-
[CANCER RESEARCH 49, 745-752, February I, 1989]
Expression of Lewis3, Lewisb, Lewis", Lewisy, Sialyl-Lewis8, and
Sialyl-Lewis"
Blood Group Antigens in Human Gastric Carcinoma and in
NormalGastric TissueJunichi Sakamoto,1 Tadashi Watanabe, Takahiko
Tokumaru, Hiroshi Takagi, Hiroaki Nakazato, and
Kenneth O. LloydDepartment of Gastroenterological Surgery, Aichi
Cancer Center, 1-1 Kanokoden Chikusaku, Nagoya, Japan fJ. S., H.
N.]; the Second Department of Surgery, NagoyaUniversity Faculty of
Medicine, 65 Tsurumaicho Showaku, Nagoya, Japan [T. W., T. T., H.
T.]; and the Memorial Sloan-Kettering Cancer Center, New York,New
York ¡0021[K. O. L.]
ABSTRACT
A panel of 6 mouse monoclonal antibodies detecting blood
groupantigens of the Lewis systems and their sialylated derivatives
have beenused to define the immunoanatomic distribution of these
antigenic structures within the normal human gastric mucosa and in
gastric cancertissues. The reagents employed detect the following
blood group specificities: Lewis', Lewisb, Lewis", Lewis',
sialylated Lewis', and sialylatedLewis". We have analyzed the
presence of these antigens in histologically
normal gastric mucosa and in gastric carcinoma from 61 patients
by theimmunoperoxidase method. In addition, we simultaneously
examined theblood group and secretor status in 31 of the 61
individuals studied.
Immunohistochemical analysis revealed that these antigenic
systemsare differentially expressed in cell types and cell layers
of the normalgastric epithelium. Major differences were observed in
surface epitheliaand in deep glands including Brenner's gland of
the gastroduodenaljunction, mainly in the pronounced expression of
Lewis* and Lewis1'antigens in the former and the expression of
Lewis" and I .CMis' in thelatter. In secretor individuals, Lewisb
was the dominant antigen in thesurface epithelium, and in
nonsecretors, Lewis' was observed in thesurface epithelium. Lewis"
and Lewis' were both detected in the deepglands and in Brenner's
glands regardless of the secretor status. The
expression of sialylated derivatives in normal gastric tissues
was considerably reduced but was consistent with the expression of
their precursorsin normal gastric epithelium.
In gastric cancers, more pronounced expression of Lewis* and
sialylated Lewis* was observed in secretor individuals and acted as
a tumor-associated antigen. Comparison of the plasma level of
sialylated Lewis*
and its tissue expression demonstrated that the shedding of the
antigeninto interstitial stroma correlated with the detection of
the antigen inserum.
These studies confirmed the importance of blood group antigens
asnormal differentiation antigens. Examination of secretor status
clarifiedthe mechanism of Lewis*and Lewisbantigen expression in
gastric surface
epithelium. Alterations in the expression of these antigens and
an increaseof sialylated derivatives in gastric cancers
demonstrated that these bloodgroup antigens are useful tools for
the analysis of histogenesis andorganogénesisin the stomach and
its neoplastic and nonneoplastic diseases.
INTRODUCTION
Blood group antigens are a group of carbohydrate determinants
typically found on erythrocytes. Their specificities arealso
expressed in many epithelial tissues and they act as
majoralloantigenic systems in humans (1, 2). Those antigens
arecarried by two types of backbone structures, type 1
chains[containing Gal(/31-3)GlcNAc] and type 2 chains
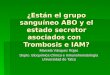
[containingGal(/31-4)GlcNAc]. As schematically presented in Fig. 1,
ABHand Lewis structures are formed by sequential addition of
Received 3/2/88; revised 9/19/88; accepted 11/2/88.The costs of
publication of this article were defrayed in part by the
payment
of page charges. This article must therefore be hereby marked
advertisement inaccordance with 18 U.S.C. Section 1734 solely to
indicate this fact.
1To whom requests for reprints should be addressed, at
Department ofGastroenterological Surgery, Aichi Cancer Center, 1-1
Kanokoden Chikusaku,Nagoya 464, Japan.
fucose, galactose and GalNAc to the backbone carbohydratechains
of both lipids and proteins (3). In addition to the
genescontrolling the synthesis of those structures, another gene
locuscontrols the expression of the antigens in secretions and
onvarious cell types of different organs. Thus the classical
terms"secretor" and "nonsecretor" indicate the capacity of an
indi
vidual to secrete or not secrete such substances in saliva
(4).Secretor individuals produce ABH, Lewisb (Leb) and Lewis*(Ley),
whereas nonsecretors produce Lewis' (Le") and Lewis"(Le") antigens
in their saliva (5).
Interest in the secretor status and Lewis expression in
normaltissues and in tumors has increased in recent years because
ofseveral clinicopathological observations in gastrointestinal
oncology. These include: (a) an apparent loss of ABH and enhanced
expression of Le" in human gastric cancers (6). (b)Evidence that
secretor individuals express Le" instead of Leb inthe distal colon,
and the appearance of Leb or Ley in cancers of
distal colon (7). (c) Patients with certain epithelial tumors
showelevated serum levels of Lewis antigens (8). (d)
Sialylatedderivatives of the Lewis antigens, such as sialylated-Le"
orsialylated-Le", may act as tumor-associated markers in
certain
alimentary tract cancers (9).In this study, we focused on the
expression of Le3, Leb, Le",
and Ley, sialylated Le" (ÇA19.9), and sialylated Le"
(CSLEX1)
antigens in stomach. We have analyzed the presence of
theseantigens in frozen and paraffin sections of normal stomach
andgastric cancers obtained from 61 gastric cancer patients by
theimmunoperoxidase method using a panel of mouse moAbs.2
We simultaneously tested salivas using an ELISA for
secretorstatus in 31 of those patients to correlate
immunohistologicaldistribution with secretor status. We also
analyzed the serumlevels of sialylated-Le" antigen by RIA and
compared them with
the results of immunopathology.
