Embed Size (px)
Citation preview
Epstein-Barr Virus in Nasopharyngeal Carcinoma
內科部 血液腫瘤科05-20-2011
徐正龍
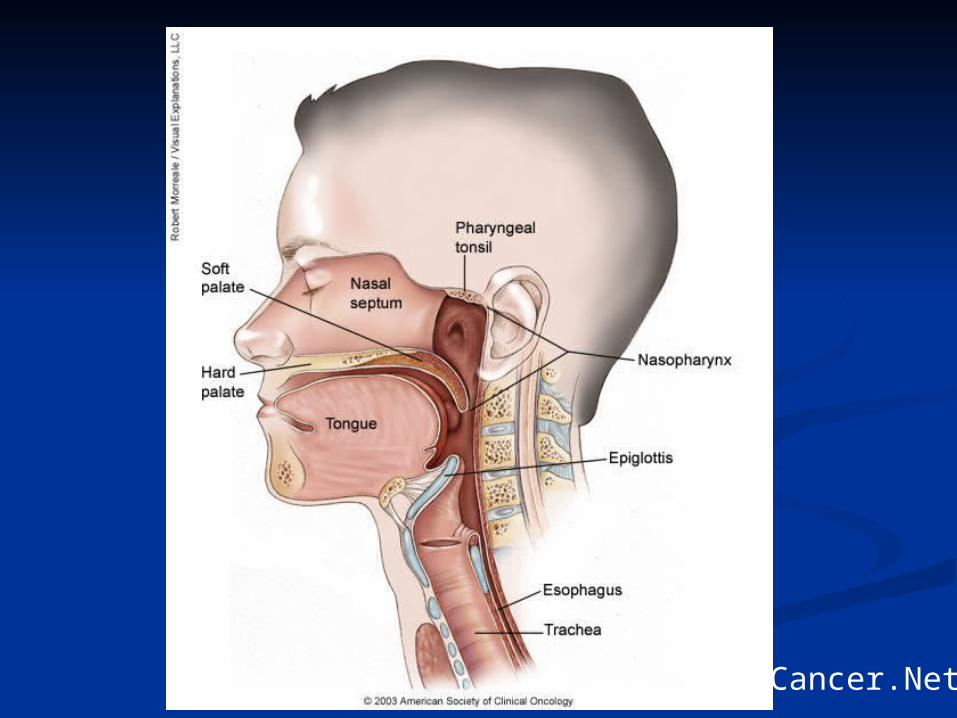
(Cancer.Net)
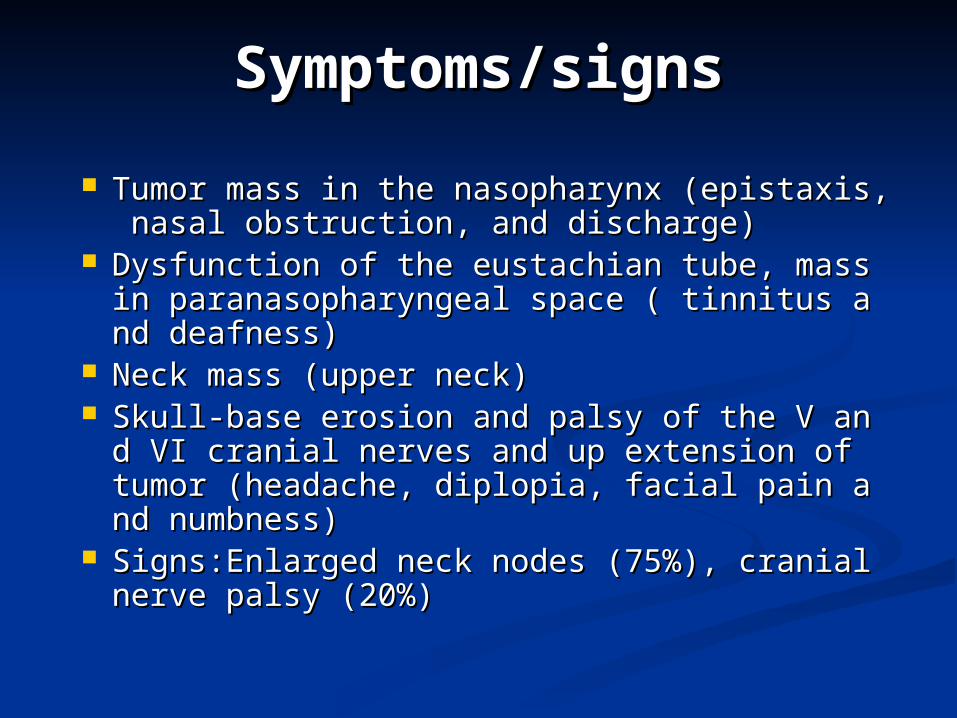
Symptoms/signsSymptoms/signs
Tumor mass in the nasopharynx (epistaxis, nTumor mass in the nasopharynx (epistaxis, nasal obstruction, and discharge)asal obstruction, and discharge)
Dysfunction of the eustachian tube, mass in Dysfunction of the eustachian tube, mass in paranasopharyngeal space ( tinnitus and deafparanasopharyngeal space ( tinnitus and deafness)ness)
Neck mass (upper neck) Neck mass (upper neck) Skull-base erosion and palsy of the V and VI cSkull-base erosion and palsy of the V and VI c
ranial nerves and up extension of tumor (hearanial nerves and up extension of tumor (headache, diplopia, facial pain and numbness)dache, diplopia, facial pain and numbness)
Signs:Enlarged neck nodes (75%), cranial nerSigns:Enlarged neck nodes (75%), cranial nerve palsy (20%)ve palsy (20%)
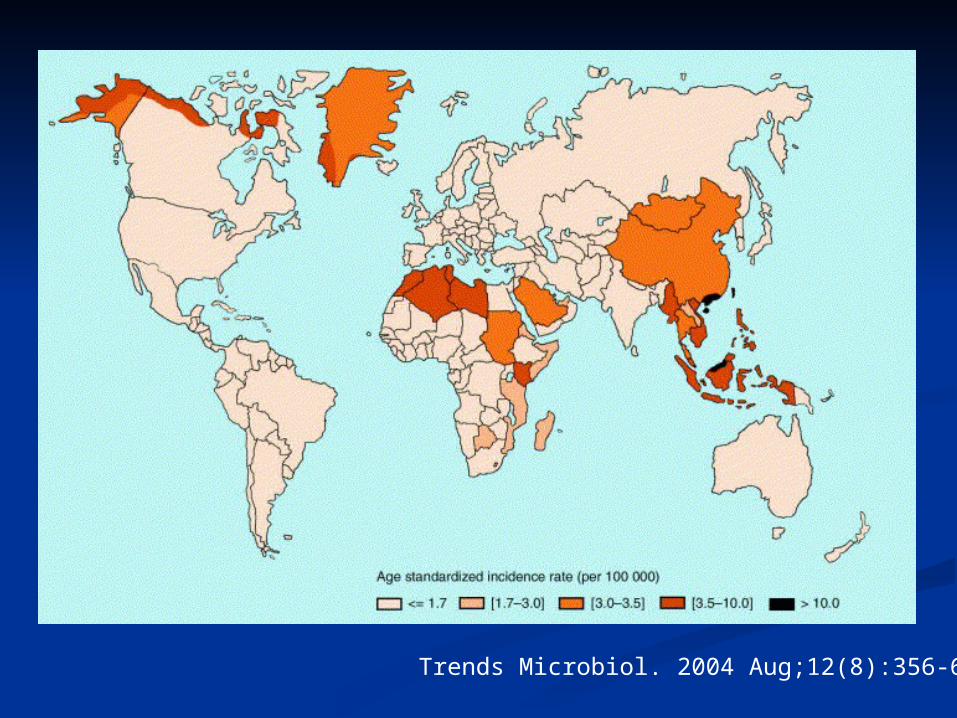
Trends Microbiol. 2004 Aug;12(8):356-60
EpidemiologyEpidemiology Male:Female = 2~3:1Male:Female = 2~3:1 Chinese native > Chinese immigrant > NortChinese native > Chinese immigrant > Nort
h American nativeh American native Both genetic and environmental factorsBoth genetic and environmental factors
EnvironmentalEnvironmental VirusesViruses
EBV- well documented viral “fingerprints” in tumor EBV- well documented viral “fingerprints” in tumor cells and also anti-EBV serologies with WHO type II cells and also anti-EBV serologies with WHO type II and III NPCand III NPC
HPV - possible factor in WHO type I lesionsHPV - possible factor in WHO type I lesions Nitrosamines - salted fishNitrosamines - salted fish Others - polycyclic hydrocarbons, chronic nasaOthers - polycyclic hydrocarbons, chronic nasa
l infection, poor hygiene, poor ventilationl infection, poor hygiene, poor ventilation
ClassificationClassification WHO classes (Based on light microscopy fWHO classes (Based on light microscopy f
indings)indings) Type I - moderate to well differentiated sqType I - moderate to well differentiated sq
uamous cell carcinomauamous cell carcinoma Type II - “non-keratinizing” carcinomaType II - “non-keratinizing” carcinoma Type III - “undifferentiated” carcinomaType III - “undifferentiated” carcinoma Differences between type I and Differences between type I and
types II & IIItypes II & III 5 year survival5 year survival
Type I - 10% Types II, III - 50%Type I - 10% Types II, III - 50% Long-term risk of recurrence for types II & IIILong-term risk of recurrence for types II & III Viral associationsViral associations
Type I - HPVType I - HPV Types II, III - EBVTypes II, III - EBV
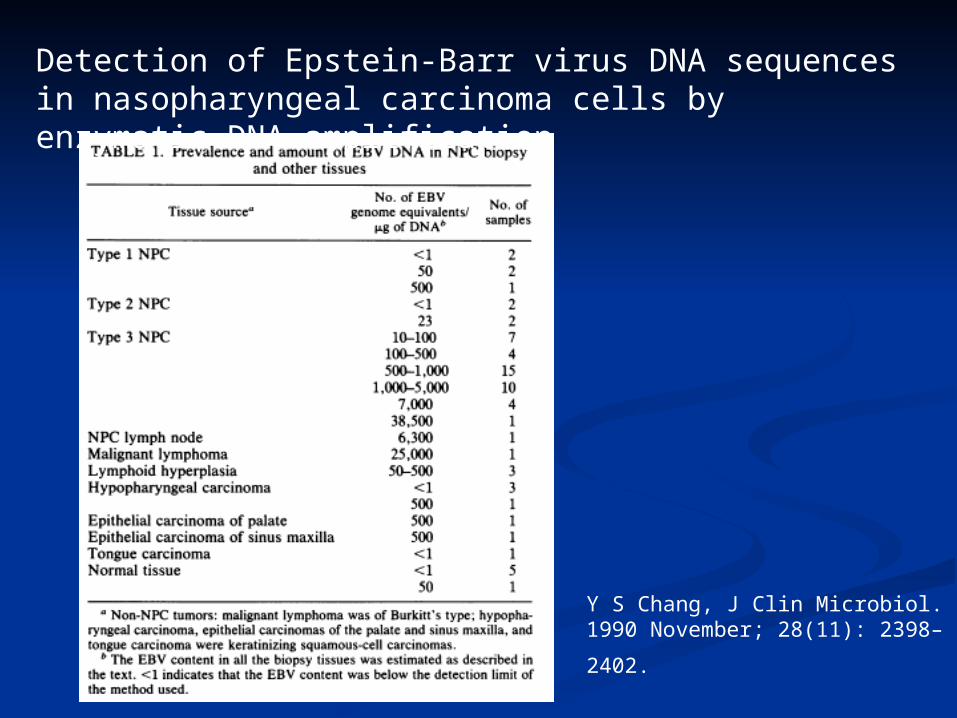
Y S Chang, J Clin Microbiol. 1990 Nove
mber; 28(11): 2398–2402.
