Embed Size (px)
Citation preview

AMERICAN JOURNAL OF OPHTHALMOLOGY VOLUME 64 JULY, 1967 NUMBER 1
FUNDUS FLAVIMACULATUS
C L I N I C A L , FUNCTIONAL AND HISTOPATHOLOGIC OBSERVATIONS
B E R T H A A. K L I E N , M.D., AND A L E X E. K R I L L , M.D. Chicago, Illinois
The term "fundus flavimaculatus" was first used by Franceschetti in 19621 to describe the eyegrounds of patients with a characteristic retinal abnormality. In his original and in subsequent publications,2"8
the fundi of 36 patients were described. The characteristic ophthalmoscopic le
sions were white or yellowish-white deep retinal flecks varying within the same fundus in shape, size, opaqueness, density and sometimes apparent depth. Among the different shapes either round or linear lesions predominated. Some linear lesions resembled fish tails and were called pisciform.
From the Eye Research Laboratories, University of Chicago, and the Department of Ophthalmology, University of Illinois. This study was supported in part by the National Institutes of Health, Public Health Service, grants NB-33S8 and FR-55.
Reprint requests to: Alex E. Krill, M.D., Eye Research Laboratories, University of Chicago, 950 East 59th Street, Chicago, Illinois 60637.
The size of the individual lesion varied greatly, from the smallest caliber vessel to larger than the widest caliber vein. Confluence of either linear or round lesions was common. Confluent round lesions sometimes resembled colonies of staphylococci. The spots varied in opaqueness, some appearing clearer than others ; occasionally one had an atrophie appearance. Their borders were fuzzy or of medium-sharp outline. Most appeared to be as deep as drusen. Pigmentation was not a prominent feature. However, some lesions had a fine powdery pigment around the border or over them, giving a dirty appearance to the color. They were either limited to the posterior polar region or else extended to the equatorial region. Sometimes a garland or crown arrangement resulted in the posterior polar region. When widespread, the flecks were particularly dense in the equatorial region.
In all 36 patients described by
Fis. 15 (Klien and Krill). Fundus flavimaculatus: Clinical, functional and histopathologic observations. A. Case 21, right eye. Pigment epithelium in inferior midperiphery. Artificial separation of retina and of portions of pigment
epithelium. Nuclei displaced inward, line of condensation of pigment granules, abnormal material accumulated in inner half of pigment epithelial cell. Many cells do not contain pigment granules outside the line of condensation. (Hematoxylin-eosin,
B. Inferior near periphery. Marked variation in sizes of pigment epithelial cells and their pigment content, small amount of abnormal material in inner half of cells in front of line of pigment condensation. Retina artificially detached, well preserved aside from glaucomatous damage to inner neurons. (Hematoxylin-eosin, XI60.)
C. Inferior near periphery. Visibility of pigment epithelium exaggerated due to content of PAS-positive granules, compare with (D) . Marked variation in sizes of cells. Normal Bruch'» membrane and choriocapillaris. (PAS, XI60.)
D. Two sections apart from (C). Pigment epithelium inconspicuous due to reduced pigment content. Over it the entire blue staining layer of neuroepithelium is intact. (Alcian blue, XI60.)
E. Nasal midperiphery. Abnormal material showing mesh I ike pattern, conglomerations of coarse PAS-positive granules in basal portion of cells. (PAS, X630.)
F. Nasal midperiphery. Confluent deposit» of abnormal material in inner half of adjacent pigment epithelial cells. Pattern of material meshlike; meshes filled with blue-staining acid mucopolysaccharides, removable by pretreatment of sections with hyaluronidase. (Rinehart Haj method for acid mucopolysaccharides, X250.)

4 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
Franceschetti1'2'3'6 or by Franceschetti and François,4 the optic nerves and retinal vessels were normal. Pigmentary migration or disturbance of the type seen in pigmentary degeneration, was absent. A very important finding was macular involvement in 18 patients.
Retinal function evaluation was normal or showed only minimal abnormalities. Visual fields were normal except for central scoto-mas in the cases with macular lesions. The electroretinogram (ERG) was usually normal but four patients had subnormal b-wave amplitudes. Dark-adaptation curves showed a slightly elevated final rod threshold in seven cases.
The longest follow-up period was 15 years. Although an increase in the number of lesions along with the progression of macular lesions was reported in some patients, none had a loss of peripheral visual field and only one had a progression of a dark-adaptation abnormality during the period of observation. Seventeen patients were less than 25 years of age when first seen. The youngest was 10 years of age and first complained of symptoms at the age of seven years.
Only two cases were familial (brother and sister) but two others had related parents (cousins). However, there are three reports6"8 (where a diagnosis of fundus flavimaculatus was definitely made6 or is suspected in retrospect from the publication pictures7·8) with familial incidence (brother and sister). In one of these families, the parents were related.7 The available data thus suggest an autosomal recessive type of inheritance.
Other cases in the literature probably fit into the fundus flavimaculatus category. The three patients described by Kandori9"11
have such lesions. These patients had dirty yellow, deep, irregular flecks of greatest concentration in the midperiphery. Two were followed for 20 years with no progression. All three had delayed, but normal, dark-adaptation thresholds as well as a
delay in the development of a maximum scotopic b-wave. These patients were similar to many of Franceschetti's in: (1) the appearance of the lesions, (2) the young age of onset, (3) the lack of progression, (4) the normal retinal vessels and optic nerves, and (5) the minimal dark-adaptation and ERG abnormalities. None of Kandori's patients had macular lesions—neither did 18 of those reported by Franceschetti.4 Many patients with juvenile macular degeneration,3'12 including some of the original cases described by Stargardt,13 had associated deep retinal flecks, but in these reports no particular emphasis was placed on these extramacular lesions.
The resemblance of these cases to those with colloid bodies or drusen and fundus albipunctatus was emphasized in previous reports.14"16 The term flecked retina syndrome was introduced to stress common findings in these three ophthalmoscopically distinct entities. These findings included (1) normal peripheral visual fields, (2) usually a mildly abnormal dark-adaptation reflected by slow subjective dark-adaptation and the slow development of a maximum scotopic b-wave of the ERG, (3) a frequently abnormal electro-oculogram (EOG), (4) a high incidence of macular abnormalities, (5) the stationary status of the minor abnormality of peripheral retinal function and (6) similar fluorescein staining patterns.
The purpose of this report is to present detailed clinical and functional observations in 27 patients with fundus flavimaculatus and the histopathologic findings in one eye of one of these patients.
REPORT OF CASES
The 27 patients were divided into two groups: Group I, a pure form, nine patients ; and Group II, a form with a macular degeneration, 18 patients.
Patients with the pure form had only typical flavimaculatus lesions. These patients were subdivided into two groups: (A) one

