Embed Size (px)
Citation preview
1
Dr. Gary Mak 麥耀光心臟科專科醫生
President of HK Association of Sports Medicine and Sports Science
Director of Pro-Cardio Heart Disease and
Stroke Prevention center
Consultant Cardiologist HK Sports Institute
Cardiovascular Impacts of Endurance Exercise: Benefits or Injuries
www.hkasmss.org.hk

2

3
http://www.facebook.com/hkmarathon#

4
Rugby 7
HK Golf Open 2014

5
2012 Para-Olympic CV screening
BENEFIT OF EXERCISERegular exercise extends 7 years of life expectancy
6
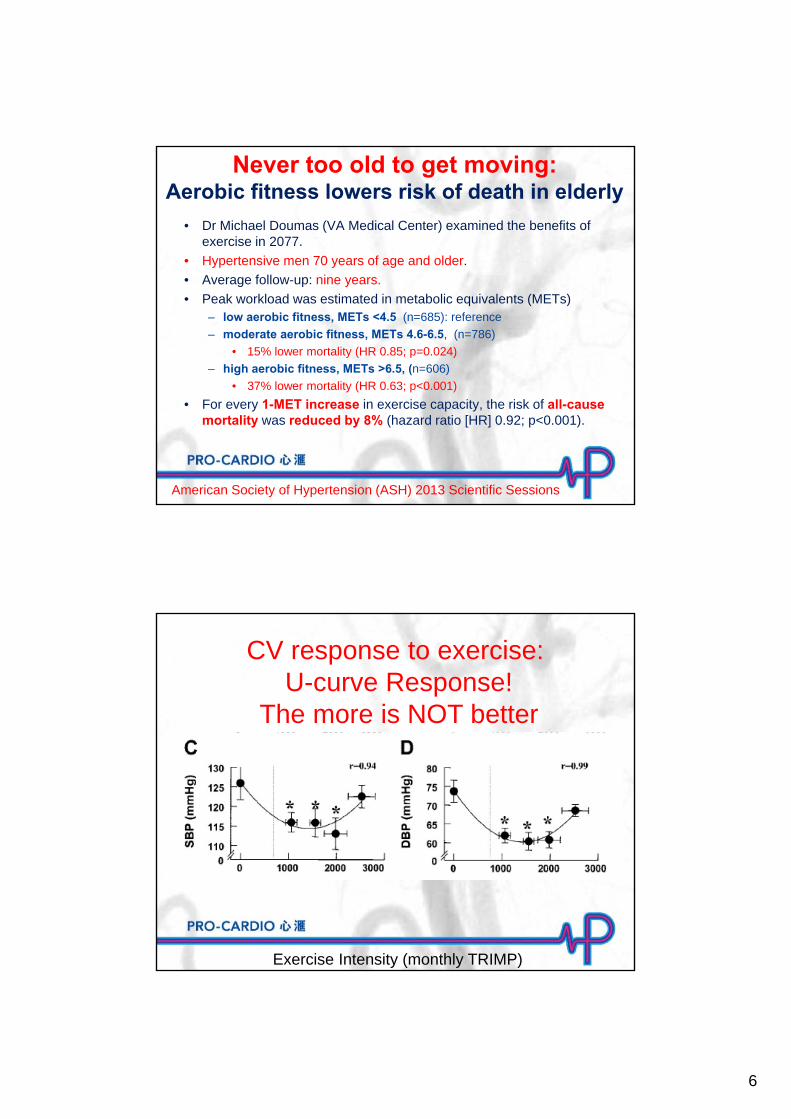
American Society of Hypertension (ASH) 2013 Scientific Sessions
• Dr Michael Doumas (VA Medical Center) examined the benefits of exercise in 2077.
• Hypertensive men 70 years of age and older.
• Average follow-up: nine years.
• Peak workload was estimated in metabolic equivalents (METs) – low aerobic fitness, METs <4.5 (n=685): reference
– moderate aerobic fitness, METs 4.6-6.5, (n=786)
• 15% lower mortality (HR 0.85; p=0.024)
– high aerobic fitness, METs >6.5, (n=606)
• 37% lower mortality (HR 0.63; p<0.001)
• For every 1-MET increase in exercise capacity, the risk of all-cause mortality was reduced by 8% (hazard ratio [HR] 0.92; p<0.001).
Never too old to get moving:Aerobic fitness lowers risk of death in elderly
Exercise Intensity (monthly TRIMP)
CV response to exercise: U-curve Response!
The more is NOT better
7
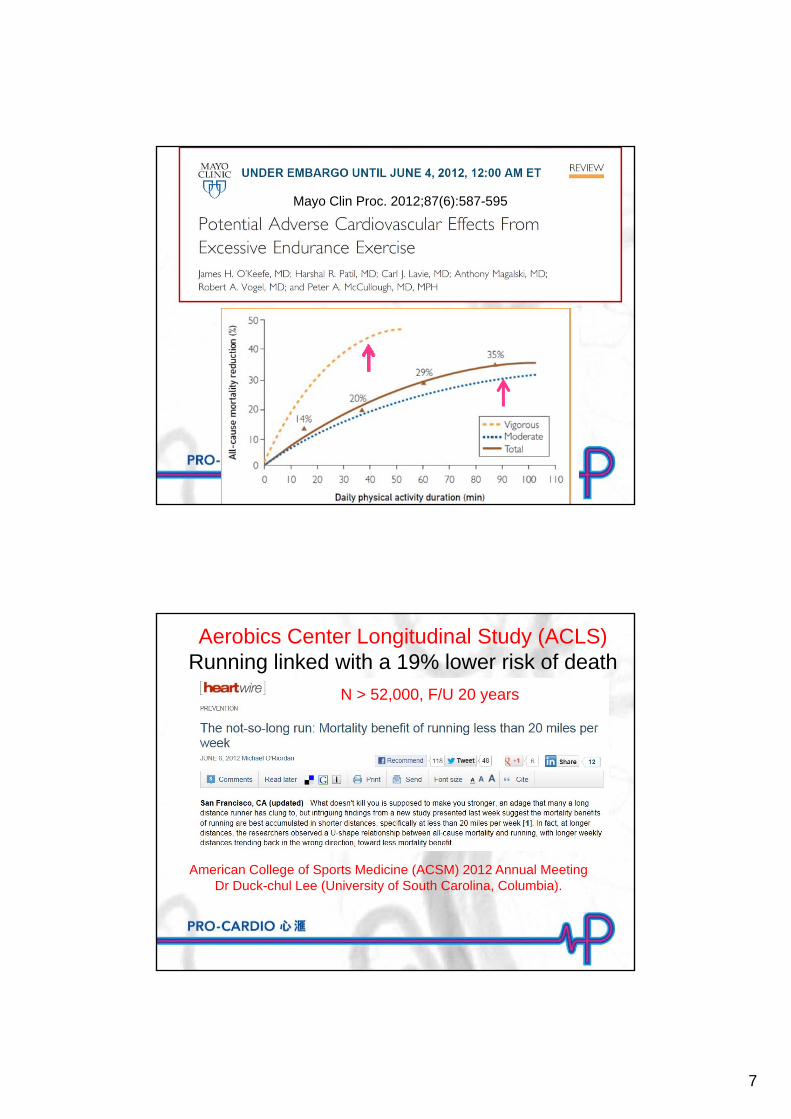
Mayo Clin Proc. 2012;87(6):587-595
American College of Sports Medicine (ACSM) 2012 Annual MeetingDr Duck-chul Lee (University of South Carolina, Columbia).
