-
8/4/2019 Dr Dinithi QUS
1/73
MD Part 1 Physiology MCQs 27
February 2011
40 MCQs
Multiple true false type MCQs
-
8/4/2019 Dr Dinithi QUS
2/73
1. Oedema in the following situations is correctly matchedwith
the relevant derangements in Starling forces of thecapillary
bed.
A. Nephrotic syndrome - decreased interstitial colloid
osmoticpressure
B. Congestive cardiac failure - increased capillary
hydrostatic
pressureC. Angio- oedema - increased capillary filtration
coefficent
D. Chronic lymphatic filariasis - decreased interstitial
hydrostaticpressure
E. Kwashiokor - decreased capillary colloid osmoticpressure
F T T F T
-
8/4/2019 Dr Dinithi QUS
3/73
Starling forces
-
8/4/2019 Dr Dinithi QUS
4/73
A. Pernicious anaemia - defective DNA synthesisB. Sideroblastic
anaemia - defective haem synthesisC. Sickle cell anaemia -
defective cytoskeleton of the
red cellD. Beta Thallasaemia major - defective globin chain
synthesisE. Hereditary spherocytosis - defective red cell
metabolism
2. The following haematological disorders are correctlymatched
with their pathophysiology
T T F T T
-
8/4/2019 Dr Dinithi QUS
5/73
Life story of the red cell
circulation
Tissuemacrophage
systemBone
marrow
Release/ quality Life span
-
8/4/2019 Dr Dinithi QUS
6/73
A. increased activity of tissue plasminogen activator (t-PA)
B. increased activity of tissue thromboplastin (TPL)C.
inhibition of cyclo-oxygenaseD. decreased synthesis of factor VIIE.
inhibition of formation of platelet IIbIIIa complex
3. A 70 year old man, who is on long term aspirin andclopidogrel
for secondary prevention of IHD presents withsevere melaena and
haematochezia. UGIE revealsoesophageal varices. Ultra sound scan
findings support
cirrhosis of the liver. He is transfused 14 packs of red
cellconcentrate, several packs of platelets and FFP to restorethe
circulating volume. The transfusion takes place over 36hours.
Malaena stops on banding oesophageal varices buton the third day he
starts to bleed from the IV puncture sites.In this patient, factors
that are likely to contribute tobleeding from IV puncture sites
include
T T T T T
-
8/4/2019 Dr Dinithi QUS
7/73
-
8/4/2019 Dr Dinithi QUS
8/73
A. Atrial systole - P waveB. Isovolumetric ventricular
contraction - R waveC. Ventricular ejection - ST segmentD.
Isovolumetric ventricular relaxation - T wave
E. Ventricular filling - PR interval
4. The following phases of the cardiac cycle is/are
correctlypaired with the waves/intervals/segments of the ECG
T T T F F
-
8/4/2019 Dr Dinithi QUS
9/73
A. EpinephrineB. DigoxinC. HypoxiaD. Hypercarbia
E. Acidaemia
5. Which of the following increases the force of contraction ofa
cardiac muscle fibre for a given length?
T T T F F
-
8/4/2019 Dr Dinithi QUS
10/73
Contractility, causes of change in-
Strokevolume
0
Ventricular End-diastolic volume
Changes in contractility
Decrease in contractility
Increase in contractility
INCREASE :Sympathetic nervesCatecholaminesDigitalisInotropic
agents
Dopamine
Force-frequency relation
DECREASE :Parasympathetic nervesHypoxia, Hypercapnia,
AcidosisPharmacologicaldepressantsLoss of myocardiumIntrinsic
depression
-
8/4/2019 Dr Dinithi QUS
11/73
A. NOB. PGI2C. EndothelinD. Angiotensin II
E. Endothelial derived hyper-polarizing factor
6. Compounds that relax vascular smooth muscle include
T T F F T
-
8/4/2019 Dr Dinithi QUS
12/73
A. Hypercapnoea cerebral vasodilatationB. Hypoxaemia - pulmonary
vasoconstrictionC. NO - pulmonary vasodilatationD. Epinephrine -
cutaneous vasoconstriction
E. Hyperkalemia - skeletal muscle vasoconstriction
7. The following stimuli are correctly matched with the
vascularresponse evoked
T T T T F
-
8/4/2019 Dr Dinithi QUS
13/73
PO2
PCO2In alveoli
PO2
PCO2In alveoli
Reduced alveolar ventilation;excessive perfusion
Enhanced alveolar ventilation;inadequate perfusion
Pulmonary arteriolesServing these alveoliconstrict
Pulmonary arteriolesServing these alveolidilate
Reduced alveolar ventilation;
