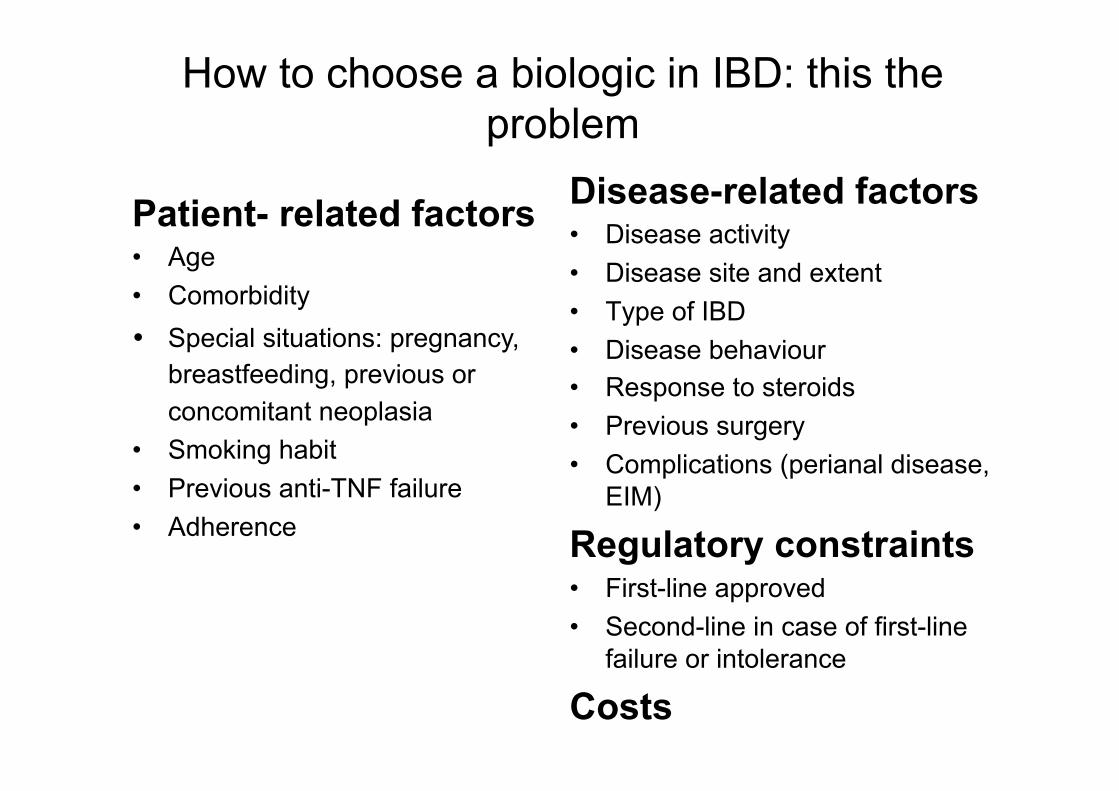
How to choose a biologic in IBD: this the problem
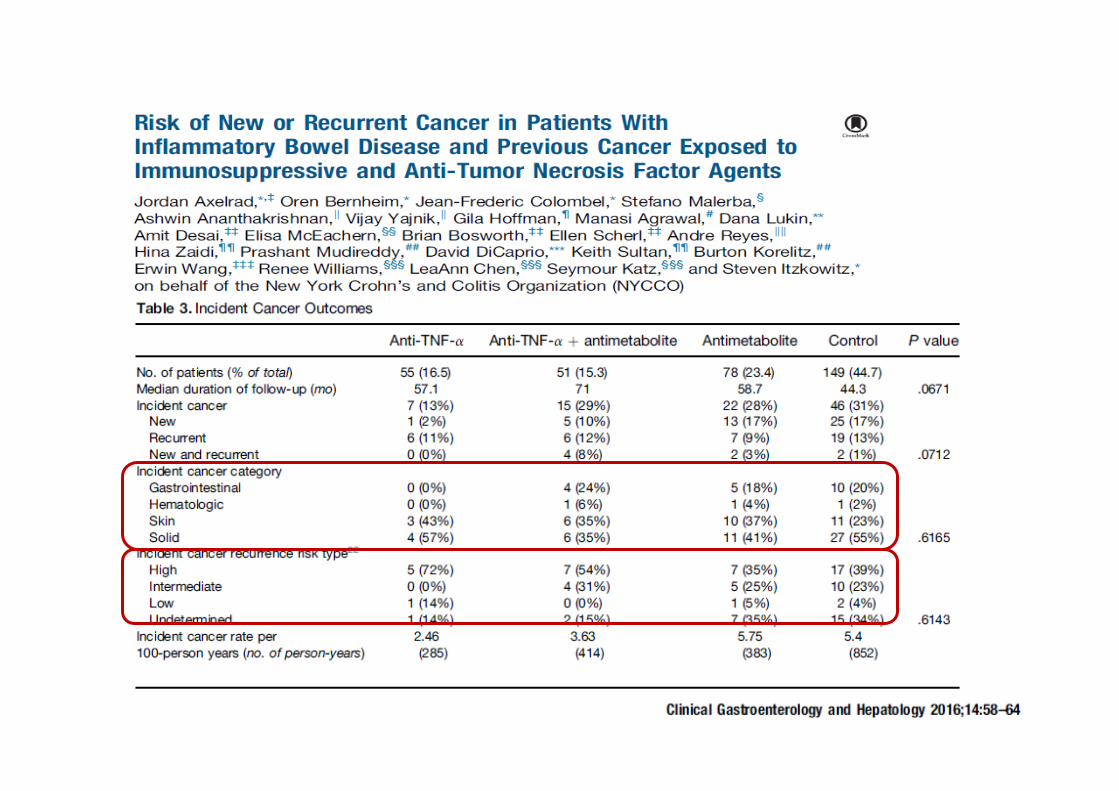
Patient- related factors • Age • Comorbidity • Special situations: pregnancy,
breastfeeding, previous or concomitant neoplasia
• Smoking habit • Previous anti-TNF failure • Adherence
