-
ORIGINAL ARTICLE
Evaluation of Next Generation Sequencing for Detecting HER2
CopyNumber in Breast and Gastric Cancers
Dongfeng Niu1 & Lei Li2 & Yang Yu2 & Wanchun Zang2
& Zhongwu Li1 & Lixin Zhou1 & Ling Jia1 & Guanhua
Rao2 &Lianju Gao2 & Gang Cheng2 & Ke Ji3 & Dongmei
Lin1
Received: 25 May 2020 /Accepted: 10 June 2020# The Author(s)
2020
AbstractAmplicon-based next generation sequencing (NGS)
approaches have been preferentially adopted by the clinical
laboratories onthe basis of a short turnaround time (TAT) and small
DNA input needs. However, little work has been done to assess
theamplicon-based NGS methods for copy number variation (CNV)
detection in comparison with current standard methods
likeimmunohistochemistry (IHC) and fluorescence in situ
hybridization (FISH). The correlation between NGS based CNV
detectionand the later standard methods has remained unexplored. We
developed an amplicon-based panel to detect human epidermalreceptor
growth factor (HER2) amplification in formalin-fixed
paraffin-embedded (FFPE) tumor tissue samples from 280 breastcancer
and 50 gastric cancer patients. Assessment by IHC and FISH was
conducted in parallel, and descriptive statistics wereused to
assess the concordance. The copy number detected by NGS was
correlated with either the average HER2 copy number(signals/cell)
(r = 0.844; p < 0.001) or the HER2/CEP17 ratio (r = 0.815; p
< 0.001). We determined a cut-off value for NGS tocategorize
HER2 amplification status by using 151 HER2 non-amplified FFPE
samples. In breast cancer patients, the cut-offvalue was 2.910,
with 95.35%, 98.67% and 97.29% sensitivity, specificity and
concordance, respectively. However, this cut-offvalue displayed low
sensitivity in gastric cancer patients (64.71%), and the following
macrodissection procedure was noteffective for increasing
sensitivity (57.14%). Evaluation of HER2 copy number with NGS in
our study was comparable withIHC and FISH in breast cancer
patients, but concordance in gastric cancer was only moderate. The
greater discordance in gastriccancer may reflect the underlying
biological mechanisms, and further study is warranted. NGS-based
HER2 assessment maydecrease the equivocal HER2 determinations in
breast cancer patients assessed by FISH/IHC.
Keywords Next generation sequencing .HER2 amplification . Breast
cancer . Gastric cancer . FISH/IHC
Background
The reliable identification of clinically actionable
genomicalteration method is critical for the precision cancer
thera-py guidance. Next generation sequencing (NGS) has
thecapability to simultaneously assess multiple genes with alimited
biopsy material, thus representing both a cost andtissue-efficient
alternative to current single-gene assess-ment methods [1–3]. Prior
studies have shown that NGSenables a reliable detection for copy
number variations(CNV) from the same assays used to detect sequence
alter-ations, but less information is available on
amplicon-basedtarget sequences [4–7]. CNV calling in the amplicon
se-quence relies on the calculation of amplicon coverage
andsuitable normalization. Several factors influence CNV
de-tection, including the number of amplicons per gene, aver-age
read dept., and tumor purity within the sample [7].
Dongfeng Niu, Lei Li and Yang Yu contributed equally to this
work.
Electronic supplementary material The online version of this
article(https://doi.org/10.1007/s12253-020-00844-w) contains
supplementarymaterial, which is available to authorized users.
* Ke [email protected]
* Dongmei [email protected]
1 Department of Pathology, Key laboratory of Carcinogenesis
andTranslational Research (Ministry of Education), Peking
UniversityCancer Hospital & Institute, Beijing, China
2 Beijing Novogene Bioinformatics Technology Co., Ltd,Beijing,
China
3 Department of Gastrointestinal Surgery, Key laboratory
ofCarcinogenesis and Translational Research (Ministry of
Education),Peking University Cancer Hospital & Institute,
Beijing, China
https://doi.org/10.1007/s12253-020-00844-w
/ Published online: 3 July 2020
Pathology & Oncology Research (2020) 26:2577–2585
http://crossmark.crossref.org/dialog/?doi=10.1007/s12253-020-00844-w&domain=pdfhttps://doi.org/10.1007/s12253-020-00844-wmailto:[email protected]:[email protected]
-
Thus, an assay and algorithm shall need to be fully vali-dated
before being clinically used.
Human epidermal receptor growth factor (HER2) amplifi-cation or
an overexpression occurs in approximately 18–20%of breast cancers,
and in nearly 20% of gastric or gastroesoph-ageal junction (GEJ)
cancers [8, 9]. Several methods havebeen recommended for HER2
amplification assessment, in-cluding in situ hybridization (ISH)
techniques, which evaluateHER2 status by measuring the number of
HER2 gene copies,or IHC, which quantifies protein expression [9].