Detection of Epstein-Barr virus DNA sequences in nasopharyngeal carcinoma cells by enzymatic DNA amplification
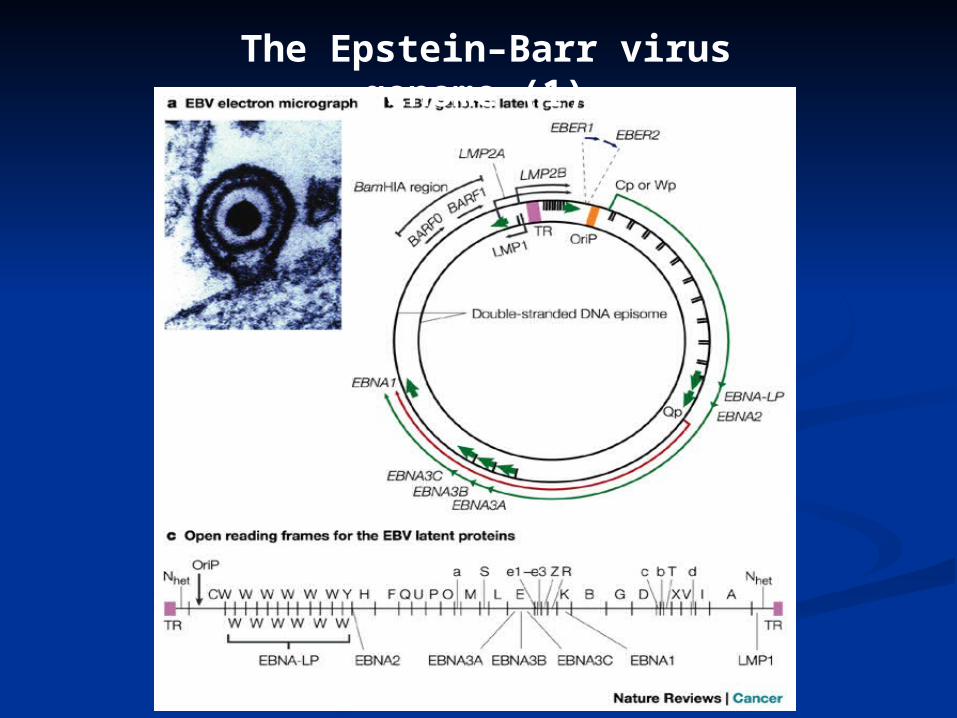
The Epstein–Barr virus genome (1)
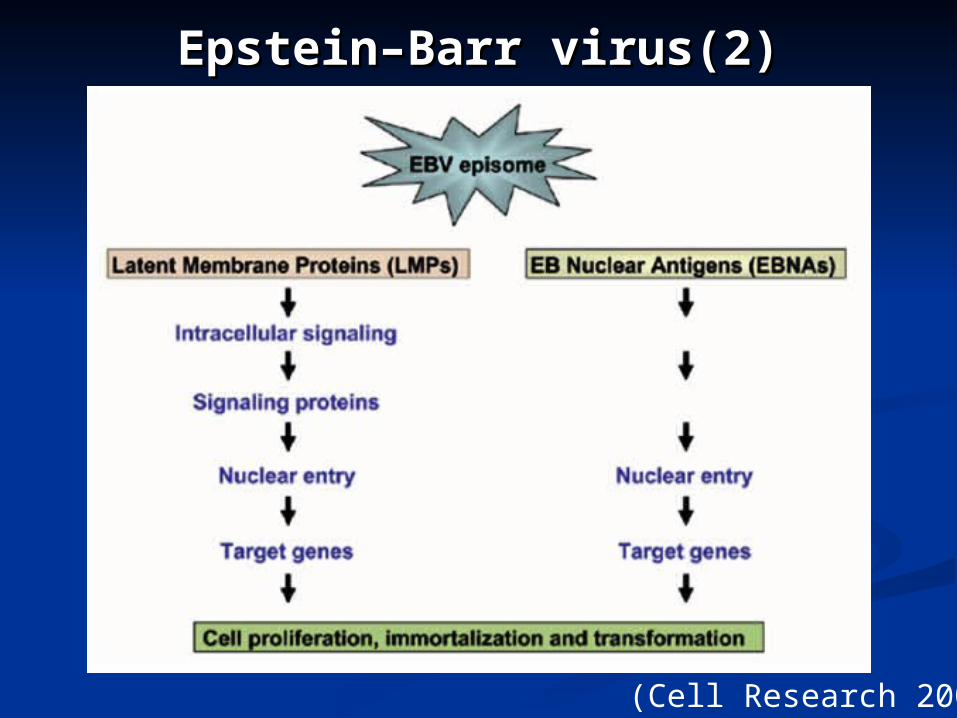
Epstein–Barr virus(2)Epstein–Barr virus(2)
(Cell Research 2006)
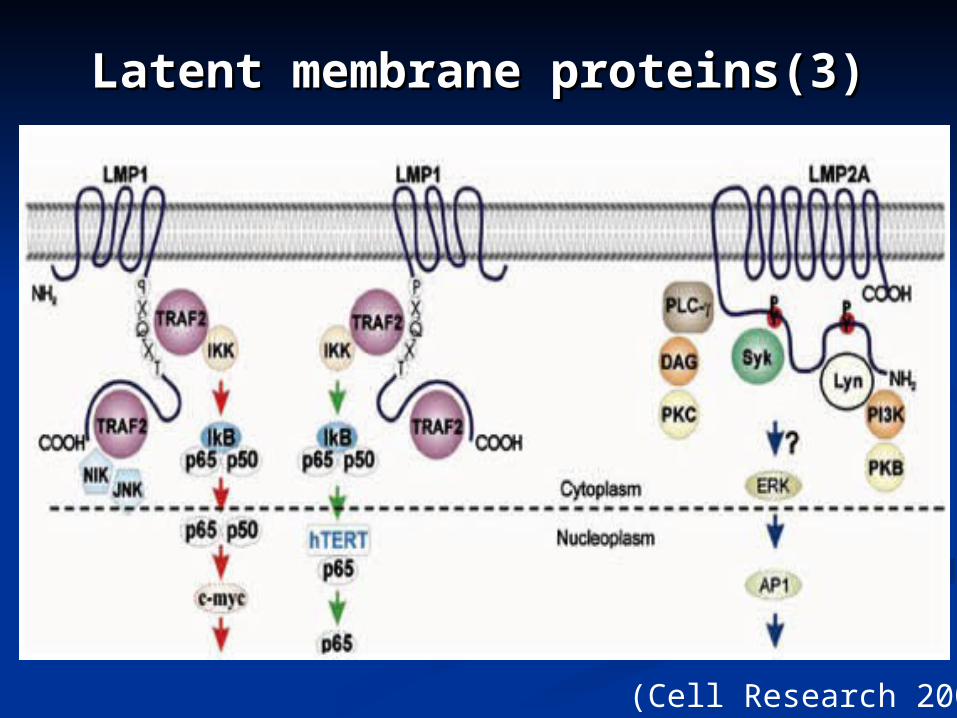
Latent membrane Latent membrane proteins(3)proteins(3)
(Cell Research 2006)
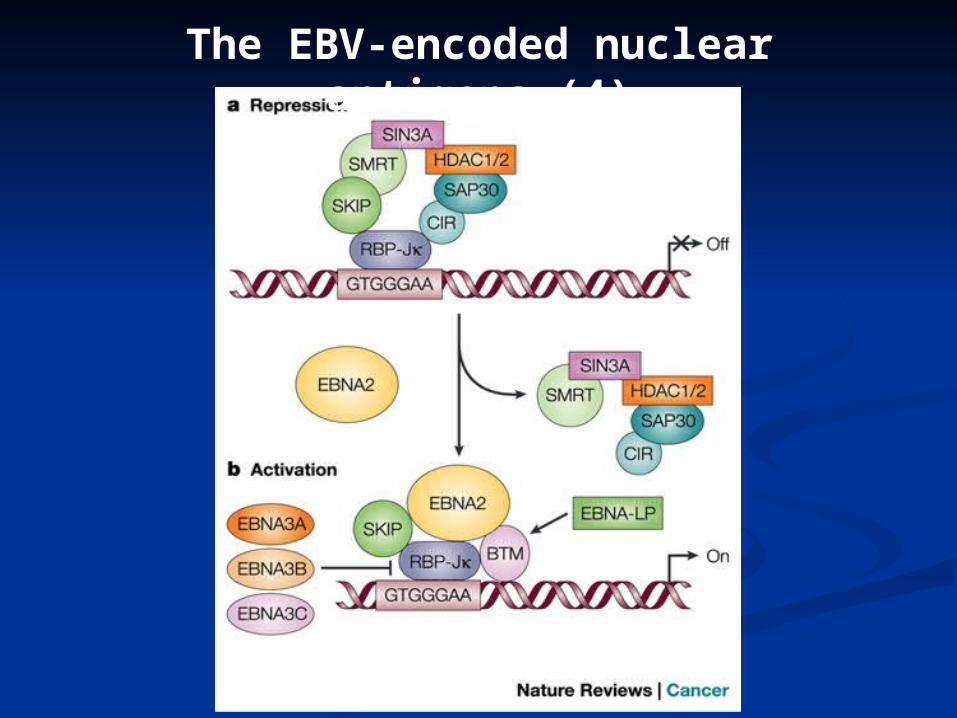
The EBV-encoded nuclear antigens (4)
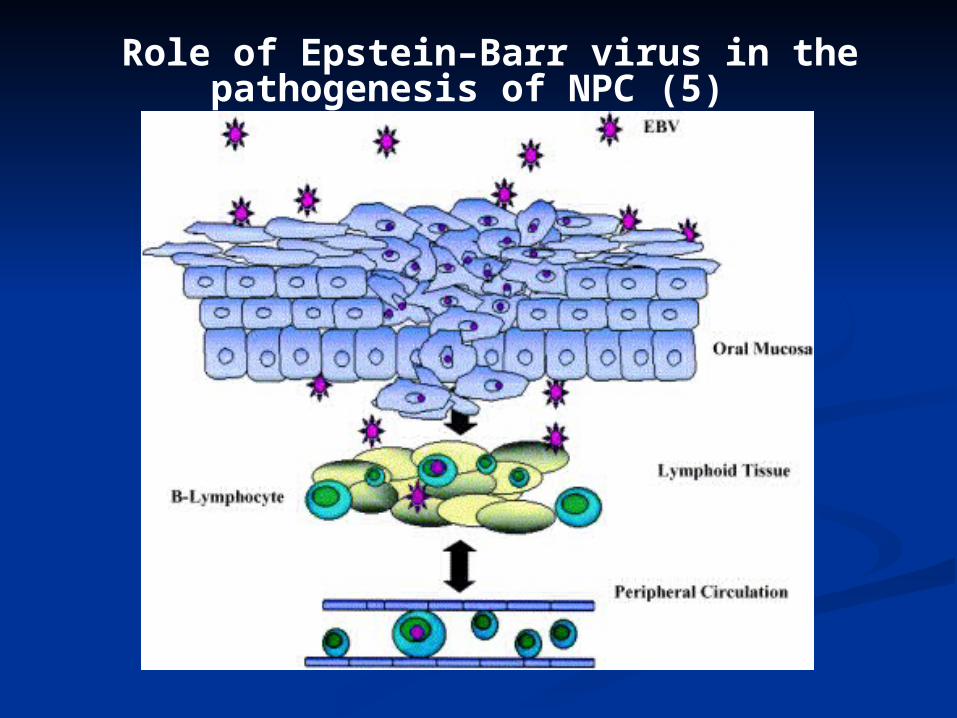
Role of Epstein–Barr virus in the pathogenesis of NPC (5)
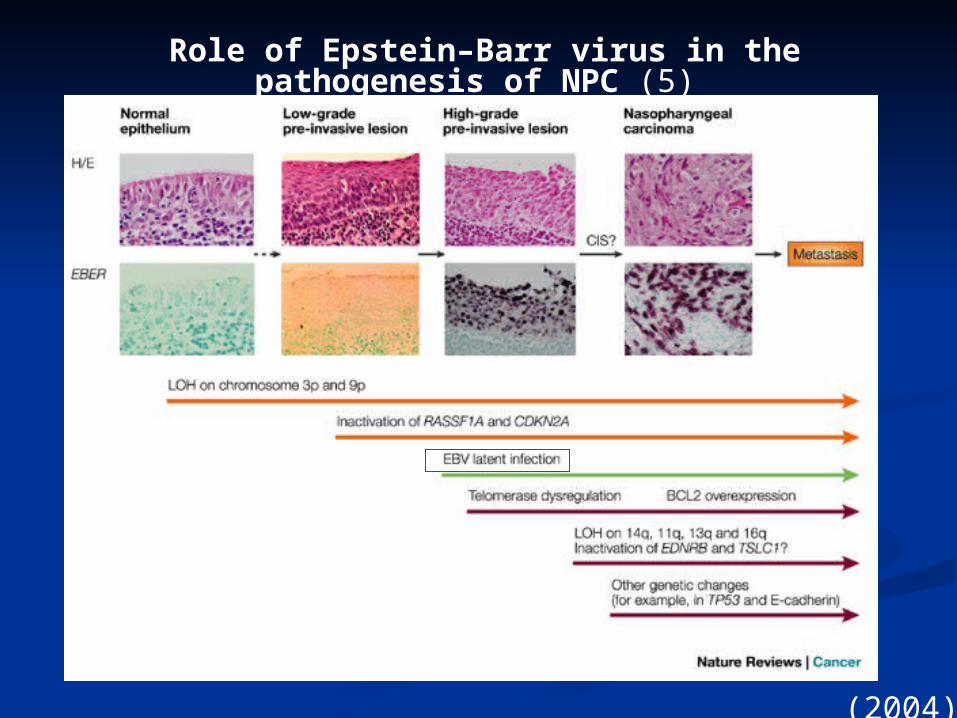
Role of Epstein–Barr virus in the pathogenesis of NPC (5)
(2004)
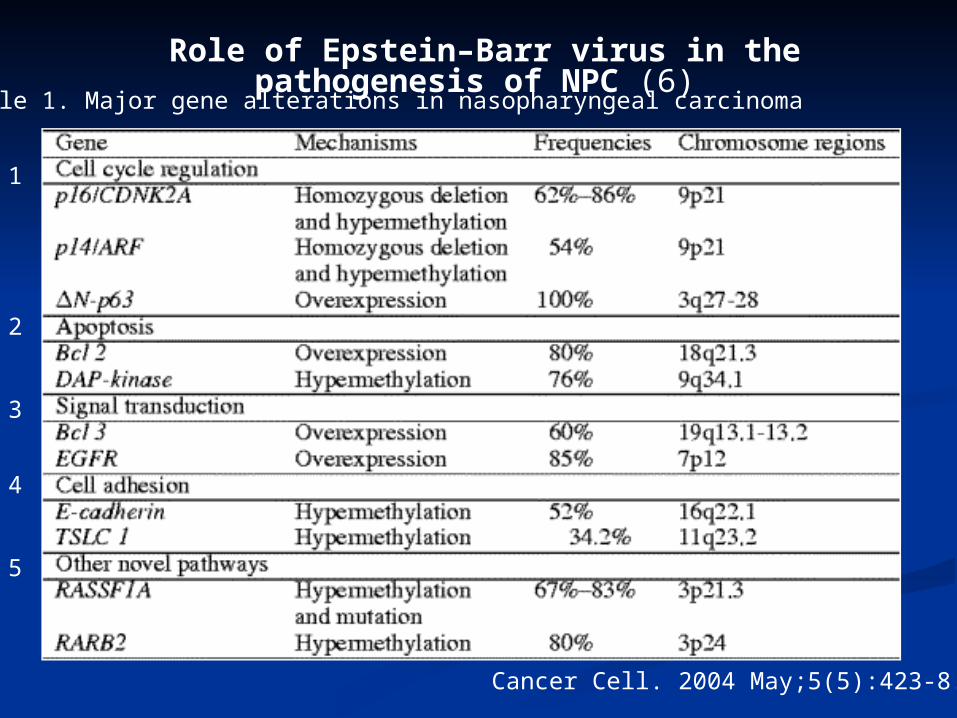
Table 1. Major gene alterations in nasopharyngeal carcinoma
Cancer Cell. 2004 May;5(5):423-8.
Role of Epstein–Barr virus in the pathogenesis of NPC (6)
1
2
3
4
5
Genetic background (1)Genetic background (1)
three new susceptibility loci, three new susceptibility loci, TNFRSF19TNFRSF19 on 13q12, EBV-LMP1, activat on 13q12, EBV-LMP1, activat
e JNK pathwaye JNK pathway MDS1-EVI1MDS1-EVI1 on 3q26, on 3q26, EVI1, MDS1 and thEVI1, MDS1 and th
e fusion protein MDS1-EVI1, e fusion protein MDS1-EVI1, transcriptitranscription factor, on factor, TGF-β signaling TGF-β signaling
CDKN2ACDKN2A--CDKN2BCDKN2B gene cluster on 9p21. gene cluster on 9p21. tumor suppressor genetumor suppressor gene
leukemogenesisleukemogenesis HLAHLA