Disease-related factors • Disease activity • Disease site and extent • Type of IBD • Disease behaviour • Response to steroids • Previous surgery • Complications (perianal disease,
EIM)
Regulatory constraints • First-line approved • Second-line in case of first-line
failure or intolerance
Costs
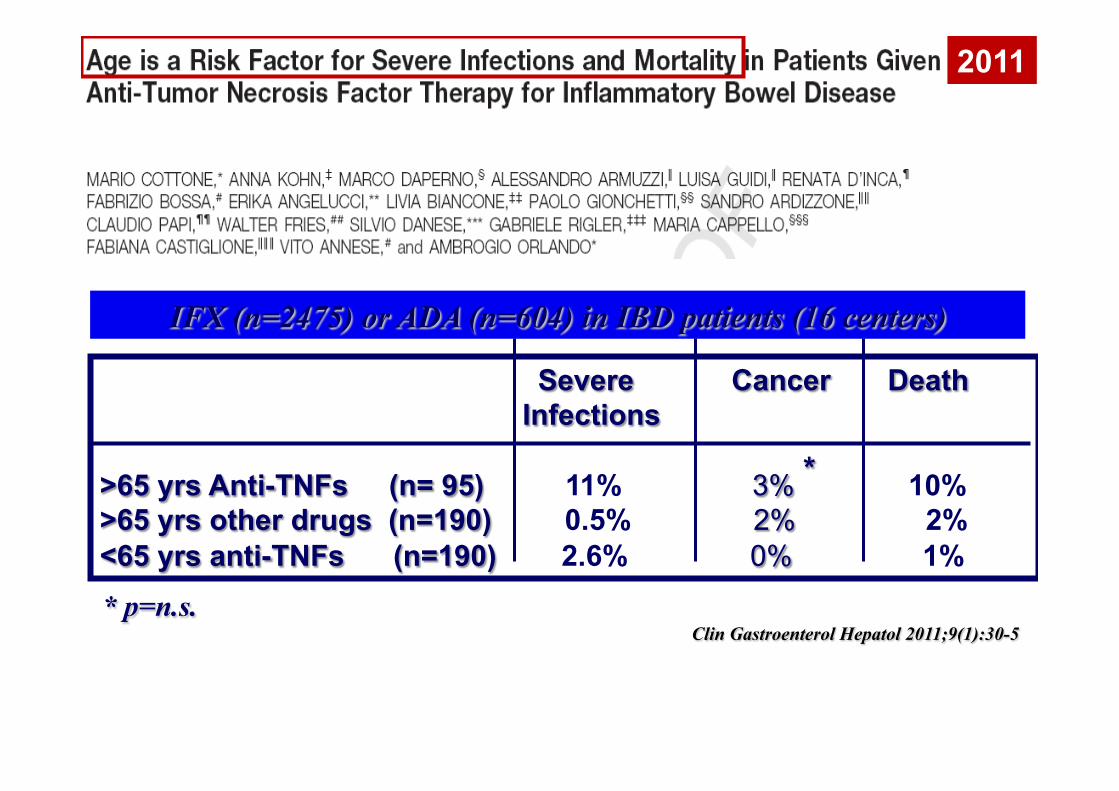
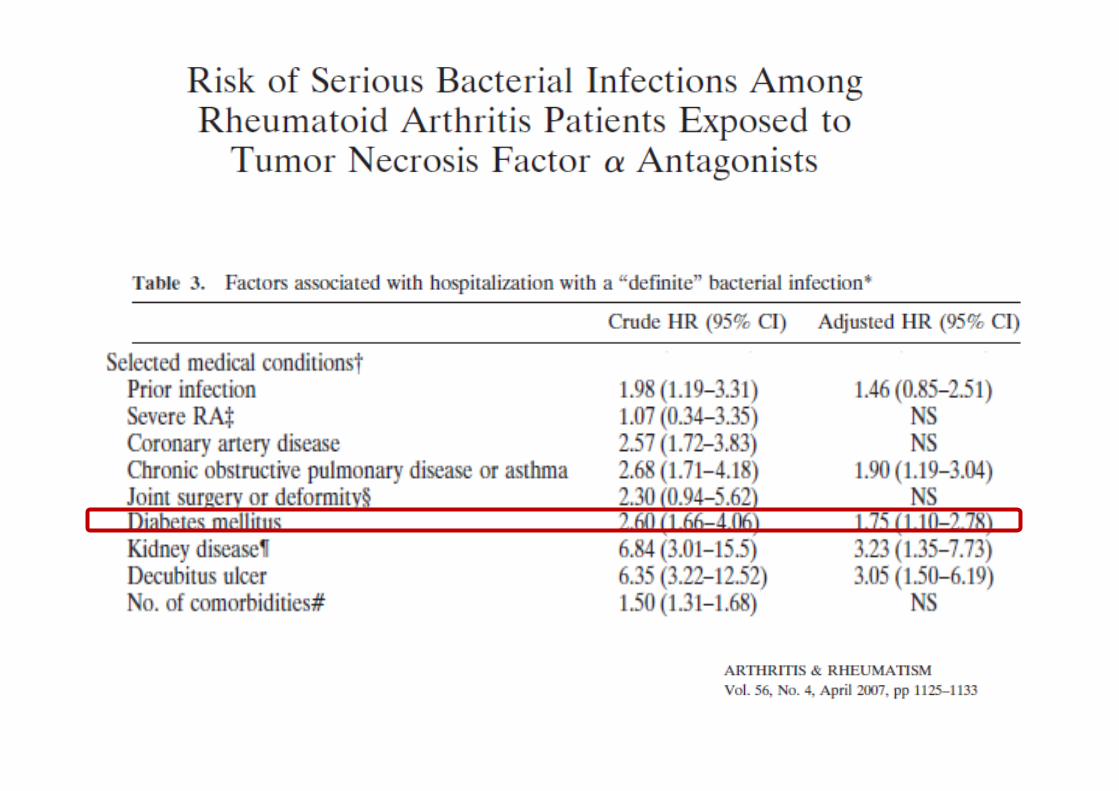
