Embed Size (px)
Citation preview

Translational Cancer Mechanisms and Therapy
Extended Adjuvant Therapy with Neratinib PlusFulvestrant Blocks ER/HER2 Crosstalk andMaintains Complete Responses of ERþ/HER2þ
Breast Cancers: Implications to the ExteNET TrialDhivya R. Sudhan1, Luis J. Schwarz1,2, Angel Guerrero-Zotano1, Luigi Formisano1,Mellissa J. Nixon1, Sarah Croessmann1, Paula I. Gonz�alez Ericsson3, Melinda Sanders3,4,Justin M. Balko1,3,5, Francesca Avogadri-Connors6, Richard E. Cutler6, Alshad S. Lalani6,Richard Bryce6, Alan Auerbach6, and Carlos L. Arteaga1,3,5,7
Abstract
Purpose: The phase III ExteNET trial showed improvedinvasive disease-free survival in patients with HER2þ breastcancer treatedwithneratinib versus placebo after trastuzumab-based adjuvant therapy. The benefit from neratinib appearedto be greater in patients with ERþ/HER2þ tumors. We thussought to discover mechanisms that may explain the benefitfrom extended adjuvant therapy with neratinib.
Experimental Design: Mice with established ERþ/HER2þ
MDA-MB-361 tumors were treated with paclitaxel plus tras-tuzumab� pertuzumab for 4 weeks, and then randomized tofulvestrant � neratinib treatment. The benefit from neratinibwas evaluated by performing gene expression analysis for 196ER targets, ER transcriptional reporter assays, and cell-cycleanalyses.
Results: Mice receiving "extended adjuvant" therapy withfulvestrant/neratinib maintained a complete response, where-as those treatedwith fulvestrant relapsed rapidly. In three ERþ/
HER2þ cell lines (MDA-MB-361, BT-474, UACC-893) but notin ERþ/HER2� MCF7 cells, treatment with neratinib inducedER reporter transcriptional activity, whereas treatment withfulvestrant resulted in increased HER2 and EGFR phosphor-ylation, suggesting compensatory reciprocal crosstalk betweenthe ER and ERBB RTK pathways. ER transcriptional reporterassays, gene expression, and immunoblot analyses showedthat treatment with neratinib/fulvestrant, but not fulvestrant,potently inhibited growth and downregulated ER reporteractivity, P-AKT, P-ERK, and cyclin D1 levels. Finally, similarto neratinib, genetic and pharmacologic inactivation of cyclinD1 enhanced fulvestrant action against ERþ/HER2þ breastcancer cells.
Conclusions: These data suggest that ER blockade leads toreactivation of ERBBRTKs and thus extended ERBBblockade isnecessary to achieve durable clinical outcomes in patientswithERþ/HER2þ breast cancer.
IntroductionHER2 gene amplification and/or overexpression occur in
approximately 20% of patients with operable breast cancer, andused to be strong predictors of early disease relapse andmortality
(1, 2). With the advent of HER2-targeted therapies, the outcomeof patients with HER2-overexpressing (HER2þ) breast cancer hasvastly improved (3–5). The current standard of care for early-stageoperable HER2þ breast cancer includes one year of trastuzumab-based adjuvant therapy. However, a fraction of patients relapsewith metastatic disease (6). The HERA trial tested 24 months ofadjuvant trastuzumab. Results from this study showed that 2 yearsof adjuvant trastuzumab had an unfavorable benefit-to-risk ratiocompared with 1 year of trastuzumab (6). Conversely, the phaseIII ExteNET trial reported that extended adjuvant therapy with 12months of treatment with neratinib, an irreversible pan-ERBBtyrosine kinase inhibitor (TKI), resulted in a significant improve-ment in invasive disease-free survival compared with placebofollowing trastuzumab-based adjuvant therapy (7–9). Interest-ingly, the benefit was greater in patients with hormone receptor–positive (HRþ) breast cancer compared with those with HR�
disease. Of note, patients with HRþ cancer remained on anties-trogen therapy during extended adjuvant neratinib. On this basis,neratinib was recently approved by the FDA for use in patientswith HER2þ breast cancer following completion of adjuvanttrastuzumab (10). Analysis of long-term outcomes of patientsenrolled in the GeparQuinto trial revealed similar survival benefitin patients with HRþ tumors receiving prolonged anti-HER2
1Department of Medicine, Vanderbilt-Ingram Cancer Center, Vanderbilt Univer-sity Medical Center, Nashville, Tennessee. 2Oncosalud-AUNA, Lima, Peru.3Breast Cancer Program, Vanderbilt-Ingram Cancer Center, Vanderbilt Univer-sity Medical Center, Nashville, Tennessee. 4Department of Pathology, Vander-bilt-Ingram Cancer Center, Vanderbilt University Medical Center, Nashville,Tennessee. 5Department of Cancer Biology, Vanderbilt-Ingram Cancer Center,Vanderbilt University Medical Center, Nashville, Tennessee. 6Puma Biotechnol-ogy Inc., Los Angeles, California. 7Harold C. Simmons Cancer Center, UTSouthwestern Medical Center, Dallas, Texas.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
D.R. Sudhan and L.J. Schwarz contributed equally to this article.
Corresponding Author: Carlos L. Arteaga, UTSW Harold C. Simmons CancerCenter, 5323 Harry Hines Blvd., Dallas, TX 75390-8590. Phone: 214-648-1677;Fax: 214-648-7084; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-18-1131
�2018 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 771
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

treatment with neoadjuvant lapatinib followed by adjuvant tras-tuzumab (11).
To study how extended adjuvant neratinib achieved a betterclinical outcome in patients with ERþ/HER2þ breast cancer, wedeveloped a human-in-mouse breast cancer model. We foundthat ERþ/HER2þ MDA-MB-361 tumors rapidly evade ER block-ade through ERBB pathway hyperactivation. Conversely, inhibi-tion of ERBB tyrosine kinase activity with neratinib stoked up ERactivity. These compensatory bypass mechanisms have beendocumented by previous studies (12, 13). However, the molec-ular underpinnings of resistance to endocrine therapies in HER2þ
setting remain incompletely understood. We further observedthat resistance to fulvestrant treatment in ERþ/HER2þ breastcancermodelswasmediated, atleast in part, throughmaintenanceof cyclinD1 expression and cell-cycle progression. The addition ofneratinib led to a complete loss of cyclinD1 expression and tumorprogression, thereby, supporting simultaneous blockade of bothaxes to achieve durable remissions in patients with ERþ/HER2þ
breast cancer.
Materials and MethodsCell culture
MCF7 (ATCC HTB-22), BT-474 (ATCC HTB-20), MDA-MB-361 (ATCC HTB-27), and UACC-893 (ATCC CRL-1902)human breast cancer cell lines were purchased from ATCCwithin the past 10 years. All cell lines were maintained inATCC-recommended media supplemented with 10% FBS(Gibco) at 37�C in a humidified atmosphere of 5% CO2 inair. All cell lines were tested for Mycoplasma contamination andauthenticated by ATCC using short tandem repeat (STR) pro-filing method in January 2017. Prior to performing any in vitroexperiments, cells were rinsed with PBS, and maintained inphenol red–free media supplemented with 10% dextran-coatedcharcoal-treated FBS (DCC-FBS) for 72 hours.