(Nature Genetics 2010)
A gender-specific (A gender-specific (malemale) association of CNV a) association of CNV at 6p21.3 with NPC susceptibilityt 6p21.3 with NPC susceptibility
the CNV (Copy number variations, a major sothe CNV (Copy number variations, a major source of human genetic polymorphism ) locateurce of human genetic polymorphism ) located at chromosome 6p21.3, with single-copy deld at chromosome 6p21.3, with single-copy deletion of the etion of the MICAMICA and and HCP5HCP5 genes, showed th genes, showed the highest association with NPC.e highest association with NPC.
The The MICAMICA gene (11.7 kb) encodes a 383-amin gene (11.7 kb) encodes a 383-amino-acid polypeptide and functions as a ligand fo-acid polypeptide and functions as a ligand for NKG2D on γ/δT cells, CD8+ α/β T cells and or NKG2D on γ/δT cells, CD8+ α/β T cells and NK cells. (NK cells. (Immune functionImmune function))
(Hum Mol Genet. 2011)
Genetic background (2)Genetic background (2)
EBV gene (1)EBV gene (1)
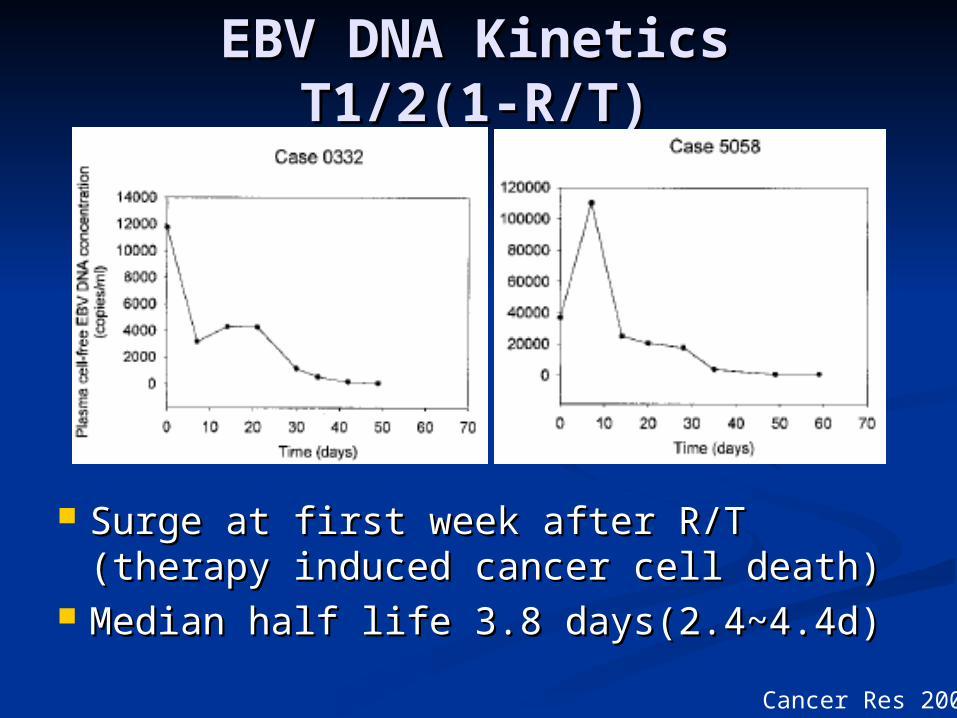
1.Circulating free EBV DNA copies increased during the initi1.Circulating free EBV DNA copies increased during the initial phase of radiotherapy after cell death.al phase of radiotherapy after cell death.118118
