Embed Size (px)
DESCRIPTION
FRAKTUR
Citation preview
FRAKTUR UMUM
DR. WAHYU EKO W, SPOTORTHOPAEDI DAN TULANG BELAKANG
RS BINA HUSADA
1
Laporan operasi•Pasien posisi supine dalam spinal anastesi•Prosedur steril dan driping•Debridement pada sendi•Amputasi cruris dekstra dengan arteri vena besar diligasi + potong tajam saraf •Cuci luka dan kontrol perdarahan •Jahit dengan satu buah dripingOperasi selesai.

SMF Bedah FK UKI2
FRAKTUR
SMF Bedah FK UKI
3
Putusnya hubungan kesinambungan/ diskontinuitas tulang dan atau tulang rawan
Fraktur tertutup :Bila kulit sekitar intakFraktur terbuka :Bila ada luka,
sehingga kemungkinan terjadi kontaminasi atau infeksi

KLASIFIKASI
SMF Bedah FK UKI
4
I. Berdasarkan hub dengan dunia luar :
1.Fraktur tertutup
2. Fraktur terbuka
KLASIFIKASI
SMF Bedah FK UKI
5
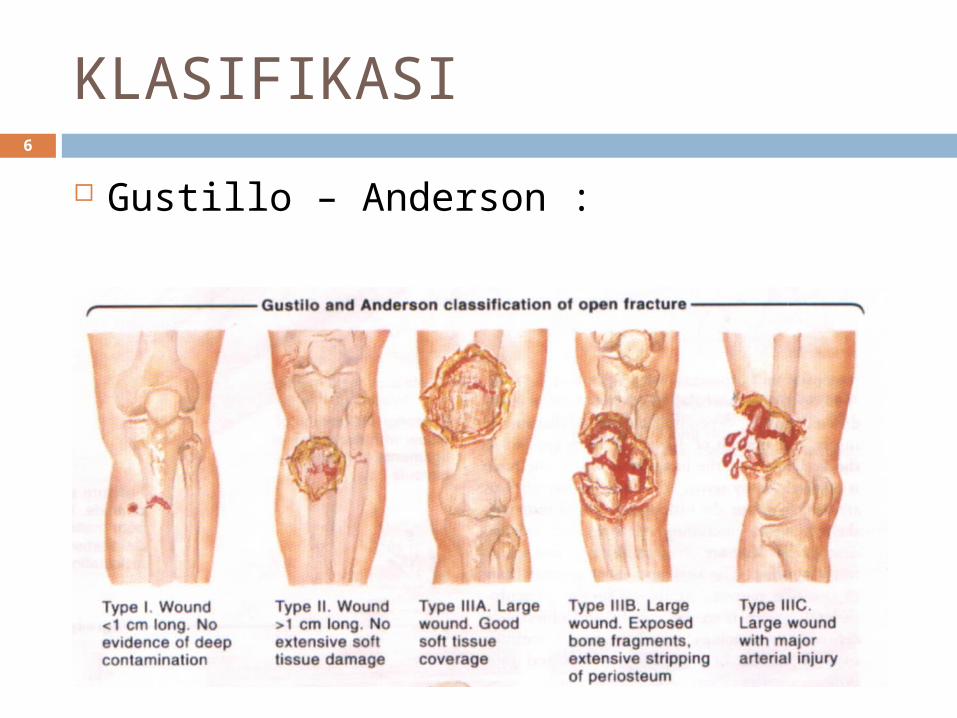
Gustillo – Anderson :I. Luka < 1 cmII. Luka 1 – 10 cmIII. Luka > 10 cm
A. Soft tissue coverageB. Bone exposedC. Neurovascular injury
KLASIFIKASI
SMF Bedah FK UKI
6
Gustillo – Anderson :
Fractures due to a traumatic incident
SMF Bedah FK UKI
7
Caused by sudden and exessive force, which may be tapping, crushing, bending, twisting or pulling.
Direct violence : blow on the arm which shatters the ulna at the point of impact
Indirect violence: forcible traction by a tendon or ligament which literally pulls the bone apart
Fatigue or stress fractures
SMF Bedah FK UKI
8
Due to repetitive stress Most often seen in the tibia or fibula
or metatarsals, especially in atheletes, dancers and army recruits.
