Embed Size (px)
Citation preview
o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 9
Available online at www.sciencedirect.com
journal homepage: www.elsevier.com/locate/odw
Research paper
Evaluation of bone regeneration by porous alpha-tricalciumphosphate/atelocollagen sponge composite in rat calvarialdefects
Yoshiyuki Arima a,*, Naoya Uemura b, Yoshiya Hashimoto c, Shunsuke Baba b,Naoyuki Matsumoto d
aDepartment of Orthodontics, Graduate School of Dentistry, Osaka Dental University, 8-1 Kuzuhahanazonocho, Hirakata,
Osaka 573-1121, JapanbDepartment of Oral Implantology, Osaka Dental University, 1-5-17 Otemae, Chuo-ku, Osaka 540-0008, JapancDepartment of Biomaterials, Osaka Dental University, 8-1 Kuzuhahanazonocho, Hirakata, Osaka 573-1121, JapandDepartment of Orthodontics, Osaka Dental University, 8-1 Kuzuhahanazonocho, Hirakata, Osaka 573-1121, Japan
a r t i c l e i n f o
Article history:
Received 28 June 2012
Received in revised form
17 October 2012
Accepted 16 November 2012
Published on line 14 December 2012
Keywords:
Porous a-tricalcium phosphate
Collagen sponge composite
Bone tissue engineering
Rat calvarial defects
a b s t r a c t
Purpose: Both atelocollagen and alpha-tricalcium phosphate (a-TCP) particles are widely
applied as bone graft materials. In this study, we combined atelocollagen and porous a-TCP
particles to form an a-TCP/atelocollagen composite sponge (a-TCP/CS), and we evaluated its
effects on bone regeneration in rat calvarial defects.
Materials and methods: a-TCP granules were mixed with a collagen solution. The mixture was
poured into plastic molds and then frozen to �80 8C and freeze-dried for 24 h. The compo-
sites were then cross-linked in vacuo at 140 8C for 24 h. The obtained composites were
characterized by XRD and SEM and observed using micro-CT and histological analysis.
Results: In vivo micro-CT images at 2, 4, and 6 weeks after surgery showed that in the a-TCP/
CS group, the bone volume, bone mineral density, and bone mineral content were higher
than those in the groups with only atelocollagen and without scaffolds at 6 weeks after
surgery. Histological analysis showed that a-TCP was completely absorbed, and new bone
that was continuous along the original bone was observed.
Conclusion: This study demonstrated that composite sponges created using porous a-TCP
lagen were sufficiently adaptable for treating bone defects.
sevier Ltd and the Japanese Orthodontic Society. All rights reserved.
# 2012 Elparticles and atelocol
1. Introduction
Cleft lip and palate is a frequently occurring congenital
malformation that is caused by alveolar bone defects [1,2]. A
cleft can lead to problems with feeding and speech, among
others, and therefore, surgical closure is strongly recom-
mended [3,4]. Among various surgical treatments, autologous
* Corresponding author. Tel.: +81 72 864 3078; fax: +81 72 864 3178.E-mail addresses: [email protected], arima_dental@ybb
1344-0241/$ – see front matter # 2012 Elsevier Ltd and the Japanesehttp://dx.doi.org/10.1016/j.odw.2012.11.001
bone grafting has become a well-accepted treatment for
restoring the function and structure of the maxillary arch at
the cleft site.
Autologous bone is widely regarded as the gold standard
graft material [5,6]. However, a limited amount of autologous
bone can be harvested from an individual, and the procedure
is invasive. Therefore, scaffold materials should be bioabsorb-
able and be ultimately replaced by autologous tissue [7].
.ne.jp, [email protected] (Y. Arima).
Orthodontic Society. All rights reserved.

o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 924
Furthermore, they should have outstanding handling char-
acteristics for surgical applications, because conventional
granular materials tend to leak from pores and are difficult to
apply to bone defects [8].
Owing to such issues, various materials have been
developed as substitutes to autologous bone. Popular among
these are hydroxyapatite (HA), tricalcium phosphate (TCP),
and tetracalcium phosphate, which are widely used in
orthopedic and maxillofacial surgery, because they show high
biocompatibility and osteocompatibility [9]. Among various
calcium phosphate materials, studies have previously
highlighted the promise of a-TCP particles as bone rebuilding
materials, because they gradually biodegrade while bone
regenerates around them [10]. For example, Kitamura et al. [11]
developed an a-TCP porous body with a continuous pore
structure via an easy processing route by using a conventional
sintering procedure—they used a slurry of b-TCP and potato
starch to produce a-TCP that was in a thermodynamically
stable phase at temperatures above 1100 8C.