Xenograft studiesAll animal experiments were approved by the Vanderbilt Insti-
tutional Animal Care and Use Committee (IACUC protocol M/14/028).MDA-MB-361 cells suspended in serum-free IMEMwereinjected subcutaneously (s.c.) into the right flank of 4- to 6-weekold, ovariectomized athymic nu/nu mice. When the averagetumor volume reached approximately 200 mm3, the mice were
treated with trastuzumab (20 mg/kg i.p. twice/week), paclitaxel(15 mg/kg i.p. twice/week; Sigma) � pertuzumab (20 mg/kg i.p. twice a week) for 4 weeks and then randomized to fulvestrant(5 mg/week s.c.; from AstraZeneca) � neratinib (20 mg/kgorally daily; from Puma Biotechnology). In our previous stud-ies, we have found neratinib to cause modest mouse weight lossdue to lack of appetite. This weight loss could be averted bydietary supplementation with flavor-enhanced DietGel 76A(clear H2O). Therefore, all mice were prophylactically supple-mented with DietGel in addition to regular chow. Animalweights and tumor dimensions were measured twice weeklyusing calipers. Tumor volume was calculated using the formula:volume ¼ width2 � length/2. Tumors were harvested 24 and 6hours after the last dose of fulvestrant and neratinib, respec-tively, fixed in 10% neutral buffered formalin, dehydrated, andparaffin embedded. Tumors were sliced into 5-mm sections andstained for P-HER2 (Cell Signaling Technology, #2249), ERa(Santa Cruz Biotechnology #8002), and Ki67 (Dako #M7240).Sections were scored by an expert pathologist (P.I. Gonz�alezEricsson) blinded to the treatment arm. Staining intensitieswere determined using a semiquantitative weighted histoscor-ing system that takes both intensity and percentage positivityinto account. H-score formula: 3 � [% of 3þ cells] þ 2 � [% of2þ cells] þ 1 � [% of 1þ cells] (14, 15).
FISHFISH was performed using CCND1/CEN11 Dual Color Probe
(ZytoVision, catalog no. ZTV-Z-2071). Images were captured at100� magnification and analyzed using Cytovision software byan expert pathologist (P.I. Gonz�alez Ericsson). CCND1 amplifi-cation was defined following HER2 guidelines.
Immunoblot analysisFlash-frozen tumor fragments were homogenized using a Tis-
suelyser (Qiagen) and lysed inRIPAbuffer (Sigma) supplementedwith 1� protease inhibitor (Roche) and phosphatase inhibitor(Roche) cocktails. Cells were washed with ice-cold PBS twice andlysed inRIPAbuffer as described above. Lysateswere gently rockedfor 30 minutes at 4�C and centrifuged at 13,000 rpm for 15minutes. Protein concentrations in supernatants were measuredwith the BCA protein assay (Pierce); 20 mg of total protein werefractionated by SDS-PAGE and transferred to nitrocellulosemem-branes (Bio-Rad). Membranes were blocked with 5% nonfat drymilk and then incubated at 4�C overnight with the followingprimary antibodies: from Cell Signaling Technology: P-HER2(#2249 1:1,000), HER2 (#2242; 1:5,000), P-HER3 (#4791;1:1,000), HER3 (#4754; 1:500), HER4 (#4795; 1:500), P-HER4(#4757; 1:500), P-EGFR (#2237; 1:1,000), EGFR (#2646;1:5,000), AKT (#9272; 1:10,000), P-AKTS473 (#9271; 1:500), P-ERK1/2 (#9101; 1:10,000), ERK (#9102; 1: 10,000), pRB (#9308;1: 1,000), and Calnexin (#2679; 1:10,000); from Santa CruzBiotechnology: ERa (sc-8002; 1:1,000) and cyclin D1 (sc-718;1:200). Nitrocellulose membranes were then incubated withhorseradish peroxidase–conjugated anti-rabbit or anti-mousesecondary antibodies for 1 hour at room temperature and immu-noreactive bands were detected by enhanced chemiluminescence(Perkin Elmer).
Cell viability assaysTo determine cell viability in the presence of drugs, cells were
seeded in 12-well plates in estrogen-free media; 24 hours later,
Translational Relevance
A significant proportion of patients with early-stage ERþ/HER2þ breast cancer relapse withmetastatic disease followingstandard-of-care treatment with 1 year of trastuzumab and5 years or longer of endocrine therapy. The phase III ExteNETtrial reported improved invasive disease-free survival inpatients with ERþ/HER2þ breast cancer receiving "extendedadjuvant" treatment with neratinib. We found that in a ERþ/HER2þ setting, endocrine therapy alone leads to rapid activa-tion of cyclin D1–regulating survival pathways and thus,combined ER and ERBB blockade is essential to achievedurable cyclin D1 suppression. Our study provides a plausibleexplanation to the benefit of extended anti-HER2 therapy intreating ERþ/HER2þ breast cancers.
Sudhan et al.
Clin Cancer Res; 25(2) January 15, 2019 Clinical Cancer Research772
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

theywere treatedwithDMSO,neratinib (200nmol/L), fulvestrant(1 mmol/L), or fulvestrant/neratinib. At experiment endpoint,plates were fixed, stained with crystal violet, and scanned usingaNikonflat-bed scanner. Staining intensities were then quantifiedusing a LI-COR Odyssey infra-red plate reader.
ERa transcriptional reporter assayCells were seeded in 96-well plates in estrogen-free media and
cotransfected with pGLB-MERE (encoding firefly luciferaseflanked by estrogen response elements) and pCMV-Renilla(encoding CMV-driven Renilla luciferase) plasmids; 16 hourslater, cells were treated with DMSO, fulvestrant (1 mmol/L),neratinib (200 nmol/L) or fulvestrant/neratinib. Luciferase activ-ities in drug-treated cells were determined 24 hours later usingDual-Luciferase reporter assay system (Promega) as per manu-facturer's instructions.
Quantitative PCR and NanoString analysisCells were seeded in 6-well dishes in estrogen-depleted
media; 72 hours later, cells were treated with DMSO, fulves-trant (1 mmol/L), neratinib (200 nmol/L), or fulvestrant/ner-atinib for 4–6 hours. Cells were then lysed and RNA wasisolated using Maxwell LEV SimplyRNA Cell Kit (Promega) asper manufacturer's instructions. Total RNA content was quan-tified using a Nanodrop spectrophotometer and reverse tran-scribed using the iScript cDNA synthesis kit (Bio-Rad). cDNAsof interest were amplified using RT2 qPCR primer assays forhuman PGR, GREB1, CCND1, and GAPDH (Qiagen). Relativegene expression was determined by performing quantitativePCR using the CFX-96 thermocycler (Bio-Rad). NanoStringanalysis was performed on human xenograft RNA using Nano-String nCounter Human Breast Cancer ER panel as describedpreviously (16). RNA was extracted from MDA-MB-361 tumorsusing Maxwell LEV SimplyRNA Tissue Kit (Promega) as permanufacturer's instructions; 50 ng of total RNA was used forinput into nCounter hybridizations. Quality control measuresand normalization of data were performed using the nSolveranalysis package and R. Data were normalized in nSolver(version 3.0) by using the geometric mean of the positivecontrol probes to compute the normalization factor as well asthe geometric mean of the housekeeping genes (CLTC, GAPDH,GUSB, HPRT1, PGK1, TUBB). Data were then log2 transformedto establish normal distribution and a one-way ANOVA wasperformed with a Benjamini and Hochberg false discovery ratecorrect to examine the difference between treatment groups.The FDR cutoff for statistical significance was set to 10%.Significant genes were then averaged for each treatment groupand z-scores were visualized using a heatmap.
Flow cytometryCells were plated in 60-mm dishes in estrogen-depleted media
and 3 days later treated with DMSO, fulvestrant (1 mmol/L),neratinib (200 nmol/L), or fulvestrant/neratinib for 24 hours.The cells were then harvested using phenol red–free TrpLE Xpressdissociation medium (Gibco), rinsed with PBS, and fixed with70% ethanol at 4�C for 30 minutes followed by 2 washes withPBS and incubationwith 0.1mg/mLRNaseA (Qiagen) and 40mg/mL propidium iodide (Sigma) for 10 minutes at room temper-ature. Cell-cycle distribution was assessed using a 3 laser LSRIIbioanalyzer.
