Embed Size (px)
Citation preview

Briefly
• What is FALP • The New RT challenge • Modelization of the project • Productivity issues and quantum leap • Relation to medical outcomes • The importance of a global cancer
management system
2

Time lapse 1954-2016
• FALP is a NGO, NPO founded 62 years ago • Acting as a stand alone “cancer only social
security” system in Chile • Covering for 20 Eu/month/family cancer
specialities: surgery, chemotherapy, RT • 500.000 suscribers of Falp cancer insurance • Due to local factors, RT was historically
poorly reimbursed in Chile thus inhibiting new investments in the field
3

Un modelo integrado y solidario de salud MEDICINA ONCOLOGICA PERSONALIZADA: RADIOTERAPIA AVANZADA –CIRUGIA COMPLEJA -ONCOGENOMICA
4

• Create an RT activity with high added value • Of recognized quality and patient centered • Offer a wide range of therapeutic tools • Competitive solutions in terms of tecnology,
quality control and pricing • Quantum leap: show how more advanced is less
complicated and efficient gap bridging • Create a comprehensive cancer center on the
existing bases started 60 years ago
The vision: new state of the art RT
5

Modelization: Time lapse 2013-2015
• Preparation of the de radiation shielding project
before the arquitectural plans (Q2-2013) • High complexity due to the fact that it had to be
build below an existing building • Need of a highly collaborative setup in the area
design • Choice of equipment • Choice of wide range of QA tools • Modelizacion of Mosaiq paperless management
system • HL7 external systems interfaces
6

