Embed Size (px)
Citation preview

全顎植體固定式贋復:治療思路與文獻回顧
Implant-Supported Full-arch Fixed Rehabilitation: Treatment Planning and Literature Review
劉閔結
新光吳火獅紀念醫院牙科部
摘要 本文將探討在自然牙全數皆缺失的上或下顎,如何診斷與訂立治療計畫,並且依
其邏輯執行診斷步驟,佐以文獻回顧與病例討論。
前言 當自然牙皆缺失而患者期待以人工植體來重建原來的美觀與咬合時,其治療計畫
與複雜度高於全口自然牙重建。因為病理性破壞與缺牙所造成的齒脊喪失使得人
工植體難以置放在與原來自然牙跟相同的 3D 位置。加上在逐漸缺牙的過程中,
患者咀嚼模式不良的適應與改變,可能需要重新引導與建立咬合。人工植牙的咬
合觀念和想法、軟組織的附連與型態、植體周圍骨質在咬合壓力與贋復體生物力
學等因素影響下的穩定度,都影響著植體的成功與患者的滿意度。 現在的醫療環境與挑戰,已經不是只要植入得到 Osseointegration 就可以滿足的
時代。而是需要跨科整合治療、醫病溝通與實證醫學來輔助完成人工植牙的全顎
贋復。
治療計畫之考量與術前診斷 植體全顎贋復常見的選擇有: 1. Implant-support/retained overdenture 2. Implant fixed partial denture 3. Fixed complete denture (also Fixed detachable or hybrid denture)
Implant Overdenture 包括 ERA, ball attachment, Locator, Dolder/Hader bar, milled bar, telescopic attachment 等。固定式的則常見的有 Implant FPD 以及 Fixed

complete denture 兩種,兩者的差異應該 Fixed complete denture 的組成包含
Supporting superstructure 以及 denture teeth,而不燒瓷,所以在金屬骨架設計與材
料選用與 FPD 非常不同。這一類固定贋復物如果使用『Fixed detachable』來稱
呼,在字義上容易與 Screw-retained FPD 混淆,因為同樣可以拆卸下來。Implant FPD 則包含 PFM 及 All-ceramic 兩種,類似傳統的 FPD,可以 Cement-retained 或者 Screw-retained。 治療計畫在訂立之時需要考量的重點如下: 1. Available Bone: 包括寬度與高度、Type I ~ IV quality、Anatomic structure 2. Maxillomandibular relationship 3. Arch form 4. Interocclusal space 5. Implant number 6. Patient factors Available Bone
Premaxilla 在拔牙後三年會喪失掉原來 40-60%的寬度,因此植體的選擇通常
沒有辦法與原來的牙根相近。以上顎正中門牙為例,牙根在 CEJ 以下 3mm 處的
直徑約略是 5-8mm 左右。自然牙缺失後 Bundle bone resoprtion,合併寬度與高度
的喪失,尤其以頰側高度降低平均>2mm 最為明顯。經過三年之後牙脊的寬度通
常只剩 3-5mm,時間更久甚至於<3mm 或者 Knife-edge。此區域的植體經過 GBR或者 Bone block 或許可以植入 3.3-4.1mm 直徑的植體,至於 Knife-edge alveolar ridge 可能無法植牙。這樣衍生的問題是,前牙與後牙的殘脊方向通常不一樣,
如果要將前後區的植體相連為一個大的贋復體必須儘量將植體取得平行,在已經
相當薄的前牙殘脊,要將植體方向往舌側傾斜或者垂直咬合面以平行後牙植體,
往往無法達成。儘管使用 Angled abutments 在某些情況可以改正平行度,但是植
體角度差異過大仍會造成印模以及 Framework try-in 上的誤差與困難。因此須考
慮調整治療計畫,例如將贋復物分段、Screw-retention 或者活動式贋復等。 另外,下顎後牙區下齒槽神經及上顎竇構造等重要組織都是植體無法侵犯的區
域。在進行全顎重建時,一個 Cone Beam CT scan 完整的探測可用的軟硬組織結
構是擬定治療計畫的第一步。 Maxillomandibular Relationship 上下顎間關係,不僅僅決定了患者的美觀與咬合型式。通常也代表了這一個
患者過去在這特定顎間關係(e.g. Severe Class II or Class III)的咀嚼習慣。 以一個 severe Class III skeletal relationship 患者為例,其咬合重心可能位於後牙。
如果因為後牙殘脊吸收使得種植體集中於前牙區,相對少數的後牙植體或是
Distal cantilever 會受到咬合壓力而出現各種併發症,例如贋復體鬆脫、斷裂、