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS
Case
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Age
37 65 30 18 28 11 15 44 30 22 28
7 10 34 32 42 40 45 60 50 23 63 19 28 20 21 40
Sex
F M F M F F M F F F F M M F M F M F M M M M M F M F M
Vision
RE
20/200 5/200
20/200 20/200 20/200 20/200 20/300 20/300 20/200 20/400 20/200 20/80 20/200 20/200
7/200 20/30 20/20 20/20 20/20 20/20 N L P 20/20 20/200 20/30 20/300 20/70 20/25
DA—dark adaptation;
LE
20/200 10/200 20/200 20/300 20/200 20/200 20/200 20/300 20/200 20/400 20/200 20/80 20/200 20/200
7/200 20/200 20/20 20/60 20/25 20/30 20/30 20/20 20/70 20/80 20/200 20/30 20/80
RCB—rod
TABLE 1 SUMMARY OF CASES STUDIED
EOG
2.5 1.7 —
1.6
— ■
1.6 1.1 1.9
1.8 1.9 — — ■
— 2.4 —
2.7 1.9 1.6 —
1.6 1.4 1.3 —
1.6
cone 1
2.4 1.7 —
1.5
1.4 —
1.2 1.8
1.7 1.7
— ■
— —
2.2 —
2.2 1.9 1.4 2.2
1.8 1.4 1.7 —
1.6
DA
N Slow Abn Slow
Slow Slow
N N
Slow Abn Slow Slow Slow Slow
N Slow Slow Slow
N
Slow Slow Slow Slow Slow
E R G
Intensities ^
17 min
Abn Abn Abn Abn
N Abn
N N
Abn Abn Abn Abn
N Abn
N Abn
N N N
Abn Abn —
Abn N
45 min
N N — N
N N N N
N Abn — N — N — N N N N
N N —· N N
break; FT—final threshold; N-
CT 5.06+
3 9 9 5
7 3 6 8
10 11 —
6 11 8 5
13 10 5 6
7 10 9
10 10
Dark-Adaptat
RCB 12.1 +
9 17 17 16
14 16 14 13
16 16
• — ■
13 16 16 11 30 12 17 15
15 20 16 15 14
—normal; Abn-
RT 35.7+
45 55
> 6 0 55
35 36 54 50
67 > 6 0
— 35 30 38 30 62 50 45 45
51 50 36 30 55
ion F T
6X102*
6.0(102) 6.4 (102) 2.3 (105) 1.6 (103)
8 (10s) 5.8 (102) 5.4 (102) 2.7 (102)
5.9 (102) 4 (10s)
—. 1.8 (102)
N 2.5 (102) 1.5 (10s) 3.2 (102) 4 .5 (102) 4 .0 (102) 3.3 (102)
4.6 (102) 5.3 (102) 5.2 (102) 4 .2 (102) 1.2 (10s)
—abnormal; RT— rod threshold; Int—intensity; +—mean time +2 standard deviations of 57 normals
* Arbitrary units for mean +2 standard deviations of 25 normals.
with no macular involvement, (B) the other with varying encroachment of the foveal region by lesions formed by confluence of typical flavimaculatus flecks. The foveal involvement caused varying degrees of diminution of vision and seemed to be an incidental involvement, sometimes present in only one eye.
The macular affections found in our patients of Group II were of two varieties, that is, (1) flat atrophie lesions (Stargardt-type) characterized in the incipient stages by relatively inconspicuous changes despite the severe visual defect, and (2) an elevated lesion (Kuhnt-Junius type). The pertinent group will be mentioned in each patient.
The age, sex and pertinent functional information are summarized in Table I. All acuities are with best correction. Since the
refractive errors showed no consistent pattern, these are not mentioned in the case reports. Fifteen of the 27 patients were 30 years of age or younger. The youngest patient was seven years of age (Case 12) and the oldest 65 (Case 22). The average age was 32 and the median age 30 years. There were 14 males and 13 females. There were five Negroes (Cases 6, 7, 11, 15 and 25) and the remainder were Caucasians.
In all fundi, optic nerves and retinal vessels were normal. Other eyeground changes will be discussed for each patient. Fluorescent spots seen after intravenous fluorescein always appeared in the arterial phase and always persisted beyond the venous phase without a change in size; therefore, these details will not be stated again where fluorescein studies were done. Follow-up ex-

6 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
Fig. 1 (Klien and Krill), Case 1. A woman, aged 30 years. Right eye. Right vision 20/200. Isolated, deep-seated, opaque, pisciform lesions in paramacular area; more confluent similar areas in mid-periphery. Atrophie area (one-sixth disc diameter) in foveal region.
aminations over 12 months will be specifically mentioned. The evaluation of eyeground changes on follow-up was made by detailed comparison of fundus photographs whenever possible. Case 1 (Group II, with atrophie macular lesion)
A woman, aged 37 years, had onset of visual disturbance in her late teens. Right and left vision were 20/200. Striking, widely spaced, deep-seated pisciform lesions were scattered over the paramacular areas (fig. 1). In tnidperiphery there was a tendency for confluence of most of the yellowish flecks into a sand-dune pattern. The maculas were occupied by sharply delineated areas of pigment rarefication with overlying dusty pigmentation. Nine years later the macular lesions were slightly larger, but the most significant change occurred in the formerly isolated pisciform paramacular lesions. These were less opaque than before, softer in outline, more numerous and confluent into various patterns (fig. 2), similar to the midperipheral lesions.
CASE 2 (Group II with atrophie macular lesion) A man, aged 65 years, was the father of the
patients in Cases 1 and 3. Rapid bilateral loss of vision began at the age of 19 years, with further deterioration1 during the past IS years. Right vision was 5/200; left vision 10/200. On fundus examination, the macular areas showed a peculiar, glistening sheen within sharply defined but rather inconpicuous reddish areas. Deep yellowish flecks, some of pisciform shape, were scattered over the paramacular and midperipheral regions. Ten years later the macular lesions were larger
and the perimacular lesions were more numerous, with many of the old ones showing softer outlines.
CASE 3 (Group II, atrophie macular lesion and progressive, peripheral pigmentary disturbance) A woman, sister of the patient in Case 1 and
daughter of the patient in Case 2, aged 29 years, had onset of visual disturbance at the age of 17 or 18. Right and left visions were 20/200. Fundus examination showed typical, partly pisciform flavimaculatus lesions scattered over paramacular and midperipheral areas. There was a diffuse peripheral pigmentary disturbance (fine deposits), and the maculas were occupied by areas of pigment atrophy. After an interval of eight years, the macular lesions and the areas of peripheral pigmentary disturbance had expanded, the latter into the midperiphery formerly occupied by deep yellow flecks. The yellowish areas in the paramacular regions had faded into less conspicuous patches. The discs and retinal vessels were still normal.
CASE 4 (Group II, with atrophie macular lesion) A man, aged 18 years, had noted visual distur
bance for one year. Right vision was 20/200, left vision 20/300. Both foveal regions were a dull, opaque, gray color. Deep-seated yellowish flecks, many of fish-tail shape, were almost evenly distributed over periphery and midperiphery of both fundi. The intensity of opacification varied greatly and was least in confluent lesions, such as in an area just above the left fovea (fig. 3). Special mention is made of this area since many more lesions were seen here after fluorescein injection
Fig 2 (Klien and Krill). Case 1. Same eye as in Figure 1, eight years later. Paramacular lesions less opaque, softer in outline, more numerous and confluent into various patterns. Atrophie macular lesion larger (1.5 disc diameters).
VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 7
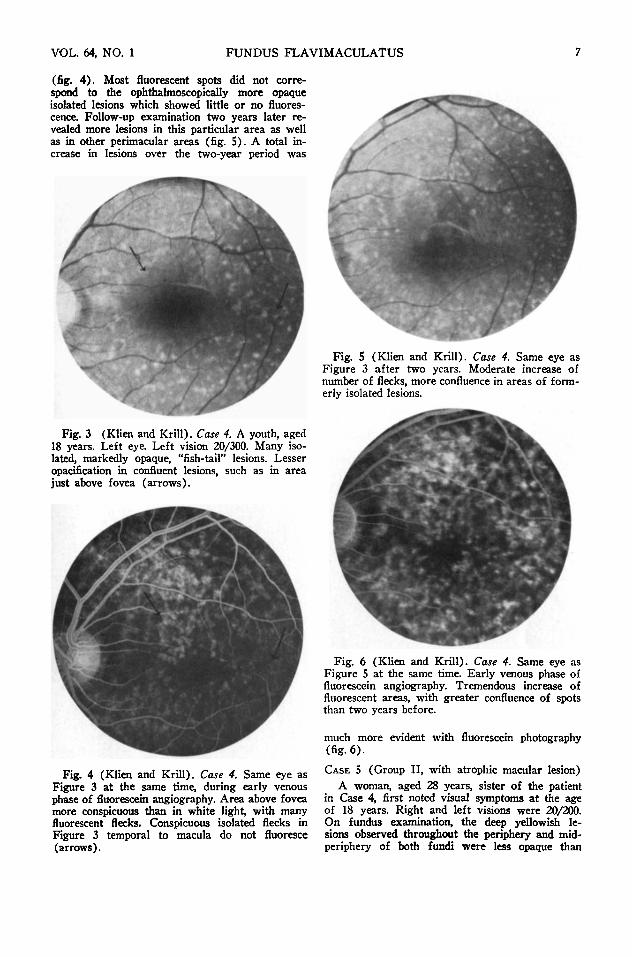
(fig. 4). Most fluorescent spots did not correspond to the ophthalmoscopically more opaque isolated lesions which showed little or no fluorescence. Follow-up examination two years later revealed more lesions in this particular area as well as in other perimacular areas (fig. 5). A total increase in lesions over the two-year period was
Fig. 3 (Klien and Krill). Case 4. A youth, aged 18 years. Left eye. Left vision 20/300. Many isolated, markedly opaque, "fish-tail" lesions. Lesser opacification in confluent lesions, such as in area just above fovea (arrows).
Fig. S (Klien and Krill). Case 4. Same eye as Figure 3 after two years. Moderate increase of number of flecks, more confluence in areas of formerly isolated lesions.
Fig. 6 (Klien and Krill). Case 4. Same eye as Figure S at the same time. Early venous phase of fluorescein angiography. Tremendous increase of fluorescent areas, with greater confluence of spots than two years before.
Fig. 4 (Klien and Krill). Case 4. Same eye as Figure 3 at the same time, during early venous phase of fluorescein angiography. Area above fovea more conspicuous than in white light, with many fluorescent flecks. Conspicuous isolated flecks in Figure 3 temporal to macula do not fluoresce (arrows).
much more evident with fluorescein photography (fig. 6). CASE S (Group II, with atrophie macular lesion)
A woman, aged 28 years, sister of the patient in Case 4, first noted visual symptoms at the age of 18 years. Right and left visions were 20/200. On fundus examination, the deep yellowish lesions observed throughout the periphery and mid-periphery of both fundi were less opaque than