Statistical analysisPaired and unpaired t tests were used to determine statistically
significant differences in cell proliferation assays, in vivo tumorgrowth assays, qRT-PCR assays, and IHCH-scores. AP value of lessthan 0.05was considered statistically significant, and all statisticaltests were two-sided. Bar graphs show mean � SEM, unlessotherwise stated in the figure legend.
ResultsAdjuvant therapy with fulvestrant/neratinib maintainscomplete responses of ERþ/HER2þ tumors
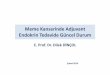
We first established a human-in-mouse model that simulatesthe clinical outcomes seen in the ExteNET trial. Mice withestablished ERþ/HER2-amplified MDA-MB-361 tumors weretreated with trastuzumab þ paclitaxel for 4 weeks, beforereceiving "extended adjuvant" therapy with fulvestrant � ner-atinib for 4 weeks (Fig. 1A). All MDA-MB-361 tumors exhibiteda prompt and marked reduction in volume after trastuzumab/paclitaxel treatment with some mice exhibiting a completeresponse (CR) and others a partial response (PR). Within theCR cohort, mice receiving fulvestrant/neratinib remained incomplete remission during treatment. After treatment discon-tinuation, only 2 of 5 tumors recurred during the next 6 weeks;these xenografts responded to retreatment with fulvestrant/neratinib. However, mice treated with fulvestrant alonerelapsed rapidly (P < 0.05 at week 8). Even within the PRcohort, fulvestrant/neratinib was able to significantly suppresstumor growth compared with single-agent fulvestrant. We didnot notice any signs of overt toxicities or considerable weightloss in mice receiving neratinib. We next evaluated ER and P-HER2 levels in fulvestrant-treated tumors on week 8 andfulvestrant/neratinib–treated tumors on week 18 (� in Fig.1A). ERa levels were markedly downregulated in both fulves-trant and fulvestrant/neratinib–treated tumors compared withuntreated controls. HER2 phosphorylation was significantlyhigher in tumors treated with fulvestrant alone but not fulves-trant/neratinib, suggesting activation of the HER2 pathway asan adaptation mechanism upon ER downregulation (Fig. 1Band C).
Since approximately 50% mice had failed to achieve a tumorCR prior to initiation of extended adjuvant therapy, we nextrepeated this experiment using double blockade of HER2 withpertuzumab and trastuzumab. Mice with established MDA-MB-361 xenografts were treated with pertuzumab/trastuzumab/pac-litaxel for 4 weeks. Following a complete tumor response, micewere randomized to fulvestrant/neratinib versus fulvestrantalone. Mice treated with the combination remained in completeremission for 6 months after treatment discontinuation and wereultimately euthanized. On the other hand, tumors inmice treatedwith fulvestrant monotherapy relapsed within a week, but theaddition of neratinib to fulvestrant on week 8 resulted in markedtumor shrinkage (Fig. 1D). Tumors recurring on fulvestrant wereharvested before and after the addition of neratinib (� in Fig. 1D).IHC analysis of tumor sections showed robust P-HER2 andundetectable ER levels before neratinib, and a significant reduc-tion in P-HER2 staining following the addition of the pan-HERTKI (Fig. 1E and F). These data suggest that extended ERBBblockade with a pan-HER inhibitor may overcome activation ofthe HER2 pathway in ERþ/HER2þ breast cancers treated withadjuvant antiestrogens alone.
Neratinib plus Fulvestrant Overcome ER/HER2 Crosstalk
www.aacrjournals.org Clin Cancer Res; 25(2) January 15, 2019 773
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

Neratinib and fulvestrant block ER/HER2 crosstalk andpotently inhibit growth of ERþ/HER2þ breast cancer cells
We next examined the effect of fulvestrant, neratinib, or bothdrugs against ERþ/HER2– MCF7 cells and a panel of ERþ/HER2þ
cell lines, BT-474, MDA-MB-361, and UACC-893. Except for P-HER3 in MCF7 cells, treatment with 200 nmol/L neratinibcompletely eliminated detectable P-HER2, P-EGFR, P-HER3, andP-HER4 levels in all cell lines. Neratinib also markedly down-regulatedP-AKT andP-ERK in all threeHER2þ cell lines, but not inMCF7 cells (Fig. 2A), suggesting that, in these cells, activation ofPI3K and MEK is not entirely dependent on the ERBB pathway.
Total EGFRand totalHER2 levelswere reduced in all four cell linesupon treatment with neratinib, with HER2 downregulation beingmore evident in MDA-MB-361 and UACC893 cells. Consistentwith the in vivo findings shown in Fig. 1B and E, fulvestranttreatment resulted in increased HER2 phosphorylation in BT-474 and UACC-893 cells but not in ERþ/HER2� MCF7 cells (Fig.2A). While MDA-MB-361 did not recapitulate the increase in P-HER2 levels at 24 hours, we noted a robust upregulation in HER2phosphorylation in response to long-term (2 weeks) fulvestrantexposure (Supplementary Fig. S1). Finally, clonogenic growthassays showed that HER2þ lines were generally resistant to
Figure 1.
Extended adjuvant therapy with neratinib/fulvestrant prevents recurrence of ERþ/HER2þ xenografts. A, Nude mice with established MDA-MB-361 xenografts weretreated with trastuzumab (20 mg/kg i.p. twice/week) and paclitaxel (15 mg/kg i.p. twice/week) for 4 weeks and then randomized to fulvestrant (5 mg/week s.c.)�neratinib (40 mg/kg orally daily). Numbers of mice per treatment are shown in parentheses. B, Representative IHC staining for ERa and P-HER2 in "CR"tumors. Scale bars, 100 mm for ERa and P-HER2. C, H-scores for ERa and P-HER2. D, Nude mice with established MDA-MB-361 xenografts were treated withtrastuzumab (20 mg/kg i.p. twice/week), pertuzumab (20 mg/kg i.p. twice a week), and paclitaxel (15 mg/kg i.p. twice/week) for 4 weeks and thenrandomized to fulvestrant (5 mg/week s.c.) � neratinib (40 mg/kg orally daily). Numbers of mice per treatment are shown in parentheses. E, Representative IHCstaining for ERa and P-HER2 in recurrent tumors from fulvestrant alone arm harvested before or after fulvestrant þ neratinib retreatment. Scale bars, 100 mm forERa and P-HER2. F, H-scores for ERa and P-HER2.
Sudhan et al.
Clin Cancer Res; 25(2) January 15, 2019 Clinical Cancer Research774
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

fulvestrant. However, in line with the effects on signal transduc-tion, treatment with fulvestrant/neratinib resulted in completegrowth inhibition of all three HER2þ cells, whereas neratinib didnot add to fulvestrant action against fulvestrant-sensitive MCF7cells (Fig. 2B and C).
We next tested whether trastuzumab would achieve similarsuppression of the adaptive responses induced by ER blockade.The growth of ERþ/HER2þ cells was onlymarginally hampered byfulvestrant or fulvestrant/trastuzumab. On the other hand, addi-tion of fulvestrant/neratinib completely ablated the growth ofcells refractory to fulvestrant/trastuzumab (Supplementary Fig.S2A and S2B). We then tested the phosphorylation status of otherERBB receptors in MDA-MB-361 tumors that recurred on fulves-trant following complete regression on trastuzumab-based ther-apy (� in Fig. 1A andD).While P-HER3 levels remained unaltered,we noted a significant increase in P-EGFR in tumors maintainedon fulvestrant but not fulvestrant/neratinib (Supplementary Fig.S2C–S2F). Consistent with these in vivo findings, long-term (2weeks) treatment of ERþ/HER2þUACC-893 cells with fulvestrantled to an increase in P-EGFR and P-HER4 in addition to P-HER2upregulation (Supplementary Fig. S2G). While the addition oftrastuzumab completely ablated HER2 phosphorylation, it didnot revert P-EGFR and P-HER4 to basal levels. Consistently, we
noted higher AKT phosphorylation in fulvestrant and fulves-trant/trastuzumab–treated cells compared with untreated con-trols. Collectively, these data suggest that ERþ/HER2þ tumorsevade ER blockade through concomitant activation of membersof the ERBB family, which would be effectively overcome by apan-HER TKI.