reduced perfusion
Enhanced alveolar ventilation;enhanced perfusion
-
8/4/2019 Dr Dinithi QUS
14/73
A. Increased discharge of aortic baroreceptorsB. Excitation of
the vagal innervations of the heart
C. Decrease in the sympathetic discharge to the heartD.
Arteriolar dilatationE. Decreased firing of atrial stretch
receptors
8. A healthy normovolaemic young adult is given anintravenous
infusion of 2L of isotonic saline over 30minutes. The
cardiovascular regulatory mechanisms that willbe initiated to
maintain his blood pressure within normal
limits include
T T T T F
-
8/4/2019 Dr Dinithi QUS
15/73
-
8/4/2019 Dr Dinithi QUS
16/73
-
8/4/2019 Dr Dinithi QUS
17/73
A. Ankle oedema - activation of RAAMB. Tachycardia - increased
stretch in the
arterial baroreceptorsC. Decreased systolic blood pressure -
decreased afterloadD. Elevated JVP - increased right atrial
contractionE. Third heart sound - increased ventricular
filling
9. A 65 year old man complains of orthopnoea and
paroxysmalnocturnal dyspnoea. On examination he has bilateral
pittingankle oedema, a pulse rate of 110 beats per minute, a
bloodpressure of 80/60 mmHg and an elevated jugular venous
pressure. His apex beat is felt in the 6th intercostal space
inthe anterior axillary line. A third heart sound is heard at
theapex.
The physical signs are correctly matched with the
pathophysiology.
T F F F T
-
8/4/2019 Dr Dinithi QUS
18/73
A. measures the function of the respiratory pump.
B. is about 6000 ml in a healthy adult.C. is measured with a
peak flow meterD. is greater in trained athletes than in sedentary
adultsE. decreases when lying down from an erect position
10. Vital capacity
T T F T T
-
8/4/2019 Dr Dinithi QUS
19/73
A. measures the integrity of the alveolo-capillary membrane
B. is estimated using carbon dioxideC. needs to be corrected for
the haemoglobin levelD. decreases in alveolar oedemaE. increases
during isotonic exercise
11. Diffusing capacity of lungs
T F T T T
-
8/4/2019 Dr Dinithi QUS
20/73
-
8/4/2019 Dr Dinithi QUS
21/73
A. is steep when PO2 is between 80- 100 mmHg
B. shows the relationship between haemoglobin content andoxygen
content in bloodC. assumes its shape because of tense- relaxed
interconversion of haemoglobinD. shows that unloading of oxygen
is facilitated when PO2 in
blood is 50 mmHgE. is shifted to the left when 2,3
biphosphoglycerate levels are
increased in blood
12. Oxygen- haemoglobin dissociation curve
F F T T F
-
8/4/2019 Dr Dinithi QUS
22/73
O2-Haemoglobin dissociation curve
P50
-
8/4/2019 Dr Dinithi QUS
23/73
Condition Response
Increased pH in body fluids - increasedrespiratory rate
Hyperinflation of lungs - bronchoconstriction Chronic hypoxia -
increased
erythropoiesis
Isotonic exercise - pulmonary vasodilatation
Reduction of blood supply to a lung segment - bronchodilatation
inthat segment
13. The following conditions are paired correctly with
theresponses evoked by them
F T T T F
-
8/4/2019 Dr Dinithi QUS
24/73
A. quiet inspirationB. quiet expirationC. forced expirationD.
PneumothoraxE. atelectasis
14. Intra-pleural pressure becomes positive relative to
theatmospheric pressure in
F F T T F
-
8/4/2019 Dr Dinithi QUS
25/73
-2.5 mmHg
0
0
AT REST
Intrapleural
space
Elastic recoil forces of the lung
and chest wall are pulling in
opposite directions, resulting in
a negative pressure in the
intrapleural space.
