Embed Size (px)
Citation preview
Journal of the American College of Cardiology Vol. 58, No. 11, 2011© 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00
Cardiovascular Pharmacology
Effects of Beta-Adrenergic Antagonistsin Patients With Chronic Kidney DiseaseA Systematic Review and Meta-Analysis
Sunil V. Badve, MBBS, MD, DNB,*† Matthew A. Roberts, MBBS, PHD,‡§Carmel M. Hawley, MBBS, MMEDSCI,*† Alan Cass, BA, MBBS, GRAD DIP CLIN EPI, PHD,*#Amit X. Garg, MD, MA, PHD,** Henry Krum, MBBS, PHD,� Andrew Tonkin, MBBS, MD,¶Vlado Perkovic, MBBS, PHD*#
Brisbane, Melbourne, and Sydney, Australia; and London, Ontario, Canada
Objectives The aim of this systematic review was to study the benefits and risks of beta-adrenergic antagonists (beta-blockers) in patients with chronic kidney disease (CKD).
Background There is an excess burden of cardiovascular disease and death in people with CKD. Despite their potential bene-fits, the effects of beta-blockers in this population are uncertain.
Methods CENTRAL (Cochrane Central Register of Controlled Trials), Medline (Medical Literature Analysis and RetrievalSystem Online), and Embase (Excerpta Medical Database) were searched for randomized controlled trials with atleast 3 months of follow-up in patients with CKD stages 3 to 5 that reported mortality outcomes. Summary esti-mates of effect were obtained using a random effects model.
Results Eight trials met criteria for review: 6 placebo-controlled trials involving 5,972 participants with chronic sys-tolic heart failure and 2 angiotensin-converting enzyme inhibitor–comparator trials involving 977 partici-pants not known to have heart failure. In CKD patients with heart failure, compared with placebo, beta-blocker treatment reduced the risk of all-cause (risk ratio [RR]: 0.72, 95% confidence interval [CI]: 0.64 to0.80) and cardiovascular mortality (RR: 0.66, 95% CI: 0.49 to 0.89), but increased the risk of bradycardia(RR: 4.92, 95% CI: 3.20 to 7.55) and hypotension (RR: 5.08, 95% CI: 3.48 to 7.41). Quantitative meta-analysis was not performed for the non–heart failure studies due to substantial clinical diversity or lack ofinformative data.
Conclusions Treatment with beta-blockers improved all-cause mortality in patients with CKD and chronic systolic heart fail-ure. There is insufficient evidence to conclude whether people with CKD who are not known to have heart failurederive benefit from beta-blockers. (J Am Coll Cardiol 2011;58:1152–61) © 2011 by the American Collegeof Cardiology Foundation
Published by Elsevier Inc. doi:10.1016/j.jacc.2011.04.041
From the *Australasian Kidney Trials Network, School of Medicine, The Universityof Queensland, Brisbane, Queensland, Australia; †Department of Nephrology,Princess Alexandra Hospital, Brisbane, Queensland, Australia; ‡Department ofNephrology, Austin Health, Melbourne, Victoria, Australia; §Department of Med-icine, University of Melbourne, Melbourne, Victoria, Australia; �Clinical Pharmacol-ogy Unit, Department of Epidemiology and Preventive Medicine, Monash Univer-sity, Melbourne, Victoria, Australia; ¶Cardiovascular Research Unit, Department ofEpidemiology and Preventive Medicine, Monash University, Melbourne, Victoria,Australia; #Renal Division, The George Institute for Global Health, Sydney, NewSouth Wales, Australia; and the **Division of Nephrology, University of WesternOntario, London, Ontario, Canada. Dr. Badve has reported that he has norelationships relevant to the contents of this paper to disclose. Dr. Roberts issupported by a National Health and Medical Research Council Training Fellowship.Dr. Hawley has received speakers’ honoraria from Shire Australia, Genzyme Austra-
lia, Roche Products Pty Ltd, Amgen Pty Ltd, and Fresenius Medical Care, as well asresearch grants from Roche Products Pty Ltd, Abbott Laboratories, Amgen Pty Ltd,Janssen Cilag Pty Ltd., Bayer HealthCare, Gambro Pty Ltd, Baxter Healthcare Pty Ltd,Shire Australia, and Fresenius Medical Care. Dr. Cass is supported by a National Healthand Medical Research Council Senior Research Fellowship and has received speakers’honoraria from Roche Products Pty Ltd and Servier Laboratories Pty Ltd, as well as aresearch grant from Roche Products Pty Ltd. Dr. Garg has received a research grant fromRoche Products Pty Ltd. Dr. Krum has served as a consultant for Roche Products PtyLtd, GlaxoSmithKline Pharmaceuticals, Merck KGaA, and CSL Limited. Dr. Tonkinhas served as consultant for AstraZeneca Pty Ltd and CSL Limited and has receivedspeakers’ honoraria from AstraZeneca Pty Ltd. Dr. Perkovic has served as a consultant forAbbott Laboratories; has received speakers’ honoraria from Roche Products Pty Ltd,Servier Laboratories Pty Ltd, AstraZeneca Pty Ltd, and Abbott Laboratories; and hasreceived research grants from Johnson and Johnson Pharmaceutical Research & Devel-opment, L.L.C., Roche Products Pty Ltd, Novartis Pharmaceuticals Corporation, andBaxter Healthcare Pty Ltd.
Manuscript received February 3, 2011; revised manuscript received April 19, 2011,accepted April 21, 2011.
ahi
rptpT
st2tCwogoutO
fdmuCwc5iOmrswSw
1153JACC Vol. 58, No. 11, 2011 Badve et al.September 6, 2011:1152–61 Beta-Blockers in Chronic Kidney Disease
Chronic kidney disease (CKD), defined as an estimatedglomerular filtration rate (eGFR) reduced to �60 ml/min/1.73 m2 or excess proteinuria (�250 mg/day or urinelbumin-creatinine ratio �30 mg/g), is a major publicealth problem affecting 8% to 12% of adults in industrial-
zed countries (1,2). Compared with the general population,
See page 1162
people with CKD, including those receiving dialysis, are atgreater risk of death (3–5). A cardiac cause accounts for 35%to 40% of all deaths in patients with end-stage renal diseaseon dialysis (6–8). In CKD patients who are not yet ondialysis (nondialysis CKD patients), the risk of having acardiovascular event is inversely proportional to eGFR(3,4,9–12). Results of a collaborative meta-analysis of gen-eral population cohorts consisting of more than 1.2 millionpeople showed that eGFR �60 ml/min/1.73 m2 was anindependent predictor of all-cause and cardiovascular mor-tality (13). Furthermore, there was an exponential increasein the risk of death at lower eGFR levels.