First project 08-2013
7
Flaws in RT management in general
• Buy machines but not foresee:
– radiotherapy solutions and workflow implications
• the importance of organizational factors
– Team building
• Training issues
– Learning to work together – Quick and easy response to IGRT and SBRT treatments team work – Solve any possible communication problems through careful department
planning • Generalized and centralized data access in order to tackle: medical,
technical and administrative records plus all the department resource mangement
8
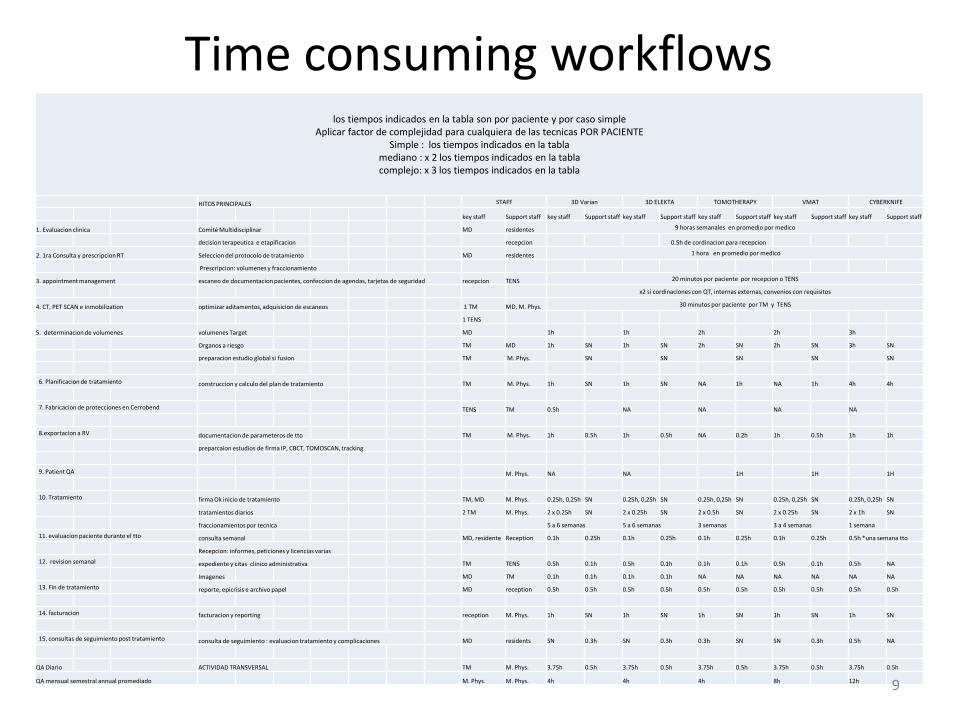
Time consuming workflows los tiempos indicados en la tabla son por paciente y por caso simple
Aplicar factor de complejidad para cualquiera de las tecnicas POR PACIENTE Simple : los tiempos indicados en la tabla
mediano : x 2 los tiempos indicados en la tabla complejo: x 3 los tiempos indicados en la tabla
HITOS PRINCIPALES STAFF 3D Varian 3D ELEKTA TOMOTHERAPY VMAT CYBERKNIFE
key staff Support staff key staff Support staff key staff Support staff key staff Support staff key staff Support staff key staff Support staff
1. Evaluacion clinica Comité Multidisciplinar MD residentes 9 horas semanales en promedio por medico
decision terapeutica e etapificacion recepcion 0.5h de cordinacion para recepcion
2. 1ra Consulta y prescripcion RT Seleccion del protocolo de tratamiento MD residentes 1 hora en promedio por medico
Prescripcion: volumenes y fraccionamiento
3. appointment management escaneo de documentacion pacientes, confeccion de agendas, tarjetas de seguridad recepcion TENS 20 minutos por paciente por recepcion o TENS
x2 si cordinaciones con QT, internas externas, convenios con requisitos
4. CT, PET SCAN e inmobilization optimizar aditamentos, adquisicion de escaneos 1 TM MD, M. Phys. 30 minutos por paciente por TM y TENS
1 TENS
5. determinacion de volumenes volumenes Target MD 1h 1h 2h 2h 3h
Organos a riesgo TM MD 1h SN 1h SN 2h SN 2h SN 3h SN
preparacion estudio global si fusion TM M. Phys. SN SN SN SN SN
6. Planificacion de tratamiento construccion y calculo del plan de tratamiento TM M. Phys. 1h SN 1h SN NA 1h NA 1h 4h 4h
7. Fabricacion de protecciones en Cerrobend TENS TM 0.5h NA NA NA NA
8.exportacion a RV documentacion de parameteros de tto TM M. Phys. 1h 0.5h 1h 0.5h NA 0.2h 1h 0.5h 1h 1h
preparcaion estudios de firma IP, CBCT, TOMOSCAN, tracking
9. Patient QA M. Phys. NA NA 1H 1H 1H
10. Tratamiento firma Ok inicio de tratamiento TM, MD M. Phys. 0.25h, 0,25h SN 0.25h, 0,25h SN 0.25h, 0,25h SN 0.25h, 0,25h SN 0.25h, 0,25h SN
tratamientos diarios 2 TM M. Phys. 2 x 0.25h SN 2 x 0.25h SN 2 x 0.5h SN 2 x 0.25h SN 2 x 1h SN
fraccionamientos por tecnica 5 a 6 semanas 5 a 6 semanas 3 semanas 3 a 4 semanas 1 semana
11. evaluacion paciente durante el tto consulta semanal MD, residente Reception 0.1h 0.25h 0.1h 0.25h 0.1h 0.25h 0.1h 0.25h 0.5h *una semana tto
Recepcion: informes, peticiones y licencias varias
12. revision semanal expediente y citas clinico administrativa TM TENS 0.5h 0.1h 0.5h 0.1h 0.1h 0.1h 0.5h 0.1h 0.5h NA
Imagenes MD TM 0.1h 0.1h 0.1h 0.1h NA NA NA NA NA NA
13. Fin de tratamiento reporte, epicrisis e archivo papel MD reception 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h
14. facturacion facturacion y reporting reception M. Phys. 1h SN 1h SN 1h SN 1h SN 1h SN
15. consultas de seguimiento post tratamiento consulta de seguimiento : evaluacion tratamiento y complicaciones MD residents SN 0.3h SN 0.3h 0.3h SN SN 0.3h 0.5h NA
QA Diario ACTIVIDAD TRANSVERSAL TM M. Phys. 3.75h 0.5h 3.75h 0.5h 3.75h 0.5h 3.75h 0.5h 3.75h 0.5h
QA mensual semestral annual promediado M. Phys. M. Phys. 4h 4h 4h 8h 12h 9