The ASCO/CAP has provided detailed guidelines for conducting
andinterpreting HER2 status in a clinical practice. These
scoringmethods classify cases into “positive”, “negative”,
and“equivocal” categories [10]. According to these
guidelines,equivocal HER2 status necessitates additional testing,
thusincreasing the cost of patient management, and delaying
thedecision to recommend HER2-targeted therapy. The correla-tion
between a copy number called by NGS with an averageHER2 copy
number, HER2/CEP17 ratio, or IHC score is notwell established. With
increasing NGS use in a clinical prac-tice it is increasingly
important to validate the amplicon-baseddetection method against
the standard methodologies.
In the current study, we performed and evaluated
anamplicon-based NGS assay to assess HER2 amplification inbreast
and gastric cancers, by using a custom designed paneland
bioinformatics pipeline. We evaluated accuracy and con-cordance of
NGS detection compared with the gold-standardFISH/IHC analysis
methodologies.
Materials and Methods
Study and Panel Design
For CNV detection, we designed an amplicon-based panelcovering
50 genes, which included 13 CNV genes and 6 base-line genes
(supplement Tables 1, 2). Briefly, we used cell lineswith known
amplifications for validating accuracy and hadgreat precision for
copy number detection. Then, it was ex-panded to the FFPE samples
from both the breast and gastriccancer patients. We further
compared the copy number detect-ed by NGS with the FISH/IHC results
from the same sample,and determined a cut-off value of NGS to
determine HER2status. The study schema is summarized in the
supplementaryFig. 1.
Cell Line CNV Detection
To validate CNV detection, we pooled four cell lines,
eachbearing single focal gene amplification (HER2, MET, EGFRand
FGFR3) with the matched normal cell lines (GM18511)in several
dilution series (40%, 30%, 25%, 20%, 15%, 10%,5%, 4.5%, 3%). The
standard materials list is shown in
supplementary Table 3. For orthogonal support, the copynumber of
the molecular standard materials were also mea-sured by digital PCR
using the QuantStudio 3D digital PCRsystem (Life Technology, CA,
USA).
Patients and Samples
To verify our custom designed 50 gene panel in clinical
ap-plication, we used FFPE samples from 280 invasive breastcancer
patients and 50 gastric cancer patients obtained fromPeking
University Cancer Hospital. Five FFPE slides, each5-μm thick, were
obtained from breast cancer patient samplesalong with ten FFPE
slides from gastric cancer. Tumors with ahigh degree of necrosis
and < 1000 tumor cells were excluded.More than 80% of the
samples we finally selected were sam-ples with tumor purity greater
than 20%. This study was ap-proved by theMedical Ethics Committee
of PekingUniversityCancer Hospital, and the investigation was
performed in ac-cordance with the Declaration of Helsinki
Principles. All pa-tients had signed informed consent for the
tissue research, andall of clinical data and samples were
deidentified prior to anal-ysis. All the experiments were carried
out in accordance withthe guideline released by the National Health
and FamilyPlanning Commission of the PRC.
DNA Extraction
Genomic DNA was extracted from unstained FFPE samplesusing
TIANamp FFPE DNA Kit (TIANGEN, Beijing,China), according to
manufacturer’s instructions. DNA wasquantified using the Qubit
dsDNA HS Assay Kit (LifeTechnology, CA, USA) and the Qubit 2.0
Flurometer (LifeTechnology, CA, USA) according to recommended
protocols.Quality checks were performed by testing 5 ng DNA in
1%agarose gel electrophoresis. Samples in which the main DNAstrip
in agarose gel electrophoresis less than 600 bp wereexcluded. The
DNA was stored at −20 °C.
NGS Library Preparation
Sequence libraries were prepared by using library
preparationreagents from Life Technology, CA, USA. The amount ofDNA
input was 15 ng. Libraries were constructed using acustom designed
panel (50 hotspot genes). Then, theamplicons by Ion Ampliseq
Library Kit 2.0 were barcodedduring library generation using the
Ion Xpress BarcodeAdapters 1–96 Kit. The libraries were purified by
AMPureXP beads, quantified using the Ion Library Quantitation
Kit,and qualified using Agilent Bioanalyzer 2100. Then the
librar-ies were pooled for sequencing. Multiplex barcoded
librarieswere enriched by clonal amplification using emulsion PCR
onIon Sphere particles (Ion PI™ Template OT2 200 Kit v3,
LifeTechnology, CA, USA) and loaded on an Ion PI™ Chip.
2578 D. Niu et al.
-
Massively parallel sequencing was carried out on Ion
Protonplatform using the Ion PI™ Sequencing 200 Kit v3 accordingto
manufacturer’s instructions.
Sequencing and Data Analysis
Torrent Suite Software (version 4.4.3) was used to performsignal
processing, base calling, quality score assignment, andadapter
trimming after the sequencing reaction. High qualityreads were
aligned to human genome 19 reference bytmap4.2.18 software. Quality
control and coverage analysiswas performed by an in-house analysis
pipeline.