Aerobics Center Longitudinal Study (ACLS)Running linked with a 19% lower risk of death
N > 52,000, F/U 20 years

8
1515
Sinus Rhythm Atrial Fibrillation400 bpm
100 – 150 bpm
Atrial Fibrillation 心房顫動LV hypertrophy in Athletes ↑ atrial
stretch
P No P
EDITORIALEur Heart J, July 24,2015
9
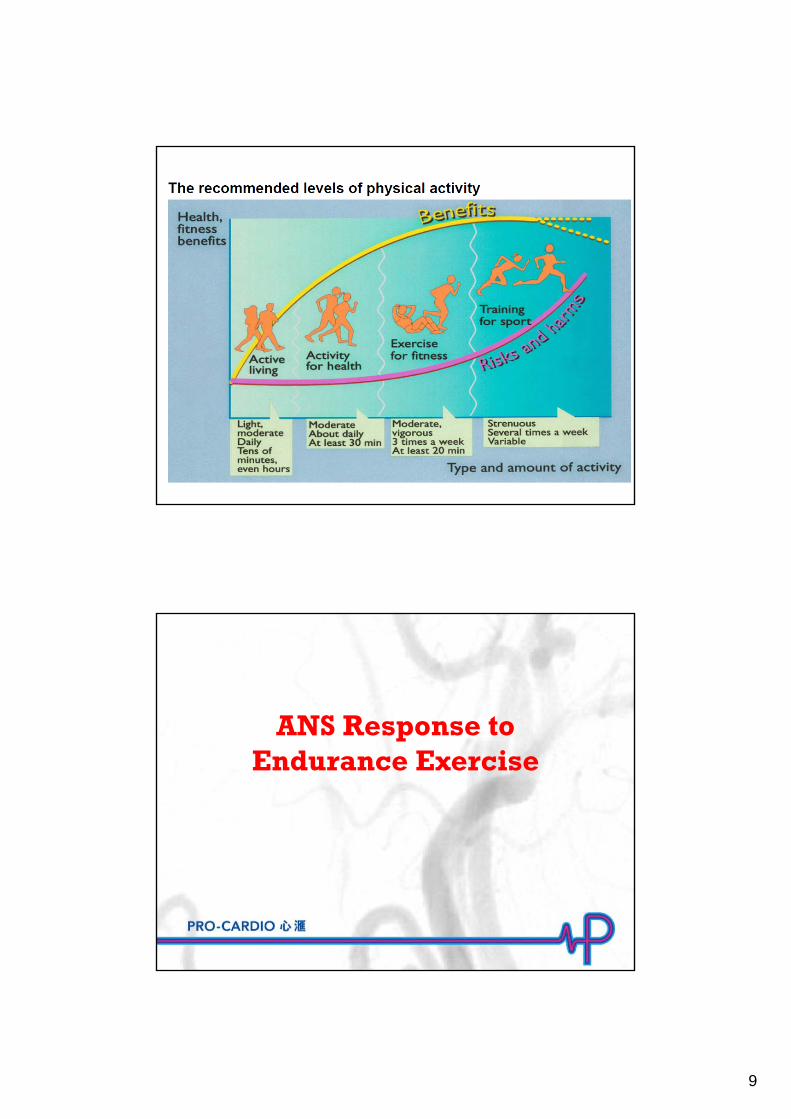
ANS Response to Endurance Exercise
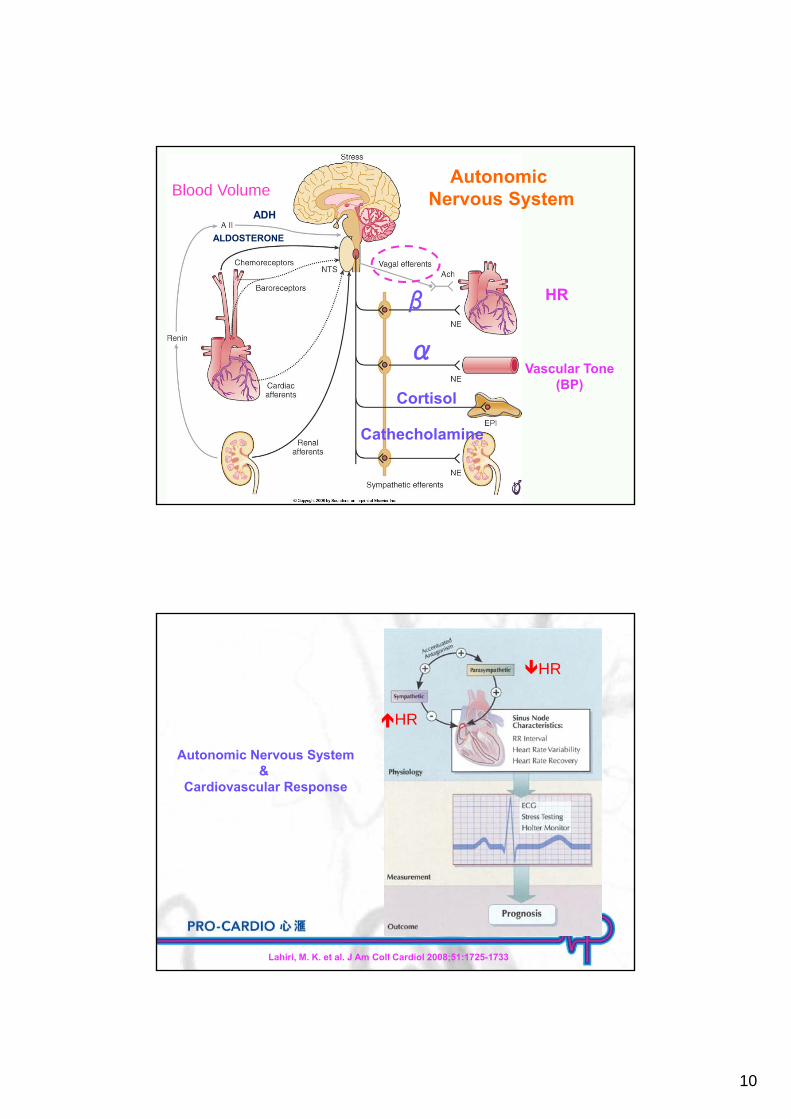
10
Vascular Tone(BP)
HR
Autonomic Nervous System
α
β
Cortisol
Cathecholamine
Blood Volume
ALDOSTERONE
ADH
Lahiri, M. K. et al. J Am Coll Cardiol 2008;51:1725-1733
Autonomic Nervous System&
Cardiovascular Response
HR
HR
11
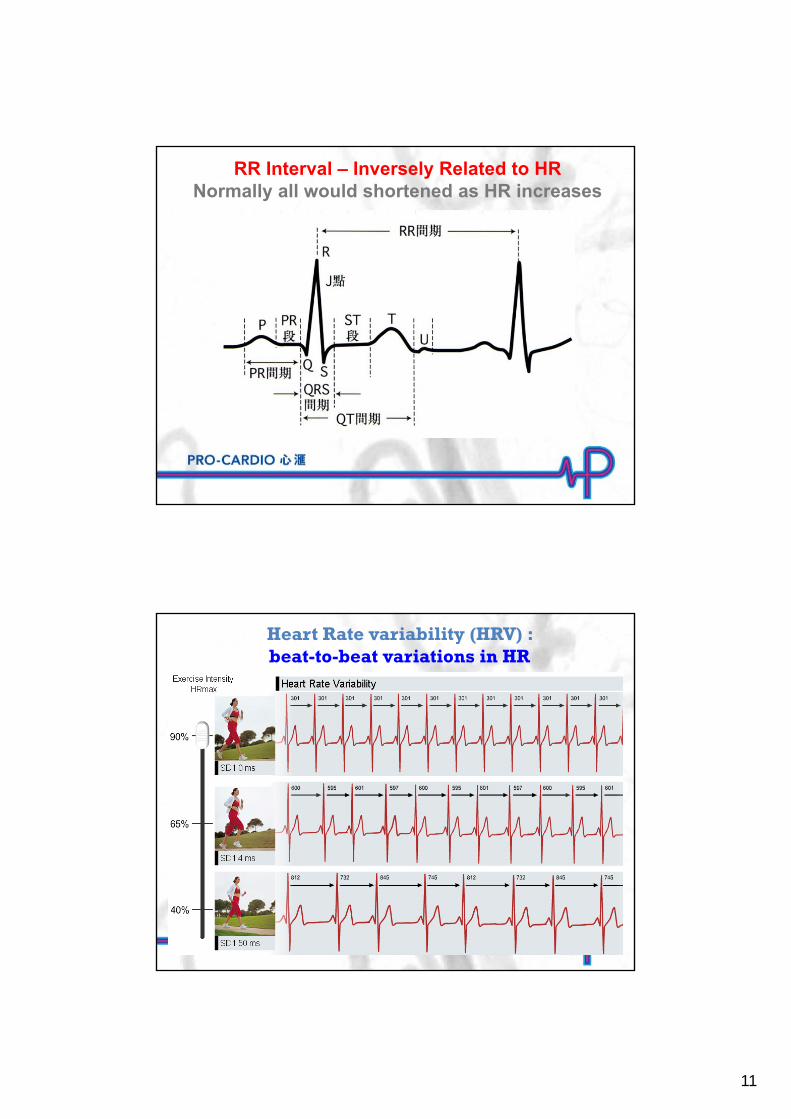
RR Interval – Inversely Related to HRNormally all would shortened as HR increases
Heart Rate variability (HRV) : beat-to-beat variations in HR
12
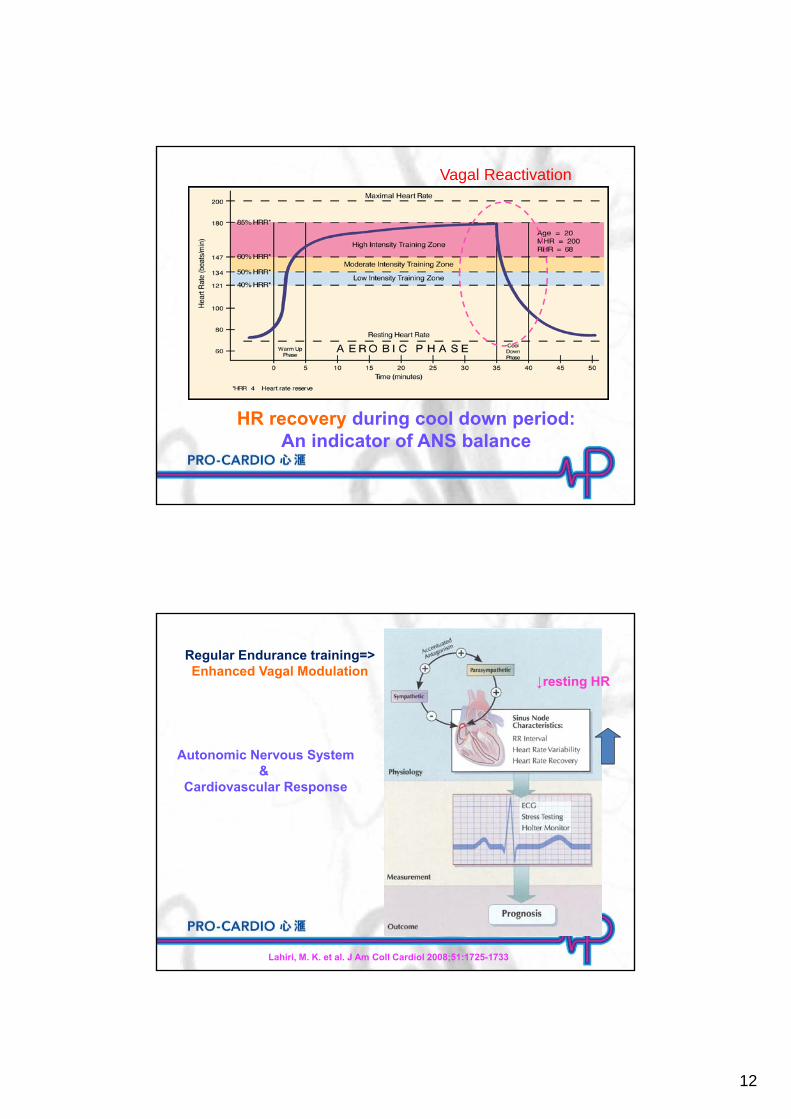
HR recovery during cool down period:An indicator of ANS balance
Vagal Reactivation
Lahiri, M. K. et al. J Am Coll Cardiol 2008;51:1725-1733
Autonomic Nervous System&
Cardiovascular Response
Regular Endurance training=>Enhanced Vagal Modulation
↓resting HR
13
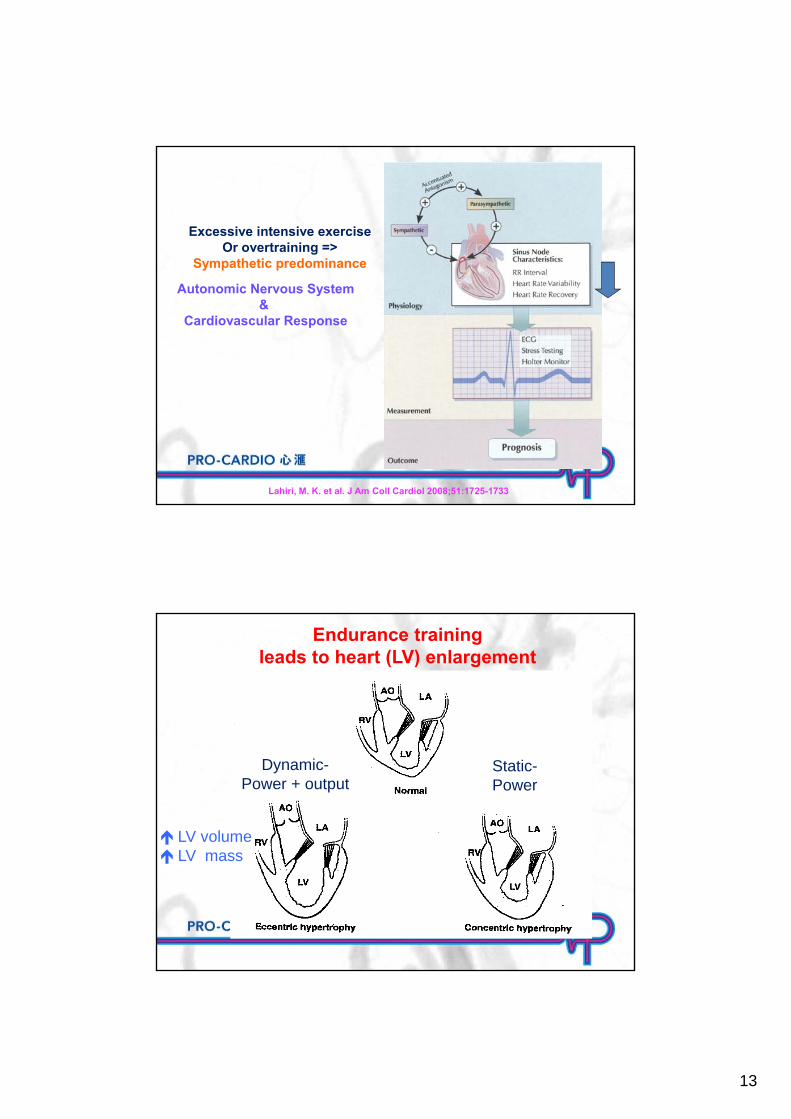
