Embed Size (px)
Citation preview

人 間
J R
09-028
アフガニスタン国 リプロダクティブヘルスプロジェクト
終了時評価調査報告書
(2009年)
平成 21 年6月
人間開発部
独立行政法人国際協力機構

アフガニスタン国 リプロダクティブヘルスプロジェクト
終了時評価調査報告書
(2009年)
平成 21 年6月
人間開発部
独立行政法人国際協力機構

目 次 序 文 地 図 写 真 略語表 評価調査結果要約表 第1章 終了時評価調査の概要 ·································································································1 1-1 終了時評価調査の背景と目的 ··················································································1 1-2 対象プロジェクトの概要(PDM Ver.4に基づく) ···················································1 1-3 調査団の構成 ···········································································································3 1-4 調査日程 ···················································································································3 1-5 主要面談者 ···············································································································4
第2章 終了時評価の方法 ········································································································7 2-1 評価調査の流れ ········································································································7 2-2 評価5項目 ···············································································································7 2-3 評価のデザイン ········································································································8 2-4 情報・データ収集方法 ··························································································· 10 2-5 PDM························································································································ 10
第3章 評価結果 ····················································································································· 11 3-1 プロジェクト実施プロセス ···················································································· 11 3-2 プロジェクトの実績 ······························································································· 11 3-3 評価5項目による評価結果 ···················································································· 17 3-4 結 論 ···················································································································· 22
第4章 提言と教訓 ················································································································· 23 4-1 提 言 ···················································································································· 23 4-2 教 訓 ···················································································································· 23
第5章 所 感 ························································································································ 24 5-1 母子保健団員所感 ·································································································· 24 5-2 団長所感 ················································································································· 27
付属資料 1.実施協議ミニッツ及び合同評価レポート ····································································· 31 2.評価グリッド ················································································································· 67

3.質問票 ···························································································································· 71 4.質問票集計結果 ············································································································· 81 5.ワークショップ結果 ······································································································ 87

序 文
本プロジェクトは、リプロダクティブ・ヘルスに係る指標が世界的にも最も劣悪な状況にある
アフガニスタン国において、保健サービス基礎パッケージ(BPHS)、病院サービス必須パッケー
ジ(EPHS)に基づいた母親と新生児への保健サービス提供者ならびに保健行政官の能力向上を目
的として、2004年9月から5年間の予定で技術協力プロジェクトとして実施されています。
2009年9月にプロジェクトの終了を迎えるにあたり、プロジェクト目標の達成状況を把握する
とともに、活動実施プロセスにおける効果発現の貢献要因・阻害要因を分析して他の類似プロジ
ェクトへの教訓を導くことを目的に、終了時評価調査団を派遣しました。
この報告書は、アフガニスタン国側との合同評価の結果に基づき取りまとめたものであり、今
後の技術協力事業を効果的かつ効率的に実施していくための参考として、広く活用されることを
願うものです。
ここに、本調査にご協力とご支援をいただいた関係各位に対し、心より感謝申し上げます。
平成21年6月
独立行政法人国際協力機構 人間開発部長 西脇 英隆

Qarah BaghKhas Uruzgan
Spin Buldak
Chehar Borjak
Deh Shu
Kadesh
Anar Darreh
Shindand-
OwbehKarokh
Towraghondi
QeysarTokzar
Andkhvoy
Dowlatabad
KeleftJeyretan
Shulgarah
Kholm
Khanabad
Rostaq
Farkhar
JormEshkashem
Qala-I-Panjeh
Khavak
Dowshi
Now Zad
Dowlat Yar
Kajaki
Delara
m
Asadabad
Jalalabad
Sharan
Ghazni
Qalat
Tirin Kot
Kandahar
Samangan
Baghlan
Sheberghan
Meymaneh
Qala-I-Naw
Chaghcharan
Farah
Lashkar Gah
Taluqan
Fayzabad
Charikar
Puli Alam
Zaranj
Khost
Sari Pul
MazariSharif Kunduz
Nuristan
MeydanShahr
MahmudRaqi
Gardez
MehtarlamKabul
FARAH
NIMROZ
HILMAND KANDAHAR
ZABULPAKTIKA
GHAZNI
URUZGAN
DAYKUNDI
LOGAR
KHOST
TAKHAR
BADAKHSHAN
BAGHLAN
BALKH
JAWZJAN
SARI PUL
FARYAB
BADGHIS
GHOR
PARWAN
PANJSHER
KABULWARDAK
PAKTYA
LA
GH
MAN
SAMANGAN
KUNDUZ
NURISTAN
NANGARHAR
KAPISA
HiratBamyan
HIRAT
KUNARBAMYAN
Zhob
Chaman
Quetta
Zabol
Zahedan
Gushgy
Kiroya
Kerki
Dusti Khorugh
Qurghonteppa(Kurgan-Tyube)
Mary
Mardan
Peshawar
Rawalpindi
Term
iz
Gilgit
Taybad
Tank
Bannu
Islamabad
TURKMENISTAN
TAJIKISTAN
PAKISTAN
UZBEKISTANIN
DIA
Jammu
and
Kashmir
CH
IN
A
IS
LA
MI
C
RE
PU
BL
IC
O
F
IR
AN
Farah
Helmand
Gowd-e Zereh
Haru
t
Khash
Rowd-e L
urah
Arg
hand
ab
Gus
hgy
Murghob
Dar
ya-ye Panj
Amu Darya
Tedzhen
Harirud
Indu
s
Pamir
Tarnak
Morghab
Murgab
Helmand
Kun
ar
Zhob
Chaman
Quetta
Zabol
Zahedan
Gushgy
Kiroya
Kerki
Dusti Khorugh
Qurghonteppa(Kurgan-Tyube)
Mary
Mardan
Peshawar
Rawalpindi
Term
iz
Gilgit
Taybad
Tank
BannuQarah Bagh
Khas Uruzgan
Spin Buldak
Chehar Borjak
Deh Shu
Kadesh
Anar Darreh
Shindand-
OwbehKarokh
Towraghondi
QeysarTokzar
Andkhvoy
Dowlatabad
KeleftJeyretan
Shulgarah
Kholm
Khanabad
Rostaq
Farkhar
JormEshkashem
Qala-I-Panjeh
Khavak
Dowshi
Now Zad
Dowlat Yar
Kajaki
Delara
m
Asadabad
Jalalabad
Sharan
Ghazni
Qalat
Tirin Kot
Kandahar
Samangan
Baghlan
Sheberghan
Meymaneh
Qala-I-Naw
Chaghcharan
Farah
Hirat
Lashkar Gah
Bamyan
Taluqan
Fayzabad
Charikar
Puli Alam
Zaranj
Khost
Sari Pul
MazariSharif Kunduz
Nuristan
MeydanShahr
MahmudRaqi
Gardez
MehtarlamKabul
Islamabad
Hi
nd
u K u
sh
Peywar Pass
Khyber Pass
FARAH
NIMROZ
HILMAND KANDAHAR
ZABULPAKTIKA
GHAZNI
URUZGAN
DAYKUNDI
LOGAR
KHOST
TAKHAR
BADAKHSHAN
BAGHLAN
BALKH
JAWZJAN
SARI PUL
BAMYAN
FARYAB
BADGHIS
HIRAT GHOR
PARWAN
PANJSHER
KABULWARDAK
KUNAR
PAKTYA
LA
GH
MAN
SAMANGAN
KUNDUZ
NURISTAN
NANGARHAR
KAPISA
TURKMENISTAN
TAJIKISTAN
PAKISTAN
UZBEKISTANIN
DIA
Jammu
and
Kashmir
CH
IN
A
IS
LA
MI
C
RE
PU
BL
IC
O
F
IR
AN
AFGHANISTAN
Map No. 3958 Rev. 5 UNITED NATIONSOctober 2005
Department of Peacekeeping OperationsCartographic Section
National capital
Provincial capital
Town, village
Airports
International boundary
Provincial boundary
Main road
Secondary road
Railroad
(
0
0 50 100 150 200 250 km
50 100 150 mi
The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations.
Dotted line represents approximately the Line of Controlin Jammu and Kashmir agreed upon by India and Pakistan.The final status of Jammu and Kashmir has not yet beenagreed upon by the parties.
AFGHANISTAN
36°
34°
32°
30°
64° 66° 68° 70° 72° 74°
36°
34°
32°
30°
62° 64° 66° 68° 70° 72° 74°

Settlement Area
Empty Area
Airport
Grassymarsh
Orchard
Cemetery
Factory
Mountain
Lake
Main River
Seasonal River
Main Road
Secondary Road
Tertiary Road
Footpath
Power Line
Telephone Line
Area Name#
Shrineþ
LEGEND
District Boundary
2 0 2 4 6 Kilometers
AIMS
Note:This information is based on best available sources.Updates and corrections would be appreciated. Pleaseforward comments directly to the AIMS office.
E-Mail: [email protected]
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ
þ þ
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
# #
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
# #
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
#
6
8
7
5
9
10
12
4
16
15
3
2
11
1
Zyarat
Zyarat
Zyarat
Zyarat
Zyarat
Zyarati Shah Aqa
Zyarati Sahibzada
Zyarati Sakhi Jan
Zyarati Baba Sangi
Zyarati Khwaja Jam
Zyarati Shah Mazar
Zyarati Khidri Wali
Zyarati Shah Husayn
Zyarati Shah Parwez
Zyarati Shahid Baba
Zyarati Tahmas Khan
Zyarati Ishan Sahib
Zyarati Moy Mobarak
Zyarati Chihil Gazi
Zyarati Dowazda Emam
Zyarati Khwaja Tawab
Zyarati Khwaja Sidiq
Zyarati Khwaja Almuhi
Zyarati Khwaja Payluch
Zyarati Walai Qalandar
Zyarati Khwaja Sabzposh
Zyarati Khwaja Sabzposh
Zyarati Khwaja Sabzposh
Zyarati Khwaja Bol Baba
Zyarati Abdurahman Agha
Zyarati Khwaja Baytullah
Zyarati Bismillah Shahid
Zyarati Khwaja Darya Abad
Zyarati Khwaja Elyas Wali
Zyarati Baba Abdullah Wali
Zyarati Khwaja Zanbur Wali
Zyarati Shikh Qalandari Wali
Zyarati Muhammad Yasin Haskar
Gudri
Pasni
Shina
Unchi
Afshar Baraki
Barchi
Gumruk
Kotgay
Kuloop
Langar
Mahbas
Maktab
Maktab
Maktab
Maktab
Maktab
Maktab
Musahi
Nakhas
Nakhas
Saraji
SinamaSinama
Tapaha
Taraki
ZakhelAliabad
Bagrami
Dih Naw
Jwazyan
Kamaree
Kampani
Maqbara
Maslakh
Matba'a
Qalacha
Qalacha
Sar Qol
Sherpur
Stadium
Taymani
Aka Khel
Alawddin
Alo Khel
Andarabi
Bala Koh
Dih Buri
Dih Dana
Gird Qol
Jangalak
Khwabgah
Naw Abad
Naw Abad
Nyaz Big
Shahrara
Sra Mena
Syahsang
Wilayati
Workshop
Asya Bini
Bala Qala
Bala Qala
Chindawul
Dih Arbab
Dih Kipak
Dih Punba
Dih Qabil
Dih Yaqub
Dugh Abad
Dugh Abad
Fayz Qala
Fazil Beg
Gul Khana
Gul Khana
Guzar Gah
Hood Khel
Khayrabad
Qabil Bay
Rang Sazi
Sar Asyab
Transport
Transport
Umar Khel
Yaka Toot
Akhundzada
Argi Shahi
Baghi Mira
Baghi Riaz
Bala Hisar
Bangseedar
Beni Hesar
Burji Barq
Char Chata
Darullaman
Dawlatzaee
Dih Mazang
Dih Araban
Diwan Bigi
Drug Store
Furmuli Ha
Jamal Mena
Kamangaran
Khwaja Jam
Microrayan
Mulla Khel
Pa'in Qala
Pa'in Qala
Pa'in Qala
Paktya Kot
Puli Pacha
Qala-i-Mir
Qala-i-Naw
Qala-i-Naw
Qala-i-Naw
Qala-i-Naw
Qala-i-Naw
Sari Karez
Shafakhana
Shafakhana
Shafakhana
Shafakhana
Shafakhana
Shafakhana
Shah Mazar
Shahre Naw
Shana Sazi
Shur BazarTakhta Pul
Tapa-i-Mir
University
Wasil Abad
Wazir Abad
Wazir Abad
Asyabi Musa
Baghi Babur
Baghi Hafiz
Baghi Kooti
Baghi Kooti
Baghi Samay
Baghi Uzbak
Bibi Mahroo Bibi Mahroo
Chahar Qala
Chahar Qala
Dawood Khel
Gudam Khana
Hisa-i-Awal
Husyan Khel
Husyan Khel
Jayi Rayees
Karta-i-Naw
Karta-i-Seh
Khwaja Safa
Kohi Afshar
Kohi Qurugh
Mahtab Qala
Masjidi Naw
Murgh GiranPuli Sokhta
Qala-i-Abas
Qala-i-Agha
Qala-i-Agha
Qala-i-Alam
Qala-i-Alif
Qala-i-Amir
Qala-i-Azad
Qala-i-Babu
Qala-i-Khan
Qala-i-Khan
Qala-i-Musa
Qala-i-Nani
Qala-i-Qazi
Qala-i-Rika
Qala-i-Saqi
Rahman Mena
Sang Trashi
Sayid Ghazi
Sayid Qasim
Shah Shahid
Shimir Zaee
Sra Miyasht
Takya Khana
Tayzu Kalay
Tor Ghunday
Yosuf Bangi
Zalmo Hotel
Aqibi Zyarat
Baghi Hindoo
Bagh-i-Uzbak
Beest Hazari
Cement Khana
Chihilsutoon
Dih AfghananHotali Kabul
Karta-i-Char
Karta-i-Panj
Karta-i-Wali
Khwaja Wiala
Kohi Aliabad
Kohi Asmayee
Kulolapushta
Masjidi Jame
Mughul Kalay
Murad Khanee
Nahri Darsan
Parki AskariParki Zanana
Qala-i-Badal
Qala-i-Barat
Qala-i-Barqi
Qala-i-Baydo
Qala-i-Dasht
Qala-i-Ghani
Qala-i-Hindu
Qala-i-Jafar
Qala-i-Kalan
Qala-i-Karim
Qala-i-Kuhna
Qala-i-Kuhna
Qala-i-Malik
Qala-i-Malik
Qala-i-Miran
Qala-i-Muhib
Qala-i-Muhib
Qala-i-Nazir
Qala-i-Nazir
Qala-i-Nazir
Qala-i-Ra'is
Qala-i-Rasul
Qala-i-Sabir
Qala-i-Sadiq
Qala-i-Salah
Qala-i-Shada
Qala-i-Shora
Qala-i-Surkh
Qala-i-Wahid
Qala-i-Wakil
Qala-i-Wazir
Qala-i-Wazir
Qala-i-Wazir
Qala-i-Wazir
Qala-i-WazirRadio Towers
Sarayi Kuhna
Shah Berahna
Ta'miri Gulf
Achik Zayeeha
Aqa Ali Shams
Baghban Kocha
Baghi Dawlati
Baghi Khanjan
Darulmualimin
Dashti Barchi
Dih Khudaydad
Dusad Familee
Ghazi Stadium
Hotali Aryana
Kamawal Kalay
Karta-i-Sakhi
Khushhal Mena
Khwaja Bughra
Khwaja Bughra
Khwaja Rawash
Kohi Bad Asya
Kushkaki Bala
Maktabi Ghazi
Mayhane FelazMili Palastik
Mozyami Kabul
Muhammad Khel
Muhammad Zaee
Noor Hospital
Parwani Dowum
Parwani Sewum
Qala-e-Khwaja
Qala-i-Afridi
Qala-i-Babush
Qala-i-Chaman
Qala-i-Chaman
Qala-i-Chaman
Qala-i-Chaman
Qala-i-Dargha
Qala-i-Dilbar
Qala-i-Farash
Qala-i-Fatooh
Qala-i-Ghaybi Qala-i-Ghulam
Qala-i-Husayn
Qala-i-Kababi
Qala-i-Kashif
Qala-i-Khatir
Qala-i-KhawasQala-i-Khwaja
Qala-i-Khwaja
Qala-i-Khwaja
Qala--i-Kochi
Qala-i-Kolala
Qala-i-Lawang
Qala-i-Logari
Qala-i-Muslim
Qala-i-Niyazi
Qala-i-Qurban
Qala-i-Safdar
Qala-i-Sultan
Qoli Abchakan
Sarayi Ghazni
Sarayi Nakhas
Sarayi Zoghal
Sifarati HindSifarati Iran
Sulayman Khel
Tangi Sayidan
Afghan Shaheen
Chamani Babrak
Dih Murad Khan
Dih Nawi Seelo
Durahi Paghman
Fabrica-i-Qeer
Jada-i-Wilayat
Karta-i-Aryana
Karta-i-Parwan
Karta-i-Parwan
Kohi Laghmanak
Masjidi Payeen
Maydani Hawaee
Pashmina Bafee
Purozha-i-Mahi
Qala-i-Ali Jan
Qala-i-Amirdad
Qala-i-Balooch
Qala-i-Barakat
Qala-i-Chitgar
Qala-i-Jamadar
Qala-i-Khandar
Qala-i-Mawlawi
Qala-i-Musalli
Qala-i-Najarha
Qala-i-Najarha
Qala-i-Noburja
Qala-i-Sayidan
Qala-i-Taymani
Qala-i-Yakatut
Qala-i-Zanabad
Qala-i-Zikriya
Qarya-i-Gulroz
Qarya-i-Kotwal
Qarya-i-Sangar
Sahib Jan Qala
Sarayi Shamali
Afshar Mountain
Ayoob Khan Mena
Baghi Gul Afzal
Chamani Huzoori
Doda Mast Kalay
Fabrica-i-Harbi
Fabrika-i-Charm
Farmi Murghdari
Ghundi Ali Khel
Gul Haydar Qala
Hotali Spozhmay
Humayoon Nasaji
Jayi Bakhtiaran
Karta-i-Mamorin
Kotali Yaklinga
Laysa-i-Shewaki
Maktab Tarakhel
Maktabi Takhnik
Panjsad FamileePurozha-i-Jadid
Qala-i-Afghanan
Qala-i-Afghanan
Qala-i-Afghanan
Qala-i-Amir Jan
Qala-i-Baghalak
Qala-i-Bakhtyar
Qala-i-Chunghaz
Qala-i-Jangalak
Qala-i-Khan Gul
Qala-i-Khan Gul
Qala-i-Khan Mir
Qala-i-Mir Abas
Qala-i-Mir Azim
Qala-i-Mir Azim
Qala-i-Pakhchak
Qala-i-Qabilbay
Qala-i-Sadrazam
Qala-i-Samandar
Qala-i-Sayid Ha
Qala-i-Sayid Ha
Qala-i-Shikh-Ha
Qala-i-Ziauddin
Qarya-i-Dyalaka
Shahraki Police
Shirindil Kalay
Shiwaki Khishti
Sifarati France
Sifarati Italia
Sifarati Russia
Sifarati Turkya
Tahiyayi Maskan
Tapa-i-Maranjan
Unchi Baghbanan
Unchi Baghbanan
Bagh-e-Gul-Khana
Baghi Baqer Khan
Baghi Hakam KhanBaghi Jamaluddin
Baghi MerajuddinBaghi Qalamuddin
Dandi Wazir Abad
Fabrika-i-HukhstFabrika-i-Isfanj
Khelwati Ghunday
Kocha-i-Chuqurak
Kushkaki Payaeen
Laysa-i-Habeebya
Maktabi Nadiriya
Masjidi Baghalak
Microrayani Awal
Muasisa-i-Niswan
Qala-i-Abas Quli
Qala-i-Adam Khan
Qala-i-Ahanullah
Qala-i-Ahmad Gul
Qala-i-Esfandyar
Qala-i-Gadiwanan
Qala-i-Gul Afzal
Qala-i-Khwaja Ha
Qala-i-Mir Samad
Qala-i-Mir Yahya
Qala-i-Mirawkhor
Qala-i-Mustamand
Qala-i-Qazi Aman
Qala-i-Safa Khan
Qala-i-Sher Alam
Qala-i-Sher Khan
Qala-i-Wazir Gul
Qala-i-Wazirabad Qala-i-Yaknukhel
Qarya-i-Chunghaz
Qarya-i-Gul Buta
Qasri Darullaman
Rishkhori-i-Bala
Riyasati Takhnik
Sahe Nindartunha
Shirkati Service
Ta'miri Shikarga
Tara Khel Tarnaw
Tarminali Hawaee
Uniti Quwayi Kar
Utaqha-i-Tijarat
Wazir Akbar Khan
Wizarati Kharija
Wizarati Ma'aden
Wizarati Zira'at
Ashiqan Wa Arifan
Baba Sahib Zyarat
Baba Sahib Zyarat
Baghi Sayid Karim
Maktabi Chihiltan
Mantaqa-i-Sanatee
Mullah Khel Kalay
Nawabadi Gul Buta
Qalacha-I-Khandan
Qala-i-Aghir Khan
Qala-i-Ahmad Khan
Qala-i-Akbar Khan
Qala-i-Ali Mardan
Qala-i-Ali Mardan
Qala-i-Fateh Khan
Qala-i-Ghaybullah
Qala-i-Haji Afzal
Qala-i-Haji Karim
Qala-i-Haji Usman
Qala-i-Husayn Gul
Qala-i-Jabar Khan
Qala-i-Kar Guzaar
Qala-i-Khwaja Naw
Qala-i-Shirin Dil
Qala-i-Sultan Jan
Qala-i-Usman Khan
Qala-i-Zaman Khan
Qarya-i-Asyab Qol
Qarya-i-Bazo Khel
Qarya-i-Karez Tut
Qarya-i-Kula Khel
Qarya-i-Mar Giran
Qarya-i-Qyamuddin
Qassaba-i-Kargari
Quwaikar Hospital
Shahraki Khurasan
Shuhadayi Salihin
Tara Khel Kuchyan
Wuluswali Bagrami
Afshari Darullaman Baghi Rahmat Sayid
Chaharahi-i-Qambar
Dastgahi Khanasazi
Dih Arabani Qargha
Electricity Center
Fabrica-i-Kichmish
Karta-i-Ghawsuddin
Karta-i-Shahshahid
Karta-i-Zendabanan Purojzha-i-Gawdari
Qala-i-Abdul Hakam
Qala-i-Abdul Karim
Qala-i-Abdul Wahid
Qala-i-Abdul Wahid
Qala-i-Allah Nazar
Qala-i-Bahramuddin
Qala-i-Chopanbashi
Qala-i-Ghulam Raza
Qala-i-Haji Zakhel
Qala-i-Hasani Bala
Qala-i-Hazarbuz Ha
Qala-i-Hazarbuz Ha
Qala-i-Ismail Khan
Qala-i-Parwez Shah
Qala-i-Qazi Ghiyas
Qala-i-Wazir Faruq
Qarya-i-Barat Khan
Qarya-i-Kakar Khel
Qarya-i-Siyah Bini
Qasri Chihilsutoon
Tapa-i-Bibi Mahroo
Baghi Ghulam Hazrat
Chawki Kota-i-Sangi
Fabrica-i-Paya Sazi
Familee Hayi QarghaHaji Muhammad Hasan
Haji Muhammad Yonus
Jakshani Omomi Barq
Khana-i-Sayid Karim
Kocha-i-Halabisazee
Masjidi Chahar Qala
Muhammad Khel Kalay
Nawabadi Dih Araban
Pushta-i-Qala-i-Naw
Qalacha-I-Gul Khana
Qala-i-Baghbanak Ha
Qala-i-Chahar Diwar
Qala-i-Fazel Rahman
Qala-i-Ghulam MajidQala-i-Hasani Pa'in
Qala-i-Hashmat Khan
Qala-i-Ibrahim Khan
Qala-i-Malik Ashoor
Qala-i-Mirza Ja'far
Qala-i-Panja Chinar
Qala-i-Qafila Bashi
Qala-i-Sayid Rahman
Qala-i-Simint Khana
Qarya-i-Ghaybi KhelTapa-i-Kululapushta
Zan Abad (Naw Abad)
Baghi Muhammad Nawaz
Baghi Muhammad Zarif
Baghi Tahir Jan Agha
Fabrica-i-Charm Gary
Fabrika-i-Seekhi Gol
Gardana-i-Baghi Bala
Khana-i-Majid Bahari
Muasisa-i-Sihati Ama
Nawabadi Hisa-i-Awal
Qala-i-Amir Muhammad
Qala-i-Muhammad Amin
Qala-i-Muhammad Khan
Qala-i-Muhammad Umar
Qala-i-Muhammad UmarQala-i-Noor Muhammad
Qala-i-Sarfaraz Khan
Shafakhana-i-Aliabad
Baghi Haji Mir Afghan
Bahadur Khani Furmoli
Fabrica-i-Tasade Chob
Kocha-i-Waziri Darbar
Maktabi Khurd Zabitan
Markazi Sihee Shewaki
Nawabadi Qala-i-Wahid
Qala-i-Mir Ahmad Shah
Qala-i-Mir Ahmad Shah
Qala-i-Muhammad Anwar
Qala-i-Muhammad Hayat
Qala-i-Muhammad Yasin
Qala-i-Muhammad Yosuf
Sari Karezi Niyaz Beg
Shirkati Prosisi Roda
Baghi Sayid Shah Naser
Bala Qala-i-Hasan Khel
Fabrica-i-Aria Battery
Fabrica-i-Zoghali Sang
Madrasa-i-Jam'atulisam
Nawabadi Qala-i-Kashif
Poly Technic Institute
Qalacha-I-Sahib Zadaha
Qala-i-Bibi Shamsi Jan
Qala-i-Ghulam Muhammad
Sari Karezi Jabar Khan
Shirkati Sahami Behsud
Fabrica-i-Keshti Banaee
Laysa-i-Mahmoodi Tarzee
Qala-i-Ghulam Umar Khan
Qala-i-Haji Abdul FatahQala-i-Haji Abdul JalilQala-i-Haji Abdul Manan
Qala-i-Haji Abdul Qader
Qala-i-Haji Abdul Wahid
Qala-i-Hakim-i-Walayati
Qarya-i-Damana-i-Kamari
Tahwil Khana-i-Abrasani
Baghi Ghulam Haydar Khan
Chahar Qala-i-Wazir Abad
Dastgahi Sakhtumani Afg.
Fabrica-i-Nasaji Bagrami
Familee Hayi Pulicharkhi
Markazi Adwiya-i-Aliabad
Nazar Jay-i-Hazrati Abas
Qala-i-Chamani Dih Kipak
Qala-i-Khandari Walayati
Shaykh Shahabbuddin Baba
Chamani Mantiqa-i-Sanaati
Hisa-i-Duwumi Khayr Khana Hisa-i-Suwumi Khayr Khana
Qala-i-Dastori Mir Ghazab
Qala-i-Haji Mohammad Nabi
Qala-i-Haji Noor Muhammad
Qala-i-Muhammad Shah Khan
Fabrica-i-Hajari Wa Najari
Nawabadi Qarya-i-Fazel Beg
Maqbara-i-Alahazrati Shahid
Qala-e-Abdul Qader (Qadiro)
Dash Hayi Haji Ghulam Husayn
Sayid Nur Muhammad Shah Mina
Purozha-i-Wazir Abad (Taimani)
Qala-i-Hindu (Saray Malik Noor)
Qala-i-Najarha
KABUL CITY
#AIMS
N