Final project 08-2014 Improved WORKFLOW through gaining 90m2 of open space for collaborative spaces
10

Workflow optimizing
11

2D 1970
3D 1980
IMRT 1999
IGRT 2006
VMAT IORT Tomotherapy Cyberknife 2010
Proton / IMPT
Carbon ion
RT ADAPTAVE…. FALP OCTOBER 2015
How to make up for the lost decades?
12

RT in 50 years
13

what is the (level 1) evidence? the budgetary impact? the cost? the value for money?
14
Methods of economical analisis in healthcare
Cost minimizing Allegedly all the benefits of competing treatments in terms of survival and y quality of life are the same. only the cost of a new treatment vs. Standard treatment is considered. The treatment of choice is the cheapest ! Value expressed in : U$
Cost effectivity The cost of an intervention is related to its impact on clínically relevant end point ("effectiveness”)… like: global survival Incremental Cost-effectivity Ratio (ICER) is the incremental cost, divided by the incremental benefit of a new intervención relatively to the STANDARD one. Value expressed in : U$ per year of saved life or U$ per QALYs US $ 50.000 / year of saved life
15

extra cost extra effect
new treatment
cost per life year gained (LYG) = incremental cost-effectiveness ratio
cost per quality-adjusted life year (QALY) = incremental cost-utility ratio
= ICER
cost effect
standard treatment
16

more effective less costly
cost
effectiveness
less effective more costly
more effective
more costly
less effective less costly
ICER 30-40.000€
per (quality adjusted) life year
17

Ploquin and Dunscombe, R&O 2008
historical evolution of the cost of radiation therapy over 20 years corrected for inflation and exchange rates
18

more complex treatments more time more resources capital investments
sophisticated equipment buildings QA
human resources treatment maintenance QA
more costly
19
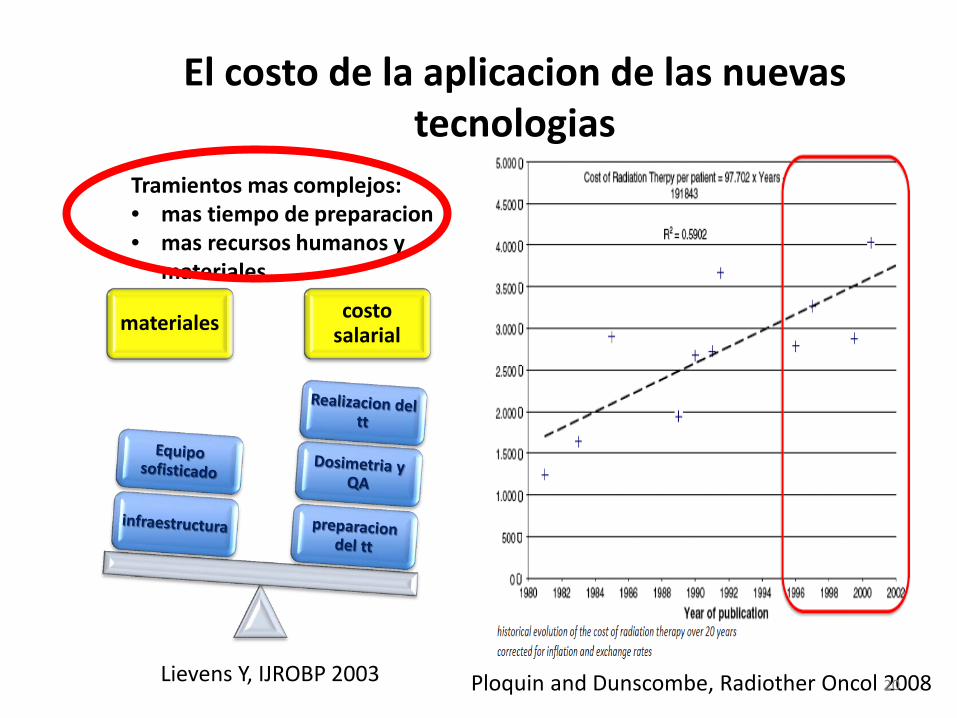
El costo de la aplicacion de las nuevas tecnologias
materiales costo salarial
Ploquin and Dunscombe, Radiother Oncol 2008
Tramientos mas complejos: • mas tiempo de preparacion • mas recursos humanos y
materiales
Lievens Y, IJROBP 2003 20

