Embed Size (px)
Citation preview

J Hepatobiliary Pancreat Surg (2004) 11:434–437DOI 10.1007/s00534-004-0922-7
Familial pancreatic cancer: report of one Japanese family
Koji Yamaguchi1, Hisafumi Kinoshita2, Koji Hokazono1, Masahiko Kawamoto1, Hirofumi Yamamoto1,Atsushi Sugitani1, Kazuhiro Mizumoto1, and Masao Tanaka1
1 Department of Surgery and Oncology, Graduate School of Medical Sciences, Kyushu University, Fukuoka 812-8582, Japan2 Department of Surgery, School of Medicine, Kurume University, Kurume, Japan
urged us to review 103 patients with pancreatic cancerwho had undergone surgical resection at our institution,and we found one family with possible familial pancre-atic cancer. In this communication, we report familialpancreatic carcinomas occurring in two first-degreerelatives and one third-degree relative.
Case report
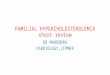
A 50-year-old Japanese woman had obstructive jaun-dice (serum level of total bilirubin, 7.2 mg/dl (normal,�1.0mg/dl) and visited us for surgical treatment. Herfamily history included pancreatic cancer in her motherand in one of her uncles on her father’s side (Fig. 1).
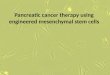
Imagings showed a pancreatic head tumor, 3cm indiameter (Fig. 2). The main pancreatic duct proximal tothe tumor was dilated, with atrophy of the pancreaticparenchyma. Intrahepatic and extrahepatic bile ductswere dilated due to occlusion by the pancreatic tumor.Serum levels of carcinoembryonic antigen (CEA) andcarbohydrate antigen (CA) 19-9 were mildly elevated,to 4.3 ng/ml (�2.5ng/ml) and 282.4 U/ml (�37 U/ml),respectively. Pylorus-preserving pancreatoduodenec-tomy with portal vein resection was done on March 10,2000. After the operation, she underwent transarterialhepatic chemotherapy (with 5-fluorouracil [5-FU])and external radiation (50 Gy). The histopathologicaldiagnosis was well-differentiated adenocarcinoma ofthe pancreatic head (Fig. 3). One regional lymph node(no. 13) showed metastasis by the carcinoma. She hasbeen well for 38 months after the operation, with nosigns of recurrence.
Family history
The patient’s mother died of pancreatic head carci-noma, at the age of 71, in our hospital. Imagings
AbstractMost familial pancreatic carcinomas have been reported fromEuropean countries and the United States, and there has beenonly one report from Japan. A 50-year-old Japanese womanpresented with a pancreatic head mass and underwentpylorus-preserving pancreatoduodenectomy with portal veinresection. The histological diagnosis was well-differentiatedadenocarcinoma of the head of the pancreas. Her mother diedof pancreatic head carcinoma, which had been shown on com-puted tomography at the age of 70 years. One of her uncles onher father’s side had had pancreatic tail carcinoma, and at theage of 59, had undergone distal pancreatectomy, splenectomy,wedge resection of the liver, and partial resection of the colon.The histological diagnosis was moderately differentiated tu-bular adenocarcinoma of the pancreas. He had had a subtotalgastrectomy for early gastric cancer (tubular adenocarcinomalimited to the mucosa) at the age of 53. He died of recurrenceof the pancreatic tail carcinoma 3 months after the distalpancreatectomy had been performed. This communicationreports a second Japanese family with familial pancreaticcancer, as shown by pancreatic carcinomas in two first-degreerelatives and in one third-degree relative.