Separately, collagen has been widely applied clinically in
various forms, such as gels or sponges, because it shows good
biodegradability, biocompatibility, and absorbability [12,13].
For example, collagen sponges are considered to be a useful
scaffold matrix for several types of tissues. Our previous study
evaluated the effects on bone formation of combining
synthesized collagen model polypeptides consisting of a
Pro-Hyp-Gly [poly(PHG)] sequence and a-TCP in a skull defect
model in mini-pigs [8].
In light of these advantageous characteristics, in this study,
we fabricated a porous a-TCP/collagen sponge (aTCP/CS)
composite for the regeneration of alveolar bone defects by
bonding collagen fibrils and a-TCP granules by a dehydrother-
mal cross-linking method. Then, we evaluated the effects of a-
TCP/CS on bone regeneration in surgically created rat calvarial
defects.
2. Materials and methods
2.1. X-ray diffraction measurements of a-TCP
X-ray diffraction (XRD) measurements were performed using a
Geigerflex diffractometer (Ultima IV; Rigaku, Tokyo, Japan)
with Cu Ka radiation generated at 40 kV and 40 mA. The scan
rate was 48/min with a step size of 0.028 over a 2u range of
10–808.
2.2. Preparation of a-TCP/collagen sponge composites
Porous a-TCP granules were kindly supplied by Taihei
Chemical Ind. Co., Ltd., Osaka, Japan. The granules were
prepared by the pulverization of an a-TCP block with total
pores of 80% having continuous pore structures of both 10 and
200 mm diameters. The collagen used was extracted from
porcine skin by enzymatic treatment with pepsin (Nippon
Meat Packers, Osaka, Japan). Next, a-TCP particles were mixed
with the homogenized collagen solution at a ratio of 150 mg/
mL (a-TCP particles/collagen solution). The mixture was then
poured into plastic molds, following which all samples were
immediately frozen to �80 8C and freeze-dried for 24 h. The
freeze-dried a-TCP/collagen composites resembled sponge-
like structures, and they were subsequently cross-linked in
vacuo at 140 8C for 24 h. The microstructures of the obtained
scaffolds were then observed using an SEM (S-450, Hitachi Ltd.,
Tokyo, Japan).
2.3. Surgical procedure
The protocol for this experiment was approved by the Osaka
Dental University Animal Ethics Committee (Approval Num-
ber 11-03043). We used the rat calvarial defect model to test
our hypothesis, as it is a convenient model for the study of
bone regenerative materials because of its lack of fixation
requirements. A total of 27 male Sprague-Dawley rats (age: 12
weeks, weight: 350–370 g) were used for transplantation. The
rats were anesthetized with a 30 mg/kg intraperitoneal
injection of pentobarbital sodium (Somnopentyl1; Kyoritsu
Seiyaku, Tokyo, Japan); in addition, 0.2 mL of local anesthetic
(1% xylocaine/epinephrine 1:100,000, AstraZeneca, Tokyo,
Japan) was injected into the surgical sites before the start of
surgery. The surgical areas were shaved and disinfected with
povidone-iodine (Isodine Surgical Scrub, Meiji, Tokyo, Japan).
Then, skin incision and subperiosteal dissection were carried
out. A skin flap was raised, and bone defect (diameter: 5 mm,
depth: 1.0 mm) was created at the center of the skull using a
bone trephine bur (external diameter: 5 mm) under running
water. Three groups were prepared for the experiments. One is
filled with a-TCP/CS; another is filled with only CS; and the
control group was not filled with any material. In all groups,
the defects were covered using a GORE-TEX1 GTR membrane
(Japan Gore-Tex Co., Tokyo, Japan). Finally, the flap was
repositioned and sutured. The skin was sutured by 3-0 silk
(Natsume Seisakusho Co., Tokyo, Japan). The animals were
euthanized at 2, 4, and 6 weeks after surgery (n = 3).