2.The quantity of free plasma EBV DNA is related to the stag2.The quantity of free plasma EBV DNA is related to the stage of the disease. The quantities of EBV DNA copies before e of the disease. The quantities of EBV DNA copies before and after treatment are significantly related to the rates of and after treatment are significantly related to the rates of overall and disease-free survival.overall and disease-free survival.119119
3.When EBV DNA was used together with Anti-EBV VCA I3.When EBV DNA was used together with Anti-EBV VCA IgA, the sensitivity of early diagnosis of nasopharyngeal cagA, the sensitivity of early diagnosis of nasopharyngeal carcinoma increased.rcinoma increased.121121
4.Raised levels of EBV DNA were only detected in 67% of p4.Raised levels of EBV DNA were only detected in 67% of patients with locoregional recurrence,atients with locoregional recurrence,116116 and and 122122 although in th although in those with distant metastasis levels of EBV DNA copies werose with distant metastasis levels of EBV DNA copies were heightened before the appearance of clinical abnormality.e heightened before the appearance of clinical abnormality.116116
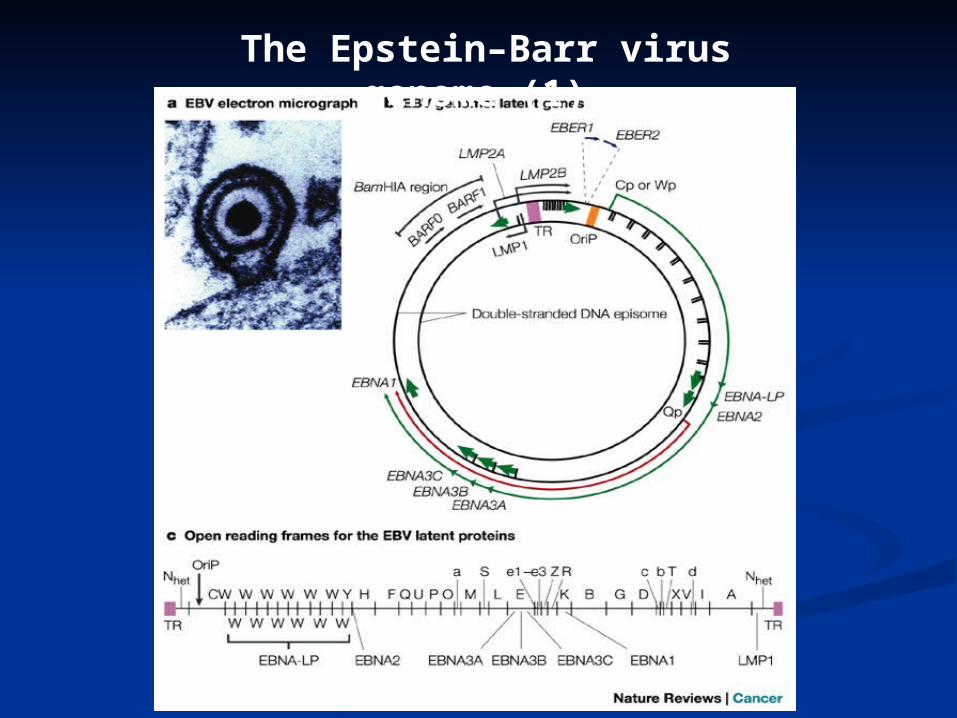
The Epstein–Barr virus genome (1)
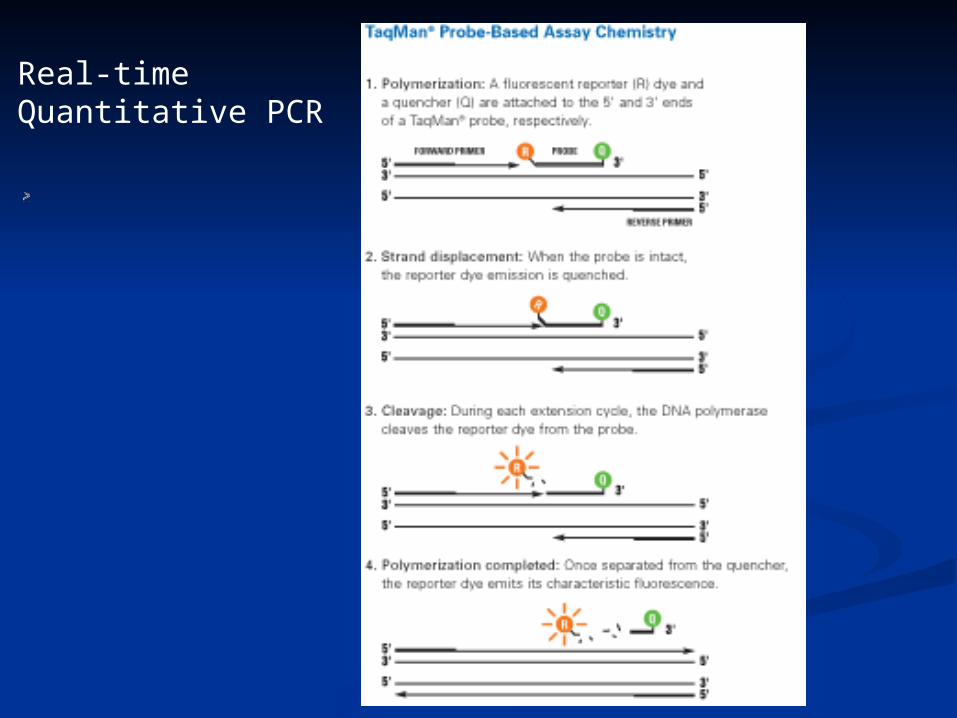
Real-time Quantitative PCR
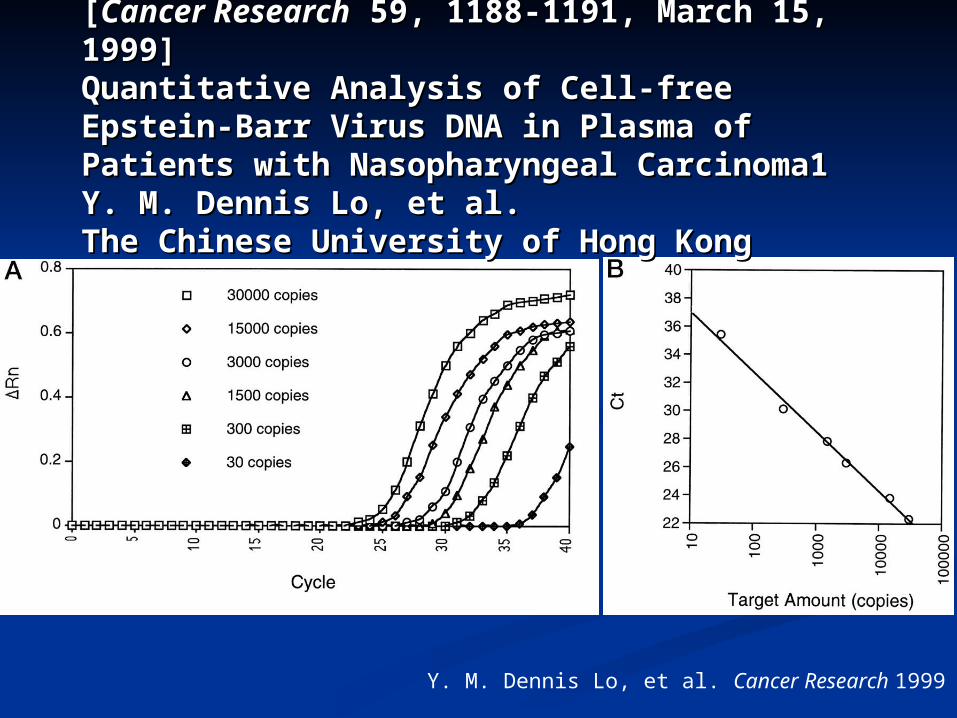
[[Cancer ResearchCancer Research 59, 1188-1191, March 15, 1999] 59, 1188-1191, March 15, 1999]Quantitative Analysis of Cell-free Epstein-Barr Virus Quantitative Analysis of Cell-free Epstein-Barr Virus DNA in Plasma of Patients with Nasopharyngeal DNA in Plasma of Patients with Nasopharyngeal Carcinoma1 Carcinoma1 Y. M. Dennis Lo, et al. Y. M. Dennis Lo, et al. The Chinese University of Hong KongThe Chinese University of Hong Kong
