Embed Size (px)
Citation preview
Introduction
Transdermal delivery of β-blockers continues to be an area of active research due to its fame in the man-agement of cardiovascular disorders (Aqil et al., 2006; Jamakandi et al., 2006). Among the β-blockers, meto-prolol, a β-1 selective antagonist adrenergic blocker, remains in the mainstay of cardiovascular therapy. It is the primary choice in the treatment of stable mild-to-moderate chronic heart failure (caused due to left ven-tricular systolic dysfunction), and is valuable in patients with ischaemic or dilated cardiomyopathy. This agent also plays a vital role in the management of angina pec-toris and moreover is useful in post-infarction patients
(Prakash & Markham, 2000). However, the efficacy of this drug is limited by its extensive first pass metabolism fol-lowing oral administration and short biological half-life (∼ 4 h), which required frequent dosing. The potential of transdermal route by virtue to avoid the hepatic first pass effect, sustained delivery of drugs to provide a steady plasma profile and condensed dosing frequency is pro-jected to be an alternative for this category of drugs. This delivery route exploits skin, the largest and most easily accessible organ of the body, to deliver drug molecules with diverse chemical properties (Ghosh et al., 1997).
Although the transdermal route represents a promising method for drug delivery, the hindrance created by the uppermost layer of skin, the stratum corneum (SC),
Drug Delivery, 2011; 18(1): 19–25
Address for Correspondence: Dr Anroop Nair, Professor, M.M. College of Pharmacy, M.M. University, Mullana, India-133203. Tel: 91-173-130-4255. E-mail: [email protected]
R E S E A R C H A R T I C L E
Effect of permeation enhancers on the iontophoretic transport of metoprolol tartrate and the drug retention in skin
Anroop Nair1, Hiral Vyas2, Jigar Shah3, and Ashok Kumar1
1M.M. College of Pharmacy, M.M. University, Mullana, India, 2PES College of Pharmacy, Bangalore, Karnataka, India, and 3Department of Pharmaceutical Technology, Nirma University of Science & Technology, Ahmedabad, India
AbstractUtilization of chemical penetration enhancers in conjunction with iontophoresis is regarded as the most effective method to enhance the passage of molecules across the skin barrier. A systematic approach to enhance the transdermal delivery of metoprolol tartrate and the subsequent release of the drug depot in the skin was investigated. Gel formulations with proximate viscosity were prepared and assessed for the effect of polymers (carbopol, hydroxypropyl methyl cellulose, and methyl cellulose), permeation enhancers (5%w/w, sodium lauryl sulfate (SLS), dimethyl formamide, n-methyl-2-pyrrolidone, and polyethylene glycol 400), and the combination approach (permeation enhancers with iontophoresis–0.5 mA/cm2) on the drug delivery. The flux values observed in passive (4.59–5.89 µg/cm2/h) and iontophoresis (37.99–41.57 µg/cm2/h) processes revealed that the permeation of metoprolol was not influenced by the polymers studied, under similar conditions, and further studies were carried out using carbopol gel as a representative polymer. Appreciable enhancement (∼ 5-fold) in drug delivery was observed with SLS in the passive process while the optimum iontophoretic delivery condition ensured better delivery (∼ 7-fold). Combination of ionto-phoresis with SLS further enhanced the drug delivery (∼ 9-fold) and leads to noticeable drug retention in the skin as well. Moreover, the drug retained in the cutaneous layer of the skin eventually released over a period of time (5 days) and followed a near first order profile. This study concludes that the combination of iontophoresis with SLS augmented the metoprolol delivery and rendered skin drug depot, which eventually released over a period of time.
Keywords: Transdermal; metoprolol; iontophoresis; permeation enhancers; drug depot
(Received 14 February 2010; revised 14 June 2010; accepted 14 July 2010)
ISSN 1071-7544 print/ISSN 1521-0464 online © 2011 Informa Healthcare USA, Inc.DOI: 10.3109/10717544.2010.509361 http://www.informahealthcare.com/drd
Drug Delivery
2010
18
1
19
25
14 February 2010
14 June 2010
14 July 2010
1071-7544
1521-0464
© 2010 Informa Healthcare USA, Inc.