8 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
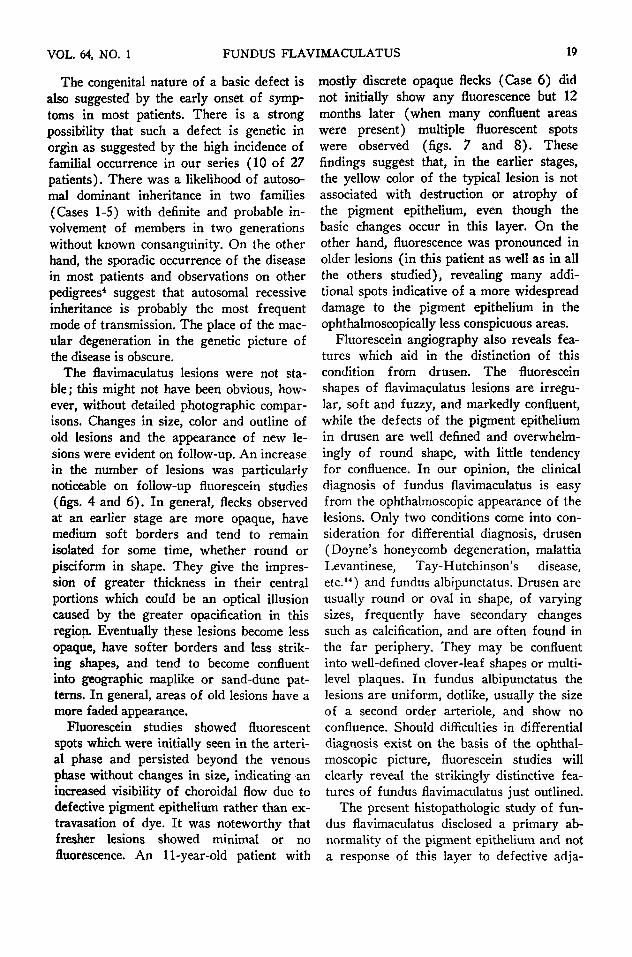
Fig. 7. (Klien and Krill). Case 6. A girl, aged 11 years. Left eye. Fluorescein study, early venous phase. Fluorescence only in macular region, even after 30 minutes' observation.
those of her brother and more confluent into a wavy sand-dune pattern. Smaller, more discrete flecks were scattered over the paramacular regions. Areas of pigment atrophy, 1.5 papillary diameters in size and dotted with fine and coarse pigment deposits occupied both maculas.
This patient's six-year-old son had a visual acuity of 20/200 in each eye. No flavimaculatus lesions were discernible but the maculas showed a
Fig. 8. (Klien and Krill). Case 6. Twelve months later, showing many more fluorescent spots in macula and for the first time extramacular fluorescent spots, which began in the arterial phase and persisted (without change in size) beyond the venous phase.
grayish discoloration with loss of the normal reflexes. This could be an early stage of the same disease observed in mother and uncle.
CASE 6 (Group II, with atrophie macular lesion) A girl, aged 11 years, sister of the patient in
Case 7, had a Negro father and white mother. Her poor vision was discovered in school. Right and left visions were 20/200. Fundus examination showed normal foveal reflexes but a dull gray, granular appearance of the remaining macular areas. Typical flavimaculatus lesions, many of them pisciform, were scattered over the peri-macular and midperipheral areas. Except for a few spots of confluence in the midperiphery, the flavimaculatus lesions were discrete and opaque. The fundi in general were light, similar in coloring to those of her German mother. Fundus study after intravenous fluorescein injection showed only light spotty fluorescence of the macular area (fig. 7). None of the flavimaculatus lesions showed fluorescence. Twelve months later, however, there were many definite extramacular fluorescent areas in addition to an increase in the number of macular fluorescent spots (fig. 8). At this time many more confluent areas were seen on routine ophthalmoscopic examination.
CASE 7 (Group II, with atrophie macular lesion) A boy, aged 15 years, the brother of the pa
tient in Case 6, had noted poor vision for the past three or four years. Right vision was 20/300, left vision 20/200. On fundus examination, a glistening sheen was seen in both maculas. Typical flavimaculatus lesions were scattered over the midperipheries and posterior polar regions, most of them pisciform. Confluence into a sand-dune pattern was noted mainly nasal to discs. The general pigment content of the fundi was of Negroid intensity.
Neither the Negro father nor the white mother had any visual complaints. The mother's fundi were normal.
CASE 8 (Group II, atrophie macular lesion) A woman, aged 44 years, had had poor vision
in both eyes since the age of seven or eight years. Right and left visions were 20/300. One sister (Case 9) had the same diagnosis. On fundus examination, the maculas were seen to be occupied by sharply defined areas of chorioretinal atrophy with moderate pigment proliferation. The macular lesions were surrounded by a network of faint confluent yellowish areas. In the intermediary regions, the less numerous in the farther periphery, there were more opaque yellowish white flecks, partly isolated round, partly linear in shape. Fluorescein studies revealed an increased number of lesions particularly in the areas surrounding the maculas.
CASE 9 (Group II, atrophie macular lesion) A white woman, aged 30 years, was the sister
of the patient in Case 8. She first became aware

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 9
of poor vision at the age of 19 years when she was rejected for a job. Right and left visions were 20/200. Fundus examination showed areas of depigmentation in both maculas. Numerous deep yellowish flecks of varying size, density and configuration were scattered over the paramacular regions and less abundantly over the near periphery nasal to the discs.
CASE 10 (Group II, atrophie macular lesion) A woman, aged 22 years, had had poor vision
since childhood. Right and left visions were 20/400. Fundus examination showed that both foveal regions were occupied by flat, inconspicuous, reddish areas with a peculiar sheen. These were surrounded by deep-seated, softly contoured, round or oblong yellowish flecks. Toward the midperipheries these lesions became larger and more isolated, many of them showing fish-tail shape.
One of the patient's four brothers, aged 18 years, had similar visual defects since early childhood. None of the patient's three young children had obvious visual difficulties.
CASE 11 (Group II, fundus flavimaculatus with atrophie macular lesions and total color blindness) A woman, aged 27 years, had noted marked
failure of vision for the past 10 years but had had some visual difficulty since childhood. Right and left visions were 20/200. Fine pendular nys-tagmoid movements were present. On fundus examination, deep-seated yellowish flecks, mostly isolated and of pisciform shape, were seen scattered over midperipheries and paramacular regions. The maculas were occupied by atrophie areas with sharp, lobulated outlines and central accumulations of pigment. Fluorescein studies showed an increased number of flecks in areas which were occupied by inconspicuous confluent lesions in white light but the prominent isolated pisciform and round flecks seen in white light showed little or no fluorescence. The diagnosis of total color blindness was made from color vision and ERG findings. (These will be discussed in the next section.) Examination 18 months later revealed an increased number of flavimaculatus lesions but no change in the density or outline of those seen on the first examination.
CASE 12 (Group II, with atrophie macular lesion) A boy, aged seven years, had his poor vision
discovered in school. Right and left visions were 20/80. Fundus examination showed the midperipheries in both eye to be covered with deep yellowish flecks, mostly confluent into the sand-dune pattern. The macular areas had a granular appearance with irregular macular and foveal reflexes.
The parents had no ocular complaints, However, a younger brother had extensive bilateral retinoschisis of the temporal retina, marked left typus inversus of the optic nerve and retinal vessels
and an ectopic left macula, which was closer to the disc, higher than normal and showed incipient hole formation. His corrected right vision was 10/200 and left vision 20/70. An older brother, 11 years, has congenital glaucoma. CASE 13 (Group II, atrophie macular lesion)
A boy, aged 10 years, noted diminution of vision for the past year and one half. Right and left vision were 20/200. On fundus examination, the midperipheries were peppered with deep yellowish dots, mostly in small groups and short rows, some showing confluence into the sand-dune pattern. The paramacular regions were almost free of flecks, the maculas were occupied by inconspicuous lesions with fine overlying pigment dust.
CASE 14 (Group II, atrophie macular lesion) A woman, aged 34 years, had right and left
vision of 20/200. The midperiphery and paramacular region in both fundi were covered with partly isolated, very opaque pisciform lesions and partly confluent flecks with definite but soft borders, which formed a sand-dune pattern in many places. The maculas were occupied by well-defined areas of pigment rarefication and pigment clumping. During a three-year period of observation, there were no obvious changes in the fundi; however, detailed comparison of fundus photographs was not done. CASE IS (Group II, with atrophie macular lesion)
A man, aged 32 years, had noted marked diminution of vision over the past five years. Right and left visions were 7/200. The periphery and midperiphery in both fundi revealed dense accumulations of deep yellowish flecks, mostly confluent into a sand-dune pattern. When first examined, the macular regions showed a peculiar golden-green metallic sheen through which no choroidal pattern was visible. A year later, the atrophie macular lesions had expanded, there was much irregular pigment clumping and the pattern of large choroidal vessels was evident.
CASE 16 (Group II, atrophie lesion in left macula, confluent flavimaculatus lesions in right macula) A woman, aged 42 years, had poor left vision,
discovered five months ago, and some recent difficulty with right vision. Right vision was 20/2S, left vision 20/200. Deep-seated yellow lesions, some pisciform, some round, were rather evenly scattered over the midperiphery of both fundi. The variability in the intensity of opacifica-tion of the lesions was especially noteworthy. The isolated ones were deeply yellow in their centers, but the confluent lesions in the paramacular region were of lesser but uniform opacification. All were softly contoured. In the foveal and parafoveal areas the flecks were at the same deep level but became very tiny and closely packed. The left foveal region showed an additional well-defined area of pigment atrophy and migration.