MATERIALS AND METHODS
Tissues. Primary gastric carcinoma tissue was obtained from
61patients undergoing surgical resection at Nagoya University
Hospitaland at Aichi Cancer Center. 18 were from cardia, 20 were
from body,and 23 were from nutrii in of the stomach. Five were well
differentiated,23 were moderately differentiated, 29 were poorly
differentiated, twowere mucinous, and two were signet ring cell
carcinomas. In all casesnormal mucosa distant from the tumor lesion
was obtained from thesame patient. The tissues were prepared from
surgical pathology specimen within 1 to 2 h of resection and fresh
tissues were fixed in 10%formaldehyde in phosphate buffered saline
(PBS), pH 7.5, and embedded in paraffin. Alternatively, tissues
were snap frozen in isopentaneprecooled in liquid nitrogen, were
embedded in OCT compound andwere stored at —¿�70°Cuntil
needed.
Reagents. moAbs T-174, T-218, P-12, and F-3 with specificities
forLe", Leb, Le", and Ley antigens, respectively, were used (7,
10-12).
1The abbreviations used are: moAb, monoclonal antibody; ELISA,
enzyme-
linked immunosorbent assay; RIA. radioimmunoassay.
745
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
BLOOD GROUPS IN STOMACH TUMORS
Type 1 Chains Type 2 Chains
Gal(3l-»3GlcNAcGalßMGlcNAc GalßMGlcNAc Gal(3l-*3GlcNAc
Gal(3H-4GlcNAc Galßl-~4GlcNAc Gal(3l-*4GlcNAc Gal0 H-4GlcNAc
1,3Fuco
1.2 1,4NANA Fuca
11.4Fuea
11.1Fuea
1,2 | 1,4Fuea Fuea
1.3Fuca
1.2Fuca
1,2 | 1,3Fuea Fuea
Sialyl-Led Lea H-l LeD Sialyl-X H-2
GalNAcal—-3Galß1—SGlcNAc Gala l—-3Galßl—-3GlcNAc
1,2Fuca
GalNAcal—-3Galß1—4GlcNAc
1.2Fuca
Gala l—-3Galßl-~4GlcNAc
jl.2Fuca
ILIFuca
A-l B-l A-2 B-2
Fig. 1. Structural relationship between A, B, H, Lewis, Le",
Le', sialylated Le* and sialylated Le* blood group determinants.
//-/ and H-2, monofucosyl type 1 andtype 2 H-determinants,
respectively. Le* and Ley specificities are also known as X and Y,
respectively. All sugars are in the D-configuration, except for
fucose, whichis in the L-form.
Mouse moAb 19.9 was used to detect the sialylated Le" structure
(9),and antibody CSLEX1 was used to define sialylated Lex structure
(13).
Immunohistochemistry-Immunoperoxidase Staining Using
moAb.Formalin-fixed and paraffin-embedded tissue sections were
depuratimi/ed with xylene and ethanol for use in this technique.
Tissue sectionswere incubated in supressor serum and then were
incubated with moAbovernight at 4"( '. Both
peroxidase-antiperoxidase and avidin-biotin
methods were used in our experiments. The secondary antibodies
werehorse anti-mouse horseradish peroxidase conjugate (Vector
Laboratories, Burlingame, California) incubated on sections for 1
h. The peroxidase reaction was performed by incubating tissue
sections for 6 to12 min with 5 mg of diaminobenzene
tetrahydrochloride (Sigma Chemical Company, St. Louis, MO) in 100
ml of Tris buffer, pH 7.6, plus100 ¿ilof 0.3% hydrogen peroxide.
Sections were washed with distilledwater counterstained with
hematoxylin and mounted with paramount.Fresh frozen sections were
also used for this method. For the negativecontrols, moAbs against
melanoma antigens of the same species andsubtype were used.
Determination of Secretor Status. Saliva was collected without
preliminary stimulation and glycoproteins were extracted. An ELISA
procedure for reactivity with anti-Le* and anti-Leb antibodies were
performed
as described previously (5).Serum Level of CA 19.9. Blood
samples were obtained from 28
patients among 61 cases tested by immunopathology. The serum
levelsof CA 19.9 antigen were determined by commercial
radioimmunoassaykits (RIA; Centocor, SRL, Tokyo, Japan). The cut
off level was set at37 unit/ml according to the study of Del
Villano (14).
Serum Level of CSLEX1. Blood samples from 16 patients
wereobtained. The serum levels of CSLEX1 antigen were tested by RIA
kit(Midori Pharmaceutical Company, Tokyo, Japan) and the titer
wasdetermined by ELISA assay using the sandwich method with
peroxi-dase-labeled CSLEX1 antibody. The dilution of serum sample
wasstarted from 1:4; reactivities below that titer were considered
to benegative.
RESULTS
Blood Group Antigen Expression in Gastric Cancer and inNormal
Gastric Epithelium. The expression of Le", Leb, Le",Ley, sialylated
Le",and sialylated Le" antigens in gastric cancer
specimens and gastric epithelium from the same individuals,
was determined using the immunoperoxidase method (Table1).
In normal gastric mucosa, Le* was expressed in 30 and Le"was
present in 49 out of 61 cases tested. Le" was present in 51and Ley
was positive in 55 cases. Sialylated Le" was detectedonly in nine
specimens of normal gastric mucosa and sialylatcd-Le" was positive
in 31 cases.