2.4. Micro-CT and computer analysis
After euthanization, the calvarial bone was scanned by micro-
CT (65 kV, 90 mA) (SMX-130CT; Shimadzu, Kyoto, Japan). The
linearity of the micro-CT scanner was established by scanning
a phantom containing several densities of a standard
calibration material. The 3D calvarial bone was measured
and its structural indices were calculated using a morpho-
metric program (TRI/3D-BON; Ratoc System Engineering,
Tokyo, Japan). For bone density measurements, an HA
calibration curve was prepared from the images of phantoms
(Ha content: 200, 300, 400, 500, 600, 700, and 800 mg/cm3). New
bone was measured using the TRI/3D-BON 3D analysis routine
using the obtained CT values. In the 3D analysis, the total
volume (TV, cm3), bone volume (BV, cm3), and bone mineral
content (BMC, mg) were measured directly. The volumetric
density was calculated as BV/TV (%), and the bone mineral
density (BMD) was calculated as BMC/BV (mg/cm3); these
indices respectively evaluated the quantity and density of new
bone.
2.5. Histological analysis
Histological examination was carried out to observe the tissue
structures and thicknesses of the new bone. Samples were

[(Fig._1)TD$FIG]
Fig. 1 – XRD patterns of a-TCP particles/CS (A) and a-TCP
particles (B).
o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 9 25
fixed with 10% phosphoric acid in neutral buffered formalin
for 2 weeks. Subsequently, they were processed for histologi-
cal examination according to standard procedures—the
samples were decalcified, embedded in paraffin, sectioned
at 4-mm thickness, and subjected to hematoxylin and eosin
(HE) staining. All the stained sections were observed by light
microscopy (BZ-9000; Keyence Co., Osaka, Japan).
2.6. Statistical analysis
All data were expressed as the mean and standard error.
Differences were evaluated by analysis of variance (ANOVA)
with Scheffe’s F-test. Differences were considered significant
at p < 0.05.
3. Results
3.1. X-ray diffraction measurements of a-TCP particles
Fig. 1 shows XRD patterns of a-TCP/CS and the original a-TCP.
The diffraction peaks of a-TCP/CS (Fig. 1A) were reduced
compared to those of the original a-TCP (Fig. 1B). However, a
comparison of the scatter plot data of the synthesized a-TCP
particles against a-TCP data registered with the Joint Com-
mittee on Powder Diffraction Standards (JCPDS) confirmed
that these peaks appeared at the same angles.
3.2. SEM observation of a-TCP/collagen sponge
Fig. 2A shows the appearance of CS, and Fig. 2B shows the
microstructure of a-TCP/CS. The composites were composed
of a-TCP granules (diameter: 0.2 mm) and a three-dimensional
porous structure (with an anatomizing network).