10.3109/10717544.2010.509361
DRD
509361
UDRD
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

20 A. Nair et al.
limits the access of drug into the systemic circulation. As a consequence there has been intensive research for the development of strategies to modulate the skin barrier and thereby facilitate the drug delivery (Hadgraft, 1999). Among these, chemical penetration enhancement and iontophoresis techniques are widely investigated and accounted as promising (Mitragotri, 2000; Wang et al., 2005). The role of a chemical enhancer is to reduce the skin barrier property (reversibly) without influencing the viable cell and eventually promote the drug permeation. Alternatively, application of a low electric current which enhances the transdermal transport of drugs is well documented. Additionally, the current trend is by pairing two such enhancing techniques to attain an upper limit of drug delivery, simultaneously reduce the skin toxicity, and improve the patient compliance (Mitragotri, 2000; Wang et al., 2005; Mutalik et al., 2009).
The current scenario of the transdermal delivery of beta blockers was described in a recent review (Aqil et al., 2006). Few attempts have been made to enhance the transdermal delivery of metoprolol, using chemi-cal permeation enhancers, pro-drugs, and physical approaches with matrix patches or solution systems (Aqil et al., 2006; Jamakandi et al., 2006; Anroop et al., 2008). However, we believe that a suitable delivery system is of utmost importance for the successful transdermal deliv-ery of drugs. Compared to the transdermal patch, the gel system is more advantageous in clinical application as it can match the contours of the skin and reduces local skin reactions (de Figueiredo Alves et al., 2000). Regarding iontophoresis, the gel formulation was widely used as it can be easily amalgamated with the iontophoretic system and the higher water content will benefit better uniform electrical conductivity (Fang et al., 1996). Moreover, sev-eral iontophoretic studies using gel-based formulations were found to deliver significantly a higher amount of drug across the skin (Nair & Panchagnula, 2003; Pillai & Panchagnula, 2003; Ghosh et al., 2009). To our knowl-edge, this is the first report which explored the feasibility of transdermal drug delivery of metoprolol using a gel system. Moreover, the application of iontophoresis with chemical enhancers to augment the metoprolol trans-port was not studied comprehensively. The objective of the current study was to assess the potential of different chemical enhancers and their combination with ionto-phoresis in the transdermal delivery of metoprolol, from a gel system.
Materials and methods
Materials
Metoprolol tartrate (Intas Pharm. Ltd. Ahmedabad, India), Carbopol 941 NF (B.F. Goodrich Co., Cleveland,
OH), and Hydroxy propyl methyl cellulose K4M (HPMC; Colorcon, Goa, India) were received as gratis samples. Methyl cellulose M 0512 (Sigma Aldrich, St Louis, MO), Poly ethylene glycol (PEG 400; S.D Fine chem., Mumbai, India), N-methyl-2-pyrrolidone (NMP: S.D Fine chem), Sodium lauryl sulfate (SLS; S.D Fine chem), Di methyl for-mamide (DMF: S.D Fine chem), and Ethanol (Ranbaxy, New Delhi, India) were procured commercially. All other chemicals and reagents used were of analytical grade. All solutions were prepared in ultra pure water.
Analytical method
The amount of metoprolol tartrate in the samples was quantified using a high performance liquid chromatog-raphy (HPLC) system (Shimadzu, LC-10ATVP, Japan) consisting of a Phenomenex C18 analytical column (4.6 × 250 mm, Luna, 5.0 µm). The column was main-tained at ambient temperature and the compounds were eluted at a flow rate of 1.0 ml/min. Acetonitrile: 100 mM pH 7.0 phosphate buffer (20:80) was used as mobile phase (Kaliszan et al., 1995). The injection volume was 20 µl and the column effluent was monitored at 222 nm. The method was validated by determination of linearity, precision, and accuracy.
Preparation of the metoprolol tartrate gels
Required quantities of polymers [carbopol 941 (1.5% w/v), HPMC (2% w/v), or methyl cellulose (5% w/v)] were weighed and soaked separately in ultra pure water overnight (12 h). Metoprolol tartrate (20 mM), enhanc-ers (5% w/w) was added to the swelled polymers and stirred gently with a mechanical stirrer to ensure the uniform dispersion of the polymer. For carbopol gel the pH was adjusted to 7 ± 0.2 by adding triethanolamine with gentle stirring. Sodium benzoate (0.1%) was finally incorporated, as a preservative, and mixed well to obtain a uniform gel. The drug content was determined in all the batches and was found to be between 93–97%.
Skin membrane preparation
From a local abattoir, ears were obtained from freshly slaughtered pigs. The skin was removed carefully from the outer regions of the ear and separated from the underlying cartilage with a scalpel. After separating the full thickness skin, the fat adhering to the dermis side was removed using a scalpel and isopropyl alcohol. Finally the skin was washed with water and stored at −20°C and was used within a week.