Base Substitution, Short Insertion and DeletionAnalysis
TVC (Torrent Variant Caller, version 4.4) was used to callSNV
and InDel variants. TVC modules use freebayes to dis-cover
candidate variants combined with the hotspots file fordetecting
genemutations. Somatic mutations were determinedusing the following
filters: (i) the minimum coverage depthwas 100 for SNP and 200 for
InDel; (ii) theminimum cutoff ofMAF was 0.01 for hotspot variants
and 0.05 for others; (iii)detected SNVs and InDels also required at
least 25 variant-contained reads to be reported as positive. Those
combinedminimum coverage, MAF and variant-contained reads to
en-sure the accuracy of variant calls.
Copy Number Variation Detection
We used an exome-like approach, rather than the averagecoverage
of exon pull-down regions with read counts peramplicon, for
identifying CNV. The coverage of eachamplicon was calculated as the
number of reads which cov-ered more than one amplicon but mostly
aligned to theamplicon. Then, the amplicon-level coverage was
divided bythe median coverage of each amplicon to normalize or
mini-mize inter-sample variation. The normalized
amplicon-levelcoverage was also corrected by GC content to remove
thedependency of coverage across the different GC
profiles.Amplicons with a coverage of less than 100 × were
excludedfrom analysis. The copy number ratio of each amplicon
wascalculated by dividing the GC corrected amplicon-level cov-erage
of tumor samples with that of the matched normal sam-ple or normal
pool. In this study, we used a normal poolderived from 14 normal
breast cancer patient FFPE samplesinstead of the matched normal
sample for a reference of dip-loid genome comparison. The copy
number ratio was thenlog-transformed to yield the log2 copy number
ratio, whichwas subsequently used to determine gene amplification
status.The gene level fold change was determined as the
weightedaverage of amplicon-level log-copy number ratios, for
whichthe weight of each amplicon was proportional to the number
of reads; basically, the reads in the matched normal samples
orthe normal pool. The final copy number of gene was equal totwice
the gene level fold change.
HER2 IHC and FISH Testing
HER2 amplification was determined by IHC and the dualprobe FISH
test. FISH results were reported as averageHER2 copy number and
HER2/CEP17 ratio. All FFPE sam-ples were reviewed by two individual
pathologists to deter-mine HER2 status.
Statistics
The accuracy (sensitivity and specificity) and precision
(re-peatability and reproducibility) of NGS was evaluated
withstandard material result. The correlations of the copy
numbercalled by NGS and that determined by digital PCR were
stud-ied by using R software. Comparisons of copy numbers whichwere
detected in the three runs, were analyzed using theANOVA test.
Results
Assay Performance of NGS Calls in Standard Materials
The NGS assay performance for detecting CNVwas analyzedby
detecting standard materials. The copy number of standardmaterials
is summarized in Supplementary Table 3. The pre-cision was assessed
in inter-assay and intra-assay studies. Wefirst simultaneously ran
the two libraries which had been pre-pared by two different
operators (Lib1 and Lib3). Then, Lib1was done on another run
(Lib2), yielding a total of 3 replicatesfor each sample. Then, it
was repeatability evaluated on a per-gene basis among the
replicates. Each gene had also a similarcopy number estimation in
the replicated libraries (Fig. 1). Nostatistical differences in the
copy number could be detectedamong the three runs (F-value = 0.022,
P value = 0.9783).The coefficient of variation (CV%) for the
variation in copynumber was
-
tumor purity than those with a low CNV (Fig. 2b).
Subsequentanalyses were focused specifically on HER2 detection.
Distribution of HER2 Amplification Status in BreastCancer
All the 280 FFPE samples from breast cancer patients weretested
using FISH and IHC for establishing the HER2 ampli-fication status.
The IHC results showed that 31.4% (88/280)
scored as IHC 3+, 185 as IHC 2+ and 7 as IHC 1+. Thespecimens
were then tested by FISH, except for one IHC 2+sample and one IHC
3+ sample, for which testing had failed.FISH results were 100%
consistent with IHC for 1+ and 3+samples. For 184 IHC 2+ samples, a
total of 121 negativesamples, 63 positive samples. Two pathologists
reviewedthese histologic findings, and ranked 143 samples as
negativeand 41 samples as positive. Overall, this led to 129
positivesamples, 151 negative samples.
Fig. 2 The correlation analysis of CNV detection by preparing
libraries. aCurve regression analysis between copy number detected
by NGS anddigital PCR. The copy number detected by digital PCR was
used asexpected copy number. The copy number detected by NGS was
used asdetected copy number. b The effect of tumor purity on the
detection limit
for gene amplifications. Four cell lines each bearing single
focal geneamplification (HER2, MET, EGFR and FGFR3) were pooled
with theirmatched normal cell lines in several dilution series.
Detection limits wereevaluated with dilution series
Fig. 1 Repeatability of copynumber variation detection.
NGS-based CNV detections were ana-lyzed using standard materialsand
replicated libraries
2580 D. Niu et al.
-
Determination and Evaluation of Cut-off toCategorize the HER2
Status in Breast Cancer UsingNGS
After the validation in the cell lines, we implemented
CNVdetection in large scale clinical FFPE specimens. The
NGS-detected copy number was correlated with the FISH results(Fig.