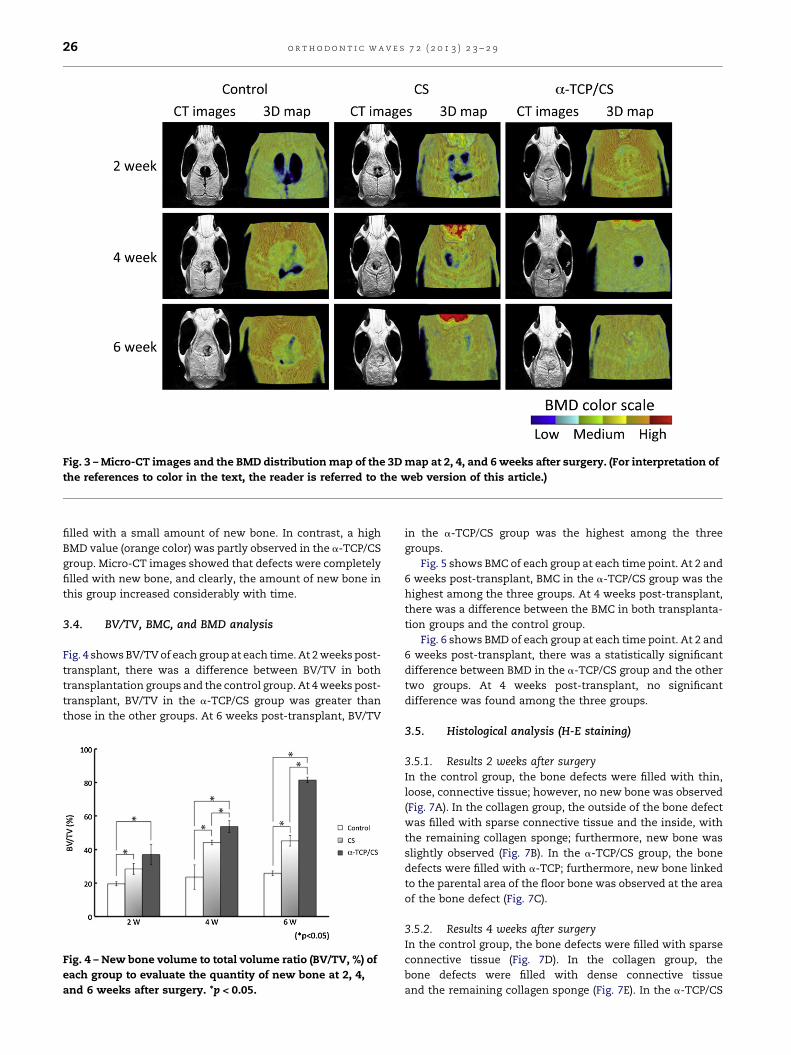
3.3. Three-dimensional color mapping (3D map) andmicro-CT examination
Fig. 3 shows a representative BMD distribution map of the 3D
map and micro-CT images of bone regeneration. Each model
was analyzed at three time points: 2, 4, and 6 weeks after
surgery. The 3D map shows the BMD at these time points. The
[(Fig._2)TD$FIG]Fig. 2 – SEM photographs of CS (A) and a-TCP/CS (B), where the a
porous a-TCP granules. Original magnification is 200T.
BMD color scale is as follows: red and orange = high BMD,
yellow and green = medium BMD, and light blue and pur-
ple = low BMD.
3.3.1. Results 2 weeks after surgeryA low BMD value (purple color) was observed in the control and
collagen groups. Micro-CT images showed that defects were
unfilled with new bone in both groups. In contrast, a low-to-
medium BMD value (green color) was observed in the a-TCP/
CS group. Micro-CT images showed that defects were filled
with a small amount of new bone.
3.3.2. Results 4 weeks after surgeryA low BMD value (purple color) was observed in the control
and collagen groups. In the control group, micro-CT images
showed that defects were unfilled with new bone. In the
CS group, more bone repair was observed compared
with the control group. In contrast, a medium BMD value
(yellow color) was observed in the a-TCP/CS group. Micro-CT
images showed that defects were filled with many hard
tissues.
3.3.3. Results 6 weeks after surgeryA low BMD value (purple color) was observed in the control and
collagen groups. Micro-CT images showed that defects were
rrow and asterisk respectively indicate collagen fibrils and
[(Fig._3)TD$FIG]
Fig. 3 – Micro-CT images and the BMD distribution map of the 3D map at 2, 4, and 6 weeks after surgery. (For interpretation of
the references to color in the text, the reader is referred to the web version of this article.)
o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 926
filled with a small amount of new bone. In contrast, a high
BMD value (orange color) was partly observed in the a-TCP/CS
group. Micro-CT images showed that defects were completely
filled with new bone, and clearly, the amount of new bone in
this group increased considerably with time.
3.4. BV/TV, BMC, and BMD analysis
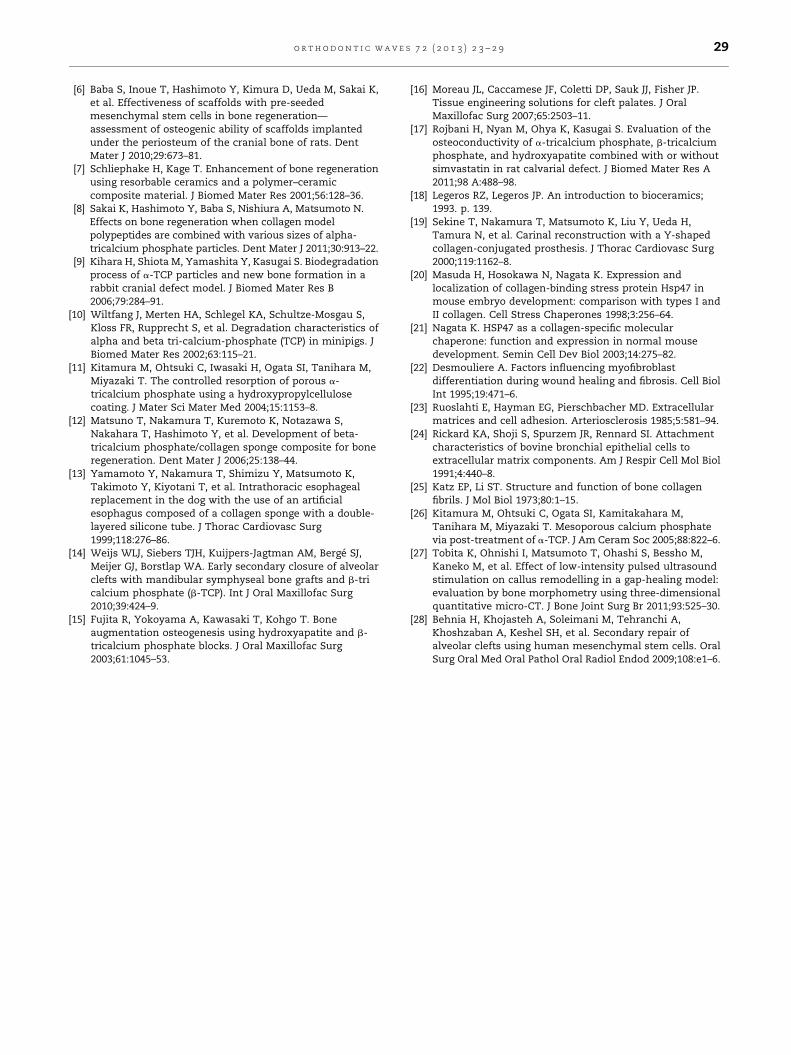
Fig. 4 shows BV/TV of each group at each time. At 2 weeks post-
transplant, there was a difference between BV/TV in both
transplantation groups and the control group. At 4 weeks post-
transplant, BV/TV in the a-TCP/CS group was greater than
those in the other groups. At 6 weeks post-transplant, BV/TV
[(Fig._4)TD$FIG]Fig. 4 – New bone volume to total volume ratio (BV/TV, %) of