PCMワークショップにて発言するRHDハミダ部長
PCMワークショップにて成果の達成度を確認する参加者たち
マラライ産科病院研修部のある建物
2008年5月に開所したダシュテバルチ郡病院研修センター
ダシュテバルチ郡病院分娩室 24時間運営となり、ダシュテバルチ郡病院の利用者数が急増
KPHD外観 KPHD敷地内のプロジェクトオフィス
中央薬品倉庫に保管された供与医薬品
とあるCHCにて整頓を実践する立山リーダー
JCCにてプロジェクトの成果を発表するソヘイラRHコーディネーター
JCCにて成果を称えるナデラ副大臣(右)
略 語 表
ANDS Afghanistan National Development Strategy アフガニスタン国家開発戦略
BHC Basic Health Center 基礎保健センター
BPHS Basic Package of Health Services 保健サービス基礎パッケージ
CGHN Consultative Group of Health and Nutrition 保健栄養コンサルティンググループ
CHC Comprehensive Health Center 広域保健センター
COC Continuum of Care 継続ケア
C/P Counterpart カウンターパート
DH District Hospital 郡病院
EPHS Essential Package of Hospital Services 病院サービス必須パッケージ
HHS Health and Human Service 米国保健省
HMIS Health Management Information System 保健管理情報システム
HSSP Health Service Support Program 保健サービス支援プログラム
IMCI Integrated Management of Childhood Illness 小児疾患統合管理
JCC Joint Coordinating Committee 合同調整委員会
JHPIEGO
Non-for-profit International Public Health Organization affiliated with Johns HopkinsUniversity
ジョンズホプキンス大学系保健NGO
KPHD Kabul Provincial Health Directorate カブール州保健局
M/M Minutes of Meetings 協議議事録
MoPH Ministry of Public Health 公衆衛生省
MOVE MOVE Welfare Organization (ローカルNGO)
NGO Non-Governmental Organization 非政府組織
ODA Official Development Assistance 政府開発援助
PCM Project Cycle Management プロジェクト・サイクル・マネージメント
PDM Project Design Matrix プロジェクト・デザイン・マトリックス
PHO Provincial Health Officer 州保健行政官
PO Plan of Operation 活動計画表
PRHO
Provincial Reproductive Health Officer
州保健局のリプロダクティブ・ヘルス行政官(脚注2参照)
PRR Priority Reform and Restructuring 公募と選考による公務員登用制度
R/D Record of Discussions 討議議事録
RH Reproductive Health リプロダクティブ・ヘルス
RHD Reproductive Health Directorate リプロダクティブ・ヘルス部
RHO Reproductive Health Officer リプロダクティブ・ヘルス行政官

SMI Safe Motherhood Initiative 安全な母性イニシアチブ
TAG Technical Advisory Group 技術諮問グループ
UNICEF United Nations Children’s Fund 国連児童基金
USAID
United States Agency for International Development
米国国際開発庁

i
評価調査結果要約表 1.案件の概要
国名:アフガニスタン国 案件名:リプロダクティブヘルスプロジェクト
分野:保健医療 援助形態:技術協力プロジェクト
所轄部署:人間開発部保健行政課 協力金額(2009年4月現在):計約639,092千円
先方関係機関:公衆衛生省 (英)Ministry of Public Health(MoPH) カブール州保健局 (英)Kabul Provincial Health Directorate(KPHD)
日本側協力機関名:国立国際医療センター(IMCJ)
協力期間:2004年9月~2009年9月
他の関連協力:緊急支援無償資金協力による「ダシュテバルチ郡病院研修センター建設」
1-1 協力の背景と概要 アフガニスタン国は、世界で最も保健状況の劣悪な国の一つであり、妊産婦死亡率が10
万出生当たり1,600(2004年 公衆衛生省)と、世界で最も劣悪な状況にある。これは、社会因習的及び物理的な問題から、リプロダクティブ・ヘルス(Reproductive Health:RH)サービスへのアクセスが非常に困難であること、また、特に女性の保健医療人材の質・量の不足、脆弱な保健システムが原因となっている。このため、RH分野の政策立案及び実施運営能力の強化、看護師及び助産師への技術水準向上などの人材育成をすることは、RH事業の推進のために不可欠である。 アフガニスタン国公衆衛生省(Ministry of Public Health:MoPH)は、妊産婦死亡率の低
下を目標として、 2004年1月にリプロダクティブ・ヘルス部( Reproductive Health Directorate:RHD)を設置した。RHDは、「質の高い家族計画サービスへのアクセス向上」「産科救急ケアへのアクセス向上」「訓練された介助者による出産介助を増やす」の3つの政策目標を実現するため、人材育成を統括する人材開発部と各州の保健局と連携し、各州へのRH行政官の配置と、マラライ産科病院をはじめとする産科教育病院でのRH分野の保健医療サービス提供者の育成を行っている。 以上を背景とし、アフガニスタン国政府は、RH事業の強化を図るために、我が国に対し
て技術支援要請を行った。 本プロジェクトは、プロジェクト目標「保健サービス基礎パッケージ(Basic Package of
Health Services:BPHS)、病院サービス必須パッケージ(Essential Package of Hospital Services:EPHS)1 に基づいた必要なRHサービスを提供するためのRH行政官とRHサービス提供者の能力が向上する」を達成すべく、2004年9月より開始した。今般、2009年9月にプロジェクトの終了を迎えるにあたり、①これまでの活動状況をレビューし、PDM指標の達成状況を把握すること、②活動実施プロセスにおける効果発現の貢献要因・阻害要因を分析して他の類似プロジェクトへの教訓を導くこと、加えて、③残り半年間の活動期間に対応すべき事項について整理するとともに、採択済みのフェーズ2プロジェクトの方向性について提言を行うこと、を目的に終了時評価調査団が派遣された。
1 BPHSは、あらゆる第一次保健施設で標準的な基礎保健サービスが提供され、住民に公平なアクセスが提供されるよう、アフガニスタン国政府が2002年より推進している国家標準である。EPHSは、病院サービスを強化することを目的とした国家標準を指す。

ii
1-2 協力内容 (1)上位目標
母親と新生児に対する質の高い保健サービスの提供可能な地域が拡大される。
(2)プロジェクト目標 BPHSとEPHSに基づいた必要なRHサービスを提供するためのRHO(RH行政官)とRH
サービス提供者の能力が向上する。
(3)アウトプット(成果) 1.国家RHプログラムが完成し、活用される。 2.卒後研修メカニズムが完成し、適切に維持される。 3.アーバン・カブールでRHシステムが機能する。
1-3 投入(2009年4月まで) (1)日本側
1)専門家派遣 長期専門家8人、短期専門家延べ13人を派遣した。
2)研修員受入れ 本邦研修を7コース実施し、計21人の研修員を受け入れた。インドネシア、カンボ
ジア、パキスタンで第三国研修を計4コース実施し、延べ18人を派遣した。 3)機材供与
プロジェクト活動に必要な車両、複写機、教材、医薬品等を供与した。 4)プロジェクト関係費用
日本人専門家の活動に必要な経費を支出した。プロジェクト開始からの支出費用の合計は、約97,692千円相当。
(2)アフガニスタン国側 1)カウンターパート配置
MoPH副大臣を含むカウンターパート(Counterpart:C/P)を配置した。配置したC/Pは途中で異動した者を含め延べ38人。 2)ローカルコスト
C/Pの人件費、活動に係る機材、消耗品等の一部を負担し、専門家の執務スペースを提供した。
2.終了時評価調査団の概要
調査者 1.渡部 晃三(団長) 国際協力機構人間開発部保健行政・母子保健グループ保健行政課長
2.尾崎 敬子(母子保健) 国際協力機構人間開発部課題アドバイザー 3.山形 律子(協力計画) 国際協力機構人間開発部保健行政・母子保健グ
ループ保健行政課職員 4.田中 恵理香(評価分析) グローバルリンクマネージメント(株)社会開
発部研究員

iii
調査期間 2009年4月17日~5月2日 評価種類:終了時評価
3.評価結果の概要
3-1 実 績 (1)上位目標
母親と新生児に対する質の高い保健サービスの提供可能な地域が拡大される。 上位目標の指標は、「包括的保健センター、24時間運営の包括的保健センター及び病
院で提供されるRHサービスから便益を受ける人の数が増える」となっている。保健管理情報システム(Health Management Information System:HMIS)のデータによれば、RH関連の指標が全国平均で向上しており、特に女性保健スタッフのいるBPHS/EPHS施設の割合、2種類以上の近代的避妊方法を提供しているBPHS/EPHS施設の割合の増加は、上記施設から便益を受ける人の数が増えることにつながると考えられる。これらの指標の向上にプロジェクトがどの程度貢献したかは明確にわからないものの、RHOとサービス提供者の能力の向上は指標の向上に貢献したものと考えられる。プロジェクトの便益が今後も維持され、活動が継続して拡大していけば、上位目標は達成されることが期待できる。
(2)プロジェクト目標 BPHSとEPHSに基づいた必要なRHサービスを提供するためのRHO(RH行政官)とRH
サービス提供者の能力が向上する。 プロジェクト開始当初に比較すると、RHOとRHサービス提供者の能力は向上してい
る。継続ケア(Continuum of Care:COC)研修のフォーカス・グループ・ディスカッションでは、カブール都市部における保健サービスに対する患者満足度が向上していることが明らかになっている。スーパービジョン報告書及び終了時評価におけるインタビューによれば、保健施設においてサポーティブ・スーパービジョンは好意的に受け入れられており、保健サービスの提供者はスーパーバイザーと協議をしながら建設的に問題解決を行うようになった、とのことである。 プロジェクト目標の指標は、「公衆衛生省RHDによって適切にモニターされた成果指
標の数」となっており、専門家等の支援なしにRHDがRH関連指標をモニタリングできることがRH行政能力を示しているという考え方に基づいている。指標達成状況は、HMISデータによりRHDでモニタリングを行っている6指標と、RHOの報告により収集され、RHDでモニタリングされている2指標である。インタビュー結果等から、指標の収集については適切にモニタリングされているが、タイムリーな分析を行うことが課題になっている。
(3)アウトプット(成果) 1)成果1:国家RHプログラムが完成し、活用される。
プロジェクト開始時は、RH部(RHD)が創設されてわずか2年程度経過した時期であり、当時は組織としての整備に着手したばかりで、人材の能力も十分でなく、RHDに関する業務が円滑に行われていなかった。プロジェクト開始当初に比較すると、RHDの能力は顕著に向上したといえる。アフガニスタン国の「国家RH政策」及び「国家RH戦略」等の国家政策を具体的な行動計画に移すための「国家RHプログラム」が策定された。RHDの事業計画・実施能力は向上しており、組織図が策定され、

iv
スーパービジョンのマニュアルが完成するなどしている。国家RHモニタリング指標の四半期ごとの分析は、2008年第1四半期までまとめられている。また、RHDからサポーティブ・スーパービジョンを受けた州の数は、2009年3月現在2州、州保健局のリプロダクティブ・ヘルス行政官(Provincial Reproductive Health Officer:PRHO)からRHDへの四半期報告については、フォーマットが作成され、報告のしくみが構築された。 2)成果2:卒後研修メカニズムが完成し、適切に維持される。
「卒後研修品質管理ガイドライン」ドラフトが完成し、承認手続中である。マラライ産科病院研修センターにおいて、研修を計画・運営するメカニズムが構築された。研修部が設立され、組織図が策定された。日当支給や研修センター予約などの事務を含む研修センター運営規則が策定され、トレーナーが訓練された。また、フォローアップとスーパービジョンを含む研修プログラムも実施されるようになった。 ダシュテバルチ郡病院研修センターは、2008年4月に建設が完了し、同年5月に正
式にオープンし、10月に職員配置が完了したばかりで、評価時点では、研修メカニズムを確立する途上にあるという状況である。 研修メカニズム構築の一環として、「COCラーニングリソースパッケージ」研修教
材が開発された。これら研修教材は承認を待つ過程にあるものもある。 プロジェクトでは、研修運営システム強化のため、データベース作成を導入し、デ
ータインプットのための研修コースを実施した。研修データベースのフォーマットは、保健サービス支援プログラム(Health Service Support Program:HSSP)が技術支援して開発された。
3)成果3:アーバン・カブールで、RHシステム 2 が機能する。 カブール州保健局(Kabul Provincial Health Directorate:KPHD)は、2004年に設立
され、設立から日が浅いが、プロジェクト開始当初に比べるとRHOの能力は向上し、日々の業務が実施されている。アーバン・カブールにおけるRHシステムが向上していると判断される。
RHOがRHプログラムを管理しスーパービジョンを実施する能力は、プロジェクト開始当初に比較し強化されている。スーパービジョンが実施されており、州保健行政官と都市部の第一次保健施設の長によるアーバン・ヘルス月例ミーティングが開催されるようになった。保健サービス提供者の能力が強化され、スーパーバイザーの支援のもと、記録を取るなどの業務を適切に行えるようになった。 薬剤配布システムも、薬剤配布・在庫管理業務遂行能力が強化されるなど、向上し
た。一方、リファラル・システムは完全に導入されたとはまだいえない状況である。プロジェクトでは、2009年2月にリファラルのためのフォーマットを開発し、その後引き続き、リファラル・システムを確立するための協議を行っている。 アウトプット3に関する指標は、指標の3-2と3-3は、傾向としては達成に向かって
いるといえるが、指標3-1のポリクリニックのCHC+/県病院への転換や、指標3-4の郡病院での帝王切開実施など、いくつかの指標は目標値を達成していない。しかしながら、設定された指標には、プロジェクトだけでは達成できないものが含まれてお
2 RHサービスを提供するために必要な保健システム。本プロジェクトでは、特に医薬品ロジスティクス、リファラル・システム、HMISの改善に取り組んだ。

v
り、当初の指標の設定そのものがプロジェクトの成果として達成困難なものとなっていた事情を考慮する必要がある。
3-2 実施のプロセス 予定していた活動はおおむね完了することができた。 PDMは、成果を整理してRHシステム強化を加えるなど、3回改訂された。改訂はいずれ
も、参加型で適切なプロセスを経て行われた。日本人専門家、アフガニスタン国C/Pとも、PDMについて共通の認識をもっており、日々の活動の中で適宜参照している。 日本人専門家とアフガニスタン国C/Pのコミュニケーションは良好であった。双方で日ご
ろから頻繁に会合をもち、問題があった場合には協議により解決することができた。プロジェクト関係機関間のコミュニケーションはおおむね良好であった。ただし、MoPHとKPHDの間でコミュニケーションの齟齬が生じることが時折あった。他の援助機関とのコミュニケーションはMoPHのRHDが中心に調整を行っており、おおむねコミュニケーションは良好であった。 プロジェクト活動は、治安による影響があった。治安状況の悪化により、スーパービジ
ョンの中止や研修の延期などがあった。2005年の9月から10月にかけては、治安の悪化により、チーフアドバイザーと業務調整員を除く日本人専門家が国外退避を余儀なくされた。しかしながら、スケジュールを綿密に調整し効率的に活動を実施することで、予定の活動をほぼ完了することができた。
3-3 評価結果の要約 (1)妥当性
アフガニスタン国の開発政策とニーズ、日本の対アフガニスタン政府開発援助(ODA)政策との整合性、及びプロジェクト・デザインの適切性の関連から、妥当性は高い。 プロジェクト目標と上位目標は、アフガニスタン国の開発政策と合致している。アフ
ガニスタン国家開発戦略( Afghanistan National Development Strategy: ANDS)(2008-2013)では、RH・子どもの健康プログラムは優先分野になっている。また、アフガニスタン国において、RH向上のニーズは非常に高く、RHサービスの向上とRHO・保健サービス提供者の能力開発は重要課題になっている。 プロジェクトは、日本のODA政策とも整合性がある。日本の対アフガニスタンODA
政策における4つの重点分野に保健分野が含まれている。 プロジェクト目標達成のためにプロジェクトが採用したアプローチは適切である。
RHDが設立されたのがプロジェクト開始のわずか2年前であり、C/Pの個人レベル及び組織レベルのオーナーシップと能力の養成を通じ、RHプログラムと人材開発のメカニズムを構築することは適切であった。また、公共部門におけるRHシステムの強化を図ろうとした。 アフガニスタン国の経済社会復興に対する支援は、国際社会において非常に重要であ
り、プロジェクトが他の援助機関との協調を重視したことは、アフガニスタン国の現状に照らし適切であった。
(2)有効性 アウトプット、プロジェクト目標とも達成されつつあり、有効性は高いといえる。

vi
アウトプットとプロジェクト目標は論理的につながっており、アウトプットはプロジェクト目標の達成に貢献した。アウトプットの1と2、すなわち、RHプログラムの確立と卒後研修メカニズムの構築はプロジェクト目標達成には不可欠なものである。アウトプット3は、カブール市内においてRHシステムが機能するよう、RHD、RHOとサービス提供者の能力を強化しようとするものである。カブール市では、BPHSが実施されていないため、カブール市でRHシステムを構築することにより、RHD、RHO、サービス提供者が研修の成果を実践に活用する場となることが期待されていた。このような観点から、アウトプット3はプロジェクト目標と論理的に関連性があり、プロジェクト目標達成に貢献したといえる。
(3)効率性 効率性はおおむね高い。専門家派遣以外の投入はおおむね予定通りなされており、ア
ウトプット発現に貢献した。 派遣された日本人専門家は、おおむね適切な専門性と経験をもち、アフガニスタン国
側C/Pの能力開発に貢献した。2008年8月にチーフアドバイザーが離任したあと後任が派遣されず、チーフアドバイザーが担っていた一部の業務が遂行されない時期があったが、他の専門家及びナショナル・スタッフで補い、影響を最小限にとどめた。 本邦と第三国におけるC/P研修は、C/Pの能力強化に有効であった。本邦研修参加者は
RH行政に必要な知識と技能を習得し、研修の成果を日々の業務に活用している。他の国で実施しているJICAプロジェクトとの技術交換は効果的であった。また、C/Pを、イスラム国であるインドネシアや、復興プロセスにあるカンボジア等、アフガニスタン国と類似の状況にある第三国に派遣した。こうした研修は、他国からの参加者と同様の経験を共有できるため、効果的であった。 日本側が供与した施設・機材は、仕様、品質、数量ともにほぼ適切であった。プロジ
ェクトで建設したマラライ産科病院研修センターは、研修活動の拠点として十分活用されている。ダシュテバルチ郡病院研修センターは、2008年5月に正式に開所したあと、同年10月頃から配置された職員が研修開始の準備を行っているが、評価時点では、まだ研修を本格的に開始するに至っていなかった。ダシュテバルチ研修センターは、最近、組織機構が承認され、KPHD、ダシュテバルチ郡病院の管轄下に置かれることが決定したが、カブール州近隣の州を含めた地域の中核となる地域研修センターとしての位置づけにはなっていない。 プロジェクトで雇用したナショナル・スタッフは、全員が高い能力と強いコミットメ
ントをもち、プロジェクト実施に不可欠な貢献を果たした。 アフガニスタン国側は、プロジェクト実施にあたり、十分な能力とオーナーシップを
もつC/Pを配置した。アフガニスタン国側のプロジェクト運営コストの負担は限られており、資機材の維持管理に必要な費用を十分に支出することができなかった。プロジェクトを円滑に運営するため、スーパービジョンや研修に係る費用は基本的に日本側で負担した。 パートナーシップ促進の観点から、薬剤供与は他ドナー機関と協調して行うこととし
ており、この計画はアフガニスタン国の状況に照らし適切であった。ただし、この協調体制による支援は、活動の当初は円滑に進捗していたが、他ドナー負担分の供与が予定通り実施されなくなっている。 実施された投入はおおむね適切に活用され、予定した活動の実施とアウトプットの発

vii
現に貢献した。 プロジェクト実施プロセスは、治安状況により影響を受けた。しかしながら制限のあ
る環境の中で予定していた活動を行えるよう、調整と工夫を十分に検討し、柔軟に対応しながらプロジェクトを遂行した。 活動から成果に至る外部条件の中でプロジェクトに影響を与えたものとしては、プロ
ジェクトの前半にC/Pの交替が頻繁にあったことが挙げられる。
(4)インパクト プロジェクトの便益がこのあとも維持されれば、上位目標は達成されることが期待で
きる。 RHD及びRHOの能力開発により、RH行政の基礎が確立されつつあり、研修メカニズ
ムの構築を通じてサービス提供者の能力が向上している。RHOとサービス提供者の能力が引き続き向上すれば、質の高い母子保健サービスの拡大が期待できるであろう。上位目標達成のモニタリングにあたっては、PDMの指標に留意が必要である。上位目標の指標は、RHサービスを受けた住民の数の増加であるが、これはプロジェクトで取り組んでいるRHOとサービス提供者の能力強化を超えたプロジェクトの枠外の条件によるところが大きい。例えば、保健施設へのアクセスや地域の治安、保健施設のインフラ整備状況などの条件もかかわってくるので、こうした条件を考慮することが必要である。
RHは、人間の安全保障における重要な要素であることから、プロジェクトはアフガニスタン国の人間の安全保障に貢献することが期待されている。 予期せぬ正のインパクトが認められる。プロジェクトでは、アウトプット3の活動の
一環として、カブール市内においてRHのリファラル・システムを構築することを試みていたが、この活動を実施する中で、プロジェクト関係者は、カブール都市部においてRHのみならず保健システム全体を構築するための政策と戦略を策定することの必要性を認識した。 負のインパクトが1点報告されている。プロジェクトでは、カブール市内のポリクリ
ニックを郡病院(District Hospital:DH)や24時間オープンの広域保健センター(CHC+)に転換することを提言し、9か所のポリクリニックのうち、1か所がCHC+に転換された。この際、組織変更がアフガニスタン国側で行われた際に配置される職員数が削減されることになり、庶務係等を含み30人から40人が職を失ったと見積もられている。
(5)自立発展性
政策面、技術面、組織面での自立発展性はおおむね高いが、財政面での自立発展性は外部からの支援なしには望めない状況である。
RHを重視する政策は継続するものと見られている。ANDSは、2013年までの戦略を規定しているが、RHは優先分野となっている。 技術的自立発展性はかなり高い。プロジェクトで研修を受けたRHO、研修コーディ
ネーター、トレーナー、サービス提供者らは、担当業務を実施するために必要な知識と技能を習得しており、また多くの者は責任を遂行する高い意欲をもっている。自立発展性を高めるには、引き続き能力開発を行うことが必要である。 組織的能力の自立発展性も高い。RHDは組織として強化されておりRHプログラムが

viii
策定されている。日本の支援により国立のマラライ産科病院とダシュテバルチ郡病院に研修センターが建設された。マラライ産科病院研修センターでは研修部が設立され、研修センター規則が整備されている。ダシュテバルチ郡病院研修センターでも研修システムが整備されつつある。このような運営のしくみが整備されていることから、両研修センターとも、プロジェクトで導入された活動が継続するものと見込まれている。 財政的自立発展性が懸念材料となっている。MoPHには、その責務を遂行するだけの
十分な予算が配分されていない。予算の大部分は人件費に割り当てられ、経常経費に充当される予算は限られており、研修やスーパービジョンに予算配分するしくみが存在していない。プロジェクトで導入した研修とスーパービジョンを継続的に実施するためには、特に経常予算の確保を行う必要がある。
3-4 効果発現に関する貢献・阻害要因 効果発現の貢献要因としては、まず、アフガニスタン国側、日本側とも、高いモティベ
ーションと専門性をもつ人材を配置したことが挙げられる。また、プロジェクト開始時期がRHDの創設後まもなく、RHDを整備していくプロセスとプロジェクトの活動が軌を一にしていたことがある。阻害要因としては、プロジェクトの前半でC/Pの頻繁な人事異動があったこと、研修を受けたサービス提供者で離職する者がいること、MoPHの予算、特に経常経費予算が十分でないことがある。 3-5 結 論 アフガニスタン国の困難な状況にもかかわらず、プロジェクトはおおむね適切に実施さ
れ、プロジェクト目標は達成されつつある。プロジェクト実施プロセスは、副大臣をはじめとするC/P組織の強力なコミットメントにより促進された。その結果、RHOとRHサービス提供者の能力が顕著に向上し、さらに向上する必要はあるにせよ、当面の任務を自分たちで遂行していくことがある程度可能になっている。アウトプットは3つとも達成されつつある。全体として、プロジェクト開始当初のMoPH及び関連機関の人的・組織的・物的状況に比較すると、プロジェクトは顕著な業績を挙げてきたといえる。プロジェクトの便益を維持拡大していくためには、RHプログラム、卒後研修メカニズム、カブール市内のRHシステムのいずれも、さらに強化していく必要がある。 3-6 提 言 評価結果に基づき、プロジェクトの残り期間で行うべきこととして、以下の点を提言す
る。 ・MoPHは、開発された研修マニュアルと卒後研修ガイドラインの承認手続きを完了すること。
・MoPHは、2008年年次報告書の英語訳を出版すること。 また、以下の点については、プロジェクトの残り期間中に取り組みを開始し、一部につ
いてはフェーズ2で継続的に取り組むことを提言する。 ・MoPHは、国家RHプログラムの文書化を行うこと。 ・MoPHは、2008年第2四半期以降に収集されたHMISデータの取りまとめと分析を行い、その結果に基づいた政策決定を行うこと。MoPHは、RHD職員のデータ分析に関する能力開発を行うこと。

ix
・MoPHは、ダシュテバルチ郡病院研修センターを地域研修センターとして機能させ、あわせてダシュテバルチ郡病院の能力向上を図ること。
・MoPHは、資金贈与・契約管理部門(Grant and Contract Management Unit)と協力し、NGOに関する情報を整備し、NGOとの共同スーパービジョンを促進すること。
・MoPHは、研修とスーパービジョンの運営コストの予算を見積もり、予算確保・配分のための努力を引き続き行うこと。
・ダシュテバルチ郡病院は、BPHSの定める必要職員数を充足しているが、増加する分娩に適切に対応するにはまだ十分でない。BPHSの規定自体が、都市部における状況には適切でないことも考えられる。BPHSの見直しを行い、都市部におけるBPHS規定を改訂することが望ましい。
3-7 教 訓 ・他の援助機関との協調により実施される投入がある場合は、パートナーとなる援助機関が予定している投入が確実に実施されるか確認することが重要である。
・アフガニスタン国のように復興過程にある国では、人事交替が頻繁に起こることがあるが、このような場合、プロジェクトの活動や成果を持続させるには、活動の結果を文書化することが効果的である。

xi
Summary of Final Evaluation 1.Outline of the Project
Country:Islamic Republic of Afghanistan Project title:Reproductive Health Project
Issue/Sector:Health Cooperation Scheme:Technical Cooperation Project
Division in Charge:Health Systems Division, Human Development Department
Total cost(As of April 2009) Total:639,092,000 yen Partner Country’s Implementing Organization: Ministry of Public Health (MoPH) Kabul Provincial Health Directorate(KPHD) Supporting Organization in Japan:International Medical Center of Japan
Period of Cooperation:Sept. 2004 – Sept. 2009
Related Cooperation: “Dasht-e Barchi Hospital Training Center” by remnant of Emergency Grant
1-1 Background of the Project Afghanistan is facing the world’s worst health conditions, e.g., maternal mortality ratio of 1,600/100,000
live births. This is due to socio-cultural and physical factors that hinder women’s access to reproductive health services, the shortage (both in number and quality) of female health service providers and the weak health systems.
Afghanistan’s Ministry of Public Health (MoPH) launched Reproductive Health Directorate (RHD) in 2004, aiming to ameliorate the maternal mortality ratio. In order to achieve the policy objectives (i.e. better access to quality family planning services, better access to emergency obstetric care, and increase in deliveries with skilled birth attendants), RHD makes efforts such as allocating a reproductive health officer to each province, training reproductive health service providers at Malalai Maternal Hospital, etc.
With this background, the Government of Afghanistan requested a technical assistance to strengthen reproductive health services. This project has started in September 2004, with its purpose: “The capacity of RHOs (Reproductive Health Officers) and RH service providers to provide necessary services based on BPHS (Basic Package of Health Services) and EPHS (Essential Package of Hospital Services) is improved.”
Before the project completion in September 2009, JICA dispatched the terminal evaluation team and conducted a joint evaluation with the Afghan side. 1-2 Project Overview (1) Overall Goal:The coverage of quality maternal and newborn health services is expanded. (2) Project Purpose:The capacity of RHOs (Reproductive Health Officers) and RH service providers to
provide necessary services based on BPHS (Basic Package of Health Services) and EPHS (Essential Package of Hospital Services) is improved.
(3) Output: Output 1
National Reproductive Health Program is established and functioning. Output 2
In-service training mechanism is established and maintained in an appropriate manner.