3). To assess the sensitivity for detecting CNV whencompared to the
gold-standard method, we evaluated thequantitative correlation
between NGS and the average HER2copy number or HER2/CEP17 ratio
detected by FISH. Weused a total of 255 samples to fit a linear
regression modelof NGS copy number and the FISH testing
results(Supplementary Table 5), excluding those with FISH
testingfailure (n = 3),HER2 status reviewed by pathologists (n =
22).The log10 copy number detected by NGS correlated witheither the
log10 average HER2 copy number (signals/cell)(y = 0.044 + 0.73x, r
= 0.844; add p < 0.001), and log10
HER2/CEP17 ratio (y = 0.26 + 0.74x, r = 0.815; addp < 0.001).
As NCCN guideline considered average copynumber of HER2 ≥ 6.0
signals/cell as positive, if the averagecopy number is 6 then the
NGS copy number is 4.09 accord-ing to this equation. Similarly, if
the average copy number is4, the NGS copy number will be 3.04, and
if theHER2/CEP17ratio is set as 2, the NGS copy number will be
3.03. No false-positive or false-negative samples were found when
the copynumber detected by NGS was >4.09. This value was
henceidentified as the confident positive cut-off.
To determine the negative cut-off value, we used 151HER2
negative samples to represent the copy number distri-bution in HER2
negative samples. The copy number datafollowed a normal
distribution (P value of Shapiro-Wilk test =0.0539). We then used
the mean + 3 ×MAD (mean absolutedeviation) as the negative cut-off
value (Supplementary Fig.2). Two false-positive sample was found
when the copy num-ber ranged between 2.91 and 4.09, and five
false-negative
Fig. 3 Amplicon-based NGS to detect CNV from breast
cancerspecimens identified by IHC and FISH. Representative
microscopicalresults of HER2 amplification (positive, negative and
equivocal HER2status) were shown by IHC (a, d, g) and dual color
FISH (b, e, h). FFPE
resection specimens with identified by FISH were further
analyzed byNGS (c, f, i). The y-axis shows log2 copy number ratios
of each ampliconfrom each gene
2581Evaluation of Next Generation Sequencing for Detecting HER2
Copy Number in Breast and Gastric Cancers
-
samples were observed when the copy number was 4.09 and <
2.91, and thecopy number between 2.91 and 4.09 as weak positive
status.Overall, we achieved a sensitivity of 95.35% (123/129) and
aspecificity of 98.67% (149/151) compared with HER2 status,which
was determined by two pathologists who consideredboth IHC and FISH
testing results in breast cancer (Table 1).
Classification of HER2 Equivocal Status Samples inBreast Cancer
Using NGS
Compared with the HER2 status by IHC score, all 7 IHC 1+samples
were classified as HER2-negative by NGS. Among88 IHC 3+ samples,
one (1/88) was identified to be negativeby NGS (copy number =
2.71). For 185 IHC 2+ samples,NGS had an 87.80% (36/41) sensitivity
and a 98.61% (142/144) specificity compared with HER2 status
determined bytwo pathologists after considering both IHC and FISH
testing.
Seven discrepancies were found, six of which had occurredin the
context of a lowered tumor content and HER2 hetero-geneity
(Supplementary Fig. 3). The average HER2 copynumber of these
samples was 10.6, 5.9, 5.1, 4.1, 13.48 and7.5, respectively. The
HER2/CEP17 ratio was 3.2, 2.9, 4.7,2.28, 6.1 and 4.4, respectively.
However, the copy number ofthese samples were < 2.91. All the
six specimens displayedhigh tumor heterogeneity, which was thought
to influenceNGS accuracy.
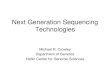
CNV Detection in Gastric Cancer Using NGS
A total number of 50 gastric cancer patients were enrolled
inthis study. In the initial 39 fully extracted FFPE samples,
NGSidentified 11 out of 17 HER2 positive samples, and all the
22HER2 negative samples. Although the positive predictive val-ue
(PPV) was 100%, NGS categorized all HER2 negativesamples correctly,
with a low sensitivity (64.71%, 11/17).Compared with breast cancer,
gastric cancer appeared to bemore heterogeneous. We hence decided
to evaluate whether amacrodissection based IHC result would help to
increase thesensitivity. There were 28 HER2 amplified samples
sequenced after macrodissection, and sensitivity was
57.14%(16/28). Although the NGS-detected copy number of mostsamples
increased after macrodissection (Fig. 4), it was notsufficient to
improve the accuracy of the NGS assay forHER2detection in gastric
cancer (Table 2).
Concurrent Detection of Other Somatic Alterations inthe Clinical
FFPE Samples
Overall, 118 breast cancer samples with at least one
genemutation detected were include in this study. The most com-mon
mutations were PIK3CA (109/280), TP53 (4/280), AKT1(3/280), KRAS
(3/280), HER2 (2/280), ALK (1/280), EGFR(1/280), and RET (1/280).