Pathological fractures
SMF Bedah FK UKI
9
Fractures may occur even with normal stresses if the bone has been weakened (by a tumor) or if it is excessivelly brittle (paget’s disease)
How fractures are disposed
SMF Bedah FK UKI
10
Complete fracturesThe bone is compeletely broken into 2
or more fragments. Transverseoblique or spiral, Impacted fractureComminuted fracture
SMF Bedah FK UKI11
•Incomplete fracture
The bone is incompeletely divided and the periosteum remains in continuity.
•Greenstick fracture
•Compression fracture

KLASIFIKASI
II. Berdasarkan garis patah
SMF Bedah FK UKI
12
1.Komplet
2.Inkomplet
KLASIFIKASI
SMF Bedah FK UKI
13
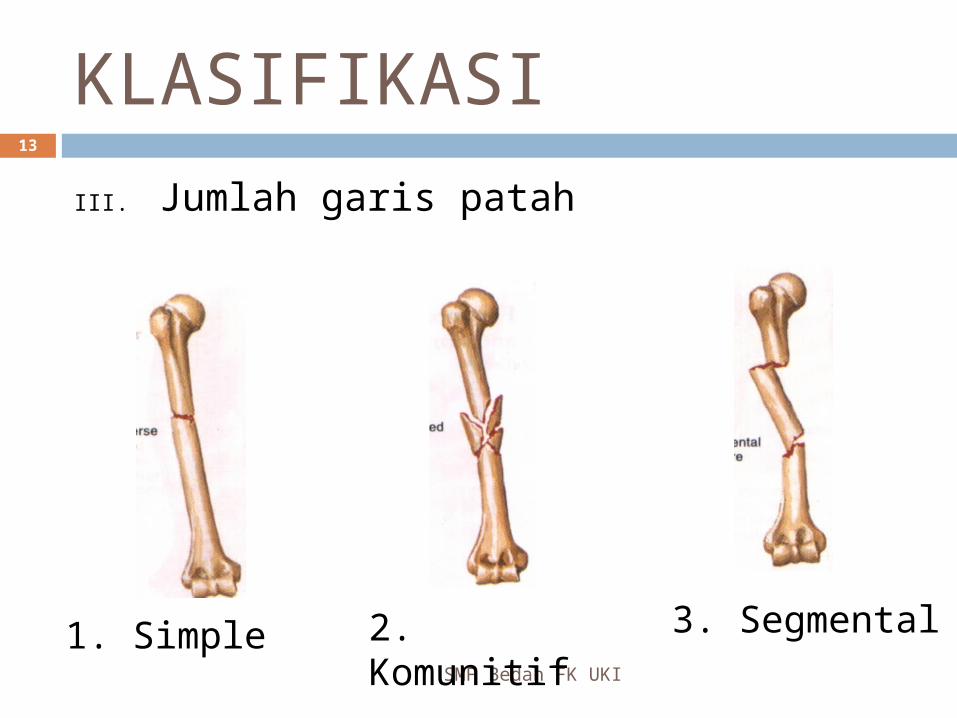
III. Jumlah garis patah
1. Simple 2. Komunitif 3. Segmental

KLASIFIKASI
SMF Bedah FK UKI
14
IV. Arah garis patah
1. Transversal
2. Oblique 3. Spiral 4. Kompresi
KLASIFIKASI
SMF Bedah FK UKI
15
V. Lokasi 1. Tulang Panjang
• 1/3 proksimal• 1/3 tengah • 1/3 distal
2. Tulang Melintang• 1/4 medial• 1/4 lateral
KLASIFIKASI
SMF Bedah FK UKI
16
VI. Dislokasi Fragmen Undisplaced Displaced
Fragmen tlg searah (ad latus) Fragmen tlg membentuk sudut (ad
axim) Fragmen distal memutar (ad
periferum)
How fractures heal
SMF Bedah FK UKI
17
Tissue destruction and haematoma formation
Inflamation and cellular proliferation Callus formation Consolidation Remodelling
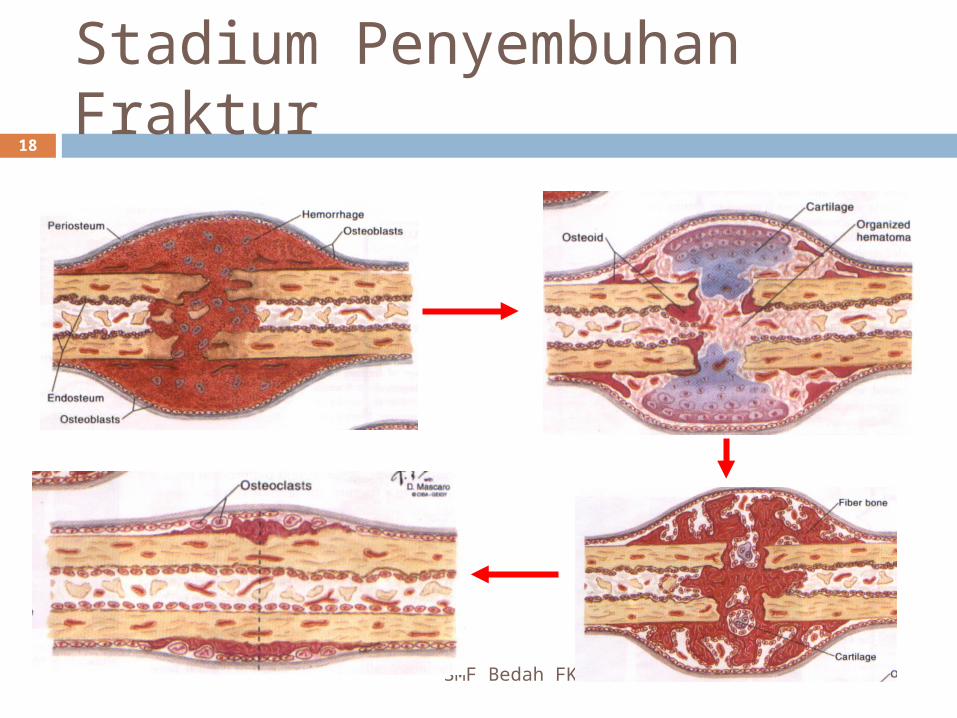
Stadium Penyembuhan Fraktur
SMF Bedah FK UKI
18
Healing by direct repair
SMF Bedah FK UKI
19