10 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
CASE 17 (Group II, incipient atrophie macular le-,sion) A man, aged 40 years, had right and left vi
sions of 20/20 and no visual complaints. The midperipheries and posterior polar regions in both fundi were studded with deep, mostly round, yellowish flecks with soft contours and no tendency for confluence. In the macular regions, there were eccentrically located discrete reddish areas with jagged outlines, suggesting beginning pigmentary atrophy.
CASE 18 (Group II, confluent flavimaculatus flecks in the right macula, hypertrophie disci-form lesion in the left) A woman, aged 45 years, had had poorer left
vision than right for many years, but marked diminution for the past year. Right vision was 20/20-2, left vision 20/60.
Deep yellowish flecks, mostly isolated in the midperipheries, and confluent into the sand-dune pattern in the paramacular areas, were noted in both eyes. The right macular area was occupied by confluent yellowish flecks with some overlying dusty pigmentation, the left macula by a coarser lesion consisting of a slightly elevated grayish ring and pigment clumps. A small deep hemorrhage was lying on the nasal slope of this fibrotic area. The patient was re-examined after four years and new lesions were seen but some of the older ones were now very inconspicuous.
A brother is red-green blind and has early macular degeneration with very small drusen in one eye.
CASE 19 (Group I, pure form A) A man, aged 60 years, had had no visual
difficulties until a blow on left eye, which resulted in a horse-shoe tear in situ in the upper temporal periphery. This was successfully repaired by diathermy and a buckling procedure. Right vision was 20/20, left vision 20/25. Deep-seated yellowish flecks, partly confluent into a sand dune pattern, partly pisciform, were scattered over the midperipheries in both eyes, encroaching upon the macular areas where their size became somewhat smaller. A few fine pigment flecks were noted in the left macula.
CASE 20 (Group I, pure form A)
A man, aged 50 years, had no visual complaints. Right vision was 20/20, left vision 20/30. There was a sparse scattering over mid-peripheries and posterior polar regions of both eyes of large, deep, mostly pisciform yellowish flecks. In the left eye, they encroached upon the foveal area without occupying it. A larger flat yellowish area at the same deep level was close to the right fovea from which fine inconspicuous pigment lines radiated for a short distance into the adjacent retina. A few of the parafoveal flecks in the left fundus showed a central speck of pigment
CASE 21
See histopathologic study for details.
CASE 22 (Group I, pure form A) A man, aged 63 years, had no visual com
plaints except need for reading lenses. Corrected right and left visions were 20/20. Deep-seated yellowish flecks, mostly pisciform, were scattered over both posterior polar regions. They were larger and spaced farther apart in the midperipheries, smaller and denser in the macular regions without involving the foveal areas. Some of the larger lesions had dirty gray centers.
During a prior examination seven years ago, the description of the fundi was essentially the same; however, detailed comparison by fundus photographs was not done.
The macular damage in the five following patients was due to confluence of typical "flavimaculatus" lesions.
CASE 23 (Group I, pure form B) A man, aged 19 years, had had visual difficulties
for the past five years. Right vision was 20/200 and left vision 20/70. Deep, isolated yellowish flecks, mostly of the pisciform type, were scattered over the midperipheries and paramacular areas, becoming more confluent and less opaque in the former and in the perifoveal regions. Fluorescein studies showed an increase in the number of flecks, especially in the less conspicuous confluent lesions of the midperipheral and perifoveal zones.
CASE 24 (Group I, pure form B) A white woman, aged 28 years, first noted
failure of left vision six years ago and recently diminution of right vision. Most marked failure of vision occurred at the time of pregnancy. Right vision was 20/30, left vision 20/80. The midperiphery and posterior polar region were covered with deep, yellowish flecks in a confluent sand-dune pattern with an occasional dustlike pigment spot. Confluence was so pronounced in certain areas, particularly in the paramacular regions, that it was reminiscent of the "discoloration in Oguchi's disease. The foveal areas were also occupied by deep-seated confluent yellowish flecks.
CASE 25 (Group I, pure form B) A man, aged 21 years, first noted poor vision
at the age of eight years. Right vision was 20/300, left vision 20/200. Softly contoured, yellowish flecks, most of them confluent into the sand-dune pattern, covered the midperipheries. More opaque isolated pisciform lesions were encountered in the farther peripheries, while the posterior polar regions, with exception of the foveal areas, were almost free of flecks. Round yellow areas with some overlying dusty pigmentation, seemingly due to confluence of typical flavimaculatus lesions, occupied the foveas.

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 11
CASE 26 (Group I, pure form B) A woman, aged 21 years, had right vision of
20/70, left vision 20/30. There was almost even distribution of pisciform lesions and round flecks in short rows over the midperipheries (fig. 9). Garlands of similar spots encircled the upper circumference of both foveal regions, encroaching upon the center from above. Fluorescein studies showed many more lesions, with pronounced fluorescence in the ophthalmoscopically less conspicuous confluent flecks, with faint or no fluorescence in areas occupied by isolated ophthalmoscopically conspicuous, more opaque lesions (fig. 10).
A 27-year old brother was said, by another ophthalmologist, to have the same retinal disease as his sister. CASE 27 (Group I, pure form B)
A white man, aged 39 years, first noted failing left vision seven years ago. Right vision was 20/25, left vision 20/80. Deep yellowish white lesions of varying size and configuration and soft outlines were scattered over both posterior polar regions and midperipheries. Their individual shapes were round, oval and linear, the last predominating. Flavimaculatus lesions encroached upon both foveal regions, with greater involvement of the left macula. Fluorescein studies showed more fluorescent areas than ophthalmoscopic lesions.
R E T I N A L FUNCTION EVALUATION
1. METHOD Visual fields, usually with the Goldmann
perimeter, and some color-vision studies were done in all subjects. Subjective dark-adaptation studies were done in 23, ERG studies in 24 and electro-oculograms in 18 subjects (table 1).
Color-vision tests included the Hardy-Rand-Rittler and Ishihara pseudoisochro-matic plates, the Farnsworth-Munsell (F-M) 100 hue test, the Nagel anomaloscope and the Sloan achromatopia test, where indicated. These tests were administered in the usual fashion. Full details of the an-omaloscopic examination are described elsewhere.17
Dark adaptation was tested with a Gold-mann-Weekers adaptometer as previously described.17 A one-degree white test target was routinely used in the superior meridian 15 and 25 degrees from the fovea. Subjects were tested for at least 50 and in some cases up to 80 minutes.
Fig. 9. (Klien and Krill). Case 28. A woman, aged 21 years. Right eye. Right vision 20/70. Almost even distribution of pisciform lesions and round flecks in short rows in midperiphery and paramacular regions. Garlands of small flavimaculatus lesions encroach upon fovea from above.
The ERG evaluation included single flash and flicker studies. The setup, details of the examination, the parameters evaluated, and the normal values are all discussed in other publications.14·18·19
Fig. 10. (Klien and Krill). Case 28. Same eye as in Figure 9 after intravenous fluorescein, venous phase. Faint or no fluorescence in conspicuous, more isolated lesions of Figure 9 inferior and temporal to macula (arrow), marked prolonged fluorescence and slightly increased number of flecks in areas of confluent lesions less conspicuous in white light