IFX (n=2475) or ADA (n=604) in IBD patients (16 centers)
Severe Cancer Death Infections >65 yrs Anti-TNFs (n= 95) 11% 3% 10% >65 yrs other drugs (n=190) 0.5% 2% 2% <65 yrs anti-TNFs (n=190) 2.6% 0% 1%
Clin Gastroenterol Hepatol 2011;9(1):30-5
*
* p=n.s.
2011
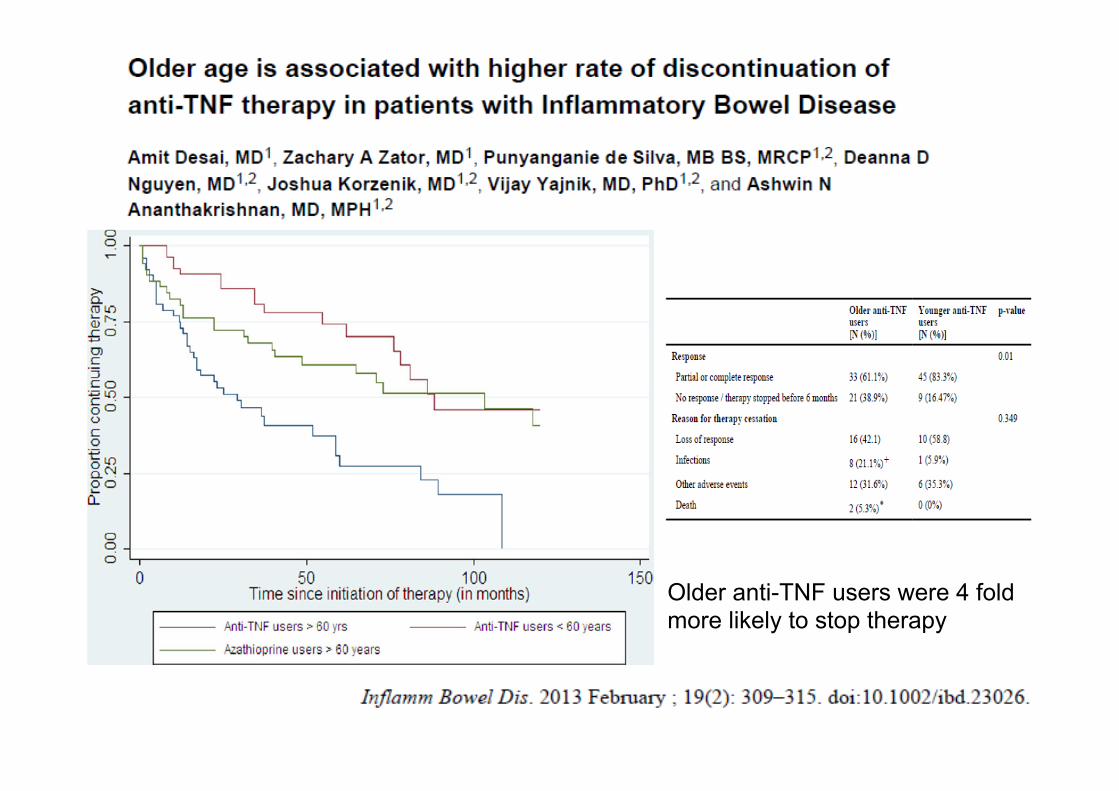
Older anti-TNF users were 4 fold more likely to stop therapy
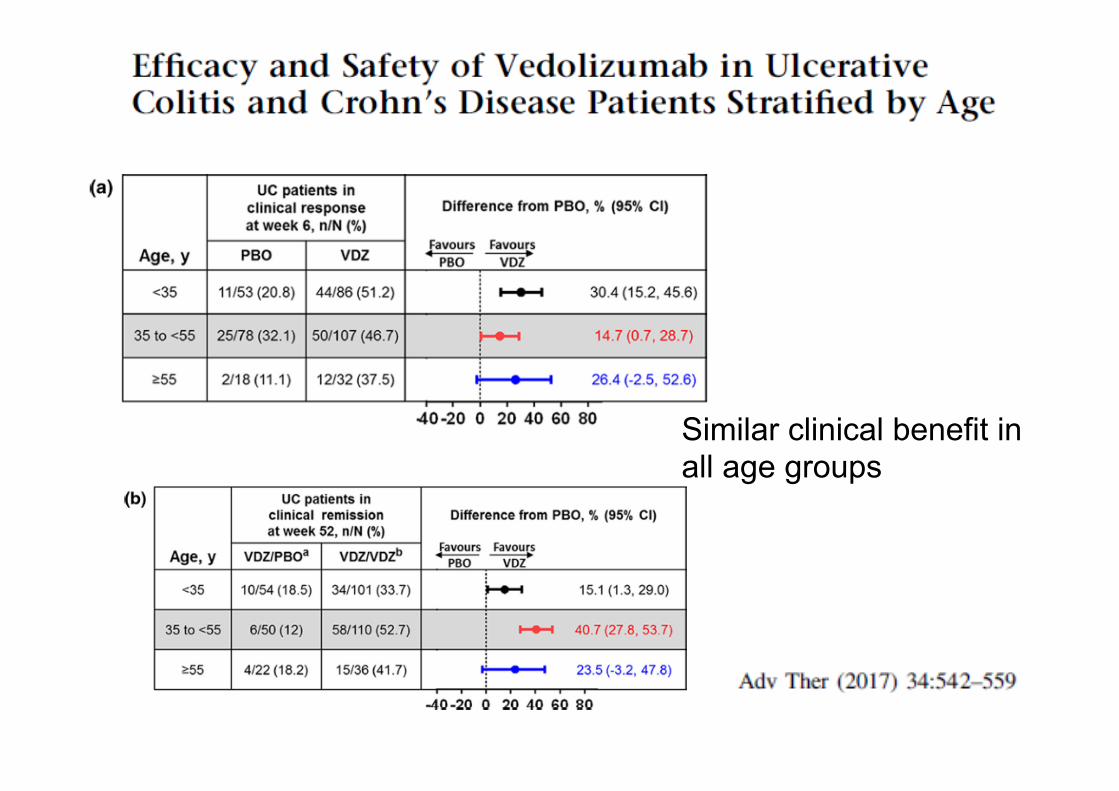