Fractures of cancellous bone Fractures treated by rigid internal
fixation
The time factor
SMF Bedah FK UKI
20
Rate of repair depends upon : the type of bone (cancellous bone heals
faster than cortical bone. type of fracture (transverse fracture takes
longer than spiral fracture) Blood supply (poor circulation means
slow healing) General constitution (healthy bone heals
faster Age (healing is almost twice as fast in
children as in adults)
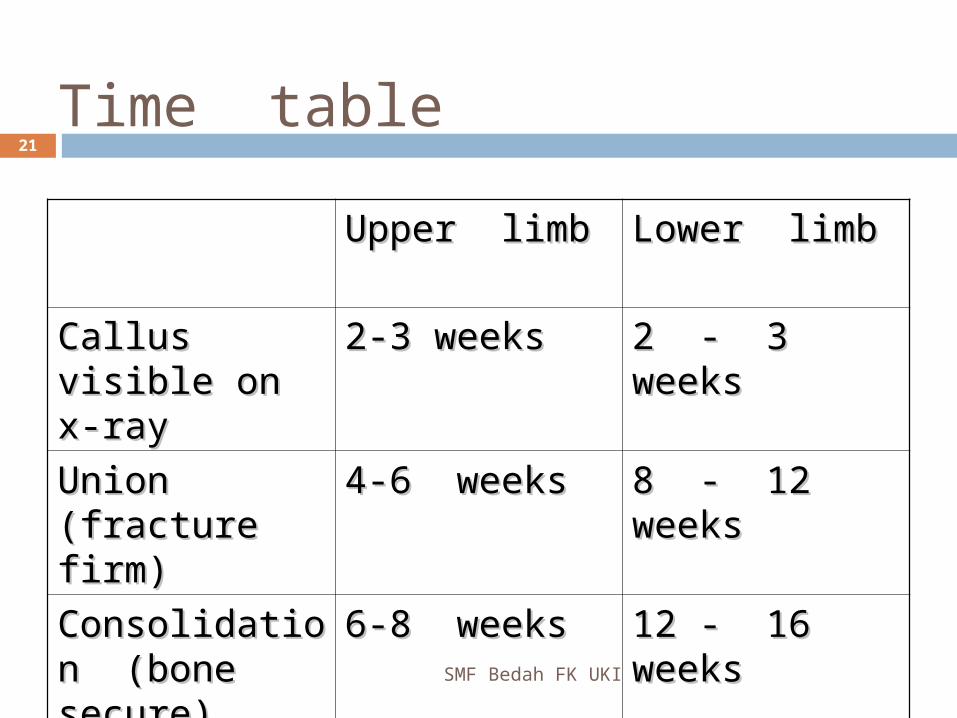
Time table
Upper limbUpper limb Lower limbLower limb
Callus visible Callus visible on x-rayon x-ray
2-3 weeks2-3 weeks 2 - 3 weeks2 - 3 weeks
Union Union (fracture (fracture firm)firm)
4-6 weeks4-6 weeks 8 - 12 8 - 12 weeksweeks
Consolidation Consolidation (bone secure)(bone secure)
6-8 weeks6-8 weeks 12 - 16 12 - 16 weeksweeks
SMF Bedah FK UKI
21
Fractures that fail to unite
SMF Bedah FK UKI
22
Causes of non union Distraction and separation of the
fragments Interposition of soft tissue between
the fragments Excessive movement at fracture line Poor blood supply
Most fracture will unite provide the bone fragments are
SMF Bedah FK UKI
23
Placed in contact with each other and
Held more or less immobile until new bone formation is apparent
Anamnesa
SMF Bedah FK UKI
24
The fracture is not always at the site of the injury
ANAMNESIS
SMF Bedah FK UKI
25
- Umur, jenis kelamin - Pekerjaan- Pendidikan - Lingkungan
rumah- Riwayat trauma:
• Arah• Jenis
- Lokalisasi nyeri - Gangguan fungsi
Examination
SMF Bedah FK UKI