The AC electrical resistance of the full thickness skin was measured by placing a load resistor R
L (100 kΩ) in
series with the skin. The voltage drop across the whole circuit (V
0) and across the skin (V
S) was measured
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Effect of permeation enhancers on the transdermal iontophoresis of metoprolol 21
using an electrical set-up consisting of a custom-made waveform generator and a digital multimeter. For meas-uring resistance, a voltage of 100 mV was applied at 10 Hz and the skin resistance in kΩ was approximated from the formula
RV R
V VSS L
S
=−0
where RS is the skin resistance and R
L is the load resistor
in kΩ. Skin with resistance > 20 kΩ.cm2 was used in the current study.
In vitro permeation studies
The in vitro permeation studies were carried out in a Franz diffusion cell (Neutron scientific, Kolkata, India) using porcine skin. The excised skin was mounted between the half-cells with the dermis in contact with receptor fluid and was equilibrated for 1 h. The receiv-ing chamber contained 10 mL of phosphate buffered saline (PBS pH 7.2) and the area available for diffusion was 0.74 cm2. The receiver compartment was stirred at 600 rpm with a 3-mm magnetic stir bar at 37 ± 0.5°C. Formulated gel (20 mM, 1 mL: gel as solution was not used) was placed in the donor chamber. Anodal ionto-phoresis was carried out by using a single channel power supply (Ultra pure Scientific, Mumbai, India). Ag/AgCl wire electrodes (0.5 mm diameter; Alfa Aesar, Wardhill, MA) were fixed at a distance of 2 mm from the skin sur-face in donor and receiver chambers. The anode was connected to the donor and the cathode to the receiver chamber. A constant current of 0.5 mA/cm2 was applied for a period of 6 h. The drug contained in each sample taken has been considered in order to calculate the cumulative amount of metoprolol permeated. Similarly, passive permeation control experiments were run in par-allel without iontophoresis (0 mA/cm2 current density) for comparison. After application of current or passive delivery, the receptor compartment was analyzed for metoprolol concentration and the cumulative amount of metoprolol permeated into the receiver chamber normalized to the surface area exposed to the drug was expressed as µg/cm2.
Metoprolol release from the skin
The skin was loaded with metoprolol using gel formu-lations containing chemical enhancers in conjunction with iontophoresis (0.5 mA/cm2) or a passive process for 6 h (similarly by the permeation study protocol). Immediately after the permeation studies, the donor (gel formulation) and receiver (PBS) were removed. The donor side was washed with 50% ethanol-water twice (1 mL), wiped with a kimwipe®, and kept occluded.
Fresh medium of phosphate buffered saline (PBS pH 7.2) containing 0.005% sodium azide (preservative) was replaced in the receiver and was stirred at 600 rpm with a 3-mm magnetic stir bar at 37 ± 0.5°C. The samples were withdrawn at regular intervals (up to 6 days) and the amount of drug released into the receiver compartment was analyzed.
Drug retained in skin
Immediately after the permeation studies the gel from the donor was removed. The skin was washed, after removing from the diffusion cell, with 50% ethanol-water twice (1 ml), wiped with a kimwipe®, and the active dif-fusion area was separated using a biopsy punch. The skin was cut into fine pieces (∼ 1 mm), soaked in a vial containing PBS (2 ml) and kept in a shaker water bath at 37 ± 0.5°C for 24 h. Then the vials were vortexed for 2 min, centrifuged (5000 rpm), and filtered (0.2 µm Millex syringe driven filter unit, Millipore Corporation, Bedford, MA). The extraction procedure was repeated until the drug concentration in the extracted fluid was detectable (the extraction period varied between 24–72 h). Amount of drug in the skin with different treatments was deter-mined by HPLC. This procedure was standardized by injecting different drug concentrations (10–200 µg) and the recovery was found to be 88 ± 5%.
Data analysis
The cumulative amount of drug permeated per unit skin surface area was plotted against time and the slope of the linear portion of the plot was estimated as the steady-state flux (Jss). Flux enhancement was calculated as the ratio of the flux of the enhancer/iontophoresis to the flux of control permeation. Statistical analysis was performed by one-way analysis of variance (ANOVA) and a t-test using Graphpad prism 5 (graphpad software, Inc., CA) to test the effects of various treatments. The data points pro-vided in the graphs are an average of six trials. The error bars represents the standard deviation. A significance level of p < 0.05 denoted significance in all cases.