We next asked whether suppression of ERBB receptor signalingwith neratinib resulted in a compensatory effect on estrogenreceptor activity. In all three ERþ/HER2þ cell lines but not inERþ/HER2� MCF7 cells, treatment with neratinib resulted in asignificant increase in ER reporter transcriptional activity (MCF7,0.2-fold; BT474, 12-fold; MDA-MB-361, 2-fold; UACC893, 8-fold), which was dampened by the addition of fulvestrant. Treat-ment with fulvestrant alone reduced ligand-independent ERreporter activity in MCF7, but not in any of the HER2þ cell lines(Fig. 3A). Whereas fulvestrant treatment downregulated ER pro-tein levels in all cell lines, neratinib treatment resulted in a subtleand transient increase in ER levels in BT474 and UACC893 cells(Fig. 3B). To examine ER transcriptional activity further, weexamined the gene expression status for progesterone receptor(PGR) and GREB1. In all three HER2þ cell lines, neratinib treat-ment induced variable increase in PGR andGREB1mRNA expres-sion which, except for GREB1 in UACC893 cells, was reduced by
Figure 2.
Combined ERandHER2blockadepotently inhibits proliferation of ERþ/HER2þbreast cancer cells.A, Immunoblot analysis of cells treatedwith fulvestrant (1mmol/L),neratinib (200 nmol/L), or both under estrogen-free conditions for 24 hours. B, Representative images of cells seeded in 24-well plates, treated every2 days with fulvestrant (1 mmol/L), neratinib (200 nmol/L), or both under estrogen-free conditions. On day 7, monolayers were stained with crystal violet.C, Quantification of viability on day 7 based on cell counting. Values are mean � SEM from three independent experiments, Student t test.
Neratinib plus Fulvestrant Overcome ER/HER2 Crosstalk
www.aacrjournals.org Clin Cancer Res; 25(2) January 15, 2019 775
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

the addition of fulvestrant (Fig. 3C). Collectively, these datafurther suggest the need of dual targeting of ER and HER2 toblock crosstalk and achieve durable growth inhibition of ERþ/HER2þ breast cancer cells.
Combined treatment with neratinib plus fulvestrant targetscyclin D1
To further investigate the effects of fulvestrant/neratinib on ER–HER2 crosstalk at a molecular level, we screened for ER-regulatedgenes that are unresponsive to fulvestrant treatment, but sensitiveto the combination. MDA-MB-361 tumor-bearing mice weretreated with fulvestrant, neratinib, or fulvestrant/neratinib for 7days and then harvested (Fig. 4A). IHC of tumor sections showeddownregulation of ERa and P-HER2 levels in fulvestrant- andneratinib-treated tumors, respectively, confirming drug targetinhibition (Fig. 4B and C). Tumor RNA was extracted and sub-jected to gene expression analysis using a NanoString breastcancer ER panel consisting of 196 ER-regulated genes. Out of196 ER-regulated genes tested, 42 were significantly altered by at
least one of the treatments as shown inheatmap in Fig. 4D. Single-agent neratinib enhanced the expressionof several ER target genes,consistent with the upregulation of ER transcriptional activityobserved in vitro (Fig. 3A). CCND1 (cyclin D1) and GABRP(Gamma aminobutyric acid A receptor, Pi subunit) were the onlygenes unaffected by fulvestrant but that were ablated by thecombination treatment (Fig. 4D). Notably,CCND1 amplificationis present in 26% of ERþ/HER2þ breast cancers in the CancerGenomeAtlas (TCGA; Fig. 4E). Interestingly, all three ERþ/HER2þ
cell lines used herein, BT-474,MDA-MB-361 andUACC-893, alsoharbor CCND1 gene amplification (Fig. 4F).
We next examined whether downregulation of cyclin D1 wascentral to the efficacy of combined ER/HER2 targeting withfulvestrant/neratinib. Immunoblot analysis of MDA-MB-361tumor lysates (shown in Fig. 4A), confirmed near complete lossof cyclin D1 expression upon treatment with fulvestrant/nerati-nib, but not in tumors treated with fulvestrant or neratinib alone(Fig. 5A). Consistent with these results, neratinib � fulvestrant,but not fulvestrant alone, reduced cyclin D1 protein and P-Rb
Figure 3.
HER2 inhibition results in upregulation of ER transcriptional activity.A, ERE reporter activity in cells cotransfected with an ERE-firefly luciferase reporter plasmid andRenilla luciferase plasmid as an internal control. Cells were treated with fulvestrant (1 mmol/L), neratinib (200 nmol/L), or both for 24 hours. Values representmean � SEM from three independent experiments, Student t test. B, Immunoblot analysis of cells treated with fulvestrant (1 mmol/L), neratinib (200 nmol/L),or both for the indicated times. C, Relative expression of ER target genes in cells treated with fulvestrant (1 mmol/L), neratinib (200 nmol/L), or both for 6 hours.Values represent mean � SEM from three independent experiments.
Sudhan et al.
Clin Cancer Res; 25(2) January 15, 2019 Clinical Cancer Research776
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

Figure 4.
Combined treatment with neratinib and fulvestrant targets cyclin D1. A, Nude mice bearing MDA-MB-361 xenografts were treated for 7 days with fulvestrant(5 mg/week s.c.), or neratinib (40 mg/kg orally daily), or both. Numbers of mice per treatment are shown in parentheses. B, Representative IHC staining for ERaand p-HER2 in FFPE sections of tumors shown in A. Scale bars, 100 mm ERa and p-HER2. C, H-scores for ERa and P-HER2. D, Gene expression analysis of196 ER-regulated genes. RNA extracted from tumors shown in A was normalized and run on the NanoString Human Breast Cancer Estrogen Receptor Panel.Genes were compared across treatments using one-way ANOVA and FDR corrected at 10%. Significantly altered genes plotted as row-standardized Z-scoresare visualized with a heatmap. E, Tile plot depicting cyclin D1 amplification status in HER2þ breast cancers in TCGA (cBioPortal.org, TCGA - Cell, 2015). Cases arecategorized by ER status. F, CCND1:CEN11 ratio measured by FISH in the indicated xenografts as described in Materials and Methods.
Neratinib plus Fulvestrant Overcome ER/HER2 Crosstalk
www.aacrjournals.org Clin Cancer Res; 25(2) January 15, 2019 777
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

Figure 5.
Combined HER2 and ER blockade is required to suppress cell-cycle progression in ERþ/HER2þ cells. A, Immunoblot analysis of MDA-MB-361 tumors treated withfulvestrant (5 mg/week s.c.), or neratinib (40 mg/kg orally daily), or both for 7 days (shown in Fig. 4A). B, Immunoblot of cells treated with fulvestrant (1 mmol/L),neratinib (200 nmol/L), or both under estrogen-free conditions for 24 hours. C, Relative cyclin D1 mRNA levels in cells treated with fulvestrant (1 mmol/L),neratinib (200 nmol/L), both, estradiol (1 nmol/L), or neuregulin (10 ng/mL) under estrogen-free conditions for 4 hours. Values represent mean � SEM from threeindependent experiments. D, Representative IHC staining for Ki67 in FFPE sections of tumors shown in Fig. 4A. E, H-scores for Ki67 staining (n � 4). F, Cell-cycleanalysis of cells treated with fulvestrant (1 mmol/L), neratinib (200 nmol/L), or both under estrogen-free conditions for 24 hours. Values represent mean � SEMfrom three independent experiments.