In carcinoma tissues, Le" expression was found in 41/61 andLeb
was detected in 42/61 tumors. Le" was expressed in 44/61and Ley was
expressed in 43/61 cases. Sialylated Le" was foundin 30 cases of
carcinoma tissues and sialylated Le" was expressed in 28 tumor
specimens. Le" and sialylated Le" expres
sion was greatly increased in carcinoma tissues as compared
totheir presence in the corresponding normal tissues. In
someindividuals (19/61 for Le" and 23/61 for sialylated Le")
the
antigen was detected in the tumor samples but not in
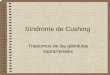
normalgastric epithelium. In Fig. 2A, tumor-associated expression
ofLe" is demonstrated. In Fig. 2B, expression of Le" antigen in
aserial section is shown. Le" was present in the normal gastric
gland but not in tumor tissues.Immunostaining of Tumor and
Normal Tissue from the Same
Individuals and Correlation with Secretor Status. 31
patientswere chosen for a more-detailed analysis in which Le", Leb,
Le",Ley, sialylated Le", and sialylated Lex expression in
tissue
sections was determined by immunoperoxidase staining of
bothfrozen and paraffin-embedded samples and the saliva samplesfrom
the same individual were analyzed to determine theirsecretor status
(Table 2).
In normal gastric epithelium of the secretor individuals,
Le"
Table 1 Reactivity of anti-blood group-related antibodies with
normal stomachand stomach carcinoma tested with immunoperoxidase
method
Le' Le" Le"
Sialyl- Sialylated ated
Le' Le' Le"
Normal
(+)/carcinoma(+)Normal(—(/carcinoma(+)Normal(+)/carcinoma
(—)Normal(-)/carcinoma
(-)22"198123841184131074121447232292171023
°Number of cases out of 61 cases tested.
746
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
BLOOD GROUPS IN STOMACH TUMORS
Sis
B
Fig. 2. Immunohistological analysis of normal gastric epithelium
and gastriccarcinoma with anti-Le* and anti-Le* blood group
antibodies using the inumimi
peroxidase technique. A, section has normal gastric epithelium
on the right handside, which is negative with anti-Le* and gastric
carcinoma tissue in the lower leftpart, which is positive with
anti-Le'; B, sequential section of the same specimenstained with
anti-Le" antibody. The normal gastric glands show positive
staining
and the cancer tissue is negative. Magnification: x 40.
was positive in 10 out of 22 patients and Leb was positive in
allsamples. The expression of Lea and Leb in secretors was
mainly
confined to the foveolar epithelium of the stomach but in
threecases, Le" expression was extended down into the deep
gastricpits. Le" was positive in deep gastric glands in only one
case of
normal gastric epithelium in secretors and in this case,
thefoveolar epithelium was strongly positive. No case was notedin
which either Le" or Leb was expressed exclusively in deep
gastric pits and not in foveolar epithelium. The expression
ofLe" antigen in normal epithelium was different from Le" andLeb.
Le* was detected in deep gastric glands in 18 out of 22
secretor individuals and was not expressed in the
foveolarepithelium. Ley antigen expression was similar to Le",
however,Ley was occasionally detected in the foveolar epithelium in
6/22 secretor cases. In all these six cases, Ley was positive in
the
deep gastric glands as well as in the foveolar epithelium. Fig.
3shows the typical staining pattern of Le", Leb, Le", and Ley
antigen in normal gastric epithelium of a secretor individual.In
nonsecretors, Le" was expressed in seven out of nine cases
and Leb was weak and heterogenously positive in two cases,
inwhich Le" was clearly positive. There were two cases of
nonsecretors, who expressed neither Le" nor Leb in their
gastric
epithelium. In these cases, analysis of saliva revealed that
theglycoprotein has no reaction with Le" or Leb but they
werepositive with anti-Le" or anti-Ley antibodies. Le" and Ley
were
positive also in the deep gastric glands of nonsecretors.
Leyexpression was weaker in nonsecretors than was Le", and
either
faint or heterogenous antibody staining was observed in thedeep
gastric pits with no extension to the foveolar epithelium.
In noncancerous pathological conditions such as
chronicgastritis, intestinal metaplasia or mucosa adjacent to
cancers,these patterns of antigen distribution were more variable
andsometimes, Le" and Leb was detected deep in gastric mucosa.
The expression of sialylated Le" and sialylated Le" in
normalgastric epithelium was consistent with the expression of
Le"and Le", respectively. That in Le"-positive specimens,
sialylatedLe", was also positive, although the staining pattern was
moreheterogenous and weaker. Sialylated Le" was positive in 17
normal gastric epithelium and its expression was mainly in
thedeep gastric glands.
In gastric cancers, the expression of Le" was increased and in10
secretor specimens, Le" was expressed only in gastric cancerwhile
normal gastric epithelium was unreactive. Sialylated Le*
expression was also increased in gastric cancer of secretors
suchthat in 11 secretor patients, sialylated Le" acted as a
tumorassociated antigen. Sialylated Lex expression was variable
in
cancers.In nonsecretors, blood group antigen expression was
en
hanced in cancers as compared to normals but no
prominenttumor-related antigens, such as Le" or sialylated Le" in
secre
tors, were noticed.Correlation between Immunoperoxidase Staining
and Serum
Level of Sialylated Le* Detected by Monoclonal Antibody
CA19.9. In 28 cases, blood samples were collected to
determinethe serum level of sialylated Le" and the results were
correlated
with the immunoperoxidase staining of tissue specimens fromthe
same patient (Fig. 4). In 16 patients, sialylated Le" was not
expressed in gastric cancer tissues and in all these cases,
serumCAI9.9 levels were under 20 U/ml and in negative range. In12
patients, sialylated Le" was expressed in gastric cancer
tissues and in those cases, serum CAI9.9 level ranged from 10to
170 U/ml and five cases were over 37 U/ml, which is thecut-off
level in the radioimmunoassay. In these 12 cases,
theimmunopathology findings showed a typical positive
stainingpattern. As shown in Fig. 5, the antigens were shed from
thecytoplasm to the surrounding stroma and interstitial tissueswere
stained. In cases with negative serum levels, especiallyunder 20
U/ml, this shedding of the sialylated Le" antigen was
not observed, and the antigen was confined to the cytoplasm
ofcancer cells.