Beta-adrenergic receptor antagonists (“beta-blockers”)reduce mortality in patients following myocardial infarc-tion and in patients with chronic systolic heart failure(14,15). Evidence-based treatment guidelines recom-mend their use in such patients unless contraindicated ornot tolerated (16,17). However, randomized controlledtrials (RCTs) providing this evidence have generallyexcluded individuals with CKD, including end-stagerenal disease patients requiring dialysis (18,19). Ischemicheart disease, congestive heart failure, arrhythmias, leftventricular hypertrophy, and increased sympathetic ner-vous system activity are highly prevalent in people withadvanced CKD, and this population could theoreticallyderive large benefits from beta-blockers (7,8,20 –25).Observational studies in patients with CKD have dem-onstrated better survival and cardiovascular outcomes inthose treated with beta-blockers (26 –28). Despite this,the use of beta-blockers in patients receiving dialysisvaries considerably, ranging from as few as 10% ofpatients in Japan to approximately 60% in the UnitedStates (29,30). In a study of nondialysis CKD patientswho had a myocardial infarction, the frequency of beta-blocker use diminished as eGFR declined (3). In theUnited States, 61% and 73% of all dialysis patients withcongestive heart failure and acute myocardial infarction,respectively, were prescribed beta-blockers (30). Thevariable rates of utilization of beta-blockers in dialysispatients may be due to uncertainty regarding potentialbenefits in this population, as well as the possibility ofhemodynamic side effects in patients subjected to widefluctuations in extracellular fluid volume. Several inves-tigators have called for an increased use of beta-blockers
in dialysis patients while awaiting RCTs (31–34). iTherefore, the aim of this sys-tematic review was to determinethe effects of beta-blockers onclinical endpoints in patientswith CKD stages 3 to 5 includ-ing those on dialysis.
Methods
A systematic review was under-taken in accordance with thePRISMA (Preferred ReportingItems for Systematic Reviewsand Meta-Analyses) Statement(35).Search strategy, study selection,and data extraction. Studies were eligible for inclusion ifthey: 1) were randomized controlled trials; 2) includedparticipants with CKD stages 3 to 5 (eGFR �60 ml/min/1.73 m2), including those on dialysis therapy, who wereandomized to an oral beta-blocking agent compared withlacebo, a cardiovascular agent of another class, or noreatment; 3) followed patients for at least 3 monthsost-randomization; and 4) reported mortality outcomes.rials performed in kidney transplant patients were excluded.Relevant studies were identified through electronic
earches of Medline (Medical Literature Analysis and Re-rieval System Online) via Ovid (from inception to October010), Embase (Excerpta Medical Database) (from incep-ion to October 2010), and the CENTRAL (Cochraneentral Register of Controlled Trials) (Issue 4, 2010)ithout any language restriction. In addition, reference listsf relevant review articles, systematic reviews, treatmentuidelines, textbook chapters, conference proceedings, andnline trial registries were searched. Missing, incomplete, ornpublished data from clinical trials were requested fromhe respective investigators/authors by e-mail. (See thenline Appendix for complete search strategy.)The following data were extracted using a standardized
orm: patient demographic details, study design and con-uct, rates of outcome events, and adverse events. Theethodological quality of each included study was assessed
sing the risk of bias assessment tool developed by theochrane Bias Methods Group (36). The following 6 itemsere assessed: 1) random sequence generation; 2) allocation
oncealment; 3) blinding; 4) incomplete outcome data;) selective outcome reporting; and 6) any other bias (e.g.,nsufficient rationale, study design).
utcomes assessed. The primary outcome assessed in thiseta-analysis was all-cause mortality. In addition, all other
eported clinical outcomes such as cardiovascular mortality,udden death, all-cause hospitalization, hospitalization fororsening of heart failure, and adverse events were assessed.tatistical analysis. For dichotomous outcomes, the resultsere expressed as risk ratios (RRs) with 95% confidence
Abbreviationsand Acronyms
CI � confidence interval(s)
CKD � chronic kidneydisease
eGFR � estimatedglomerular filtration rate
GFR � glomerular filtrationrate
LVEF � left ventricularejection fraction
RCT � randomizedcontrolled trial
RR � risk ratio
ntervals (CIs). Summary estimates
were obtained by ran-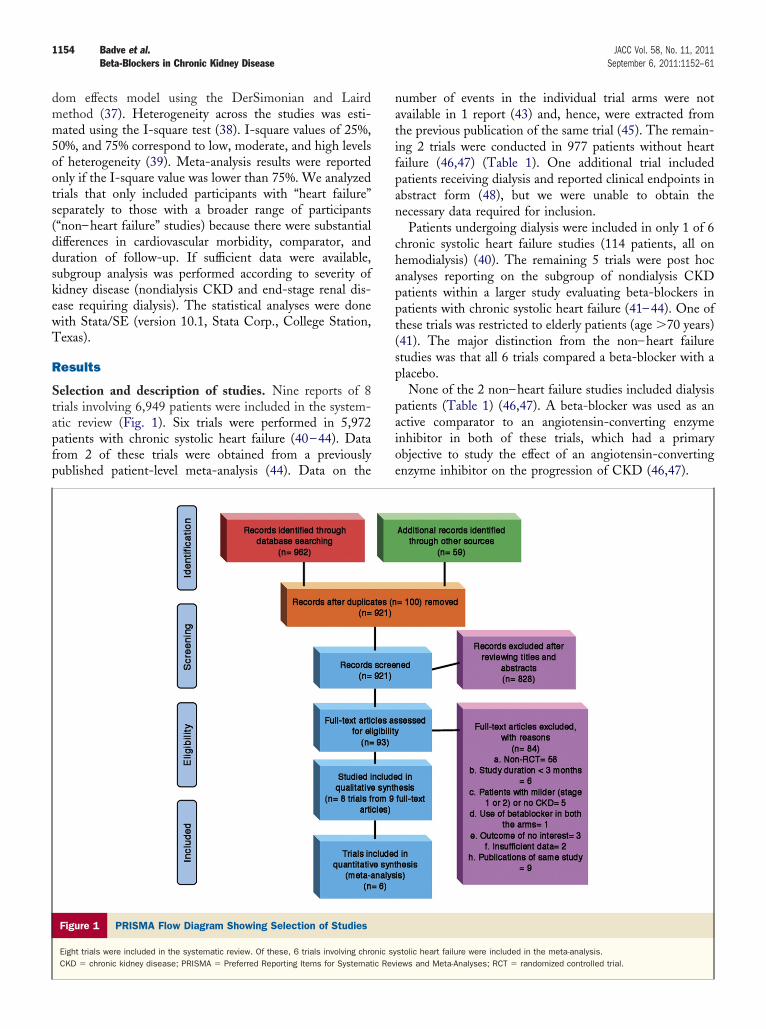
1154 Badve et al. JACC Vol. 58, No. 11, 2011Beta-Blockers in Chronic Kidney Disease September 6, 2011:1152–61
dom effects model using the DerSimonian and Lairdmethod (37). Heterogeneity across the studies was esti-mated using the I-square test (38). I-square values of 25%,50%, and 75% correspond to low, moderate, and high levelsof heterogeneity (39). Meta-analysis results were reportedonly if the I-square value was lower than 75%. We analyzedtrials that only included participants with “heart failure”separately to those with a broader range of participants(“non–heart failure” studies) because there were substantialdifferences in cardiovascular morbidity, comparator, andduration of follow-up. If sufficient data were available,subgroup analysis was performed according to severity ofkidney disease (nondialysis CKD and end-stage renal dis-ease requiring dialysis). The statistical analyses were donewith Stata/SE (version 10.1, Stata Corp., College Station,Texas).