Results and discussion
Preliminary in vitro permeation studies were carried out to assess the effect of metoprolol concentration (5–20 mM) on the permeation rate. The data obtained were in support to the known theory that the higher the drug concentration, the greater is the flux (data not shown). Hence, the highest concentration tested (20 mM) was selected for further studies. In the next stage, we evaluated the effect of the three polymers on the transdermal delivery of metoprolol by passive and
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

22 A. Nair et al.
iontophoretic delivery. To hold promise for further in vivo investigations, polymers which are most com-monly employed in the transdermal gel fabrication were selected. Described herein before, three polymers (carbopol, HPMC, and methyl cellulose) were selected based on their renowned contribution and suitability for the transdermal application. Carbopol is the primary choice in cutaneous application and has received much attention among the research scientists because of its fine rheological properties and good buffering capacity (Merclin et al., 2004). Alternatively, cellulose polymers (HPMC, methyl cellulose) are equally captivated in transdermal delivery formulations (Fang et al., 1999). Hence, in the present work, these polymers were selected and gels were prepared at proximate viscosity (∼ 9000 cp) in order to eliminate the viscosity effect on drug delivery [carbopol (1.5% w/v), HPMC (2% w/v), and methyl cel-lulose (5% w/v)]. The results of this study indicated that the drug delivery from different gel bases were compa-rable regardless of the polymers (4.59–5.89 µg/cm2/h, ANOVA, p = 0.3299, and 37.99–41.57 µg/cm2/h, ANOVA, p = 0.4658) in passive and iontophoresis processes, respectively). Moreover, the permeation profile displayed a similar trend. This set of experiments concluded that the permeation of metoprolol was not influenced by the polymers studied, under similar conditions, and hence further studies were carried out using carbopol gel as a representative polymer.
Chemical agents such as N-decyl methyl sulfoxide, azone, L-menthol, and (±)-linalool were previously screened for their potential to enhance the metopro-lol skin delivery (Aqil et al., 2006). Hence, we used a different group of proven chemical agents such as SLS, DMF, NMP, and PEG 400 to assess the effect of these enhancers on the metoprolol transport, by passive proc-ess. The enhancer concentration was fixed at 5%w/w, which is reported to be safe in vivo (Femenia-Font et al., 2005). All the enhancers were incorporated in the formulations and the pre-treatment effect was not studied, as the activities of all these chemicals were previously demonstrated and moreover the current experimental condition (in vitro) is inappropriate. Reasonable enhancement in drug flux (∼ 3–5-fold, ANOVA, p < 0.0001) was observed in the presence of permeation enhancers. However, these enhancers do not increase metoprolol flux to the same extent (SLS > DMF > NMP > PEG 400). The substantial amount of metoprolol permeation by SLS (25.87 ± 2.97 µg/cm2/h) could be attributed to its well known mechanism; i.e. fluidization of the lipid bilayer of SC and increase in skin hydration level (Shokri et al., 2001; Borras-Bolasco et al., 2004). Further, it is possible that the negatively charged SLS may increase the negative charge in the skin and increase the skin penetration of positively charged metoprolol, in the current experimental condition.
Figure 1 also signified that iontophoresis (0.5 mA/cm2) alone achieved significant enhancement in metoprolol flux (∼ 7-fold, t-test, p < 0.0001) when compared to con-trol. This higher flux (37.99 ± 4.39 µg/cm2/h) could be due to the optimum delivery condition provided which favors the iontophoretic delivery. Briefly, the drug properties like hydrophilicity, charge (positive), and ionization (> 99%; pKa 9.5 and pH 7.0), membrane charge (negative), and permeation processes such as electrorepulsion (anodal) and electrosmotic flow (anode to cathode) favored the process.
As seen from Figure 1, a combination of iontophoresis and chemical enhancer yielded a moderate effect (∼ 7–9-fold compared to passive, ANOVA, p < 0.0001) and the highest permeation was recorded when SLS was used (51.17 ± 4.59 µg/cm2/h), among the enhancers stud-ied. Such low enhancement in flux was unanticipated and contradicts the conventional thought of the addi-tive effect (permeation enhancer and iontophoresis in this case). As said before, passive delivery using these enhancers demonstrated the capability of the selected enhancers in improving the metoprolol flux (Figure 1). Hence the plausible explanation for low enhancement during the combination approach (iontophoresis and chemical enhancer) could be most likely due to the drug’s behavior with enhancers under the influence of an electric field or changes in the electrical and structural properties of the skin, due to the incorporation of these
60
50
40
30
20
10
0
Met
opro
lol f
lux
(µg/
cm2 /
h)
Pas
sive
gel
5% S
LS
5% D
MF
5% N
MP
5% P
EG
400 ITP
ITP
+SLS
ITP
+DM
F
ITP
+NM
P
ITP
+PE
G 4
00
Treatments
Figure 1. Steady state flux of metoprolol in passive delivery with dif-ferent permeation enhancers, iontophoresis (ITP; 0.5 mA/cm2), and their combined approach from carbopol gel containing 20 mM drug. Permeation was carried out for 6 h, the concentration of enhancers was 5% w/w and the area available for diffusion was 0.74 cm2. Poly ethylene glycol (PEG 400), Sodium lauryl sulfate (SLS), Di methyl formamide (DMF), and N-methyl-2-pyrrolidone (NMP). Each data represented the mean ± SD of six experiments.