xii
Output 3 RH system is functioning in Urban Kabul.
1-3 Inputs (As of April 2009) <Japanese side>
Long-term expert 8 Short-term expert 13 Acceptance of trainees (in Japan) 21 Afghan C/P participants in Training in Third Countries (Cambodia, Indonesia, Pakistan) 18 Equipment supplied Vehicles, photocopier, training materials, drug supplies, etc. Local Cost 97,692,000 (Japanese yen)
<Afghan side>
Counterparts (C/P) 38 (including those who were replaced during the Project) Local cost Personnel cost for C/P, provision of office for Japanese experts, cost for materials and consumables
2.Evaluation Team
Members of Evaluation Team
1. Mr. Kozo Watanabe (Team Leader) Director, Health Systems Division, Health Systems and Reproductive Health Group, Human Development Department, JICA 2. Ms. Keiko Osaki (Maternal and Child Health) Senior Advisor, JICA 3. Ms. Ritsuko Yamagata (Project Planning) Staff, Health Systems Division, Human Development Department, JICA 4. Ms. Erika Tanaka (Evaluation and Analysis) Researcher, Social Development Department, Global Link Management
Period of Evaluation
17 April 2009 – 2 May 2009 Type of Evaluation:Terminal evaluation
3.Results of Evaluation
3-1 Summary of Evaluation Results (1) Relevance
Relevance is high in terms of Afghan development policy, needs in Afghanistan, Japanese official development assistance (ODA) policy to Afghanistan, and Project design.
The Project Purpose and Overall goal are consistent with Afghan development policy. In Afghanistan National Development Strategy (ANDS: 2008-2013), reproductive and child health program is given high priority. Improvement of reproductive health is highly needed in Afghanistan. Maternal mortality rate is extremely high, 1600/100,000 live births (Ministry of Public Health, 2004).
The Project is consistent with Japanese ODA policy as well. In the Japanese ODA policy to Afghanistan, improvement of health is included in one of the four priority areas.
The approach that the Project adopt to achieve Project Purpose is appropriate. Given the fact that the RHD was established only two years before the start of the Project, establishment of mechanism of RH program and human resource development is highly adequate. The Project puts importance on fostering ownership and capacity of C/Ps both as individual and as institution. Another distinctive approach of the

xiii
Project is to achieve its goal through strengthening the RH systems in the public sector. As the assistance to economic and social reconstruction of Afghanistan is a highly important issue in international community, the Project gives consideration to collaboration with other aid agencies, which is desirable in current Afghan situation.
(2) Effectiveness
Project Purpose is being achieved and effectiveness is high. Outputs are being gradually achieved. National RH program has been developed and the capacity of
RHD (RH Directorate) is improved. Training mechanism is established at Malalai Maternity Hospital Training Center and is being established at Dasht-e Barchi District Hospital Training Center as well. Some tasks to be achieved are; developed training manuals are still under procedure of official approval; training database is not developed although reporting system is established. Objectively Verifiable Indicators of Output 1 and Output 2 in PDM are generally achieved. As to Output 3, RH system in Kabul City has been remarkably improved since the start of the Project. Not all the PDM Indicators are fully achieved due to complicated setting of Indicators. To make RH system in Kabul City fully function, further capacity development of KPHD and establishment of referral system is necessary.
Project Purpose is being achieved. The administrative capacity of RHOs is greatly enhanced as compared to the beginning of the Project and RH program is appropriately implemented. The capacity of RH service providers is also strengthened and the RH services are also improved. To further improve the capacity of RHOs and RH service providers it is necessary to strengthen supervision and training system.
Three Outputs are logically related to Project Purpose and contributed to achieve Project Purpose. Output 1 and Output 2, establishment of RH program and in-service training mechanism are essential to achieve Project Purpose. Output 3 is to strengthen capacity of RHD, RHO, and service providers to make RH system function in Kabul City. In Kabul City, BPHS is not contracted-out and it is expected that establishing RH system there will serve as a setting to practically implement the outcome of training of RHD, RHO, and service providers. Thus Output 3 is also related to Project Purpose and contributed to achieve Project Purpose.
(3) Efficiency
Efficiency is generally high. Most part of Inputs was implemented as planned and contributed to produce sufficient Outputs.
Most Japanese experts had adequate knowledge and experiences and helped capacity development of Afghan C/Ps.
Training in Japan was effective to strengthen capacity of C/Ps. Participants in Training in Japan acquired skills and method of RH administration and utilize the fruit of the Training in their daily duties. Technical Exchange with projects in other countries was proved to be effective. Some C/Ps participated in Third Country Training provided by JICA in countries with situation similar to that of Afghanistan, e.g. Indonesia as Islamic country, and Cambodia in a reconstruction process. These training courses also helped to enhance knowledge and administrative skills of RHO as they can share similar experiences.
Equipment and materials provided by Japanese side are adequate in terms of specifications and quantity. Malalai Maternity Hospital Training Center provided by the Project serves well as a basis of training activities. Dasht-e Barchi District Hospital Training Center opened only in May 2008 and is not

xiv
fully utilized yet at the time of terminal evaluation. Recently the organogram in regard to Dasht-e Barchi District Hospital Training Center was approved and the Training Center is placed under the Dasht-e Barchi District Hospital and KPHD. However, the Training Center is not positioned as regional training center.
All the national staff of the Project has high capacity and strong commitment and made essential contribution to the Project implementation.
The Afghan side allocated C/Ps with sufficient capacity and ownership to implement the Project. The budget for operational cost by the Afghan side is limited. It was difficult for MoPH to provide expenses of maintenance cost for equipment and materials, and the cost for supervision and training was basically born by the Japanese side.
As a part of partnership, the Project successfully planned provision of drugs in collaboration with other donors. This collaborative support made smooth progress in the beginning. However, the share of partner donors was not implemented as planned.
Inputs were generally well utilized and contributed to implement planned activities and to produce Outputs.
The Project implementation process was affected by security to some extent. As to Important Assumptions, replacement of C/Ps occurred quite frequently in the first part of the
Project, causing inconvenience in smooth Project implementation sometimes. After the Mid-Term Review, the C/Ps remain stable in their positions.
(4) Impact
Overall Goal is expected to be achieved if the current benefit of the Project is sustained and activities are expanded after the Project period. The foundation of RH administration is being established through capacity development of RHD and RHO, and the capacity of service providers is being improved through establishment of training mechanism. If the capacity of RHO and service providers is continuously improved, quality maternal and newborn health services are expected to be expanded. It should be noted, however, that achievement of Objectively Verifiable Indicators of Overall Goal, i.e., the number of people benefiting from the RH services, depends on conditions outside of framework of the Project. In order that people enjoy benefit of the RH services, some important factors other than capacity of RHO and service providers should be fulfilled: access to health facilities and security, to name a few.
It is expected that this Project will make great contribution to human security in Afghanistan as reproductive health is an important issue in human security.
Unexpected positive impact is observed. The Project aims to establish referral system in reproductive health in Kabul City as Output 3. During implementation of activities, those involved in the Project realized that it is necessary to develop policy and strategy to build more comprehensive health systems in urban Kabul.
One negative impact is pointed out. The Project made suggestion to convert policlinics to DH (District Hospital) and CHC+ (Comprehensive Health Center with 24-hour service) in Kabul City. Out of nine policlinics, two were converted to DH and one to CHC+. When the policlinic was converted to CHC+, the number of staff was reduced. According to interview, it is estimated that 30 to 40 employees, including workers, lost their job.
xv
(5) Sustainability Sustainability is generally high in terms of policy, technical, and institutional aspects, but financial
sustainability is not expected without external support. The policy to put importance on reproductive health is expected to continue. In ANDS, which describes
policy until 2013, reproductive health is a prioritized area. Technical sustainability is quite high. Those who were trained by the Project, including RHOs, training
coordinators, trainers, and service providers have acquired knowledge and skills to implement their duties on their own. Most of them have strong commitment to execute their responsibilities as well. To enhance sustainability, continuous capacity development is required. It is also important to conduct training when staff is replaced.
Institutional sustainability is also high. RHD was strengthened as an organization and RH program was developed. Training Centers were constructed by Japanese support at Malalai District Hospital and Dasht-e Barchi District Hospital. Training Department was established at Malalai Maternity Hospital and training center regulations were developed. Activities introduced by the Project are expected to be sustained.
Financial sustainability is the concern. MoPH is not provided sufficient budget to implement its responsibilities. The majority of the budget is allocated to personnel cost and running cost is limited. There is not an established mechanism to allocate budget to training and supervision. Therefore, the Malalai Hospital Training Center is not provided with enough budget to conduct training courses and supervision. KPHD is not provided with sufficient budget either. To conduct training and supervision introduced by the Project, it is necessary to secure the budget, especially in terms of running cost.
3-2 Factors that promoted realization of effects
One of contributing factors to achieve Project Purpose is strong commitment of both Japanese experts and Afghan C/Ps. Another contributing factor is the situation of RHD at the start of the Project. The Project was launched soon after MoPH set up RHD and appointed Deputy Minister in charge of reproductive health. Almost simultaneous start of the Project promoted smooth implementation of the Project. 3-3 Factors that impeded realization of effects
One concern to fully achieve Project Purpose is that the trained service providers sometimes leave their position. 3-4 Conclusion
The Project has been implemented appropriately in general and the Project Purpose is being achieved in spite of difficult situations in Afghanistan. Project implementation process was promoted by strong commitment of C/P organizations led by Deputy Minister. As a result, the capacity of RHOs and RH service providers has been significantly increased and it is expected that they will be able to continue their tasks on their own to some extent.
The three Outputs are also being achieved. National Reproductive Health Program is established although it is not yet in documentation. National Reproductive Health Program is established but further capacity development of RHD is required. In-service training mechanism is being established but it is still necessary to strengthen the training management mechanism and the capacity of training coordinators, trainers, and service providers. RH system in Kabul City has been clearly improved as well. However, as

xvi
the RH system covers a variety of components, such as referral system and drug distribution, it is still necessary to further enhance the capacity of KPHD and strengthen RH system in Kabul City. 3-5 Recommendations Based on the results of evaluation, recommendations on actions to be taken during the remaining period of the Project are as follows. - MoPH will compile National Reproductive Health Program in documentation. - MoPH will complete the procedure for approval of developed training manuals and in-service training
guideline. - MoPH will compile and analyze HMIS data collected after the first quarter of 2008, and make decisions
based on the results. MoPH will strengthen the capacity of RHD staff in data analysis. - MoPH will translate Annual Report 2008 into English. - MoPH will have Dasht-e Barchi District Hospital Training Center function as regional training center and
improve the capacity of Dasht-e Barchi District Hospital as well. - MoPH will compile information on NGOs in collaboration with Grant and Contract Management Unit to
facilitate joint supervision with NGOs. - MoPH will make continuous effort to estimate, secure, and distribute budget to cover running cost for
management of training and supervision. During Evaluation, the following suggestion was raised. It may not be a matter to be considered during the
remaining Project period, but it is desirable to give consideration. - Although Dasht-e Barchi District Hospital meets the requirement of number of staff specified by BPHS,
the staff is not sufficient to adequately conduct increasing deliveries. The criteria of BPHS may not be appropriate in urban situation. It is recommended to review BPHS and revise BPHS regulations to be adopted in urban area.
3-6 Lessons Learned
Through the Terminal Evaluation of the Project, following lessons learned were extracted. - When a certain input is implemented in collaboration with other donor agency, it is important to assure that
expected input by partner agency will be surely implemented. - Personnel replacement occurs frequently in a country in the process of reconstruction like Afghanistan.
In this case it is effective to establish the results of activities in documentation to sustain the activities and achievements of the project.
-1-
第1章 終了時評価調査の概要 1-1 終了時評価調査の背景と目的
アフガニスタン国は、世界で最も保健状況の劣悪な国の一つであり、妊産婦死亡率が10万出
生当たり1,600(2004年 公衆衛生省)と、世界で最も劣悪な状況にある。これは、社会因習的及び物理的な問題から、リプロダクティブ・ヘルス(Reproductive Health:RH)サービスへのアクセスが非常に困難であること、また、特に女性の保健医療人材の質・量の不足、脆弱な保
健システムが原因となっている。このため、RH分野の政策立案及び実施運営能力の強化、看護師及び助産師への技術水準向上などの人材育成をすることは、RH事業の推進のために不可欠である。
アフガニスタン国公衆衛生省(Ministry of Public Health:MoPH)は、妊産婦死亡率の低下を目標として、2004年1月にリプロダクティブ・ヘルス部(Reproductive Health Directorate:RHD)を設置した。RHDは、「質の高い家族計画サービスへのアクセス向上」「産科救急ケアへのアクセス向上」「訓練された介助者による出産介助を増やす」の3つの政策目標を実現する
ため、人材育成を統括する人材開発部と各州の保健局と連携し、各州へのRH行政官の配置と、マラライ産科病院をはじめとする産科教育病院でのRH分野の保健医療サービス提供者の育成を行っている。
以上を背景とし、アフガニスタン国政府は、RH事業の強化を図るために、我が国に対して技術支援要請を行った。
本プロジェクトは、プロジェクト目標「保健サービス基礎パッケージ(Basic Package of Health Services:BPHS)、病院サービス必須パッケージ(Essential Package of Hospital Services:EPHS)1 に基づいた必要なRHサービスを提供するためのRH行政官とRHサービス提供者の能力が向上する」を達成すべく、2004年9月より開始した。今般、2009年9月にプロジェクトの終了を迎え
るにあたり、①これまでの活動状況をレビューし、Project Design Matrix(PDM)指標の達成状況を把握すること、②活動実施プロセスにおける効果発現の貢献要因・阻害要因を分析して他
の類似プロジェクトへの教訓を導くこと、加えて、③残り半年間の活動期間に対応すべき事項
について整理するとともに、採択済みのフェーズ2プロジェクトの方向性について提言を行う
ことを目的に終了時評価調査団が派遣された。
1-2 対象プロジェクトの概要(PDM Ver.4に基づく)
(1)上位目標
母親と新生児に対する質の高い保健サービスの提供可能な地域が拡大される。
(2)プロジェクト目標
BPHS、EPHSに基づいた必要なRHサービスを提供するためのRH行政官とRHサービス提供者の能力が向上する。
1 BPHSは、あらゆる第一次保健施設で標準的な基礎保健サービスが提供され、住民に公平なアクセスが提供されるよう、アフガニスタン国政府が2002年より推進している国家標準である。EPHSは、病院サービスを強化することを目的とした国家標準を指す。

-2-
(3)アウトプット
1.国家RHプログラムが完成し、活用される。 2.卒後研修メカニズムが完成し、適切に維持される。
3.アーバン・カブールでRHシステムが機能する。
(4)活動
1-1 PRHO(Provincial Reproductive Health Officer:州保健局のリプロダクティブ・ヘルス行政官)とRHO(Reproductive Health Officer:リプロダクティブ・ヘルス行政官)の職務分掌を作成する。
1-2 中央レベルのRHOの研修を実施する。 1-3 州レベルのPRHOの研修ニーズ・アセスメントを実施する。 1-4 PRHOの研修プログラムを準備する。 1-5 PRHOの研修を実施する。 1-6 PRHOの業務実績(パフォーマンス)を監督するメカニズムを開発する。 1-7 PRHOの業務実績を監督する。 1-8 カブールのBPHS施設の質確保(QA)プログラムを実施する。 1-9 PRHOとRH局間における報告システムを確立する。 1-10 EPHS施設における治療技術実施要項を開発する。 1-11 MoPH関連部署と開発パートナー間の調整機能を強化する。 1-12 中央レベルのRHOに対しマネジメントの研修を実施する。 1-13 RHOから住民に対するRHアドボカシー活動を支援する。
2-1 研修病院としてマラライ産科病院の治療サービスが向上するようにマネジ
メントを強化する。
2-2 内外的に研修の調整機関として、マラライ産科病院の研修部を確立し維持する。
2-3 郡病院レベルに研修センターを設立する。
2-4 母子保健サービス分野における標準的な研修を調整し開発する。
2-5 国家研修調整機関を設立する。
2-6 他国と技術交換プログラムを実施する。
2-7 研修カレンダーをアップデートする
2-8 標準化されたプロセスと教材のある研修プログラムを開発する。
3-1 保健施設と住民におけるベースライン調査を実施する。
3-2 アーバン・カブールの保健計画を作成する。
3-3 ポリクリニックをBPHS施設に転換し、CHC(Comprehensive Health Center:広域保健センター)とCHC+をアップデートする。
3-4 アーバン・カブールのロジスティックス・システムを修正し実施する。
3-5 PRR(Priority Reform and Restructuring:公募と選考による公務員登用制度)プロセスを促進する。
3-6 カブール州保健局と州保健行政官(Provincial Health Officer:PHO)の能力を強化する。

-3-
3-7 アーバン・カブール・コミュニティベース保健ケアシステムを確立する。
3-8 アーバン・ヘルス関連パートナーの活動を調整する。
3-9 継続ケア(Continuum of Care:COC)研修の準備をする。 3-10 サポーティブ・スーパービジョンのマニュアルを作成する。
3-11(内外の)サポーティブ・スーパービジョン・チームを結成する。
3-12 サポーティブ・スーパービジョンとフィードバックを実施する。
3-13 リファラル・システムを強化する。
3-14 HMISシステム(Health Management Information System:保健管理情報システム)を強化する。
3-15 アーバン・カブールにおいて産科病院間の調整機能を確立する。
1-3 調査団の構成
担当分野 氏名 所属
団長 渡部 晃三 JICA人間開発部保健行政・母子保健グループ保健行政課長
母子保健 尾崎 敬子 JICA人間開発部課題アドバイザー
協力計画 山形 律子 JICA人間開発部保健行政・母子保健グループ保健行政課職員
評価分析 田中 恵理香 グローバルリンクマネジメント(株)社会開発部研究員
1-4 調査日程
活動内容 活動場所 宿泊
1 17-Apr Fri 11:35 東京→デリ → カブール 機内泊
2 18-Apr Sat AM カブール着 PM ナデラ副大臣表敬・RHD及びKPHD C/Pとのミーティ
ング・日本人専門家へのインタビュー カブール カブール
3 19-Apr Sun
AM マラライ産科病院C/Pへのインタビュー・マラライ産科病院視察・リプロ部のC/P及びショコマンド保健サービス局長へのインタビュー
PM RHD C/Pへのヒアリングとブレインストーミング・USAID Dr.スミスからヒアリング・アハマドジャン政策局長表敬・JICAアフガニスタン事務所長表敬・団内打ち合わせ
カブール カブール
4 20-Apr Mon
AM KPHD C/P・ナショナルスタッフへのインタビュー PM ダシュテバルチ郡病院、研修センターC/Pへのインタ
ビュー・ダシュティバルチ郡病院、研修センターの視察・団内打ち合わせ
カブール カブール
5 21-Apr Tue AM PCMワークショップ(プロジェクト実施確認、成果、
課題の同定) PM RHDでの協議(フェーズ2について)
カブール カブール
6 22-Apr Wed AM ナショナル・スタッフへのインタビュー・カブール
RHO Dr.ラジアへのインタビュー PM HSSPでのヒアリング・団内打ち合わせ
カブール カブール
7 23-Apr Thu AM オスモイヨCHC視察・HHS アリシンギ氏ヒアリング PM 団内協議
カブール カブール

-4-
8 24-Apr Fri
AM Dr.ラフマン(2007年第三国研修参加者・IMCIフォーカルポイント)からヒアリング・団内協議(フェーズ2について:プロジェクト)
PM 団内協議(フェーズ2について:磯野専門家)・団内協議(合同評価報告書:プロジェクト)
カブール カブール
9 25-Apr Sat
AM RHDとの協議・NGOのMOVEでヒアリング PM KPHDとの協議(タマナ副局長)
ナデラ副大臣・ハミダRHD部長、アハマドジャン政策局長との協議(合同評価報告書) 団内打ち合わせ(JICA事務所・在アフガニスタン日本国大使館報告)
カブール カブール
10 26-Apr Sun
AM RHDとの協議(ハミダ部長ほか) Dr.カディール(WB Strengthening Mechanismプロジェクト代表)にヒアリング
PM M/Mサイン(合同評価報告書)
カブール カブール
11 27-Apr Mon AM RH部との協議(フェーズ2) PM JICA事務所報告・大使館報告
カブール カブール
12 28-Apr Tue AM 団内打ち合わせ
C/Pとの会食 PM 団内打ち合わせ
カブール カブール
13 29-Apr Wed AM ハイルハナCHC(結核調査団への同行) PM カブール発
カブール 機内泊
14 30-Apr Thu ドバイ着→関空着→羽田着
15 1-May Fri 追加調査 資料整理(コンサルタント)
16 2-May Sat ドバイ着→関空発→羽田着(コンサルタント)
1-5 主要面談者
(1)公衆衛生省(Ministry of Public Health:MoPH) Dr. Nadera Hayat Burhani Deputy Minister for Public Health( Health Care Services
Provision) Dr. Ahmad Shah Shokohmand General Director, Health Care Service Provision Dr. Ahmad Jan Naeem Acting GD, Policy & Planning Dr. Hamida Ebadi Director, Reproductive Health Directorate(RHD) Dr. Sadia Ayubi Head of Safe Motherhood Initiative Unit, RHD Dr. Najiba Yaftali Safe Motherhood Initiative Officer, RHD Dr. Karima Mayar Head of Family Planning Unit, RHD Dr. Hamra Khan Head of Gender Unit, RHD Dr. Sohaila Ziaee RH Coordinator, RHD Dr. Edris Toukhi RH Training Coordinator, RHD Dr. Farzana Salimi RH Training Coordinator, RHD(前任者) Dr. Homayee Leader of Reform Implementation & Capacity Development Mr. Jafar HMIS Consultant, HMIS Department Dr. Basheer Noormal Director of Afghan Public Health Institute Dr. Abdul Samih Waheb Trainer, Afghan Public Health Institute Dr. Mir Lais Mustafa Director of Public Health Research

-5-
Dr. Nastin Oryakhail Director of Malalai Maternity Hospital Dr. Homa Kabiri Director of Malalai Training Center Dr. Homa Akseer Deputy Director of Malalai Training Center Ms. Nafisa Amiri Training Coordinator of Malalai Training Center Dr. Abdullah Bakhteyari Director of Dasht-e Barchi Hospital Dr. Marzia Director of Dasht-e Barchi Training Center Ms. Rokeya & Ms. Adela Training Coordinator of Dasht-e Barchi Training Center Mr. Safa Director of Central Warehouse
(2)カブール保健局(Kabul Provincial Health Directorate:KPHD) Dr. Fazil Karim Saidi Director, KPHD Dr. Saheb Noor Tamana Deputy Director(Urban Health) Dr. Razia Ferozi RH Officer Mr. Ghulam Mohamad Pharmacy Officer
(3)国連児童基金(United Nations Children’s Fund:UNICEF) Dr. Henry Mdebwe Health and Nutrition Officer Dr. Adeline Aslak MCH Officer Dr. Malalai Health Officer
(4)米国国際開発庁(United States Agency for International Development:USAID) Dr. Faiz Mohammad Health Team Leader, Office of Social Sector Development
(5)USAID/MOVE Welfare Organization(MOVE) Dr. Abdul Malek Director
(6)ジョンズホプキンス大学系保健NGO(Non-for-profit International Public Health Organization affiliated with Johns Hopkins University:JHPIEGO)/保健サービス支援プログラム(Health Service Support Program:HSSP) Dr. Nasratullah Ansari Technical Advisor
(7)米国保健省(Health and Human Services:HHS) Dr. Alishungi Program Manager
(8)世界銀行(World Bank:WB)/Strengthening Mechanism Project Dr. Abdul Qadir MoPH SM Coordinator
-6-
(9)Italian Cooperation Dr. Arif Oryakhail Expert
(10)JICAアフガニスタン事務所 木邨 洗一 所 長 渡辺 健 次 長 大宮 航時 所 員 村上 淳 所 員 十川 早苗 健康管理員 Dr. Khyber Hassas Program Officer(Health)
(11)リプロダクティブヘルスプロジェクト 立山 恭子 チーフアドバイザー/地域保健 石嶋 忠行 業務調整 Ms. Hangama Hamid RH Program Officer Mr. Rabiulla Mayar Wardak Assistant Project Coordinator Mr. Nasir Ahmad Ahmady Provincial Health Coordinator Ms. Nasrin Azizi Training Coordinator Ms. Nargis Jawad Technical Assistant Mr. Suleman Pakray Administrative Assistant
(12)結核対策プロジェクト 磯野 光夫 チーフアドバイザー(国際協力専門員)
(13)在アフガニスタン日本国大使館 井上 賢司 経済協力班二等書記官 木村 修平 経済協力班二等書記官

-7-
第2章 終了時評価の方法 2-1 評価調査の流れ
本評価調査は、JICAの「事業評価ガイドライン」に基づき、プロジェクト・サイクル・マネージメント(Project Cycle Management:PCM)手法により実施した。PCM手法に基づく評価は、①プロジェクトの諸要素を論理的に配置したプロジェクト・デザイン・マトリックス(Project Design Matrix:PDM)に基づいた評価のデザイン、②プロジェクトの実績を中心とした必要情報の収集、③「妥当性」「有効性」「効率性」「インパクト」「自立発展性」の5つの評価の観点
(評価5項目)からの収集データの分析、④分析結果からの提言・教訓の導出、という流れか
らなっている。 PDMの概要については、以下のとおりである。
<PDMの概要>
上位目標 達成されたプロジェクト目標の貢献が期待される長期の開発目標
プロジェクト目標 プロジェクトの終了時までに達成されることが期待される中期的な目標であり、「ターゲットグループ」への具体的な便益やインパクト
アウトプット プロジェクト目標を達成するためにプロジェクトが実現しなければならない、短期的かつ直接的な目標
活動 アウトプットの目標を達成するために投入を効果的に用いて行う具体的な行為
指標 プロジェクトのアウトプット、目標及び上位目標の達成度を測るもので、客観的に検証できる基準
指標データ入手手段 指標を検証するためのデータ・ソース
外部条件 各レベルの目標を達成するために必要な条件であるが、プロジェクトではコントロールできない条件
前提条件 プロジェクトを開始するために必要な条件
投入 プロジェクトの活動を行うのに必要な人員・機材・資金など
評価にあたっては、日本側とアフガニスタン国側の合同評価とし、評価結果を合同評価レポ
ート(付属資料1)に取りまとめ、合同調整委員会(Joint Coordinating Committee:JCC)で合同評価レポートを双方で検討し合意した。 2-2 評価5項目
本評価調査における評価5項目の定義は次のとおりである。