Sudhan et al.
Clin Cancer Res; 25(2) January 15, 2019 Clinical Cancer Research778
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

levels in all three ERþ/HER2þ breast cancer cell lines (Fig. 5B).These results were corroborated at themRNA level as we observedsignificant inhibition of CCND1 mRNA in all three ERþ/HER2þ
breast cancer cell lines treated with neratinib � fulvestrant (Fig.5C). These observations were further supported by a significantreduction in Ki67-positive cells in fulvestrant/neratinib–treatedtumors compared with fulvestrant-treated and untreated tumors(Fig. 5D and E). There was no statistically significant difference inthe number of apoptotic cells among all treatments as measuredby TUNEL analysis. Cell-cycle analysis of ERþ/HER2þ breastcancer cell lines also showed a marked reduction in the numberof cells in "S-phase" upon treatment with fulvestrant/neratinib(Fig. 5F).
Cyclin D1 inactivation adds to fulvestrant action against ERþ/HER2þ breast cancer cells
In MCF7 cells, with low levels of HER2, but not in ERþ/HER2gene–amplified cells, treatmentwith fulvestrant resulted in down-regulation of cyclin D1 mRNA and protein levels. Addition ofneratinib to fulvestrant suppressed cyclin D1 expression in ERþ/
HER2þ cells (Fig. 5C), suggesting cyclin D1 transcription iscoregulated by ERa andPI3K/AKT and/orMEK/ERK, downstreamof amplified HER2 (17–19). Phosphorylation of the tumor sup-pressor Rb by the cyclinD1–CDK4/6 complex uncouples Rb fromE2F transcription factors. As a result, E2Fs induce transcription ofgenes necessary for theG1-to-S transition (20). Also, cyclinD1 hasbeen shown tobenecessary for ErbB2 (neu)-driven carcinogenesis(21, 22). Thus, we next examined whether genetic and pharma-cologic inactivation of cyclin D1 would resemble the growth-inhibitory effect of neratinib � fulvestrant against ERþ/HER2þ
cells. Treatment with the CDK4/6 antagonist abemaciclib (23)inhibited growth of BT-474, MDA-MB-361, and UACC893 cells.The combination of abemaciclib/fulvestrant was markedly moreinhibitory than single-agent fulvestrant (Fig. 6A). Similar resultswere observed with two independent cyclin D1 siRNAs (Fig. 6C).In all 3 ERþ/HER2þ cell lines, cyclin D1 knockdown resulted ingrowth inhibition. The combination of cyclin D1 siRNA andfulvestrant was generally more potent at inhibiting cell growththan each intervention alone (Fig. 6C). Because of the transientnature of siRNA-mediated knockdown, growth-modulating
Figure 6.
Cyclin D1 inactivation adds to fulvestrant action against ERþ/HER2þ breast cancer cells. A, Growth assay of cells seeded in a 24-well plate and treated withfulvestrant(1 mmol/L), neratinib (200 nmol/L), abemaciclib (500 nmol/L), or indicated drug combinations, under estrogen-free conditions. Threedays later, cells were stained with crystal violet and viability was quantified on the basis of crystal violet staining intensity. Values are mean � SEM fromthree independent experiments (Student t test). B, Immunoblot analysis of cyclin D1 knockdown efficiency. C, Growth assay of cells treated with fulvestrant(1 mmol/L), neratinib (200 nmol/L) in the presence or absence of cyclin D1 ablation; after 3 days of treatment, cells were stained with crystal violet and viabilitywas determined on the basis of staining intensity of cell monolayers.
Neratinib plus Fulvestrant Overcome ER/HER2 Crosstalk
www.aacrjournals.org Clin Cancer Res; 25(2) January 15, 2019 779
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

effects were assessed within 3 days of drug treatment. MDA-MB-361 cells have a PIK3CA E545K–activating mutation, which wespeculate may dampen their responsiveness to a brief exposure toneratinib compared with longer term treatments (Fig. 2C). Col-lectively, these data suggest a central role of cyclin D1 in limitingthe action of antiestrogens alone against ERþ/HER2þ breastcancer cells. They also provide a plausible explanation for thesynergistic effect of adjuvant fulvestrant/neratinib against ERþ/HER2þ xenografts following treatment with chemotherapy andanti-HER2 therapy (Fig. 1), reminiscent of the results in theExteNET trial.
DiscussionPatients with early-stage ERþ/HER2þ breast cancer receive at
least 5 years of adjuvant antiestrogen therapy with one year oftrastuzumab after completion of primary therapy. Since theadvent of trastuzumab and other HER2-targeting agents, theoutcome of patients with HER2þ breast cancer has vastlyimproved. However, approximately 15% patients still recur withmetastatic disease (6). Neratinib has been recently approved as anextended adjuvant treatment for patients with early-stage HER2þ
breast cancer who have completed trastuzumab-based adjuvanttherapy. The approval was based on the phase III ExteNET trial,which showed a significant improvement in invasive disease-freesurvival in patients receiving 12 months of neratinib treatmentafter completion of adjuvant trastuzumab (7, 8).
In this study, using experimental models of ERþ/HER2þ breastcancer, we attempted to identify potential mechanisms thatwould support the results of the ExteNET trial. We found thatERþ/HER2þMDA-MB-361 tumors in micemaintained on fulves-trant alone, relapsed rapidly compared with mice receiving ner-atinib and fulvestrant (Fig. 1A and D). Tumor recurrences withinthe fulvestrant arm exhibited a marked increase in HER2 andEGFR phosphorylation suggesting that ERþ/HER2þ cancers canadapt to ER blockade through hyperactivation of the ERBB RTKpathway (Fig. 1; Supplementary Fig. S2). These observations areconsistent with previous preclinical and clinical reports of HER2overexpression as a mechanism of intrinsic or acquired resistanceto endocrine therapy (12, 24, 25). Using HER2-overexpressingERþ MCF7 cells, Massarweh and colleagues demonstrated thatresistance to prolonged estrogen deprivation or fulvestrant treat-ment was achieved through HER2 reactivation (12). Similarly,retrospective analysis of the IMPACTneoadjuvant trial comparingthe clinical efficacy of tamoxifen versus aromatase inhibitorsrevealed a lower response rate amongHER2þ tumors, irrespectiveof the antiestrogen arm (26).
In line with HER2-mediated resistance to antiestrogens, wenoted a prompt upregulation in P-HER2 levels upon fulvestranttreatment, in three ERþ/HER2þ breast cancer cell lines (Fig. 2A).In addition, we observed a significant increase in P-EGFR intumors recurring on fulvestrant (Supplementary Fig. S2C–S2F)as well as in cells exposed to fulvestrant for 2 weeks (Supple-mentary Fig. S2G). The addition of trastuzumab to fulvestrantdid not overcome activation of ERBB receptors or AKT (Sup-plementary Fig. S2G). These findings are consistent with severalpreclinical and clinical reports that have associated EGFRactivation with resistance to both endocrine therapy (27–30)and trastuzumab (31, 32). Furthermore, phase II randomizedtrials in patients with ERþ metastatic breast cancer have shownan improvement in progression-free survival with the addition
of the EGFR inhibitor gefitinib to tamoxifen or to anastrazole(33, 34). Similarly, high EGFR expression has been associatedwith lesser benefit to adjuvant trastuzumab in the NCCTGN9831 (Alliance) trial (32). Of note, phase III GeparQuintotrial reported similar survival benefit in patients with ERþ
tumors receiving prolonged HER2 blockade with 6 monthsof neoadjuvant lapatinib, followed by 1 year of adjuvanttrastuzumab (11).