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.
Effect of permeation enhancers on the transdermal iontophoresis of metoprolol 23
enhancers (Chesnoy et al., 1999; Choi et al., 1999; Wang et al., 2005). On the other hand, it is tempting to specu-late that this phenomenon could also result in retaining some amount of drug-enhancer in the skin tissues. In this direction, in another set of experiments, metoprolol was loaded into the skin using gel formulations by ion-tophoresis (0.5 mA/cm2) in conjunction with chemical enhancers, and the drug released into the receiver was assessed.
The existing permeation techniques in the transder-mal drug delivery are mainly employed to overcome the skin barrier with respect to drug permeation rather than the drug retention in the skin. This is because the drug retention within the skin may hamper the efficient absorption by the skin and permeation across the skin, as the drug reservoir in tissues is likely to increase the skin barrier resistance. The drug reservoir in the skin is most commonly observed when the drug is delivered from vesicular systems or the drug-complex with polymers or the ion pairs (Green et al., 1989; Doliwa et al., 2001; Choi & Maibach, 2005; Cosco et al., 2008). Few reports also exist with the drug depot formation during transdermal iontophoresis (Banga & Chien, 1993; Sachdeva et al., 2010). The main parameters that may likely cause drug retention in skin are the partition coefficient of drug, solubility of drug in the membrane, concentration of drug, pH-pKa conditions of the experiment, and the presence of a polymer/enhancer. However, the pKa and
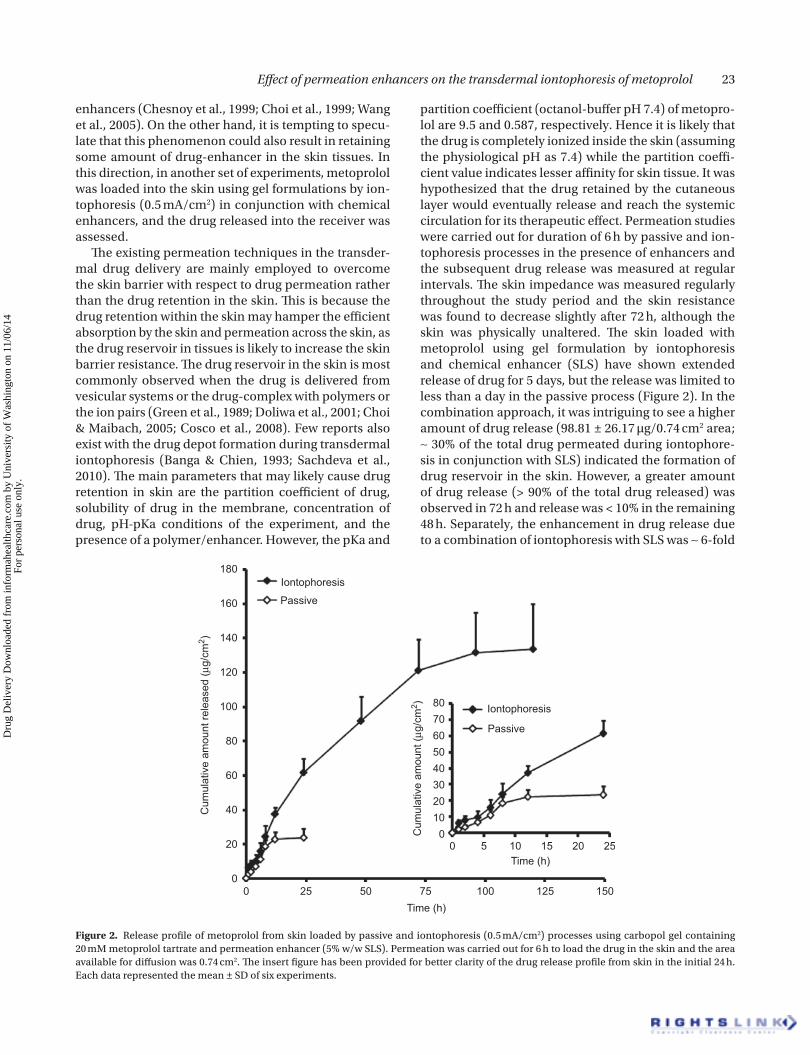
partition coefficient (octanol-buffer pH 7.4) of metopro-lol are 9.5 and 0.587, respectively. Hence it is likely that the drug is completely ionized inside the skin (assuming the physiological pH as 7.4) while the partition coeffi-cient value indicates lesser affinity for skin tissue. It was hypothesized that the drug retained by the cutaneous layer would eventually release and reach the systemic circulation for its therapeutic effect. Permeation studies were carried out for duration of 6 h by passive and ion-tophoresis processes in the presence of enhancers and the subsequent drug release was measured at regular intervals. The skin impedance was measured regularly throughout the study period and the skin resistance was found to decrease slightly after 72 h, although the skin was physically unaltered. The skin loaded with metoprolol using gel formulation by iontophoresis and chemical enhancer (SLS) have shown extended release of drug for 5 days, but the release was limited to less than a day in the passive process (Figure 2). In the combination approach, it was intriguing to see a higher amount of drug release (98.81 ± 26.17 µg/0.74 cm2 area; ∼ 30% of the total drug permeated during iontophore-sis in conjunction with SLS) indicated the formation of drug reservoir in the skin. However, a greater amount of drug release (> 90% of the total drug released) was observed in 72 h and release was < 10% in the remaining 48 h. Separately, the enhancement in drug release due to a combination of iontophoresis with SLS was ∼ 6-fold
Cum
ulat
ive
amou
nt re
leas
ed (µ
g/cm
2 )
Cum
ulat
ive
amou
nt (µ
g/cm
2 )
180
160
140
120
100
80
80706050403020100
60
40
20
0
Iontophoresis
Iontophoresis
Passive
Passive
0
0 5 10 15 20 25
25 50 75 100 125 150Time (h)
Time (h)