Lahiri, M. K. et al. J Am Coll Cardiol 2008;51:1725-1733
Autonomic Nervous System&
Cardiovascular Response
Excessive intensive exerciseOr overtraining =>
Sympathetic predominance
Endurance training leads to heart (LV) enlargement
Dynamic-Power + output
Static-Power
LV volume LV mass
14
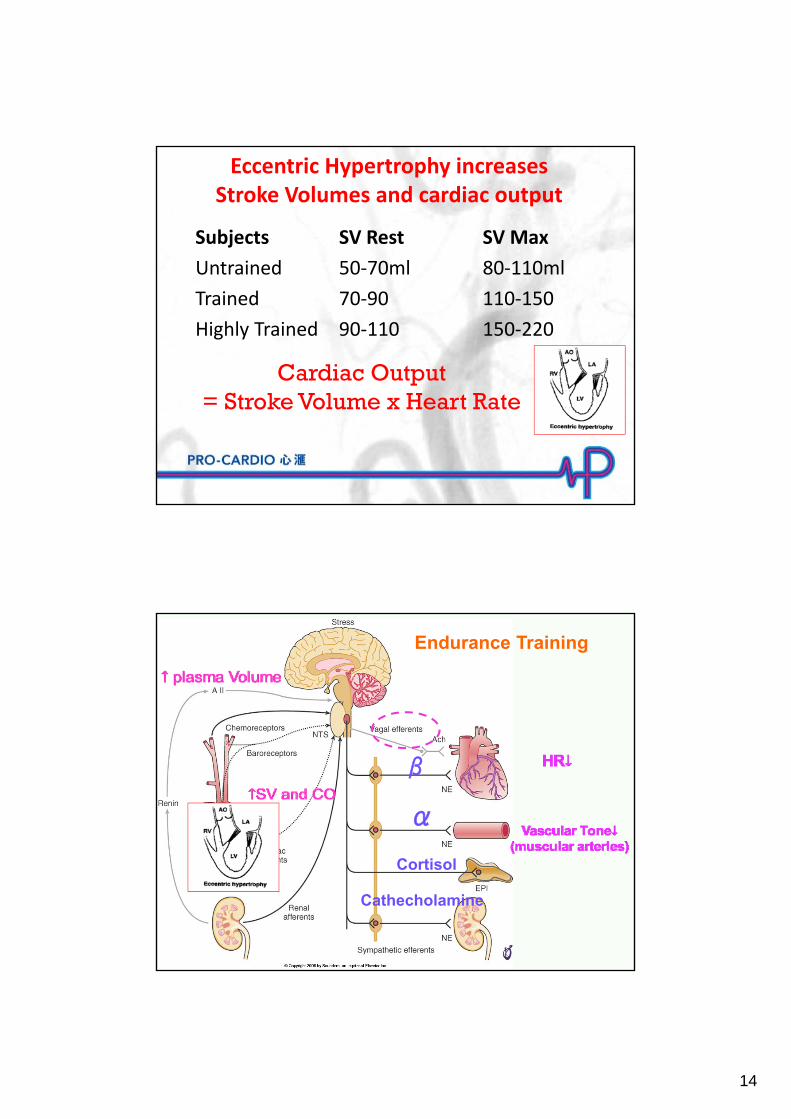
Eccentric Hypertrophy increases Stroke Volumes and cardiac output
Subjects SV Rest SV Max
Untrained 50‐70ml 80‐110ml
Trained 70‐90 110‐150
Highly Trained 90‐110 150‐220
Cardiac Output = Stroke Volume x Heart Rate
Endurance Training
α
β
Cortisol
Cathecholamine
15
Cardiovascular Adaptations to Endurance Training
Left ventricle size and wall thickness increase.
Resting, submaximal, and maximal stroke volume increases.
Maximal heart rate stays the same or decreases.
Blood volume increases, as does red cell volume, but to a lesser extent.
Cardiac output is better distributed to active muscles and maximal cardiac output increases.
Resting blood pressure does not change or decreases slightly, while blood pressure during submaximal exercise decreases.