Marginal bone loss 等。 Arch form 牙弓的型態影響植體的分布以及 Biomechanical properties,尤其是當考量有
distal cantilever 時,A-P spread 的長度在 Taper arch 較 Square arch 有利。然而,
過去關於 A-P spread 的文獻相當有限,其中被教科書所引用的 English(1990) 數據: A-P : Distal cantilever = 1 :1.5 完全沒有實驗數據,只是該作者的個人意見。另
外,Implant-abutment connection 在其後出現了許多重大的改變,internal geometric connection 或是 conical connection(含 Morse taper)究竟對於 A-P spread 是否有影
響,仍待觀察。(Fig.1) Fig.1 Square 及 taper arch form 可能會出現不同的 A-P spread
Interocclusal Space 上下顎贋復空間過多與過少皆會造成問題。Interocclusal space 的估量是指從
對咬牙之咬合面到 Implant platform(或者 bone crest)的空間,根據 Phillips 1(1995)的意見,Fixed-detachable(hybrid denture)所需的空間為 18mm = tissue depth (3mm) +hygiene (2mm) + framework (8mm) + pink acrylic (2mm) + denture tooth (3mm) 其中 Hygiene space 應該可以節省至 1mm(使用牙間刷清潔)或者 0mm(牙線清潔)。 Framework 之設計與 denture tooth 所需之空間也可能不同。LoCascio and Salinas 2(1997) 則是估算為 15mm。 相較於 Bar and clip overdenture 所需空間 14mm=tissue depth (3mm) + hygiene (1.5 mm) + bar (4.5mm) + acrylic and housing (2mm) + denture tooth (3mm) 。 以及 Implant Fixed Partial Denture (PFM)的 9-12mm=tissue depth (3mm) + abutment (4-7mm) + occlusal restoration space (2mm)。可知 Fixed detachable prostheses 空間需求相對較多。甚至如果製作 Two-piece superstructure for fixed detachable (Wee3 1997)可能會再多出 2mm( for fixed frame)的需求。

另一方面,當嚴重的殘脊吸收造成 Interocclusal space 相當多時,
Crown-implant ratio(C/I)會變得很大。儘管對於多大的 C/I 會影響 marginal bone level 目前沒有定輪,Malchiodi et al4(COIR 2013)指出 Critical threshold of crown-implant ratio 介於 3.1-3.4 之間。超過這個數值容易造成過度的邊緣骨喪
失。舉例來說,如果某下顎後牙植體的長度在 8-12mm 之間,則合理的贋復空間
應該在 24-36mm。這樣的數值看起來似乎很安全,但只代表著邊緣骨喪失的臨
界值,不能代表沒有贋復方面的併發症。另一篇 2014 年的 systematic review(Garaicoa-Pazmiño et al5)則指出 C/I ratio 顯著地對於 marginal bone level 有影響。過大的贋復空間和 C/I ratio 也意味著咬合面距離 Implant platform 增加,
同樣的咬合力因為力臂增加使得 Implant-abutment connection 的壓力也同時增
加。3-D Finite Element 的研究 6(2013)證明在當 Crown 或者贋復體變得越高時,
咬合所產生的側向力會增加Bone crest及 Implant-abutment connection附近的壓力
(Fig.2A-C)。如此一來,很容易造成螺絲與交接面的磨耗,最後導致斷裂或鬆脫。
另外,當 restorative space 變大時,metal framework 必須隨著增加以支持
porcelain,否則容易瓷裂。當金屬量變大時,鑄造與焊接的誤差也會隨之變大。
傳統 FPD 製作的困難度也會提高。燒瓷的過程中,因為金屬體積大使得降溫速
度變慢,燒結降溫的過程也要減慢以面殘餘應力產生瓷裂。 若是製作 overdenture,在 interocclusal space 相當多的情況使用類似 Locator等空間需求少的 attachment 也未必有好處。如同先前的論述,當咬合面距離
attachment 遠時,力臂增加勢必使得 attachment 受到比較大的力矩而翻動。可能
造成穩定性降低或著磨耗加快。因此,可以考慮使用 Bar and click 或者 Milled bar with Locator 將 Attachment 的位置從接近牙脊的位置提升到接近咬合面以增加
retention/stability。 Fig.2A-C C/I ratio and occlusal load distribution (de Moraes et al, 2013) A. Oblique occlusal load
B. Aixal occlusal load