We acknowledge that our mouse model does not entirelyrecapitulate the design of the ExteNET trial. It is extremelychallenging to power mouse studies to evaluate disease recur-rence rates in response to sequential adjuvant treatments in astatistically meaningful manner. To overcome this inherentlimitation of mouse models, we tested the efficacy of trastu-zumab- and neratinib-based treatments in tumor-bearing mice.Even though our model is closer to metastatic setting, webelieve that the overall findings could be extended to adjuvantsettings as well.
HER2 signaling has been previously shown to promoteligand-independent activation of ER through various mechan-isms including ER phosphorylation and modulation of core-gulators of ER transcription (35, 36). We therefore tested theeffect of HER2 inactivation with neratinib on ER activity.Counterintuitive to the above studies, we noted a significantupregulation in ER transcriptional activity upon neratinibtreatment, thereby suggesting that effective ERBB inhibitionleads to rapid restoration of ER function in HER2 gene–ampli-fied cells (Fig. 3). This is in agreement with the reportedinduction of ER activity in primary HER2þ tumors uponshort-term treatment with the HER2 TKI lapatinib (36). Fur-thermore, a retrospective analysis of HER2þ primary tumorstreated with neoadjuvant lapatinib showed a switch from ER�
to ERþ status in about 20% of patients' cancers (37). Otherpreclinical studies have also reported ER activation as a mech-anism of acquired resistance to HER2 targeting in experimentalmodels of HER2þ breast cancer (37–39). Collectively, thesefindings suggest that ER upregulation might occur as a promptresponse to HER2 inhibition and gradually gets hardwired as amechanism of resistance to anti-HER2 therapy.
Although patients with ER– tumors did not gain benefit fromextended adjuvant neratinib, there appeared to be a benefitwhile the patients remained on treatment (8). The discrepancyin treatment outcomes within ERþ versus ER� cohorts could beascribed to several factors. The biology and natural history ofERþ/HER2þ versus ER�/HER2þ breast cancers are very distinct.ER�/HER2þ tumors are at a higher risk of early recurrence (40).Retrospective subgroup analysis of patients receiving 1 year ofadjuvant trastuzumab in the HERA trial revealed a trendtoward inferior 3-year disease-free survival in patients withER� cancers compared with the ERþ cohort, likely due to theirinherent higher risk of early relapse (41). On the other hand,ERþ tumors may recur late and, as such, may require moreprolonged combined blockade of ER–HER2 signaling cross-talk. In line with this notion, the phase III TAnDEM andEGF30008 trials in patients with ERþ/HER2þ metastatic breastcancer, showed an improved PFS with the addition of trastu-zumab to anastrazole and of lapatinib to letrozole, respectively(42, 43). Collectively, these preclinical and clinical observa-tions suggest a plausible explanation to the benefit of com-bined anti-ER and anti-HER2 therapies in the ExteNET andGeparQuinto trials.
Sudhan et al.
Clin Cancer Res; 25(2) January 15, 2019 Clinical Cancer Research780
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

While the question of combined ER/HER2 targeting has beenaddressed to some extent by previous studies (42, 44, 45), themolecular underpinnings of the observed benefit remain lessunderstood. Thus, to further our understanding of potentialmechanisms to explain how addition of the HER2 inhibitorneratinib overcame fulvestrant resistance, we screened for ER-regulated genes that are unresponsive to fulvestrant but remainsensitive to the combination. Gene expression analysis of 196 ER-regulated genes revealed that cyclin D1 was one of the two mainER-responsive genes that remained unaffected by fulvestrant butablated by fulvestrant/neratinib. CyclinD1upregulation has beenshown to drive resistance to both endocrine therapy and anti-HER2 agents. CyclinD1 has also been shown to be a keymediatorof the mitogenic effects of estrogen and thus purported as apotential driver of endocrine resistance (46). Similarly, robustcyclin D1 downregulation has been shown to be required for theantitumor action of HER2-targeted drugs (47). Goel and collea-gues recently demonstrated that tumor recurrences in a geneticallyengineered mouse model of HER2þ breast cancer was primarilymediated by cyclin D1/Cdk4 upregulation and thus could beovercome by combined inhibition of HER2 and Cdk4/6 (48).Mousemammary glands deficient in cyclinD1are largely resistantto the tumor-initiating effects of ErbB2 (21, 22, 49). The mito-genic effects of several distinct growth stimuli converge on cyclinD1 either via its transcriptional upregulation or through increasedstabilization, and ERBB-mediated activation of RAS/RAF/MEK/ERK signaling promotes cyclin D1 transcription throughincreased recruitment of E2F and SP1 transcription factors toCCND1 promoter (17). Likewise, AKT, a major substrate of PI3Kdownstream of the HER2 receptor, posttranslationally stabilizesintracellular cyclin D1 levels by inhibiting its proteasomal deg-radation (50). In the study reported herein, we show that fulves-trant monotherapy yields incomplete suppression of cyclin D1levels in ERþ/HER2þ cells and tumors, whereas addition ofneratinib results in robust ablation of cyclin D1 levels and cell-cycle progression.
In conclusion, we show herein that fulvestrant/neratinib butnot fulvestrant monotherapy maintained complete responses ofERþ/HERþ tumors following treatment with trastuzumab/pacli-taxel or pertuzumab/trastuzumab/paclitaxel, reminiscent of theresults in the phase III ExteNET trial. We found that ERþ/HER2þ
tumors rapidly evade ER blockade through ERBB pathway hyper-activation and, conversely, inhibition of ERBB tyrosine kinaseactivity with neratinib stoked up ER activity. Finally, treatmentwithneratinib/fulvestrant but not fulvestrant alone reduced cyclinD1 mRNA and protein levels, and induced cell-cycle arrest,
suggesting that simultaneous targeting of both ER and HER2 axesis required to overcome compensatory crosstalk between ER andamplified HER2.
Disclosure of Potential Conflicts of InterestA. S. Lalani is an employee of and holds ownership interest (including
patents) in Puma Biotechnology, Inc. R. Bryce is an employee of and holdsownership interest (including patents) in PumaBiotechnology, Inc. A. Auerbachis an employee of and holds ownership interest (including patents) in PumaBiotechnology, Inc. C. L. Arteaga reports receiving research grants from PumaBiotechnology, Inc., Pfizer, Lilly, Bayer, Takeda, and Radius, holds ownershipinterest (including patents) in Provista and Y-TRAP, is a consultant/advisoryboard member for Novartis, Merck, Lilly, Symphogen, Daiichi Sankyo, Radius,Taiho Oncology, H3Biomedicine, OrigiMed, Puma Biotechnology, and Sanofi,and reports other remuneration from the Komen Foundation. No potentialconflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: D.R. Sudhan, L.J. Schwarz, A.S. Lalani, R. Bryce,C.L. ArteagaDevelopment of methodology: L.J. Schwarz, C.L. ArteagaAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): D.R. Sudhan, L.J. Schwarz, A. Guerrero-Zotano,M.J. Nixon, S. Croessmann, P.I. Gonzalez-Ericsson, M. Sanders, R.E. Cutler,C.L. ArteagaAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): D.R. Sudhan, L.J. Schwarz, A. Guerrero-Zotano,M.J. Nixon, S. Croessmann, P.I. Gonzalez-Ericsson, M. Sanders, J.M. Balko,A. Auerbach, C.L. ArteagaWriting, review, and/or revision of themanuscript:D.R. Sudhan, L.J. Schwarz,A. Guerrero-Zotano, M.J. Nixon, S. Croessmann, P.I. Gonzalez-Ericsson,M. Sanders, J.M. Balko, R.E. Cutler, A.S. Lalani, R. Bryce, A. Auerbach,C.L. ArteagaAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): D.R. Sudhan, A.S. Lalani, A. Auerbach,C.L. ArteagaStudy supervision: C.L. Arteaga
AcknowledgmentsThis study was supported by NIH Breast SPORE grant P50 CA098131,
Vanderbilt-Ingram Cancer Center P30 CA68485, UTSW Simmons CancerCenter P30 CA142543, CPRIT RR170061 grant, Susan G. Komen Breast CancerFoundation grant SAC100013 (CLA), and a grant from the Breast CancerResearch Foundation (CLA). J.M. Balko was supported by Susan G. KomenCareer Catalyst Grant CCR14299052 and NIH/NCI R00CA181491.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received April 13, 2018; revised August 9, 2018; accepted September 26,2018; published first October 1, 2018.