-8-
<評価5項目> 妥当性 評価時点においても、プロジェクト目標、上位目標が妥当であるかどうか
を、アフガニスタン国政府の政策、裨益者のニーズ、日本の援助政策との整合性の観点から検討する。
有効性 プロジェクトのアウトプットの達成の度合い及びアウトプットがプロジェクト目標の達成度にどの程度結びついているかを検討する。
効率性 プロジェクトの投入から生み出される成果の程度は、タイミング、質、量の観点から妥当であったかどうかを分析する。
インパクト プロジェクトが実施されたことにより生じる波及効果の正・負の効果を、当初予期しなかった効果も含め検討する。
自立発展性 協力終了後、プロジェクトによってもたらされた成果や効果が持続されるか、あるいは拡大されていく可能性があるかどうかを予想するために、制度的(政策的)側面、財政的側面、技術的側面からプロジェクトの自立発展性の見込みを考察する。
2-3 評価のデザイン
評価のデザインを策定するにあたり、討議議事録(Record of Discussions:R/D)、PDM、活動計画表(Plan of Operation:PO)、調査団報告書、事業進捗報告書、その他プロジェクト関連文書等に基づき、評価項目案を作成し評価グリッドにまとめた。評価項目は、評価分析団員が、
評価調査団との協議を経て確定されたものである。主な評価項目は、以下に示すとおりである。
評価グリッドの詳細は付属資料2のとおり。 <主な評価項目>
評価設問 5項目その他の基準 大項目 小項目
アフガニスタン国側
カウンターパート(C/P)とスタッフの配置
資機材の提供
ローカルコスト
日本側
専門家派遣
資機材の供与
C/P研修(本邦、第三国)
投入の予定は予定通りか
ローカルコスト支援
アウトプット1:国家RHプログラムが完成し、活用される
実績の検証
アウトプットは達成されているか
アウトプット2:卒後研修メカニズムが完成し、適切に維持される

-9-
アウトプット3:アーバン・カブールでRHシステムが機能する
プロジェクト目標は達成される見込みか
BPHSとEPHSに基づいた必要なRHサービスを提供するための、RHOsとRHサービス提供者の能力が向上する
上位目標の達成の見込みはあるか
母親と新生児に対する質の高い保健サービスの提供可能な地域が拡大される
活動は予定通り行われたか
プロジェクト運営実施システムは適切であったか
活動の進捗状況は予定通りか
治安などを含む環境に対して適切な対応が取られたか
モニタリングのしくみは適切か
PDMの修正は適切に行われたか
モニタリングは適切に実施されているか
外部条件の変化に応じた対応は行われたか
専門家とC/Pのコミュニケーションは円滑に行われたか
専門家とC/Pの関係は適切か
問題が生じた際に適切な解決方法が取られたか
C/Pのは高いか 相手国実施機関のオーナーシップは高いか
プロジェクト実施に際し適切な予算配分・人材配置を行っているか
実施プロセスの検証
関連機関との協力は適切に行われたか
アフガニスタン国の関連機関及び他の援助機関との連携は適切に行われたか アフガニスタン国の開発計画に照らした上位目標とプロジェクト目標の妥当性 アフガニスタン国のニーズに照らした上位目標とプロジェクト目標の妥当性 日本のODA政策に照らした上位目標とプロジェクト目標の妥当性
妥当性 上位目標とプロジェクト目標はドナーと相手国の政策及びターゲットグループのニーズと整合しているか
プロジェクト目標達成に照らしたアプローチの適切性
プロジェクト目標の達成度
各アウトプットのプロジェクト目標達成との関連性
有効性 プロジェクトの実施により、期待される効果が得られているか。プロジェクトは有効であるか
外部条件の影響
日本側投入の適切性 投入の規模、時期、コスト、効果は適切であったか アフガニスタン国側投入の適切性
投入の活用度
効率性
投入はどのように活用され管理されたか プロジェクト運営管理体制

-10-
プロジェクト実施の効果はあるか
上位目標達成の見込み
予期しなかった正のインパクト 予期しないインパクトが見られたか 予期しなかった負のインパクト
インパクト
外部条件の影響を受けたか 外部条件の影響
制度的(政策的)側面
財政的側面
プロジェクトの便益はプロジェクト終了後も持続する見込みか
技術的側面
自立発展性
自立発展性に関する貢献要因・阻害要因は何か
貢献要因・阻害要因
2-4 情報・データ収集方法
調査にあたっては、プロジェクト専門家、アフガニスタン国側カウンターパート
(Counterpart:C/P)、MoPH、カブール州保健局(Kabul Provincial Health Directorate:KPHD)、マラライ産科病院、ダシュテバルチ郡病院、ドナー機関等、関連機関担当者に対する質問票に
よるサーベイとインタビューを行った。質問票は、評価グリッドに基づき作成したものである。
質問票を付属資料3、その集計結果については付属資料4に掲載した。また、質問票・インタ
ビューによる調査に加え、MoPH、KPHD、病院の関係者の意見を幅広く聴取するため、ワークショップを開催した。ワークショップでは、PDMのアウトプット1、2、3のそれぞれにつき、達成状況とその阻害要因・貢献要因を洗い出した。ワークショップの結果については、付属資
料5を参照。 2-5 PDM
評価は、最新版のPDM(PDM Version 4:合同評価レポートANNEX 1)に基づいて実施した。

-11-
第3章 評価結果
3-1 プロジェクト実施プロセス
プロジェクト実施プロセスはおおむね順調で、予定していた活動はおおむね完了することが
できた。2008年8月にチーフアドバイザーが離任したあと、チーフアドバイザーが担当するこ
とになっていたドナー会議の調整等一部の業務が、2009年4月に後任が着任するまで行われな
かったが、プロジェクト全体の進捗に大きな影響はなかった。
PDMは3回改訂された。改訂はいずれも、参加型で適切なプロセスを経て行われた。日本人専門家、アフガニスタン国C/Pとも、PDMについて共通の認識をもっており、日々の活動の中で、適宜参照している。
日本人専門家とアフガニスタン国C/Pのコミュニケーションは良好であった。双方で日ごろから頻繁に会合をもち、問題があった場合には協議により解決することができた。プロジェク
ト関係機関間のコミュニケーションはおおむね良好であった。ただし、MoPHとKPHDの間でコミュニケーションの齟齬が生じることが時折あった。他の援助機関とのコミュニケーションは
MoPHのRHDが中心に調整を行っており、おおむねコミュニケーションは良好であったと判断される。
プロジェクト活動は、治安による影響が若干あった。治安状況の悪化により、スーパービジ
ョンが中止になったことが数回あり、また研修を延期することが何度かあった。2005年の9月
から10月にかけては、治安の悪化により、チーフアドバイザーと業務調整員を除く日本人専門
家が国外退避を余儀なくされた。しかしながら、スケジュールを綿密に調整し効率的に活動を
実施することで、予定の活動をほぼ完了することができた。
3-2 プロジェクトの実績
(1)投入の実績
アフガニスタン国側、日本側とも、PDM/POに基づき投入を行った。投入実績については、合同評価レポートのANNEX 2(2-1~2-6)を参照のこと。
(2)活動の実績
活動は、PDM/POに基づき実施された。活動実績の詳細は、合同評価レポートのANNEX 3を参照のこと。
(3)アウトプット達成の実績
1)アウトプット1:国家RHプログラムが完成し、活用される。 プロジェクト開始時は、RHDが創設されて2年程度しか経過していない時期であり、
当時は、組織としての整備に着手してあまり時間がたっていなかったため、人材の能力
も十分でなく、RHに関する業務が円滑に行われていなかった。プロジェクト開始当初に比較すると、RHDの組織能力は顕著に向上し、事業の計画・実施能力が向上している。RHDの組織能力の向上を具体的に示すものとして、以下のものが挙げられる。 ・「国家RH政策(Reproductive Health Policy 2006)」と「国家RH戦略(Reproductive Health
Strategy 2006-2009)」に基づき、「国家RHプログラム」が策定された。

-12-
・組織図が策定された。
・RHO(RH行政官)2 の業務内容(job description)が策定された。 ・年間活動計画及び研修計画が策定された。
・RH四半期ミーティングが定期的に開催されるようになった。 ・RHに関する事業の計画とモニタリングが四半期ミーティングで定期的に行われるようになった。
・スーパービジョンのメカニズムが構築され、サポーティブ・スーパービジョン 3 のマ
ニュアルが開発された。
・サポーティブ・スーパービジョンの質が向上し、スーパービジョンを受けた保健サー
ビス提供者によるRHケアサービスの質も向上している。 ・2007年に、年次報告書がダリ語と英語で作成された。2008年の年次報告書はダリ語の
み作成されている。
上記のうち、「国家RHプログラム」は、「国家RH政策」及び「国家RH戦略」を具体的な行動計画に移すための行動計画として策定されたものである。ただし、「RHプログラム」は、RHに関する業務分掌規定や個々の活動計画を統合したものを「プログラム」として呼んでいるものであり、まとまって文書化されたものではない。
アウトプット1の指標の達成状況は以下のとおりである。
<アウトプット1の指標達成状況>
1-1 国家RHモニタリング指標の四半期ごとの分析の実施
RHモニタリング指標がHMIS*担当部門で収集されRHDで分析されている。HMIS担当で収集している指標は6種類である。四半期ごとの分析が2008年の第1四半期までまとめられているが、その後は取りまとめが行われていない。
1-2 RHDからサポーティブ・スーパービジョンを受けた州の数が、2009年までに2007年の10州から増える。
サポーティブ・スーパービジョンを受けた州の数は、2007年には13、2008年には10、2009年の初めには2となっている**。
1-3 PRHOからRHDへの四半期報告の実施 報告のためのフォーマットが作成され、報告のしくみ(レポーティング・システム)が構築された。
*HMIS:保健管理情報システム(Health Management Information System) **2007年PDMを改訂した当初は10州であったのを指標の基準としたが、2007年終了までに13州となった。2009年は3月までのデータである。
2 RHOという呼称の示す範囲については、MoPH職員の間でも定義が一定しておらず、州のRH担当行政官も含める場合、あるいはMoPH本省のRHDのRH担当行政官だけを指し、州のRH担当行政官はPRHO(Provincial Reproductive Health Officer)と呼んで区別する場合などが見受けられた。本報告書では、特に断りのない限り、「RHO」は「RHD(公衆衛生省RH部)とPHD(州保健局)のRH行政官」を指すものとする。
3 サポーティブ・スーパービジョンでは、本省のRHOが保健施設を訪問し、規定のチェックリストを用いて各州のRHサービスの状況を調査する。その結果は各州のRHO及び施設長、RHサービスプロバイダーにフィードバックされ、助言指導が行われる。報告書はRHD部長へ提出される。

-13-
2)アウトプット2:卒後研修メカニズムが完成し、適切に維持される。
卒後研修メカニズムは構築されつつある。プロジェクトでは、カブール市内の第三次
病院であるマラライ産科病院とダシュテバルチ郡病院に、それぞれ研修センターを建設
し 4 、この2か所を研修実施の拠点として研修メカニズムを構築してきた。
マラライ産科病院研修センターにおいて、研修を計画・運営するメカニズムが構築さ
れた。研修部が設立され、組織図が策定された。日当支給や研修センター予約などの事
務を含む研修センター運営規則が策定され、トレーナーが訓練された。同研修センター
では、プロジェクト前半期から活発に研修を実施している。
ダシュテバルチ郡病院研修センターでは、評価時点では、研修メカニズムを確立する
途上にあるという状況である。同研修センターは、2008年4月に建設が完了し、同年5
月に正式にオープンし、10月に職員配置が完了したばかりである。現在、マラライ産科
病院研修センターの支援を得て研修センター職員の研修実施及び研修運営のための能
力強化を行っている。マラライ産科病院研修センターほど活発ではないものの、研修コ
ースを実施している。
研修メカニズム構築の一環として、研修教材が開発された。「COC 5 ラーニングリソースパッケージ」が開発され、RH研修運営委員会で承認された。すでに、MoPH内の保健栄養コンサルティンググループ(Consultative Group of Health and Nutrition:CGHN)に提出されており、その後、技術諮問グループ(Technical Advisory Group:TAG)に提出されることになっている。「卒後研修品質管理ガイドライン(Guideline for Quality Management of In-Service Training)」のドラフトが完成し、CGHNに提出されるばかりになっている。作成したマニュアル類については、合同評価レポートのANNEX2-5を参照。 プロジェクトでは、研修運営システム強化のため、データベース作成を導入し、デー
タインプットのための研修コースを実施した。研修データベースのフォーマットは、保
健サービス支援プログラム(Health Service Support Program:HSSP)6 が技術支援して開発された。
アウトプット2に関する指標の達成状況は、以下のとおりである。
<アウトプット2の指標達成状況>
2-1 MoPHによる研修コースの国家標準の承認
「卒後研修品質管理ガイドライン」ドラフトが完成し承認の手続中である。マラライ産科病院に研修部が設立された。研修部の組織図と業務内容が策定された。
2-2 MoPHによる“COCラーニングリソースパッケージ”の国家標準の承認
COCラーニングリソースパッケージが開発されCGHNに提出された。
4 プロジェクト開始当初は、カブール市の第三次病院であるマラライ産科病院を拠点として活動を行っており、病院の敷地内にプロジェクトの費用で研修センターを建設した。その後研修ニーズの拡大に伴い、マラライ産科病院のほかにも研修の拠点が必要となり、ダシュテバルチ郡病院の敷地に、緊急支援無償資金協力の残余金により研修センターを建設した。
5 本プロジェクトでは、「継続ケア(Continuum of Care:COC)」を「母親と子どもの継続的・包括的ケア」と「保健人材の卒後継続研修」を合わせた意味をもつものとして扱っている。
6 BPHS、EPHSを支援するためのプログラム。JHPIEGO(ジョンズホプキンズ大学の外郭団体)のプロジェクトでありUSAIDが中心となって支援している。

-14-
2-3 フォローアップとスーパービジョンを含めた研修プログラムが国家研修調整機関によって実施される。
フォローアップとサポーティブ・スーパービジョンを含む研修プログラムが実施されている。
3)アウトプット3:アーバン・カブールで、RHシステムが機能する。 KPHDは、2004年に設立され、設立から日が浅いが、プロジェクト開始当初に比べる
とRHOの能力は格段に向上し、日々の業務が円滑に実施されている。リファラル・システムの確立など今後の課題が残るものの、アーバン・カブールにおけるRHシステムが向上していると判断される。
RHOがRHプログラムを管理しスーパービジョンを実施する能力は、プロジェクト開始当初に比較し強化されている。スーパービジョンが活発に実施されており、州保健行
政官(Provincial Health Officer:PHO)と都市部の第一次保健施設の長によるアーバン・ヘルス月例ミーティングが開催されるようになった。保健サービス提供者の能力が強化
され、スーパーバイザーの支援のもと、記録を取るなどの業務を適切に行えるようにな
った。これにより、RH関連のデータが第一次施設から適切に収集され、KPHDのHMIS部門に報告されるようになった。
薬剤配布システムも向上した。薬剤配布担当のPHOの薬剤配布・在庫管理業務遂行能力が向上しており、また、薬剤供与については、プロジェクト及び他の援助機関による
支援により、保健施設における薬剤の配布状況が改善した。薬剤配布及び在庫に関する
情報は、KPHDによるスーパービジョンによって報告されている。 リファラル・システムは完全に導入されたとはまだいえない状況である。プロジェク
トでは、開始間もない時期から、保健施設を訪問し、モニタリングを実施し、関連機関
とリファラルに係る協議を続け、2009年2月にリファラルのためのフォーマットを開発
した。その後引き続き、リファラル・システムを確立するための協議を行っている。
アウトプット3に関する指標の達成度は以下に示すとおりである。指標の3-2と3-3は、
傾向としては、達成に向かっているといえる。設定された指標には、プロジェクトだけ
では達成できないものが含まれており、当初の指標の設定そのものがプロジェクトの成
果として達成困難なものとなっていた事情を考慮する必要がある。例えば、指標3-1の、
ポリクリニックのCHC+/県病院 7 への転換は、プロジェクトで取り組んだRHOの能力強化やKPHDの組織強化だけでは達成することが困難で、MoPHその他関連官庁を含む膨大な行政手続きを要するものである。また、リファラル・システムが機能すれば、正常
分娩は第三次病院でなく、DH、CHC+で取り扱われるものであり、指標3-2、3-3に示すとおり、正常分娩の取扱い数は、第三次病院では減少し、DH、CHC+では増加するはずである。しかしながら、実際には、患者がどのレベルの病院に行くかは施設へのア
クセスなども関係しているため、リファラル・システムの機能の度合いが施設別の正常
7 アフガニスタン国の保健サービス施設は、リファラルの下のレベルから順に、ヘルスポスト、基本ヘルスセンター(Basic Health
Center:BHC)、広域保健センター(Comprehensive Health Center:CHC)、県(郡)病院(District Hospital:DH)、三次病院となっている。三次病院は、カブール州内では、マラライ産科病院など4か所ある。CHCの中で24時間対応を行っているものを「CHC+」と呼んでいる。また、旧ソ連支配下時代における保健医療システムに基づいた施設を「ポリクリニック」と呼んでいる。ポリクリニックは、BPHS・EPHSで規定されたリファラル・システムの中で明確に位置づけられておらず、再編が必要となっていた。ダシュテバルチ郡病院は、プロジェクト開始当初はポリクリニックだったものがDHに転換されたものである。

-15-
分娩数の変化に反映されるとは必ずしも限らない。帝王切開の実施(指標3-4)は、プ
ロジェクトで強化しようとしたRHシステムのみならず、医師の臨床技術や施設の整備にもかかわってくる問題である。このように、PDMのアウトプット3に関する指標には、プロジェクトの活動だけでは達成できないものが含まれており、プロジェクトの成果を
適切に測るためには、指標の設定そのものをより検討しておく必要があったといえる。
上記のような指標の問題があるため、アウトプット3については、PDMの指標だけでは明確に判断できないが、インタビューやプロジェクトの記録等から、アーバン・カブ
ールにおけるRHシステムは強化されつつあると評価された。
<アウトプット3の指標達成状況>
3-1 2007年から2009年までに80%のポリクリニックがCHC+/郡病院に転換される。
9か所あるポリクリニックのうち、2か所が郡病院に、1か所がCHC+に転換された。
3-2 第三次医療施設における正常分娩の数が、2009年までに2007年より40%減少する。
第三次医療施設における正常分娩の数は、2007年に4,201件、2008年に3,886件で、7%減少している。
3-3 郡病院とCHC+における正常分娩の数が、2009年までに2007年より40%増加する。
郡病院とCHC+における正常分娩の月平均件数は、2007年に105件、2008年に268件であり、155%の増加となっている。
3-4 郡病院が2009年までに帝王切開を実施できるようになる。
2009年4月時点で、郡病院では帝王切開を実施していない。RHDでは、帝王切開導入に向けたアセスメントと技術支援を行っている。
3-5 アーバン・カブールでカブール保健局と施設内でサポーティブ・スーパービジョンをしている保健施設数
34か所の都市部保健施設のうち、5か所で、スーパービジョンに関するワークショップをパイロットベースで実施し、その後スーパービジョンを実施している。
(4)プロジェクト目標達成の実績
<プロジェクト目標>
BPHSとEPHSに基づいた必要なRHサービスを提供するためのRHO(RH行政官)とRHサービス提供者の能力が向上する。
プロジェクト開始当初に比較すると、RHOとRHサービス提供者の能力は向上していると判断される。COC研修のフォーカス・グループ・ディスカッションでは、カブール都市部における保健サービスに対する患者の満足度が向上していることが明らかになってい
る。スーパービジョン報告書及び終了時評価におけるインタビューによれば、保健施設に
おいてサポーティブ・スーパービジョンは好意的に受け入れられており、サポーティブ・
スーパービジョンの実施により、保健サービス提供者はスーパーバイザーと協議をしなが
ら建設的に問題解決を行うようになった、とのことである。HMISのデータによれば、RH関連の指標が全国平均で向上している。これら指標の向上にプロジェクトがどの程度の貢
献をしたかは明確にはわからないものの、RHOとサービス提供者の能力の向上は指標の向

-16-
上に貢献したものと考えられる。HMISデータの実績は以下に示すとおりである。
<HMIS統計によるRH関連指標>
2006年第4四半期 2007年第2四半期 2008年第4四半期
HMISを報告している施設の割合
70.6% 76.5% 87%
女性保健スタッフのいるBPHS/EPHS施設の割合
50.1% 60.4% 78%
2種類以上の近代的避妊方 法 を 提 供 し て い るBPHS/EPHS施設の割合
66.8% 68.7% 69%
施設分娩の割合 13.2% 25.0% 31%
近代的家族計画サービスを受けている生殖年齢の女性の割合
7.7% 12.4% 18%
少なくとも1回の出産前ケアを受けた妊婦の割合
57.9% 82.3% データなし
プロジェクト目標であるRH関連指標につき、RHDでは、PDMで設定されている指標のモニタリングと分析を行っている 8。HMIS部門を通じ6つの指標がRHDに報告されており、2つの指標は州のRHOからRHDに報告されている。データの収集は継続的に行っているものの、収集されたデータは、2008年第2四半期までは分析され、取りまとめられていたが、
その後分析が行われていない 9。分析が行われていない大きな要因は人材が適切に配置さ
れていないことで、プロジェクトでは、RHDの業務内容の策定を行ったが、TORにデータ分析が含まれている行政官が現在のところいない。
プロジェクト目標の指標達成状況は次のとおりである。RHDでは、8つの指標をモニタリングしている。インタビュー結果等から、指標の収集については、適切にモニタリング
されているといえる。前述したとおり、タイムリーな分析を行うことが課題になっている。
8 PDMのプロジェクト目標の指標は「公衆衛生省RHDによって適切にモニターされた成果指標の数」となっているが、これは、専門家等の支援なしにRHDがRH関連指標をモニタリングできることがRH行政能力を示している、という考え方に基づいたものである(インタビューによる)。
9 <HMIS統計によるRH関連指標>の2008年第4四半期のデータは、終了時評価用に、必要なデータのみ急ぎ取りまとめたものである。

-17-
<プロジェクト目標指標>
MoPH/RHDによって適切にモニターされた成果指標の数
HMISデータによりRHDでモニタリングを行っている6指標 ・HMISを報告している施設の割合 ・女性保健スタッフのいるBPHS/EPHS施設の割合
・2種類以上の近代的避妊方法を提供しているBPHS/EPHS施設の割合
・施設分娩の割合 ・近代的家族計画サービスを受けている生殖年齢の女性の割合
・少なくとも1回の出産前ケアを受けた妊婦の割合
州RHOの報告により収集されRHDでモニタリングされている2指標 ・基本的緊急産科ケアができる施設数 ・包括的緊急産科ケアができる施設数
3-3 評価5項目による評価結果
(1)妥当性
アフガニスタン国の開発政策とニーズ、日本の対アフガニスタン政府開発援助(Official Development Assistance:ODA)政策との整合性、及びプロジェクト・デザインの適切性の関連から、妥当性は高い。
プロジェクト目標と上位目標は、アフガニスタン国の開発政策と合致している。アフガ
ニスタン国家開発戦略(Afghanistan National Development Strategy:ANDS,2008-2013)では、RH・子どもの健康プログラムは優先分野になっており、妊産婦死亡率と5歳未満児死亡率の引き下げが保健分野の目標の中に掲げられている。
アフガニスタン国において、RH向上のニーズは非常に高い。妊産婦死亡率は出産10万件当たり1,600(2004年 MoPH)と非常に高く、RHサービスの向上とRHO・保健サービス提供者の能力開発は重要課題になっている。
プロジェクトは、日本のODA政策とも整合性がある。日本の対アフガニスタンODA政策における重点分野は、治安の改善、インフラ整備、教育及び保健・医療分野への支援強化、
農業・農村開発を中心とする地方総合開発、の4点であり(ODA国別データブック2008)、保健分野が含まれている。
プロジェクト目標達成のためにプロジェクトが採用したアプローチは適切である。RHDが設立されたのがプロジェクト開始のわずか2年前であったことを考慮すると、RHプログラムと人材開発のメカニズムを構築することは非常に適切であった。プロジェクトでは、
C/Pの個人レベル及び組織レベルのオーナーシップと能力を養成することに重点をおいていた。MoPHのRHD、KPHD、マラライ産科病院とダシュテバルチ郡病院の研修センター、保健施設を含むRHに関連する組織と人材の能力開発を行うことにより、コミュニティの人々に裨益する国家RH政策の実施を促進した。日本人専門家によるアフガニスタン国C/P

-18-
の能力開発は、自ら考え問題を解決する能力を開発するという概念に基づいたものである。
終了時評価調査中のインタビューでは、何人かのアフガニスタン国側関係者が、プロジェ
クトのアプローチにつき「魚を与えるのでなく魚の釣り方を教えるもの」とコメントして
いたが、このアプローチは、プロジェクト期間終了後にプロジェクトの便益を持続させよ
うとするものである。
プロジェクトのもう一つの特徴的な点は、公共部門におけるRHシステムの強化を図ろうとしたことである。BPHSは、2003年に開始後、NGOに委託して保健サービスの提供を行う「コントラクトアウト」によりアフガニスタン国の8割程度の地域で実施されるまでに、
カバー範囲が劇的に拡大したが、サービスの質を監督し維持するために、MoPHと州保健局がリーダーシップを取ることの重要性が高まっている。このため、プロジェクトでは、
スーパービジョンとリポーティングのシステムを構築した。これは、州保健局RHOとNGOのRHOが合同で、MoPH職員の保健サービス提供者とNGO雇用の保健サービス提供者に対しスーパービジョンを行い、改善のために必要なフィードバックを行うものである。
アフガニスタン国の経済社会復興に対する支援は、国際社会において非常に重要であり、
プロジェクトでは、他の援助機関との協調を重視した。これはアフガニスタン国の現状に
照らし適切であったといえる。RHDでは、全国RHワークショップを年2回開催しており、これには援助機関とNGOも参加している。ワークショップは、支援パートナーの会合の機会となっており、援助機関が開催費用を持ち回りで負担している。プロジェクトはワーク
ショップを援助機関の協調の場として活用し、研修を実施している。また、プロジェクト
では、アーバンヘルス・タスクフォースの調整をしており、これは、MoPHの保健サービス部及び関連部署、KPHD、援助パートナー機関による情報共有と問題解決の協議の機会となっている。
(2)有効性
アウトプット、プロジェクト目標とも達成されつつあり、有効性は高いといえる。
アウトプットはおおむね達成されつつある。国家RHプログラムが開発され、RHDの能力が向上した。マラライ産科病院研修センターでは研修のメカニズムがすでに確立されて
おり、ダシュテバルチ郡病院研修センターでも確立されつつある。今後達成すべき課題は、
開発された研修マニュアルがまだ公式な承認手続きの途上にあること、研修のレポーティ
ング・システムが構築されたがデータベースが開発されていないこと、である。アウトプ
ット1と2の指標はほぼ達成されている。アウトプット3のカブール市内のRHシステムについては、PDMでプロジェクトだけでは達成困難な指標が一部設定されていたこともあり、すべての指標が達成されているわけではないが、プロジェクト開始当初に比較するとカブ
ール市内のRHシステムは格段に整備されている。また、プロジェクトでは、公務員の人事制度改革であるPriority Reform and Restructuring(PRR)に関して助言を行うなど、PPRプロセス促進を効果的に支援した。カブール市内のRHシステムを完全に機能させるためには、KPHDの一層の能力強化とリファラル・システムの確立が必要である。 プロジェクト目標は達成されつつある。RHOの行政能力は、プロジェクト開始時に比較
すると顕著に向上しており、RHプログラムが適切に実施されている。RHサービス提供者の能力も向上しており、RHサービスが改善している(「3-2」の(4)の「HMIS統計に