each group to evaluate the quantity of new bone at 2, 4,
and 6 weeks after surgery. *p < 0.05.
in the a-TCP/CS group was the highest among the three
groups.
Fig. 5 shows BMC of each group at each time point. At 2 and
6 weeks post-transplant, BMC in the a-TCP/CS group was the
highest among the three groups. At 4 weeks post-transplant,
there was a difference between the BMC in both transplanta-
tion groups and the control group.
Fig. 6 shows BMD of each group at each time point. At 2 and
6 weeks post-transplant, there was a statistically significant
difference between BMD in the a-TCP/CS group and the other
two groups. At 4 weeks post-transplant, no significant
difference was found among the three groups.
3.5. Histological analysis (H-E staining)
3.5.1. Results 2 weeks after surgeryIn the control group, the bone defects were filled with thin,
loose, connective tissue; however, no new bone was observed
(Fig. 7A). In the collagen group, the outside of the bone defect
was filled with sparse connective tissue and the inside, with
the remaining collagen sponge; furthermore, new bone was
slightly observed (Fig. 7B). In the a-TCP/CS group, the bone
defects were filled with a-TCP; furthermore, new bone linked
to the parental area of the floor bone was observed at the area
of the bone defect (Fig. 7C).
3.5.2. Results 4 weeks after surgeryIn the control group, the bone defects were filled with sparse
connective tissue (Fig. 7D). In the collagen group, the
bone defects were filled with dense connective tissue
and the remaining collagen sponge (Fig. 7E). In the a-TCP/CS

[(Fig._5)TD$FIG]
Fig. 5 – BMC (mg) of each group to evaluate the quantity of
new bone at 2, 4, and 6 weeks after surgery. *p < 0.05.[(Fig._6)TD$FIG]
Fig. 6 – BMD (mg/cm3) of each group to evaluate the
strength of new bone at 2, 4, and 6 weeks after surgery.
*p < 0.05.
o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 9 27
group, a-TCP inside the bone defect was decreased compared
with that in week 2. Furthermore, the remaining a-TCP was
found, and new bone was formed surrounding the a-TCP
(Fig. 7F).[(Fig._7)TD$FIG]
Fig. 7 – Histological micrographs of HE-stained sections from ea
magnification: 100T. Scale bars: 200 mm. NB, new bone; CT, conn
3.5.3. Results 6 weeks after surgeryIn the control group, most parts of the bone defects were filled
with connective tissue; a small amount of new bone was
observed (Fig. 7G). In the collagen group, new bone that was
not continuous along the original bone was observed (Fig. 7H).
In the a-TCP/CS group, a-TCP was completely substituted by
bone and matured bone was recognized over the entire bone
defect (Fig. 7I).