References1. Arteaga CL, Sliwkowski MX, Osborne CK, Perez EA, Puglisi F, Gianni L.
Treatment of HER2-positive breast cancer: current status and future per-spectives. Nat Rev Clin Oncol 2011;9:16–32.
2. SlamonDJ, Clark GM,Wong SG, LevinWJ, Ullrich A,McGuireWL. Humanbreast cancer: correlation of relapse and survival with amplification of theHER-2/neu oncogene. Science 1987;235:177–82.
3. Swain SM, Baselga J, Kim SB, Ro J, Semiglazov V, Campone M, et al.Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastaticbreast cancer. N Engl J Med 2015;372:724–34.
4. Vogel CL, CobleighMA, Tripathy D, Gutheil JC, Harris LN, Fehrenbacher L,et al. Efficacy and safety of trastuzumab as a single agent in first-linetreatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol2002;20:719–26.
5. MartyM,Cognetti F,MaraninchiD, Snyder R,Mauriac L, Tubiana-HulinM,et al. Randomized phase II trial of the efficacy and safety of trastuzumabcombined with docetaxel in patients with human epidermal growth factorreceptor 2-positive metastatic breast cancer administered as first-line treat-ment: the M77001 study group. J Clin Oncol 2005;23:4265–74.
6. Goldhirsch A, Gelber RD, Piccart-Gebhart MJ, de Azambuja E, Procter M,Suter TM, et al. 2 years versus 1 year of adjuvant trastuzumab for HER2-positive breast cancer (HERA): an open-label, randomised controlled trial.Lancet 2013;382:1021–8.
7. Chan A, Delaloge S, Holmes FA,Moy B, Iwata H, Harvey VJ, et al. Neratinibafter trastuzumab-based adjuvant therapy in patients with HER2-positivebreast cancer (ExteNET): a multicentre, randomised, double-blind, place-bo-controlled, phase 3 trial. Lancet Oncol 2016;17:367–77.
Neratinib plus Fulvestrant Overcome ER/HER2 Crosstalk
www.aacrjournals.org Clin Cancer Res; 25(2) January 15, 2019 781
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

8. Martin M, Holmes FA, Ejlertsen B, Delaloge S, Moy B, Iwata H,et al. Neratinib after trastuzumab-based adjuvant therapy in HER2-positive breast cancer (ExteNET): 5-year analysis of a randomised,double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2017;18:1688–700.
9. Unni N, Sudhan DR, Arteaga CL. Neratinib: Inching up on the cure rate ofHER2þ breast cancer? Clin Cancer Res 2018;24:3483–5.
10. SinghH,WalkerAJ, Amiri-Kordestani L,Cheng J, Tang S, Balcazar P, et al. U.S. Food and drug administration approval: Neratinib for the extendedadjuvant treatment of early stage HER2-positive breast cancer. Clin CancerRes 2018;24:3486–91.
11. UntchM, vonMinckwitz G, Gerber B, SchemC, RezaiM, Fasching PA, et al.Survival analysis after neoadjuvant chemotherapy with trastuzumab orlapatinib in patients with human epidermal growth factor receptor 2-positive breast cancer in the GeparQuinto (G5) study (GBG 44). J ClinOncol 2018;36:1308–16.
12. Massarweh S, Osborne CK, Jiang S, Wakeling AE, Rimawi M,Mohsin SK, et al. Mechanisms of tumor regression and resistanceto estrogen deprivation and fulvestrant in a model of estrogenreceptor-positive, HER-2/neu-positive breast cancer. Cancer Res 2006;66:8266–73.
13. Bender LM, Nahta R. Her2 cross talk and therapeutic resistance in breastcancer. Front Biosci 2008;13:3906–12.
14. Kurebayashi J, Kanomata N, Yamashita T, Shimo T, Mizutoh A, Moriya T,et al. Prognostic value of phosphorylated HER2 in HER2-positive breastcancer patients treated with adjuvant trastuzumab. Breast Cancer 2015;22:292–9.
15. Spears M, Pederson HC, Lyttle N, Gray C, Quintayo MA, Brogan L, et al.Expression of activated type I receptor tyrosine kinases in early breastcancer. Breast Cancer Res Treat 2012;134:701–8.
16. Balko JM, Giltnane JM, Wang K, Schwarz LJ, Young CD, Cook RS, et al.Molecular profiling of the residual disease of triple-negative breast cancersafter neoadjuvant chemotherapy identifies actionable therapeutic targets.Cancer Discov 2014;4:232–45.
17. Lee RJ, Albanese C, Fu M, D'Amico M, Lin B, Watanabe G, et al. CyclinD1 is required for transformation by activated Neu and is inducedthrough an E2F-dependent signaling pathway. Mol Cell Biol 2000;20:672–83.
18. Sabbah M, Courilleau D, Mester J, Redeuilh G. Estrogen induction of thecyclin D1 promoter: involvement of a cAMP response-like element. ProcNatl Acad Sci U S A 1999;96:11217–22.
19. Yakes FM, Chinratanalab W, Ritter CA, King W, Seelig S, Arteaga CL.Herceptin-induced inhibition of phosphatidylinositol-3 kinase and AktIs required for antibody-mediated effects on p27, cyclinD1, and antitumoraction. Cancer Res 2002;62:4132–41.
20. Knudsen ES, Knudsen KE. Tailoring to RB: tumour suppressor status andtherapeutic response. Nat Rev Cancer 2008;8:714–24.
21. YuQ,Geng Y, Sicinski P. Specific protection against breast cancers by cyclinD1 ablation. Nature 2001;411:1017–21.
22. Yu Q, Sicinska E, Geng Y, Ahnstrom M, Zagozdzon A, Kong Y, et al.Requirement for CDK4 kinase function in breast cancer. Cancer Cell2006;9:23–32.
23. Sledge GW Jr, ToiM,Neven P, Sohn J, Inoue K, Pivot X, et al. MONARCH2:Abemaciclib in combination with fulvestrant in women with HRþ/HER2-advanced breast cancer who had progressed while receiving endocrinetherapy. J Clin Oncol 2017;35:2875–84.
24. Prat A, Baselga J. The role of hormonal therapy in the management ofhormonal-receptor-positive breast cancer with co-expression of HER2. NatClin Pract Oncol 2008;5:531–42.
25. Lipton A, Ali SM, Leitzel K, Demers L, Chinchilli V, Engle L, et al. Elevatedserum Her-2/neu level predicts decreased response to hormone therapy inmetastatic breast cancer. J Clin Oncol 2002;20:1467–72.
26. Dowsett M, Ebbs SR, Dixon JM, Skene A, Griffith C, Boeddinghaus I,et al. Biomarker changes during neoadjuvant anastrozole, tamoxifen,or the combination: influence of hormonal status and HER-2 inbreast cancer–a study from the IMPACT trialists. J Clin Oncol 2005;23:2477–92.
27. Zhang X, Diaz MR, Yee D. Fulvestrant regulates epidermal growth factor(EGF) family ligands to activate EGF receptor (EGFR) signaling in breastcancer cells. Breast Cancer Res Treat 2013;139:351–60.