Among these mutations, annotatedbased on the OncoKb Knowledge Base
[11], PIK3CA, AKT1and HER2 mutations were labelled with a 3A
level(Compelling clinical evidence supports the biomarker as be-ing
predictive of response to a drug in this indication, butneither
biomarker nor drug are standard care).When assigningsamples to the
level of the most actionable alteration, 40.71%(114/280) patients
harbored at least one potentially actionablealteration, which may
be a response to a drug, although this isnot been defined as
standard care so far.
In gastric cancer, MSH3 was the most common mutation,occurring
in 74% (37/50) patients. The frequency of this mu-tation was higher
in gastric cancer without HER2 amplifica-tions (HER2-negative
patients: 91%, HER2-positive patients:61%; p = 0.036, Chi-square
test).
Discussion
HER2 amplification has both predictive and prognostic valuefor
breast cancer. Currently, it is regarded as the only biomark-er
established for selecting specific therapy for patients
withadvanced gastric cancer [12, 13]. The current
gold-standardapproach for assessing HER2 amplification status is
based onthe IHC and ISH techniques. However, debate continues
overthe best way to relate HER2 test results with treatment
out-comes. One drawback of the HER2 test is that the scoringsystem
used to determine HER2 status is subjective. In thisstudy, we
developed an amplicon-based NGS panel to accu-rately detect
clinically relevant copy number alterations.EvaluatingHER2 copy
number with NGS in our study yieldedcomparable results to the
gold-standard FISH/IHC analyses inbreast cancer patients, achieving
95.35% sensitivity and98.67% specificity.
The cell line dilution study showed that the detection
foramplification is strongly influenced by tumor purity. Asshown in
Fig. 2b, copy number was reduced in parallel withdecrease of tumor
purity. For example, the initial copy numberwas about 4 for FGFR1
at 80% tumor purity, whilst the copynumber was approximately 2.45
at 20% tumor purity. Thus, if
Table 1 Performance of NGS assay inHER2 amplification detection
inbreast cancer patients
Platform FISH Total Sensitivity Specificity Concordance
+ –
NGS + 123 2 125 95.35% 98.67% 97.14%
– 6 149 155
Total 129 151 280
2582 D. Niu et al.
-
the initial amplification level was low, it would not be
detect-able at a low tumor purity. Other studies also shown
thatsamples with poor quality or lowDNA content can yield noisyCN
plots, thus limiting accurate assessment. The performancewas also
affected with lower CNVs (6–7 copies) and in sam-ples with poor
purity (20–30%) [14]. Thus, determining ade-quate tumor purity
would be mandatory, for an accurate as-sessment. Furthermore, an
alternate method shall be recom-mended for cases with amplification
in combination with lowtumor content.
In addition to providing an accurate copy number, we alsoneed to
transfer the continuous copy number value into abinary
amplification status. In this study, we used known neg-ative
samples to determine the negative cut-off value of NGSand
established that 2.91 yielded a 95.35% sensitivity and98.67%
specificity when compared to the gold-standard meth-od. To be more
confident with NGS CNV detection, we usedthe established cut-off
value for FISH, to estimate a positivecut-off value of NGS
according to their correlation. It showedthat a copy number using
NGS higher than 4.09 corresponded
Fig. 4 Effect of macrodissection on HER2 detection by NGS in
gastriccancer. a Diagram showing macrodissection of FFPE tissue
area of HEstained section of gastric cancer. b Serial section from
the same specimen
for HER2 IHC. cHER2 FISH (red signal,HER2; green signal,CEP17).
dCNV detection by NGS after macrodissection. e CNV detection by
NGSbefore macrodissection
Table 2 Performance of NGSassay in HER2 amplificationdetection
in gastric cancer
Platform FISH Total Sen Spe Con PPV NPV
+ –
NGS Macro dissection + 16 0 16 57.14% – 57.14% 100% 0.00%– 12 0
12
Full extraction + 11 0 11 64.71% 100% 84.62% 100% 78.57%– 6 22
28
2583Evaluation of Next Generation Sequencing for Detecting HER2
Copy Number in Breast and Gastric Cancers
-
to an average HER2 copy number higher than 6 signs/cell.Thus, we
recommended an NGS copy number between 2.91and 4.09 to take an
additional reflex test. However, it could beforeseen that larger
validated samples would reduce thisgreyscale. In fact, our methods
derive a nearly identical cutoffto call HER2 amplificated by NGS as
the large commercialNGS provided Foundation Medicine, Inc. which
uses 4 NGS-derived copies to call amplification in HER2.
According to updated 2018 ASCO/CAP guideline, con-comitant IHC
assays are required to arrive at the most accurateHER2 status
designation after HER2 FISH equivocal results.Currently, our
research gave preliminary suggestions, whetherdual-probe ISH group
2 to 4 in 2018 ASCO/CAP guidelinecan be considered for inclusion in
the negative. NGS mightprovide accurate assessment for the HER2
status designation,and thus reduces the risk of misdiagnosis, and
further verifi-cation is required.
NGS still has some shortcomings for detection mutations,e.g.,
CNV detection accuracy was based on accuratelyassessing coverage
depth of genes, which can be biased byhigh GC content and
repetitive regions. A previous study re-ported that the number of
amplicons per gene on the panelmay influence performance of CNV
detection [7]. The highernumber of amplicons per gene would have
somehow de-creased the variance in CNV assessment, but it would
havealso restricted the list of assessable genes.