Similar clinical benefit in all age groups
Choosing a biologic in obese pts
IV route Dose titration
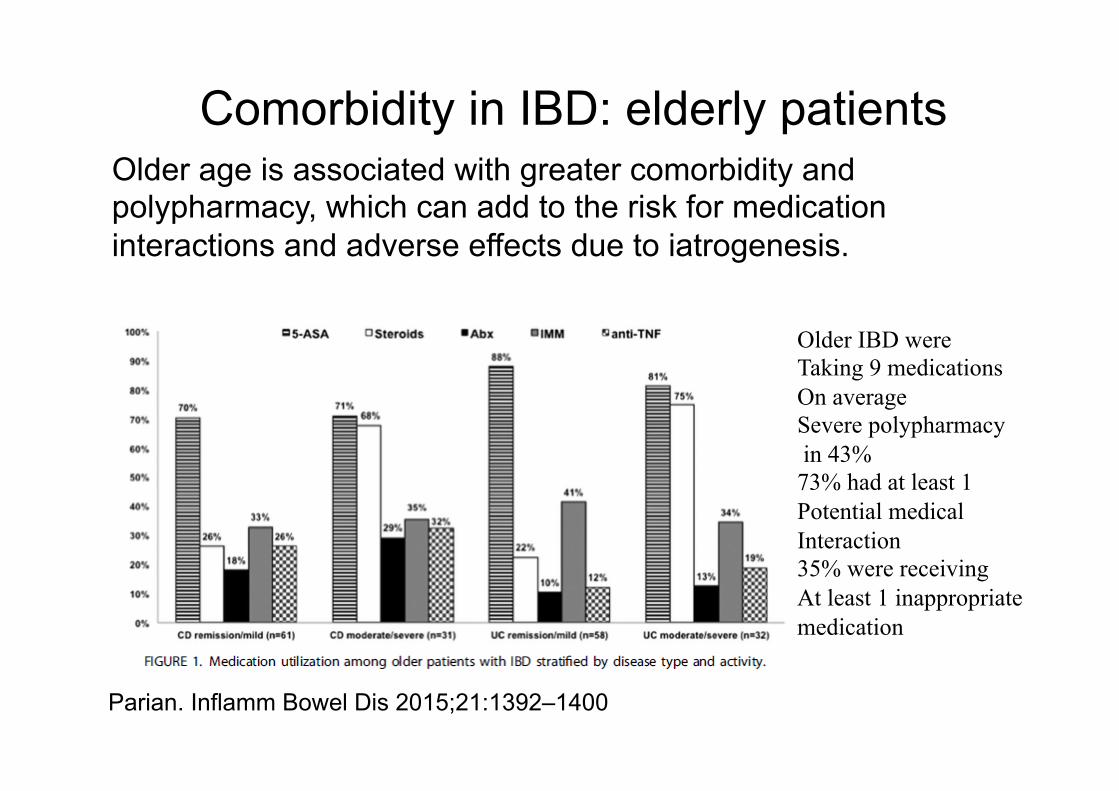
Comorbidity in IBD: elderly patients Older age is associated with greater comorbidity and polypharmacy, which can add to the risk for medication interactions and adverse effects due to iatrogenesis.