IPP
These forces just
balance each other
-
8/4/2019 Dr Dinithi QUS
26/73
A. is the state of contraction of bronchial smooth muscle
B. has a circadian rhythmC. when increased leads to turbulent
air flowD. remains unchanged during a normal respiratory cycleE. is
decreased with cholinergic stimulation of bronchial smooth
muscle
15. Bronchial tone
T T T F F
-
8/4/2019 Dr Dinithi QUS
27/73
Calibre of airways and resistance
Diameter 1
Narrower the airway higher the
resistance
Airway resistance
Asthma
Increased smooth muscle tone
Oedema of the submucosal layer
Obstruction of the lumen by secretions
Smooth muscleSubmucosa
Mucosa
d
-
8/4/2019 Dr Dinithi QUS
28/73
A. is a determinant of arterial oxygenation
B. changes with postural differencesC. is independent of right
ventricular outputD. is influenced by the concentration of inhaled
oxygenE. when increased is referred to as alveolar dead space
16. V/Q ratio in the lungs
T T F T T
-
8/4/2019 Dr Dinithi QUS
29/73
A. Most of it is transported as carbamino compounds
B. Chloride shift occurs in the red cells in venous bloodC. A
large partial pressure gradient is seen across the
alveolocapillary membraneD. Release of O2 at tissue level
increases the affinity of
haemoglobin to CO2
E. Its solubility in biological membranes facilitates the
process
17. Regarding elimination of CO2
F T F T T
Binds toInterstitial
-
8/4/2019 Dr Dinithi QUS
30/73
Tissue cell
CO2
CO2
CO2
O2
O2
O2 (dissolved in plasma)
Bloodplasma
CO2
CO2
CO2 CO2 (dissolved in plasma)
CO2 CO2 + H2O H2CO3 HCO3- + H+
Binds toplasma proteins
CO2 + H2O H2CO3 HCO3- + H+
Fast
Carbonicanhydrase
CO2 + Hb = HbCO2Carbamino-hemoglobin
HbO2 O2 + HbRed blood cell
HCO3-
Cl-
HHb
Cl-
Chlorideshift
fluid
Fused basal laminae
-
8/4/2019 Dr Dinithi QUS
31/73
CO2 CO2 (dissolved in plasma)
CO2 CO2 + H2O H2CO3 HCO3- + H+
CO2 + H2O H2CO3 H+ + HCO3
-Fast
Carbonicanhydrase
CO2 + Hb
HbCO2
Fused basal laminae
Slow
O2 + HHb HbO2 + H+
Carbamino-hemoglobin
HCO3-
Cl-
Reverse Chlorideshift
Cl-
Blood plasma
Red blood cell
O2 (dissolved in plasma)
CO2
CO2
O2
O2
-
8/4/2019 Dr Dinithi QUS
32/73
A. Increased uptake of glucose into skeletal muscle cells.B.
Increased activity of the thoracic pump.C. Decrease in lymph
flow.D. Accumulation of interstitial fluid in exercising muscles.E.
Increased alveolar capillary oxygen gradient in lungs.
18. Following are known to occur during moderate
isotonicexercise.
T T F T T
19 A 24 ld di l t d t i t d i f hi fi l
-
8/4/2019 Dr Dinithi QUS
33/73
A. Growth hormoneB. InsulinC. NorepinephrineD. ThyroxineE.
Vasopressin
19. A 24- year old medical student is studying for his
finalMBBS. He has had a clean record of health so far. He misseshis
dinner on the day before the medicine paper and staysup the whole
night. Which of the following hormones will be
present in excess amounts in his circulation, just
beforebreakfast, the following morning?
T F T F T
-
8/4/2019 Dr Dinithi QUS
34/73
Endocrine regulation ofcarbohydrate metabolism
Starch
Gut
Glucose
Blood
Tissues
Glycogen
insulin
insulin
catecholamines
Thyroidhormones
Thyroid hormones
Glucocorticoids/glucagon
GH/Glucocorticoids
Protein catabolismLipid catabolism
Glucocorticoids/GH/ Glucagon
-
8/4/2019 Dr Dinithi QUS
35/73
A. Acromegaly - insulin hypoglycaemia testB. Hypopituitarism -
glucose tolerance testC. Syndrome of inappropriate ADH secretion -
water deprivation testD. Addisons disease - short synacthen testE.