M/41, former Olympic triathlon, with regular training and competition.
Stopped training for 3 weeks after Sebaceous Cyst excision. Developed fast HR (105 bpm) and high BP (140/100 mmHg)
Seen by Endocrinologist: Thyroid function - normalPhaeochromocytoma - unlikely
16
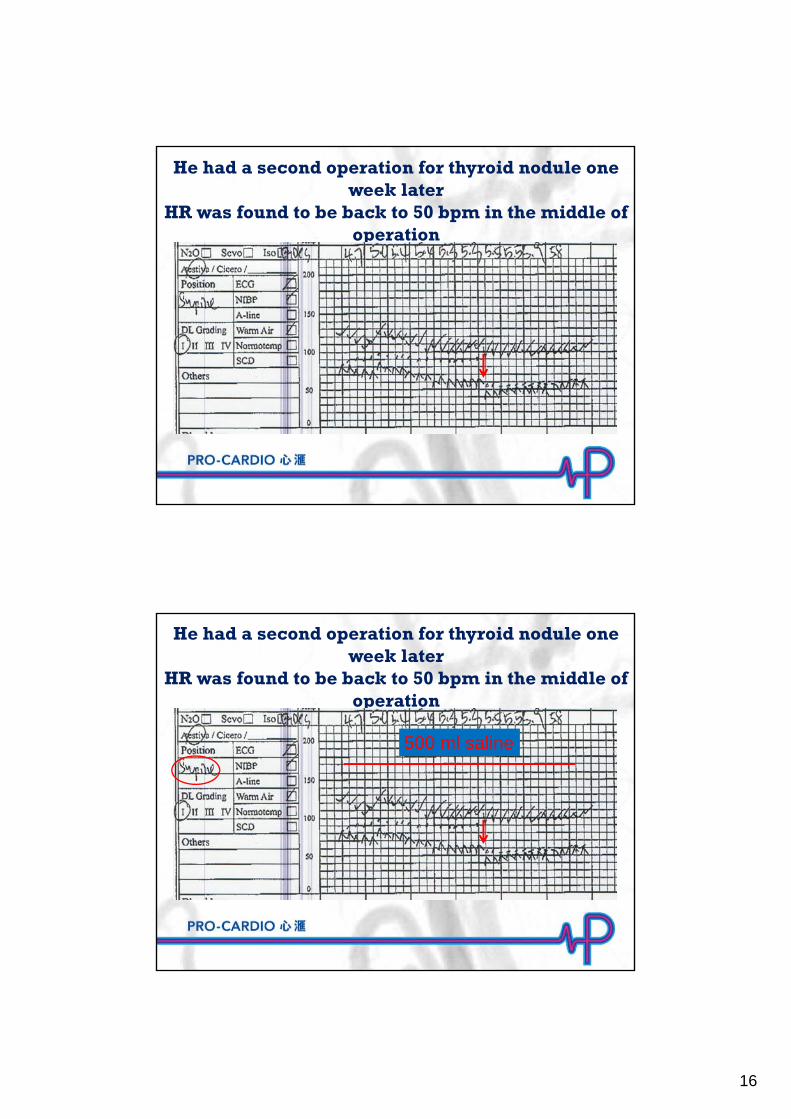
He had a second operation for thyroid nodule one week later
HR was found to be back to 50 bpm in the middle of operation
He had a second operation for thyroid nodule one week later
HR was found to be back to 50 bpm in the middle of operation
500 ml saline
17
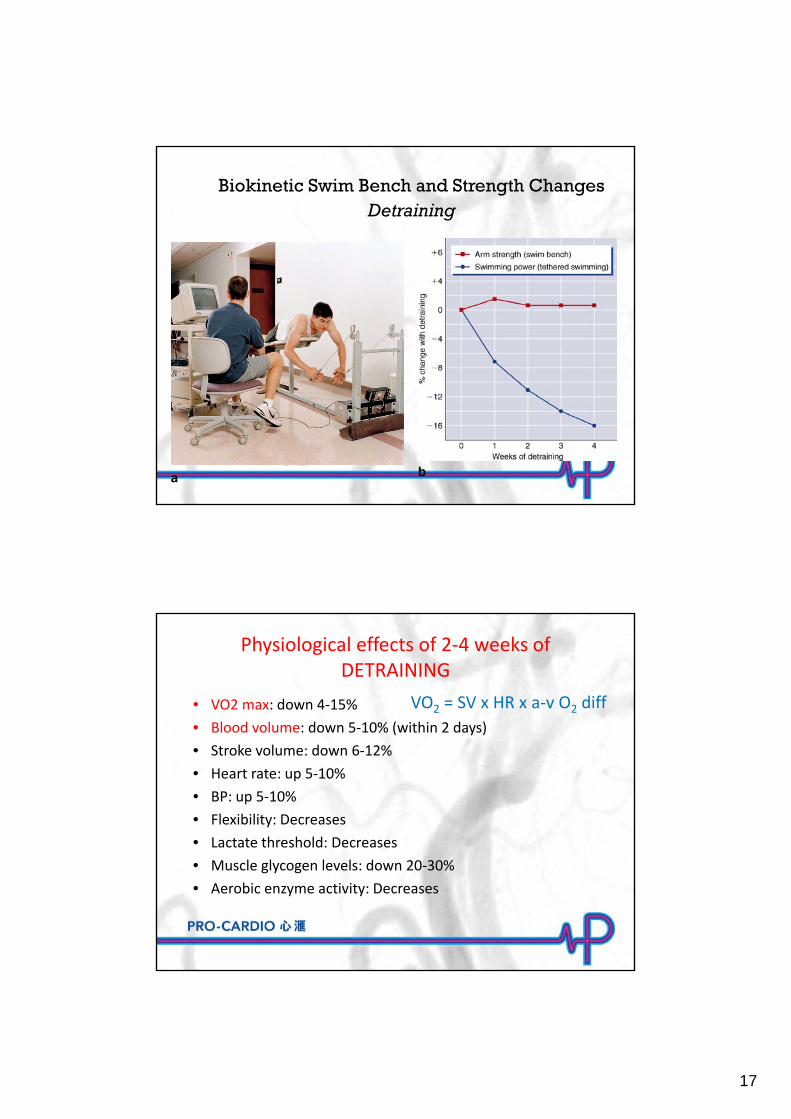
Biokinetic Swim Bench and Strength ChangesDetraining
a b
Physiological effects of 2‐4 weeks of DETRAINING
• VO2 max: down 4‐15%
• Blood volume: down 5‐10% (within 2 days)
• Stroke volume: down 6‐12%
• Heart rate: up 5‐10%
• BP: up 5‐10%
• Flexibility: Decreases
• Lactate threshold: Decreases
• Muscle glycogen levels: down 20‐30%
• Aerobic enzyme activity: Decreases
VO2 = SV x HR x a‐v O2 diff
18
Maintenance Training is ImportantThe negative effect of detraining is rapid (in less than 2 week)
The recovery from retraining is slow (well over 20 weeks)!!!