Y. M. Dennis Lo, et al. Cancer Research 1999
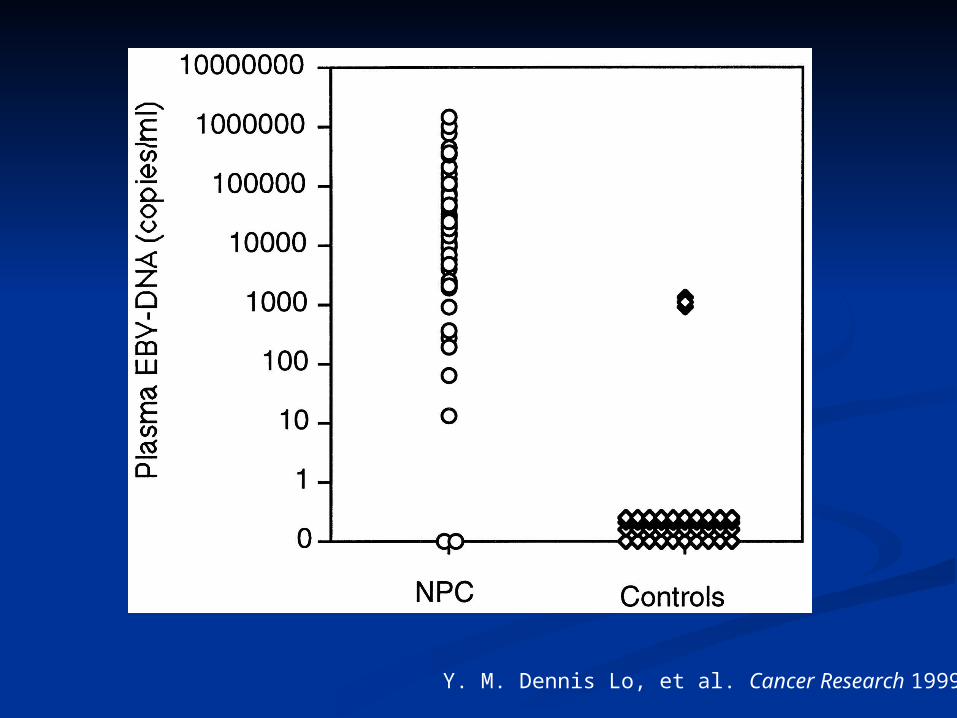
Y. M. Dennis Lo, et al. Cancer Research 1999
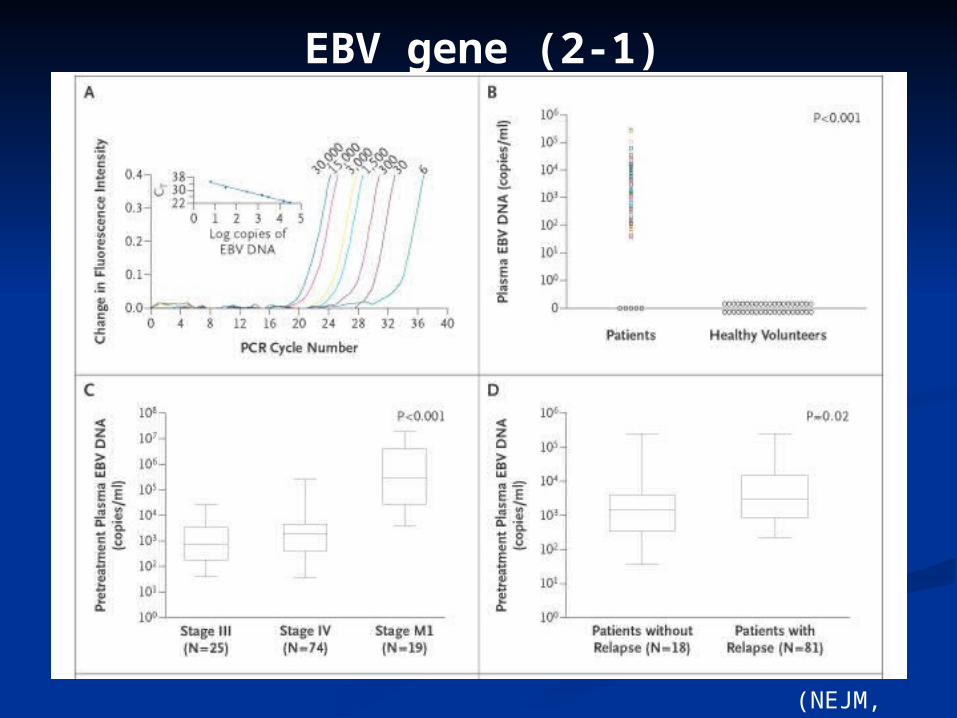
(NEJM, 2004)
EBV gene (2-1)
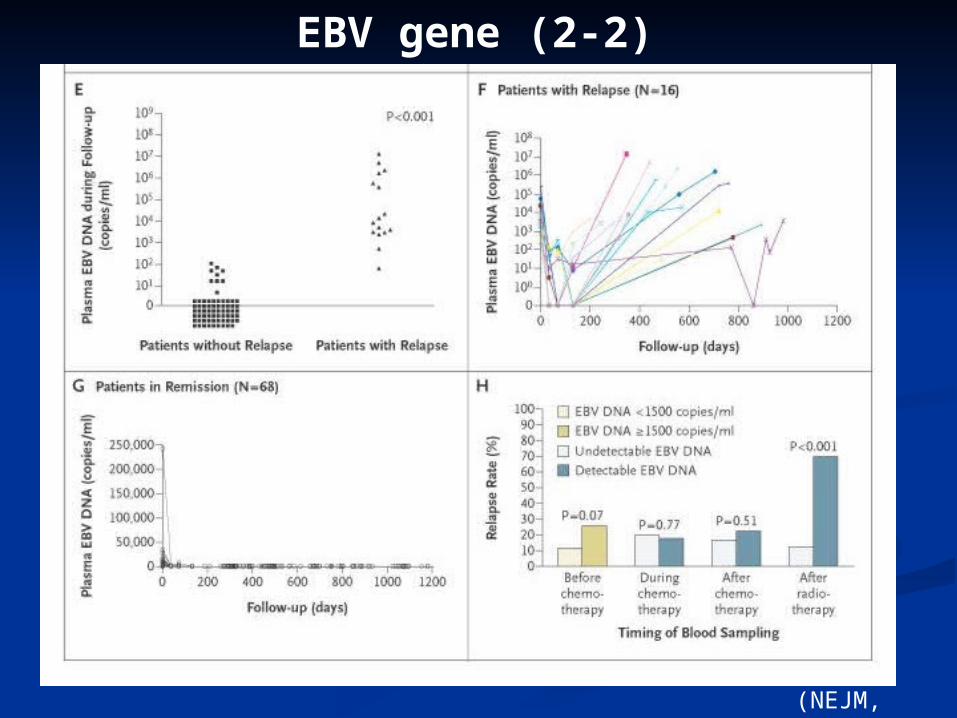
EBV gene (2-2)
(NEJM, 2004)
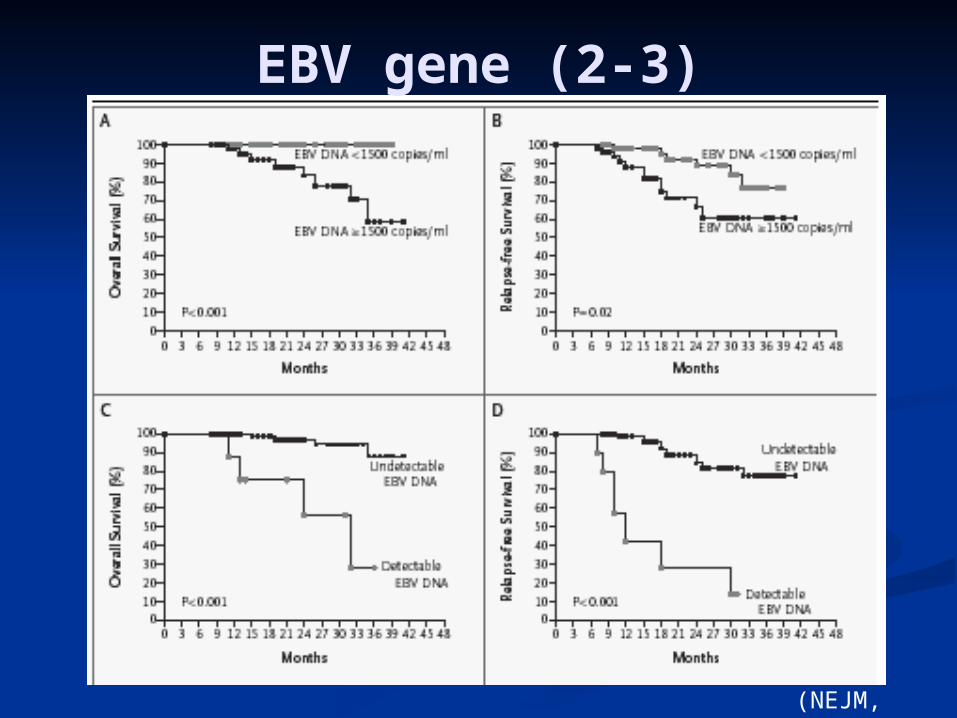
EBV gene (2-3)
(NEJM, 2004)
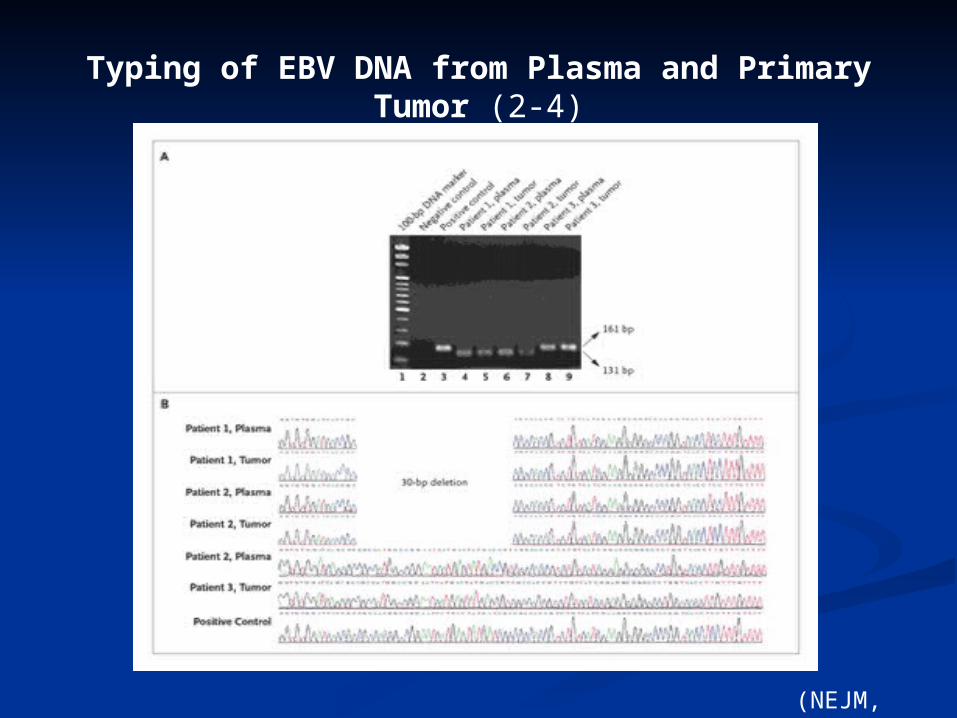
Typing of EBV DNA from Plasma and Primary Tumor (2-4)
(NEJM, 2004)
EBV DNA Kinetics EBV DNA Kinetics T1/2(1-R/T)T1/2(1-R/T)
Surge at first week after R/T Surge at first week after R/T (therapy induced cancer cell death)(therapy induced cancer cell death)
Median half life 3.8 days(2.4~4.4d)Median half life 3.8 days(2.4~4.4d)Cancer Res 2000
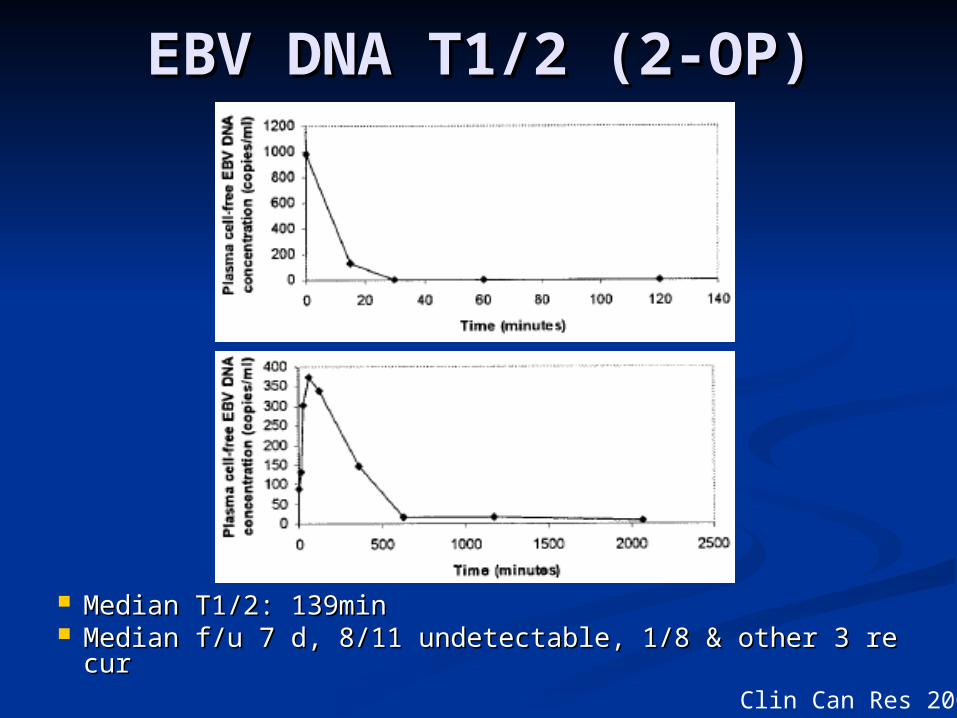
Median T1/2: 139minMedian T1/2: 139min Median f/u 7 d, 8/11 undetectable, 1/8 & other 3 recurMedian f/u 7 d, 8/11 undetectable, 1/8 & other 3 recur
EBV DNA T1/2 (2-OP)EBV DNA T1/2 (2-OP)
Clin Can Res 2003
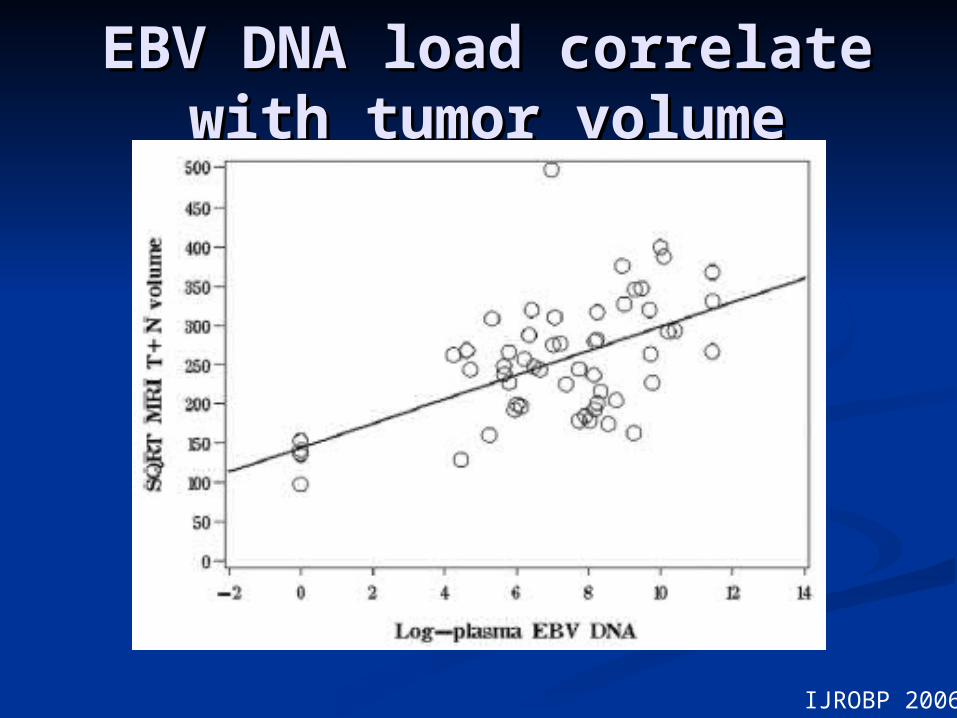
EBV DNA load correlate EBV DNA load correlate with tumor volumewith tumor volume
IJROBP 2006
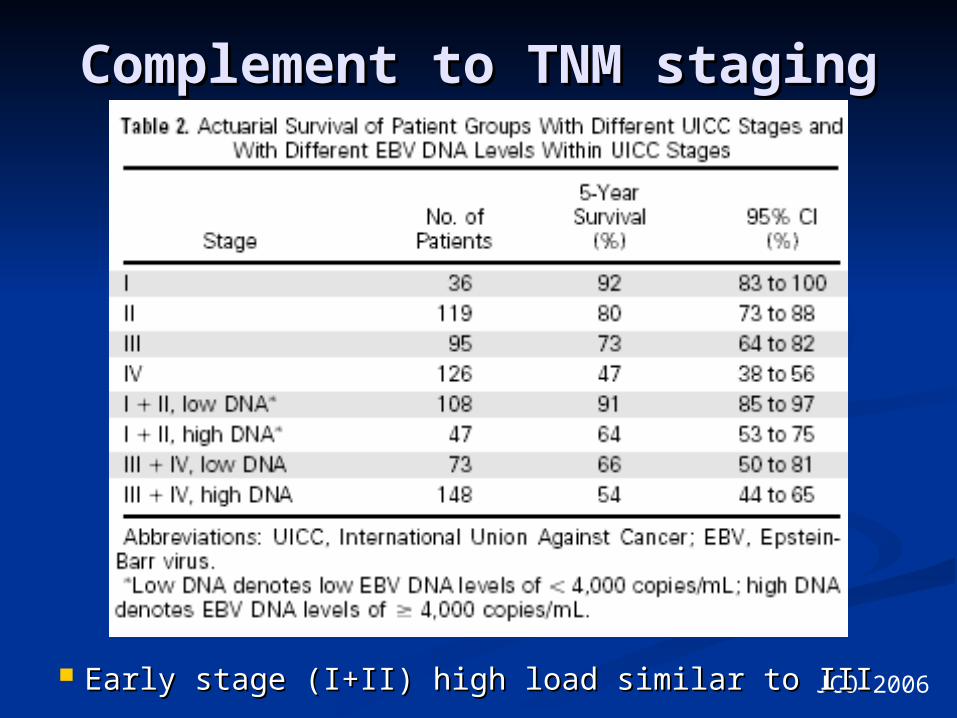
Complement to TNM Complement to TNM stagingstaging
JCO 2006 Early stage (I+II) high load similar to IIIEarly stage (I+II) high load similar to III