Cushings syndrome - dexamethasone suppression
test
20. The following disorders are paired correctly with the
teststhat help in diagnosis
F F F T T
-
8/4/2019 Dr Dinithi QUS
36/73
A. secretion is stimulated by increased stretch of atrial
baroreceptosB. primarily act on cytoplasmic receptorsC. increases
the number of aquaporins in the collecting ductsD. facilitates
reabsorption of water in the proximal convoluted tubuleE. when
secreted in excess cause dilutional hyponatreamia
21. Antidiuretic hormone
F F T F T
22 A 25 year old woman complains of weight loss over the
last
-
8/4/2019 Dr Dinithi QUS
37/73
A. weight loss is due to increased calorigenic action of
thyroxineB. warmth in the hands is due to cutaneous
vasodilatationC. increased heart rate is due to direct action of
thyroxine on the SA
nodeD. sweating is best treated by parasympathetic blockers.E. a
high LDL level is an expected finding
22. A 25 year old woman complains of weight loss over the last6
months. She feels unusually warm and sweaty all the timeand
complains of rising from a squatting position. Onexamination her
hands are warm and moist and have fine
tremors. Her pulse is irregularly irregular with a rate
ofapproximately 120 beats per minute. She has proptosis anda
palpable smooth goiter. Investigations show an increasedFT4 with
suppressed TSH. In this woman
T T T F F
-
8/4/2019 Dr Dinithi QUS
38/73
A. decreased bone resorptionB. decreased renal tubular
absorption of calciumC. decreased gut absorption of calciumD.
reduced excretion of phosphate by kidneysE. poor dietary intake of
calcium
23. A 54 year old man complains of severe anorexia,
nausea,generalized swelling and parasthesia of hands and feet.
Hehas a serum calcium of 3.3 meq/L (4.3-5.3 meq/L). His GFR is
25 ml/ minute. Ultrasonically his kidneys are small with
poorcorticomedullary demarcation. He has not yet beenprescribed
calcium replacement therapy. In this person, themechanisms leading
to a low serum calcium level include
F T T T T
-
8/4/2019 Dr Dinithi QUS
39/73
-
8/4/2019 Dr Dinithi QUS
40/73
A. Amino acidsB. GlucoseC. PotassiumD. CalciumE. Ketones
24. Insulin facilitates the entry of following compounds
toskeletal muscle cells.
T T T F T
25 Pathophysiology of hyperglycaemia in insulin deficiency
-
8/4/2019 Dr Dinithi QUS
41/73
A. increased intestinal absorption of glucose
B. increased renal tubular absorption of glucoseC. decreased
number of GLUT transporters in adipose tissueD. decreased number of
GLUT transporters in skeletal muscle cellsE. decreased activity of
glucokinase in the hepatocytes
25. Pathophysiology of hyperglycaemia in insulin
deficiencyinvolves
F F T T T
-
8/4/2019 Dr Dinithi QUS
42/73
Pool of GLUT 4
26 The follo ing meas rements belong to an 18 ear old
-
8/4/2019 Dr Dinithi QUS
43/73
A. Renal plasma flow is calculated by above informationB. GFR is
calculated by above informationC. He has diminished renal
functionsD. The investigations are consistent with volume
depletionE. He is likely to have eaten a high protein meal soon
before the
investigations
26. The following measurements belong to an 18 year
oldindividual.
urine creatinine - 35 mg/dL
Urine volume 3300 ml/ 24 hoursPlasma creatinine-0.7 mg/dLBlood
urea- highHaematocrit - normal
Which of the following are true/false about this person?
F T F F T
-
8/4/2019 Dr Dinithi QUS
44/73
GFR= UV/P
U=35
V=3300/24X60=2.29
P=0.7
35X 2.29/0.7=114.5
27 Kid f f ll i h
-
8/4/2019 Dr Dinithi QUS
45/73
A. Erythropoietin
B. 1 25 DHCCC. AldosteroneD. Atrial natriuretic peptideE.
Parathyroid hormone
27. Kidneys are target organs of following hormones
F T T T T
28 A 54 ld l i d i d h di l l i h
-
8/4/2019 Dr Dinithi QUS
46/73
A. Decreased Na reabsorption in the proximal convoluted tubuleB.
Decreased renal threshold for glucoseC. increased secretion of
angiotensin IID. Increased secretion of vasopressinE. Increased
HCO3 in the extracellular fluid
28. A 54 year old male is admitted to the medical casualty
with
dyspnoea and drowsiness. He has a history of diabetes
mellitusand has suffered from polyuria and polydipsia in the recent
fewweeks. On examination his pulse is thread with a rate of 110
beats
per minute. His blood pressure is 90/60 mmHg.