C. Abutment screws(由左至右為 C/I ratio 由小至大)
Implant Number 植體的數量不僅決定固定贋復物的設計與分段,同時也主導著美觀和生物力
學考量。以上顎為例,六支、七支或八支 implant 的治療計畫會將 implant 放置
在不同的位置上。(Fig.3) 因骨質密度差異以及下顎後牙區常見嚴重吸收難以植牙,上顎區常會出現比
下顎多的植體數目。 下顎植體若考量 Cross-arch splinting 應注意 mandibular flexure/torsion 的問
題,尤其是嚴重吸收的下顎骨,患者在張口時以及單側作 Power chewing 都會因
為咀嚼肌的運動力量使下顎產生向中心收縮或著單側扭轉的形變(Fig.4,5)。Cross-arch splinting 不僅僅影響患者的關節、肌肉或韌帶的舒適度,對於贋復醫
師而言最大的問題是在張口印模時的 Mandibular flexure,誤差可能會被轉移到
Master cast 之上。 近年來 All-on-four concept 逐漸在 Case control studies 及 systematic review 中
出現,Butura et al7(2011)在 DCNA 上關於下顎 All-on-four 三年 857 支植體的臨
床研究(Fig.6),Cumulative survival rate 為 99.6%。Balshi et al8(2013)回顧上顎 300支及下顎 500 支使用在 All-on-four protocol 植體的臨床存活率,分別為
96.3%(maxilla)及 97.8%(mandible)。這些成功率報告顯示了對於全顎固定式的作

法,在適當的選擇患者條件之下,All-on-four protocol 是一個可以接受的選項。 Fig.3 Implant number and design for full-arch implant FPD
Fig.4 Mandibular flexure
Fig.5 Milled bar splinting mandibular implants may also be affected by mandibular flexure
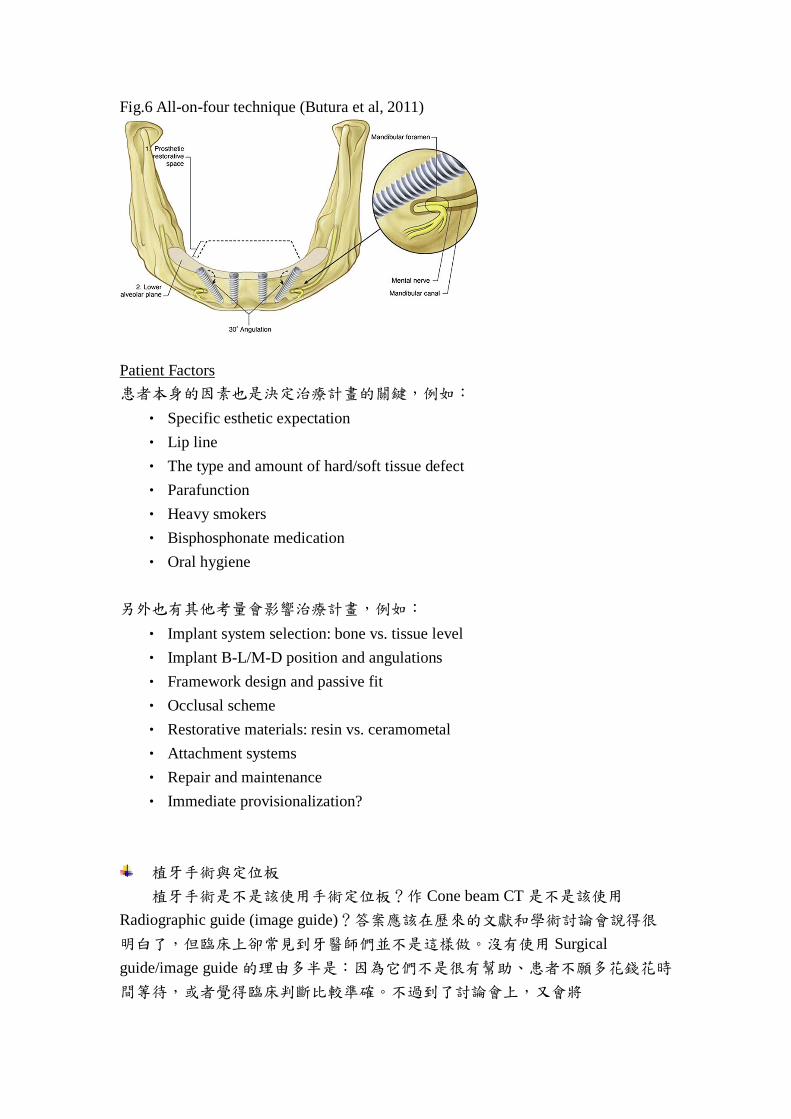
Fig.6 All-on-four technique (Butura et al, 2011)
Patient Factors 患者本身的因素也是決定治療計畫的關鍵,例如:
• Specific esthetic expectation • Lip line • The type and amount of hard/soft tissue defect • Parafunction • Heavy smokers • Bisphosphonate medication • Oral hygiene
另外也有其他考量會影響治療計畫,例如:
• Implant system selection: bone vs. tissue level • Implant B-L/M-D position and angulations • Framework design and passive fit • Occlusal scheme • Restorative materials: resin vs. ceramometal • Attachment systems • Repair and maintenance • Immediate provisionalization?
植牙手術與定位板 植牙手術是不是該使用手術定位板?作 Cone beam CT 是不是該使用
Radiographic guide (image guide)?答案應該在歷來的文獻和學術討論會說得很
明白了,但臨床上卻常見到牙醫師們並不是這樣做。沒有使用 Surgical guide/image guide 的理由多半是:因為它們不是很有幫助、患者不願多花錢花時
間等待,或者覺得臨床判斷比較準確。不過到了討論會上,又會將