-19-
よるRH関連指標」参照)。RHOとRHサービス提供者の能力を一層向上させるには、スーパービジョンと研修システムの強化が必要である。
プロジェクト目標達成の促進要因としては、日本人専門家とアフガニスタン国側C/Pの強いコミットメントが挙げられる。また、プロジェクト開始時のRHDの状況が、促進要因になった。すなわち、MoPHがRHDを創設してわずか2年ほど経過した時点でプロジェクトが開始されており、開始当時は、RH担当の副大臣が任命されて間もないころであった。RHDを整備していく時期とプロジェクトの進行がほぼ同時であったことが、プロジェクトには追い風となり、円滑な進捗を促進したといえる。
プロジェクト目標達成を阻害する可能性のある要因として懸念されることは、研修を受
けたサービス提供者で離職する者が時折見られることである。
アウトプットとプロジェクト目標は論理的につながっており、アウトプットはプロジェ
クト目標の達成に貢献した。アウトプットの1と2、すなわち、RHプログラムの確立と卒後研修メカニズムの構築はプロジェクト目標達成には不可欠なものである。アウトプット
3は、カブール市内においてRHシステムが機能するよう、RHD、RHOとサービス提供者の能力を強化しようとするものである。カブール市では、他地域の多くで実施されている
コントラクトアウトによるBPHSが実施されていないため、カブール市でRHシステムを構築することにより、RHD、RHO、サービス提供者が研修の成果を実践に活用する場となることが期待されていた。このような観点から、アウトプット3はプロジェクト目標と論理
的に関連性があり、プロジェクト目標達成に貢献したといえる。
(3)効率性
効率性はおおむね高い。専門家派遣以外の投入はおおむね予定通りなされており、アウ
トプットの発現に貢献した。
派遣された日本人専門家は、ごく一部の専門家が業務遂行に必要な十分な経験とコミュ
ニケーション能力を持ち合わせていなかったことが関係者のインタビューなどで報告さ
れているが、それ以外は、適切な専門性と経験をもち、アフガニスタン国側C/Pの能力向上に貢献した。2008年8月にチーフアドバイザーが離任したあと、後任が派遣されず、チ
ーフアドバイザーが担っていた一部の業務が遂行されない時期があった。本プロジェクト
に短期専門家として派遣実績のあった専門家が、2009月4月よりチーフアドバイザーとし
て派遣されている。
本邦と第三国におけるC/P研修は、C/Pの能力強化に有効であった。本邦研修参加者はRH行政に必要な知識と技能を習得し、研修の成果を日々の業務に活用している。研修の成果
は、ミーティングをもち他の職員と共有されている。また、C/Pをイスラム国であるインドネシアや、復興プロセスにあるカンボジア等、アフガニスタン国と類似の状況にある第
三国に派遣した。こうした研修は、他国からの参加者と類似した経験を共有できるため、
RHOの知識や行政スキルを向上させるのに効果的であった。一方、第三国研修参加者の一部は、研修内容と直接的な関連性の薄い業務を担当しているため、研修の成果を通常業務
に十分活用できていないことが報告されている。研修員の選考にあたっては、研修後の業
務環境を含め慎重に検討を行うべきであったと思料される。
日本側が供与した施設・機材は、仕様、品質、数量ともに適切であった。プロジェクト

-20-
で建設したマラライ産科病院研修センターは、研修活動の拠点として十分活用されている。
ダシュテバルチ郡病院研修センターは、2008年5月に正式に開所したばかりであるため、
評価時点ではまだ十分に活用されるに至っていなかった。職員が配置されたのは2008年10
月になってからであり、現在、研修メカニズムの構築を行っている過程である。ダシュテ
バルチ研修センターは、郡病院であるダシュテバルチ郡病院の敷地に建設されているが、
組織的位置づけが明確でない。最近、組織機構が承認され、KPHD、ダシュテバルチ郡病院の管轄下に置かれることが決定したが、カブール州近隣の州を含めた地域の中核となる
地域研修センターとしての位置づけにはなっていない。また、同研修センターに関する懸
念材料として、地理的条件が指摘されている。カブール市中心から約15km離れたところに位置しており、不便を感じる者がいると思われる。インタビューしたアフガニスタン国側
関係者の中では、一部の者からは周辺地域の治安を懸念する声が聞かれたが、治安は特に
問題ないとする者のほうが多かった 10。
プロジェクトで雇用したナショナル・スタッフは、全員が高い能力と強いコミットメン
トをもち、プロジェクト実施に不可欠な貢献を果たした。治安状況により日本人専門家が
国外退避を余儀なくされた時期には、ナショナル・スタッフが、プロジェクトを継続して
実施する重要な役割を担った。
アフガニスタン国側は、プロジェクト実施にあたり、十分な能力とオーナーシップをも
つC/Pを配置した。一方、アフガニスタン国側のプロジェクト運営コストの負担は限られたものであった。MoPHは、C/Pの人件費を負担していたが 11、それ以外のプロジェクトの経常経費の負担は十分でなく、資機材の維持管理に必要な費用を十分に支出することがで
きなかった。プロジェクトを円滑に運営するため、スーパービジョンや研修に係る費用は
基本的に日本側で負担した。
プロジェクトの実施体制は、適切であった。専門家とナショナル・スタッフ、アフガニ
スタン国側C/Pの間の日常の会合やJCCは、プロジェクトの活動を促進し関係者の合意を形成する場として機能していた。
パートナーシップ促進の観点から、薬剤供与は他ドナー機関と協調して行うこととして
おり、この計画はアフガニスタン国の状況に照らし適切であった。ただし、この協調体制
による支援は、活動の当初は円滑に進捗していたが、他ドナー負担分の供与が予定通り実
施されなくなっている。
実施された投入はおおむね適切に活用され、予定した活動の実施とアウトプットの発現
に貢献した。
プロジェクト実施プロセスは、治安状況により多少の影響を受けた。プロジェクトでは
治安には細心の注意を払っており、制限のある環境の中で計画された活動を行えるよう、
調整と工夫を図り、柔軟に対応しながらプロジェクトを遂行した。結果的にプロジェクト
実施は効率的であったといえる
活動から成果に至る外部条件の中でプロジェクトに影響を与えたものとしては、プロジ
ェクトの前半にC/Pの交替が頻繁にあったことが挙げられる。プロジェクトの円滑な実施
10 周辺は、アフガニスタン国では少数派の民族が多い地域で、これが治安に対する「印象」に影響を与えているとする意見もあった。 11 C/Pの人件費はアフガニスタン国側が負担しているが、MoPHには十分な予算が配分されておらず、一般に給与は生活の維持に十分な額ではなく遅配も起こっている。

-21-
に多少の支障があったことは認めざるを得ない。しかしながら、中間評価以降はC/Pの配置は安定し同じ職位にとどまっていた。
(4)インパクト
プロジェクトの便益がこの後も維持され活動が継続して拡大していけば、上位目標は達
成されることが期待できる。
RHD及びRHOの能力開発により、RH行政の基礎が確立されつつあり、研修メカニズムの構築を通じてサービス提供者の能力が向上している。終了時評価調査中には、具体的な
サービス受益者の数の推移については確認できなかったが、RHOとサービス提供者の能力が引き続き向上すれば、質の高い母子保健サービスの拡大が期待できると考えられる。上
位目標達成のモニタリングにあたっては、PDMの指標に留意が必要である。上位目標の指標は、RHサービスを受けた住民の数の増加であるが、これは、プロジェクトで取り組んでいるRHOとサービス提供者の能力強化を超えたプロジェクトの枠外の条件によるところが大きい。PDMでは、プロジェクト目標達成から上位目標達成への外部条件として、MoPHの資金確保を記載しているが、それ以外にも、保健施設へのアクセスや地域の治安、保健
施設のインフラ整備状況などの条件もかかわってくる。こうした条件を考慮し、上位目標
の達成に向けた取り組みを行い、そのモニタリングを行うことが必要である。
プロジェクトはアフガニスタン国の人間の安全保障に貢献することが期待されている。
RHは、人間の安全保障における重要な要素である。省レベルからサービス提供者に至る包括的な能力開発を通じRHの向上を図ることは、将来的な人間の安全保障の向上に貢献するものと思料される。
予期せぬ正のインパクトが認められる。プロジェクトでは、アウトプット3の活動の一
環として、カブール市内においてRHのリファラル・システムを構築することを試みていたが、この活動を実施する中で、プロジェクト関係者は、カブール都市部においてRHのみならず保健システム全体を強化するための政策と戦略を策定することの必要性を認識した。
負のインパクトが1点報告されている。プロジェクトでは、カブール市内のポリクリニ
ックをDH/CHC+に転換することを提言し、9か所のポリクリニックのうち、2か所がDHに、1か所がCHC+に転換された。ポリクリニックがCHC+に転換される際、配置される職員数が削減されることになった。インタビューによると、庶務係等を含み30人から40人
が職を失ったと見積もられている。
(5)自立発展性
政策面、技術面、組織面での自立発展性はおおむね高いが、財政面での自立発展性は外
部からの支援なしには望めない状況である。
RHを重視する政策は継続するものと見られている。ANDSは、2013年までの戦略を規定しているが、RHは優先分野となっている。 技術的自立発展性はかなり高い。プロジェクトで研修を受けたRHO、研修コーディネー
ター、トレーナー、サービス提供者らは、担当業務を実施するために必要な知識と技能を
習得しており、また多くの者は責任を遂行する意欲をもっている。自立発展性を高めるに
は、引き続き能力開発を行うことが必要である。また、職員に人事異動があった場合には、

-22-
組織内で研修を実施することが重要である。
組織的能力の自立発展性も高い。RHDは組織として強化されており、RHプログラムが策定されている。日本の支援によりマラライ産科病院とダシュテバルチ郡病院に研修セン
ターが建設された。マラライ産科病院研修センターでは研修部が設立され、研修センター
規則が整備されている。ダシュテバルチ郡病院研修センターでも研修システムが整備され
つつある。このような運営のしくみが整備されていることから、両研修センターとも、プ
ロジェクトで導入された活動が継続するものと見込まれている。
財政的自立発展性が懸念材料となっている。MoPHには、その責務を遂行するだけの十分な予算が配分されていない。予算の大部分は人件費に割り当てられ、経常経費に充当さ
れる予算は限られており、研修やスーパービジョンに予算配分するしくみが存在していな
い。このため、マラライ産科病院研修センターでは研修コースやスーパービジョンを実施
する予算が十分でなく、KPHDの予算も同じ状況である。プロジェクトで導入した研修とスーパービジョンを継続的に実施するためには、特に経常予算の確保を行う必要がある。
3-4 結 論
アフガニスタン国の困難な状況にもかかわらず、プロジェクトはおおむね適切に実施され、
プロジェクト目標は達成されつつある。プロジェクト実施プロセスは、副大臣をはじめとする
C/P組織の強力なコミットメントにより促進された。その結果、RHOとRHサービス提供者の能力が顕著に向上し、さらに向上する必要はあるにせよ、当面の任務を自分たちで遂行していく
ことがある程度可能になっている。
アウトプットは3つとも達成されつつある。国家RHプログラムは、文書化が完了していないものの、すでに策定されている。策定された国家RHプログラムを継続的に実施するために、RHDの一層の能力強化が必要である。卒後研修メカニズムが確立されつつあるが、研修運営メカニズムと研修コーディネーター、トレーナーの更なる強化が必要である。カブール市内のRHシステムも、明らかに向上している。しかしながら、RHシステムは、リファラル・システムや薬剤配布を含む広範な要素を含むため、KPHDの能力をさらに高め、カブール市内のRHシステムを強化することがまだ必要である。
全体として、プロジェクトは顕著な業績を挙げてきた。プロジェクト開始当初のMoPH及び関連機関の人的・組織的・物的状況に比較すると、特筆すべきことといえる。プロジェクトの
便益を維持拡大していくためには、RHプログラム、卒後研修メカニズム、カブール市内のRHシステムのいずれも、さらに強化していく必要がある。終了時評価の結果を踏まえ、本プロジ
ェクトのフェーズ2ではRHプログラムの強化を中心としたプロジェクトを開始することを提言する。また、カブール市内において、RHシステムのみならず、保健システムを包括的に強化する新たなプロジェクトを立ち上げる予定である。
-23-
第4章 提言と教訓
4-1 提 言
評価結果に基づき、プロジェクトの残り期間で行うべきこととして、以下の点を提言する。
・MoPHは、開発された研修マニュアルと卒後研修ガイドラインの承認手続きを完了すること。 ・MoPHは、2008年年次報告書の英語訳を出版すること。
また、以下の点については、プロジェクトの残り期間中に取り組みを開始し、一部について
はフェーズ2で継続的に取り組むことを提言する。
・MoPHは、国家RHプログラムの文書化を行うこと。 ・MoPHは、2008年第2四半期以降に収集されたHMISデータの取りまとめと分析を行い、その結果に基づいた政策決定を行うこと。MoPHは、RHD職員のデータ分析に関する能力開発を行うこと。
・MoPHは、ダシュテバルチ郡病院研修センターを地域研修センターとして機能させ、あわせてダシュテバルチ郡病院の能力向上を図ること。
・MoPHは、資金贈与・契約管理部門(Grant and Contract Management Unit)と協力し、NGOに関する情報を整備し、NGOとの共同スーパービジョンを促進すること。
・MoPHは、研修とスーパービジョンの運営コストの予算を見積もり、予算確保・配分のための努力を引き続き行うこと。
・ダシュテバルチ郡病院は、BPHSの定める必要職員数を充足しているが、増加する分娩に適切に対応するには、まだ十分でない。BPHSの規定自体が、都市部における状況には適切でないことも考えられる。BPHSの見直しを行い、都市部におけるBPHS規定を改訂することが望ましい。
4-2 教 訓
終了時評価を通じ、同様のプロジェクトに適用される教訓として、以下の点が挙げられた。
・他の援助機関との協調により実施される投入がある場合は、パートナーとなる援助機関が予
定している投入が確実に実施されるか確認することが重要である。
・アフガニスタン国のように復興過程にある国では、人事交替が頻繁に起こることがあるが、
このような場合、プロジェクトの活動や成果を持続させるには、活動の結果を文書化するこ
とが効果的である。

-24-
第5章 所 感
5-1 母子保健団員所感
最初に、前チーフアドバイザーの離任後、次期チーフアドバイザーの着任までに空白があり、
また治安状況が悪化し、行動もさらに制約されるなかで、プロジェクトを実施してきたプロジ
ェクト日本人専門家及びナショナル・スタッフ、C/Pの熱意とコミットメントに深く敬意を表す。また、他のドナーの支援と対比させて、「魚の捕まえ方を教える」という本プロジェクト
のアプローチを表す比喩が、今回多数のC/Pから聞かれたことは、大変印象深いものであった。特に、協力の最初の拠点であったマラライ産科病院のC/P、次にMoPH/RHDのC/Pには、本プロジェクトのアプローチ、あるいはその基盤となる哲学が受け入れられ、彼らの中にそれが根付
いていることの証といえるだろう。
(1)RHの観点から 1)概要
現在、国レベルのデータとして利用できるものは、2002年のアフガニスタン健康調査
(Afghanistan Health Survey)である。高い妊産婦死亡率(1,600対出生100,000)に対し、その後様々な介入が行われており、最近のデータを取るために、現在、妊産婦死亡率調
査をUSAIDで計画中という情報を得た。なお、妊産婦死亡率など健康指標を考えるときに、地域差を捉える必要があるが-例えばカブール州418(235-602),Alisheng州774(433-1115),Maywand 2182(1451-2913),そしてRagh州6507(5026-7988)12、ただ、カブール州は国の人口の約10%(約350万人)を占めており、妊産婦死亡率は低いが妊
産婦死亡数が少ないわけではないことは言うまでもない。
アフガニスタンRH政策(2006)では、ヘルスケアへの障害を、三段階に整理している。第一に、個人、家族が問題を認識するか、問題と認識したうえで受療するか、第二に、
物理的に(距離・交通手段)、経済的にアクセスが困難ではないか、そして第三に、受
療した施設で質の高い迅速な治療を適切な保健医療従事者から受けることができるか、
である。後述するようにアクセス(第二)を高めるために、施設・サービスの配置は大
幅に進んできていた。これまで個人、家族へのアプローチ(第一)は委託NGOを中心に行われてきたが、行政の役割が意識され始めていた(RHD局長Dr.Hamida、USAID/HSSPのサブ委託先である現地NGOのMOVE)。施設におけるサービスの質(第三)のサービスの質については、後述する。
なお、本プロジェクトで支援してきた領域は、RHの中でも、主に母親の健康(含む新生児)であるが、家族計画などは含まれていない。また産科病院と小児病院の連携推進
など、小児に関する活動もあるが、MoPHにおけるC/PがRHDであることから、小児の健康はごく限定的に扱ってきたといえる(小児の担当は、小児及び青少年保健部)。
2)保健医療行政のあり方
アフガニスタン国では、サービスへのアクセスを保障するために、基本的なサービス
12 Barlett LA, Mawji S, Whitehead S et. al. Where giving birth is a forecast of death:maternal mortality in four districts of Afghanistan, 1999-2002.
Lancet. 2005Mar 5-11;365(9462):864-70.

-25-
パッケージ(Basic Package of Health Services:BPHS)をNGOに委託(コントラクトアウト)することで、サービスカバレジを飛躍的に伸ばしてきた。現在、カブール市など
いくつかの市を除いた全州においてBPHSをNGOに委託している。2002年の試算では一人当たり4.55米ドル、約80%の人口をカバーするに至った2006年の4ドナーのデータに
基づいた試算によると、人口一人当たり4.30~5.12米ドルで提供されており、行政機構
が脆弱な復興国においては効率的な手段とされている 13。
サービスを委託した州においては、委託されたNGOが実施者であり、NGOごとにRHOをおき、州における実施状況を監督している。州保健局のRHOは彼らと合同でモニタリングをし、技術的な助言を行う役割を担っている。プロジェクトでは、全国の州保健局
のRHOを集めた四半期会議を通じて支援してきた。さらに、今回RHD及び委託されたNGOからも州におけるコーディネーションの必要性と、州保健局のPRHOにマネージャーとしての技能を高めることを期待する声が聞かれた。
また、例外的にNGOでの委託が行われていないカブール市のRHサービスの強化を、本プロジェクトでは行ってきた。MoPHはカブール市などでのみ実施者(他州ではモニタリング・監督者)としての役割を担っていたからである。カブール市などでの実施を
通じて、政策と実施の間の乖離を確認し、現実的な政策を考える機会となっていたとい
える。このことは、今回のナデラ副大臣から、「カブール市で都市における保健医療サ
ービスを考えることが、NGOへの委託と国の政策をつなぐ役割を提供してくれた」という発言に現れている。
3)保健医療従事者の研修
現在、保健医療技術者の養成については、助産師学校の認定制度やカリキュラム作り
といった卒前研修と 14、RH卒後研修戦略(2007~2009年)やRH卒後研修指針案(2008年)が作成され、緊急産科ケアや家族計画などの卒後研修とも、整備が進んできている。
プロジェクトではCOC/LRP(継続ケアのためのラーニングパッケージ)を開発したが、RH卒後研修指針案に含まれており、サポーティブ・スーパービジョンによる研修後のフォローアップなどとセットになっていることなどがC/P側から評価され、現在承認過程にある「RH卒後研修指針」にも含まれている。 委託されたNGOは、スタッフの研修を含めてサービス提供を行うことになっている。
しかし、今回NGOスタッフの研修への要望がC/Pから聞かれ、またEmOC(緊急産科ケア)などの研修コンテンツ作りとトレーニングを提供してきたUSAID系ドナー(HSSP)も、対象とする13州以外にも全国の州保健局職員への研修を計画しているという。これは
NGO委託により施設数と要員数は確保されたが、サービスの質に関しては委託NGO間にギャップが存在することを示していると思われる。今後さらに、現状とNGO委託との整合性についての情報を集める必要がある。
RHに限らず、研修部門は個人の利益、省庁部署の利益、及びドナーの思惑があいまって、多くの国で最も整理しにくい分野の一つである。しかしながら、特にアフガニスタ
13 Newbrander W, Yoder R, Debevoise AB. Rebuilding health systems in post-conflict countries: estimating the costs of basic services. Int J Health
Plann Manage. 2007 Oct-Dec;22(4):319-36. 14 Smith JM, Currie S, Azfar P et.al. Establishment of an accreditation system for midwifery education in Afghanistan: maintaining quality during
national expansion. Public Health. 2008 Jun;122(6):558-67. Epub 2008 May 5.

-26-
ン国のように復興期(あるいは開発期)にあって制度作りの只中にある国では、ドナー
による重複を避けた制度作りをめざすべきは言うまでもない。例えば、フェーズ1で開
発されたCOC/LRPであるが、単純に展開地域をカブール市から全国に広げる(要請書の成果2)ことを計画する前に、卒後研修のしくみ作りをMoPHとしてどう考えるのか、それをフェーズ2でどのように支援していくのか、という段階を追った整理が必要にな
る。
4)フェーズ2に向けて
各種のRH関係の指針などの改訂時期に入ることから(RH戦略2006~2009年、RHインサービス研修戦略2007~2009年など)、RHタスクフォースにおいて作業が始まろうとしている。これらの改訂作業においてRHDをサポートし、その議論をフェーズ2にも反映させる必要がある。
今後、カブール市においてもJSDFにより、NGOへの委託が導入される見込みであることから、NGOへの委託を前提とした行政支援のあり方、更には委託後いずれ自律的に機能する行政をめざすのかを念頭において支援していく必要がある。
全国の医療従事者に実施された研修の現状(HSSPによる実施された研修のデータ、委託NGOへの技能研修が必要とされることを裏付けるデータ)、コミュニティへのアプローチの現状(現在の実施状況関する全体像、有効な事例)、州行政官の現状と課題など、
今回入手するように試みたがまだ収集しきれていない。このようなデータを分析し、フ
ェーズ1のC/Pを超えて、関係諸機関(含むAPHI、HRD、UNFPA、WHOなど)との協議を行い、デザインしていく必要がある。
フェーズ1は、まさにRHD(旧局)が産声を上げたときに始まり、RHDが整備されていくことに本プロジェクトは寄り添ってきた。そのことはアフガニスタン国側からも、
また他のドナー(HSSP)から評価されていた。何もないところから現在の段階まで整備されてきたことは評価できるだろう。フェーズ2は、この立ち位置を基準点として、プ
ロジェクトを形成していくことになる。RH及び母子の健康の問題は、この国において最優先課題であることからこそ、三大ドナーによるBPHSの目玉であり、それゆえにドナーの意向が強く影響する-言い換えればドナーが好き勝手をやってきた-分野である
こと認識しておく必要がある。すなわち結核などの感染症のように、垂直プログラムと
は異なる難しさを包含しているということである。ドナーの動向を含めて、状況の変化
も早い。それゆえにフェーズ2のデザインには、関係諸機関に関する十分な情報収集と
協議を経て、注意深く組み立てる必要がある。短期間の調査では十分に情報収集し協議
することは不可能であったため、JICAアフガニスタン事務所を中心に磯野専門員の助言も得ながらフォローアップをすることになった。
(2)最後に
初めてのアフガニスタン国であったが、インドネシアでの技術交換・第三国研修の受入
れ、そして各種国際会議などを通じて、知己であったアフガニスタン人と、今回の協議を
通じて複数名再会することができた。また、インドネシア大使館の若く意欲的な外交官た
ちとの交流からも多いに刺激を受けた。アフガニスタン国とインドネシアというイスラム
国同志の交流が生まれ、それをJICAも支援できたことは嬉しい。

-27-
大宮所員をはじめとしたJICAアフガニスタン事務所、立山チーフアドバイザー、石嶋調整員に、深く謝意を表す。彼らのサポートがなければ、今回の調査活動を無事に終えるこ
とはできなかった。プロジェクト終了まで無事に過ごされ帰国されることを祈念している。
また、前政策アドバイザーの四方先生、結核プロジェクトのリーダーで国際協力専門員の
磯野先生には、アフガニスタン国の保健医療状況・政策という大きなコンセプトを理解す
るために有用なご助言を数々いただいた。
5-2 団長所感
MoPH、KPHDをはじめとするアフガニスタン国側の各C/PとJICA専門家、ナショナル・スタッフ双方の尽力によって、本プロジェクトはこれまでに、様々な障害(治安関連、C/Pの交替、チーフアドバイザーが2008年8月から3月まで不在になるなど)に直面しながらも、おおむね
計画した活動を実施し、高い成果を上げてきたことを確認した。復興支援の段階にあるアフガ
ニスタン国において、人材育成を中心とする開発協力に、C/Pのオーナーシップを重視しながら、組織強化と制度化を後押しするキャパシティ・ディベロップメントに取り組み、持続性を
めざしてきた本プロジェクトの姿勢は、C/Pによく受け入れられ高く評価されながら、成果に結びついていた。これまで、治安対策上の制約の大きいなかで、忍耐強く活動に取り組んでこ
られたすべての専門家のご尽力に深く感謝申し上げる。
(1)MoPH/RHDの立ち上げからの支援の成果 これまでにプロジェクトが支援したRHDへの組織能力の強化や制度化支援の成果は、着
実に継続しているものと見受けられた。具体的には、RHO四半期会合の実施、PRHOへのスーパービジョンの継続、2回目のRHD年次報告の発行、インサービストレーニングガイドラインやCOC研修パッケージなどの組織的承認手続きの継続などである。RHDは、PRHOの育成をサポーティブ・スーパービジョンにより強化し、MoPHとPRHOの連携強化を図りながら、RH分野での技術的なリーダーシップを担うことへの強い意気込みが感じられた。この技術的リーダーシップとは、ANDSに記す行政の果たすべき役割でもある。 一方、チーフアドバイザー不在となったあと、RHDによる他ドナーやMoPH他部署との
調整機能は停滞気味と見受けられた(例えば、行政からのスーパービジョンを行ううえで
重要な地方でのBPHSのコントラクトアウト先のNGOに関する情報などを更新できていないことなど)。また、外部条件として、治安悪化によりスーパービジョンが計画通り実施
できなかった。
(2)インサービストレーニングとダシュテバルチ郡病院研修センターの活用
三次病院であるマラライ産科病院を拠点として国レベルの研修センターの設置を支援
し、プロジェクト前半での病院への技術的支援と後半の研修センター運営への支援を行っ
たことにより同研修センターの機能が強化され、MoPHのインサービストレーニング政策の実践とフィードバックのために重要な役割を果たすに至っており、同研修センターは本
プロジェクトの大きな成果となっている。また、プロジェクトが推進したCOC研修は、カブール都市部の助産師等への研修を行い(2008年7月現在、勤務者全員に対して完了)、
COC研修の重要な要素である研修後のスーパービジョンが有効に働いて、研修受講者の人