Results
Selection and description of studies. Nine reports of 8trials involving 6,949 patients were included in the system-atic review (Fig. 1). Six trials were performed in 5,972patients with chronic systolic heart failure (40–44). Datafrom 2 of these trials were obtained from a previouslypublished patient-level meta-analysis (44). Data on the
Figure 1 PRISMA Flow Diagram Showing Selection of Studies
Eight trials were included in the systematic review. Of these, 6 trials involving chroCKD � chronic kidney disease; PRISMA � Preferred Reporting Items for Systemat
number of events in the individual trial arms were notavailable in 1 report (43) and, hence, were extracted fromthe previous publication of the same trial (45). The remain-ing 2 trials were conducted in 977 patients without heartfailure (46,47) (Table 1). One additional trial includedpatients receiving dialysis and reported clinical endpoints inabstract form (48), but we were unable to obtain thenecessary data required for inclusion.
Patients undergoing dialysis were included in only 1 of 6chronic systolic heart failure studies (114 patients, all onhemodialysis) (40). The remaining 5 trials were post hocanalyses reporting on the subgroup of nondialysis CKDpatients within a larger study evaluating beta-blockers inpatients with chronic systolic heart failure (41–44). One ofthese trials was restricted to elderly patients (age �70 years)(41). The major distinction from the non–heart failurestudies was that all 6 trials compared a beta-blocker with aplacebo.
None of the 2 non–heart failure studies included dialysispatients (Table 1) (46,47). A beta-blocker was used as anactive comparator to an angiotensin-converting enzymeinhibitor in both of these trials, which had a primaryobjective to study the effect of an angiotensin-convertingenzyme inhibitor on the progression of CKD (46,47).
stolic heart failure were included in the meta-analysis.iews and Meta-Analyses; RCT � randomized controlled trial.
nic syic Rev
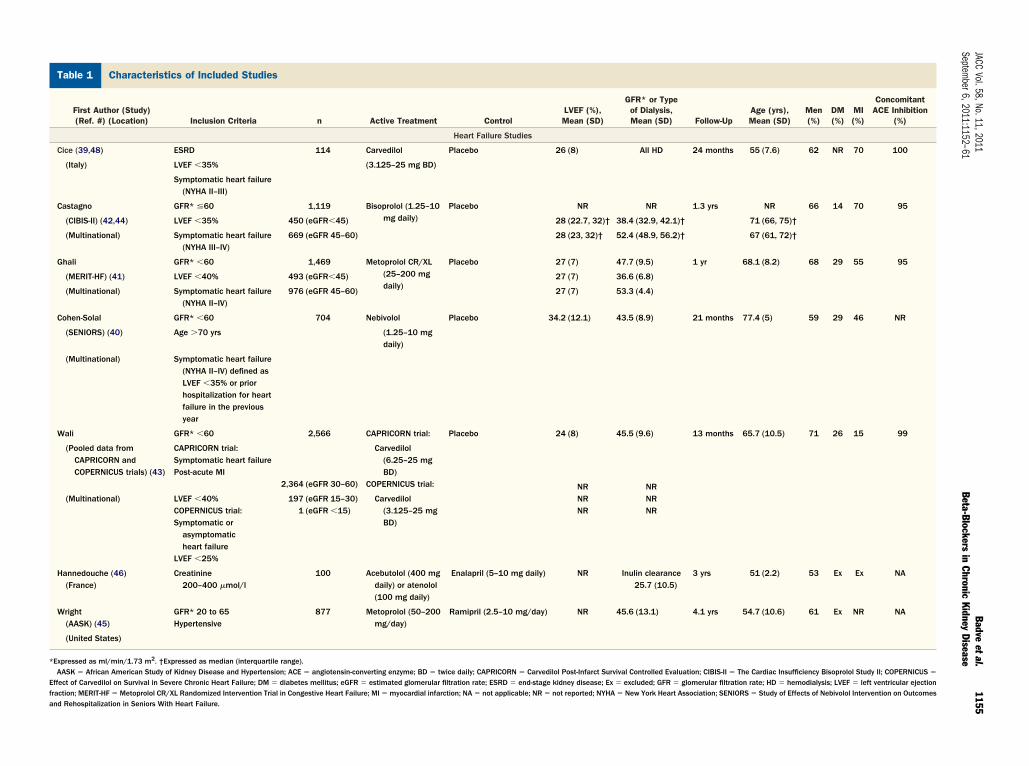
Characteristics of Included StudiesTable 1 Characteristics of Included Studies
First Author (Study)(Ref. #) (Location) Inclusion Criteria n Active Treatment Control
LVEF (%),Mean (SD)
GFR* or Typeof Dialysis,Mean (SD) Follow-Up
Age (yrs),Mean (SD)
Men(%)
DM(%)
MI(%)
ConcomitantACE Inhibition
(%)
Heart Failure Studies
Cice (39,48) ESRD 114 Carvedilol Placebo 26 (8) All HD 24 months 55 (7.6) 62 NR 70 100
(Italy) LVEF �35% (3.125–25 mg BD)
Symptomatic heart failure(NYHA II–III)
Castagno GFR* �60 1,119 Bisoprolol (1.25–10mg daily)
Placebo NR NR 1.3 yrs NR 66 14 70 95
(CIBIS-II) (42,44) LVEF �35% 450 (eGFR�45) 28 (22.7, 32)† 38.4 (32.9, 42.1)† 71 (66, 75)†
(Multinational) Symptomatic heart failure(NYHA III–IV)
669 (eGFR 45–60) 28 (23, 32)† 52.4 (48.9, 56.2)† 67 (61, 72)†
Ghali GFR* �60 1,469 Metoprolol CR/XL(25–200 mgdaily)
Placebo 27 (7) 47.7 (9.5) 1 yr 68.1 (8.2) 68 29 55 95
(MERIT-HF) (41) LVEF �40% 493 (eGFR�45) 27 (7) 36.6 (6.8)
(Multinational) Symptomatic heart failure(NYHA II–IV)
976 (eGFR 45–60) 27 (7) 53.3 (4.4)
Cohen-Solal GFR* �60 704 Nebivolol Placebo 34.2 (12.1) 43.5 (8.9) 21 months 77.4 (5) 59 29 46 NR
(SENIORS) (40) Age �70 yrs (1.25–10 mgdaily)
(Multinational) Symptomatic heart failure(NYHA II–IV) defined asLVEF �35% or priorhospitalization for heartfailure in the previousyear
Wali GFR* �60 2,566 CAPRICORN trial: Placebo 24 (8) 45.5 (9.6) 13 months 65.7 (10.5) 71 26 15 99
(Pooled data fromCAPRICORN andCOPERNICUS trials) (43)
CAPRICORN trial:Symptomatic heart failurePost-acute MI
2,364 (eGFR 30–60)
Carvedilol(6.25–25 mgBD)
COPERNICUS trial:
(Multinational) LVEF �40%COPERNICUS trial:Symptomatic or
asymptomaticheart failure
LVEF �25%
197 (eGFR 15–30)1 (eGFR �15)
Carvedilol(3.125–25 mgBD)
NRNRNR
NRNRNR
Hannedouche (46)(France)
Creatinine200–400 �mol/l
100 Acebutolol (400 mgdaily) or atenolol(100 mg daily)
Enalapril (5–10 mg daily) NR Inulin clearance25.7 (10.5)
3 yrs 51 (2.2) 53 Ex Ex NA
Wright(AASK) (45)
GFR* 20 to 65Hypertensive
877 Metoprolol (50–200mg/day)
Ramipril (2.5–10 mg/day) NR 45.6 (13.1) 4.1 yrs 54.7 (10.6) 61 Ex NR NA
(United States)
*Expressed as ml/min/1.73 m2. †Expressed as median (interquartile range).AASK � African American Study of Kidney Disease and Hypertension; ACE � angiotensin-converting enzyme; BD � twice daily; CAPRICORN � Carvedilol Post-Infarct Survival Controlled Evaluation; CIBIS-II � The Cardiac Insufficiency Bisoprolol Study II; COPERNICUS �
Effect of Carvedilol on Survival in Severe Chronic Heart Failure; DM � diabetes mellitus; eGFR � estimated glomerular filtration rate; ESRD � end-stage kidney disease; Ex � excluded; GFR � glomerular filtration rate; HD � hemodialysis; LVEF � left ventricular ejectionfraction; MERIT-HF � Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure; MI � myocardial infarction; NA � not applicable; NR � not reported; NYHA � New York Heart Association; SENIORS � Study of Effects of Nebivolol Intervention on Outcomesand Rehospitalization in Seniors With Heart Failure.