Multidisciplinary cordination
21

Perrier et al. R&O 2013
IGRT, prostate
22

Van de Werf et al. R&O 2012 23

more complex treatments contain costs without impact on quality?
1. limit cost of resources
2. optimize use of resources
3. decrease total treatment time 4. (time per fraction X number of fractions)
24

Unique range of solutions in South America • Cyberknife
• Tomotherapy • Elekta VMAT • LIAC (IORT) • Mosaiq Paperless
25

Lievens Y. The Breast 2010
hypofractionation, breast resource costs
26

“It’s always too early until, unfortunately, it’s suddenly too late!” (Buxton)
exte
nt c
linic
al u
se
time development Phase I-II
use in selected centres
RCT unethical? belief / widespread use still avoidable?
premarket emerging diffusing established obsolete cost calculation
finan
cing
finan
cing
>
>
effectiveness
cost effectiveness
uncertainty
27

Bonastre et al. Bull cancer 2006
Impact of training and previous experience
28

25 SUB-PROJECTS IN ORDER TO GO LIVE in 2015
1 Tomotherapy HD WORK FLOWS ARQUITECTURA ERGONOMETRICA INTERFACES CON SICI
2015: PET-CT big bore RADIOTERAPIA
1 Acelerador VMAT
IORT /HDR
- CENTRO PAPER LESS MOSAIQ 30 LICENCIAS
- CONECTIVIDAD 100% SICI Y RCC
3 XIO 2 MONACO 8 FOCAL
Neuro-Radiocirugía
1 CYBERKNIFE M6
29

The booster: Elekta Consulting services
• 100% paperless since day 1 means all your processes and interfaces with other services are 100% operational and optimized
• Centralized document fast scanning • Workflow modeling • Workflow automation with IQ Script • ESI :
– ADT (in and out) – SIU (agendas in and out) – DOC export (comite requests) – DOC Import (comite results)
30

THE MANAGEMENT SYSTEM IS KEY
MOSAIQ paperless in 2015 MOSAIQ big data in 2016
ESI+ IQ SCRIPT
MICRO-MANAGEMENT
31

MANAGING THE CHANGE= NEW STREAMLINED ORGANIZATION 1. NEW MD AGENDA ALLOWING TO CONTROL
1. PATIENTS WORKFLOW 2. QUALITY OF PET CT IMAGING 3. QUALITY OF CONTOURING 4. QUALITY OF TREATMENT PLANS REVIEWS AND SIGNATURE 5. PATIENT TREATMENT QA 6. MACHINE QA 7. OPTIMIZATION OF RESOURCE USAGE (TECHNICIANS, RADIOGRAPHERS ETC..} 8. WAIT LIST REMOVAL 9. ALL RT TASKS UNDER CONTROL 10. ALL TASKS MANAGED THROUGH MOSAIQ QCL
2. NEW JOB DESCRIPTIONS FOR ALL THE PERSONNEL INVOLVED IN RT 3. DOCUMENT ALL SOP (STANDARD OPERATION PROCEDURES) OF NEW TECHNIQUES
EMPLOYED, FROM END TO END 1. CONSULTATION 2. SCAN 3. CONTOURING 4. PRESCRIPCION 5. TREATMENT PLAN REVIEW 6. PATIENT SETUP AND IGRT 7. END OF TREATMENT EVALUATION 8 FOLLOW UP SCHEMES
32