-28-
材育成の成果が上がっている。これらの成果は、フェーズ2でもプロジェクトの強みとし
て活用するべきである。
ダシュテバルチ郡病院研修センターについては、2008年の施設完成後、職員が配置され、
職員のトレーニングを短期専門家が行った結果、マラライ産科病院研修センターの協力を
得ながら同研修センターは活用を開始しつつある。センターの活用促進に向けてカブール
州RHOの意見を聞くと、全国各地の代表者を集めた研修などを誘致し、その中で要人が出席するセレモニーをメディアでPRするなどにより、一層の認知度を高めるとよいのではないかとの意見があった。
(3)カブール市都市型保健システム強化について
2008年7月に就任したKPHD局長は、強力に新しい方針を打ち出していたため、部下との間で軋轢を生じており、最近では郡部担当次長を交替させた。一方、C/Pの取り組みを中心としてそれを支援するとのJICAの協力方針に対する理解は進んだ模様である。保健情報の収集、医薬品ロジスティックなどに、プロジェクトの支援の成果が見られる。
また、カブール市内の保健施設の改善のための取り組みとして着手されたCHC+(24時間運営の基礎保健施設)へのPRRによる人材配置は進展(手続中)しつつあるが、お産を行うには技術的な強化も必要である。
今後、カブール都市部保健システム強化のプロジェクトを準備する際に、①本プロジェ
クトの成果をいかに有効活用するか、②カブールの事情に適合した世銀JSDF資金を活用した貧困層への保健サービス提供改善(総合政策局によりコントラクトアウトによることが
検討されているが、カブールの事情に適合させて契約内容などは適切にモディファイを図
ることが課題)のあり方、③コントラクトアウトの場合に契約先NGOと行政機構(KPHD)によるリーダーシップのあり方、などが課題である。事務所から実施中のMoPHとKPHDの関係者間の意見調整を踏まえつつ、2009年6月の事前調査を準備する。
(4)プロジェクト終了時までの取り組み
大統領選挙に伴う安全対策措置の関係から、実質的な日本人専門家の活動可能期間は7
月中旬までとなる見込みである。その間、評価報告書の提言にも記載した継続研修ガイド
ラインやCOC研修パッケージなどのMoPHにおける承認手続の完了への促進などに加え、RHDによるRHプログラムの成文化着手への支援なども、フェーズ1の成果定着のための重要な取り組みである。同時に、COC研修(カブール州郡部からの要望を検討中)、ダシュテバルチ郡病院研修センターの活用促進(研修手当等の運用規則を地理的な実情に応じ
た見直しなども検討課題)は、ナショナル・スタッフを活かしつつ継続実施願いたい。カ
ブール市都市型保健システム強化に関しては、短期専門家派遣を通じて、カブール都市部
保健システム強化のプロジェクトにつながる支援を継続する。

付 属 資 料
1.実施協議ミニッツ及び合同評価レポート
2.評価グリッド
3.質問票
4.質問票集計結果
5.ワークショップ結果








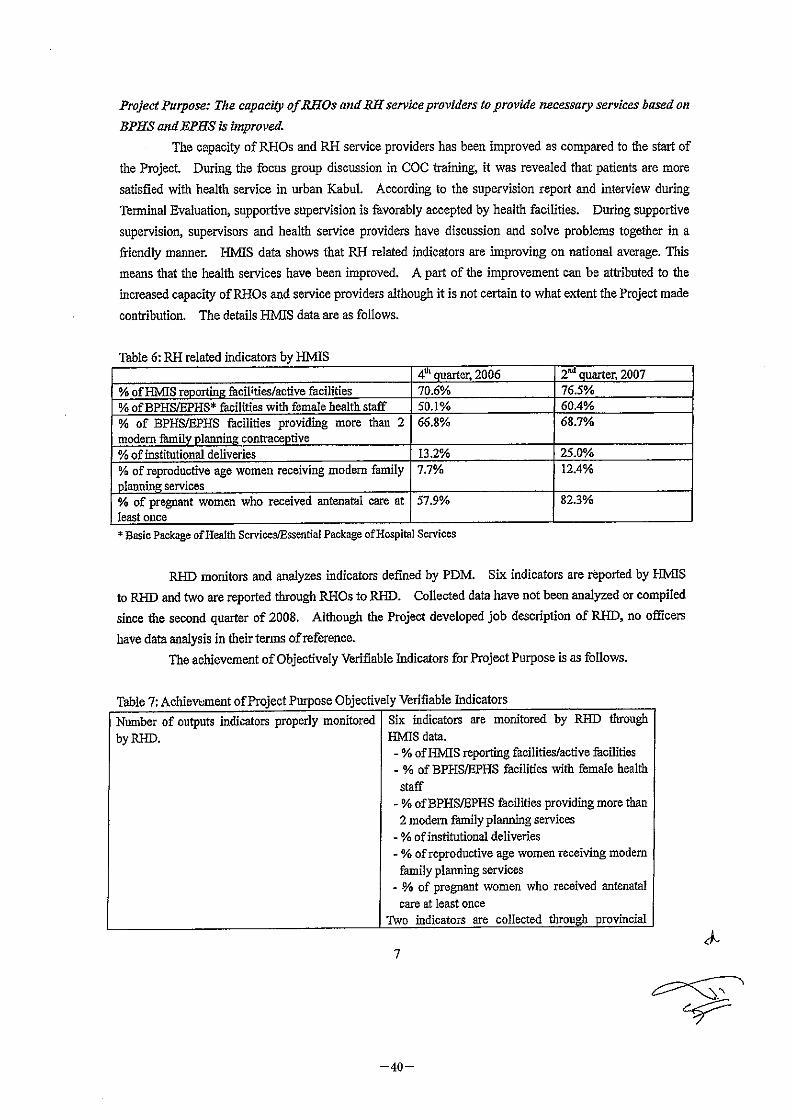






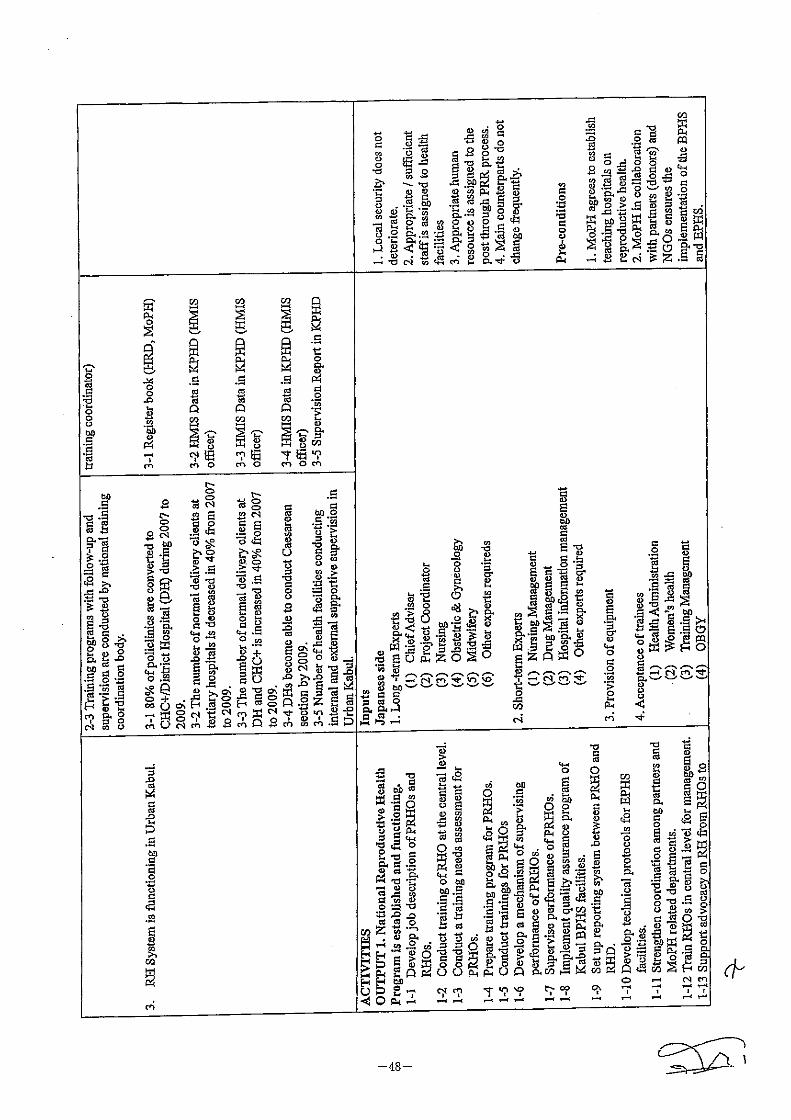







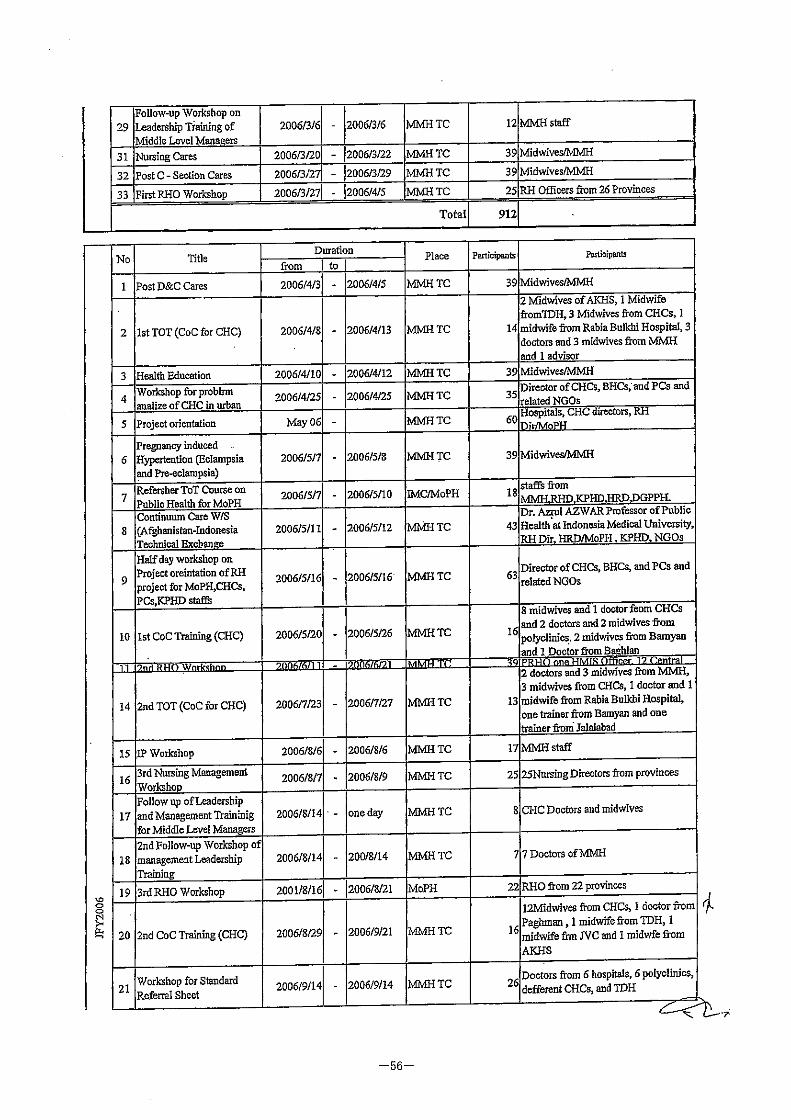






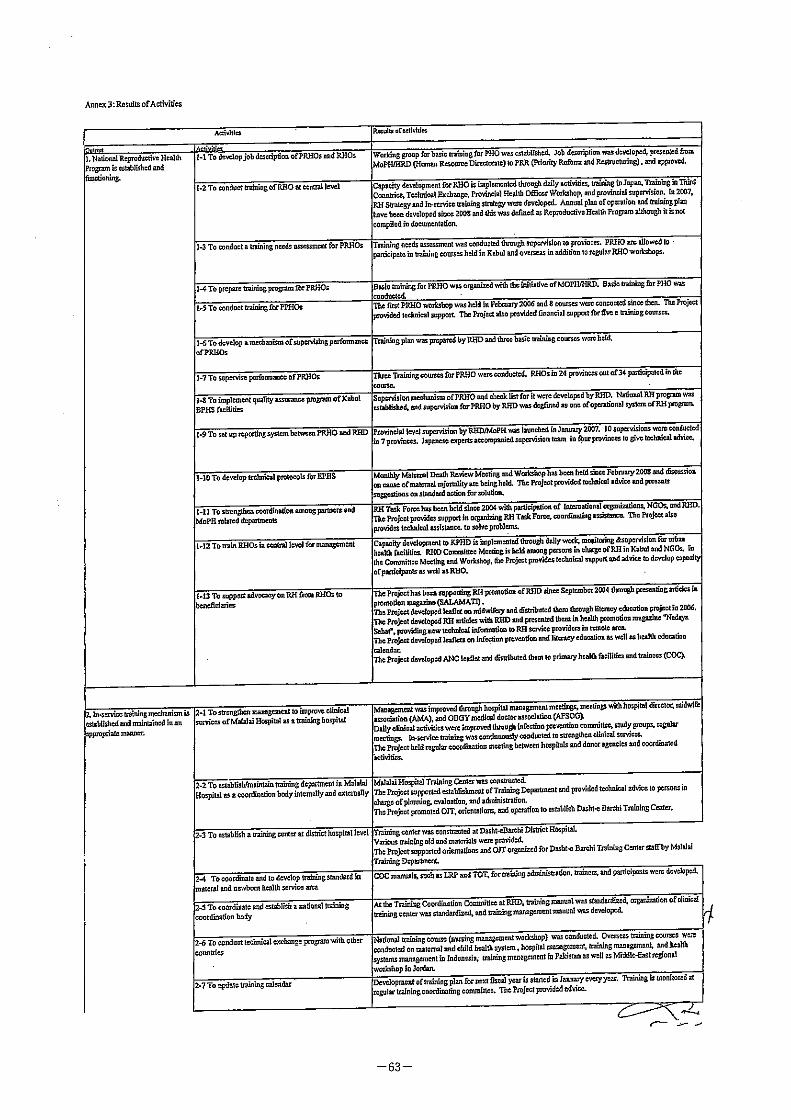



Evaluation Grid: Reproductive Health Project in Afghanistan
Evaluation item Criteria of evaluation Necessary data and information Data source Means of analysis
Achievement Afghan side
Assignment of counterparts andadministrative personnel
Comparison with initial plan. Relevance of input Record of assignment of counterparts andadministrative personnel
Project report, CP, experts Document review, Questionnaires,Interview
Supply of facilities and equipment Comparison with initial plan. Relevance of input Record of supply of facilities and equipment Project report, CP, experts Document review, Questionnaires,Interview
Local cost Comparison with initial plan. Relevance of input Record of local cost Project report, CP, experts Document review, Questionnaires,Interview
Japanese side
Dispatch of experts Comparison with initial plan. Relevance of input Record of timing, area and number of expertsdispatched
Project report, CP, experts Document review, Questionnaires,Interview
Supply of facilities and equipment Comparison with initial plan. Relevance of input Reocrd of timing, area and quantity of facilities andequipment supplied
Project report, CP, experts Document review, Questionnaires,Interview
Counterpart training in Japan and inthird countries
Comparison with initial plan. Relevance of input Record of timing, contents, number of CP trainingcourses in Japan and in third cocuntries
Project report, CP, experts Document review, Questionnaires,Interview
Local cost support Comparison with initial plan. Relevance of input Record of support of local cost Project report, CP, experts Document review, Questionnaires,Interview
Achievement of output 1. National Reproductive HealthProgram is established andfunctioning.
1-1 Quarterly analysis of national RH monitoringindicators is implemented.
1-1 Seven RH related indicators from HMIS data (RHDHMIS monitoring officer, provincial & central HMISofficer)
RH related indicators, Project report, CP,experts
Document review, Questionnaires,Interview
1-2 The number of provinces which received supportivesupervision by the RHD is increased in 2009 from 10 in2007.
1-2 RHD Supervision Report (RHD) RHD report, Project report, CP, experts Document review, Questionnaires,Interview
1-3 Quarterly reporting from PRHO to the RHD is inplace.
1-3 PRHO Activity Report (RHD) PRHD Report, Project report, CP, experts Document review, Questionnaires,Interview
Achievements other than indicators listed in PDM. Record of Project, opinions of related actors Project report, CP, experts Document review, Questionnaires,Interview
2-1 National standard for organizing training is approvedby MoPH.
2-1 National standards (RHD) National standards, Project report, CP,experts
Document review, Questionnaires,Interview
2-2 "Continuum of Care Learning Resource Package" isapproved by MoPH.
2-2 National training modules (RHD trainingcoordinator)
National training modules, Project report,CP, experts
Document review, Questionnaires,Interview
2-3 Training programs with follow-up and supervision areconducted by national training coordination body.
2-3 Training record (Training department at MMH andRHD training coordinator)
Training record, Project report, CP,experts
Document review, Questionnaires,Interview
Achievements other than indicators listed in PDM. Record of Project, opinions of related actors Project report, CP, experts Document review, Questionnaires,Interview
3-1 80% of policlinics are converted to CHC+/DistrictHospital (DH) during 2007 to 2009.
3-1 Register book (HRD, MoPH) Register book, Project report, CP, experts Document review, Questionnaires,Interview
3-2 The number of normal delivery clients at tertiaryhospitals is decreased in 40% from 2007 to 2009.
3-2 HMIS Data in KPHD (HMIS officer) HMIS Data, Project report, CP, experts Document review, Questionnaires,Interview
3-3 The number of normal delivery clients at DH andCHC+ is increased in 40% from 2007 to 2009.
3-3 HMIS Data in KPHD (HMIS officer) HMIS Data, Project report, CP, experts Document review, Questionnaires,Interview
3-4 DHs become able to conduct Caesarean section by2009.
3-4 HMIS Data in KPHD (HMIS officer) HMIS Data, Project report, CP, experts Document review, Questionnaires,Interview
3-5 Number of health facilities conducting internal andexternal supportive supervision in Urban Kabul.
3-5 Supervision Report in KPHD Supervision Report, Project report, CP,experts
Document review, Questionnaires,Interview
Achievements other than indicators listed in PDM. Record of Project, opinions of related actors Project report, CP, experts Document review, Questionnaires,Interview
Achievement ofproject purpose
Number of outputs indicators properly monitored by RHD RHD report, Project report, CP, experts Document review, Questionnaires,Interview
Achievements other than indicators listed in PDM. Record of Project, opinions of related actors, includingservice users
Project report, CP, experts Document review, Questionnaires,Interview
3. RH System is functioning in UrbanKabul
April, 2009
2. In-service training mechanisms isestablished and maintained in anappropriate manner.
Input
Items of investigation
The capacity of RHOs and RH serviceproviders to provide necessaryservices based on BPHS and EPHS isimproved
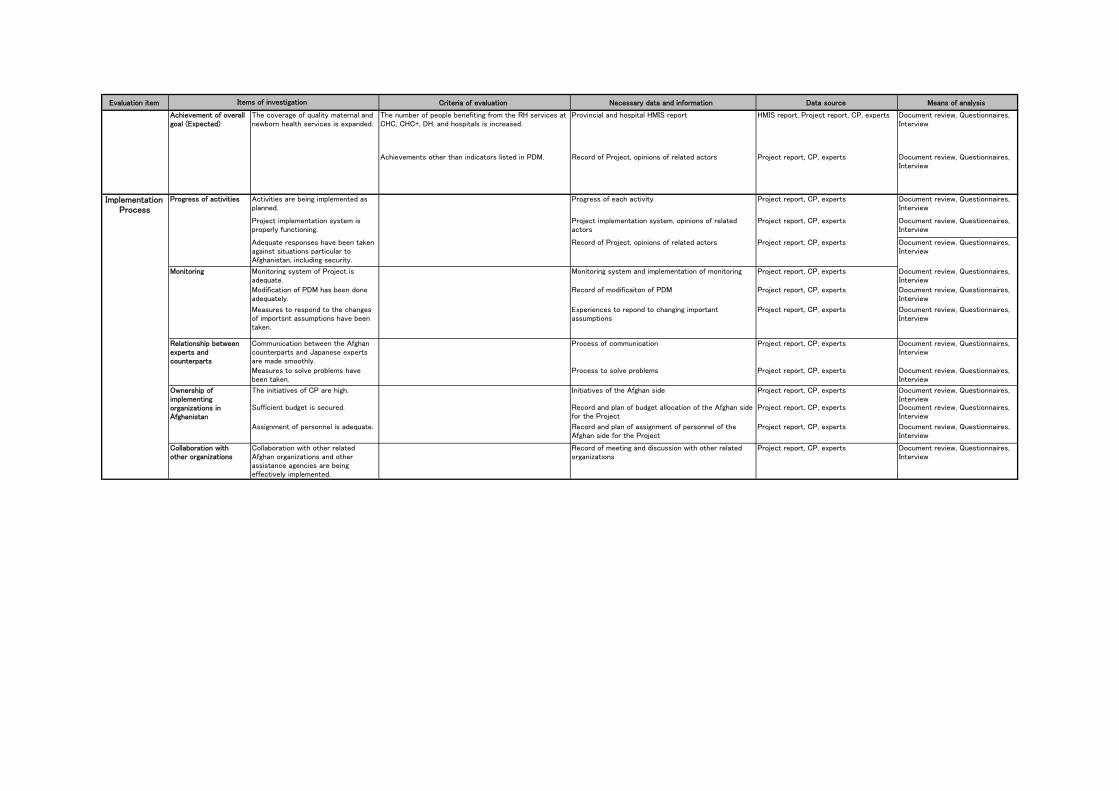
Evaluation item Criteria of evaluation Necessary data and information Data source Means of analysisItems of investigation
The number of people benefiting from the RH services atCHC, CHC+, DH, and hospitals is increased.
Provincial and hospital HMIS report HMIS report, Project report, CP, experts Document review, Questionnaires,Interview
Achievements other than indicators listed in PDM. Record of Project, opinions of related actors Project report, CP, experts Document review, Questionnaires,Interview
Progress of activities Activities are being implemented asplanned.
Progress of each activity Project report, CP, experts Document review, Questionnaires,Interview
Project implementation system isproperly functioning.
Project implementation system, opinions of relatedactors
Project report, CP, experts Document review, Questionnaires,Interview
Adequate responses have been takenagainst situations particular toAfghanistan, including security.
Record of Project, opinions of related actors Project report, CP, experts Document review, Questionnaires,Interview
Monitoring system of Project isadequate.
Monitoring system and implementation of monitoring Project report, CP, experts Document review, Questionnaires,Interview
Modification of PDM has been doneadequately.
Record of modificaiton of PDM Project report, CP, experts Document review, Questionnaires,Interview
Measures to respond to the changesof importsnt assumptions have beentaken.
Experiences to repond to changing importantassumptions
Project report, CP, experts Document review, Questionnaires,Interview
Communication between the Afghancounterparts and Japanese expertsare made smoothly.
Process of communication Project report, CP, experts Document review, Questionnaires,Interview
Measures to solve problems havebeen taken.
Process to solve problems Project report, CP, experts Document review, Questionnaires,Interview
The initiatives of CP are high. Initiatives of the Afghan side Project report, CP, experts Document review, Questionnaires,Interview
Sufficient budget is secured. Record and plan of budget allocation of the Afghan sidefor the Project
Project report, CP, experts Document review, Questionnaires,Interview
Assignment of personnel is adequate. Record and plan of assignment of personnel of theAfghan side for the Project
Project report, CP, experts Document review, Questionnaires,Interview
Collaboration withother organizations
Collaboration with other relatedAfghan organizations and otherassistance agencies are beingeffectively implemented.
Record of meeting and discussion with other relatedorganizations
Project report, CP, experts Document review, Questionnaires,Interview
ImplementationProcess
Ownership ofimplementingorganizations inAfghanistan
Relationship betweenexperts andcounterparts
Monitoring
Achievement of overallgoal (Expected)
The coverage of quality maternal andnewborn health services is expanded.

April, 2009
Evaluation item Criteria of evaluation Necessary data and information Data source Means of analysis
1.Relevance 1.1 Relevance of the overall goal andproject purpose to the Afghandevelopment policy
Comparison with governmentdevelopment policy
Afghan development policies onreproductive health
Afghan development policies onreproductive health, CP, experts
Document review, Questionnaires,Interview
1.2 Relevance of the overall goal andproject purpose to the target group
Comparison with the needs oftarget group
Importance of reproductive health in overalldevelopment policies in Afghanistan
Afghan development policies onreproductive health, CP, experts
Document review, Questionnaires,Interview
1.3 Relevance of the overall goal andproject purpose to the Japanese ODApolicy
Comparison with Japanese ODApolicy
Japanese ODA policy to Afghanistan Policy papers of Japanese Ministry ofForeign Affairs and JICA
Document review
1.4 Relevance of approach to achieveProject Purpose
Opinions of related actors Project report, CP, experts Document review, Questionnaires,Interview
2. Effectiveness 2.1 Achievement of project purpose Number of outputs indicators RHD documents RHD documents, Project report, CP, expeDocument review, Questionnaires,Interview
2.2 Contribution of each output to theachievement of Project Purpose
Relation of each Output and ProjectPurpose
Project report, CP, experts Document review, Questionnaires,Interview
2.3 Influence of Important Assumptions Inhibiting factors of outputs to achieve theproject purpose and outputs
Project report, CP, experts Document review, Questionnaires,Interview
3. Efficiency Experts (number, field of expertise, timing ofdispatch)
Project report, CP, experts Document review, Questionnaires,Interview
Supply of facilities and equipment (quantity,specifications, timing of provision)
Project report, CP, experts Document review, Questionnaires,Interview
CP training in Japan (numbers, field oftraining, timing )
Project report, CP, experts Document review, Questionnaires,Interview
Training in third countries (Cambodia,Indonesia, Pakistan)
Project report, CP, experts Document review, Questionnaires,Interview
Local cost support Project report, CP, experts Document review, Questionnaires,Interview
Assignment of CPs ( number, field, timing) Project report, CP, experts Document review, Questionnaires,Interview
Project management cost Project report, CP, experts Document review, Questionnaires,Interview
Supply of facilities (land, facilities, andequipment for project activities)
Project report, CP, experts Document review, Questionnaires,Interview
Human resources (experts, CPs) Project report, CP, experts Document review, Questionnaires,Interview
Facilities, Equipment, Machines Project report, CP, experts Document review, Questionnaires,Interview
Budget allocation Project report, CP, experts Document review, Questionnaires,Interview
3.4 Project management system Working process and function of JointCoordination Committee
Project report, CP, experts Document review, Questionnaires,Interview
4. Impact Is the Project expectedto have an impact onachieving overall goal?
4.1 Impact on quality maternal andnewborn health services in Afghanistan
Status and progress of maternaland newborn health services
Achievement level of Overall Goal and theprocess of achievement in relation withProject component
Project report, CP, experts Document review, Questionnaires,Interview
4.2 Unintended positive impact Positive cases experienced during Projectincluding focal persons, community people,and related organizations
Project report, CP, experts Document review, Questionnaires,Interview
4.3 Unintended negative impact Negative cases experienced during Project,including focal persons, community people,and related organizations
Project report, CP, experts Document review, Questionnaires,Interview
Has the Project beenaffected by ImportantAssumptions?
4.4 Influence of Important Assumption Items influenced by the importantassumption
Project report, CP, experts Document review, Questionnaires,Interview
Are the overall goal andproject purpose still inline with the policydirections of both thedonor and recipientcountries and the needsof the target group?
How have inputs beenutilized and managed?
3.1 Appropriateness of Japanese input
3.2 Appropriateness of Afghan input
3.3 Utilization of inputs
Evaluation Grid: Reproductive Health Project in Afghanistan
Scale, timing and cost of Afghaninputs and the benefits of them
Scale, timing and cost ofJapanese inputs and the benefitsof them
Has the Project producedexpected outputs? Hasthe Project beeneffective?
Items of investigation
Has the Project hadunintended impact?
To what extent haveinput been appropriate interms of scale, timing,cost, and benefit?