12 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
The EOG was evaluated both in the light-and dark-adapted state, as described elsewhere.14'19 The evaluation consisted of comparing the ratio of the maximum light-adapted to the minimum dark-adapted response with the same ratios obtained from normal controls.
An abnormal value for any test was outside of the range of the normal mean plus or minus two standard deviations.
2. RESULTS
Peripheral visual fields were normal in all patients. Central scotomas were noted in eyes with severe macular involvement due either to macular degeneration or direct invasion of the foveal region with flavimacu-latus lesions. In some patients confluent para-foveal flavimaculatus lesions produced para-central scotomas in one or both eyes. (Cases 19, 20, 21, 24, 26 and 27) with little or no impairment of acuity.
All subjects with macular abnormalities had varying red-green color-vision defects. The more severe cases also had blue-yellow defects demonstrable on the 100 hue test. Case 11, thought to be totally color blind, missed most pseudoisochromatic plates, made errors over the entire range of the 100 hue test, made brightness and color matches over the entire Nagel anomaloscope, and showed typical responses of a total colorblind subject on the Sloan achromatopia test.
Twenty-two of the 23 patients tested had a dark-adaptation abnormality, usually mild in degree (table 1). Slower than normal dark adaptation with normal final thresholds was found in 18 patients. Cone thresholds, rod-cone break times and rod thresholds (some or all) were delayed (table 1). Five patients showed elevated thresholds (even after 80 minutes in the dark). In four (Cases 4, 6, 12 and 17) the elevations were less than one log unit (mild in degree) but in Case 3 an elevation of almost three log units was noted.
Twenty of the 24 patients tested had an abnormal ERG. In 17 patients this was only a mild abnormality and consisted of a delay in reaching a normal maximum b-wave amplitude (table 1). Two patients (Cases 3 and 12) had subnormal responses at all intensities even after 45 minutes in the dark. Case 11 (total color blindness) had no pho-topic responses, a flicker fusion frequency of four cycles per second, an absence of the first portion of a scotopic red-light response and showed a delay in reaching a maximum b-wave amplitude. The scotopic b-wave amplitudes from all patients (except Case 11) obtained at different times in the dark with one intensity were compared with the same data from a control group of 25 subjects (average age 30 years). A two-sample stu-dent-t statistic was used and significant differences were noted for all responses up to 16 minutes in the dark (the patients' b-waves were smaller up to then). At 20 minutes the average normal and patient b-wave data overlapped (see fig. 8 in ref. 14 for a plot of such calculations).
The electro-oculogram was abnormal in 14 of 18 patients studied (table 1). A plot of the ratios from one or both eyes of these 18 patients is shown in Figure 11.
Follow-up functional studies were done at two- to nine-year intervals in nine patients (Cases 1-4, 11, 18, 21, 23 and 26). Peripheral visual fields, repeated in all patients, were always normal. Electroretinograms, repeated in seven, showed changes in only one patient (Case 3) . An average b-wave amplitude decrease of 100 microvolts (comparing four intensities) was noted, although no deterioration of subjective dark-adaptation was found. Furthermore, her sister (Case 1), tested at eight-year intervals, and her father (Case 2) , tested at nine-year intervals, showed no change in the ERG. Dark-adaptation, repeated in seven subjects, and electro-oculograms, repeated in five, showed no significant changes. Table 2 shows original and repeat data obtained

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 13
Φ CO c o ct CO Φ or ■o Φ
^ v
o. σ "O < 1
σ -1 E 3 E X σ 2
Φ CO c o o. CO Φ tr "O Φ
^ w Q. O
■Ö < 1
o Q E 3 E c 2
3.5
3.0
2.0
1.5
/ / / / / / t / / / _ / / / Normal Mean / / ·/ / / / ± 2 S.D.· / / //////U/.//
• · • ·
• · · · • · · ·
— · • · · ·
•
" · One Eye of Patient
V/A •
• •
• ·
• •
0.5 Fig. 11 (Klien and Krill). Electro-oculogram ratios from 18 patients (33 eyes). The ratios from 14 pa
tients (25 eyes) were abnormal. Ratios from four patients (eight eyes) were normal.
with identical techniques for dark-adaptation from six subjects and for the EOG from five subjects.
HISTOPATHOLOGIC EVALUATION (Case 21)
HISTORY AND CLINICAL FINDINGS
A man, 19 years at the time of the first examination.
Right eye. Two corneal lacerations, one with iris prolapse, were received during an automobile accident. There was injury to and dislocation of the lens. Right vision was light perception with correct projection. There was gradual absorption of the lens during the following eight months, permitting a view of the superior fundus after that time. Examination revealed an extensive choroidal rupture above the optic disc. Intermittent attacks of pain from secondary glaucoma during the subsequent three years were initially relieved by posterior sclerec-
tomy with scierai cautery and iridectomy. However, during the next three years the ocular tension varied between 25 and 50 mm Hg (Schlitz) and, at the end of this period, uncontrollable pain necessitated enucleation of the right eye.
Left eye. Left vision was 20/25, J l . Refraction was: -0 .25D sph C +0.75D cyl ax 90°. No abnormalities were initially noted. On follow-up four years later, however, lesions were discovered in the eye-ground. The posterior polar region, macular and perimacular areas were sprinkled with mostly isolated round or pisciform, deep, yellowish flecks with definite but soft contours. Confluence of some had produced a sand-dune pattern around the foveal area, encroaching upon it but leaving a small oval area apparently uninvolved.
Subjective dark adaptation at that time showed a definite delay in the times of the cone threshold, rod-cone break, and final

14 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
Case Date
TABLE 2 EVALUATION OF RETINAL FUNCTION
Dark Adaptation
CT RCB RT FT EOG
Ratio*
4
11
18
21
23
26
9/64 12/66 7/64
12/66 12/63 12/66 11/64 12/66 2/63 1/67
12/64 1/67
S 3.
10 10 13 10 6 6 7 6
10 10
16 14 16 17 30 25 15 16 15 15 15 15
55 53 67 63 62 58 45 47 51 55 30 35
1.6X103 1.3X108 5.9X10» 6.5x10s 3.2X10» 3.4X10» 3.3X10« 2.5X10' 4.6X10» 3.9X10» 4.2X10» 9.0X10»
1.6 1.4 1.8 1.8 2.7 2.5 — —
1.6 1.6 —
1.5 1.5 1.7 1.7 2.2 2.3 2.2 2.2 1.8 1.6 —
CT—time ofcone threshold; RT—time of rod threshold; RCB—time of rod-cone break; FT—-value of final threshold in arbitrary units
* Maximum light-adapted response Minimum dark-adapted response
Fig. 12 (Klien and Krill). Case 21. A man, aged 23 years. Left eye. Left vision 20/25, J l . Note approximately square area between vessels above macula (arrow), which contains only one conspicuous flavimaculatus lesion; nasally and above this square a group of isolated flecks. Fo-veal region spared.
rod threshold (table 1). The ERG and EOG were normal. Color-vision tests showed an equation on the Nagel anomalo-scope displaced toward the red end, and 381 errors on the F-M 100 hue test, with no definite axis.
Fundus photographs taken two years apart were compared after a recent re-ex
amination. The recent picture showed many more flavimaculatus lesions (fig. 13). An area for area comparison revealed isolated pisciform lesions in places where no obvious flecks existed two years before, and confluent patterns where isolated lesions prevailed in the early photograph (fig. 12). Fluorescein studies done at the time of the
Fig. 13 (Klien and Krill). Case 21. Same eye as in Figure 12, two years later. Flavimaculatus lesions appear more numerous. Square area noted in Figure 12 now contains several isolated, quite opaque flecks ; area nasally and above it now shows greater confluence of lesions. Vision still 20/25, J l .

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 15
second fundus photographs, showed minimal or no fluorescence of the newer pisci-form lesions and marked fluorescence in the areas of less conspicuous confluent patterns (fig. 14).
Recent ERG, EOG and dark-adaptation tests showed no significant changes from those done two years ago. (See Table 2 for details of past and recent dark-adaptation and EOG studies.)
GROSS DESCRIPTION OF THE ENUCLEATED RIGHT EYE
The globe measured 25.0 by 24.5 by 24.5 mm. There was a corneal leukoma in the inferior temporal quadrant with the pupil drawn toward it. A bluish scierai ectasia was noted two mm behind the upper limbus. The eye was opened in the horizontal plane with large superior and inferior calottes. In the posterior segment, a glaucomatous excavation of the optic nerve and a 1.0 by 2.0 papillary diameter sized pigmented macular scar with a yellowish rim and an arcuate extension into the suprapapillary region were noted. There was a narrow zone of grossly visible pigment rarefication and proliferation anterior to the equator, more pronounced in the upper half. Between it and the obvious macular scar, the fundus appeared grossly normal. The retina was in situ. The main part and the inferior calotte were embedded in paraffin and serial sections were made. Series of 20 or more adjacent sctions were stained with hematoxylin-eosin, alcian blue, PAS, after Fontana for premelanin, and after Rinehard-Haj for acid-mucopolysaccharides. Grossly normal appearing portions of the upper calotte were used for flat preparations of retina and choroid.
HlSTOPATHOLOGIC FINDINGS
The anterior segment showed the healed penetrating wound, almost complete closure of the chamber angle by anterior peripheral synechiae, and capsular and cortical lens remnants. There were delicate strands of
Fig. 14 (Klien and Krill). Case 21. Same eye as in Figure 12 at the same time after intravenous fluorescein, venous phase. Increase in the number of lesions in general. Isolated flecks in square area noted in Figure 13 show weak or no fluorescence; in area of confluent lesions nasally and above it, the number of lesions appears increased by fluorescence.
proliferated nonpigmented ciliary epithelium running forward to the remnants of the lens. Portions of the oral retina were distorted and displaced forward as if under traction. There was no evidence of an in-travitam retinal separation.
There was a pronounced glaucomatous excavation of the optic nerve and a corresponding atrophy of the ganglion-cell layer. Aside from the areas of healed choroidal ruptures, the remainder of the retina was well preserved. Scars after a deep choroidal rupture were running through the macula to the region above the optic papilla. In these places choroidal stroma and the outer half of the retina were replaced by masses of hy-alinized fibrous tissue and proliferated pigment epithelium. A second less extensive partial choroidal rupture had resulted in similar scarring concentric with and nasally to the first. Elsewhere, Bruch's membrane, choriocapillaris and remaining choroid were normal.
A narrow zone anterior to the equator showed chorioretinal adhesions with knob-