4. Discussion
At present, autologous bone is the preferred material used for
the closure of osseous defects in the alveolar process [14,15].
However, harvesting an autologous bone graft involves several
disadvantages. Donor site morbidity after bone graft harvest
remains a recognized limitation in the reconstruction of the
cleft primary palate [16]. In this study, we fabricated a
biodegradable sponge composite for bone regeneration by
combining porous a-TCP and collagen sponge. a-TCP/CS can
be easily cut with scissors or a sharp knife, and therefore, it
can be easily molded for use for alveolar bone augmentation.
We evaluated its effects on bone regeneration after implanta-
tion into rat calvarial defects.
Many studies have investigated the use of calcium
phosphate as a bone graft material because of its good
biocompatibility [9]. The in vivo degradation rate of TCP is
higher than that of HA. a-TCP dissolves more easily in water
than b-TCP even though they have exactly the same
chemical composition [17]. Furthermore, a-TCP has a higher
dissolution rate in solutions with low pH values [18]. The
collagen used in this study was dissolved in HCl aqueous
solution at pH 3. In addition, porous a-TCP was used
to fabricate the composite scaffold. However, the XRD
pattern of a-TCP/CS was not particularly different from that
of a-TCP.
Collagen sponge works well as a scaffold matrix for tissue
regeneration [19]. Collagen is the most abundant macromole-
cule in the body, and its molecular structures are very similar
across animal species. Collagen exists as an extracellular
ch group at 2, 4, and 6 weeks after surgery. Original
ective tissue; TCP, a-TCP particles/CS; CS, collagen sponge.

o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 928
matrix in various tissues. During development and regenera-
tion processes [20–24], the highly ordered structure of collagen
plays an important role in various biological events in the
body. One example is the calcification process in bone tissue
[25].
In our previous study [12], we have shown that the stress
values of b-TCP/CS (0.2 g/mL) were significantly greater than
those of b-TCP/CS (0.1, 0.05, and 0.02 g/mL) over the entire
strain range through compression testing. In particular, the
initial Young’s modulus of b-TCP/CS (0.2 g/mL) differed
significantly from those of the other three composites. In this
study, a composite sponge was not molded because there were
too many granules at a 0.2 g/mL mixing concentration of a-
TCP and the atelocollagen solution. Thus, the optimal mixing
concentration of a-TCP and the atelocollagen solution was
decided as 0.15 g/mL.
The TCP’s porous body gradually dissolves away from bone
defects during bone repair, allowing for its substitution by
regenerated bone [26]. Such a bioabsorbable ceramic with
macropores is attractive for use as a bone filler in medical
applications because its porous structure allows cell invasion
[26]. However, the solubility of porous a-TCP might be higher
than that of the original a-TCP, making it liable to be
completely resorbed in the body before a bone defect can be
repaired by bone regeneration. Kitamura et al. [11] demon-
strated that the dissolution rate of porous a-TCP could be
reduced by coating it with an organic polymer; their in vivo
evaluation showed that such a coating is effective for
controlling the degradation rate of implanted a-TCP. In this
study, we expect that the mixture of porous a-TCP and
collagen will be similarly effective.
Micro-CT has a high resolution and uses very thin slices. A
larger number of slices means that the spatial differences
within areas of the specimen become negligible [27]. The
geometrical properties of the healing bone can be acquired
along with the spatial distribution of BMD by simultaneous
scans of a calibration phantom using micro-CT [27]. The BMD
distribution map may be useful for evaluating the regenera-
tion of new bone. We selected the BV/TV, BMD, and BMC of
mineralized tissue comprising the bone quality as the
denominator along with the bone volume. In our study,
micro-CT analysis showed that BV/TV and BMD in the a-TCP/
CS group was highest at 2–6 weeks and BMC was the highest
among the three groups at 4–6 weeks post-transplant. On the
other hand, BMD in the CS group showed no significant
difference compared with the control group at all weeks post-
transplant. The bone quantity and quality of the experimental
group had increased considerably compared with that of the
CS group. These results suggested that porous a-TCP promot-
ed new bone formation, and the use of only CS might not
promote an increase in bone quantity.