1155JACC
Vol.58,No.11,2011Badve
etal.Septem
ber6,2011:1152–61Beta-Blockers
inChronic
KidneyDisease
iohiaalE
fbrtHwawpAaurt
1156 Badve et al. JACC Vol. 58, No. 11, 2011Beta-Blockers in Chronic Kidney Disease September 6, 2011:1152–61
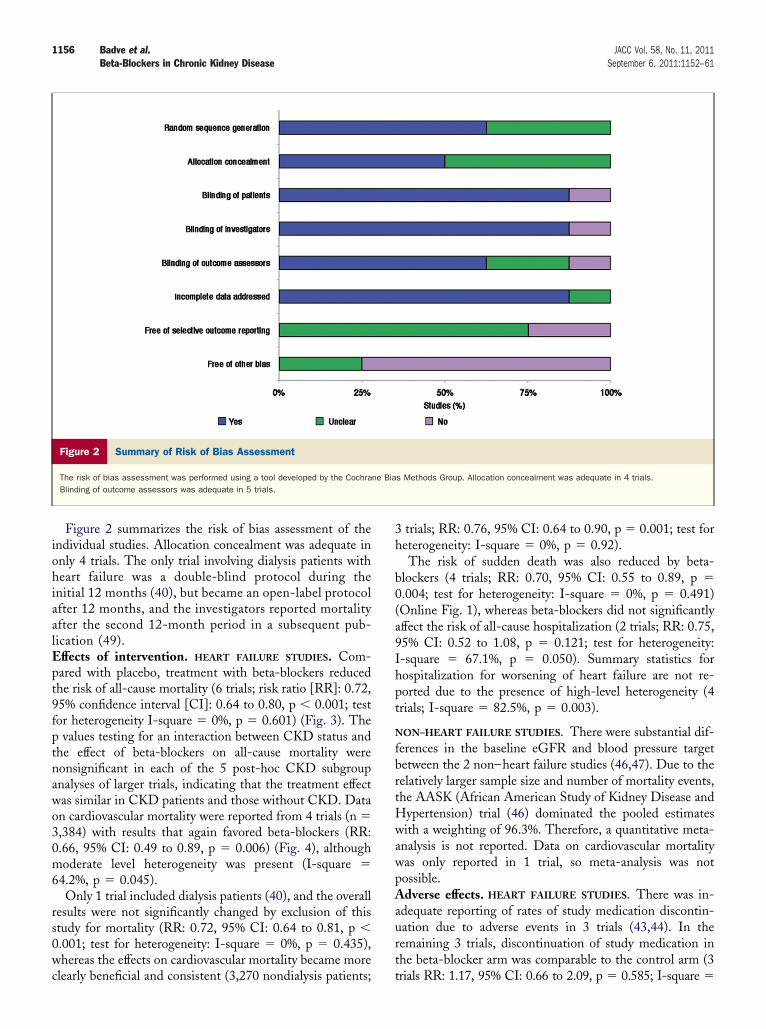
Figure 2 summarizes the risk of bias assessment of thendividual studies. Allocation concealment was adequate innly 4 trials. The only trial involving dialysis patients witheart failure was a double-blind protocol during the
nitial 12 months (40), but became an open-label protocolfter 12 months, and the investigators reported mortalityfter the second 12-month period in a subsequent pub-ication (49).