16 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
like proliferations of the pigment epithelium and marked retinal gliosis. From the equatorial region backward there was a zone, varying in width, of normal-appearing pigment epithelium with even distribution of pigment granules and basally placed nuclei. From this zone backward, a gradual transition into the pathologic manifestations to be discussed in detail was noted.
The following observations on the pigment epithelium were made in the nasal near-periphery and the temporal midperi-phery of the main part of the eye, and in the midperiphery of the inferior calotte. The morphologic changes of the pigment epithelium were immediately evident; other alterations of this layer were brought out by special stains.
I. Altered morphologic characteristics were:
1. A displacement of the nucleus from the base of the cell toward the center or inner surface (fig. 15-a).
2. A peculiar line of condensation of pigment granules in the center or near the inner surface of the cell, frequently at the level of the displaced nucleus (fig. 15-b and d).
3. Accumulations of a pathologic substance, largely within the inner half of the cell, in circumscribed areas (fig. 15-a, b and d) .
4. Great variations in the size of the cells, some much larger than normal, others small, without pigment granules or discernible nuclei (fig. 15-b and d) .
There was a gradual transition from the morphologically normal-appearing pigment epithelium behind the equator into a region where the cells still had basically placed nuclei, but a beginning line of pigment condensation. Next in the sequence of changes was an increasingly frequent inward displacement of nuclei and, finally, pathologic material appeared in the inner half of some cells. In the most proximal zone variations in the size of the cells were most pronounced.
The deposits of pathologic material were largest in the midperiphery (fig. 15-1 and f ) . There appeared to be a tendency for confluence of these accumulations, the lateral cell borders becoming indistinct, while the apical cell membrane remained well defined, leaving no doubt that the material was intra-cellular. In most places, this substance had a meshlike pattern, which became accentuated with some special stains. In one place only, some of this material was lying in the subret-inal space; this place, however, was very near the scar from the choroidal rupture, and traction upon this whole area was evident. Thus, rupture of the pigment epithelial cells filled with the abnormal material probably does not represent the natural course of this change.
While these deposits occupied conspicuously the inner half of the cell, some of this material was also found near the base (fig. 15-e), leaving the site of its elaboration within the cell uncertain. Indeed, the displacement of nuclei inward, the line of condensation of pigment granules near center or apex, and the accumulations of pathologic material in the innermost aspects of the cell were suggestive of a dynamic force moving inward from the base.
II. Special stains: 1. PAS. Two distinctive features were
noted with this procedure : a. All of the cells were packed with
PAS-positive granules, rendering the pigment epithelium very conspicuous compared to its appearance in sections stained with other methods, where it was less noticeable than normal due to its reduced pigment content (compare fig. 15-b and c) .
b. Round or oval conglomerations of coarse PAS-positive granules were found within many cells, usually between basement membrane and displaced nucleus (fig. 15-e).
Bruch's membrane was normal. No dru-sen formation was noted anywhere.
The flat preparation of the choroid, stained with hematoxylin and PAS, showed

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 17
VwA?·**
Fig. 16 (Klien and Krill). Section near that shown in Figure 15-E. Granules of premelanin densest around ball-like conglomerations show prominently by PAS in Figure 1S-E. (Fontana stain X630).
deeply purple islands of pigment epithelium still attached to the processed choroid, indicating staining properties identical with those shown in the meridional sections. The flat preparation of the retina was normal.
2. Fontana stain. Behind the line of pigment condensation and in otherwise pigment-free cells numerous dark granules appeared, indicating the presence of chromo-genic substance (figs. 15-e and 16).
3. Alcian blue stain. Two important features were shown by this method :
a. A completely intact layer of acid mu-copolysaccharides lining the outer surface of the neuroepithelium, even over the most markedly altered pigment epithelium (fig. 15-d), and
b. Alcian blue positive material in the meshes of the pathologic intracellular substance. Since our routine stain is done with a pH of 2.5, this indicated the presence of a weakly sulfated acid mucopolysaccharide, such as hyaluronic or scialic acid.
4. AMP stain after Rinehart Haj. Pattern and distribution of the pathologically elaborated material was best demonstrated by this method. The content of its fine meshwork stained deeply blue. Here and there, confluence of the fine blue globules into larger oval or round bodies was ob
served. Pretreatment of sections with hyalu-ronidase completely removed the blue staining material from the meshwork, indicating that the substance elaborated by the pathologically altered pigment epithelial cells was mostly hyaluronic acid (fig. 15-f).
Most alterations of the pigment epithelium were diffuse and not always associated with accumulations of abnormal substance. There was no proof that some of the areas with most marked cellular alteration, as indicated by abnormal sizes, displacement or loss of nuclei, and changes in pigmentation (features which were present in all affected cells to a greater or lesser degree) were actually preceded by elaboration of pathologic material, although this is a possibility.
The clinical photograph of the fundus of the fellow eye showed the older flavimacula-tus lesions in the posterior polar region, and more of the early isolated pisciform areas in the intermediary periphery (figs. 12 and 13). Since the clinical pattern of distribution of the lesions has proved to be similar in the two eyes in all patients, the conclusion that the regions showing the greatest accumulations of abnormal material, found in the intermediary periphery in this eye, represented the fresher lesions might be justified.
Speculating that these areas actually