The booster: Elekta Consulting services
• Build a procedure code nomenclature • Configure MOSAIQ with the procedure code
nomenclature • Develop charge capture quality control
reporting • Implement charge capture process and
controls for quote process and billing process • Validate account and charge exchange process
with CISI (FALP billing system)
33

Out of scope
Treatment cost
DIRECTINDIRECT
Personnel MaterialEquipment
RT patient related activities RT support act.
Intake consultation
Medical review …
APBI -brachytherapy
SBRT – lung –5 fractions …
Overhead
OtherEquipment Maint. & QA
Material
Time driven
Activity consumption Per fraction
Non-RT, care
activities
Non- care activities
RT patient related
RT support
Mark-up % on treatment cost
80% fraction20% patient
56.6%
Hulstaert et al, Rapport 198 KCE 2013
The booster: Elekta Consulting services, reducing overheads and operations costs through automated interfaces
34

Time consuming workflows los tiempos indicados en la tabla son por paciente y por caso simple
Aplicar factor de complejidad para cualquiera de las tecnicas POR PACIENTE Simple : los tiempos indicados en la tabla
mediano : x 2 los tiempos indicados en la tabla complejo: x 3 los tiempos indicados en la tabla
HITOS PRINCIPALES STAFF 3D Varian 3D ELEKTA TOMOTHERAPY VMAT CYBERKNIFE
key staff Support staff key staff Support staff key staff Support staff key staff Support staff key staff Support staff key staff Support staff
1. Evaluacion clinica Comité Multidisciplinar MD residentes 9 horas semanales en promedio por medico
decision terapeutica e etapificacion recepcion 0.5h de cordinacion para recepcion
2. 1ra Consulta y prescripcion RT Seleccion del protocolo de tratamiento MD residentes 1 hora en promedio por medico
Prescripcion: volumenes y fraccionamiento
3. appointment management escaneo de documentacion pacientes, confeccion de agendas, tarjetas de seguridad recepcion TENS 20 minutos por paciente por recepcion o TENS
x2 si cordinaciones con QT, internas externas, convenios con requisitos
4. CT, PET SCAN e inmobilization optimizar aditamentos, adquisicion de escaneos 1 TM MD, M. Phys. 30 minutos por paciente por TM y TENS
1 TENS
5. determinacion de volumenes volumenes Target MD 1h 1h 2h 2h 3h
Organos a riesgo TM MD 1h SN 1h SN 2h SN 2h SN 3h SN
preparacion estudio global si fusion TM M. Phys. SN SN SN SN SN
6. Planificacion de tratamiento construccion y calculo del plan de tratamiento TM M. Phys. 1h SN 1h SN NA 1h NA 1h 4h 4h
7. Fabricacion de protecciones en Cerrobend TENS TM 0.5h NA NA NA NA
8.exportacion a RV documentacion de parameteros de tto TM M. Phys. 1h 0.5h 1h 0.5h NA 0.2h 1h 0.5h 1h 1h
preparcaion estudios de firma IP, CBCT, TOMOSCAN, tracking
9. Patient QA M. Phys. NA NA 1H 1H 1H
10. Tratamiento firma Ok inicio de tratamiento TM, MD M. Phys. 0.25h, 0,25h SN 0.25h, 0,25h SN 0.25h, 0,25h SN 0.25h, 0,25h SN 0.25h, 0,25h SN
tratamientos diarios 2 TM M. Phys. 2 x 0.25h SN 2 x 0.25h SN 2 x 0.5h SN 2 x 0.25h SN 2 x 1h SN
fraccionamientos por tecnica 5 a 6 semanas 5 a 6 semanas 3 semanas 3 a 4 semanas 1 semana
11. evaluacion paciente durante el tto consulta semanal MD, residente Reception 0.1h 0.25h 0.1h 0.25h 0.1h 0.25h 0.1h 0.25h 0.5h *una semana tto
Recepcion: informes, peticiones y licencias varias
12. revision semanal expediente y citas clinico administrativa TM TENS 0.5h 0.1h 0.5h 0.1h 0.1h 0.1h 0.5h 0.1h 0.5h NA
Imagenes MD TM 0.1h 0.1h 0.1h 0.1h NA NA NA NA NA NA
13. Fin de tratamiento reporte, epicrisis e archivo papel MD reception 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h 0.5h
14. facturacion facturacion y reporting reception M. Phys. 1h SN 1h SN 1h SN 1h SN 1h SN
15. consultas de seguimiento post tratamiento consulta de seguimiento : evaluacion tratamiento y complicaciones MD residents SN 0.3h SN 0.3h 0.3h SN SN 0.3h 0.5h NA
QA Diario ACTIVIDAD TRANSVERSAL TM M. Phys. 3.75h 0.5h 3.75h 0.5h 3.75h 0.5h 3.75h 0.5h 3.75h 0.5h
QA mensual semestral annual promediado M. Phys. M. Phys. 4h 4h 4h 8h 12h 35