EK
45 yo male badminton coach• Recurrent palpitation, mostly at night
• Seldom have attacks during exercise.
• ECG: paroxysmal atrial fibrillation,
19
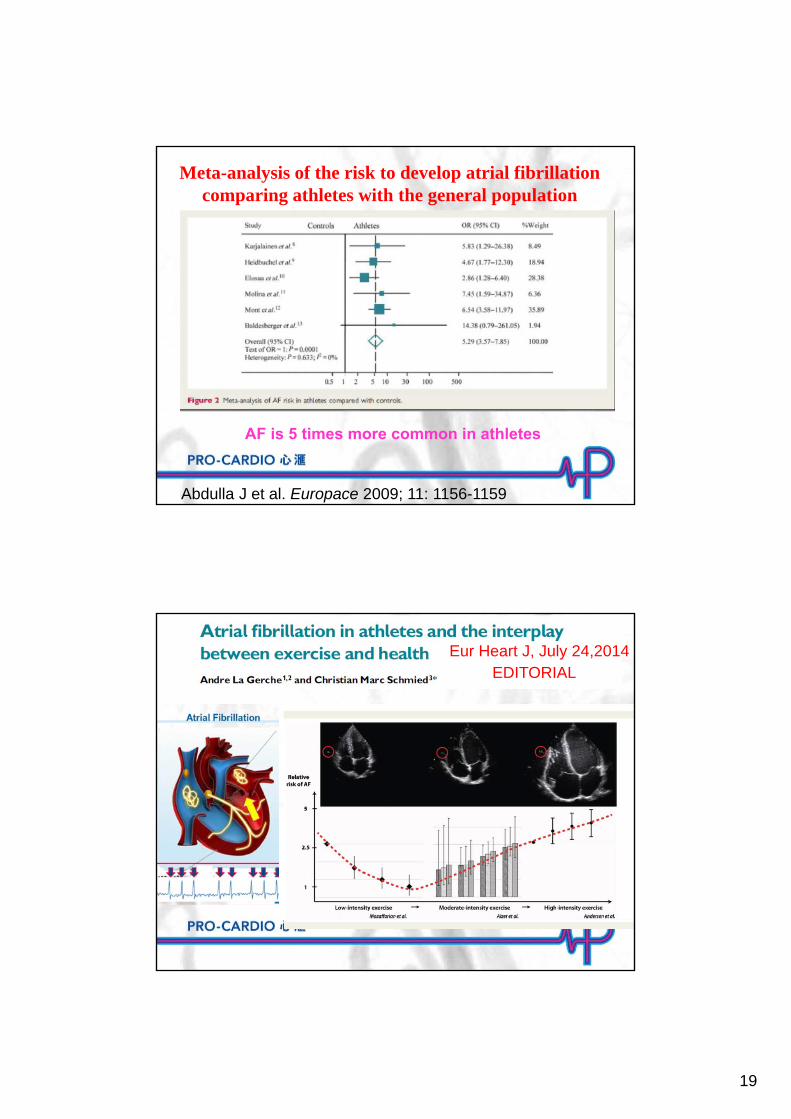
Meta-analysis of the risk to develop atrial fibrillationcomparing athletes with the general population
Abdulla J et al. Europace 2009; 11: 1156-1159
AF is 5 times more common in athletes
EDITORIALEur Heart J, July 24,2014
20
Marathon runningThe legend, 490 BC
22 miles run from the plains of Marathon to the city of Athens to report the victory of the Athenian army over the Persians. Upon his arrival, Pheidippedes exclaimed “Rejoice,
we conquer” and drop dead.
Marathon running- a slow roasting
• Hyperthermia:– 15X fold in heat production
• Hypothermia: - heat loss increase of 10 to 25 times
• Dehydration / Water intoxication• Glycogen depletion / hypoglycemia