26
General signsA broken bone is part of a patient. It is
important to look for evidence of : (1) shock or haemorrhage; (2) associted damage to brain, spinal cord or viscera; and (3) a prediposing cause
Look
SMF Bedah FK UKI
27
Swelling, bruising, Deformity Skin intact ?
Feel
SMF Bedah FK UKI
28
Local tenderness Examine distal to the fracture in
order to feel the pulse and test the sensation
Compartement syndrome ?
Move
SMF Bedah FK UKI
29
Crepitus and abnormal movement may be present, but it is more important to ask if the patient can move the joint distal to injury
Pemeriksaan Fisik
SMF Bedah FK UKI
30
Move : Nyeri gerak Sensorik Motorik
aktif
pasif

Bekas dukun
SMF Bedah FK UKI
31

Bekas dukun
SMF Bedah FK UKI
32

Xray
SMF Bedah FK UKI
33
Special imaging
SMF Bedah FK UKI
34
Tomography CT- scan MRI Radioisotope scanning
RADIOLOGI
SMF Bedah FK UKI
35
Rule of 2 : 2 proyeksi 2 sendi 2 ekstremitas 2 waktu
SMF Bedah FK UKI36
PRINCIPLES OF FRACTURE TREATMENT
First aid
SMF Bedah FK UKI
37
Make sure that the airway is clear If there is a wound, cover it with clean
material Stop bleeding by local compression Give something for pain If the neck or the bak is injured, prevent
flexion which may damage the spinal cord
If there is fracture,prevent movement
Assesment in hospital
SMF Bedah FK UKI
38
Examine the airway and treat asphyxia Make sure the patient can breathe Note the obvious haemorrhage and stop it Assess the degree of blood loss and shock Check for spinal cord injury Look for injuries of abdominal or pelvic viscera Examine for the presence of fractures or