Evaluation item Criteria of evaluation Necessary data and information Data source Means of analysisItems of investigation
5.1 Institutional (policies) aspect Relation of government policywith Project
Afghan government policy on reproductivehealth
Policy paper on reproductive health, CP,experts
Document review, Questionnaires,Interview
Organization system of MoPHand related health servicei tit ti
Organization policy paper of MoPH,KPHD and related health institutions,CP t
Document review, Questionnaires,Interview
5.2 Financial aspect Financial status of MoPH andrelated health servicel institution
Financial status of MoPH Documents on policy and budget ofMoPH and related organizations
Document review, Questionnaires,Interview
Capacity of trained personnel Capacity of trained personel Project report, CP, experts, donors Document review, Questionnaires,Interview
Capacity of MoPH and relatedhealth service institutions
Institutional capacity to sustain activitiessuch as training and supervision
Project report, CP, experts, donors Document review, Questionnaires,Interview
What are the contributingand inhibiting factors forsustainability?
5.4 Contributing and inhibiting factors Analysis of promoting and inhibiting factors Project report, CP, experts, donors Document review, Questionnaires,Interview
5.3 Technical aspect
5. Sustainability Is the benefit of theProject expected to besustained after JICA'sassistance is terminated?
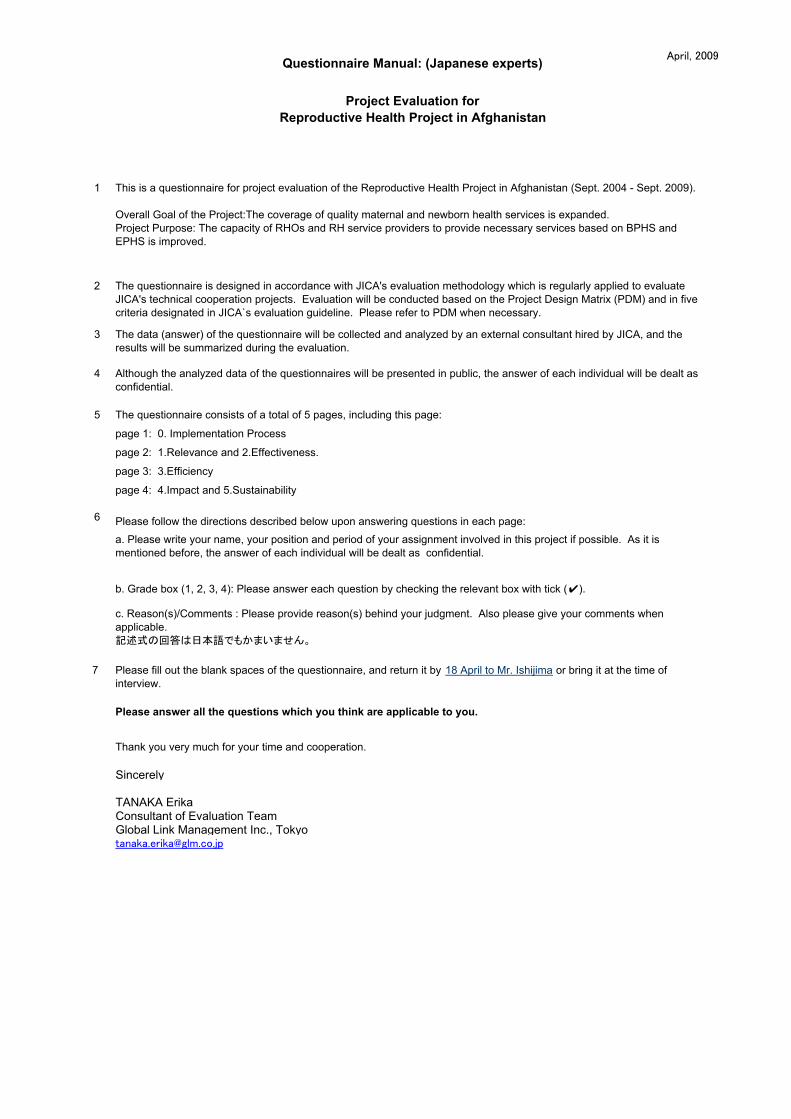
April, 2009Questionnaire Manual: (Japanese experts)
Project Evaluation forReproductive Health Project in Afghanistan
1 This is a questionnaire for project evaluation of the Reproductive Health Project in Afghanistan (Sept. 2004 - Sept. 2009).
Overall Goal of the Project:The coverage of quality maternal and newborn health services is expanded.Project Purpose: The capacity of RHOs and RH service providers to provide necessary services based on BPHS andEPHS is improved.
2 The questionnaire is designed in accordance with JICA's evaluation methodology which is regularly applied to evaluateJICA's technical cooperation projects. Evaluation will be conducted based on the Project Design Matrix (PDM) and in fivecriteria designated in JICA`s evaluation guideline. Please refer to PDM when necessary.
3 The data (answer) of the questionnaire will be collected and analyzed by an external consultant hired by JICA, and theresults will be summarized during the evaluation.
4 Although the analyzed data of the questionnaires will be presented in public, the answer of each individual will be dealt asconfidential.
5 The questionnaire consists of a total of 5 pages, including this page:
page 1: 0. Implementation Process
page 2: 1.Relevance and 2.Effectiveness.
page 3: 3.Efficiency
page 4: 4.Impact and 5.Sustainability
6 Please follow the directions described below upon answering questions in each page:a. Please write your name, your position and period of your assignment involved in this project if possible. As it ismentioned before, the answer of each individual will be dealt as confidential.
b. Grade box (1, 2, 3, 4): Please answer each question by checking the relevant box with tick (✔).
c. Reason(s)/Comments : Please provide reason(s) behind your judgment. Also please give your comments whenapplicable.記述式の回答は日本語でもかまいません。
7 Please fill out the blank spaces of the questionnaire, and return it by 18 April to Mr. Ishijima or bring it at the time ofinterview.
Please answer all the questions which you think are applicable to you.
Thank you very much for your time and cooperation.
Sincerely
TANAKA ErikaConsultant of Evaluation TeamGlobal Link Management Inc., [email protected]

EVALUATION QUESTIONNAIRE for Experts Your Name: 1/4Project Title : Reproductive Health Project in Afghanistan Your Position / Speciality:
Period of your assignment :
0. Implementation Process
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S)/COMMENTS0.1.1 Was the implementation of each activity conducted smoothly as planned during the Projectperiod? Not at all Rarely More or less Very much
0.1.2 If it was not, what were the problems?
0.1.3 How did you cope with the problems?
0.2.1 Has the implementation system of the Project been appropriate? Not at all Rarely More or less Very much
0.2.2 Has the monitoring system of the overall Project been appropriate? Not at all Rarely More or less Very much
0.2.3 Was the PDM modified appropriately when necessary? Not at all Rarely More or less Very much
0.2.4 To what extent has the Project been able to cope with unplanned or unexpected importantassumptions*? Not at all Rarely More or less Very much
0.3.1. Do you think that you have had a good communication with Afghan CPs? Not at all Rarely More or less Very much
0.3.2. If you have not had a good communication with Afghan CPs, what are the problems?
0.3.3 If you have taken any measures to improve communication among Project, please describe.
0.3.4 Do you think that technical assitance by Japanese experts has been provided in anappropriate manner? If not, please describe your problems. Not at all Rarely More or less Very much
0.4 Ownership of Afghanside
0.4.1. Do you think that the counterparts (CPs) on the Afghan side have taken an initiative toproceed the Project? Not at all Rarely More or less Very much
0.4.2 Do you think that the CP organizations (MoPH, KPHD, Malalai Hospital, DHs, CHCs, etc. )have taken an initiative to proceed the Project? Not at all Rarely More or less Very much
0.4.3 Do you think that CP agencies and organizations on the Afghan side have allocatednecessary budget for Project implementation? Not at all Rarely More or less Very much
0.4.4 Do you think that the Afghan side has assigned counterparts appropriately in terms of numberand expertise? Not at all Rarely More or less Very much
0.4.5What are the problems for Afghan CPs and related agencies to be actively involved in theProject, if any? Not at all Rarely More or less Very much
0.5 Collaboration withother organizations
0.5.1 Has communication among related organizations such as MoPH, KPHD, Malalai Hospital,DHs, CHCs, etc. been appropriate? Not at all Rarely More or less Very much
0.5.2 Has communication with other assistance agencies such as WHO, USAID, etc. beenappropriate? Not at all Rarely More or less Very much
* Important Assumptions mean conditions important for project success, but that cannot be controlled by the project. Please seethe column of Important Assumption in PDM.
0.3 Relationship betweenAfghan CPs and JapaneseExperts
0.1 Implementationprocess.
0.2 Monitoring of projectimplementation

EVALUATION QUESTIONNAIRE for Experts Your Name: 2/4Project Title : Reproductive Health Project in Afghanistan Your Position / Speciality:
Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S) / Comments
1.1.1 Is the overall goal still in line with the Afghan development policy in reproductive health? Not at all Rarely More or less Very much
1.1.2 Is the project purpose still in line with the Afghan development policy in reproductive health? Not at all Rarely More or less Very much
1.2 Relevance of the overall goal andproject purpose to the target group 1.2.1 Does the overall goal match the needs of the target group (RHOs at RHD and PHD and RH service provides)? Not at all Rarely More or less Very much
1.2.2 Does the project purpose match the needs of the target group? Not at all Rarely More or less Very much
1.3 Relevance of the overall goal andproject purpose to Japanese ODA policy 1.3.1 Are the overall goal and project purpose still in line with Japanese current ODA policy ? Not at all Rarely More or less Very much
1.4 Relevance of Project approach toachieve Project Purpose 1.4.1 Is the approach adopted by the Project to achieve Project Purpose appropriate? Not at all Rarely More or less Very much
1.4.2 Does the approach adopted by the Project incorporate Japanese technical advantage and related experiences? Not at all Rarely More or less Very much
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S)/ COMMENTS
2.1.1 To what extent do you think that the Project Purpose is likely to be achieved? Not at all Rarely More or less Very much
2.1.2. What do you think are the promoting factors to achieve the project purpose?
2.1.3 What do you think are the inhibiting factors to achieve the project purpose?
2.2.1 OUTPUT 1 - National Reproductive Health Program is established and functioning.
2.2.1.1 How much do you think has OUTPUT1 been achieved? Not at all A little More or less Very much
2.2.1.2 What are the challenges to achieve the OUTPUT 1?
2.2.1.3 How much do you think has OUTPUT 1 contributed to achieve the project purpose? Not at all Rarely More or less Very much
2.2.2 OUTPUT 2 - In-service training mechanisms is established and maintained in an appropriate manner.
2.2.2.1 How much do you think has OUTPUT 2 been achieved? Not at all A little More or less Very much
2.2.2.2 What are the challenges to achieve the OUTPUT 2?
2.2.2.3 How much do you think has OUTPUT 2 contributed to achieve the project purpose? Not at all Rarely More or less Very much
2.2.3 OUTPUT 3 - RH System is functioning in Urban Kabul.
2.2.3.1 How much do you think hasOUTPUT 3 been achieved? Not at all A little More or less Very much
2.2.3.2 What are the challenges to achieve the OUTPUT 3?
2.2.3.3 How much do you think has OUTPUT 3 contributed to achieve the project purpose? Not at all Rarely More or less Very much
2.2.4 Other output
2.2.4 If there are outputs other than above that have contributed to achieve the project purpose, please describe.
2.3 Logic of PDM 2.3.1 Do you think that activities, outputs, and project purpose described in PDM are logically and appropriately linked? Not at all A little More or less Very much
2.4.1 Do you think that there is any influence of important assumptions in achieving project purpose and outputs? Very much More or less A little No
2.4.2 If yes, please describe briefly.
1. RELEVANCE
2. EFFECTIVENESS
1.1 Relevance of the overall goal andproject purpose to theAfghandevelopment policy
2.1 Achievement of expected outcome
2.2 Achievements and contribution ofEACH OUTPUT
2.4 Influence of important assumptions

EVALUATION QUESTIONNAIRE for Experts Your Name: 3/4
Your Position / Speciality:Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S) / COMMENTS
Not at all Rarely More or less Very much
a. The number of experts
b. Timeliness of dispatching experts
c. Fields of expertise
a. Quantity
b. Quality
c. Timeliness of provision
d. Cost
a. Timing of activities
b. Quality of activities (materials, training)
a. Timing of activities
b. Quality of activities (materials, training)
a. Timeliness
b. Amount of support
a. The number of CPs
b. Timeliness of assignment
c. Professional fields of CPs
a. Facilities (Project office, training sites, etc.)
b. Equipment and supplies
a. Amount
b. Timeliness of disbursement
a. Personnel
b. Facilities/equipment/supplies
c. Operational Costs
a. Timing
d. Effectiveness of management3.4 Have the inputsbeen utilizedefficiently toproduce Outputs?
3.4.1 Do you think that the inputswere efficient to produce Outputs?
Not at all Rarely More or less Very much
Project Title : Reproductive Health Project in Afghanistan
3. EFFICIENCY:
3.1 Have theJapanese inputsbeen appropriate?
3.2 Have theAfghan inputs beenappropriate?
---> > These grades are applied for all questions of this sheet.
3.1.1 Japanese Experts
3.1.2 Provision of equipment andfacilities (including Dasht-e BarchiTraining Center)
3.1.3 Training in Japan
3.1.4 Training in third countries(Cambodia, Indonesia, Pakistan)
3.3 Have the inputsbeen effectivelyutilized?
3.2.3 Operational Costs
3.1.5 Local cost support
3.2.1 Assignment of Afghan CPs
3.2.2 Provision of Facilities /Equipment
3.3.2 Has the Joint CoordinationCommittee functioned well?
3.3.1 Utilization of inputs

EVALUATION QUESTIONNAIRE for Experts Your Name: 4/4
Your Position / Speciality:Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASONS (S) / COMMENTS
4.1 Impact on overall goal4.1.1 Do you think that the Project is likely to have animpact on quality maternal and newborn healthservices?
Not at all Rarely More or less Very much
4.2.1 Is there any intended positive situation producedby the Project? Please describe briefly.
4.2.2 Is there any unintended positive situationproduced by the Project? Please describe briefly.
4.3 Negative Impact 4.3.1 Is there any unintended negative situationproduced by the Project? Please describe briefly.
4.4 Influence of externalcondition
4.4.1 Is there any change of activities influenced by theimportant assumption (external conditions)? Pleasedescribe briefly.
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S) / COMMENTS5.1.1 Is the Afghan government likely to continue its policyin terms of reproductive health? Not at all Rarely More or less Very much
5.1.2 Are MoPH and related institutes sich as hospitals andhealth centers likely to be able to be independentlymanaged by itself?
Not at all Rarely More or less Very much
5.1.3 Are MoPH and related institutes likely to work in acollaborative manner? Not at all Rarely More or less Very much
5.2.1 Is the Afghan government likely to allocate sufficientoperational budget to MoPH and related institutes after theProject period to sustain activities introduced by theProject?
Not at all Rarely More or less Very much
5.2.2 Is the Afghan government likely to allocate sufficientbudget to MoPH and related institutes after the Projectperiod to sustain activities introduced by the Project ?
Not at all Rarely More or less Very much
5.3.1 Are the transferred knowledge and technique likely tobe properly maintained and utilized by reprodutive healthservice providers?
Not at all Rarely More or less Very much
5.3.2 Are the facilities, equipment, and training materialsare likely to be well maintained by the Afghan side? Not at all Rarely More or less Very much
5.3.3 Are MoPH and related health institutions likely tocontinue supervision and training on reproductive health ontheir own after the Project period?
Not at all Rarely More or less Very much
5.4.1 What will be the promoting factors to sustain theproject impact after the termination of the Project?
5.4.2 What will be the inhibiting factors of the projectimpact after the termination of the Project?
Project Title : Reproductive Health Project in Afghanistan
5.4 Important factors forsustainability
5.3 Technical Sustainability
5.SUSTAINABILITY:
5.2 Financial Sustainability
5.1 InstitutionalSustainability
4. IMPACT:
4.2 Positive Impact

April, 2009Questionnaire Manual: (Afghan CPs)
Project Evaluation forReproductive Health Project in Afghanistan
1 This is a questionnaire for project evaluation of the Reproductive Health Project in Afghanistan (Sept. 2004 - Sept. 2009).
Overall Goal of the Project:The coverage of quality maternal and newborn health services is expanded.Project Purpose: The capacity of RHOs and RH service providers to provide necessary services based on BPHS and EPHSis improved.
2 The questionnaire is designed in accordance with JICA's evaluation methodology which is regularly applied to evaluate JICA'stechnical cooperation projects. Evaluation will be conducted based on the Project Design Matrix (PDM) and in five criteriadesignated in JICA`s evaluation guideline. Please refer to PDM when necessary.
3 The data (answer) of the questionnaire will be collected and analyzed by an external consultant hired by JICA, and the resultswill be summarized during the evaluation.
4 Although the analyzed data of the questionnaires will be presented in public, the answer of each individual will be dealt asconfidential.
5 The questionnaire consists of a total of 5 pages, including this page:
page 1: 0. Implementation Process
page 2: 1.Relevance and 2.Effectiveness.
page 3: 3.Efficiency
page 4: 4.Impact and 5.Sustainability
6 Please follow the directions described below upon answering questions in each page:
a. Please write your name, your position and period of your assignment involved in this project if possible. As it is mentionedbefore, the answer of each individual will be dealt as confidential.
b. Grade box (1, 2, 3, 4): Please answer each question by checking the relevant box with tick ( ✔).
c. Reason(s)/Comments : Please provide reason(s) behind your judgment. Also please give your comments when applicable.
7 Please fill out the blank spaces of the questionnaire, and return it by 18 April to Mr. Ishijima or bring it at the time of interview.
Please answer all the questions which you think are applicable to you.
Thank you very much for your time and cooperation.
Sincerely
TANAKA ErikaConsultant of Evaluation TeamGlobal Link Management Inc., [email protected]

EVALUATION QUESTIONNAIRE for CPs Your Name: 1/4Project Title : Reproductive Health Project in Afghanistan Your Position / Speciality:
Period of your assignment :
0. Implementation Process
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S)/COMMENTS0.1.1 Was the implementation of each activity conducted smoothly as planned during the Projectperiod? Not at all Rarely More or less Very much
0.1.2 If it was not, what were the problems?
0.1.3 How did you cope with the problems?
0.2.1 Has the implementation system of the Project been appropriate? Not at all Rarely More or less Very much
0.2.2 Has the monitoring system of the overall Project been appropriate? Not at all Rarely More or less Very much
0.2.3 Was the PDM modified appropriately when necessary? Not at all Rarely More or less Very much
0.2.4 To what extent has the Project been able to cope with unplanned or unexpected importantassumptions*? Not at all Rarely More or less Very much
0.3.1. Do you think that you have had a good communication with Japanese experts? Not at all Rarely More or less Very much
0.3.2. If you have not had a good communication with Japanese experts, what are the problems?
0.3.3 If you have taken any measures to improve communication among Project, please describe.
0.3.4 Do you think that technical assitance by Japanese experts has been provided in anappropriate manner? If not, please describe your problems. Not at all Rarely More or less Very much
0.4 Ownership of Afghanside
0.4.1. Do you think that the counterparts (CPs) on the Afghan side have taken an initiative toproceed the Project? Not at all Rarely More or less Very much
0.4.2 Do you think that the CP organizations (MoPH, KPHD, Malalai Hospital, DHs, CHCs, etc. )have taken an initiative to proceed the Project? Not at all Rarely More or less Very much
0.4.3 Do you think that CP agencies and organizations on the Afghan side have allocatednecessary budget for Project implementation? Not at all Rarely More or less Very much
0.4.4 Do you think that the Afghan side has assigned counterparts appropriately in terms of numberand expertise? Not at all Rarely More or less Very much
0.4.5What are the problems for Afghan CPs and related agencies to be actively involved in theProject, if any? Not at all Rarely More or less Very much
0.5 Collaboration withother organizations
0.5.1 Has communication among related organizations such as MoPH, KPHD, Malalai Hospital,DHs, CHCs, etc. been appropriate? Not at all Rarely More or less Very much
0.5.2 Has communication with other assistance agencies such as WHO, USAID, etc. beenappropriate? Not at all Rarely More or less Very much
* Important Assumptions mean conditions important for project success, but that cannot be controlled by the project. Please seethe column of Important Assumption in PDM.
0.3 Relationship betweenAfghan CPs and JapaneseExperts
0.1 Implementationprocess.
0.2 Monitoring of projectimplementation

EVALUATION QUESTIONNAIRE for CPs Your Name: 2/4Project Title : Reproductive Health Project in Afghanistan Your Position / Speciality:
Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S) / Comments
1.1.1 Is the overall goal still in line with the Afghan development policy in reproductive health? Not at all Rarely More or less Very much
1.1.2 Is the project purpose still in line with the Afghan development policy in reproductive health? Not at all Rarely More or less Very much
1.2 Relevance of the overall goal andproject purpose to the target group 1.2.1 Does the overall goal match the needs of the target group (RHOs at RHD and PHD and RH service provides)? Not at all Rarely More or less Very much
1.2.2 Does the project purpose match the needs of the target group? Not at all Rarely More or less Very much
1.3 Relevance of Project approach toachieve Project Purpose 1.3.1 Is the approach adopted by the Project to achieve Project Purpose appropriate? Not at all Rarely More or less Very much
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S)/ COMMENTS
2.1.1 To what extent do you think that the Project Purpose is likely to be achieved? Not at all Rarely More or less Very much
2.1.2. What do you think are the promoting factors to achieve the project purpose?
2.1.3 What do you think are the inhibiting factors to achieve the project purpose?
2.2.1 OUTPUT 1 - National Reproductive Health Program is established and functioning.
2.2.1.1 How much do you think has OUTPUT1 been achieved? Not at all A little More or less Very much
2.2.1.2 What are the challenges to achieve the OUTPUT 1?
2.2.1.3 How much do you think has OUTPUT 1 contributed to achieve the project purpose? Not at all Rarely More or less Very much
2.2.2 OUTPUT 2 - In-service training mechanisms is established and maintained in an appropriate manner.
2.2.2.1 How much do you think has OUTPUT 2 been achieved? Not at all A little More or less Very much
2.2.2.2 What are the challenges to achieve the OUTPUT 2?
2.2.2.3 How much do you think has OUTPUT 2 contributed to achieve the project purpose? Not at all Rarely More or less Very much
2.2.3 OUTPUT 3 - RH System is functioning in Urban Kabul.
2.2.3.1 How much do you think hasOUTPUT 3 been achieved? Not at all A little More or less Very much
2.2.3.2 What are the challenges to achieve the OUTPUT 3?
2.2.3.3 How much do you think has OUTPUT 3 contributed to achieve the project purpose? Not at all Rarely More or less Very much
2.2.4 Other output
2.2.4 If there are outputs other than above that have contributed to achieve the project purpose, please describe.
2.3 Logic of PDM 2.3.1 Do you think that activities, outputs, and project purpose described in PDM are logically and appropriately linked? Not at all A little More or less Very much
2.4.1 Do you think that there is any influence of important assumptions in achieving project purpose and outputs? Very much More or less A little No
2.4.2 If yes, please describe briefly.2.4 Influence of important assumptions
2.2 Achievements and contribution ofEACH OUTPUT
1. RELEVANCE
2. EFFECTIVENESS
1.1 Relevance of the overall goal andproject purpose to theAfghandevelopment policy
2.1 Achievement of expected outcome

EVALUATION QUESTIONNAIRE for CPs Your Name: 3/4
Your Position / Speciality:Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S) / COMMENTS
Not at all Rarely More or less Very much
a. The number of experts
b. Timeliness of dispatching experts
c. Fields of expertise
a. Quantity
b. Quality
c. Timeliness of provision
d. Cost
a. Timing of activities
b. Quality of activities (materials, training)
a. Timing of activities
b. Quality of activities (materials, training)
a. Timeliness
b. Amount of support
a. The number of CPs
b. Timeliness of assignment
c. Professional fields of CPs
a. Facilities (Project office, training sites, etc.)
b. Equipment and supplies
a. Amount
b. Timeliness of disbursement
a. Personnel
b. Facilities/equipment/supplies
c. Operational Costs
a. Timing
d. Effectiveness of management3.4 Have the inputsbeen utilizedefficiently toproduce Outputs?
3.4.1 Do you think that the inputswere efficient to produce Outputs?
Not at all Rarely More or less Very much
3.3 Have the inputsbeen effectivelyutilized?
3.2.3 Operational Costs
3.1.5 Local cost support
3.2.1 Assignment of Afghan CPs
3.2.2 Provision of Facilities /Equipment
3.3.2 Has the Joint CoordinationCommittee functioned well?
3.3.1 Utilization of inputs
Project Title : Reproductive Health Project in Afghanistan
3. EFFICIENCY:
3.1 Have theJapanese inputsbeen appropriate?
3.2 Have theAfghan inputs beenappropriate?
---> > These grades are applied for all questions of this sheet.
3.1.1 Japanese Experts
3.1.2 Provision of equipment andfacilities (including Dasht-e BarchiTraining Center)
3.1.3 Training in Japan
3.1.4 Training in third countries(Cambodia, Indonesia, Pakistan)