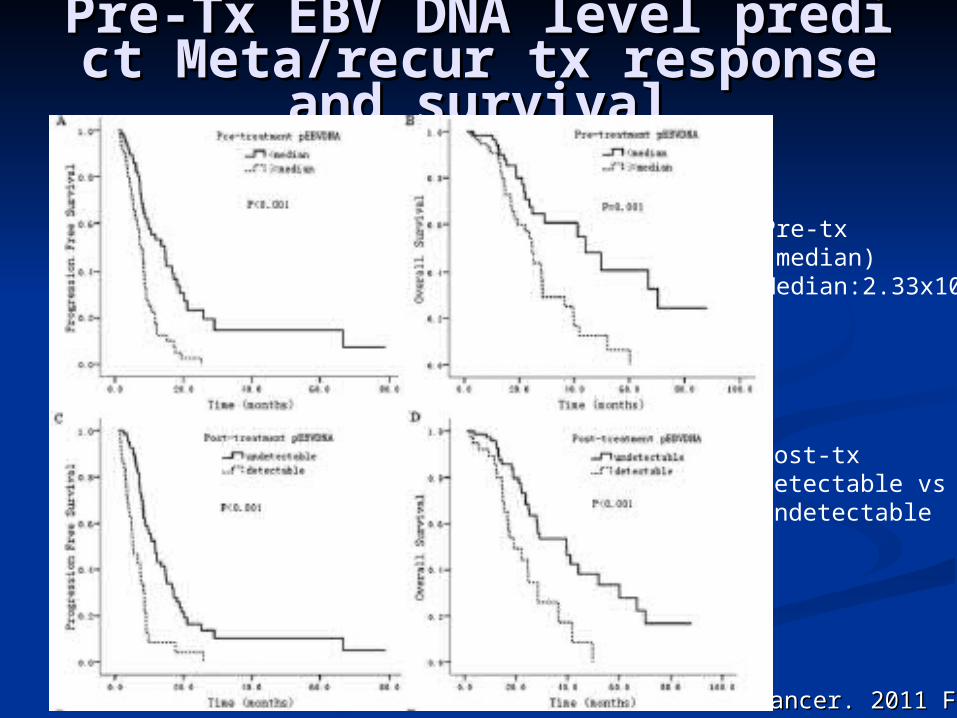
Pre-Tx EBV DNA level predict Pre-Tx EBV DNA level predict Meta/recur tx response and suMeta/recur tx response and su
rvivalrvival
Cancer. 2011 FebCancer. 2011 Feb
Pre-tx(median)Median:2.33x105
Post-txDetectable vsundetectable
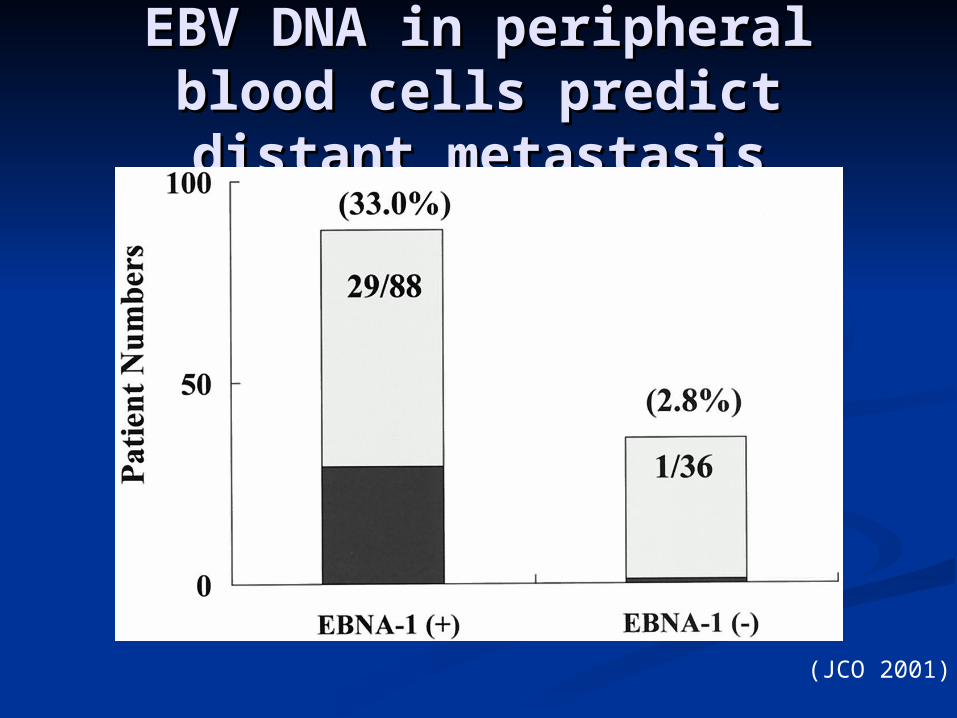
EBV DNA in peripheral EBV DNA in peripheral blood cells predict distant blood cells predict distant
metastasismetastasis
(JCO 2001)
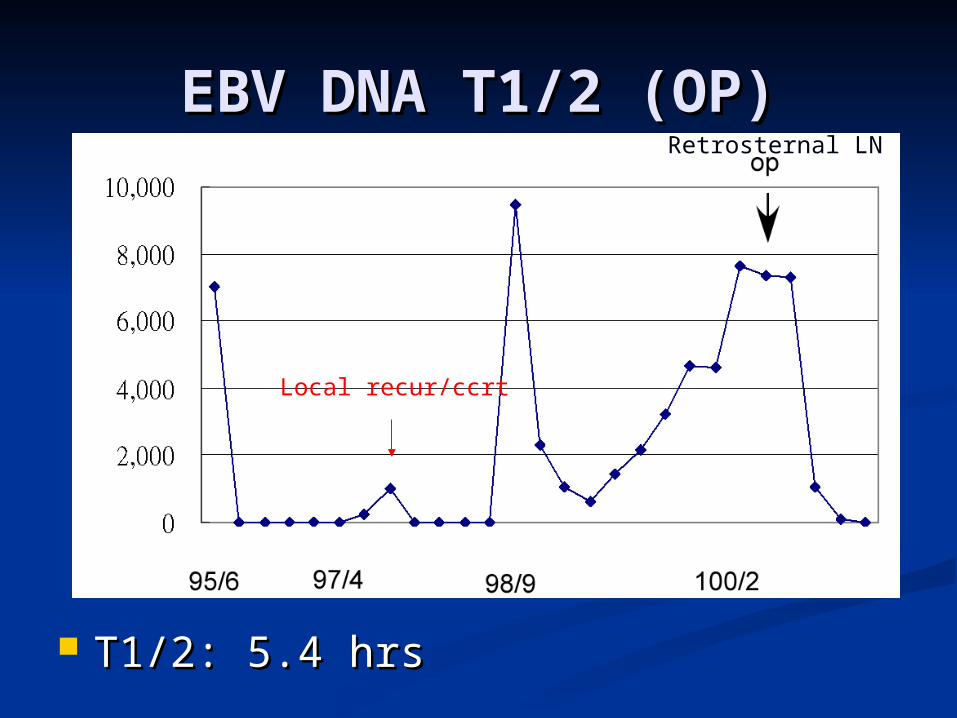
EBV DNA T1/2 (OP)EBV DNA T1/2 (OP)
T1/2: 5.4 hrsT1/2: 5.4 hrs
Local recur/ccrt
Retrosternal LN
煥
1420 0 0 0 0
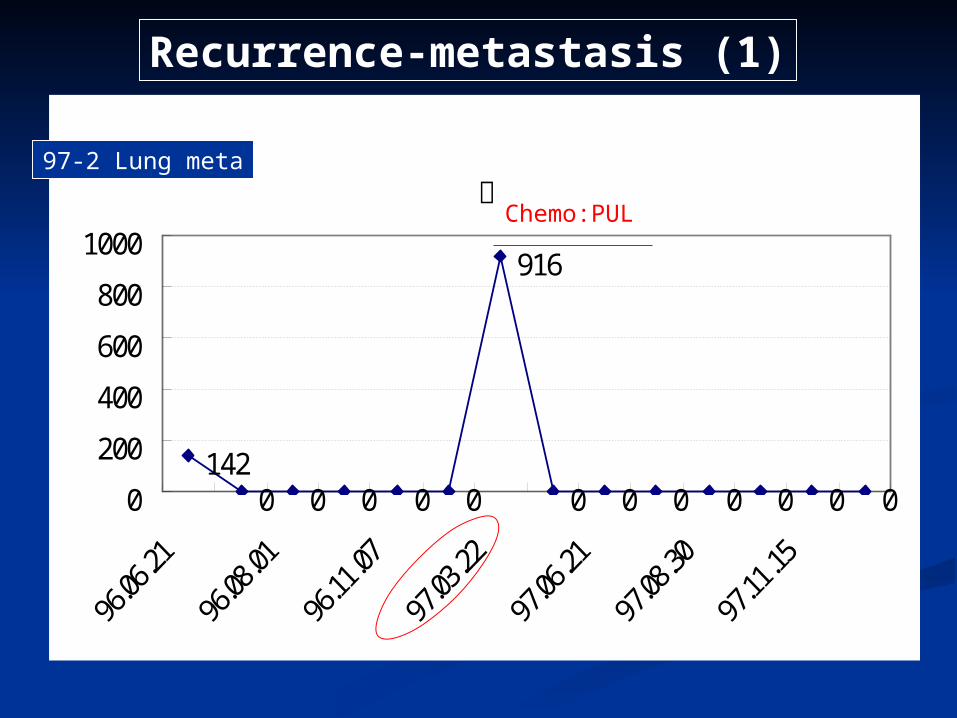
916
0 0 0 0 0 0 00
200
400
600
800
1000
Recurrence-metastasis (1)
Chemo:PUL
97-2 Lung meta
興
01234567
95.06.07
95.10.18
95.11.01
95.12.13
96.01.17
96.02.14
96.03.07
96.03.28
96.05.09
96.07.04
96.08.28
LOG
10
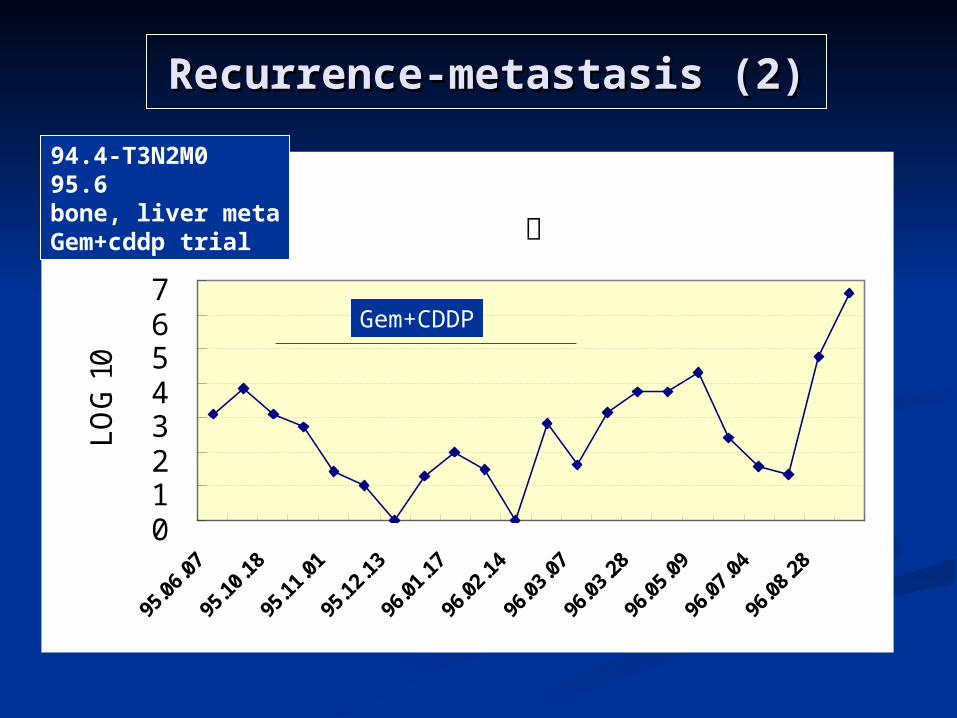
Gem+CDDP
94.4-T3N2M095.6 bone, liver metaGem+cddp trial
Recurrence-metastasis (2)Recurrence-metastasis (2)
XX呂
0
1
2
3
4
5
695
.04.
12
95.1
0.25
96.0
6.13
96.1
0.17
97.1
1.06
97.1
2.03
97.1
2.10
98.0
1.07
LOG
10
XX呂
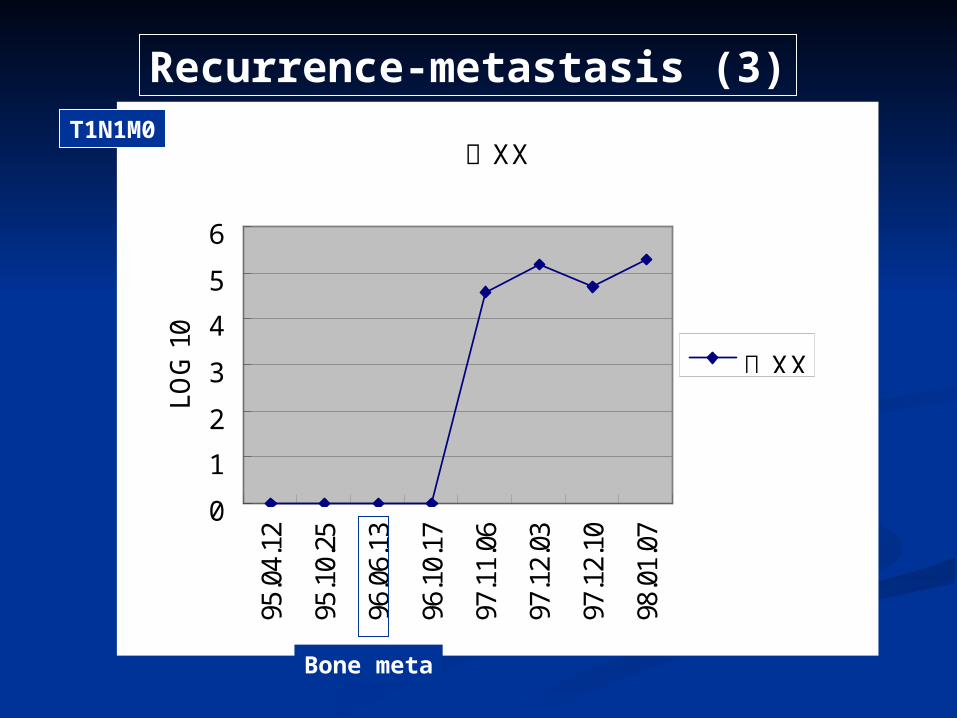
T1N1M0
Recurrence-metastasis (3)
Bone meta
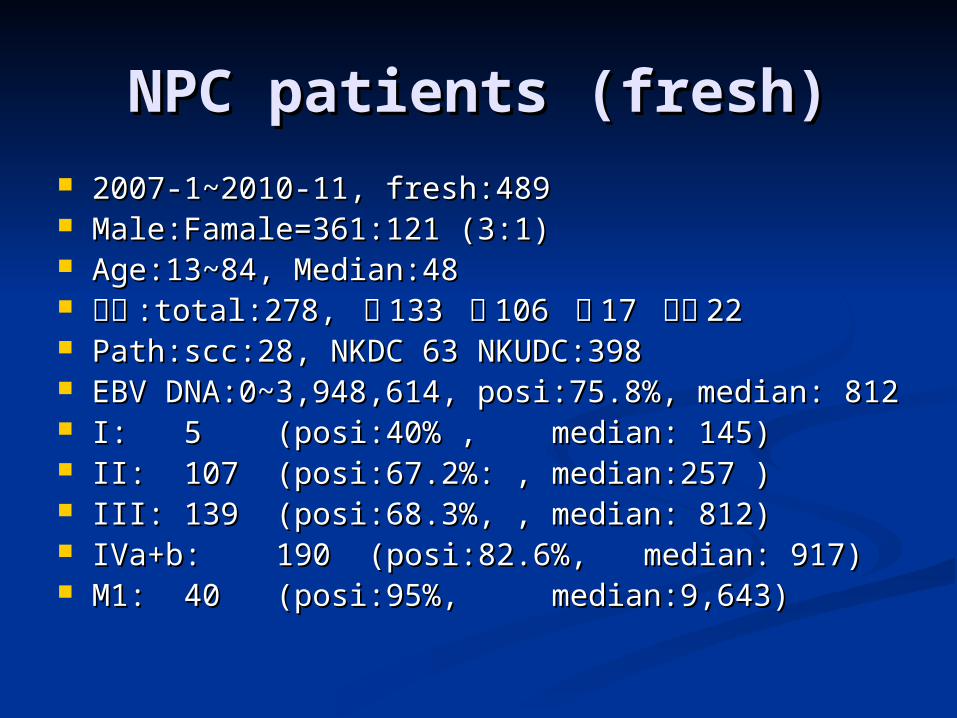