Parian. Inflamm Bowel Dis 2015;21:1392–1400
Older IBD were Taking 9 medications On average Severe polypharmacy in 43% 73% had at least 1 Potential medical Interaction 35% were receiving At least 1 inappropriate medication
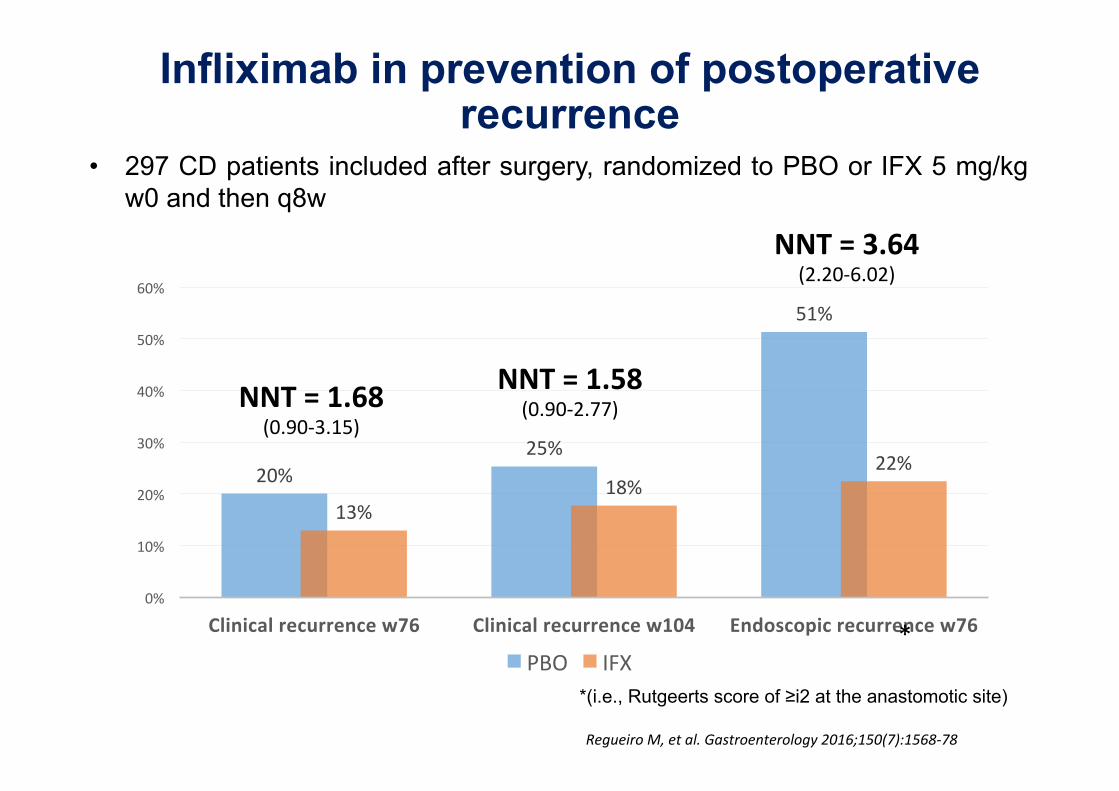
Infliximab in prevention of postoperative recurrence
*(i.e., Rutgeerts score of ≥i2 at the anastomotic site)
• 297 CD patients included after surgery, randomized to PBO or IFX 5 mg/kg w0 and then q8w