Restorative-driven (or esthetic-driven) implant placement 的概念拿出來講。 這樣實際的臨床情況其實恰恰好反映了一個重要的問題,如果 surgical guide不夠精準(To be dead on!),那麼反而會造成誤差,手術醫師沒有辦法完全的依賴
而必須當場作調整。一個準確而實用的手術定位板,不僅只是參考贋復方面的需
求,應該要考量手術完成的困難程度。齒槽骨的寬度與高度僅管可以利用 GBR或 Bone block 去作增加,但是過大角度的植體或是無法取得 Primary stability,都可能造成補骨程序困難。因此設計手術定位板的醫師應當充分理解植體手術步
驟與患者狀況,利用 X 光片及 CT 反覆確認與更正植體位置。如果沒有充分把握
確切位置,可以考慮使用 Non-restricted guide(e.g. vacuum formed matrix),界定植
體合理的範圍,讓手術醫師當場決定。 植體置入前診斷與前置作業參考流程: 1. Diagnostic setup/waxup 2. Esthetic try-in 3. Occlusal scheme and interocclusal space evaluation 4. Radiographic guide duplicating the waxup 5. Bone augmentation before implant placement 6. Re-evaluation of bone volume 7. Surgical guide/template
病例討論 上顎植體固定贋復:Implant-supported PFM FPD Fig.7 Presurgical frontal view

Fig.8 Presurgical occlusal view
Fig.9 Presurgical panoramic film
Fig.10A&B Diagnostic setup
A.

B.
Fig.11 Radiographic guide
Fig.12A-D Implant surgery with use of surgical guide

A.
B.
C.

D.
Fig.13A&B Implant healing and final impression
A.
B.

Fig.14A-D Provisional FPD with pink acrylic gingival
A.
B.
C.

D.
Fig.15A-D Framework try-in
A.
B.

C.
D.
Fig.16A-F Final implant abutment and prostheses
A.

B.
C.
D.

E.
F. Reference
1. Phillips K, Wong KM. Vertical space requirement for the fixed-detachable, implant-supported prosthesis. Compend Contin Edu Dent 2002 Aug 23(8):750-6
2. LoCascio SJ, Salinas TJ. Rehabilitation of an edentulous mandible with an implant supported prosthesis. Pract Periodontic Aesthet Dent1997; 9:357-70
3. Golden et al. Fabrication of a two-piece superstructure for a fixed detachable implant supported mandibular complete denture. J Prosthet Dent 2000;84:205-9
4. Malchiodi L, Cucchi A, Ghensi P, Consonni D, Nocini PF. Influence of crown-implant ratio on implant success rates and crestal bone levels: a 36-month follow-up prospective study. Clin Oral Implants Res. 2014 Feb;25(2):240-51

5. Garaicoa-Pazmiño C, Suarez F, Monje A, Catena A, Ortega-Oller I, Galindo-Moreno P, Wang HL. Influence of Crown-Implant Ratio Upon Marginal Bone Loss. A Systematic Review. J Periodontol. 2014 Jan 20 Epub ahead of print.
6. de Moraes SLD, Verri FP, Santiago JF, Almeida DA, Mello CC, Pellizzer EP. A 3-D Finite Element Study of the Influence of Crown-Implant Ratio on Stress DistributionBraz. Dent. J. vol.24 no.6 Ribeirão Preto Nov./Dec. 2013
7. Butura CC, Galindo DF, Jensen OT. Mandibular all-on-four therapy using angled implants: a three-year clinical study of 857 implants in 219 jaws. Dent Clin North Am. 2011 Oct;55(4):795-811.
8. Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF. Retrospective Analysis of 800 Brånemark System Implants Following the All-on-FourTM Protocol J of Prosthodont 2013Jul 25:1-6 [Epub ahead of print]