Embed Size (px)
DESCRIPTION
支氣管封堵器用於小孩子的方法. Endobronchial Blockers in Babies and Children. 何名熙 Anthony M.-H. Ho Department of Anaesthesia and Intensive Care The Chinese University of Hong Kong Prince of Wales Hospital. 單肺 麻醉 通 气气管 One lung anesthesia. 双腔管支气管插管. 首选. Device of Choice. Double-lumen tube. - PowerPoint PPT Presentation
Citation preview

Endobronchial Blockersin Babies and Children
何名熙 Anthony M.-H. HoDepartment of Anaesthesia and Intensive Care
The Chinese University of Hong Kong
Prince of Wales Hospital
支氣管封堵器用於小孩子的方法





單肺麻醉通气气管 One lung anesthesia
双腔管支气管插管 首
选
Double-lumen tube
Device of Choice

http://funcage.com/blog/cute-baby-animals/funcage-cute-baby-animal-14/

不适合用于 <6-8岁的小孩子和婴儿
DLTs and Univent are not suitable for children <6-8 years of age

Situations in which 1-lung is required in children include:
• Lung abscess/empyema
• Bronchopulmonary fistula
• TEF/TOF
• Mediastinal and paraspinal tumours
• Lung tumours
• Congenital cystic adenomatoid malformation
• Congenital lobar emphysema

Source: Christian Seefelder, MD

http://www.google.com.hk/imglanding?q=congital+lobar+emphysema&um=1&hl=zh-TW&client=firefox-a&sa=X&rls=org.mozilla:en-US:official&source=lnt&tbs=isz:l&tbm=isch&tbnid=RpKWa7GLnt_-rM:&imgrefurl=http://www.radpod.org/2008/06/16/congenital-lobar-emphysema-2/&imgurl=http://www.radpod.org/wp-content/uploads/2008/06/congenital_lobar_emphysema_2.jpg&w=1204&h=1130&ei=oe20TYzvHZDCvgOlga2FBw&zoom=1&iact=hc&page=1&tbnh=136&tbnw=161&start=0&ndsp=15&ved=1t:429,r:0,s:0&biw=1005&bih=576
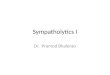
Congenital lobar emphysema


Source: Christian Seefelder, MD

http://www.google.com.hk/imglanding?q=congenital+cystic+adenomatoid+malformation+of+the+lung&um=1&hl=zh-TW&client=firefox-a&sa=X&rls=org.mozilla:en-US:official&source=lnt&tbs=isz:l&tbm=isch&tbnid=Qpszx03iaIdVOM:&imgrefurl=http://www.radpod.org/2008/02/28/congenital-cystic-adenomatoid-malformation/&imgurl=http://www.radpod.org/wp-content/uploads/2008/02/ccam.jpg&w=1570&h=1034&ei=Ge-0TbGqKYvyvwPNvsWOBw&zoom=1&iact=hc&page=1&tbnh=131&tbnw=176&start=0&ndsp=15&ved=1t:429,r:0,s:0&biw=1005&bih=576

Calvert JK, et al. Arch Dis Child Fetal Neonatal Ed 2006;91:F26-F28

Collapsing a lung in a small patient
• 1-lung anaesthesia– Deliberate endobronchial intubation– Endobronchial blocker with endotracheal tube– Endobronchial blocker with LMA
• Insufflation of pneumothorax by surgeon
• Open thoracotomy+retraction
• Some combination of the above

• Big scar 大的伤疤 (100%)• Severe postoperative pain 手术后极度疼痛 (100%)• Asymmetry of the thoracic wall 胸膛不对称 (20%)• “Winged” scapula (24%)• Scoliosis 脊椎骨畸形发展 (8%) • Fusion of the ribs 肋骨连接起来 (10%)• Breast maldevelopment 胸部畸形发展 (3.3%)• Shoulder deformity 肩畸形发展 (reported)
MSK sequelae of open thoracotomy in children 并发及后遗症
Jaureguizar E, et al. (1985) Morbid musculoskeletal sequelae of thoracotomy for tracheoesophageal fistula. J Pediatr Surg 20:511–514 6.
Freeman NV, Walkden J (1969) Previously unreported shoulder deformity follow-ing right lateral thoracotomy for esophageal atresia. J Pediatr Surg 4:627–636

ETT
ID
3.5-4
4.0-4.5
4.5-5.5
5.0-6.0
ETT
OD
4.9-5.6
5.6-6.2
6.2-7.5
6.6-8.2

From: Hammer G, Hall S, Davis PJ. Anesthesia for general abdominal, thoracic, urologic, and bariatric surgery. In: Smith’s Anesthesia for Infants and Children, 7th ed. Ed. Motoyama EK, Davis PJ, Mosby 2006, Philadelphia. 685-722
单内腔管不 适合用 于單肺麻醉
Use of a single-lumen ETT to effect 1-lung anesthesia

Microcuff


适合用于
<6-8岁的小孩子和婴儿

Endotracheal tube
Conventional technique for lung isolation in small children (<6-8 years of age).
<6-8岁的小孩子和婴儿的單肺麻醉方法

Retrograde dislodgement of endobronchial blocker causing loss of lung isolation and airway obstruction.
经常出现的一个问题
3 of 23 cases (13%)

Retrograde Dislodgement of Endobronchial Blocker
• Problem – not an uncommon problem with low pressure high volume Fogarty embolectomy catheters; even with the new 5 Fr Arndt endobronchial blocker with high volume low pressure balloon, retrograde migration of blocker occurred in 3 out of 23 cases (Wald SH, et al. Experience with the Arndt paediatric bronchial blocker. Br J Anaesth 2005; 94:92-4)

Loss of OLA
• Inconvenient
• Repositioning very difficult, especially in tiny patients (stooping down and crawling under the drapes and interfering with surgery)
• Highly exhausting
• Desperate surgeons trying to stem a major bleed leading to blocker dislodgement

Trachoesophageal Fistula

Airway Management -Anatomy
• Bronchoscopic findings (113 patients) Paediatr Anaesth 1992;2:297-303
– 11% at or below carina– 22% within 1 cm above– 67% above
• Ventilation difficulties, gastric distention (16%, N=61) Paediatr Anaesth 1998;8:313-319 – Large fistula (>3mm)

Fistula quite a bit above carina
• Pass the ETT distally enough to block the fistula
• May be even achieving endobronchial intubation using the same ETT

切去 /cut away Murphy eye


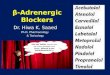
Step 1: Suctioning of oesophageal stumpStep 2: Induction of anaesthesia, lignocaine sprayStep 3: Fibrescopic bronchoscopy (left panel)Step 4: Pass blocker with tip bent toward posteriorStep 5: Intubate with tracheal tube (ET)Step 6: Fibrescopy via ET lumen (middle panel)Step 7: Remove ETStep 8: Pass 2nd blocker with tip bent toward rightStep 9: Intubate followed by bronchoscopy (right panel)











Ho AMH, Karmakar MK. Ann Roy Coll Surg Engl 2007; 89:532-3
(Mini Step, InnerDyne, Salt Lake City, Utah, USA)

(Mini Step, InnerDyne, Salt Lake City, Utah, USA)
Ho AMH, Karmakar MK. Ann Roy Coll Surg Engl 2007; 89:532-3