Investigation results are as follows.
RBS- 568 mg/dL
Urinalysis - reducing substances +++ketone bodies positive
Which of the following findings are consistent with this
patient?
T F T T F
29 A 25 ld h lth f l i d i d f t f 8
-
8/4/2019 Dr Dinithi QUS
47/73
29. A 25 year old healthy female is deprived of water for
8hours. Her hydration status was satisfactory prior towater
deprivation. Her plasma and urine osmolalitybefore and after water
deprivation are shown below
At the end of 8 hoursA. Her ADH levels will be higher than
normalB. Increased urine osmolality is due to increased
aldosterone
secretionC. Osmoreceptors in the hypothalamus are inhibitedD.
Urine output will be decreasedE. Specific gravity of urine will be
high.
Normal
range(mosm/kg H2O)Before
deprivationAfter
deprivation
Plasma
osmololality280-295 285 289
Urine osmolality 50- 1400 400 750
T F F T T
30 A 60 year old man suffered a massive bout of
-
8/4/2019 Dr Dinithi QUS
48/73
30. A 60 year old man suffered a massive bout ofhaematemesis. On
admission to the hospital he is pale,restless, and has cold
peripheries. The blood pressure is90/60mmHg with a pulse rate of
120 per minute. An in-
dwelling urinary catheter is inserted and 30 ml dark urineis
collected. In this man,
A. GFR is reduced due to decreased renal plasma flowB. Urinary
Na excretion is increasedC. There is maximal vasopressin
secretionD. ANP secretion is increasedE. Thirst is stimulated via
baro- receptors in blood vessels
T F T F T
-
8/4/2019 Dr Dinithi QUS
49/73
Peripheralvasoconstriction
Sympathetic activation
BP
Increased HR &contractility
Adrenal medullaryCatecholaminesecretion
Baro
VMC
Baro
activation of RAAM
Renal Na & H2Oretention
Vasopressinsecretion
- +
Thirst
hypothalamusVagal stimulation
-
+
-
-
8/4/2019 Dr Dinithi QUS
50/73
Normal values for questions 31 and 32.
PaO2- 85-100 mmHgPaCO2- 35-45 mmHg
H+ concentration- 37-42 nanomol/LHCO3 concentration- 24-28
mmol/L
31 A 54 year old male is suffering from cardiac failure
-
8/4/2019 Dr Dinithi QUS
51/73
31. A 54 year old male is suffering from cardiac
failurefollowing a myocardial infarction. He is breathless
andmildly cyanotic on examination. His arterial blood gasanalysis
reveals a pH of 7.2, HCO3 concentration of 14
mmol/L, PCO2 of 32 mmHg and PO2 of 65 mmHg. In thispatient
A. the actual H+ concentration is likely to be 20 nanomol/LB.
the primary acid base disorder is in the respiratory systemC. urine
is likely to have a decreased HCO3/H+ ratioD. renal acid excretion
is facilitated by the current PCO2 level.E. arterial oxygen
saturation is likely to be 95%.
F F T F F
32 A 30 ld h lth l t i li bi
-
8/4/2019 Dr Dinithi QUS
52/73
32. A 30 year old healthy male goes on a mountain
climbingexpedition in the Himalayas. He reaches the first camp
at3000 meters and spends two days there. On the secondday he is
found to have a respiratory rate of 34 breaths/minute and complains
of faintness. This person is likelyto have
A. a plasma pH of > 7.4B. a PCO2 of 45 mmHgC.
bicarbonaturiaD. an increased anion gapE. cerebral
vasodilatation
T F T F F
33 Stimulants of Gastric acid secretion include
-
8/4/2019 Dr Dinithi QUS
53/73
33. Stimulants of Gastric acid secretion include
A. stretching of the stomach wall
B. presence of a high protein content in the stomachC.
Helicobacter pylori infection of the stomachD. presence of a high
fat content in the duodenumE. hypoglycaemia
T T F F T
34 A 32 ld f d t h bili bi f
-
8/4/2019 Dr Dinithi QUS
54/73
34. A 32 year old man was found to have a serum bilirubin of5
mg/dL on a routine medical check. All the other liverbiochemistry
and physical examination is normal. Hisreticulocyte count is within
normal limits. Hishyperbilirubinaemia is likely to be due to
A. decreased UDP glucuronyl transferase activity.B. decreased
uptake of bilirubin into liver cells.C. impaired secretion of bile
in to the biliary canaliculi.D. increased breakdown of red cells.E.
intrahepatic bile duct obstruction.