– “ bonking” or “hitting the wall”: – depletion of 30 km worth glycogen
• Injuries (40 km takes 30,000 - 50,000 steps)• Upper respiratory tract infection / asthma
21
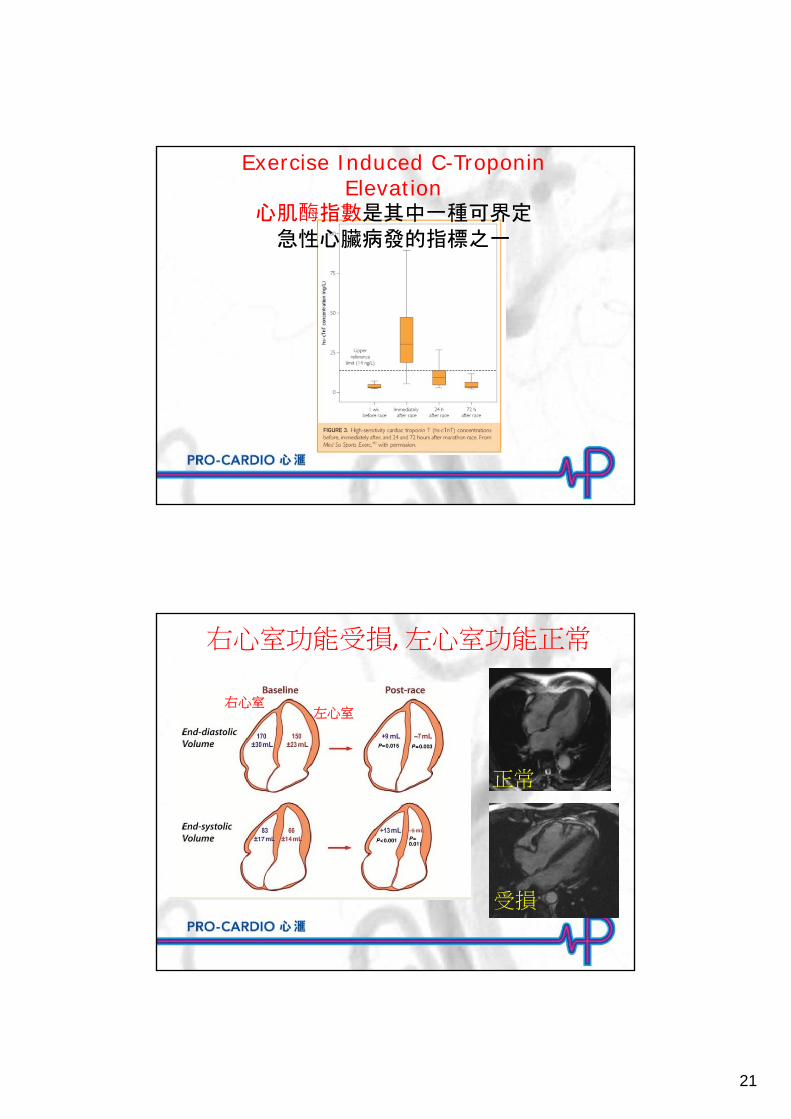
Exercise Induced C-Troponin Elevation
心肌酶指數是其中一種可界定急性心臟病發的指標之一
右心室功能受損, 左心室功能正常
右心室左心室
受損
正常
22
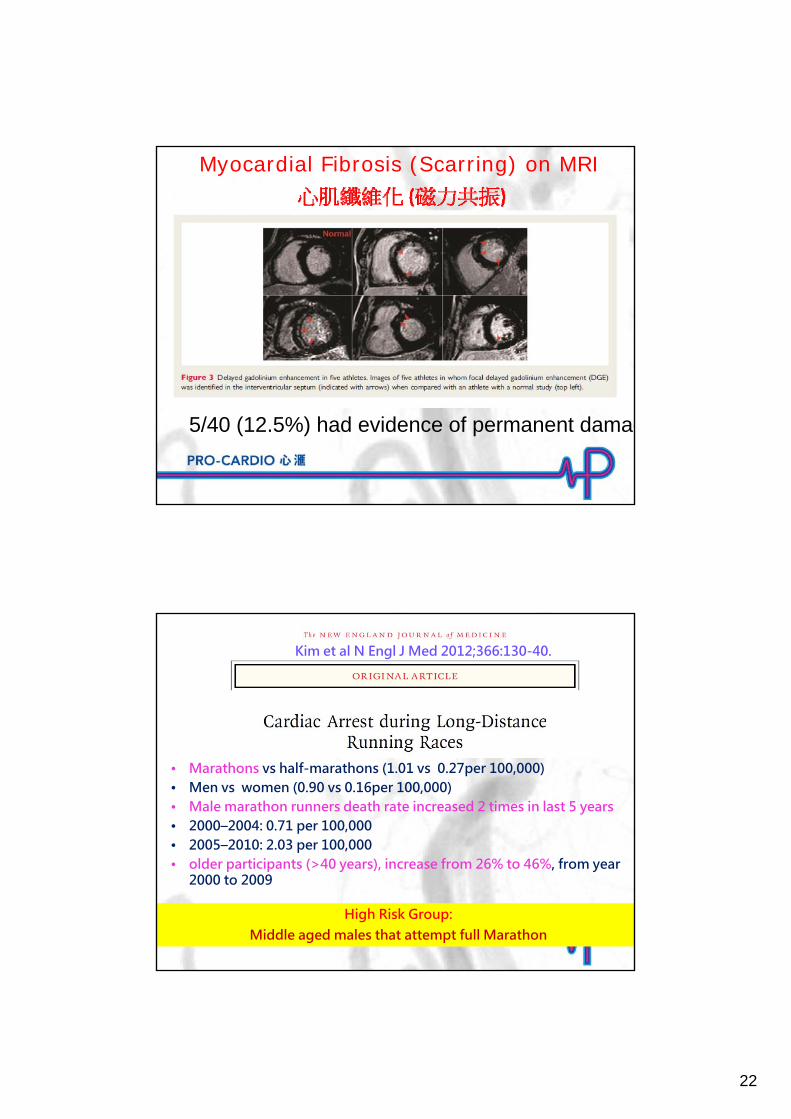
Myocardial Fibrosis (Scarring) on MRI
5/40 (12.5%) had evidence of permanent damag
Kim et al N Engl J Med 2012;366:130-40.
• Marathons vs half-marathons (1.01 vs 0.27per 100,000) • Men vs women (0.90 vs 0.16per 100,000) • Male marathon runners death rate increased 2 times in last 5 years• 2000–2004: 0.71 per 100,000 • 2005–2010: 2.03 per 100,000• older participants (>40 years), increase from 26% to 46%, from year
2000 to 2009
High Risk Group: Middle aged males that attempt full Marathon
23