In some cases, metastatic tumors have different
molecularalterations from the primary tumors. Even in breast
cancer, adiscrepancy of HER2 status between primary tumor and
dis-tant metastases has been observed in 7–26% of patients
[15].Regarding gastric cancer, tumor heterogeneity could be
pre-cisely identified using ctDNA [16] or planning reflex testingon
residual materials or additional tumor blocks. Similar find-ings
have been reported in advanced gastric cancer patients,whose
primary tumors were found to be HER2 negative, butwhose circulating
tumor cells displayed HER2 amplification[17].
Conclusions
Our study demonstrate that an optimized NGS-based test
canaccurately detect most clinically targetable CNV in a
broadspectrum of cancer patients. NGS-based HER2 assessmentmay
decrease the equivocal HER2 determinations in breastcancer patients
assessed by FISH/IHC. However, due to het-erogeneity of gastric
cancer tumor tissue, detection of HER2amplification by NGS seems
still problematic in thismalignancy.
Acknowledgments We acknowledge all other studies that support
ourwork and were not cited due to length limitations.We would like
to thankall the patients who have participated in this study.We are
also thankful to
the doctors from departments of oncology, doctors from
departments ofpathology for technics and staff of the Novogene
Bioinformatics. Thisarticle has been edited by Jeremy Dean
Chapnick, English LanguageEditor, AME Publishing Company.
Availability of Data and Materials The datasets supporting the
conclu-sions of this article are included within the article and
additional files.
Authors’ Contributions Jiafu Ji, Dongmei Lin and Yang Yu
conceivedthe research idea and designed this study. Zhongwu Li,
Lixin Zhou andLing Jia performed sample collection. Yun Gao,
Donfeng Niu, Lei Li,Wanchun Zang and Lianju Gao analyzed and
interpreted data. All authorsparticipated in writing, review and
final approval of the manuscript.
Funding This study was funded by National Natural Science
Foundationof China (81472743).
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Peking
UniversityCancer Hospital (2014TW04), and written informed consent
was obtain-ed from all patients.
Competing Interests Lei Li, Wanchun Zang, Lianju Gao,
GuanhuaRao, Yun Gao, Gang Cheng and Yang Yu were employee
ofNovogene Bioinformatics Technology Co., Ltd., Beijing, China. No
po-tential conflicts of interest were disclosed by the other
authors. SJK hasreceived consulting/advisory fees from Lilly
Oncology, Astellas, BostonBiomedical and Foundation Medicine, Inc.
SJK has stock/equity in TPTherapeutics and receives institutional
research funding from Merck,Leap therapeutics, and Astellas
Pharmaceuticals.
Abbreviations NGS, next generation sequencing; CNV, copy
numbervariation; IHC, immunohistochemistry; FISH, fluorescence in
situ hy-bridization; HER2, human epidermal receptor growth factor;
FFPE, for-malin-fixed paraffin-embedded
Open Access This article is licensed under a Creative
CommonsAttribution 4.0 International License, which permits use,
sharing,adaptation, distribution and reproduction in any medium or
format, aslong as you give appropriate credit to the original
author(s) and thesource, provide a link to the Creative Commons
licence, and indicate ifchanges weremade. The images or other third
party material in this articleare included in the article's
Creative Commons licence, unless indicatedotherwise in a credit
line to the material. If material is not included in thearticle's
Creative Commons licence and your intended use is notpermitted by
statutory regulation or exceeds the permitted use, you willneed to
obtain permission directly from the copyright holder. To view acopy
of this licence, visit
http://creativecommons.org/licenses/by/4.0/.
References
1. Hirsch FR, Scagliotti GV, Mulshine JL, Kwon R, Curran WJ
Jr,Wu YL, Paz-Ares L (2017) Lung cancer: current therapies and
newtargeted treatments. Lancet 389(10066):299–311.
https://doi.org/10.1016/S0140-6736(16)30958-8
2. Rehm HL, Bale SJ, Bayrak-Toydemir P, Berg JS, Brown
KK,Deignan JL, Friez MJ, Funke BH, Hegde MR, Lyon E, WorkingGroup
of the American College of Medical G, GenomicsLaboratory Quality
Assurance C (2013) ACMG clinical laboratory
2584 D. Niu et al.
http://creativecommons.org/licenses/by/4.0/https://doi.org/10.1016/S0140-6736(16)30958-8https://doi.org/10.1016/S0140-6736(16)30958-8
-
standards for next-generation sequencing. Genet Med
15(9):733–747. https://doi.org/10.1038/gim.2013.92
3. Hamblin A, Wordsworth S, Fermont JM, Page S, Kaur K, CampsC,
Kaisaki P, Gupta A, Talbot D,MiddletonM, Henderson S, CuttsA,
Vavoulis DV, Housby N, Tomlinson I, Taylor JC, Schuh A(2017)
Clinical applicability and cost of a 46-gene panel for geno-mic
analysis of solid tumours: retrospective validation and
prospec-tive audit in the UK National Health Service. PLoS Med
14(2):e1002230. https://doi.org/10.1371/journal.pmed.1002230
4. Pfarr N, Penzel R, Endris V, Lier C, Flechtenmacher C,
VolckmarAL, Kirchner M, Budczies J, Leichsenring J, Herpel E, Noske
A,Weichert W, Schneeweiss A, Schirmacher P, Sinn HP, StenzingerA
(2017) Targeted next-generation sequencing enables reliable
de-tection of HER2 (ERBB2) status in breast cancer and
providesancillary information of clinical relevance. Gene
ChromosomeCancer 56(4):255–265.