T T F F F
Matured red cellRed cell production and
-
8/4/2019 Dr Dinithi QUS
55/73
Life span 120 days
Globin ReutilizedDestruction inreticuloendothelial system
Fe
Haem
Iron Reutilized
C CBilirubin
Transport in plasma bound to albuminEnterohepatic Circulation of
urobilinogen
Urinary urobilinogen
Gut
Stercobilinogen
Urobilinogen
Bilirubinglucuronide
pbreakdown
-
8/4/2019 Dr Dinithi QUS
56/73
Bile pigments
Heam Globin
Porphyrin Fe++
Biliverdin
Bilirubin
Bilirubin +albumin
Circulation
RES cell eg.Kupffer cellsof liver
Hepatocyte
Bilirubin + 2UDPGA
glucuronyltransferase
Bilirubin
diglucuronide
breakdown
RBC Hb Hb
Excreted in bile
35 Following GI hormones and their actions are correctly
-
8/4/2019 Dr Dinithi QUS
57/73
35. Following GI hormones and their actions are
correctlypaired.
A. Gastrin - stimulation of mucosalgrowth of the stomachB.
Secretin - stimulation of pancreatic
juice secretionC. Cholecystokinin-Pancreozymin - relaxation of
the gall
bladder
D. Somatostatin - inhibition of gastric acidsecretionE.
Vasoactive Intestinal Polypeptide - secretion of electrolytes
from the small intestine
T T F T T
36 The following structures are depolarized due to opening
-
8/4/2019 Dr Dinithi QUS
58/73
36. The following structures are depolarized due to openingof
Voltage gated Na channels.
A. Visceral smooth muscleB. Motor nervesC. Skeletal muscleD.
Cardiac muscleE. Cardiac pace maker tissue
F T T T F
37 A myelinated nerve
-
8/4/2019 Dr Dinithi QUS
59/73
37. A myelinated nerve
A. evokes a local response with a sub-threshold stimulus
B. has sodium channels distributed evenly along its lengthC. is
refractory to stimulation during the spike potentialD. is
susceptible to conduction block with hypoxiaE. does not regenerate
after damage
T F T T F
-
8/4/2019 Dr Dinithi QUS
60/73
38 Regarding the stretch reflex
-
8/4/2019 Dr Dinithi QUS
61/73
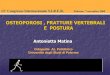
38. Regarding the stretch reflex
A. Muscle spindle is the receptor.
B. The excitatory pathway is polysynaptic.C. The main efferents
are motor neurons.D. Motor cortex has inhibitory inputs to the
stretch reflex.E. Basal ganglia facilitate the stretch reflex.
F F T T T
Dorsal rootganglion
-
8/4/2019 Dr Dinithi QUS
62/73
g g
MotorNeuron of
Protagonistmuscle
Ventralroot
Antagonist muscle
Motor
neuron ofAntagonist
muscle
interneuronreleasingglycine
Protagonistmuscle
39 Withdrawal reflex
-
8/4/2019 Dr Dinithi QUS
63/73
39. Withdrawal reflex
A. is prepotent.
B. is monosynaptic.C. occurs as a result of contractions of
ipsilateral extensormuscles.
D. removes the limbs from harmful stimuli.
E. is accompanied with a crossed extensor response.
T F F T T
40 Sensory receptors
-
8/4/2019 Dr Dinithi QUS
64/73
40. Sensory receptors
A. are sensory nerve endings
B. produce generator potentials proportionate to the strength
ofthe stimulusC. are found more concentrated in the viscera than
the somaD. can transform chemical energy in to action potentialsE.
have a low threshold for their adequate stimuli
T T F T T
-
8/4/2019 Dr Dinithi QUS
65/73
Best response MCQS
Select the best answer.
1 A 22 year old previously healthy young woman was
-
8/4/2019 Dr Dinithi QUS
66/73
1. A 22 year old previously healthy young woman wasfound to be
hyperventilating on admission to thehospital. She complained of
dizziness and pins andneedles in her hands and feet. On examination
she hadcarpal spasms. Rest of the system examination
wasunremarkable. Which of the following biochemical profilematches
her clinical profile?