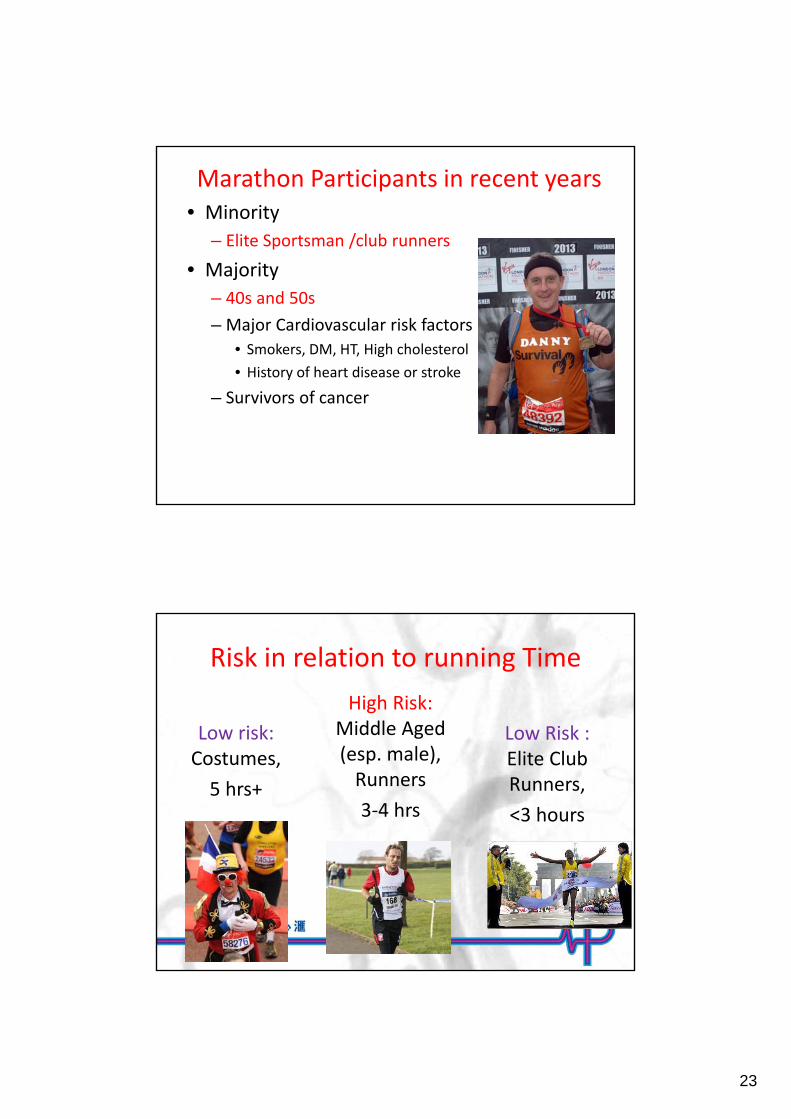
Marathon Participants in recent years • Minority
– Elite Sportsman /club runners
• Majority
– 40s and 50s
– Major Cardiovascular risk factors
• Smokers, DM, HT, High cholesterol
• History of heart disease or stroke
– Survivors of cancer
Risk in relation to running Time
Low Risk : Elite Club Runners,
<3 hours
High Risk: Middle Aged (esp. male), Runners
3‐4 hrs
Low risk: Costumes,
5 hrs+
24
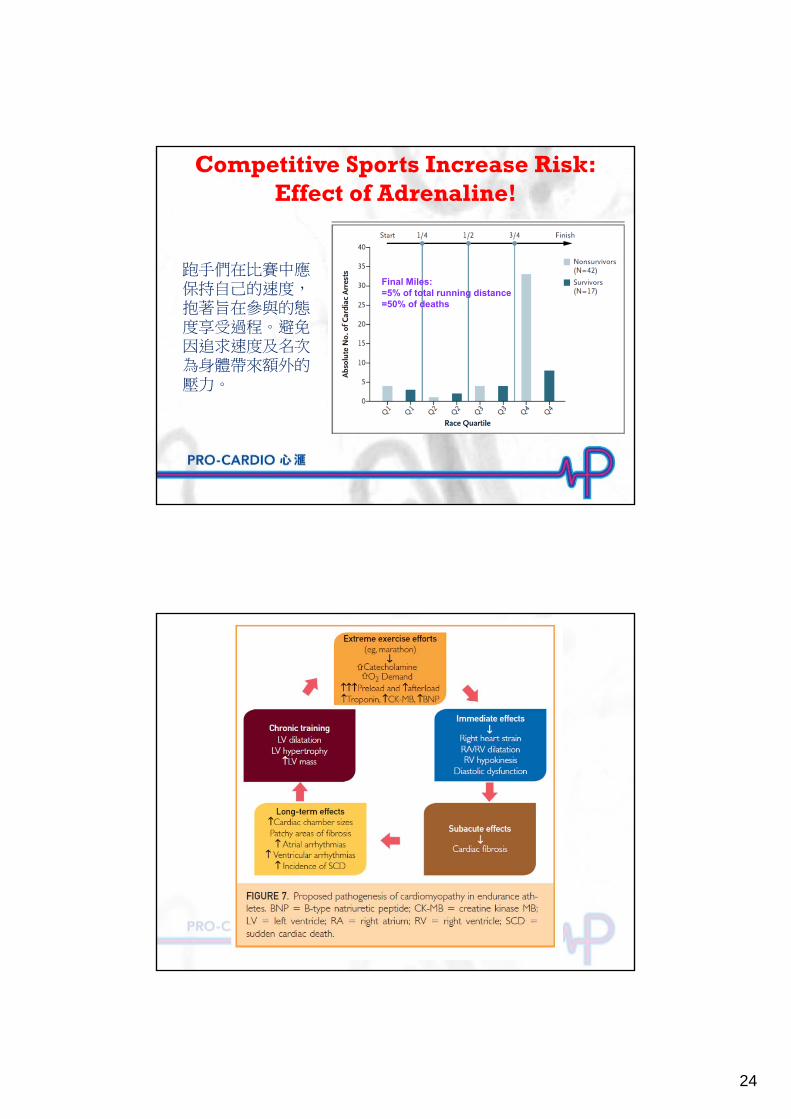
Competitive Sports Increase Risk:Effect of Adrenaline!
Final Miles:=5% of total running distance=50% of deaths
跑手們在比賽中應保持自己的速度,抱著旨在參與的態度享受過程。避免因追求速度及名次為身體帶來額外的壓力。
25
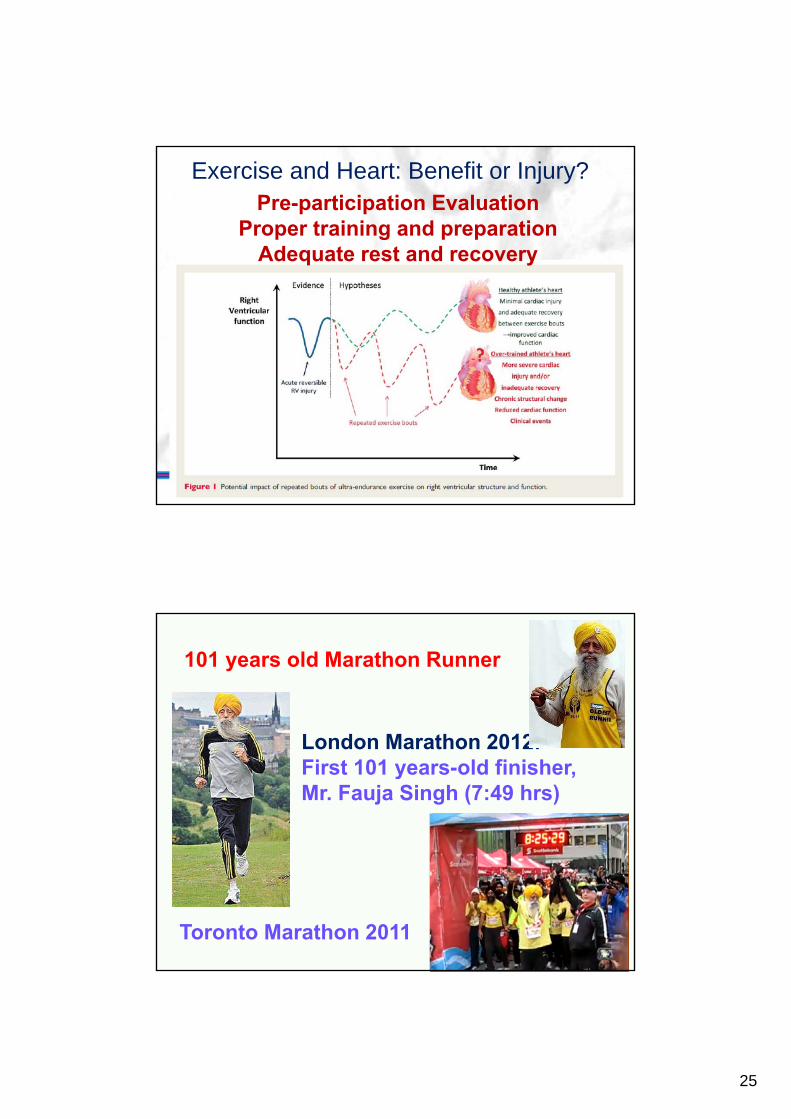
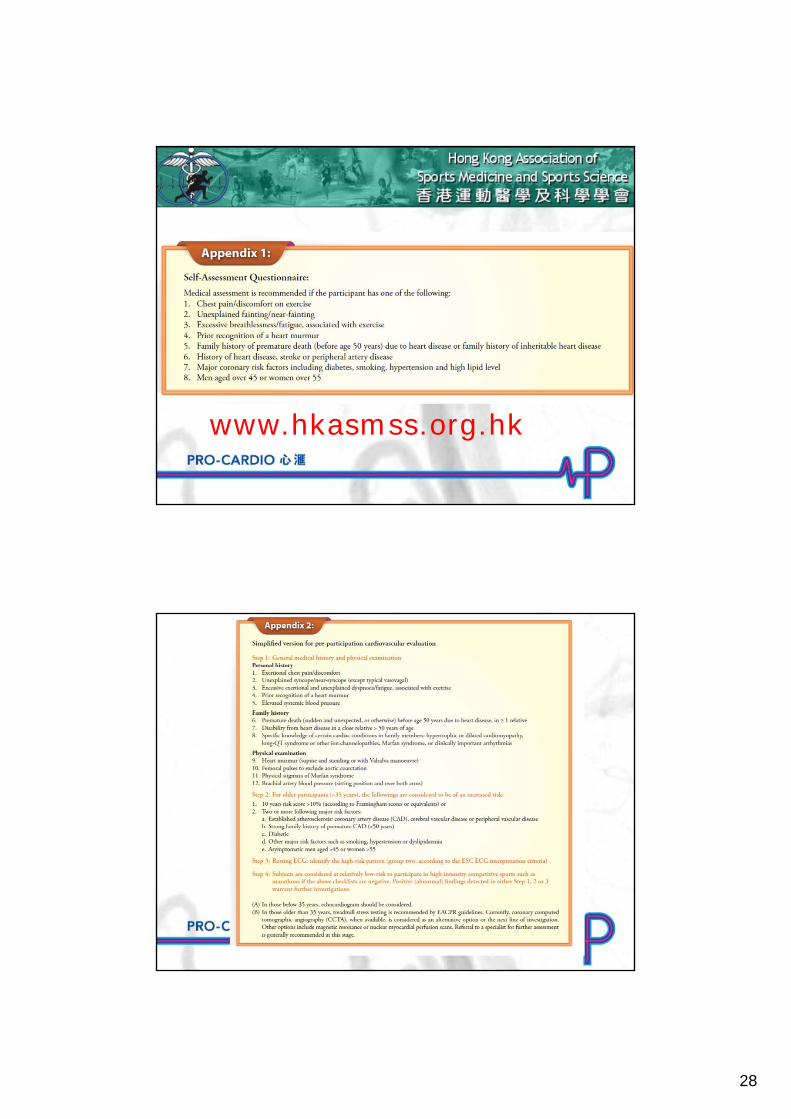
Pre-participation EvaluationProper training and preparation
Adequate rest and recovery
Exercise and Heart: Benefit or Injury?