Correlation between Immunoperoxidase Staining and SerumLevel of
Sialylated-Le" Detected by Monoclonal Antibody
CSLEX1. Blood samples were collected from 16 cases to testthe
serum level of sialylated Le", and the results were compared
with the immunoperoxidase staining of the corresponding cancer
tissues (Fig. 6). In six cases, sialylated Le" was not
expressed
in cancer sections and in 12 cases the staining was positive
withCSLEX1 antibody. As shown in Fig. 6, two cases of
negativeimmunoperoxidase staining had high serum titer of
sialylatedLe" antigen. In the cases which showed positive
immunoper
oxidase staining, one had a serum titer of 1:16 and 3 had
titersof 1:8. No significant differences in the serum CSLEX1
titerswere observed between immunohistochemistry-positive
patientsand -negative patients.
DISCUSSION
Glycolipids and glycoproteins with blood group specificitieshave
been regarded as differentiation antigens, defining partic-
747
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
BLOOD GROUPS IN STOMACH TUMORS
Table 2 Immunoreactivity of antibodies detecting blood group
antigens in adult gastric foveolar epithelium, deep gland cells,
and in gastric carcinoma
Bloodtype
Case ABOno.(RhD)1
O(+)2
O(+)3
A(+)4
O(+)5
A(+)6
A(+)7
A(+)8
B(+)9
A(+)10
O(+)1
1 AB(+)12
B(+)13
O(+)14
O(+)15
O(+)16
A (+)Blood
group-relatedantigens'Secretor
status"SSSSssssssssssssLocus*FEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCLe10O0ooeoo•oo•oo0ooo0o•oo0oo•oo•ooooo•0oo9o0•oo0o0Le"•OO•o99o90O00O00o00e•0o00o00o••o•0o•00o•o00o00o0Le"O0ooo0ooeo•0o00o00o00o00o00000o0ooooo0oo00o00o0oLe"e0oo00o00000o00e00O00000o00o00000000o0oo00000o0•Sialyl-atedLe"OOoooooo9oo0oo0ooooo0oo0oo0oo0ooooo0ooooo0ooooooSialyl-atedLe"e0oo09O00O0eoeooooooo990O90000Oooo00e0oo00o900oeBloodtypeCase
ABOno.(RhD)17
A(+)18
O(+)19
B(+)20
AB(+)21
O(+)22
A(+)23
A(+)24
A(+)25
B(+)26
O(+)27
O(+)28
O(+)29
B(+)30
AB(+)31
A(+)Blood
group-relatedantigens'Secretor
status"SSSSSSNSNSNSNSNSNSNSNSNSLocus*FEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCFEDGGCLe"0O00O00oo0o00o00o00o00o00o09Ooooooo00o00oo0o0Leb0O00oe0oo0O00oo0o0ooooo0oo0oo000oooo9o9ooo9O0Le"O00O00o00oooo00o00o00o0o900o90O0Oo0o009O00o00Le>900O00Oe0o0000o900Oeo0o0990Oo0o0ooeo09Oo0ooo0Sialyl-atedLe10O0Oo9Ooo0o09Ooooo9O00ooo0oe90o0oooo0oo9oooo0Sialyl-atedLe"Oe0900O0Ooe0ooooeoo00oo0eee0e9o0oo0oo00oo00oo
°S, secretor; NS, nonsecretor.* FE, antigen positive in
foveolar epithelium; DG, antigen positive in deep gastric glands;
GC, antigen positive in gastric cancer.' Immunoreactivities:
•¿�,homogenous staining; 0, heterogenous staining; O,
unreactive.
ular cell or tissue types representing developmental pathwaysand
specific functions. These structures are formed by thesequential
addition of different saccharides to the side chainsof both lipids
and proteins (3, 15-17). It has been suggestedthat development and
differentiation could be mediated bycontinuous changes of these
cell surface glycoconjugatesthrough which cell-cell interactions
may take place (18). Studies
in the murine embryo (19, 20) suggested that these
structuresmight be the signals for cell recognition.
Interest in the blood group antigen expression in normaltissues
and tumors has increased a great deal in recent yearsbecause of
several observations demonstrating changes in theseantigenic
systems following tumorigenesis (21-23). In the gastrointestinal
system, expression of the antigens in colorectalcancers have been
extensively discussed in the literature. Anapparent deletion of A
and B antigens (6, 24); incompatibleexpression of A, B, and H
antigens (25, 26); and expression ofnovel blood group-related
antigens (9, 27, 28) were reported.Also, several studies on Lewis
system antigens have been carriedout. Increased expression of Ley
(4, 29) and incompatible
expression of Leb (4, 31) in nonsecretor individuals were ob
served in colorectal cancers.Concerning stomach tissues and
tumors, the pioneering work
of Ernst et al. (31) demonstrated the presence of Lea antigen
innonsecretors and Leb in secretors using an immunoperoxidasemethod
on paraffin-embedded normal stomach tissues. Theyalso observed two
Lea-positive cases in secretors and one Leb-positive case in a
nonsecretor. In gastric cancers, Le" antigen
expression was more frequent and 80% of cancers were
positivewith Le". These findings are also supported by the study
of
Hirohashi et al. (32) using gastric cancer specimens. In
anotherreport, Ernst et al. (6) demonstrated the deletion of A and
Bantigens in gastric carcinomas. Mollicone et al. (33) demonstrated
specific antigen localization in pyloric and duodenalmucosa using
polyclonal and monoclonal antibodies againstLewis
blood-group-related antigens. These reports (31, 33, 34)were not in
complete agreement on the localization of Lewisantigens in normal
gastric mucosa.