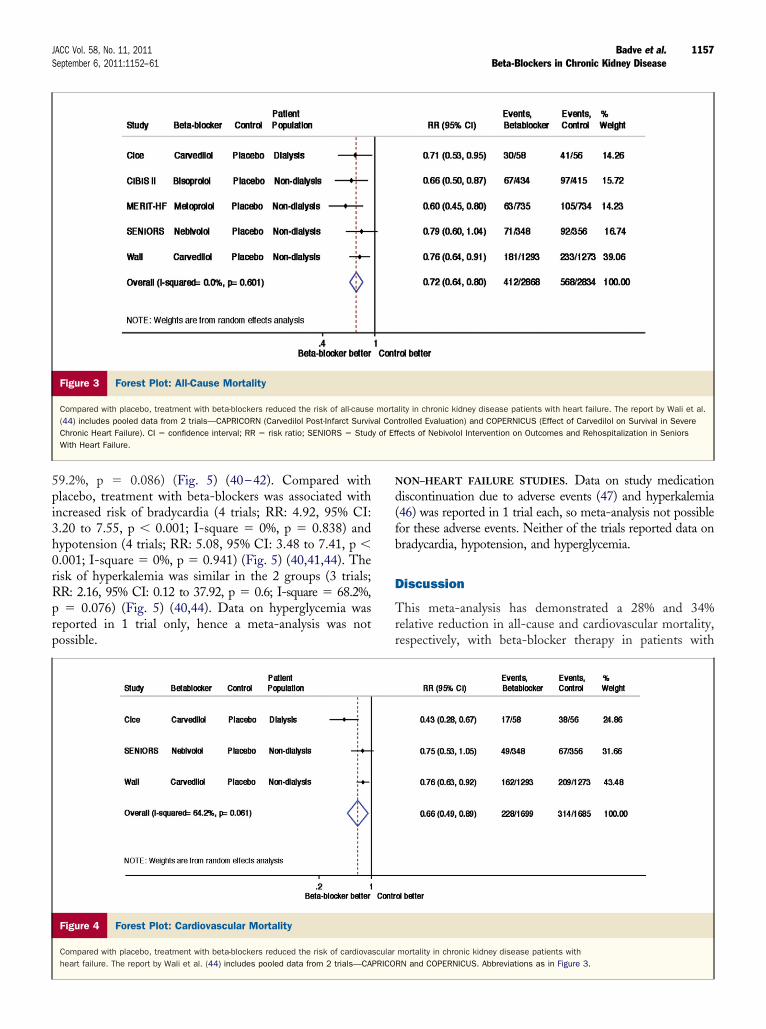
ffects of intervention. HEART FAILURE STUDIES. Com-pared with placebo, treatment with beta-blockers reducedthe risk of all-cause mortality (6 trials; risk ratio [RR]: 0.72,95% confidence interval [CI]: 0.64 to 0.80, p � 0.001; testfor heterogeneity I-square � 0%, p � 0.601) (Fig. 3). Thep values testing for an interaction between CKD status andthe effect of beta-blockers on all-cause mortality werenonsignificant in each of the 5 post-hoc CKD subgroupanalyses of larger trials, indicating that the treatment effectwas similar in CKD patients and those without CKD. Dataon cardiovascular mortality were reported from 4 trials (n �3,384) with results that again favored beta-blockers (RR:0.66, 95% CI: 0.49 to 0.89, p � 0.006) (Fig. 4), althoughmoderate level heterogeneity was present (I-square �64.2%, p � 0.045).
Only 1 trial included dialysis patients (40), and the overallresults were not significantly changed by exclusion of thisstudy for mortality (RR: 0.72, 95% CI: 0.64 to 0.81, p �0.001; test for heterogeneity: I-square � 0%, p � 0.435),whereas the effects on cardiovascular mortality became more
Figure 2 Summary of Risk of Bias Assessment
The risk of bias assessment was performed using a tool developed by the CochraBlinding of outcome assessors was adequate in 5 trials.
clearly beneficial and consistent (3,270 nondialysis patients; t
3 trials; RR: 0.76, 95% CI: 0.64 to 0.90, p � 0.001; test forheterogeneity: I-square � 0%, p � 0.92).
The risk of sudden death was also reduced by beta-blockers (4 trials; RR: 0.70, 95% CI: 0.55 to 0.89, p �0.004; test for heterogeneity: I-square � 0%, p � 0.491)(Online Fig. 1), whereas beta-blockers did not significantlyaffect the risk of all-cause hospitalization (2 trials; RR: 0.75,95% CI: 0.52 to 1.08, p � 0.121; test for heterogeneity:I-square � 67.1%, p � 0.050). Summary statistics forhospitalization for worsening of heart failure are not re-ported due to the presence of high-level heterogeneity (4trials; I-square � 82.5%, p � 0.003).
NON–HEART FAILURE STUDIES. There were substantial dif-erences in the baseline eGFR and blood pressure targetetween the 2 non–heart failure studies (46,47). Due to theelatively larger sample size and number of mortality events,he AASK (African American Study of Kidney Disease and
ypertension) trial (46) dominated the pooled estimatesith a weighting of 96.3%. Therefore, a quantitative meta-
nalysis is not reported. Data on cardiovascular mortalityas only reported in 1 trial, so meta-analysis was notossible.dverse effects. HEART FAILURE STUDIES. There was in-
dequate reporting of rates of study medication discontin-ation due to adverse events in 3 trials (43,44). In theemaining 3 trials, discontinuation of study medication inhe beta-blocker arm was comparable to the control arm (3
s Methods Group. Allocation concealment was adequate in 4 trials.
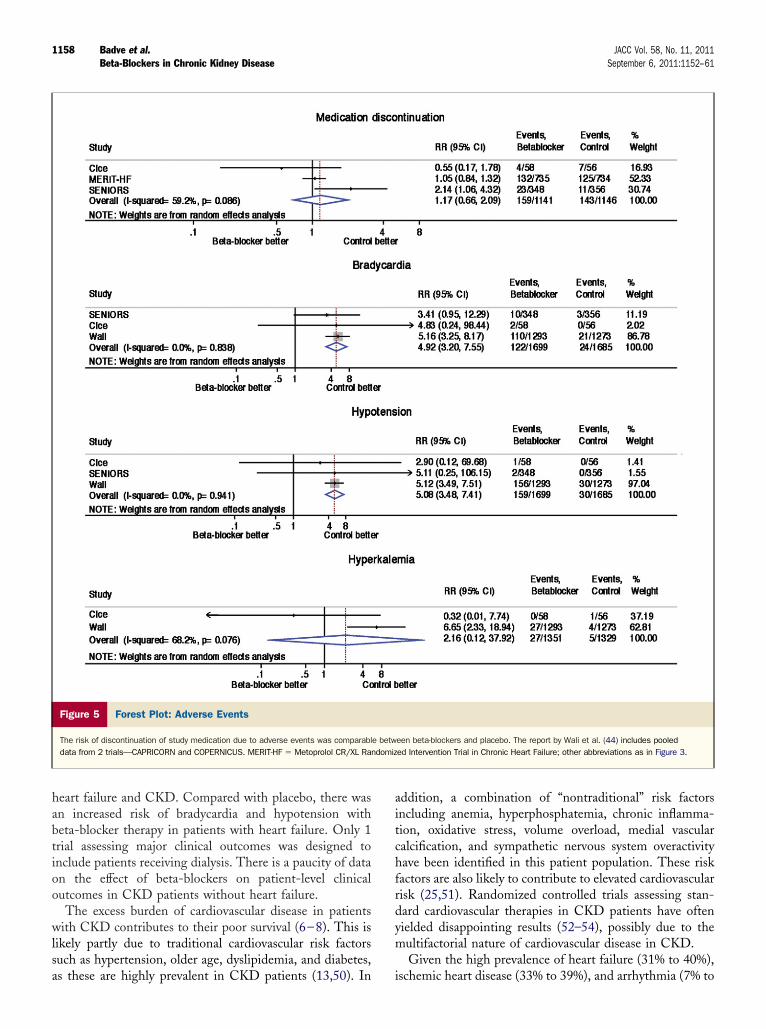
ne Biarials RR: 1.17, 95% CI: 0.66 to 2.09, p � 0.585; I-square �
1157JACC Vol. 58, No. 11, 2011 Badve et al.September 6, 2011:1152–61 Beta-Blockers in Chronic Kidney Disease
59.2%, p � 0.086) (Fig. 5) (40–42). Compared withplacebo, treatment with beta-blockers was associated withincreased risk of bradycardia (4 trials; RR: 4.92, 95% CI:3.20 to 7.55, p � 0.001; I-square � 0%, p � 0.838) andhypotension (4 trials; RR: 5.08, 95% CI: 3.48 to 7.41, p �0.001; I-square � 0%, p � 0.941) (Fig. 5) (40,41,44). Therisk of hyperkalemia was similar in the 2 groups (3 trials;RR: 2.16, 95% CI: 0.12 to 37.92, p � 0.6; I-square � 68.2%,p � 0.076) (Fig. 5) (40,44). Data on hyperglycemia wasreported in 1 trial only, hence a meta-analysis was notpossible.