dislocation Look for soft tissue complications, especially
nerve and vascular injury Arrange for an x-ray
Definitive treatment of closed fracture
SMF Bedah FK UKI
39
Manipulation to improve the position of the fragments, followed by splintage to hold them together until they unite; meanwhile joint movement and function must be preserved
Reposisi
SMF Bedah FK UKI
40
Mengembalikan kedudukan tulang
Cara :
• Manual
• Traksi
• Operatif
SMF Bedah FK UKI41
Fracture involving an articular surface; this should
be reduced as near to perfection as possible
because any irregularity will
predispose to degenerative arthritis
Closed reduction
SMF Bedah FK UKI
42
The distal part of limb is pulled in the line of the bone
As the fragment disengage, they are repositioned
Alignment is adjusted in each plane
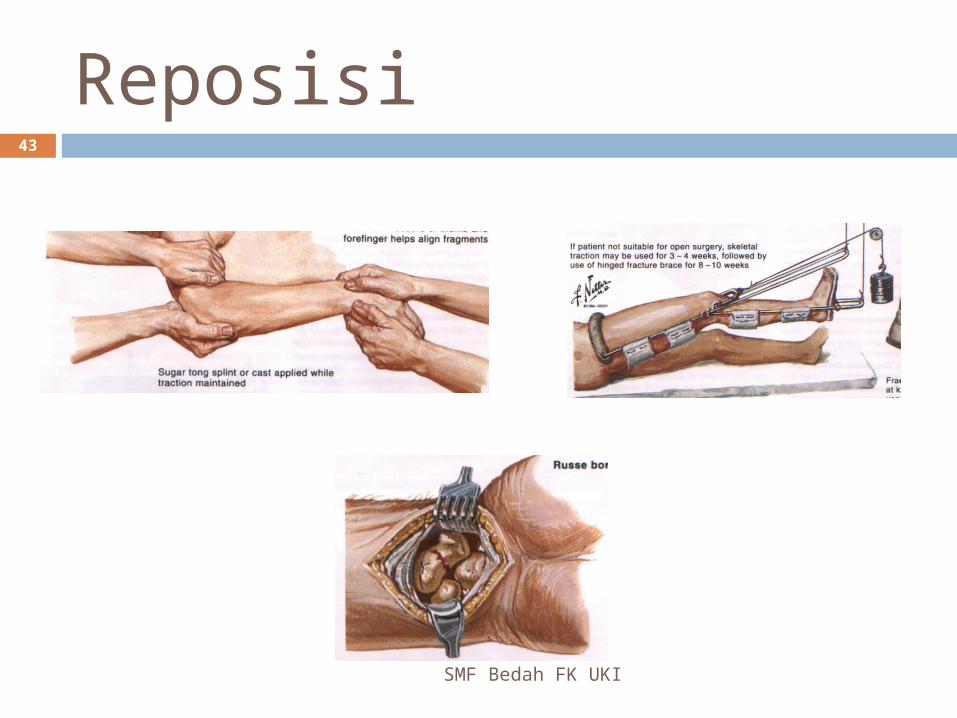
Reposisi
SMF Bedah FK UKI
43
Reposisi
SMF Bedah FK UKI
44
Keberhasilan dinilai dari : Alignment Contact > 50 % Rotation (-) Discrepancy (-) Sudut < 15 °
Indikasi konservatif
SMF Bedah FK UKI
45
Anak dalam masa pertumbuhan Impending infeksi Jenis fraktur tidak cocok untuk ORIF Toleransi operasi tidak baik Pasien menolak operasi
Indikasi Operasi
SMF Bedah FK UKI
46
Sukar reposisi tertutup Fraktur multipel Fraktur patologis Fraktur intra artikular
HOLD REDUCTION
SMF Bedah FK UKI
47
In order to unite, a fracture must be imobilized