Our present results are basically consistent with these
ofMollicone et al. (33) in terms of antigen expression in
normal
748
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
BLOOD GROUPS IN STOMACH TUMORS
Fig. 3. Localization of Lewis blood group-related antigens in
normal adult stomach of asecretor individual detected by
immunoperox-idase method. A, Le* antigen was not detected
in gastric mucosa! cells from this secretor individual. B, Leb
antigen was present in the
foveolar epithelium but not detected in thedeep gastric glands.
C, Lex antigen was de
tected only in the deep gastric glands and notpresent in the
foveolar epithelium. D, distribution of Le" antigen was very
similar to thelocalization of Le" antigen. Magnification: x
40.
C D
gastric epithelium. Le" was present in the surface foveolar
epithelium of nonsecretors but was also detected in 50% of
thesecretors, which was not noticed in their study. Leb was
positive
in secretors and mostly negative in nonsecretors. Both type
1antigens were almost exclusively detected in the foveolar
epithelium of intact gastric mucosa. In epithelial tissues
adjacentto cancer or in the concomittant inflammatory lesions,
theexpression of type 1 antigens often extended deep into
thegastric gland tissues and the distinct pattern of type 1 and
type2 antigens in normal gastric mucosa disappeared. In
contrast,Le" and Ley antigens were detected in deep gastric glands
bothin secretors and in nonsecretors, although the expression of
Ley
in nonsecretors was either weak or heterogenous. The patternof
type 2 antigen distribution was also changed in
pathologicalconditions, where the extension of antigen expression
to foveolar epithelium or the loss of antigens was observed.
Ourfindings on antigen expression in noncancerous
pathologicalconditions might explain the dominant expression of Leb
anti
gens in deep glands (1, 31). Another possible cause of
thedivergent results observed by different investigators could
becross-reactions of some of the reagents with type 2 structures.In
fact, cross-reactivity of caprin anti-Leb and monoclonal anti-Leb
antibodies with a Ley-like tetrasaccharide has been reported
(35, 36).The expressions of sialylated Le" and sialylated Le"
antigens
in normal mucosa were weaker and heterogenous in most ofthe
specimens. Sialylated Le" was negative in most of the
secretors but weakly positive in nonsecretors. In the report
ofBara et al. (37), the antigen was positive in only 7% of
thepatients. In our results, the antigen was often present in
normal
gastric mucosa of the nonsecretors. Sialylated-Lex was
claimed
to be absent in normal stomach (13), however we found theantigen
in nearly 50% of the cases tested.
To define the immunoanatomic distribution of blood groupantigens
in an organ, in our opinion, at least 40 to 50 specimensfrom
different individuals should be examined to obtain anappropriate
perspective. Such a large number of specimensmight be needed to
eliminate biases caused by allospecificitiesof the individuals.
The conclusions of our study are summarized schematicallyin Fig.
7. We have noticed that secretor individuals could besubdivided
into two categories based on their expression of Le"antigen. In one
group, Le" was expressed in foveolar epithelium,as was Leb; in the
other group, Le" was not present in any part
of the normal gastric mucosa. A possible explanation for
thesedifferent patterns may reside in whether an individual is
heterozygous or homozygous for the dimorphic genes Se and se
(38,39). Cordon-Cardo et al. (22) found a similar phenomenon
withLewis antigen expression in urothelium and they also
claimedthat the difference of genotype in the secretor gene may be
thecause of different antigen expression among the secretor
individuals.
Alterations in blood group expression in malignancy havebeen
classified (40) into five groups: (a) simplification of
maturecarbohydrate structures; (b) enhanced expression of
normalblood group antigens; (c) oncofetal or inappropriate
tissueexpression; (
-
BLOOD GROUPS IN STOMACH TUMORS
1000 n
a- 100
10
•¿�•¿�
U n re a c t ivc with
Immunoperox idase
Staining
Positive Staining
with
Immunoperox i dase
Fig. 4. Serum level of sialylated Le" (CA 19.9) antigen of
patients with gastric
carcinoma compared with tumor tissue distribution. 16 patients
were sialylatedLe* negative in cancer tissues by immunoperoxidase
method (left). Serum titersof sialylated Le* antigen in these
patients were all negative. 12 patients weresialylated Le" antigen
positive in tissue immunostaining (right). Serum titers
ofsialylated Le" antigen among these patients were positive ¡nfive
cases (>37 U/
ml).
Fig. 5. Sialylated Le* antigen distribution in gastric cancer
tissue of a case
with positive antigen in serum. The antigen was detected in the
cytoplasm ofmalignant cells and was also diffusely distributed in
the surrounding stroma.Magnification: x 100.