Key words Familial pancreatic cancer
Introduction
The clinical course of patients with pancreatic carci-noma remains dismal, and improvements in the clinicalcourse of patients with pancreatic cancer is desired.Familial pancreatic carcinoma has become a target todiscover early pancreatic carcinoma in the UnitedStates. However, only one case has been reported inJapan.1 This may be due to a really low incidence offamilial pancreatic carcinoma, or it may be due to a lackof interest in this entity in Japan. This background
Offprint requests to: K. YamaguchiReceived: January 14, 2004 / Accepted: June 9, 2004

K. Yamaguchi et al.: Familial pancreatic cancer in a Japanese family 435
noma, at the age of 53 years. The histological diagnosiswas tubular adenocarcinoma of the stomach limited tothe mucosa. No lymph node metastasis was evident. Atthe age of 59, he had undergone distal pancreatectomywith combined resection of the transverse colon, forpancreatic tail carcinoma, at Kurume University Hospi-tal. Figure 5 shows a computed tomography scan of the
Fig. 1. Family tree shows that the presentpatient, her mother, and one of her uncleshad a pancreatic carcinoma
Fig. 2. Computed tomography in the patient shows a pancre-atic head mass, 3cm in diameter
Fig. 3. Section of the resected specimen shows malignantglands invading the surrounding pancreas. H&E, �85
3 months before her death showed a pancreatic headmass, 3cm in diameter (Fig. 4). Unfortunately, neithersurgical resection nor autopsy was done.
One of the patient’s uncles on her father’s side hadundergone subtotal gastrectomy for early gastric carci-
Fig. 4. Computed tomography in the patient’s mother demon-strates a pancreatic head mass, 3cm in diameter
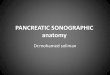
Fig. 5. Computed tomography in the patient’s uncle displays apancreatic body mass, 3cm in diameter

436 K. Yamaguchi et al.: Familial pancreatic cancer in a Japanese family
pancreatic mass. The histological diagnosis was moder-ately differentiated tubular adenocarcinoma of the pan-creatic tail invading the colon, liver, splenic artery, andspleen (Fig. 6). Intraoperative radiation therapy (30 Gy)was done. He died of local and metastatic recurrences ofthe pancreatic cancer 3 months after the distal pancre-atectomy had been performed.
Discussion
Familial pancreatic cancer is defined as pancreatic carci-noma occurring in at least two family members who arefirst-degree relatives. In the present family, diagnosis ofpancreatic duct carcinoma was proved by histology ofthe resected specimen in the patient and one of heruncles (third-degree relative). Pancreatic carcinoma inher mother (first-degree relative) was diagnosed bycomputed tomography, but histological diagnosis wasnot obtained. Strictly speaking, histological or cytologi-cal confirmation was mandatory for the diagnosis ofpancreatic cancer in her mother. The incidence ofpancreatic carcinoma is not high (about 1 per 10000people) and the resectability of pancreatic cancer re-mains low, being about 10%–30%. Therefore, histologi-cal or cytological confirmation of pancreatic carcinomafrom a resected specimen is sometimes difficult.
To our knowledge, there has been only one case re-port of familial pancreatic cancer in Japan.1 Accordingto the national registration of pancreatic cancer inJapan, the incidence of a family history (not limitedto first-degree relatives) of pancreatic cancer is 3.7%(48/1296).2 Studies over the past three decades in Euro-pean countries and the United States of America haveshown that 4%–16% of patients with pancreatic cancer
had a family history of pancreatic cancer.3–5 Therefore,it is possible that more cases of familial pancreatic can-cer may exist in Japan, as well as in western countries.This prompted us to review our series of 103 patientswith pancreatic cancer. Of these patients, 1 was found tobe a possible familial pancreatic cancer.
Rieder et al.4 reported that a shift towards a youngerage at diagnosis in familial pancreatic cancer may in-dicate a genetic predisposition and/or changes in pat-terns of exogenous risk factors. In the present family,the patients with pancreatic cancer were a 50-year-oldwoman, a 59-year-old man, and a 71 year-old woman, allof whom were somewhat younger than the patients withusual pancreatic cancer in Japan, the incidence by de-cades being 21.7% (5053/23 302) in the sixth decade,34.3% (8003/23 302; the peak), in the seventh decade,and 26.4% (6147/23 302) in the eighth decade, accordingto the national registration of pancreatic cancer.5
Familial pancreatic cancer suggests a high possibilityof occurrence of pancreatic cancer in members of thefamily. In families where three first-degree relatives hadbeen diagnosed as having pancreatic cancer, the risk tothe other individuals of developing pancreatic cancerrose to 57 times the baseline risk.6 The risk andincidence of pancreatic cancer is extraordinarily highamong first-degree relatives in a family with familialpancreatic cancer in which at least three first-degreerelatives have already been diagnosed as having pancre-atic cancer.7 Rulyak et al. and Rulyak and Brentnall9
proposed the endoscopic screening of carefully selectedmembers of families with familial pancreatic cancerto increase patient life expectancy in a cost-effectivemanner. Klein et al.3 from Johns Hopkins University,reported that individuals with a family history of pan-creatic cancer in multiple first-degree relatives hada high risk of pancreatic cancer themselves, and theidentification of such high-risk individuals would helpclinicians to target screening programs and to developpreventive interventions with the hope of reducing themortality of pancreatic cancer in these families. In thepresent family, screening of the patient’s three brothers(first-degree relatives) was advised, but they were reluc-tant to undergo screening.