Objetivos del control de calidad • Ni errores aleatorios (puesta del paciente, reproductibilidad
entre fracciones) • Ni errores sistemáticos (TPS, equipo mal calibrado,
contención defectuosa) • radioterapia es un multi-proceso complejo, de alta
tecnicidad, que requiere reflexión profunda sobre la seguridad de todas las etapas: SISTEMA DE CALIDAD
• Valorar constantemente la practica y organización de un servicio : implantar la CULTURA DE LA SEGURIDAD
• Cultura de la transparencia y declaración de los fallos • Fiabilisacion et automatización
– Peer review et CQE antes 1er tratamiento – Doble calculo independiente – Verify & Record avanzado – In vivo – Protocolos de Imágenes Portales/ IGRT – CQI (leyes y responsabilidades Físicos) – CQE (organismos de control, APAVE, ASN, etc..)

IMPLEMENTACION FALP: SQL DB MYQA (IBA)


AUDITORIA EXTERNA Y CERTIFICACION FALP: EQUAL ESTRO
• UN TEST POR CONO • TEST PREVIOS CON CC01 • IMPRESCINDIBLE
Safety basics
If you think safety is expensive, think about an accident (Epinal) or a
plane crash.

TOMOTHERAPY HD
• RT EN 360°
• IMRT-IGRT con Tomo View (megavoltaje).
• Varias localizaciones únicas, simultáneas o voluminosas.
• Tumores pediátricos.
• Tratamientos hipofraccionados.
SYNERGY AGILITY VMAT
• RT en hemi-arcos.
• IMRT – IGRT cone beam CT (kilovoltaje)
• Tumores con fraccionamiento convencional.
CENTRO DE RADIOTERAPIA AVANZADA RADIOTERAPIA DE INTENSIDAD MODULADA-GUIADA POR IMÁGENES

PARA QUÉ UN PLAN DE CALIDAD
• Para mejorar la supervivencia con la máxima calidad vital de los pacientes oncológicos
• Para evitar accidentes. • Para optimizar los recursos sanitarios • Para optimizar el uso racional de las radiaciones
ionizantes. • Para prevenir demandas legales.
Curso de Actualización para Tecnólogos en Radioterapia. ARCAL RLA6/058 Tema 22 : Garantía de Calidad J. M. Delgado 32 2008-10
Increasing health care expenses force us to consider the value for money of novel treatments.
Shorter treatment times compensate for the higher cost of complexity.
Hypofractionation has the potential of being “economically dominant”.
Coverage with Evidence Development can facilitate the early introduction of promising new technologies.
Convince with figures through careful big data planning,,, being the pioneer
Conclusions
44

FALP GRACIAS…. 45