With regard to the biodegradability of the atelocollagen,
collagen sponge was almost completely degraded at 4 weeks
after implantation in the CS and a-TCP/CS groups. However,
CS was replaced only by soft connective tissue and not by
completely newly formed bone. In contrast, a-TCP/CS was
replaced by a network of newly formed bone. Furthermore, the
remaining a-TCP granules observed after 4 weeks were in
direct contact with the newly formed bone. Osteogenic
progenitor cells migrated from the adjacent bone edge or
bottom, adhered to the surface of the a-TCP granules, and
subsequently formed new bone [12]. In addition, porous a-TCP
often shows early absorption before adequate bone replace-
ment has occurred. The atelocollagen composite should
effectively control the degradation rate of the porous a-TCP
implant. A continuous, thick, lamellar structural bone was
formed at the top of the defect 4–6 weeks after operation in the
a-TCP/CS group. These observations indicated that the a-TCP/
CS composites supported bone regeneration, including lamel-
lar and trabecular bone formation and remodeling.
The reconstruction of alveolar cleft defects is a well-
established procedure, with the most widely applied approach
being secondary alveolar cleft osteoplasty. Successful grafting
allows eruption of teeth into the former cleft area and further
orthodontic expansion of a typically collapsed maxilla [28].
Biomaterials for bone grafting are required to possess
sufficient mechanical strength to sustain their shape until
they are replaced by newly formed bone. The morphology of
bony defects in cleft lip and palate is usually complicated, and
therefore, it is typically difficult to adapt the shape that is to be
fitted into a bone defect. However, the proposed a-TCP/CS
composite can be easily cut with scissors or a sharp knife, and
therefore, it can be easily molded for use such as alveolar bone
augmentation.
In conclusion, this study demonstrated that composites
created using porous a-TCP granules and collagen sponges
were sufficiently adaptable for treating bone defects.
Furthermore, the biodegradable a-TCP/CS was replaced by
newly formed bone without any adverse responses. There-
fore, this newly developed type of sponge composite may be
useful for bone tissue engineering. The clinical application
of a-TCP/CS as bone graft materials for alveolar cleft defects
should be successful. Further studies of bone regeneration
will be required in an alveolar cleft defect model in a larger
animal.
Acknowledgments
The authors express their sincere gratitude to Taihei Chemical
Industrial Co., Ltd. (Osaka, Japan), for providing the a-TCP
particles. The authors also thank Ratoc System Engineering
Co., Ltd. (Tokyo, Japan).
r e f e r e n c e s
[1] Amanat N, Langdon JD. Secondary alveolar bone grafting inclefts of the lip and palate. J Craniomaxillofac Surg1991;19:7–14.
[2] Murray JC. Face facts: genes, environment, and clefts. Am JHum Genet 1995;57:227–32.
[3] Jansen RG, van Kuppevelt TH, Daamen WF, Kuijpers-Jagtman AM, Von den Hoff JW. Interferon-g-loaded collagenscaffolds reduce myofibroblast numbers in rat palatalmucosa. Eur J Orthod 2011;33:1.
[4] Panetta NJ, Gupta DM, Slater BJ, Kwan MD, Liu KJ, LongakerMT. Tissue engineering in cleft palate and other congenitalmalformations. Pediatr Res 2008;63:545–51.
[5] Cohen M, Polley JW, Figueroa AA. Secondary (intermediate)alveolar bone grafting. Clin Plast Surg 1993;20:691–705.
o r t h o d o n t i c w a v e s 7 2 ( 2 0 1 3 ) 2 3 – 2 9 29
[6] Baba S, Inoue T, Hashimoto Y, Kimura D, Ueda M, Sakai K,et al. Effectiveness of scaffolds with pre-seededmesenchymal stem cells in bone regeneration—assessment of osteogenic ability of scaffolds implantedunder the periosteum of the cranial bone of rats. DentMater J 2010;29:673–81.
[7] Schliephake H, Kage T. Enhancement of bone regenerationusing resorbable ceramics and a polymer–ceramiccomposite material. J Biomed Mater Res 2001;56:128–36.
[8] Sakai K, Hashimoto Y, Baba S, Nishiura A, Matsumoto N.Effects on bone regeneration when collagen modelpolypeptides are combined with various sizes of alpha-tricalcium phosphate particles. Dent Mater J 2011;30:913–22.
[9] Kihara H, Shiota M, Yamashita Y, Kasugai S. Biodegradationprocess of a-TCP particles and new bone formation in arabbit cranial defect model. J Biomed Mater Res B2006;79:284–91.