Figure 3 Forest Plot: All-Cause Mortality
Compared with placebo, treatment with beta-blockers reduced the risk of all-cause(44) includes pooled data from 2 trials—CAPRICORN (Carvedilol Post-Infarct SurvivChronic Heart Failure). CI � confidence interval; RR � risk ratio; SENIORS � StudWith Heart Failure.
Figure 4 Forest Plot: Cardiovascular Mortality
Compared with placebo, treatment with beta-blockers reduced the risk of cardiovaheart failure. The report by Wali et al. (44) includes pooled data from 2 trials—CA
NON–HEART FAILURE STUDIES. Data on study medicationdiscontinuation due to adverse events (47) and hyperkalemia(46) was reported in 1 trial each, so meta-analysis not possiblefor these adverse events. Neither of the trials reported data onbradycardia, hypotension, and hyperglycemia.
Discussion
This meta-analysis has demonstrated a 28% and 34%relative reduction in all-cause and cardiovascular mortality,respectively, with beta-blocker therapy in patients with
lity in chronic kidney disease patients with heart failure. The report by Wali et al.trolled Evaluation) and COPERNICUS (Effect of Carvedilol on Survival in Severefects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors
mortality in chronic kidney disease patients withRN and COPERNICUS. Abbreviations as in Figure 3.
mortaal Cony of Ef
scularPRICO
1158 Badve et al. JACC Vol. 58, No. 11, 2011Beta-Blockers in Chronic Kidney Disease September 6, 2011:1152–61
heart failure and CKD. Compared with placebo, there wasan increased risk of bradycardia and hypotension withbeta-blocker therapy in patients with heart failure. Only 1trial assessing major clinical outcomes was designed toinclude patients receiving dialysis. There is a paucity of dataon the effect of beta-blockers on patient-level clinicaloutcomes in CKD patients without heart failure.
The excess burden of cardiovascular disease in patientswith CKD contributes to their poor survival (6–8). This islikely partly due to traditional cardiovascular risk factorssuch as hypertension, older age, dyslipidemia, and diabetes,
Figure 5 Forest Plot: Adverse Events
The risk of discontinuation of study medication due to adverse events was comparabldata from 2 trials—CAPRICORN and COPERNICUS. MERIT-HF � Metoprolol CR/XL Ra
as these are highly prevalent in CKD patients (13,50). In
addition, a combination of “nontraditional” risk factorsincluding anemia, hyperphosphatemia, chronic inflamma-tion, oxidative stress, volume overload, medial vascularcalcification, and sympathetic nervous system overactivityhave been identified in this patient population. These riskfactors are also likely to contribute to elevated cardiovascularrisk (25,51). Randomized controlled trials assessing stan-dard cardiovascular therapies in CKD patients have oftenyielded disappointing results (52–54), possibly due to themultifactorial nature of cardiovascular disease in CKD.
Given the high prevalence of heart failure (31% to 40%),
een beta-blockers and placebo. The report by Wali et al. (44) includes pooleded Intervention Trial in Chronic Heart Failure; other abbreviations as in Figure 3.
e betwndomiz
ischemic heart disease (33% to 39%), and arrhythmia (7% to

peam
emfmmubcdwtatsSvtdteCstBtt6Cats
lG
satsffptsfsvtff
C
Tbpsb
cwsrfeuetdpaCpa
1159JACC Vol. 58, No. 11, 2011 Badve et al.September 6, 2011:1152–61 Beta-Blockers in Chronic Kidney Disease
31%) in CKD patients (7,55), particular those requiringdialysis (8), it is possible that CKD patients may derivebenefit from beta-blocker therapy that is similar to orperhaps greater than that observed in other populations(14,15). In this systematic review, data regarding nondialy-sis CKD patients was obtained exclusively from post hocsubgroup analyses of RCTs in patients with heart failure.Although these studies were not specifically designed toassess effects in people with CKD, the absence of aninteraction suggests that the benefits for all-cause andcardiovascular mortality in nondialysis CKD patients aresimilar to those in people who do not have CKD. Given thatatients with CKD have a higher frequency of cardiovascularvents than patients with GFR �60 ml/min/1.73 m2 do, thebsolute risk reduction with beta-blocker therapy should beuch greater in this group.This systematic review also highlights the absence of specific
vidence that beta-blockers reduce all-cause or cardiovascularortality in the individuals with CKD who do not have heart
ailure, particularly those undergoing dialysis. Such individualsay still have ischemic heart disease or arrhythmias and thusay derive benefit from beta-blockers. However, in patients
ndergoing hemodialysis, the hypotensive side effects of beta-lockers may be exacerbated by marked fluctuations in extra-ellular fluid volume. Only 1 trial reported clinical outcomes inialysis patients (40,49), and this included only 114 patientsith symptomatic heart failure, contributing less than 15% of
he weight for the mortality outcome. The small sample sizend the lack of blinding during the second 12-month period ofhe study (when most events occurred) suggest that moretudies are required.tudy limitations. The limitations of this systematic re-iew include the relatively small number of eligible studies,he post hoc nature of analyses of the largest studies, theifficulties in defining “symptomatic” heart failure in pa-ients with CKD, and the lack of systematic data on adverseffects. In this systematic review, data regarding nondialysisKD patients was obtained exclusively from post hoc
ubgroup analyses of RCTs in patients with heart failurehat defined CKD as an eGFR �60 ml/min/1.73 m2.ecause patients with advanced CKD were excluded from
hese 5 heart failure studies, the majority of participants inhe CKD subgroups had relatively mild CKD. For example,0% and 66% of participants from the CKD cohort of theIBIS-II (Cardiac Insufficiency Bisoprolol Study II) (43)
nd MERIT-HF (Metoprolol CR/XL Randomized Interven-ion Trial in Congestive Heart Failure) (42) studies, re-pectively, had an eGFR between 45 and 60 ml/min/1.73 m2
at baseline. In the combined cohort of CAPRICORN(Carvedilol Post-Infarct Survival Controlled Evaluation)and COPERNICUS (Effect of Carvedilol on Survival inSevere Chronic Heart Failure) studies, only 8% of all CKDparticipants had eGFR �30 ml/min/1.73 m2 (44). There-fore, the application of these results to patients with very
low levels of GFR (particularly �30 ml/min/1.73 m2) isimited by the smaller number of participants with such lowFR in these studies.The definition of heart failure in terms of presence and
everity of symptoms was not uniform across the studies andlmost all studies defined patients as “symptomatic” based onhe New York Heart Association functional classification ofymptoms. Patients with CKD may report symptoms of heartailure, such as fatigue or dyspnea, even in the absence of heartailure. This was demonstrated in an analysis of 2,883 CKDatients without heart failure, in which 25% of the cohort hadhe modified Kansas City Cardiomyopathy Questionnairecore �75, a threshold suggestive of moderate burden of heartailure symptoms (56). However, as described in Table 1, alltudies were uniformly composed of participants with low leftentricular ejection fraction (LVEF). Hence, the findings ofhis systematic review apply to patients with CKD and heartailure with decreased LVEF, but not to patients with heartailure and preserved LVEF.
onclusions
his systematic review demonstrates that treatment with beta-lockers decreased all-cause and cardiovascular mortality inatients with CKD who have heart failure and low LVEF,uggesting these individuals will obtain similar or greaterenefits than people with heart failure who do not have CKD.