We splint most fractures, not to ensure union but (1) to alliviate pain and (2) to ensure that union takes place in good position
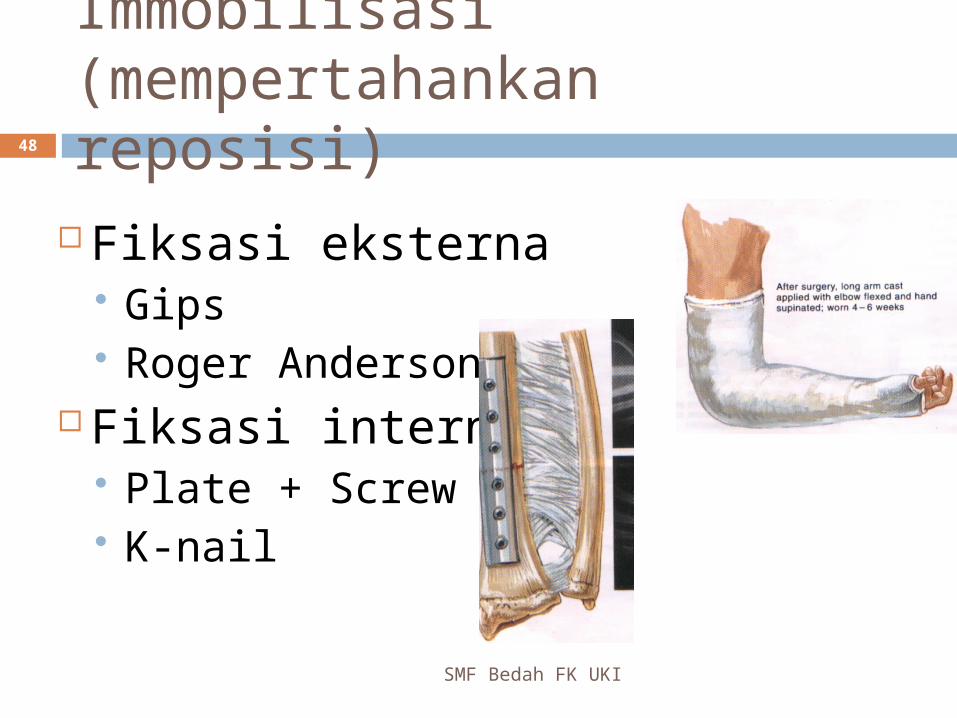
Immobilisasi (mempertahankan reposisi)
SMF Bedah FK UKI
48
Fiksasi eksterna Gips Roger Anderson
Fiksasi interna Plate + Screw K-nail
ORIF ; indications
SMF Bedah FK UKI
49
# that cannot be reduced except by operation
# that inherently unstable and prone to redisplacemaent after reduction (#mid shaft forearm)
# that unite poorly and take long time (# femoral neck)
Pathological # Multiple # # in patients who prsent nursing
difficulties (paraplegics, multiple injuries and very elderly
ORIF; complications
SMF Bedah FK UKI
50
INFECTION NON – UNION IMPLANT FAILURE REFRACTURE
OREF (open reduction external fixation) ; indications
SMF Bedah FK UKI
51
# associated wih severe soft tissue damage
# associated with nerve or vessel damage
Severely comminuted and unstable # # pelvis Infected #

SMF Bedah FK UKI52
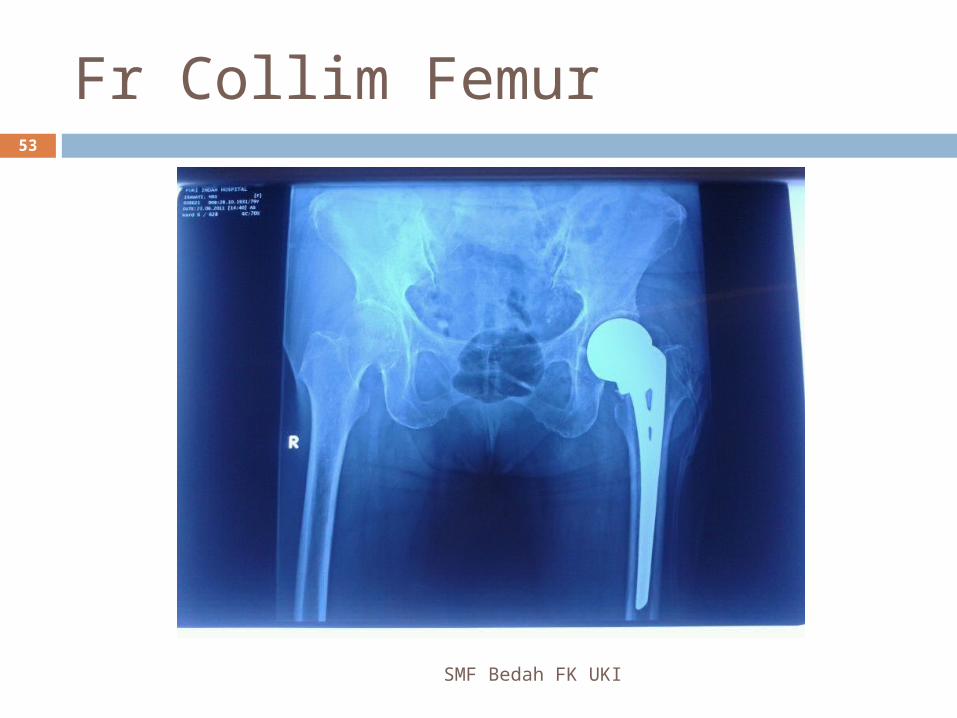
Fr Collim Femur
SMF Bedah FK UKI
53
OREF ; Complication
SMF Bedah FK UKI
54
Overdistraction Reduced load transmission trough
bone, which delays fracture healing causes osteoporosis (EF shoul be removed after 6-8 wo,and replace)
Pin tract infection
OPEN FRACTURE
SMF Bedah FK UKI
55
EMERGENCY GOLDEN PERIOD 6 – 8 HO
OPEN FRACTURE; assesment
SMF Bedah FK UKI
56
Is circulation intact ? Peripheral nerve intact ? State of skin arround the wound Does the wound communicate with