28. Frogne T, Benjaminsen RV, Sonne-Hansen K, Sorensen BS, Nexo E, Laen-kholmAV, et al. Activation of ErbB3, EGFRandErk is essential for growth ofhumanbreast cancer cell lineswith acquired resistance to fulvestrant. BreastCancer Res Treat 2009;114:263–75.
29. Okubo S, Kurebayashi J, Otsuki T, Yamamoto Y, Tanaka K, Sonoo H.Additive antitumour effect of the epidermal growth factor receptor tyrosinekinase inhibitor gefitinib (Iressa, ZD1839) and the antioestrogen fulves-trant (Faslodex, ICI 182,780) in breast cancer cells. Br J Cancer2004;90:236–44.
30. Massarweh S, Osborne CK, Creighton CJ, Qin L, Tsimelzon A, Huang S,et al. Tamoxifen resistance in breast tumors is driven by growth factorreceptor signaling with repression of classic estrogen receptor genomicfunction. Cancer Res 2008;68:826–33.
31. Ritter CA, Perez-Torres M, Rinehart C, Guix M, Dugger T, Engelman JA,et al. Human breast cancer cells selected for resistance to trastuzumab invivo overexpress epidermal growth factor receptor and ErbB ligands andremain dependent on the ErbB receptor network. Clin Cancer Res2007;13:4909–19.
32. ChengH, BallmanK, VassilakopoulouM,DueckAC, ReinholzMM, TennerK, et al. EGFR expression is associated with decreased benefit from tras-tuzumab in the NCCTG N9831 (Alliance) trial. Br J Cancer 2014;111:1065–71.
33. Cristofanilli M, Valero V, Mangalik A, Royce M, Rabinowitz I, ArenaFP, et al. Phase II, randomized trial to compare anastrozole combinedwith gefitinib or placebo in postmenopausal women with hormonereceptor-positive metastatic breast cancer. Clin Cancer Res 2010;16:1904–14.
34. Osborne CK, Neven P, Dirix LY, Mackey JR, Robert J, Underhill C, et al.Gefitinib or placebo in combination with tamoxifen in patients withhormone receptor-positive metastatic breast cancer: a randomized phaseII study. Clin Cancer Res 2011;17:1147–59.
35. Osborne CK, Shou J, Massarweh S, Schiff R. Crosstalk between estrogenreceptor and growth factor receptor pathways as a cause for endocrinetherapy resistance in breast cancer. Clin Cancer Res 2005;11(2 Pt2):865s–70s.
36. Shou J, Massarweh S, Osborne CK, Wakeling AE, Ali S, Weiss H, et al.Mechanisms of tamoxifen resistance: increased estrogen receptor-HER2/neu cross-talk in ER/HER2-positive breast cancer. J Natl Cancer Inst2004;96:926–35.
37. Giuliano M, Hu H, Wang YC, Fu X, Nardone A, Herrera S, et al. Upregula-tion of ER signaling as an adaptive mechanism of cell survival in HER2-positive breast tumors treated with anti-HER2 therapy. Clin Cancer Res2015;21:3995–4003.
38. XiaW, Bacus S, Hegde P, Husain I, Strum J, Liu L, et al. Amodel of acquiredautoresistance to apotent ErbB2 tyrosine kinase inhibitor and a therapeuticstrategy to prevent its onset in breast cancer. Proc Natl Acad Sci U S A2006;103:7795–800.
39. Sabnis G, Schayowitz A, Goloubeva O, Macedo L, Brodie A. Trastuzumabreverses letrozole resistance and amplifies the sensitivity of breast cancercells to estrogen. Cancer Res 2009;69:1416–28.
40. Vaz-Luis I, Ottesen RA, Hughes ME, Marcom PK, Moy B, Rugo HS,et al. Impact of hormone receptor status on patterns of recurrenceand clinical outcomes among patients with human epidermalgrowth factor-2-positive breast cancer in the National Comprehen-sive Cancer Network: a prospective cohort study. Breast Cancer Res2012;14:R129.
41. Untch M, Gelber RD, Jackisch C, Procter M, Baselga J, Bell R, et al.Estimating themagnitude of trastuzumab effects within patient subgroupsin the HERA trial. Ann Oncol 2008;19:1090–6.
42. Kaufman B, Mackey JR, Clemens MR, Bapsy PP, Vaid A, Wardley A, et al.Trastuzumab plus anastrozole versus anastrozole alone for the treat-ment of postmenopausal women with human epidermal growth factorreceptor 2-positive, hormone receptor-positive metastatic breast cancer:results from the randomized phase III TAnDEM study. J Clin Oncol2009;27:5529–37.
43. Bauerfeind I, Elling D, Heinemann V. Lapatinib in the treatment ofhormone receptor-positive/ErbB2-positive breast cancer. Breast Care2010;5(s1):13–5.
44. Johnston S, Pippen J Jr, Pivot X, Lichinitser M, Sadeghi S, Dieras V, et al.Lapatinib combinedwith letrozole versus letrozole andplaceboasfirst-line
Clin Cancer Res; 25(2) January 15, 2019 Clinical Cancer Research782
Sudhan et al.
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

therapy for postmenopausal hormone receptor-positive metastatic breastcancer. J Clin Oncol 2009;27:5538–46.
45. Huober J, Fasching PA, Barsoum M, Petruzelka L, Wallwiener D,Thomssen C, et al. Higher efficacy of letrozole in combination withtrastuzumab compared to letrozole monotherapy as first-line treat-ment in patients with HER2-positive, hormone-receptor-positive met-astatic breast cancer - results of the eLEcTRA trial. Breast 2012;21:27–33.
46. Butt AJ, McNeil CM, Musgrove EA, Sutherland RL. Downstream targets ofgrowth factor and oestrogen signalling and endocrine resistance: thepotential roles of c-Myc, cyclin D1 and cyclin E. Endocr Relat Cancer2005;12Suppl 1:S47–59.
47. Lenferink AE, Busse D, Flanagan WM, Yakes FM, Arteaga CL. ErbB2/neukinase modulates cellular p27(Kip1) and cyclin D1 through multiplesignaling pathways. Cancer Res 2001;61:6583–91.
48. Goel S, Wang Q,Watt AC, Tolaney SM, Dillon DA, Li W, et al. Overcomingtherapeutic resistance in HER2-positive breast cancers with CDK4/6 inhi-bitors. Cancer Cell 2016;29:255–69.
49. Landis MW, Pawlyk BS, Li T, Sicinski P, Hinds PW. Cyclin D1-dependentkinase activity in murine development and mammary tumorigenesis.Cancer Cell 2006;9:13–22.
50. Diehl JA, Cheng M, Roussel MF, Sherr CJ. Glycogen synthase kinase-3betaregulates cyclin D1 proteolysis and subcellular localization. Genes Dev1998;12:3499–511.
www.aacrjournals.org Clin Cancer Res; 25(2) January 15, 2019 783
Neratinib plus Fulvestrant Overcome ER/HER2 Crosstalk
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131

2019;25:771-783. Published OnlineFirst October 1, 2018.Clin Cancer Res Dhivya R. Sudhan, Luis J. Schwarz, Angel Guerrero-Zotano, et al.
Breast Cancers: Implications to the ExteNET Trial+/HER2+ER/HER2 Crosstalk and Maintains Complete Responses of ER
Extended Adjuvant Therapy with Neratinib Plus Fulvestrant Blocks
Updated version
10.1158/1078-0432.CCR-18-1131doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2018/09/29/1078-0432.CCR-18-1131.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/25/2/771.full#ref-list-1
This article cites 50 articles, 25 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/25/2/771.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/25/2/771To request permission to re-use all or part of this article, use this link
on July 5, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 1, 2018; DOI: 10.1158/1078-0432.CCR-18-1131