Figure 2. Release profile of metoprolol from skin loaded by passive and iontophoresis (0.5 mA/cm2) processes using carbopol gel containing 20 mM metoprolol tartrate and permeation enhancer (5% w/w SLS). Permeation was carried out for 6 h to load the drug in the skin and the area available for diffusion was 0.74 cm2. The insert figure has been provided for better clarity of the drug release profile from skin in the initial 24 h. Each data represented the mean ± SD of six experiments.
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

24 A. Nair et al.
higher (t-test, p < 0.0001) than its corresponding passive process. The release of drug from the skin followed a near first order profile [passive (R2 = 0.899) and iontophoresis (R2 = 0.951)], when analyzed kinetically. However, the other enhancers (in passive and iontophoresis) could not yield any significant effect and the release was limited to < 24 h (data not shown).
The drug release data observed in the current study suggests that iontophoresis in conjunction with SLS could lead to greater drug retention in the skin, eventu-ally releasing over a period of time. Hence, in another set of experiments, we measured the amount of drug loaded in the skin with different treatments, which were depicted in Figure 3. It was evident from Figure 3 that higher magnitude of drug was retained in the skin layer (149.57 ± 35.79 µg/cm2) when a chemical enhancer, SLS, was combined with iontophoresis. In contrast, the other enhancers (DMF, NMP, and PEG 400) when combined with iontophoresis had little or no effect on drug load in the skin layers (26–52 µg/cm2). In the passive process, it was also observed that the drug retention in skin was moderately high with SLS (30.62 ± 6.92 µg/cm2), when compared to other enhancers. Further it is also appar-ent from the figure that the treatment with iontophoresis (alone) could not significantly improve the drug load (28.14 ± 8.58 µg/cm2) in the skin tissues. On the other hand, the moderate amount of drug retention in the skin with various treatments (except with SLS combined with
iontophoresis) could be likely due to the entrapped drug in the skin in the final phase of the permeation study, which eventually diffused out due to a concentration gra-dient into the receiver during the release study. Moreover, the drug release studies indicated that the drug depot in the skin released > 90% of total drug loaded in the skin (irrespective of the treatments), indicating reversible binding of the drug with the skin tissue. Further studies need to be carried out to determine the drug distribu-tion in the skin layers (epidermis and dermis). Regarding the clearance of drug from the skin in vivo, it is strictly limited to the drug retention in the particular layers of skin (due to the difference in vasculature), i.e. one can expect a sustained effect provided the drug depot has occurred in the stratum corneum or epidermis, while rapid clearance could be observed from the viable der-mis due to its highly vasculature nature. Although it is too early to predict the exact mechanism, the influence of electric field on the surfactant (SLS) which might have a propensity to form micelles of amphiphatic nature or the ion-pair complex formation with SLS or the enhanced drug skin affinity or retention are not ruled out. However, an elaborate mechanistic study has to be carried out to get a deep insight into the mechanism, which is beyond the scope of this project.