NPC patients (fresh)NPC patients (fresh) 2007-1~2010-11, fresh:4892007-1~2010-11, fresh:489 Male:Famale=361:121 (3:1)Male:Famale=361:121 (3:1) Age:13~84, Median:48Age:13~84, Median:48 籍貫籍貫 :total:278, :total:278, 閩閩 133 133 客客 106 106 原原 17 17 其他其他 2222 Path:scc:28, NKDC 63 NKUDC:398Path:scc:28, NKDC 63 NKUDC:398 EBV DNA:0~3,948,614, posi:75.8%, median: 812EBV DNA:0~3,948,614, posi:75.8%, median: 812 I:I: 55 (posi:40% , (posi:40% , median: 145) median: 145) II:II: 107107 (posi:67.2%: ,(posi:67.2%: , median:257 ) median:257 ) III:III: 139139 (posi:68.3%, , (posi:68.3%, , median: 812) median: 812) IVa+b:IVa+b: 190 190 (posi:82.6%, (posi:82.6%, median: 917) median: 917) M1:M1: 4040 (posi:95%, (posi:95%, median:9,643) median:9,643)
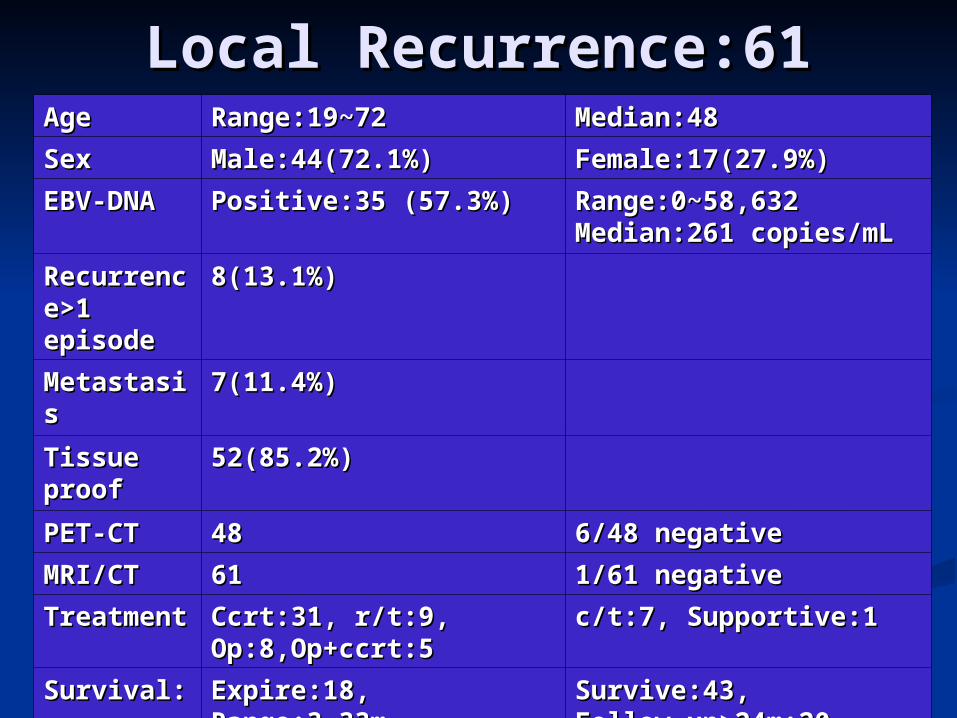
Local Recurrence:61Local Recurrence:61AgeAge Range:19~72Range:19~72 Median:48Median:48
SexSex Male:44(72.1%)Male:44(72.1%) Female:17(27.9%)Female:17(27.9%)
EBV-DNAEBV-DNA Positive:35 (57.3%)Positive:35 (57.3%) Range:0~58,632Range:0~58,632Median:261 copies/mLMedian:261 copies/mL
Recurrence>Recurrence>1 episode1 episode
8(13.1%)8(13.1%)
MetastasisMetastasis 7(11.4%)7(11.4%)
Tissue proofTissue proof 52(85.2%)52(85.2%)
PET-CTPET-CT 4848 6/48 negative6/48 negative
MRI/CTMRI/CT 6161 1/61 negative1/61 negative
TreatmentTreatment Ccrt:31, r/t:9, Ccrt:31, r/t:9, Op:8,Op+ccrt:5Op:8,Op+ccrt:5
c/t:7, Supportive:1c/t:7, Supportive:1
Survival:Survival: Expire:18, Range:3~33mExpire:18, Range:3~33mMedian:9mMedian:9m
Survive:43, Survive:43, Follow-up>24m:20Follow-up>24m:20Median:32mMedian:32m
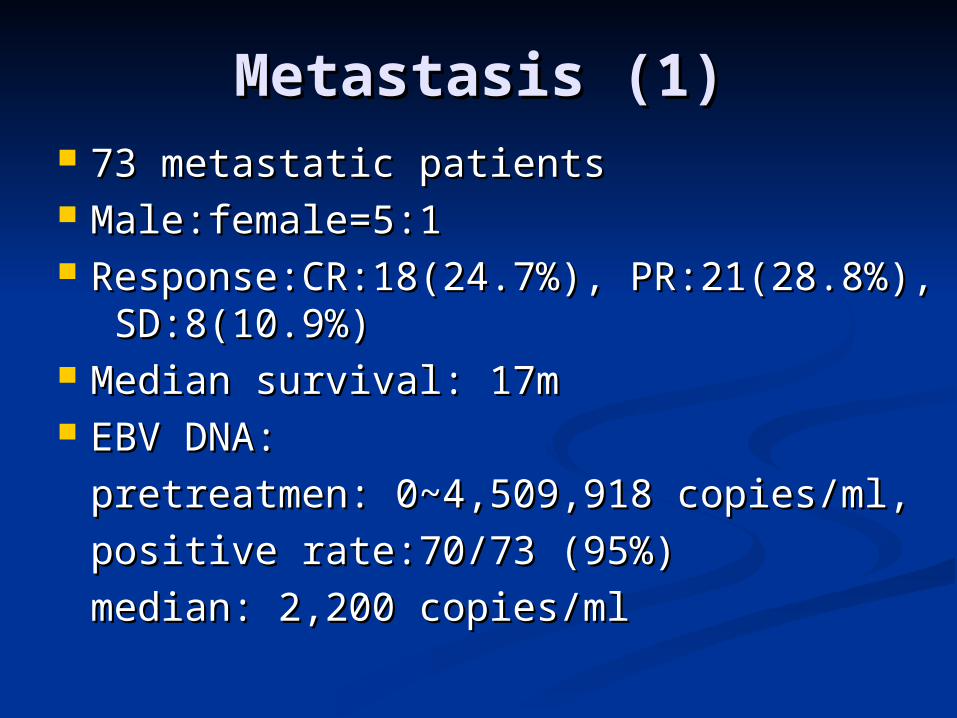