The widespread use of beta-blockers to reduce cardiovas-ular events and improve patient-level outcomes in patientsith CKD who do not have heart failure or those with
ymptomatic heart failure and a normal LVEF cannot beecommended based on existing RCT evidence. The needor adequately powered prospective RCTs assessing theffects of beta-blockers in a broader population of individ-als with advanced CKD are supported by the demonstratedffects in people with CKD and heart failure, as well as byhe known cardiovascular pathophysiology that has beenescribed in this patient population. Such trials shouldrovide a clear demonstration of the benefits and risksssociated with beta-blockers in patients with advancedKD, particularly those receiving dialysis, and informotential use of a treatment to reduce the burden of deathnd disability suffered by this patient population.
AcknowledgmentsThe authors are grateful to Dr. Jalal K. Ghali and Dr. JohnWikstrand for providing data.
Reprint requests and correspondence: Dr. Sunil V. Badve,Princess Alexandra Hospital, Level 2, ARTS Building, Wool-loongabba, Queensland 4102, Australia. E-mail: [email protected].
REFERENCES
1. Chadban SJ, Briganti EM, Kerr PG, et al. Prevalence of kidneydamage in Australian adults: The AusDiab kidney study. J Am Soc
Nephrol 2003;14:S131–8.
1160 Badve et al. JACC Vol. 58, No. 11, 2011Beta-Blockers in Chronic Kidney Disease September 6, 2011:1152–61
2. Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidneydisease in the United States. JAMA 2007;298:2038–47.
3. Anavekar NS, McMurray JJV, Velazquez EJ, et al. Relation betweenrenal dysfunction and cardiovascular outcomes after myocardial infarc-tion. N Engl J Med 2004;351:1285–95.
4. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C-Y. Chronickidney disease and the risks of death, cardiovascular events, andhospitalization. N Engl J Med 2004;351:1296–305.
5. Villar E, Remontet L, Labeeuw M, Ecochard R. Effect of age, gender,and diabetes on excess death in end-stage renal failure. J Am SocNephrol 2007;18:2125–34.
6. McDonald SP, Excell L, Livingston B. Chapter 3: Deaths. In:McDonald SP, Excell L, Livingston B, editors. ANZDATA RegistryReport 2009. Adelaide, South Australia: Australia and New ZealandDialysis and Transplant Registry, 2009:3.1–3.10.
7. Cheung AK, Sarnak MJ, Yan G, et al., for the HEMO Study Group.Cardiac diseases in maintenance hemodialysis patients: results of theHEMO Study. Kidney Int 2004;65:2380–9.
8. Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardio-vascular disease in chronic renal disease. Am J Kidney Dis 1998;32:S112–9.
9. Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S. Renal insufficiencyas a predictor of cardiovascular outcomes and the impact of ramipril:the HOPE randomized trial. Ann Intern Med 2001;134:629–36.
10. Perkovic V, Ninomiya T, Arima H, et al. Chronic kidney disease,cardiovascular events, and the effects of perindopril-based bloodpressure lowering: data from the PROGRESS Study. J Am SocNephrol 2007;18:2766–72.
11. Verma A, Anavekar NS, Meris A, et al. The relationship betweenrenal function and cardiac structure, function, and prognosis aftermyocardial infarction: the VALIANT Echo Study. J Am Coll Cardiol2007;50:1238–45.
12. Weiner DE, Tighiouart H, Amin MG, et al. Chronic kidney diseaseas a risk factor for cardiovascular disease and all-cause mortality: apooled analysis of community-based studies. J Am Soc Nephrol2004;15:1307–15.
13. Matsushita K, van der Velde M, Astor BC, et al., for the ChronicKidney Disease Prognosis Consortium. Association of estimatedglomerular filtration rate and albuminuria with all-cause and cardio-vascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010;375:2073–81.
14. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Betablockade after myocardial infarction: systematic review and metaregression analysis. BMJ 1999;318:1730–7.
15. Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heartfailure: a Bayesian meta-analysis. Ann Intern Med 2001;134:550–60.
16. Jessup M, Abraham WT, Casey DE, et al. 2009 focused update:ACCF/AHA guidelines for the diagnosis and management of heartfailure in adults: a report of the American College of CardiologyFoundation/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 2009;53:1343–82.
17. Antman EM, Hand M, Armstrong PW, et al. 2007 focused update ofthe ACC/AHA 2004 guidelines for the management of patients withST-elevation myocardial infarction: a report of the American Collegeof Cardiology/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 2008;51:210–47.
18. Charytan D, Kuntz RE. The exclusion of patients with chronic kidneydisease from clinical trials in coronary artery disease. Kidney Int2006;70:2021–30.
19. Coca SG, Krumholz HM, Garg AX, Parikh CR. Underrepresentationof renal disease in randomized controlled trials of cardiovasculardisease. JAMA 2006;296:1377–84.
20. Zoccali C, Benedetto FA, Mallamaci F, et al. Prognostic value ofechocardiographic indicators of left ventricular systolic function inasymptomatic dialysis patients. J Am Soc Nephrol 2004;15:1029–37.
21. Zoccali C, Benedetto FA, Tripepi G, et al. Left ventricular systolicfunction monitoring in asymptomatic dialysis patients: a prospectivecohort study. J Am Soc Nephrol 2006;17:1460–5.
22. Foley RN, Parfrey PS, Kent GM, Harnett JD, Murray DC, Barre PE.Serial change in echocardiographic parameters and cardiac failure inend-stage renal disease. J Am Soc Nephrol 2000;11:912–6.
23. Roberts MA, Hare DL, Ratnaike S, Ierino FL. Cardiovascularbiomarkers in CKD: pathophysiology and implications for clinical
management of cardiac disease. Am J Kidney Dis 2006;48:341–60.24. Koomans HA, Blankestijn PJ, Joles JA. Sympathetic hyperactivity inchronic renal failure: a wake-up call. J Am Soc Nephrol 2004;15:524–37.
25. Hausberg M, Kosch M, Harmelink P, et al. Sympathetic nerve activityin end-stage renal disease. Circulation 2002;106:1974–9.
26. Chonchol M, Benderly M, Goldbourt U. Beta-blockers for coronaryheart disease in chronic kidney disease. Nephrol Dial Transplant2008;23:2274–9.