EVALUATION QUESTIONNAIRE for CPs Your Name: 4/4
Your Position / Speciality:Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASONS (S) / COMMENTS
4.1 Impact on overall goal4.1.1 Do you think that the Project is likely to have animpact on quality maternal and newborn healthservices?
Not at all Rarely More or less Very much
4.2.1 Is there any intended positive situation producedby the Project? Please describe briefly.
4.2.2 Is there any unintended positive situationproduced by the Project? Please describe briefly.
4.3 Negative Impact 4.3.1 Is there any unintended negative situationproduced by the Project? Please describe briefly.
4.4 Influence of externalcondition
4.4.1 Is there any change of activities influenced bythe important assumption (external conditions)?Please describe briefly.
QUESTIONS SUB-QUESTIONS 1 2 3 4 REASON(S) / COMMENTS5.1.1 Is the Afghan government likely to continue its policyin terms of reproductive health? Not at all Rarely More or less Very much
5.1.2 Are MoPH and related institutes sich as hospitals andhealth centers likely to be able to be independentlymanaged by itself?
Not at all Rarely More or less Very much
5.1.3 Are MoPH and related institutes likely to work in acollaborative manner? Not at all Rarely More or less Very much
5.2.1 Is the Afghan government likely to allocate sufficientoperational budget to MoPH and related institutes after theProject period to sustain activities introduced by theProject?
Not at all Rarely More or less Very much
5.2.2 Is the Afghan government likely to allocate sufficientbudget to MoPH and related institutes after the Projectperiod to sustain activities introduced by the Project ?
Not at all Rarely More or less Very much
5.3.1 Are the transferred knowledge and technique likely tobe properly maintained and utilized by reprodutive healthservice providers?
Not at all Rarely More or less Very much
5.3.2 Are the facilities, equipment, and training materialsare likely to be well maintained by the Afghan side? Not at all Rarely More or less Very much
5.3.3 Are MoPH and related health institutions likely tocontinue supervision and training on reproductive health ontheir own after the Project period?
Not at all Rarely More or less Very much
5.4.1 What will be the promoting factors to sustain theproject impact after the termination of the Project?
5.4.2 What will be the inhibiting factors of the projectimpact after the termination of the Project?
4.2 Positive Impact
Project Title : Reproductive Health Project in Afghanistan
5.4 Important factors forsustainability
5.3 Technical Sustainability
5.SUSTAINABILITY:
5.2 Financial Sustainability
5.1 InstitutionalSustainability
4. IMPACT:

April, 2009
アフガニスタン国リプロダクティブヘルスプロジェクト
質問票の集計結果を以下にまとめる。
質問票は、日本側は専門家、アフガニスタン側は、MoPH、KPHDのCP及びプロジェクトナショナルスタッフに配布した。
質問票の回答数は以下の通りである。
専門家 4名CP 5名ナショナルスタッフ 2名
専門家とCPに対する質問票のうち、選択式回答の結果を集計結果としてまとめた。有効回答数は11となる。質問項目によっては、担当外ということで、無回答、または「わからない」としている項目がある回答者があるが、回答があったもののみの平均値を集計した。記述式回答については割愛する。
集計表のフォーマットは、専門家用質問票をもとに作成した。専門家用質問票とCP用質問票はほぼ同様である。専門家とCPに対する質問が違っているところは、質問票の小項目の質問文のあとに、その旨記載している。また、特に記載していないが、専門家用とCP用では、同じ内容の質問であっても、表現を調整した箇所が一部ある。

EVALUATION QUESTIONNAIRE Your Name: 1/4Project Title : Reproductive Health Project in Afghanistan Your Position / Speciality:
Period of your assignment :
0. Implementation Process
QUESTIONS SUB-QUESTIONS 1 (1) 2 (2) 3 (3) 4 (4) Total Avg0.1.1 Was the implementation of each activity conducted smoothlyas planned during the Project period? Not at all Rarely 2 More or less 4 Very much 5 11 3.27
0.1.2 If it was not, what were the problems?
0.1.3 How did you cope with the problems?
0.2.1 Has the implementation system of the Project beenappropriate? Not at all Rarely More or less 5 Very much 6 11 3.55
0.2.2 Has the monitoring system of the overall Project beenappropriate? Not at all Rarely More or less 2 Very much 8 10 3.80
0.2.3 Was the PDM modified appropriately when necessary? Not at all Rarely More or less 3 Very much 5 8 3.63
0.2.4 To what extent has the Project been able to cope withunplanned or unexpected important assumptions*? Not at all 1 Rarely 1 More or less 1 Very much 5 8 3.25
0.3.1. Do you think that you have had a good communication withAfghan CPs? Not at all Rarely More or less 2 Very much 8 10 3.80
0.3.2. If you have not had a good communication with Afghan CPs,what are the problems?
0.3.3 If you have taken any measures to improve communicationamong Project, please describe.0.3.4 Do you think that technical assitance by Japanese experts hasbeen provided in an appropriate manner? If not, please describeyour problems.
Not at all Rarely More or less 2 Very much 9 11 3.82
0.4 Ownership of Afghanside
0.4.1. Do you think that the counterparts (CPs) on the Afghan sidehave taken an initiative to proceed the Project? Not at all 1 Rarely 3 More or less 5 Very much 2 11 2.73
0.4.2 Do you think that the CP organizations (MoPH, KPHD, MalalaiHospital, DHs, CHCs, etc. ) have taken an initiative to proceed theProject?
Not at all 2 Rarely 2 More or less 5 Very much 1 10 2.50
0.4.3 Do you think that CP agencies and organizations on the Afghanside have allocated necessary budget for Project implementation? Not at all 2 Rarely 6 More or less 3 Very much 11 2.09
0.4.4 Do you think that the Afghan side has assigned counterpartsappropriately in terms of number and expertise? Not at all Rarely 2 More or less 7 Very much 1 10 2.90
0.4.5What are the problems for Afghan CPs and related agencies tobe actively involved in the Project, if any? Not at all 3 Rarely 1 More or less 3 Very much 7 2.00
0.5 Collaboration withother organizations
0.5.1 Has communication among related organizations such asMoPH, KPHD, Malalai Hospital, DHs, CHCs, etc. been appropriate? Not at all Rarely More or less 3 Very much 7 10 3.70
0.5.2 Has communication with other assistance agencies such asWHO, USAID, etc. been appropriate? Not at all Rarely 1 More or less 5 Very much 4 10 3.30
* Important Assumptions mean conditions important for project success, but that cannot becontrolled by the project. Please see the column of Important Assumption in PDM.
0.3 Relationship betweenAfghan CPs and JapaneseExperts
0.1 Implementationprocess.
0.2 Monitoring of projectimplementation

EVALUATION QUESTIONNAIRE for Experts Your Name: 2/4Project Title : Reproductive Health Project in Afghanistan Your Position / Speciality:
Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 (1) 2 (2) 3 (3) 4 (4) Total AVG
1.1.1 Is the overall goal still in line with the Afghan development policy in reproductive health? Not at all Rarely More or less Very much 11 114.00
1.1.2 Is the project purpose still in line with the Afghan development policy in reproductive health? Not at all Rarely More or less Very much 11 114.00
1.2 Relevance of the overall goal andproject purpose to the target group 1.2.1 Does the overall goal match the needs of the target group (RHOs at RHD and PHD and RH service provides)? Not at all Rarely More or less Very much 11 11
4.00
1.2.2 Does the project purpose match the needs of the target group? Not at all Rarely More or less Very much 10 104.00
1.3 Relevance of the overall goal andproject purpose to Japanese ODA policy* 1.3.1 Are the overall goal and project purpose still in line with Japanese current ODA policyy* ? Not at all Rarely More or less 2 Very much 2 4
3.501.4 Relevance of Project approach toachieve Project Purpose 1.4.1 Is the approach adopted by the Project to achieve Project Purpose appropriate? Not at all Rarely More or less 3 Very much 8 11
3.73
1.4.2 Does the approach adopted by the Project incorporate Japanese technical advantage and related experiencesy*? Not at all Rarely More or less 2 Very much 2 43.50
*本質問項目はCP用質問票にはない。
QUESTIONS SUB-QUESTIONS 1 (1) 2 (2) 3 (3) 4 (4) Total AVG
2.1.1 To what extent do you think that the Project Purpose is likely to be achieved? Not at all Rarely 1 More or less 6 Very much 3 103.20
2.1.2. What do you think are the promoting factors to achieve the project purpose?
2.1.3 What do you think are the inhibiting factors to achieve the project purpose?
2.2.1 OUTPUT 1 - National Reproductive Health Program is established and functioning.
2.2.1.1 How much do you think has OUTPUT1 been achieved? Not at all A little More or less 3 Very much 7 103.70
2.2.1.2 What are the challenges to achieve the OUTPUT 1?
2.2.1.3 How much do you think has OUTPUT 1 contributed to achieve the project purpose? Not at all Rarely More or less 2 Very much 7 93.78
2.2.2 OUTPUT 2 - In-service training mechanisms is established and maintained in an appropriate manner.
2.2.2.1 How much do you think has OUTPUT 2 been achieved? Not at all A little More or less 4 Very much 6 103.60
2.2.2.2 What are the challenges to achieve the OUTPUT 2?
2.2.2.3 How much do you think has OUTPUT 2 contributed to achieve the project purpose? Not at all Rarely More or less 4 Very much 6 103.60
2.2.3 OUTPUT 3 - RH System is functioning in Urban Kabul.
2.2.3.1 How much do you think hasOUTPUT 3 been achieved? Not at all A little 2 More or less 6 Very much 1 92.89
2.2.3.2 What are the challenges to achieve the OUTPUT 3?
2.2.3.3 How much do you think has OUTPUT 3 contributed to achieve the project purpose? Not at all Rarely More or less 5 Very much 3 83.38
2.2.4 Other output
2.2.4 If there are outputs other than above that have contributed to achieve the project purpose, please describe.
2.3 Logic of PDM 2.3.1 Do you think that activities, outputs, and project purpose described in PDM are logically and appropriately linked? Not at all A little 2 More or less 1 Very much 6 93.44
2.4.1 Do you think that there is any influence of important assumptions in achieving project purpose and outputs? Very much 2 More or less 5 A little 1 No 1 92.11
2.4.2 If yes, please describe briefly.
2.2 Achievements and contribution ofEACH OUTPUT
1. RELEVANCE
2. EFFECTIVENESS
1.1 Relevance of the overall goal andproject purpose to theAfghandevelopment policy
2.1 Achievement of expected outcome
2.4 Influence of important assumptions

EVALUATION QUESTIONNAIRE for Experts Your Name: 3/4
Your Position / Speciality:Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 (1) 2 (2) 3 (3) 4 (4) Total AVG
Not at all Rarely More orless Very much
a. The number of experts 1 3 6 10 3.50
b. Timeliness of dispatching experts 1 5 4 10 3.30
c. Fields of expertise 1 3 6 10 3.50
a. Quantity 1 3 7 11 3.55
b. Quality 1 2 8 11 3.64
c. Timeliness of provision 1 3 7 11 3.55
d. Cost 1 2 7 10 3.60
a. Timing of activities 6 1 7 3.14
b. Quality of activities (materials, training) 3 4 7 3.57
a. Timing of activities 6 6 4.00
b. Quality of activities (materials, training) 1 5 6 3.83
a. Timeliness 2 3 5 3.60
b. Amount of support 3 3 6 3.50
a. The number of CPs 2 1 4 3 10 2.80
b. Timeliness of assignment 2 3 2 2 9 2.44
c. Professional fields of CPs 2 1 4 3 10 2.80
a. Facilities (Project office, training sites, etc.) 3 1 3 2 9 2.44
b. Equipment and supplies 3 1 3 2 9 2.44
a. Amount 2 3 3 8 2.88
b. Timeliness of disbursement 1 3 3 7 3.14
a. Personnel 3 6 9 3.67
b. Facilities/equipment/supplies 2 7 9 3.78
c. Operational Costs 2 7 9 3.78
a. Timing 3 4 7 3.57
d. Effectiveness of management 3 4 7 3.573.4 Have the inputsbeen utilizedefficiently toproduce Outputs?
3.4.1 Do you think that the inputswere efficient to produce Outputs?
Not at all Rarely More or less 1 Very much 5 6 3.83
Project Title : Reproductive Health Project in Afghanistan
3. EFFICIENCY:
3.1 Have theJapanese inputsbeen appropriate?
3.2 Have theAfghan inputs beenappropriate?
---> > These grades are applied for all questions of this sheet.
3.1.1 Japanese Experts
3.1.2 Provision of equipment andfacilities (including Dasht-e BarchiTraining Center)
3.1.3 Training in Japan
3.1.4 Training in third countries(Cambodia, Indonesia, Pakistan)
3.3 Have theinputs beeneffectively utilized?
3.2.3 Operational Costs
3.1.5 Local cost support
3.2.1 Assignment of Afghan CPs
3.2.2 Provision of Facilities /Equipment
3.3.2 Has the Joint CoordinationCommittee functioned well?
3.3.1 Utilization of inputs

EVALUATION QUESTIONNAIRE for Experts Your Name: 4/4
Your Position / Speciality:Period of your assignment :
QUESTIONS SUB-QUESTIONS 1 (1) 2 (2) 3 (3) 4 (4) Total AVG
4.1 Impact on overall goal4.1.1 Do you think that the Project is likely to have aimpact on quality maternal and newborn healthservices?
Not at all Rarely 1 More or less 3 Very much 7 11 3.55
4.2.1 Is there any intended positive situation producedby the Project? Please describe briefly.
4.2.2 Is there any unintended positive situationproduced by the Project? Please describe briefly.
4.3 Negative Impact 4.3.1 Is there any unintended negative situationproduced by the Project? Please describe briefly.
4.4 Influence of externalcondition
4.4.1 Is there any change of activities influenced bythe important assumption (external conditions)?Please describe briefly.
QUESTIONS SUB-QUESTIONS 1 (1) 2 (2) 3 (3) 4 (4) Total AVG5.1.1 Is the Afghan government likely to continue its policyin terms of reproductive health? Not at all 1 Rarely More or less 2 Very much 7 10 3.50
5.1.2 Are MoPH and related institutes sich as hospitals andhealth centers likely to be able to be independentlymanaged by itself?
Not at all 2 Rarely 2 More or less 5 Very much 1 10 2.50
5.1.3 Are MoPH and related institutes likely to work in acollaborative manner? Not at all 1 Rarely 1 More or less 5 Very much 4 11 3.09
5.2.1 Is the Afghan government likely to allocate sufficientoperational budget to MoPH and related institutes after theProject period to sustain activities introduced by theProject?
Not at all 1 Rarely 5 More or less 3 Very much 1 10 2.40
5.2.2 Is the Afghan government likely to allocate sufficientbudget to MoPH and related institutes after the Projectperiod to sustain activities introduced by the Project ?
Not at all 1 Rarely 6 More or less 2 Very much 1 10 2.30
5.3.1 Are the transferred knowledge and technique likely tobe properly maintained and utilized by reprodutive healthservice providers?
Not at all Rarely 1 More or less 7 Very much 2 10 3.10
5.3.2 Are the facilities, equipment, and training materialsare likely to be well maintained by the Afghan side? Not at all 1 Rarely 1 More or less 7 Very much 1 10 2.80
5.3.3 Are MoPH and related health institutions likely tocontinue supervision and training on reproductive health ontheir own after the Project period?
Not at all Rarely 2 More or less 8 10 2.80
5.4.1 What will be the promoting factors to sustain theproject impact after the termination of the Project?
5.4.2 What will be the inhibiting factors of the project impactafter the termination of the Project?
Project Title : Reproductive Health Project in Afghanistan
5.4 Important factors forsustainability
5.3 Technical Sustainability
5.SUSTAINABILITY:
5.2 Financial Sustainability
5.1 InstitutionalSustainability
4. IMPACT:
4.2 Positive Impact

-87-
5.ワークショップ結果
ここでは、終了時評価中に実施したワークショップの結果をまとめる。
ワークショップは 4月 21日の午前中に実施した。
ワークショップでは、参加者を3つのグループに分け、それぞれのグループに、PDMの 3つのアウトプットのひとつを割当て、実績につき検討した。検討内容は、指標の達成度、指標に表れていない実績、成果達成の貢献要因・阻害要因、残された課題、である。
以下にまとめるものは、各グループの最終的なプレゼンテーションで発表されたものである。オリジナルは模造紙にカードを貼ったものであったが、カードの内容をプロジェクトのナショナルスタッフがタイプしたものである。カードの中には文章として完結していないものもあったが、原則として、カードに書かれたことをそのまま掲載した。ただし、明らかなスペルミスなどは修正したものもある。全体の表の枠組みがグループによって若干違うが、これもそのままにした。
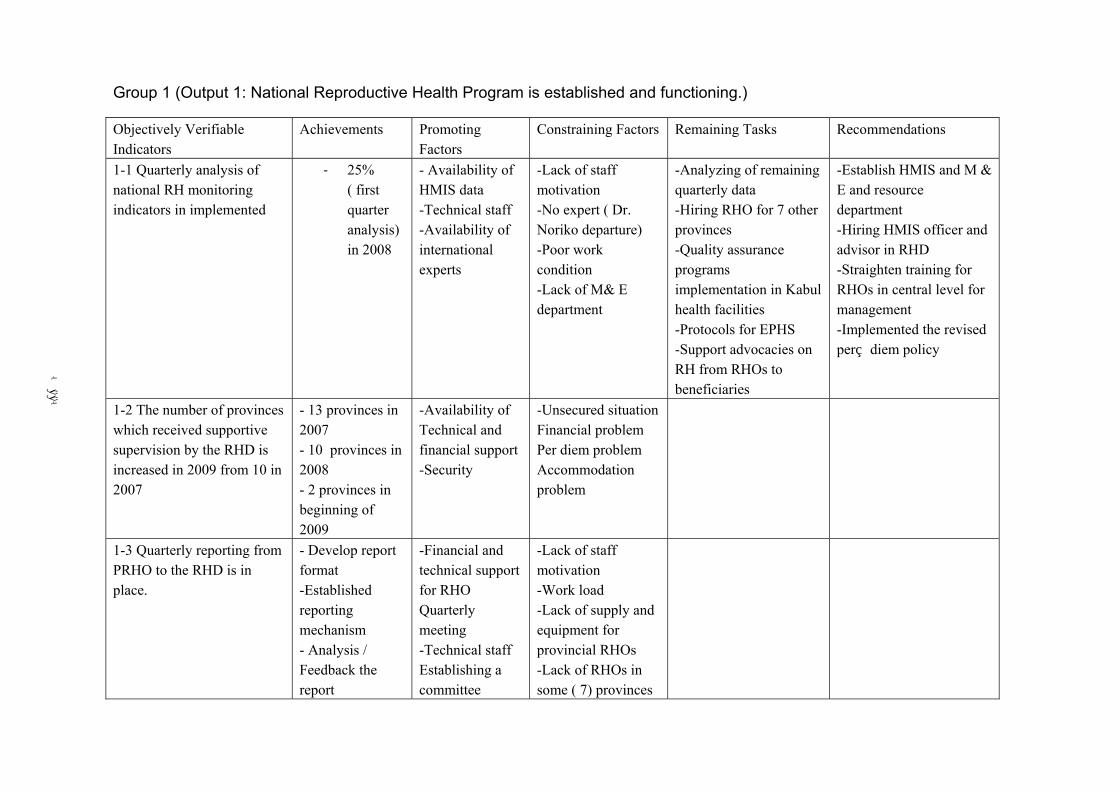
-88-
Group 1 (Output 1: National Reproductive Health Program is established and functioning.)
Objectively Verifiable Indicators
Achievements Promoting Factors
Constraining Factors Remaining Tasks Recommendations
1-1 Quarterly analysis of national RH monitoring indicators in implemented
- 25% ( first quarter analysis) in 2008
- Availability of HMIS data -Technical staff -Availability of international experts
-Lack of staff motivation -No expert ( Dr. Noriko departure) -Poor work condition -Lack of M& E department
-Analyzing of remaining quarterly data -Hiring RHO for 7 other provinces -Quality assurance programs implementation in Kabul health facilities -Protocols for EPHS -Support advocacies on RH from RHOs to beneficiaries
-Establish HMIS and M & E and resource department -Hiring HMIS officer and advisor in RHD -Straighten training for RHOs in central level for management -Implemented the revised per diem policy
1-2 The number of provinces which received supportive supervision by the RHD is increased in 2009 from 10 in 2007
- 13 provinces in 2007 - 10 provinces in 2008 - 2 provinces in beginning of 2009
-Availability of Technical and financial support -Security
-Unsecured situation Financial problem Per diem problem Accommodation problem
1-3 Quarterly reporting from PRHO to the RHD is in place.
- Develop report format -Established reporting mechanism - Analysis / Feedback the report
-Financial and technical support for RHO Quarterly meeting -Technical staff Establishing a committee
-Lack of staff motivation -Work load -Lack of supply and equipment for provincial RHOs -Lack of RHOs in some ( 7) provinces

-89-
Group 2 (Output 2: In service training mechanism is established and maintained in appropriate manner)
Objectively Verifiable Indicators
Achievement Promoting Factor Constraining Factor Remaining Task
2-1 National standards for organizing training is approved by MOPH
2-1 Training management system is established and functioning
2-1 establishment of training department as coordination body
2-1 in service training guideline finalized but not approved
2-1 training department job description is established
2-1 policy per diem approved
2-1 training department organ gram established
2-1 update training calendar
2-1 establish Dasht-e-Barchi training center
2-2 Continuum of care learning resource package is established and
2-2 COC LRP endorsement
2-2 COC LRP presented to CGHN
-Staff motivation
-Impact of Japanese expert character
-Urgent need for management of training program
-Bad security situation
-Time limitation
-work over load
-IT equipment problem
-limited number of qualified trainers
-some NGOs do not accept rule and regulation of Training center
-Lack of resource for repairing IT equipment in future
-clinical services of MMH is not improved
-maintenance system of MMH TD is not clear
-technical exchange program with other country was canceled
-in service guideline not approved
-COC LRP not approved
-supportive supervision manual is not approved
-trainer do not have idea about supportive supervision

-90-
approved by MOPH 2-2 COC LRP was revised
2-2 COC lectures were revised
2-2 COC has completed content including Health system
2-3 Training program with follow up and supervision are conducted by national training coordination body
2-3 Follow up and supervision system was established
2-3 supportive supervision was implemented
2-3 Internal supervision was established in MMH
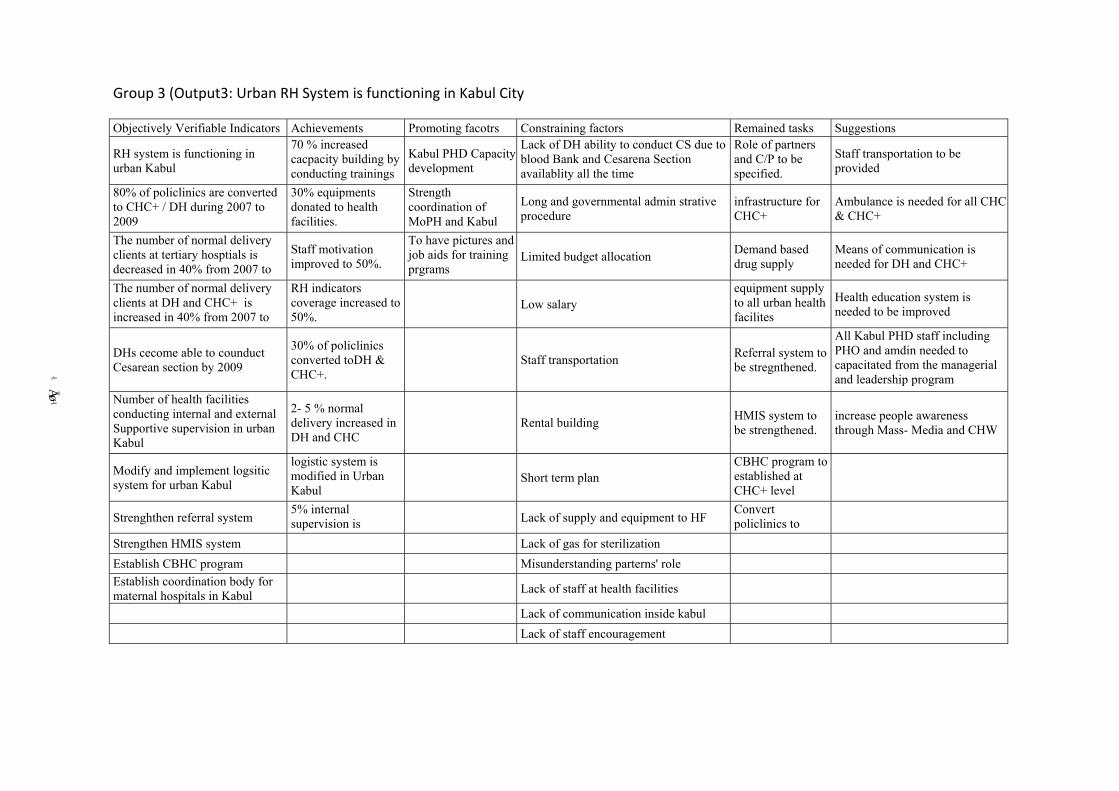
-91-
Group 3 (Output3: Urban RH System is functioning in Kabul City
Objectively Verifiable Indicators Achievements Promoting facotrs Constraining factors Remained tasks Suggestions
RH system is functioning in urban Kabul
70 % increased cacpacity building by conducting trainings
Kabul PHD Capacity development
Lack of DH ability to conduct CS due to blood Bank and Cesarena Section availablity all the time
Role of partners and C/P to be specified.
Staff transportation to be provided
80% of policlinics are converted to CHC+ / DH during 2007 to 2009
30% equipments donated to health facilities.
Strength coordination of MoPH and Kabul
Long and governmental admin strative procedure
infrastructure for CHC+
Ambulance is needed for all CHC & CHC+
The number of normal delivery clients at tertiary hosptials is decreased in 40% from 2007 to
Staff motivation improved to 50%.
To have pictures and job aids for training prgrams
Limited budget allocation Demand based drug supply
Means of communication is needed for DH and CHC+
The number of normal delivery clients at DH and CHC+ is increased in 40% from 2007 to
RH indicators coverage increased to 50%.
Low salary
equipment supply to all urban health facilites
Health education system is needed to be improved
DHs cecome able to counduct Cesarean section by 2009
30% of policlinics converted toDH & CHC+.
Staff transportation Referral system to
be stregnthened.
All Kabul PHD staff including PHO and amdin needed to capacitated from the managerial and leadership program
Number of health facilities conducting internal and external Supportive supervision in urban Kabul
2- 5 % normal delivery increased in DH and CHC
Rental building HMIS system to
be strengthened. increase people awareness through Mass- Media and CHW
Modify and implement logsitic system for urban Kabul
logistic system is modified in Urban Kabul
Short term plan
CBHC program to established at CHC+ level
Strenghthen referral system 5% internal supervision is
Lack of supply and equipment to HF Convert policlinics to
Strengthen HMIS system Lack of gas for sterilization Establish CBHC program Misunderstanding parterns' role Establish coordination body for maternal hospitals in Kabul
Lack of staff at health facilities
Lack of communication inside kabul Lack of staff encouragement







![Untitled-1 [] Ghumrnan Jrishti Ohonda Sudíksha Khana SolcniSiog JashanieepSingh Scrxhi bvraiSingh WedhaAWwal AgrzooShcrmo MiyatiGupta Mr.hDe.an HorsirnrunKuur Pratishthc Gourri Parmar](https://img.pdfslide.tips/doc/110x75/5b2028b27f8b9ac0628b4ac6/untitled-1-ghumrnan-jrishti-ohonda-sudiksha-khana-solcnisiog-jashanieepsingh.jpg)





![Dast o Gareban (Barelvi RazaKhaniyo Ki Khana Jangi) by Maulana Abu Ayub Qadri [DB]](https://img.pdfslide.tips/doc/110x75/55cf9cfb550346d033abc440/dast-o-gareban-barelvi-razakhaniyo-ki-khana-jangi-by-maulana-abu-ayub-qadri.jpg)