RegueiroM,etal.Gastroenterology2016;150(7):1568-78
20%25%
51%
13%18%
22%
0%
10%
20%
30%
40%
50%
60%
Clinicalrecurrencew76 Clinicalrecurrencew104 Endoscopicrecurrencew76
PBO IFX
NNT=1.68(0.90-3.15)
NNT=1.58(0.90-2.77)
NNT=3.64(2.20-6.02)
*
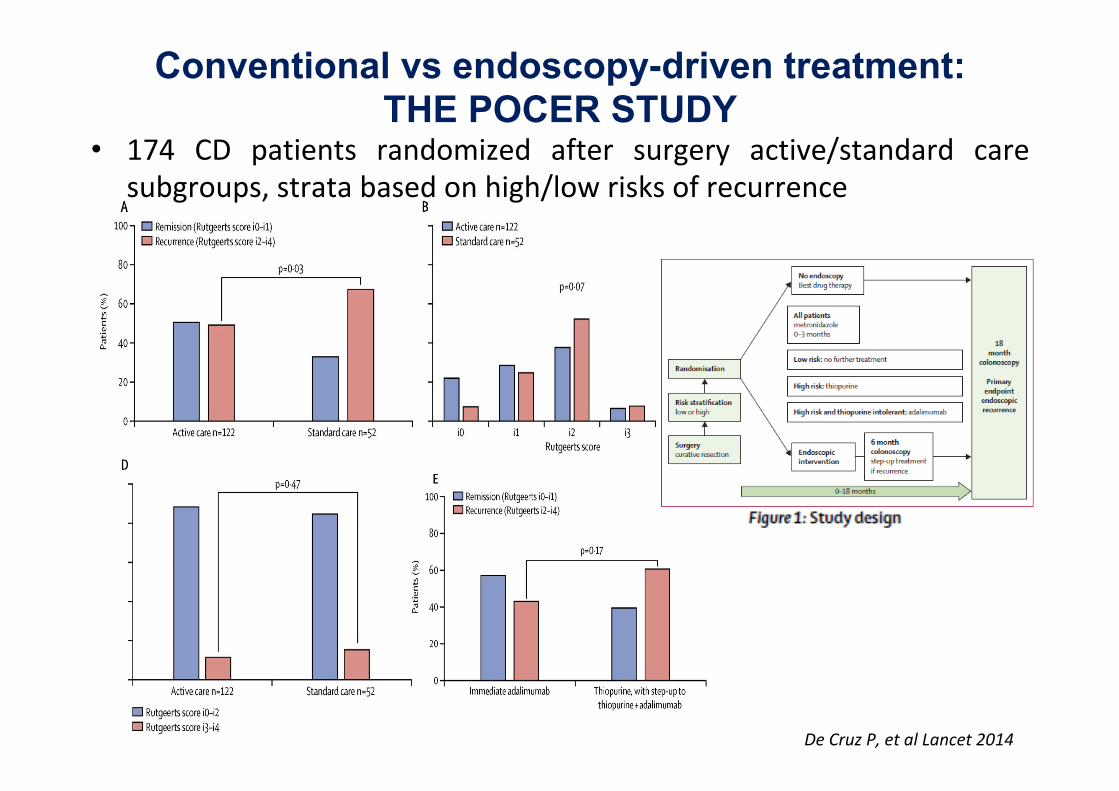
DeCruzP,etalLancet2014
• 174 CD patients randomized after surgery active/standard caresubgroups,stratabasedonhigh/lowrisksofrecurrence
Conventional vs endoscopy-driven treatment: THE POCER STUDY