27. Abbott KC, Trespalacios FC, Agodoa LY, Taylor AJ, Bakris GL.Beta-blocker use in long-term dialysis patients: association withhospitalized heart failure and mortality. Arch Intern Med 2004;164:2465–71.
28. McCullough PA, Sandberg KR, Borzak S, Hudson MP, Garg M,Manley HJ. Benefits of aspirin and beta-blockade after myocardialinfarction in patients with chronic kidney disease. Am Heart J2002;144:226–32.
29. Tentori F. Trends in medication use and clinical outcomes in twelvecountries: results from the Dialysis Outcomes and Practice PatternsStudy (DOPPS). Contrib Nephrol 2008;161:48–54.
30. U.S. Renal Data System. USRDS 2010 Annual Data Report: Atlas ofChronic Kidney Disease and End-Stage Renal Disease in the UnitedStates. Bethesda, MD: National Institutes of Health, National Insti-tute of Diabetes and Digestive and Kidney Diseases, 2010.
31. Kalaitzidis R, Bakris G. Should nephrologists use beta-blockers? Aperspective. Nephrol Dial Transplant 2009;24:701–2.
32. Furgeson SB, Chonchol M. Beta-blockade in chronic dialysis patients.Semin Dial 2008;21:43–8.
33. Bakris GL, Hart P, Ritz E. Beta blockers in the management ofchronic kidney disease. Kidney Int 2006;70:1905–13.
34. Zuanetti G, Maggioni A, Keane W, Ritz E. Nephrologists neglectadministration of betablockers to dialysed diabetic patients. NephrolDial Transplant 1997;12:2497–500.
35. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement forreporting systematic reviews and meta-analyses of studies that evaluatehealth care interventions: explanation and elaboration. Ann InternMed 2009;151:W65–94.
36. Higgins J, Altman DG. Assessing risk of bias in included studies. In:Higgins JP, Green S, editors. Cochrane Handbook for SystemicReviews of Interventions: Cochrane Book Series. Chichester, WestSussex: John Wiley & Sons Ltd., 2008.
37. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control ClinTrials 1986;7:177–88.
38. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuringinconsistency in meta-analyses. BMJ 2003;327:557–60.
39. Borenstein M, Hedges LV, Higgins J, Rothstein HR. Introduction toMeta-Analysis. 1st edition. Chichester, West Sussex: John Wiley &Sons, Ltd., 2009.
40. Cice G, Ferrara L, Di Benedetto A, et al. Dilated cardiomyopathy indialysis patients—beneficial effects of carvedilol: a double-blind,placebo-controlled trial. J Am Coll Cardiol 2001;37:407–11.
41. Cohen-Solal A, Kotecha D, van Veldhuisen DJ, et al., for theSENIORS Investigators. Efficacy and safety of nebivolol in elderlyheart failure patients with impaired renal function: insights from theSENIORS trial. Eur J Heart Fail 2009;11:872–80.
42. Ghali JK, Wikstrand J, Van Veldhuisen DJ, et al., for the MERIT-HFStudy Group. The influence of renal function on clinical outcome andresponse to beta-blockade in systolic heart failure: insights fromMetoprolol CR/XL Randomized Intervention Trial in Chronic HF(MERIT-HF). J Card Fail 2009;15:310–8.
43. Castagno D, Jhund PS, McMurray JJ, et al. Improved survival withbisoprolol in patients with heart failure and renal impairment: ananalysis of the Cardiac Insufficiency Bisoprolol Study II (CIBIS-II)trial. Eur J Heart Fail 2010;12:607–16.
44. Wali RK, Iyengar M, Beck GJ, et al. Efficacy and safety of carvedilolin treatment of heart failure with chronic kidney disease: a meta-analysis of randomized trials. Circ Heart Fail 2011;4:18–26.
45. Erdmann E, Lechat P, Verkenne P, Wiemann H. Results from post-hocanalyses of the CIBIS II trial: effect of bisoprolol in high-risk patientgroups with chronic heart failure. Eur J Heart Fail 2001;3:469–79.
46. Wright JT, Bakris G, Greene T, et al., for the AASK Research Group.Effect of blood pressure lowering and antihypertensive drug class onprogression of hypertensive kidney disease: results from the AASK
trial. JAMA 2002;288:2421–31.
5
5
5
5
c
1161JACC Vol. 58, No. 11, 2011 Badve et al.September 6, 2011:1152–61 Beta-Blockers in Chronic Kidney Disease
47. Hannedouche T, Landais P, Goldfarb B, et al. Randomised controlledtrial of enalapril and (beta) blockers in non-diabetic chronic renalfailure. BMJ 1994;309:833–7.
48. Nakao N, Hasegawa H, Fujimori A, Seno H, Toriyama T, KawaharaH. Effects of combined beta-blocker and anti-aldosterone antagonisttreatment for cardiovascular prevention in patients receiving mainte-nance haemodialysis (abstr). J Am Soc Nephrol 2007;18:709A.
49. Cice G, Ferrara L, D’Andrea A, et al. Carvedilol increases two-yearsurvival in dialysis patients with dilated cardiomyopathy: a prospective,placebo-controlled trial. J Am Coll Cardiol 2003;41:1438–44.
50. Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a riskfactor for development of cardiovascular disease: a statement from theAmerican Heart Association Councils on Kidney in CardiovascularDisease, High Blood Pressure Research, Clinical Cardiology, andEpidemiology and Prevention. Hypertension 2003;42:1050–65.
51. Muntner P, He J, Astor BC, Folsom AR, Coresh J. Traditional andnontraditional risk factors predict coronary heart disease in chronickidney disease: results from the atherosclerosis risk in communitiesstudy. J Am Soc Nephrol 2005;16:529–38.
52. Wanner C, Krane V, Marz W, et al., for the German Diabetes andDialysis Study Investigators. Atorvastatin in patients with type 2
diabetes mellitus undergoing hemodialysis. N Engl J Med2005;353:238–48.
3. Fellstrom BC, Jardine AG, Schmieder RE, et al., for the AURORAStudy Group. Rosuvastatin and cardiovascular events in patientsundergoing hemodialysis. N Engl J Med 2009;360:1395–407.
4. Zannad F, Kessler M, Lehert P, et al. Prevention of cardiovascular eventsin end-stage renal disease: results of a randomized trial of fosinopril andimplications for future studies. Kidney Int 2006;70:1318–24.
5. Foley RN, Parfrey PS, Harnett JD, et al. Clinical and echocardio-graphic disease in patients starting end-stage renal disease therapy.Kidney Int 1995;47:186–92.
6. Shlipak MG, Lash JP, Yang W, et al., for the CRIC Investigators.Symptoms characteristic of heart failure among CKD patients withoutdiagnosed heart failure. J Card Fail 2011;17:17–23.
Key Words: beta-adrenergic antagonists y cardiovascular disease yhronic kidney disease y heart failure y meta-analysis.
APPENDIX
For the complete search strategy,
please see the online version of this article.