Inherited cancer syndromes include familial atypicalmultiple-mole melanoma, Peutz-Jeghers syndrome, he-reditary breast-ovarian cancer, hereditary pancreatitis,and hereditary nonpolyposis colorectal cancer. Thesesyndromes arise as a result of germline mutations inthe BRCA2, p16 (familial atypical multiple-molemelanoma), mismatch repair (hereditary nonpolyposiscolorectal cancer), and STK11 (Peutz-Jeghers syn-drome) genes. Hahn et al.10 examined BRCA2 germlinemutations in 26 European families with familial pancre-atic cancer and concluded that 19% of the families hadeither a frameshift mutation or an unclassified variant of
Fig. 6. Section of the resected specimen from the patient’suncle shows moderately differentiated adenocarcinoma of thepancreas. H&E, �85

K. Yamaguchi et al.: Familial pancreatic cancer in a Japanese family 437
BRCA2. Murphy et al.11 also confirmed an increasedrisk of pancreatic cancer in individuals with BRCA2mutations, and they identified germline BRCA2 muta-tions as the most common inherited genetic alteration.In our series of patients, we have not examined thegenetic changes to date.
After reviewing 103 Japanese patients with pan-creatic cancer who underwent a surgical resection,one family with possible familial pancreatic cancer wasfound. We would like to draw Japanese clinicians’ at-tention to familial pancreatic cancer, because suchfamilies may be a target to screen for early pancreaticcancer.
References
1. Toyama K, Noto M, Sakaguchi T (1984) Pancreatic cancer infather and daughter. Gan No Rinsho (Jpn J Cancer Clinics) 30:1331–1336
2. Japan Pancreas Society (2000) Report of national rergistration ofpancreatic cancer, 1998. Suizo (J Jpn Panc Soc) 15:179–211
3. Klein AP, Hruban RH, Brune KA (2001) Familial pancreaticcancer. Cancer J 7:266–273
4. Rieder H, Sina-Frey M, Ziegler A (2002) German national casecollection of familial pancreatic cancer—clinical-genetic analysisof the first 21 families. Onkologie 25:262–226
5. Japan Pancreas Society (2003) Report of national registration ofpancreatic cancer, 20-year summary. Suizo (J Jpn Panc Soc)18:101–169
6. Hruban RH, Canto MI, Yeo CJ (2001) Prevention of pancreaticcancer and strategies for management of familial pancreaticcancer. Dig Dis 19:76–84
7. Tersmette AC, Petersen GM, Offerhaus GJ (2001) Increased riskof incident pancreatic cancer among first-degree relatives of pa-tients with familial pancreatic cancer. Clin Cancer Res 7:738–744
8. Rulyak SJ, Kimmey MB, Veenstra DL, Brentnall TA (2003)Cost-effectiveness of pancreatic cancer screening in familialpancreatic cancer kindreds. Gastrointest Endosc 57:23–29
9. Rulyak SJ, Brentnall TA (2001) Inherited pancreatic cancer:surveillance and treatment strategies for affected families.Pancreatology 1:477–485
10. Hahn SA, Greenhalf B, Ellis I (2003) BRCA2 germline mutationsin familial pancreatic carcinoma (comment). J Natl Cancer Inst95:214–221
11. Murphy KM, Brune KA, Griffin C (2002) Evaluation of candidategenes MAP2K4, MADH4, ACVR1B, and BRCA2 in familialpancreatic cancer: deleterious BRCA2 mutations in 17%. CancerRes 62:3789–3793