The formation of drug depot in skin could be utilized in several applications for systemic and local skin therapy. In the case of anti-hypertensive drugs, an optimized delivery of drug depot could reduce the frequency of the applica-tion or the interval between the subsequent applications. Alternatively, topical delivery of several antibiotics for prolonged therapeutic effect could be achieved. Thus, the results observed in the current investigation have their own significance from the drug delivery outlook.
Conclusion
Metoprolol tartrate gel formulations were prepared using carbopol (1.5% w/v), HPMC (2% w/v), and methyl cellulose (5% w/v). Preliminary studies indicated that the permeation of metoprolol was not influenced by the polymers selected and, hence, further studies were carried out using carbopol gel as representative. Passive permeation studies using chemical enhancers (SLS, DMF, NMP, and PEG 400 at 5%w/w) increased the transdermal flux to a greater extent (∼ 3–5-fold). However, application of iontophoresis alone enhanced the permeation considerably (∼ 7-fold) when compared to the passive process. Drug delivery using iontophore-sis in conjunction with chemical agents yielded a moderate effect (∼ 7–9-fold compared to passive). Permeation studies with iontophoresis in conjunction with SLS created a drug depot in the skin which released over a period of time (5 days). An optimization of this
120
140
160
180
200
100
80
60
40
20
0
Am
ount
of d
rug
in s
kin
(µg/
cm2 )
Pas
sive
gel
5% S
LS
5% D
MF
5% N
MP
5% P
EG
400 ITP
ITP
+SLS
ITP
+DM
F
ITP
+NM
P
ITP
+PE
G 4
00
Treatments
Figure 3. Amount of metoprolol loaded in the skin in passive delivery with different permeation enhancers, iontophoresis (ITP; 0.5 mA/cm2), and their combined approach from carbopol gel con-tain 20 mM drug. Permeation was carried out for 6 h, the concentra-tion of enhancers was 5% w/w, and the area available for diffusion was 0.74 cm2. Poly ethylene glycol (PEG 400), Sodium lauryl sulfate (SLS), Di methyl formamide (DMF), and N-methyl-2-pyrrolidone (NMP). Each data represented the mean ± SD of six experiments.
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Effect of permeation enhancers on the transdermal iontophoresis of metoprolol 25
phenomenon could be carried out by screening various chemical agents in general and surfactants in particular under the influence of electric current and polymers. The results in this study suggest that the duration of treatment in topical/transdermal drug delivery could be prolonged for existing and new transdermal drugs, which could be challenging but interesting in the days to come.
Declaration of interest
The Author(s) declare(s) that we have no conflicts of interest to disclose.
References
Aqil, M., Sultana, Y., Ali, A. (2006). Transdermal delivery of beta-blockers. Expert Opin Drug Deliv. 3:405–18.
Anroop, B., Ghosh, B., Parcha, V., Khanam, J. (2008). Comparative skin permeability of metoprolol tartrate and its ester prodrugs by passive permeation and iontophoresis. Asian J Pharm Sci. 3:1–11.
Banga, A.K., Chien, Y.W. (1993). Characterization of in vitro transder-mal iontophoretic delivery of insulin. Drug Dev Ind Pharm. 19:2069–87.
Borras-Bolasco, J., Diez-Sales, O., Lopez, A., Herraez-Dominguez, M. (2004). A mathematical approach to predicting the percutane-ous absorption enhancing effect of sodium lauryl sulphate. Int J Pharm. 269:121–9.
Chesnoy, S., Durand, D., Doucet, J., Couarraze, G. (1999). Structural parameters involved in the permeation of propranolol HCl by iontophoresis and enhancers. J Contr Rel. 58:163–75.
Choi, E.H., Lee, S.H., Ahn, S.K., Hwang, S.M. (1999). The pretreatment effect of chemical skin penetration enhancers in transdermal drug delivery using iontophoresis. Skin Pharmacol Appl Skin Physiol. 12:326–35.
Choi, M.J., Maibach, H.I. (2005). Liposomes and niosomes as topical drug delivery systems. Skin Pharmacol Physiol. 18:209–19.