https://doi.org/10.1002/gcc.22431
5. Yamamoto T, Shimojima K, Ondo Y, Imai K, Chong PF, Kira
R,Amemiya M, Saito A, Okamoto N (2016) Challenges in
detectinggenomic copy number aberrations using next-generation
sequenc-ing data and the eXome hidden Markov model: a clinical
exome-first diagnostic approach. Hum Genome Var 3:16025.
https://doi.org/10.1038/hgv.2016.25
6. Ellingford JM, Campbell C, Barton S, Bhaskar S, Gupta S,
TaylorRL, Sergouniotis PI, Horn B, Lamb JA, Michaelides M,
WebsterAR, Newman WG, Panda B, Ramsden SC, Black GC
(2017)Validation of copy number variation analysis for
next-generationsequencing diagnostics. Eur J Hum Genet
25(6):719–724. https://doi.org/10.1038/ejhg.2017.42
7. Grasso C, Butler T, Rhodes K, Quist M, Neff TL, Moore
S,Tomlins SA, Reinig E, Beadling C, Andersen M, Corless CL(2015)
Assessing copy number alterations in targeted, amplicon-based
next-generation sequencing data. J Mol Diagn
17(1):53–63.https://doi.org/10.1016/j.jmoldx.2014.09.008
8. Van Cutsem E, Bang YJ, Feng-Yi F, Xu JM, Lee KW, Jiao
SC,Chong JL, Lopez-Sanchez RI, Price T, Gladkov O, Stoss O, Hill
J,Ng V, Lehle M, Thomas M, Kiermaier A, Ruschoff J (2015)
HER2screening data from ToGA: targeting HER2 in gastric and
gastro-esophageal junction cancer. Gastric Cancer 18(3):476–484.
https://doi.org/10.1007/s10120-014-0402-y
9. Owens MA, Horten BC, Da Silva MM (2004) HER2
amplificationratios by fluorescence in situ hybridization and
correlation withimmunohistochemistry in a cohort of 6556 breast
cancer tissues.Clin Breast Cancer 5(1):63–69.
https://doi.org/10.3816/cbc.2004.n.011
10. Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu
PB,Bartlett JMS, Bilous M, Ellis IO, Fitzgibbons P, Hanna W,
JenkinsRB, Press MF, Spears PA, Vance GH, Viale G, McShane
LM,Dowsett M (2018) Human epidermal growth factor receptor 2
test-ing in breast cancer: American Society of Clinical
Oncology/College of American Pathologists Clinical Practice
GuidelineFocused Update. J Clin Oncol 36(20):2105–2122.
https://doi.org/10.1200/JCO.2018.77.8738
11. Chakravarty D, Gao J, Phillips SM, Kundra R, Zhang H, Wang
J,Rudolph JE, Yaeger R, Soumerai T, Nissan MH, Chang
MT,Chandarlapaty S, Traina TA, Paik PK, Ho AL, Hantash FM,Grupe A,
Baxi SS, Callahan MK, Snyder A, Chi P, Danila D,Gounder M, Harding
JJ, Hellmann MD, Iyer G, Janjigian Y,
Kaley T, Levine DA, Lowery M, Omuro A, Postow MA,Rathkopf D,
Shoushtari AN, Shukla N, Voss M, Paraiso E, ZehirA, Berger MF,
Taylor BS, Saltz LB, Riely GJ, Ladanyi M, HymanDM, Baselga J,
Sabbatini P, Solit DB, Schultz N (2017) OncoKB: aprecision oncology
Knowledge Base. JCO precision oncology2017.
https://doi.org/10.1200/PO.17.00011
12. Bartley AN, Washington MK, Colasacco C, Ventura CB,
IsmailaN, Benson AB 3rd, Carrato A, Gulley ML, Jain D, Kakar
S,Mackay HJ, Streutker C, Tang L, Troxell M, Ajani JA (2017)HER2
Testing and Clinical Decision Making in
GastroesophagealAdenocarcinoma: Guideline From the College of
AmericanPathologists, American Society for Clinical Pathology, and
theAmerican Society of Clinical Oncology. J Clin Oncol
35(4):446–464. https://doi.org/10.1200/JCO.2016.69.4836
13. Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane
LM,Allison KH, Allred DC, Bartlett JM, Bilous M, Fitzgibbons
P,Hanna W, Jenkins RB, Mangu PB, Paik S, Perez EA, Press MF,Spears
PA, Vance GH, Viale G, Hayes DF, American Society ofClinical O,
College of American P (2014) Recommendations forhuman epidermal
growth factor receptor 2 testing in breast cancer:American Society
of Clinical Oncology/College of AmericanPathologists clinical
practice guideline update. Arch Pathol LabMed 138(2):241–256.