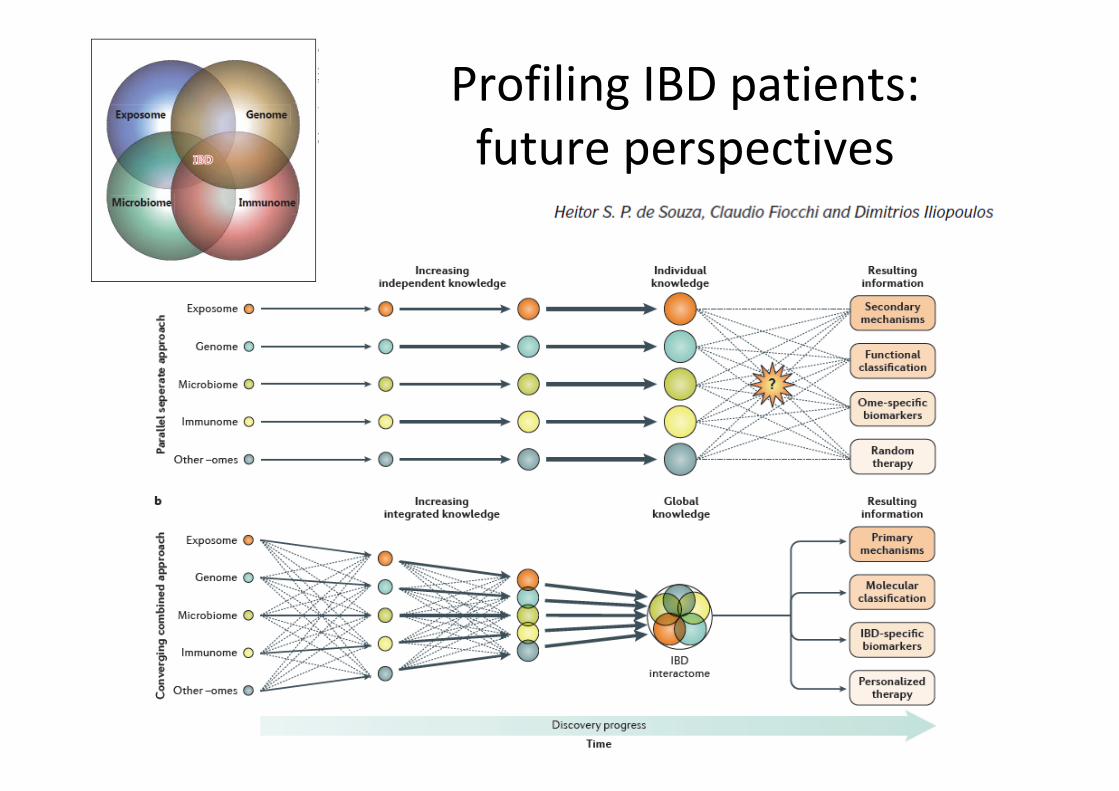
ProfilingIBDpatients:futureperspectives
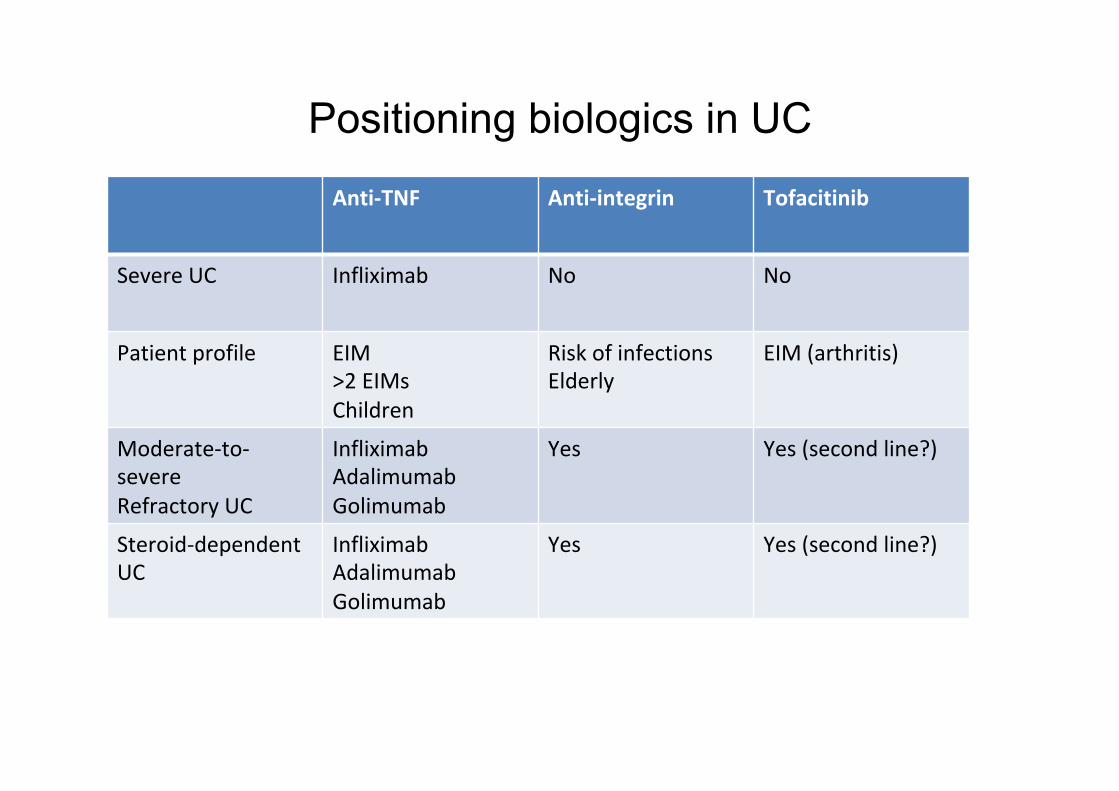
Positioning biologics in UCAnti-TNF Anti-integrin Tofacitinib
SevereUC Infliximab No No
Patientprofile EIM>2EIMsChildren
RiskofinfectionsElderly
EIM(arthritis)
Moderate-to-severeRefractoryUC
InfliximabAdalimumabGolimumab
Yes Yes(secondline?)
Steroid-dependentUC
InfliximabAdalimumabGolimumab
Yes Yes(secondline?)