A. Both serum ionized calcium and free hydrogen levels will
beincreasedB. Both serum ionized calcium and free hydrogen levels
will be
decreasedC. Both serum ionized calcium and free hydrogen levels
will be
normal
D. Serum ionized calcium will be increased and free Hydrogen
ionswill be decreasedE. Serum ionized calcium will be decreased and
free Hydrogen ions
will be increased
B
2. A 35 year old female tea estate worker from Talawakelle is
admitted tothe rural hospital with fever, productive cough with
rusty sputum and
-
8/4/2019 Dr Dinithi QUS
67/73
the rural hospital with fever, productive cough with rusty
sputum anddifficulty in breathing. She has left sided pleuritic
pain. Onexamination she has a respiratory rate of 30 breaths/
minute, reducedchest expansion on the left side, dull percussion
note and crepitationsin the left lower zone. She is mildly pale but
not cyanotic. Theinvestigations reveal a haemoglobin content of 10
g/dL, a white cellcount of 17000/mm3 with a differential neutrophil
leucocytosis and anESR of 78 mm in the first hour. On the second
day followingadmission her respiratory symptoms worsen and she
becomesrestless. The attending medical officer suspects severe
tissue hypoxia
and plans to transfer her to a provincial hospital for
specializedmanagement.
The most likely reason for suspected tissue hypoxia here is
A. severe ventilation perfusion imbalance
B. respiratory muscle fatigueC. a combination of ventilation
perfusion imbalance and respiratory musclefatigue
D. decreased concentration of inhaled oxygenE. decreased
cellular cytochrome oxidase level activity
C
3. A 30 year old woman presents with drooping of eyelids
-
8/4/2019 Dr Dinithi QUS
68/73
and diplopia for 3 months. She notes that symptomsworsen towards
the end of the day. EMG showsdecremental potentials during
repetitive stimulation and
is otherwise normal. Mediastinal magnetic resonanceimaging
confirms thymic hyperplasia.
The most probable reason for the symptoms in thiswoman is
A. post- synaptic inhibition of ligand gated Na+- K+ channelsB.
decreased quantal release of acetylcholine from the pre
synaptic end
C. pre- synaptic inhibition of voltage gated Ca channelsD. a
raised level of acetylcholine esterase in the synaptic cleftE.
decreased conduction velocity of motor nerves
A
EVENTS AT NERVE ENDING
-
8/4/2019 Dr Dinithi QUS
69/73
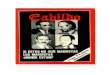
EVENTS AT NERVE ENDING
Ca
Ach
Ach
Ach
Ach
Ach
- - - - - - - - - - -
- - - - - - - - - - -
+ + + + + + + +
+ + + + + + + ++
+
+
- - +
-
- -+
Ach --vesicles containing Acetylcholine
Ca -- Calcium ionsSynaptic
cleft
Axon Ca
Ca
CaCa
Events at motor end plate
-
8/4/2019 Dr Dinithi QUS
70/73
Events at motor end plate
Na+
K+
- - - - -
+ + +
-- Acetylcholine molecule
-- Acetylcholine receptor
Motor end plate
Na+
sarcolemma
+ + + + + + + +
+ + +
- - -
Ligand- gated
channel
4. A 40 year old man presents with changing faciali ht i d diffi
lt i tti f
-
8/4/2019 Dr Dinithi QUS
71/73
appearance, weight gain, and difficulty in getting up froma
squat, polyuria and polydipsia. He has a history ofunsupervised
treatment for severe chronic asthma.
Examination and investigations reveal abdominalobesity, proximal
muscle weakness, a raised bloodpressure and hyperglycaemia. In this
patient, which ofthe following is nota component of the
pathophysiologyof raised blood pressure?
A. Permissive action of glucocorticoids on catecholaminesB.
Increased sodium and water retentionC. Direct action of
glucocorticoids on blood vessels
D. Direct action of angiotensin II on blood vesselsE.
Compromised renal blood supply
E
-
8/4/2019 Dr Dinithi QUS
72/73
Further reading:
Review of Medical Physiology WF Ganong 22nd editionTextbook of
Medical Physiology Guyton & HallKumar and Clarks Clinical
Medicine 7th edition
-
8/4/2019 Dr Dinithi QUS
73/73
Acknowledgements
Dr. Suresh Dissanayake
Dr. Dilshani Dissanayake
Mrs. Nadeesha Keragala
All of department of Physiology, Colombo