https://doi.org/10.5858/arpa.2013-0953-SA
14. Frampton GM, Fichtenholtz A, Otto GA, Wang K, Downing SR,He
J, Schnall-Levin M, White J, Sanford EM, An P, Sun J, Juhn
F,Brennan K, Iwanik K, Maillet A, Buell J, White E, Zhao
M,Balasubramanian S, Terzic S, Richards T, Banning V, Garcia
L,Mahoney K, Zwirko Z, Donahue A, Beltran H, Mosquera JM,Rubin MA,
Dogan S, Hedvat CV, Berger MF, Pusztai L, LechnerM, Boshoff C,
Jarosz M, Vietz C, Parker A, Miller VA, Ross JS,Curran J, Cronin
MT, Stephens PJ, Lipson D, Yelensky R (2013)Development and
validation of a clinical cancer genomic profilingtest based on
massively parallel DNA sequencing. Nat Biotechnol31(11):1023–1031.
https://doi.org/10.1038/nbt.2696
15. Fehm T, Muller V, Aktas B, Janni W, Schneeweiss A, Stickeler
E,Lattrich C, Lohberg CR, Solomayer E, Rack B, Riethdorf S, KleinC,
Schindlbeck C, Brocker K, Kasimir-Bauer S, Wallwiener D,Pantel K
(2010) HER2 status of circulating tumor cells in
patientswithmetastatic breast cancer: a prospective, multicenter
trial. BreastCancer Res Treat 124(2):403–412.
https://doi.org/10.1007/s10549-010-1163-x
16. Gao J, Wang H, Zang W, Li B, Rao G, Li L, Yu Y, Li Z, Dong
B,Lu Z, Jiang Z, Shen L (2017) Circulating tumor DNA functions asan
alternative for tissue to overcome tumor heterogeneity in ad-vanced
gastric cancer. Cancer Sci 108(9):1881–1887.
https://doi.org/10.1111/cas.13314
17. Mishima Y, Matsusaka S, Chin K, Mikuniya M, Minowa
S,Takayama T, Shibata H, Kuniyoshi R, Ogura M, Terui Y,Mizunuma N,
Hatake K (2017) Detection of HER2 amplificationin circulating tumor
cells of HER2-negative gastric Cancer patients.Target Oncol
12(3):341–351. https://doi.org/10.1007/s11523-017-0493-6
Publisher’s Note Springer Nature remains neutral with regard to
juris-dictional claims in published maps and institutional
affiliations.
2585Evaluation of Next Generation Sequencing for Detecting HER2
Copy Number in Breast and Gastric Cancers
https://doi.org/10.1038/gim.2013.92https://doi.org/10.1371/journal.pmed.1002230https://doi.org/10.1002/gcc.22431https://doi.org/10.1038/hgv.2016.25https://doi.org/10.1038/hgv.2016.25https://doi.org/10.1038/ejhg.2017.42https://doi.org/10.1038/ejhg.2017.42https://doi.org/10.1016/j.jmoldx.2014.09.008http://creativecommons.org/licenses/by/4.0/http://creativecommons.org/licenses/by/4.0/https://doi.org/10.3816/cbc.2004.n.011https://doi.org/10.3816/cbc.2004.n.011https://doi.org/10.1200/JCO.2018.77.8738https://doi.org/10.1200/JCO.2018.77.8738https://doi.org/10.1200/PO.17.00011https://doi.org/10.1200/JCO.2016.69.4836https://doi.org/10.5858/arpa.2013-0953-SAhttps://doi.org/10.1038/nbt.2696https://doi.org/10.1007/s10549-010-1163-xhttps://doi.org/10.1007/s10549-010-1163-xhttps://doi.org/10.1111/cas.13314https://doi.org/10.1111/cas.13314https://doi.org/10.1007/s11523-017-0493-6https://doi.org/10.1007/s11523-017-0493-6
Evaluation of Next Generation Sequencing for Detecting HER2 Copy
Number in Breast and Gastric CancersAbstractBackgroundMaterials and
MethodsStudy and Panel DesignCell Line CNV DetectionPatients and
SamplesDNA ExtractionNGS Library PreparationSequencing and Data
AnalysisBase Substitution, Short Insertion and Deletion
AnalysisCopy Number Variation DetectionHER2 IHC and FISH
TestingStatistics
ResultsAssay Performance of NGS Calls in Standard
MaterialsDistribution of HER2 Amplification Status in Breast
CancerDetermination and Evaluation of Cut-off to Categorize the
HER2 Status in Breast Cancer Using NGSClassification of HER2
Equivocal Status Samples in Breast Cancer Using NGSCNV Detection in
Gastric Cancer Using NGSConcurrent Detection of Other Somatic
Alterations in the Clinical FFPE Samples
DiscussionConclusionsReferences