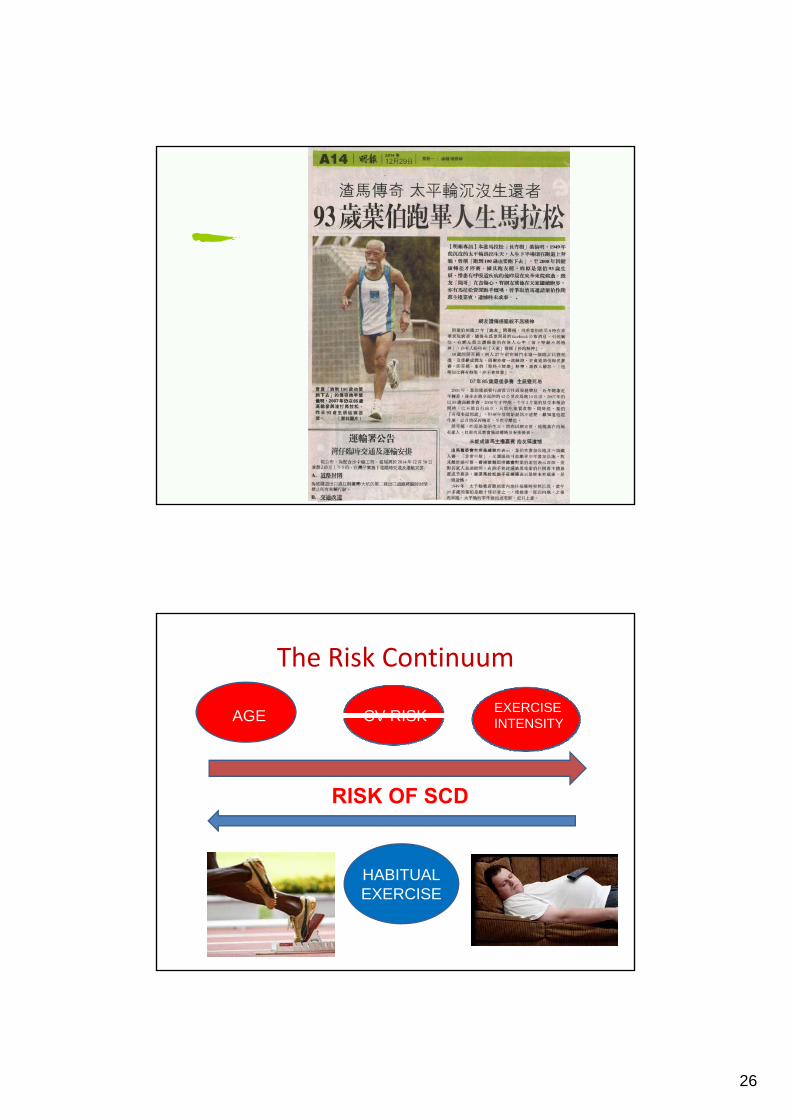
101 years old Marathon Runner
London Marathon 2012:First 101 years-old finisher,Mr. Fauja Singh (7:49 hrs)
Toronto Marathon 2011
26
The Risk Continuum
AGE CV RISKEXERCISEINTENSITY
HABITUALEXERCISE
RISK OF SCD

27
Major cause of SCD: < 35 years old – Hypertropic
cardiomyopathy (HCM)> 35 years old – coronary artery diseases
28
www.hkasmss.org.hk
29
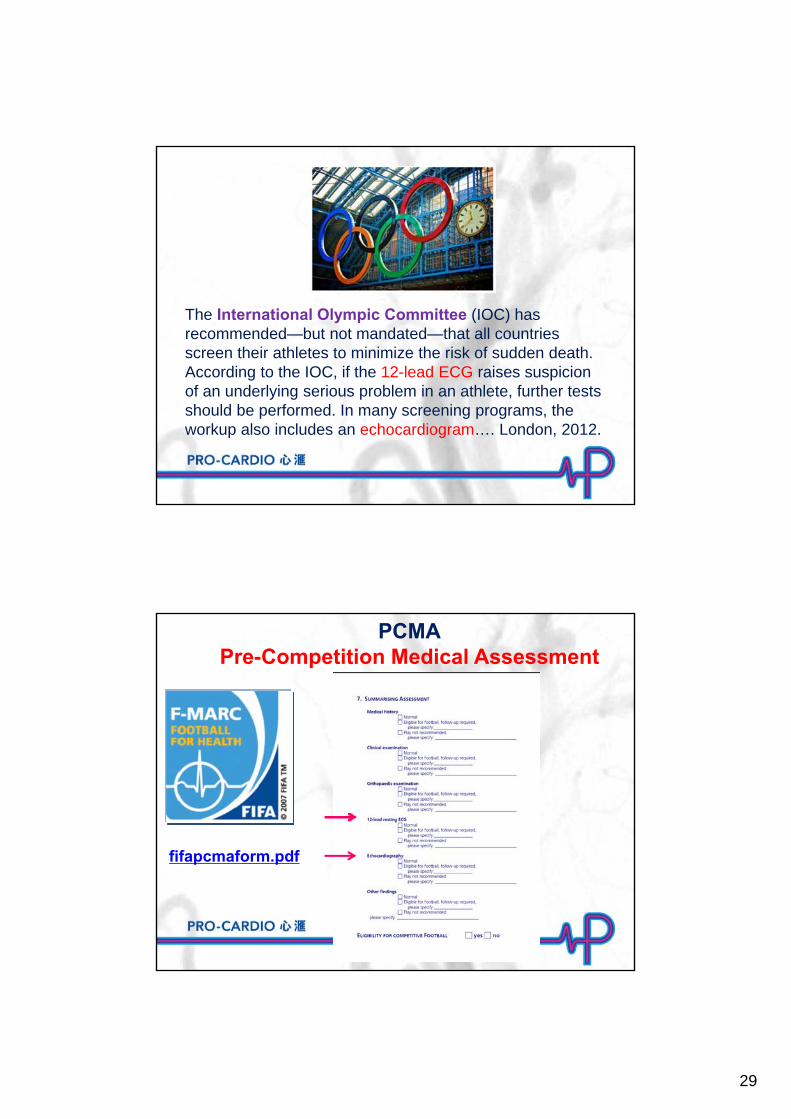
The International Olympic Committee (IOC) has recommended—but not mandated—that all countries screen their athletes to minimize the risk of sudden death. According to the IOC, if the 12-lead ECG raises suspicion of an underlying serious problem in an athlete, further tests should be performed. In many screening programs, the workup also includes an echocardiogram…. London, 2012.
fifapcmaform.pdf
PCMAPre-Competition Medical Assessment
30
Conclusion • Exercise related Sudden Cardiac Arrest (SCA) are not infrequent and are
potentially preventable. They are usually related to congenital or structural abnormalities in younger than 35 and coronary artery disease in those 35 years and above.
• The combination of carefully conducted history and examination (according to the 12‐element AHA recommendations) and 12‐lead resting ECG are generally effective screening protocols.
• The additional use of echocardiograms in the younger athletes (<35 years of age) and the low radiation dose Coronary CT Angiography in the old athletes (>35 years of age) are sensitive and specific in identify those at risk of exercise related sudden cardiac arrest.(SCA) .
• Pre‐participation Evaluation are recommended for high intensity competitive athletes especially the elite and professional athletes where resources are usually available.
以心為心
www.hkasmss.org.hk
www.pro-cardio.com





