18 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
TABLE 3 SIZES OF SIX LESIONS WITH PATHOLOGIC DEPOSITS
Width
1. Lesion 2. Lesion 3. Lesion 4. Lesion 5. Lesion
6. Lesion
Distal
200 μ 280 μ 160 μ 400 μ
200 μ
Central
240 M 460 μ 640 μ 150 μ 240 μ
680 μ
Proximal
320 μ
300 μ 720 μ
280 μ
Length
240 μ + 800 μ + 600 μ + 800 μ + 800 Μ+ +
800 μ +
Shape
Round Pisciform Oval or short pisciform Pisciform Hour glass·—2 pisciform
end to end? Pisciform
might represent the clinically visible yellow pisciform or round isolated flecks, measurements of approximate length and width of a few of these lesions were carried out. One small area and a group of five large lesions, all in the nasal midperiphery, were measured. Clear guide marks, such as cross sections of intrascleral nerves or vessels, were used to identify the same lesion in a sequence of sections.
The smallest lesion measured, 240 microns wide, could be followed through about 30 sections, 8.0 microns thick, thus indicating an approximately round shape. The large areas were followed through 100 sections, with measurements taken in the beginning, approximate center, and at the end of this sequence. Three of them had an elongated shape, wider at one end, suggesting fish-tail configuration. One of them turned out to be narrow in the center and broad at the first and last section measured, neither of the end measurements representing even approximately the termination of the lesion, giving the impression of linear forms joined together in their axial direction (table 3) .
Most of the measured values of a width and a length of 800 microns or more assure the clinical visibility of these areas, and their shapes support the view that they probably represent the clinically visible isolated, early flavimaculatus lesion.
DISCUSSION
There appeared to be two basic forms of fundus flavimaculatus. One form showed
only the characteristic flavimaculatus flecks, while in the other there were associated macular lesions, mostly of the atrophie type. Visual acuity, however, was also impaired in some patients with the pure form due to direct invasion of the foveal region with typical flavimaculatus lesions. The macular involvement was then incidental and marked differences in acuity between the two eyes were noted, reflecting asymmetrical or unilateral foveal damage.
The form combined with macular degeneration appeared to be more common in our material (18 of 27 patients). In this form the macular involvement was more symmetrical, the visual impairment more marked, and the chance of further visual loss greater.
The macular abnormality in this latter group may precede the appearance of visible flavimaculatus lesions. This was suggested by the bilateral loss of central vision in the six-year-old son and nephew, respectively, of two patients with typical fundus flavimaculatus (Cases 4 and 5) in whom an early atrophie macular degeneration but no visible flavimaculatus lesion could be demonstrated. An early fundus flavimaculatus was suspected in this child because of the existence of a typical dark-adaptation abnormality (marked delay but close to normal thresholds) in addition to the early macular lesion and the family history. In general, it may well be that a basic widespread functional disturbance, perhaps congenital in origin, precedes both the macular degeneration and the appearance of flavimaculatus lesions.
VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 19
The congenital nature of a basic defect is also suggested by the early onset of symptoms in most patients. There is a strong possibility that such a defect is genetic in orgin as suggested by the high incidence of familial occurrence in our series (10 of 27 patients). There was a likelihood of autoso-mal dominant inheritance in two families (Cases 1-5) with definite and probable involvement of members in two generations without known consanguinity. On the other hand, the sporadic occurrence of the disease in most patients and observations on other pedigrees* suggest that autosomal recessive inheritance is probably the most frequent mode of transmission. The place of the mac-ular degeneration in the genetic picture of the disease is obscure.
The flavimaculatus lesions were not stable; this might not have been obvious, however, without detailed photographic comparisons. Changes ίη size, color and outline of old lesions and the appearance of new lesions were evident on follow-up. An increase in the number of lesions was particularly noticeable on follow-up fluorescein studies (figs. 4 and 6) . In general, flecks observed at an earlier stage are more opaque, have medium soft borders and tend to remain isolated for some time, whether round or pisciform in shape. They give the impression of greater thickness in their central portions which could be an optical illusion caused by the greater opacification in this region. Eventually these lesions become less opaque, have softer borders and less striking shapes, and tend to become confluent into geographic maplike or sand-dune patterns. In general, areas of old lesions have a more faded appearance.
Fluorescein studies showed fluorescent spots which were initially seen in the arterial phase and persisted beyond the venous phase without changes in size, indicating an increased visibility of choroidal flow due to defective pigment epithelium rather than extravasation of dye. It was noteworthy that fresher lesions showed minimal or no fluorescence. An 11-year-old patient with
mostly discrete opaque flecks (Case 6) did not initially show any fluorescence but 12 months later (when many confluent areas were present) multiple fluorescent spots were observed (figs. 7 and 8 ) . These findings suggest that, in the earlier stages, the yellow color of the typical lesion is not associated with destruction or atrophy of the pigment epithelium, even though the basic changes occur in this layer. On the other hand, fluorescence was pronounced in older lesions (in this patient as well as in all the others studied), revealing many additional spots indicative of a more widespread damage to the pigment epithelium in the ophthalmoscopically less conspicuous areas.
Fluorescein angiography also reveals features which aid in the distinction of this condition from drusen. The fluorescein shapes of flavimaculatus lesions are irregular, soft and fuzzy, and markedly confluent, while the defects of the pigment epithelium in drusen are well defined and overwhelmingly of round shape, with little tendency for confluence. In our opinion, the clinical diagnosis of fundus flavimaculatus is easy from the ophthalmoscopic appearance of the lesions. Only two conditions come into consideration for differential diagnosis, drusen (Doyne's honeycomb degeneration, malattia Levantinese, Tay-Hutchinson's disease, etc.14) and fundus albipunctatus. Drusen are usually round or oval in shape, of varying sizes, frequently have secondary changes such as calcification, and are often found in the far periphery. They may be confluent into well-defined clover-leaf shapes or multilevel plaques. In fundus albipunctatus the lesions are uniform, dotlike, usually the size of a second order arteriole, and show no confluence. Should difficulties in differential diagnosis exist on the basis of the ophthalmoscopic picture, fluorescein studies will clearly reveal the strikingly distinctive features of fundus flavimaculatus just outlined.
The present histopathologic study of fundus flavimaculatus disclosed a primary abnormality of the pigment epithelium and not a response of this layer to defective adja-

20 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
cent structures. No drusen formation was encountered. Deposition of the pathologic material, an acid mucopolysaccharide, occurred at the inner end of the cell rather than adjacent to Bruch's membrane.
On the basis of microscopic measurements of five circumscribed deposits of this material it was concluded that it probably represents the clinically visible isolated early flavimaculatus lesion. The cells containing this substance are completely intact, thus, the lack of fluorescence of most early clinical flavimaculatus lesions is understandable. Areas of atrophy or involution of the pigment epithelium, on the other hand, may represent the less conspicuous older confluent lesions with increased fluorescence noted clinically. The yellowish color of the clinical lesion has almost certainly a variety of causes; in recent lesions it is probably due to deposits of an opaque substance; in areas of older damage this color is due to loss or disturbance of melanin content.
Considering a possible role of the longstanding glaucoma in the production of some of the morphologic changes enumerated in this histologie study, only the variation in the sizes of the cells offers a remote possibility of such connection. The other changes (the displacement of the nucleus inward, the line of condensation of pigment granules, and the accumulations of pathologic substance in the inner half of the cell in circumscribed areas) were distinctive enough to rule out such cause and effect relationship. In advanced glaucoma, obliteration of the choriocapillaris in circumscribed areas is followed by degenerative change in the pigment epithelium, such as flattening of the cells with loss of pigment, and later degeneration of the neuroepithelium. In the eye under discussion choriocapillaris and neuroepithelium were unusually well preserved in areas of markedly abnormal pigment epithelium.
In this particular eye, the pigment epithelium was normal at and for a short distance posterior to the equator. Since the
characteristic pathologic alterations increased in severity toward the posterior pole, it is possible that prior to the trauma the pigment epithelium anterior to the equator was also normal. A definite conclusion in this regard could not be reached. If, however, this supposition on the amount of normal pigment epithelium were true, one could explain the following clinical findings in the other eye of this patient: (1) the normal ERG and EOG (probably most of the pigment epithelium has to be altered to affect these tests), (2) the mildly abnormal dark adaptation (small area testing was done well within the equator at 15 and 25 degrees where definite alterations of the pigment epithelium in the enucleated eye were noted), and (3) the presence of ophthalmoscopically visible lesions only in the macular area and intermediary midperiphery.
It is probable that in some patients the abnormalities of the pigment epithelium are present over most of its expanse thereby explaining the frequently abnormal ERG and EOG. Even in these patients the most severe involvement may be proximal to the equator since ophthalmoscopically visible lesions are rarely seen anterior to this region. Dark adaptation of a one degree area was always tested in the proximal retina, thus it is understandable that abnormal responses were found in 22 of 23 patients tested.
The normal appearance of the receptor elements adjacent to even markedly altered pigment epithelium explains the absence of major alterations of the ERG and dark adaptation in most patients. On the other hand, markedly altered pigment epithelium probably produces enough functional alteration of the adjacent retina frequently to result in mild abnormalities of dark adaptation and the ERG. Many patients with markedly abnormal electro-oculograms were found, reflecting the important relationship of this test to the integrity of the pigment epithelium.
Other diseases in which a primary abnor-

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 21
mality of the pigment epithelium may exist include fundus albipunctatus, diffuse colloid bodies or drusen, and the vitelliruptive degeneration. Supportive evidence for this view includes :
1. Fluorescein findings in the three conditions. The fluorescence noted in each abnormality is present in the arterial phase and persists beyond the venous phase without changing in size, thus indicating defective pigment epithelium rather than leakage. In vitelliruptive degeneration the macular region shows fluorescence,20 even in young patients with typical egglike lesions. Multiple widespread fluorescent spots are evident in fundus albipunctatus20 and in drusen.15 It may be fallacious to assume that drusen are primarily a disease of Bruch's membrane.
2. Similar retinal function profiles in all of these conditions14·21 (normal visual fields, normal or only mildly abnormal subjective dark adaptation and scotopic electroretino-grams, and often severely abnormal electro-oculograms).
3. Similar course on follow-up. Peripheral function is usually stationary although there are changes in the appearance of the fundus and a progression of associated macular disease.
The combination of ophthalmoscopically visible progression of the disease, sometimes quite marked, without any or only minimal deterioration of peripheral retinal function was shown for nine patients in this study seen at two- to nine-year intervals. This same relationship holds true for drusen,14
most cases of fundus albipunctatus14 and probably for vitelliruptive macular degeneration.
The concept of a primary disease of the pigment epithelium readily explains the fundus picture reported in drusen15·22 after intravenous fluorescein of an "increased number of lesions." This behavior has been interpreted as an additional number of drusen rendered visible by this method. Knowing, however, that histologically even fairly large drusen may be covered by morphologically
normal pigment epithelium, it seems unlikely to have an additional number of smaller drusen with overlying defects of the pigment epithelium revealed by fluorescence. In our opinion, this phenomenon is due to increased visibility of defects in the epithelium under fluorescein, not necessarily at the site of drusen, associated with drusen formation but not caused by it. Similarly, the increased areas of fluorescence at the site of some, seemingly the older lesions in fundus flavimaculatus, indicate a more widespread pathologic condition of the pigment epithelium than is visible in white light.
The diseases of the flecked retina group (fundus flavimaculatus, fundus albipunctatus and drusen) and vitelliruptive macular degeneration are thus probably all primary abnormalities of the pigment epithelium. Primary pigment epithelial disease was demonstrated in this report for fundus flavimaculatus. Histologie studies are still needed from fundus albipunctatus, from the typical early stages of vitelliruptive macular degeneration and more detailed studies would be helpful from drusen. Future histologie investigations of these conditions should particularly focus on the pigment epithelium with careful scrutiny of morphologic changes by light and electron microscopy and histochemical evaluation to search for possible enzymatic defects.
SUMMARY AND CONCLUSIONS
Fundus flavimaculatus is probably a genetic disorder characterized by a primary defect in the pigment epithelium. A definite familial incidence was observed in 10 of 27 patients.
The evolution of the typical flavimaculatus lesion, as revealed by long-term observation and comparison of photographs made in white light and during fluorescein angiog-raphy, was characterized by a transition from conspicuous isolated, markedly opaque, round or pisciform, non- or weakly fluorescent areas into less opaque, confluent sand-dune or garland patterns with pro·