Decrease of Leb and appearance of Le" may be the
simplification
of mature carbohydrate structure, and enhanced expression
ofsialylated Le" may be categorized as enhanced expression of
normal blood group antigen.The serum level of the sialylated Le"
and sialylated Le"
antigens were evaluated in our study to determine whether
thereis any significant correlation between tissue expression and
theserum titer of the antigens. Serum level of sialylated Le
wasextensively studied in colorectal cancers (8) and tested in
11specimens in gastric cancers (41) by Koprowski et al.. In
theirreport, 72% of the patients with gastric cancers
expressedsialylated Le" in their serum whereas all the patients
expressed
«1:16ad
a:•¿�JMU
1:4 -
Negat ive
Unreactive withImmunoperoxidaseStaining
Positive StainingwithTmmunoperoxidase
Fig. 6. Serum level of sialylated Le* antigen of gastric cancer
patients compared with tumor tissue expression. Right, tumor
antigen-positive cases (N —¿�10);left, negative cases (N = 6). No
significant difference in the presence of serumantigen between the
two groups was observed.
the antigen in tissues. In our present study, we detected
theantigens in the serum of the five out of 12 patients whose
tumorwas antigen positive by immunoperoxidase staining. In
fiveother patients who were positive in tissues but negative
inserum, the staining pattern of the antigen was restricted to
thecell cytoplasm, whereas in both positive cases, shedding of
thesialylated Le" antigen into stromal tissues was observed.
Cor
relation between this pattern of tissue expression and
serumlevel of the antigens has been discussed in colorectal
cancers(42) and in pancreatic cancers (43). Although the serum
titerof the antigen does not always correspond to the presence
andprogression of gastric cancers in tissues, testing of
sialylatedLea antigen or maybe Le" antigen itself, might to a
certain
extent, be exploitable in the diagnosis of advanced or
recurrentgastric cancers.
Another aspect of blood-group-related antigens in gastriccancers
is the change in secretor gene-control expression. Insome
nonsecretors, anomalous Leb expression was observed incancers. In
colorectal cancers, anomalous Leb and Ley antigen
expression has been reported (7, 44). This observation is ofmuch
interest in terms of ABO antigen expression because therelated H
antigen could be a precursor of A or B structures. In
750
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
BLOOD GROUPS IN STOMACH TUMORS
SECRETORSTATUS
SECRETOR NONSECRETOR
ANTIGENS, a b x y SIALYL SIALYLLe Le Le Le , a x"*
—¿�Le-Lef
v a b x y SIALYL SIALYLLe Le Le Le' _Lea _L(;x
M TJ-O OI-H <
H MaeoM rr->i-iPO
d/CÖ
o oc->> WZ Ho soW h-i
o ln o> >SO WO H-i POZ h-1o n
Fig. 7. Schematic representation of the immunoanatomic
dissection of the blood group-related antigens within the human
adult gastric epithelium and in gastriccancer and their pattern of
expression in secretor versus nonsecretor individuals. Lines and
bars, positive immunoreactivity with each monoclonal antibody; bar
widths,relative intensity of an immunostaining pattern.
many cases of gastric cancers, expression of Lea and the
deletionof Leb was observed. This means that the H antigen present
in
normal gastric mucosa was lost in cancers and that might leadto
the deletion of A and B antigens reported by several investigators
(6, 24). From our present data, it seems possible thatenhanced
expression of Lea antigen, accompanied by the changeof sialylated
Le" could be indicators of malignant transforma
tion of gastric tissues. A panel of these reagents could be
usefulin the immunopathological analysis of gastric cancers,
particularly when the secretor status of the patient is
available.
Although attempts have made to produce monoclonal antibodies
against gastric cancer-related antigens (45, 46) or togastric
mucosa! cells (47), this has been difficult because
bloodgroup-related antigens seem to be major components of
gastrointestinal tissues. However, with proper selection of
antigen,together with the determination of secretor status, those
anti-blood group monoclonal antibodies might be exploitable in
theclinical and immunopathological diagnosis of
gastrointestinalcancers.
REFERENCES
1. Szulman, A. E., and Marcus, D. M. The histologie distribution
of the bloodgroup substances in man as disclosed by
immunofluorescence. VI: The Le"and Leb antigens during fetal
development. Lab. Invest.. 28: 565-574, 1973.
2. Marcus, D. M., and Cass, L. E. Glycosphingolipids with Lewis
blood groupactivity. Uptake by human erythrocytes. Science (Wash.
DC), 164: 553-555,1969.
3. Hakomori, S. Blood group ABH and li antigen of human
erythrocytes:chemistry, polymorphism, and their developmental
changes. Semin. Hema-tol., 18: 39-62, 1981.
4. Race, C. C., and Sanger, R. Blood group antigens in man (6th
edition).Blackwell Scientific Publications. Oxford, 1975.
5. Sakamoto, J., Yin, B. T., and Lloyd, K. O. Analysis of the
expression of H,Lewis. X, Y and precursor blood group determinants
in saliva and red cellsusing a panel of mouse monoclonal
antibodies. Mol. Immunol., 21: 1093-1098, 1984.
6. Ernst, C.. Thurin, J., Atkinson, B.. Wurzel, H., Herlyn, M.,
Stromberg, N.,Civin, C.. and Koprowski, H. Monoclonal antibody
localization of A and Bisoantigens in normal and malignant fixed
human tissues. Am. J. l'alimi..7/7:451-461, 1984.
7. Sakamoto, J., Furukawa, K., Cordon-Cardo, C., Yin, B. M. T.,
Rettig, W.J., Oettgen, H. F., Old. L. J., and Lloyd, K. O.
Expression of Lewis1, Lewis6,
X, and Y blood group antigens in human colonie tumors and normal
tissueand in human tumor-derived cell lines. Cancer Res., 46:
1553-1561, 1986.
8. Koprowski, H., Herlyn, M., Steplewski, Z., and Sears, H. F.
Specific antigenin serum of patients with colon carcinoma. Science
(Wash. DC), 212: 53-55,1981.