Metastasis (1)Metastasis (1) 73 metastatic patients73 metastatic patients Male:female=5:1Male:female=5:1 Response:CR:18(24.7%), PR:21(28.8%), Response:CR:18(24.7%), PR:21(28.8%),
SD:8(10.9%)SD:8(10.9%) Median survival: 17mMedian survival: 17m EBV DNA: EBV DNA:
pretreatmen: 0~4,509,918 copies/ml, pretreatmen: 0~4,509,918 copies/ml, positive rate:70/73 (95%)positive rate:70/73 (95%)median: 2,200 copies/mlmedian: 2,200 copies/ml
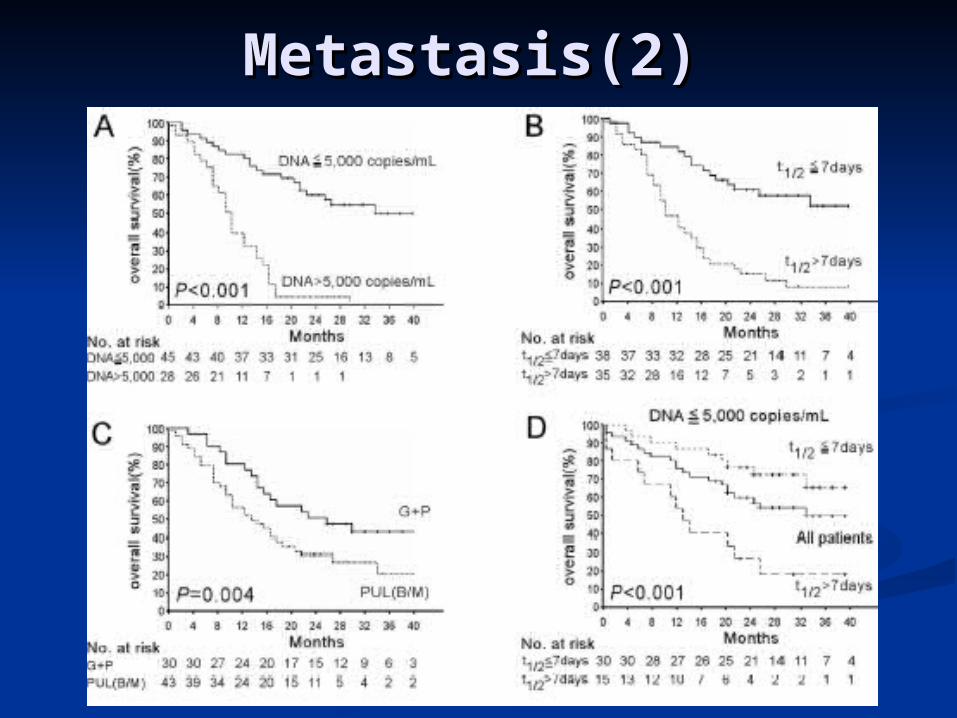
Metastasis(2)Metastasis(2)
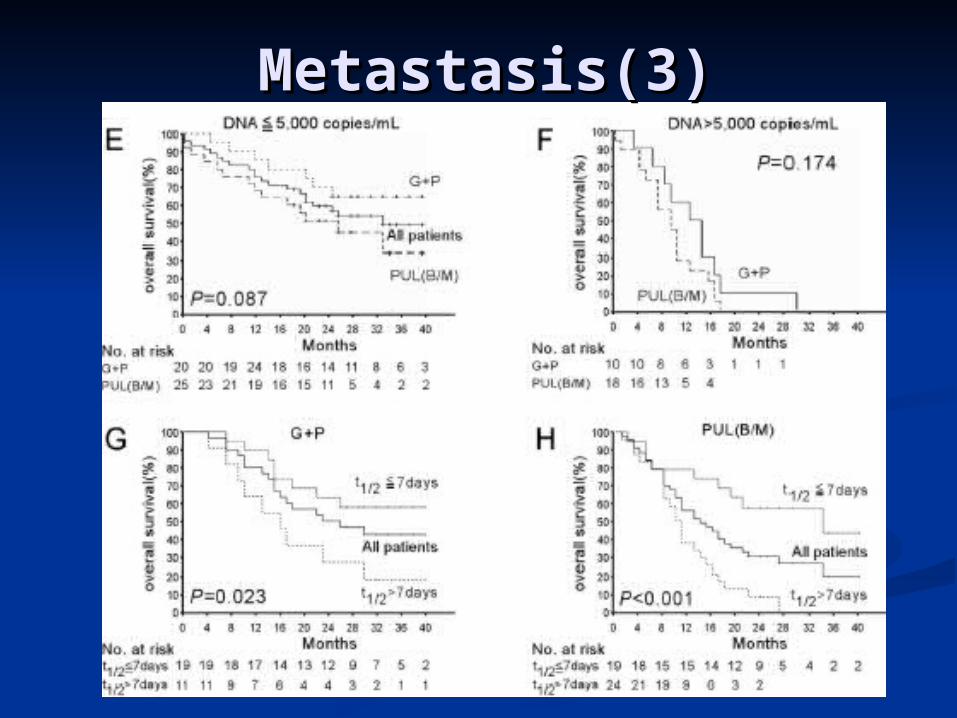
Metastasis(3)Metastasis(3)
SummarySummary Plasma EBV DNA is a Plasma EBV DNA is a novel tumor markernovel tumor marker
and independent prognostic factor in and independent prognostic factor in NPCNPC
Correlate with Correlate with tumor burdentumor burden, , complement to TNM staging (especially complement to TNM staging (especially in in early stage with high viral loadearly stage with high viral load), and ), and correlate with disease status.correlate with disease status.
More higher positive rate and viral load More higher positive rate and viral load in in metastasismetastasis than local recurrence than local recurrence
Predict prognosisPredict prognosis (treatment response (treatment response and survival) in metastasis patientsand survival) in metastasis patients
AcknowledgementAcknowledgement
長庚醫院長庚醫院醫研部醫研部內科部內科部血液腫瘤科血液腫瘤科
施麗雲教授施麗雲教授王宏銘副教王宏銘副教
授授
頭頸部腫瘤團隊頭頸部腫瘤團隊
長庚大學長庚大學 張玉生教授張玉生教授黎欣白老師黎欣白老師