[10] Wiltfang J, Merten HA, Schlegel KA, Schultze-Mosgau S,Kloss FR, Rupprecht S, et al. Degradation characteristics ofalpha and beta tri-calcium-phosphate (TCP) in minipigs. JBiomed Mater Res 2002;63:115–21.
[11] Kitamura M, Ohtsuki C, Iwasaki H, Ogata SI, Tanihara M,Miyazaki T. The controlled resorption of porous a-tricalcium phosphate using a hydroxypropylcellulosecoating. J Mater Sci Mater Med 2004;15:1153–8.
[12] Matsuno T, Nakamura T, Kuremoto K, Notazawa S,Nakahara T, Hashimoto Y, et al. Development of beta-tricalcium phosphate/collagen sponge composite for boneregeneration. Dent Mater J 2006;25:138–44.
[13] Yamamoto Y, Nakamura T, Shimizu Y, Matsumoto K,Takimoto Y, Kiyotani T, et al. Intrathoracic esophagealreplacement in the dog with the use of an artificialesophagus composed of a collagen sponge with a double-layered silicone tube. J Thorac Cardiovasc Surg1999;118:276–86.
[14] Weijs WLJ, Siebers TJH, Kuijpers-Jagtman AM, Berge SJ,Meijer GJ, Borstlap WA. Early secondary closure of alveolarclefts with mandibular symphyseal bone grafts and b-tricalcium phosphate (b-TCP). Int J Oral Maxillofac Surg2010;39:424–9.
[15] Fujita R, Yokoyama A, Kawasaki T, Kohgo T. Boneaugmentation osteogenesis using hydroxyapatite and b-tricalcium phosphate blocks. J Oral Maxillofac Surg2003;61:1045–53.
[16] Moreau JL, Caccamese JF, Coletti DP, Sauk JJ, Fisher JP.Tissue engineering solutions for cleft palates. J OralMaxillofac Surg 2007;65:2503–11.
[17] Rojbani H, Nyan M, Ohya K, Kasugai S. Evaluation of theosteoconductivity of a-tricalcium phosphate, b-tricalciumphosphate, and hydroxyapatite combined with or withoutsimvastatin in rat calvarial defect. J Biomed Mater Res A2011;98 A:488–98.
[18] Legeros RZ, Legeros JP. An introduction to bioceramics;1993. p. 139.
[19] Sekine T, Nakamura T, Matsumoto K, Liu Y, Ueda H,Tamura N, et al. Carinal reconstruction with a Y-shapedcollagen-conjugated prosthesis. J Thorac Cardiovasc Surg2000;119:1162–8.
[20] Masuda H, Hosokawa N, Nagata K. Expression andlocalization of collagen-binding stress protein Hsp47 inmouse embryo development: comparison with types I andII collagen. Cell Stress Chaperones 1998;3:256–64.
[21] Nagata K. HSP47 as a collagen-specific molecularchaperone: function and expression in normal mousedevelopment. Semin Cell Dev Biol 2003;14:275–82.
[22] Desmouliere A. Factors influencing myofibroblastdifferentiation during wound healing and fibrosis. Cell BiolInt 1995;19:471–6.
[23] Ruoslahti E, Hayman EG, Pierschbacher MD. Extracellularmatrices and cell adhesion. Arteriosclerosis 1985;5:581–94.
[24] Rickard KA, Shoji S, Spurzem JR, Rennard SI. Attachmentcharacteristics of bovine bronchial epithelial cells toextracellular matrix components. Am J Respir Cell Mol Biol1991;4:440–8.
[25] Katz EP, Li ST. Structure and function of bone collagenfibrils. J Mol Biol 1973;80:1–15.
[26] Kitamura M, Ohtsuki C, Ogata SI, Kamitakahara M,Tanihara M, Miyazaki T. Mesoporous calcium phosphatevia post-treatment of a-TCP. J Am Ceram Soc 2005;88:822–6.
[27] Tobita K, Ohnishi I, Matsumoto T, Ohashi S, Bessho M,Kaneko M, et al. Effect of low-intensity pulsed ultrasoundstimulation on callus remodelling in a gap-healing model:evaluation by bone morphometry using three-dimensionalquantitative micro-CT. J Bone Joint Surg Br 2011;93:525–30.
[28] Behnia H, Khojasteh A, Soleimani M, Tehranchi A,Khoshzaban A, Keshel SH, et al. Secondary repair ofalveolar clefts using human mesenchymal stem cells. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e1–6.