Take-home messages
• Old and new biologics have enriched the therapeutic armamentarium in IBD
• The choice of the appropriate drug is and will be the ultimate «challenge» for IBD specialists
• RCTs, guidelines, SMPCs, regulatory rules, indirect comparison studies are the sources that guide decision-making in view of the paucity of head-to-head RCTs
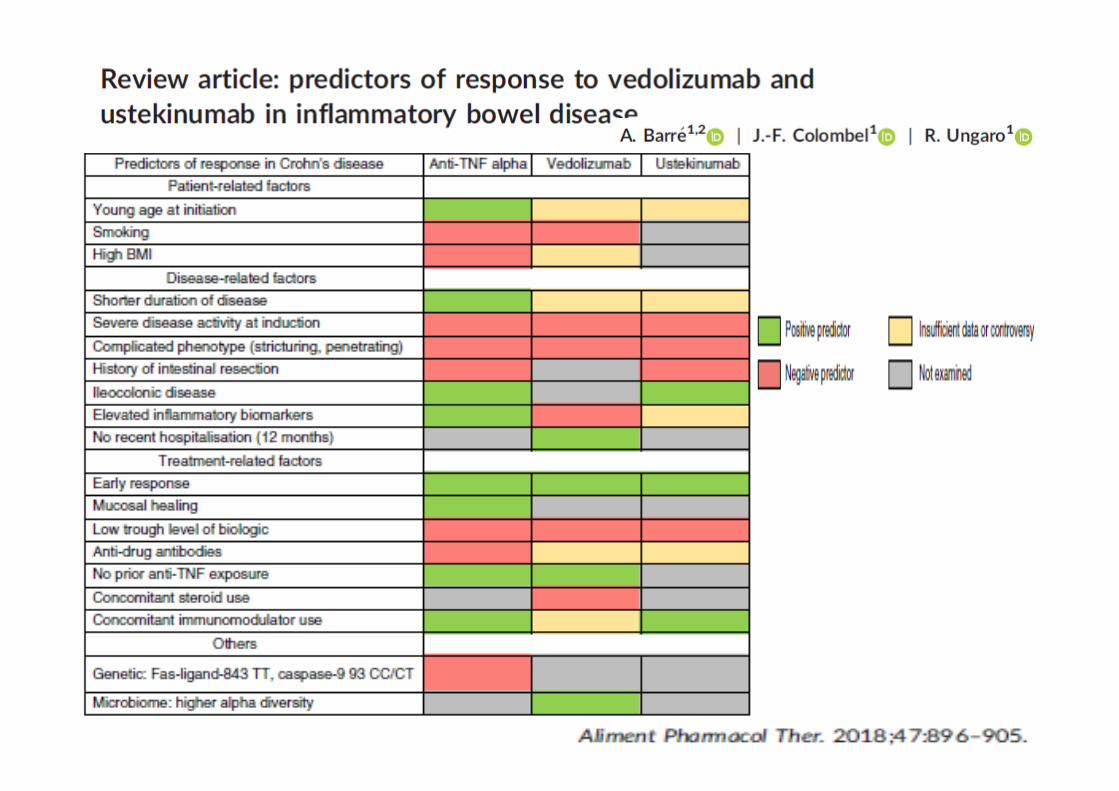
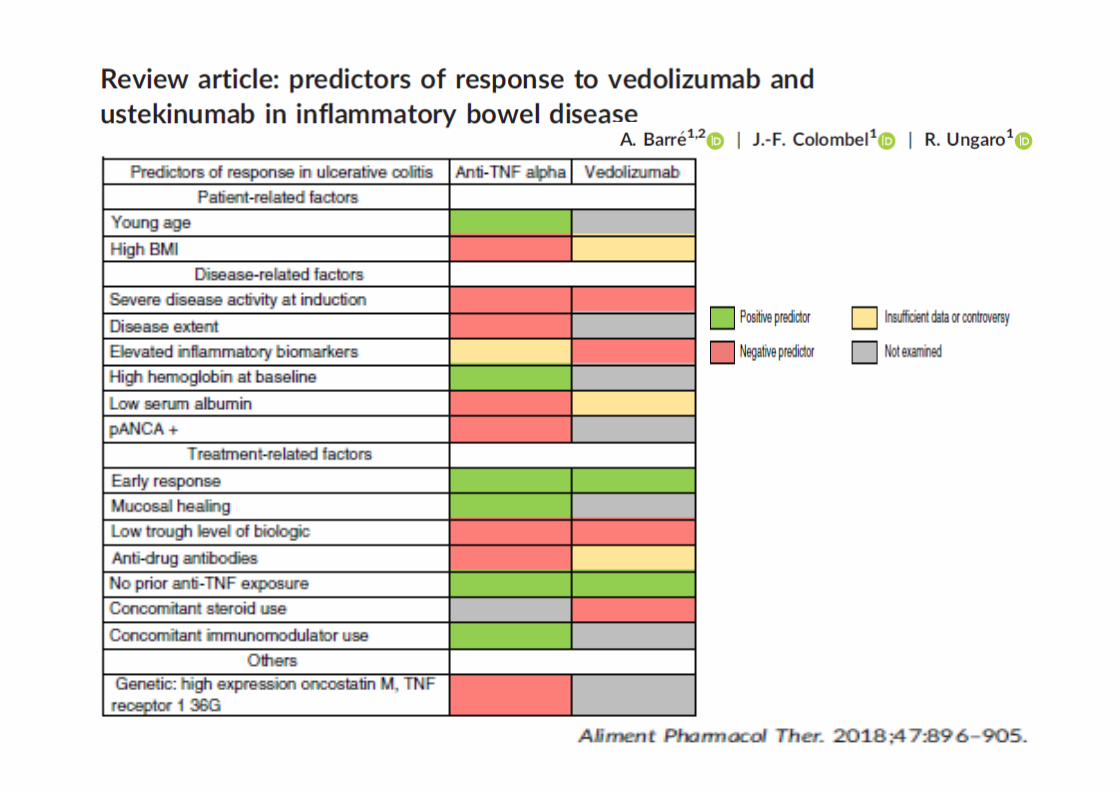
• Identication of predictive factors for response is an important issue which should be addressed by clinical researchers
• Waiting for molecular profiles and omics revolution…





