9. Koprowski, H., Steplewski, Z., Mitchell, K., Herlyn. M..
Herlyn, D., andFuhren, P. Coloréela!carcinoma antigens detected by
hybridoma antibodies.Somat. Cell Genet., 5: 957-972, 1979.
10. Rettig, W. J., Cordon-Cardo, C., Ng, J. S., Oettgen, H. F.,
Old, L. J., andLloyd, K. O. High-molecular weight glycoproteins of
human teratocarcinomadefined by monoclonal antibodies to
carbohydrate determinants. Cancer Res.,Â¥5:815-821, 1985.
11. Anger, B., Lloyd, K. O., Oettgen, H. F., and Old, L. J.
Mouse monoclonalantibody against human lung cancer line SK-LC-3
with specificity for H(O)blood group antigen. Hybridoma, /:
139-147. 1982.
12. Lloyd, K. O., Larson, G., Stromberg, N., Thurin, J.. and
Karlsson, K-A.Mouse monoclonal antibody F-3 recognizes the
difucosyl type 2 blood groupstructure. Immunogenetics, 17: 537-541,
1983.
13. Fukushima, K.. Hirota, M., Terasaki, P., Wakisaka. A.,
Togashi, H., Chia.D., Suyama, N.. Fukushi, Y., Nudelman, E., and
Hakomori, S. Characterization of sialosylated Lewis* as a new tumor
associated antigen. CancerRes., 44: 5279-5285, 1984.
14. Del Villano, B. C., Brennan, S., and Brock, P.
Radioimmunometric assayfor a monoclonal antibody defined tumor
marker, CA-19.9. Clin. Chem.. 29:549-552. 1983.
15. Feizi, T., and Childs, R. A. Carbohydrate structures of
glycoproteins andglycolipids as differentiation antigens, tumor
associated antigens and components of receptor systems. TIBS, 15:
24-29, 1985.
16. Watkins, W. M. Biochemistry and genetics of the ABO, Lewis
and P bloodgroup systems. Adv. Hum. Genet., 10: 1-136. 1980.
17. Hakomori, S., and Kobata, A. Blood group antigens. In: M.
Sela (ed.). The
751
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
BLOOD GROUPS IN STOMACH TUMORS
Antigens, Vol. 2, pp. 79-140. New York: Academic Press, 1974.18.
Hakomori, S. Glycosphingolipids in cellular interaction,
differential ion, and
oncogenesis. Annu. Rev. Biochem., 50: 733-764, 1981.19.
Shevinsky, I,.. Knowles, B.. Damajanov, I., and Solter, D. A
stage-specific
embryonic antigen (SSEA-3) defined by mouse monoclonal antibody
tomurine embryos, expressed on mouse embryos and on human
teratocarci-noma cells. Cell, 30: 697-705, 1982.
20. Kannagi, R., Nudelman, E., Levery, B., Solter, D., and
Knowles, B. A seriesof human glycosphingolipids reacting to the
monoclonal antibody directedto a developmentally regulated antigen,
SSEA-1. J. Biol. Chem., 257:14865-14874, 1982.
21. Yokota, M., Warner, G., and Hakomori, S. Blood group A-like
glycolipidand a novel Forssman antigen in the hepatocarcinoma of
blood group Oindividuals. Cancer Res., 41: 4185-4190, 1981.
22. Cordon-Cardo, C, Lloyd, K. O., Finstad, C. L., McGroaty, M.
E., Reuter,V. E., Bander, H. N., Old, L. J., and Melamed, M. R.
Immunoanatomicdistribution of blood group antigens in human urinary
tract. Lab. Invest., 55:444-454, 1986.
23. Okada, Y., Arima, T., Togawa, K., Nagashima, H., Jinno, K.,
Moriwaki, S.,Kunimoto, T., Thurin, J., and Koprowski, H.
Neoexpression of ABH andLewis blood group antigens in human
hepatocellular carcinomas. J. Nati.Cancer Inst., 78: 19-28,
1987.
24. Yuan, M., Itkowitz, S., Palekar, A., Shamsuddin, A., Phelps,
P., Trump, B.,and Kim, Y. Distribution of blood group antigens A,
B, H, Lewis" and Lewis1'in human normal, fetal and malignant
colonie tissue. Cancer Res., 45:4499-4511, 1985.
25. Cooper, H., and Haesler, W. Blood group substances as tumor
antigens inthe distal colon. Am. J. Clin. Pathol., 69: 594-598,
1978.
26. Clausen, H., Hakomori, S., Gream, N., and Dabelsteen, E.
Incompatible Aantigen expressed in tumors of blood group O
individuals: immunochemical,immunohistologic, and enzymatic
characterization. J. Immunol., 136: 326-330, 1986.
27. Itzkowitz, S., Yuan, M., Fukushi, Y., Palekar, A., Phelps,
P., Shaumsuddin,A., Trump, B., Hakomori, S., and Kim, Y. Lewis and
sialylated Lewis relatedantigen expression in human malignant and
nonmalignant colonie tissues.Cancer Res., 46: 2627-2632, 1986.
28. Fukushi, Y., Nudelman, E., Levery, S., Hakomori, S., and
Rauvala, H. Novelfucolipids accumulating in human adenocarcinoma.
III. A hybridoma antibody (FH6) defining a human cancer associated
difucoganglioside. J. Biol.Chem., 259: 10511-10517, 1984.
29. Kim, Y., Yuan, M., Itzkowitz, S., Sun, Q., Kaizu, T.,
Palekar, A., Trump,B., and Hakomori, S. Expression of Le" and
Extended Le" blood groupantigens in human malignant pre-malignant
and nonmalignant colonie tissues.Cancer Res., 46: 5985-5992,
1986.