# ?
Fraktur Terbuka
SMF Bedah FK UKI
57
Perbaiki KU Debridement, kultur/resistensi ATS-Toxoid, Antibiotik Tutup luka dengan kasa bersih Reposisi Imobilisasi
ANTIBACTERIAL
SMF Bedah FK UKI
58
Antibiotics : asap, combination ampicilline and cloxacillin, given 6ho; if wound heavily contaminated, give gentamycin or metronidazole for 4-5 do
Tetanus prophylaxis
TREATMENT OF WOUND
SMF Bedah FK UKI
59
To cleanse the wound of foreign material
Remove devitalized tissue (debridement)
4 C : ColourConsistencyContractilityCapacity of bleeding
Complications of fractureGeneral complication
SMF Bedah FK UKI
60
Shock Crush syndrome Venous thrombosis and pulmonary
embolism Tetanus Gas gangrene Fat embolism
Complication involving # bone
SMF Bedah FK UKI
61
Infection Delayed union and non union Malunion Growth disturbance Avascular necrosis
Complication involving soft tissue
SMF Bedah FK UKI
62
Vascular injury Compartement syndrome (Volkmann”s
ischaemia) Nerve injury Visceral injury Myositis osificans
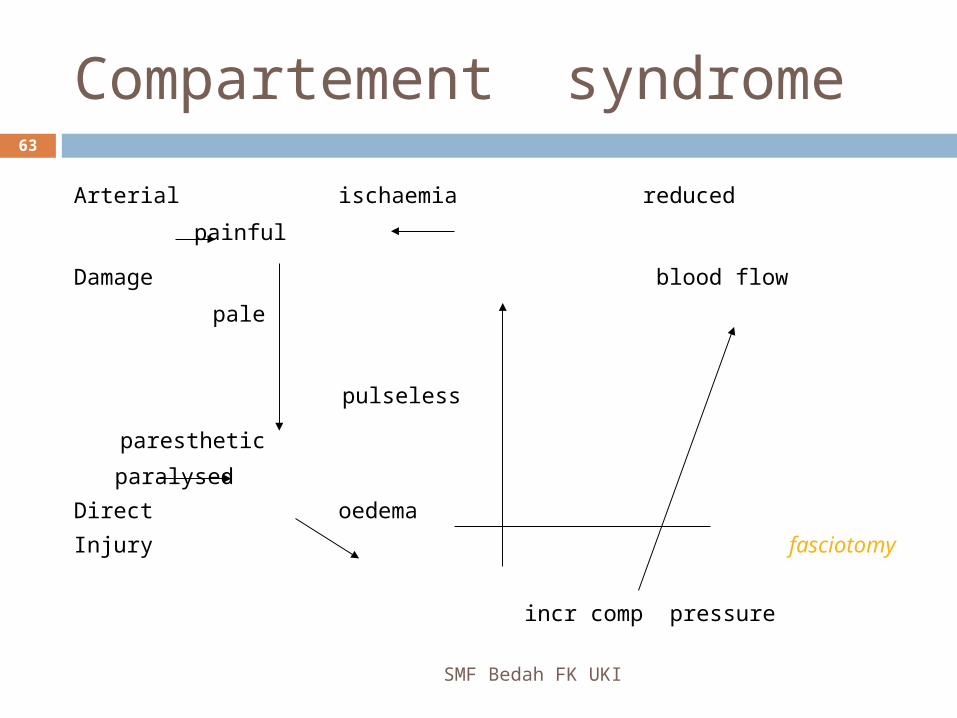
Compartement syndrome
SMF Bedah FK UKI
63
Arterial ischaemia reduced painful
Damage blood flow pale
pulseless
paresthetic
paralysed
Direct oedema
Injury fasciotomy
incr comp pressure
Complication involving joints
SMF Bedah FK UKI
64
Joint stiffness Osteoarthritis Sudeck’s atrophy

SMF Bedah FK UKI65

?SMF Bedah FK UKI
66
TERIMA KASIH
SMF Bedah FK UKI
67
Created by : “ Tepeng “

SMF Bedah FK UKI68