22 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1967
nounced fluorescence and an increased number of fluorescent spots. Additional fresh lesions were always discovered on follow-up.
The pattern of fluorescence in the older flavimaculatus lesion resembled that of a fundus with diffuse drusen in the increase of their number, pointing to more profound disturbances of the pigment epithelium than expected from the ordinary ophthalmoscopic picture in both conditions. Fluorescein an-giography, on the other hand, clearly distinguishes the two entities by emphasizing structural differences between them.
A high incidence of abnormal visual acuity in fundus flavimaculatus is due either to an associated macular degeneration or to an involvement of the fovea by flavimaculatus lesions. The latter has incidental character, with less diminution of visual acuity and with a better visual prognosis.
Characteristic retinal function findings included normal peripheral visual fields, mildly abnormal dark adaptation and elec-troretinograms, and often a severely abnormal electro-oculogram. Retinal function was stationary in eight and only mildy progressive in a ninth patient retested. The total area of pigment epithelium involved probably varies from patient to patient.
Histopathologic examination of an eye with fundus flavimaculatus showed distinctive changes in the pigment epithelium, while the neuroepithelium, Bruch's membrane and choroid were normal. The characteristic early flavimaculatus lesions appear to be produced by deposits of an acid muco-polysaccharide, which is elaborated by groups of malfunctioning pigment epithelial cells.
Clinical, functional and histopathologic findings suggest the concept of a primary abnormality of the pigment epithelium, familial in character, and probably congenital, in fundus flavimaculatus and possibly in drusen, fundus albipunctatus and vitellirup-tive macular degeneration.
ACKNOWLEDGMENT
We wish to thank Dr. Tibor Farkas for his assistance in the preparation and photography of the histologie sections.
REFERENCES
I. Franceschetti, A. : Ueber tapeto-retinale Degenerationen im Kindesalter (Kongenitale Form (Leber), amaurotische Idiotie, rezessive-geschle-chtsgebundene tapeto-retinale Degenerationen, fundus albipunctatus cum hereralopia, fundus flavimaculatus). Dritter Fortbildungskurs der Deutschen Ophthalmologischen Gesellschaft, Hamburg 1962, herausgegeben von Prof. Dr. H. Sautter. In Entwicklung und Fortschritt in der Augenheilkunde Stuttgart, F. Enke, 1963, pp. 197-120.
2. . : La Rétinapathie ponctuée albescente. Bull. Mém. Soc. Franc. Ophtal. 76:14, 1963.
3. Franceschetti, A., François, J. and Babel, J. : Les Héredo-Dégenéréscences (Dégénérescences Tapeto-Rétiniennes). Paris, Masson, 1963, v. 1.
4. Franceschetti, A. and François, J. : Fundus flavimaculatus. Arch. Ophtal. (Paris), 6:505, 1965.
5. Franceschetti, A.: A special form of tape-toretinal degeneration. Tr. Am. Acad. Ophth. Oto-laryn. 69:1048, 1965.
6. Hollwich, F. : Familiäres Auftreten des fundus flavimaculatus. Klin. Mbl. Augenh. 143:817, 1964.
7. Caocci, G. : Contribute alla conoscenza délia degenerazione famigliare délia macula (sindrome di Stargardt). Boll. Ocul. 14:717, 1935.
8. Friemann, W. : Heredodegeneration der Maku-la mit Hyperkinesen. Klin. Mbl. Augenh. 126:460, 1955.
9. Kandori, F. : Upon new cases of congenital nightblindness with fleck retina. Yonago Acta Medica, 4:169, 1960.
10. Kandori, F., Setogawa, T. and Tanoi, A. : Electroretinographical studies on fleck retina with congenital nonprogressive nightblindness. Yonago Acta Medica, 10:98, 1966.
II. Kandori, F., Setogawa, T. and Tamai, A.: ERG of new cases of congenital nightblindness with fleck retina. Jap. J. Ophth. lO(Suppl) :301, 1966.
12. Waardenburg, P. J., Franceschetti, A. and Klein, D. : Genetics and Ophthalmology. Springfield, 111., Thomas, 1963, v. 2.
13. Stargardt, K. : Ueber Familiäre, progressive Degeneration in der Makulagegend des Auges. Graefes Arch. Ophth. 71:534, 1909.
14. Krill, A. E. and Klien, B. A. : Flecked retina syndrome. Arch. Ophth. 74:496, 1965.
15. Ernest, J. T. and Krill, A. E. : Fluorescein studies in fundus flavimaculatus and drusen. Am. J. Ophth. 62:1,1966.
16. Krill, A. E. : ERG in fundus flavimaculatus. Jap. J. Ophth. lO(Suppl) :293, 1966.
17. Krill, A. E. and Beutler, E.: The red light absolute threshold in hétérozygote protan car-

VOL. 64, NO. 1 FUNDUS FLAVIMACULATUS 23
riers: Possible genetic implications. Invest. Ophth. 2:107, 1964.
18. Krill, A. E. and Lee, G. B. : The electroret-inogram in albinos and carriers of the ocular albino trait. Arch. Ophth. 69:32, 1963.
19. Krill, A. E. : The electroretinographic and electrcoculographic findings in patients with mac-ular lesions. Tr. Am. Acad. Ophth. Otolaryn 70:1063,1966.
This paper describes a method of dissolving, emulsifying and aspirating a mature cataract through a two to three mm incision. Until now, only congenital cataracts could be aspirated because of the semifluid consistency of the lens. For the past four years, I have concerned myself with the possibility of transforming the mature cataract into a solution or an emulsion, thereby making aspiration possible.
The methods which come to mind for dissolving or emulsifying a cataract are chemical (enzymatic) and mechanical. Although the enzymatic approach holds some promise, and although I am continuing investigation along these lines, the possibility of finding an agent which will dissolve the lens without affecting other structures of the eye seems remote at this time. The mechanical approach lends itself more easily, at present, to experimentation. Various types of micro-drills, microburrs and microblenders (similar to the Waring blender) have been developed and evaluated but are considered to be either too ineffective, too dangerous, or
From the Cryo-Research Department, Manhattan Eye, Ear and Throat Hospital. The canine surgery was performed at New York Medical College. This investigation is supported by a grant from the John A. Hartford Foundation.
20. : Unpublished observations. . 21. Krill, A. E, Morse, P. A., Potts, A. M.
and Klien, B. A.: Hereditary vitelliruptive macu-lar degeneration. Am. J. Ophth. 61:1405, 1966.
22. Norton, E. W. D., Gass, J. D., Smith, J. L., Curtin, V. T., David, N. J. and Justice, J., Jr.: Symposium: Macular diseases diagnosis. Fluores-cein in the study of macular disease. Tr. Am. Acad. Ophth. Otolaryn. 69:631, 1965.
unworkable. The most promising approach, and the one I have used successfully in animals and on human cadaver eyes, is the phaco-emulsification of a lens, using a low frequency (sonic-ultrasonic) needle combined with controlled irrigation and suction.*
In this preliminary paper, the technical specifications of the instruments will not be discussed because they are being constantly changed in an effort to find a combination of optimum size, stroke and frequency.
The working tip consists of the following (fig. 1) :
1. A central needle with an outside diameter of approximately one mm and with a very slightly tapered point.
2. A protective outer jacket made of Teflon.
3. A flow of water between the outer wall of the needle and the protective sheath.
4. Suction in the interior of the needle. The use of an operating microscope is
mandatory. The needle is made of titanium and certain other inert superhard alloys to withstand the acceleration and deceleration without fragmenting. The tip is connected to
* The phaco-emulsifier was developed in conjunction with Cavitron Corporation.
PHACO-EMULSIFICATION AND ASPIRATION
A NEW TECHNIQUE OF CATARACT REMOVAL
A PRELIMINARY REPORT
CHARLES D. KELMAN, M.D. New York