Cosco, D., Celia, C., Cilurzo, F., Trapasso, E., Paolino, D. (2008). Colloidal carriers for the enhanced delivery through the skin. Expert Opin Drug Deliv. 5:737–55.
de Figueiredo Alves, S.T., Gomes, M.A.S., Clapauch, R. (2000). Comparison of gel and patch estradiol replacement in Brazil, a tropical country. Maturitas. 36:69–74.
Doliwa, A., Santoyo, S., Ygartua, P. (2001). Transdermal iontophore-sis and skin retention of piroxicam from gels containing piroxi-cam: hydroxypropyl-beta-cyclodextrin complexes. Drug Dev Ind Pharm. 27:751–8.
Fang, J., Huang, Y., Wu, P., Tsai, Y. (1996). Transdermal iontophoresis of sodium nonivamide acetate II: optimization and evaluation on solutions and gels. Int J Pharm. 145:175–86.
Fang, J., Kuo, C., Huang, Y., Wu, P., Tsai, Y. (1999). Transdermal deliv-ery of sodium nonivamide acetate from volatile vehicles: effects of polymers. Int J Pharm. 176:157–67.
Femenia-Font, A., Balaguer-Fernandez, C., Merino, V., Rodilla, V., Lopez-Castellano, A. (2005). Effect of chemical enhancers on the in vitro percutaneous absorption of sumatriptan succinate. Eur J Pharm Biopharm. 61:50–5.
Ghosh, B., Jain, A., Ashok, P., Patel, B., Tarafdar, K. (2009). Passive and iontophoretic permeation of glipizide gel: an in vitro and in vivo study. Curr Drug Deliv. 6:444–50.
Ghosh, T.K., Adimola, J.A., Pfister, W.R., Yum, S.I. (1997). Transdermal delivery of beta adrenergic therapeutics. In: Ghosh, T.K., Pfister, W.R., Yum, S.I., eds. Transdermal and topical drug delivery sys-tems. Illinois: Interpharm Press Inc, 299–320.
Green, P.G., Hadgraft, J., Ridout, G. (1989). Enhanced in vitro skin per-meation of cationic drugs. Pharm Res. 6:628–32.
Hadgraft, J. (1999). Passive enhancement strategies in topical and transdermal drug delivery. Int J Pharm. 184:1–6.
Jamakandi, V.G., Ghosh, B., Desai, B.G., Khanam, J. (2006). Recent trends in transdermal cardiovascular therapy. Indian J Pharm Sci. 68:556–61.
Kaliszan, R., Nasal, A., Turowski, M. (1995). Binding site for basic drugs on α
1- acid glycoprotein as revealed by chemometric analysis of
biochromatographic data. Biomed Chrom. 9:211–5.Merclin, N., Bramer, T., Desmán, K. (2004). Iontophoretic delivery of
5-aminolevulinic acid and its methyl ester using a carbopol gel as vehicle. J Contr Rel. 98:57–65.
Mitragotri, S. (2000). Synergistic effect of enhancers for transdermal drug delivery. Pharm Res. 17:1354–9.
Mutalik, S., Parekh, H.S., Davies, N.M., Udupa, N. (2009). A com-bined approach of chemical enhancers and sonophoresis for the transdermal delivery of tizanidine hydrochloride. Drug Deliv. 16:82–91.
Nair, V., Panchagnula, R. (2003). Poloxamer gel as vehicle for transder-mal iontophoretic delivery of arginine vasopressin: evaluation of in vivo performance in rats. Pharmacol Res. 47:555–62.
Pillai, O., Panchagnula, R. (2003). Transdermal delivery of insulin from poloxamer gel: ex vivo and in vivo skin permeation studies in rat using iontophoresis and chemical enhancers. J Contr Rel. 89:127–40.
Prakash, A., Markham, A. (2000). Metoprolol: a review of its use in chronic heart failure. Drugs. 60:647–78.
Sachdeva, V., Siddoju, S., Yu, Y.Y., Kim, H.D., Friden, P.M., Banga, A.K. (2010). Transdermal iontophoretic delivery of terbinafine hydro-chloride: quantitation of drug levels in stratum corneum and underlying skin. Int J Pharm. 388:24–31.
Shokri, J., Nokhodchi, A., Dashbolaghi, A., Zadeh, D.H., Jalali, M.B. (2001). The effect of surfactants on the skin penetration of diazepam. Int J Pharm. 228:99–107.
Wang, Y., Thakur, R., Fan, Q., Michnaik, B. (2005). Transdermal ionto-phoresis: combination strategies to improve transdermal ionto-phoretic drug delivery. Eur J Pharm Biopharm. 60:179–91.
Dru
g D
eliv
ery
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.





