30. Blaszcyk, M., Pak, K., Herlyn, M., Sears, H., and
Steplewski, Z. Characterization of Lewis antigens in normal colon
and gastrointestinal adenocarci-nomas. Proc. Nati. Acad. Sci. USA,
«2:3552-3556, 1985.
31. Ernst, C., Atkinson, B., Wysocka, M., Blaszcyk, M., Herlyn,
M., Sears, H.,Steplewski, Z., and Koprowski, H. Monoclonal antibody
localization ofLewis antigens in fixed tissue. Lab. Invest., 50:
394-400, 1984.
32. Hirohashi, S., Shimosato, Y., Ino, Y., and Tome, Y.
Distribution of bloodgroup antigens and CA 19-9 in gastric cancers
and non- neoplastic gastricmucosa. Gann, 75: 540-547, 1984.
33. Mollicone, R., Bara, J., Le Pendu, J., and Oriol, R.
Immunohistologic patternof type l and type 2 blood group related
antigens in the human pyloric andduodenal mucosae. Lab. Invest.,
53: 219-227, 1985.
34. Cordon-Cardo, C., Lloyd, K. O., Sakamoto, J., McGroaty, M.
E., Old, L. J.,and Melamed, M. R. Immunohistologic expression of
blood-group antigensin normal human gastrointestinal tract and
colonie carcinoma. Int. J. Cancer,37:667-676, 1986.
35. Marcus, D. M., and Grollman, A. P. Studies of blood group
substances. I.Caprine precipitating antisera to human Le* and
Le1'blood group substances.J. Immunol., 97: 867-875, 1966.
36. Messeter, L., Brodin, T., Chester, M. A., Karlsson, K. A.,
Zopf, D., andLundblad, A. Immunochemical characterization of a
monoclonal anti-Le1'blood group reagent. Vox Sang, 46: 66-74,
1984.
37. Bara, J., Zabaleta, E. H., Mollicone, R., Nap, M., and Hun
in, P. Distributionof GICA in normal gastrointestinal and
endocervical mucosae and in muci-nous ovarian cysts using antibody
NS 19-9. Am. J. Clin. Pathol., 82: 152-159, 1986.
38. Watkins, W. M. Biochemistry and genetics of the ABO, Lewis
and P bloodgroup systems. Adv. Hum. Genet., 10: 1-136, 1980.
39. Oriol, R., Danilovs, J., and Hawkins, B. R. A new genetic
model proposingthat the Se gene is a structural gene closely linked
to the H gene. Am. J.Hum. Genet., 33:421-431, 1984.
40. Lloyd, K. O. Blood group antigens as markers for normal
differentiation andmalignant change in human tissues. Am. J. Clin.
Pathol., 87:129-139,1987.
41. Koprowski, H., Blaszczyk, M., Steplewski, Z., Brockhaus, M.,
Magnani, J.,and Ginsburg, V. Lewis blood type may affect the
incidence of gastrointestinalcancer. Lancet, 1(8285): 1332-1333,
1982.
42. Hamada, Y., Yamaura, M., Hioki, K., Yamamoto, M., Nagura,
H., andWatanabe, K. Immunohistochemical study of carcinoembryonic
antigen inpatients with colorectal cancer. Cancer (Phila.),
55:136-141, 1985.
43. Ichihara. T., Nagura, H., Nakao, A., Sakamoto,J., Watanabe,
T., andTakagi,H. Immunohistochemical localization of CA 19-9 and
CEA in pancreaticcarcinoma and associated diseases. Cancer
(Phila.), 61: 324-333, 1988.
44. Brown, A., Ellis, I. O., Embleton, M. J., Baldwin, R. W.,
Turner, D. R., andHardcastle, J. D. Immunohistochemical
localization of Y hapten and thestructurally related H type 2 blood
group antigen on large bowel tumors andnormal adult tissues. Int.
J. Cancer, 33:727-736, 1984.
45. Prat, M., Rossino, P., Bussolati, G., Morra, I., and
Comoglio, P. M. Production of monoclonal antibodies for the
immunohistochemical detection ofgastric carcinomas. Cancer Detec.
Près.,10: 293-301,1987.
46. Watanabe, M., Hirohashi, S., Shimosato, Y., Ino, Y., Yamada,
T., Teshima,S., Sekine, T., and Abe, O. Carbohydrate antigen
defined by a monoclonalantibody raised against a gastric cancer
xenograft. Gann, 76:43-52, 1985.
47. Vecchi, M., Sakamaki, S., Diamond, B., Novikoff, A. B.,
Novikoff, P. M.,and Das, K. M. Development of a monoclonal antibody
specifically reactiveto gastrointestinal goblet cells. Proc. Nati.
Acad. Sci. USA, 84: 3425-3429,1987.
752
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
1989;49:745-752. Cancer Res Junichi Sakamoto, Tadashi Watanabe,
Takahiko Tokumaru, et al. Carcinoma and in Normal Gastric
Tissue
Blood Group Antigens in Human Gastricxand Sialyl-Lewis,a,
Sialyl-Lewisy, Lewisx, Lewisb, LewisaExpression of Lewis
Updated version
http://cancerres.aacrjournals.org/content/49/3/745
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected] at
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/49/3/745To request
permission to re-use all or part of this article, use this link
on June 9, 2021. © 1989 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/content/49/3/745http://cancerres.aacrjournals.org/cgi/alertsmailto:[email protected]://cancerres.aacrjournals.org/content/49/3/745http://cancerres.aacrjournals.org/