Embed Size (px)
Citation preview
Gastric ESD in Korea and personal experience
Jun Haeng Lee. Department of Medicine
Sungkyunkwanuniversity School of Medicie, Seoul, Korea
Contents
• Brief history of gastric ESD in Korea
• Outcomes of ESD for EGC
• 환자에게 어떻게 설명할 것인가?
• Technical aspects
• ESD training
Brief history of gastric ESD in Korea
Jun Haeng Lee. Department of Medicine
Sungkyunkwanuniversity School of Medicie, Seoul, Korea
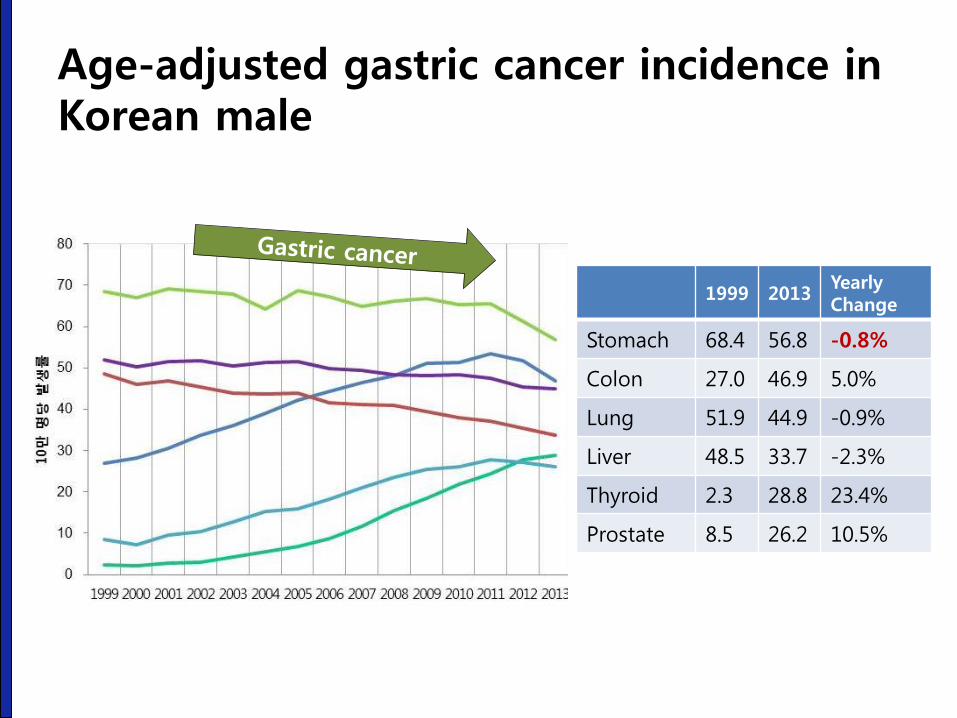
Age-adjusted gastric cancer incidence in Korean male
1999 2013 Yearly Change
Stomach 68.4 56.8 -0.8%
Colon 27.0 46.9 5.0%
Lung 51.9 44.9 -0.9%
Liver 48.5 33.7 -2.3%
Thyroid 2.3 28.8 23.4%
Prostate 8.5 26.2 10.5%
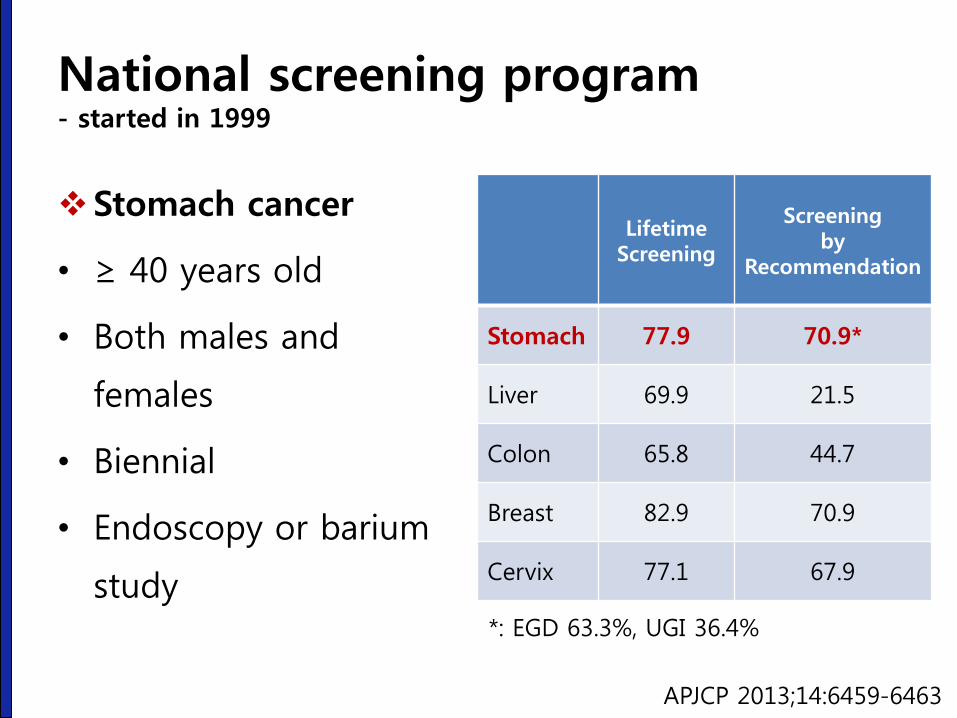
National screening program - started in 1999
Stomach cancer
• ≥ 40 years old
• Both males and
females
• Biennial
• Endoscopy or barium
study
Lifetime Screening
Screening by
Recommendation
Stomach 77.9 70.9*
Liver 69.9 21.5
Colon 65.8 44.7
Breast 82.9 70.9
Cervix 77.1 67.9
APJCP 2013;14:6459-6463
*: EGD 63.3%, UGI 36.4%
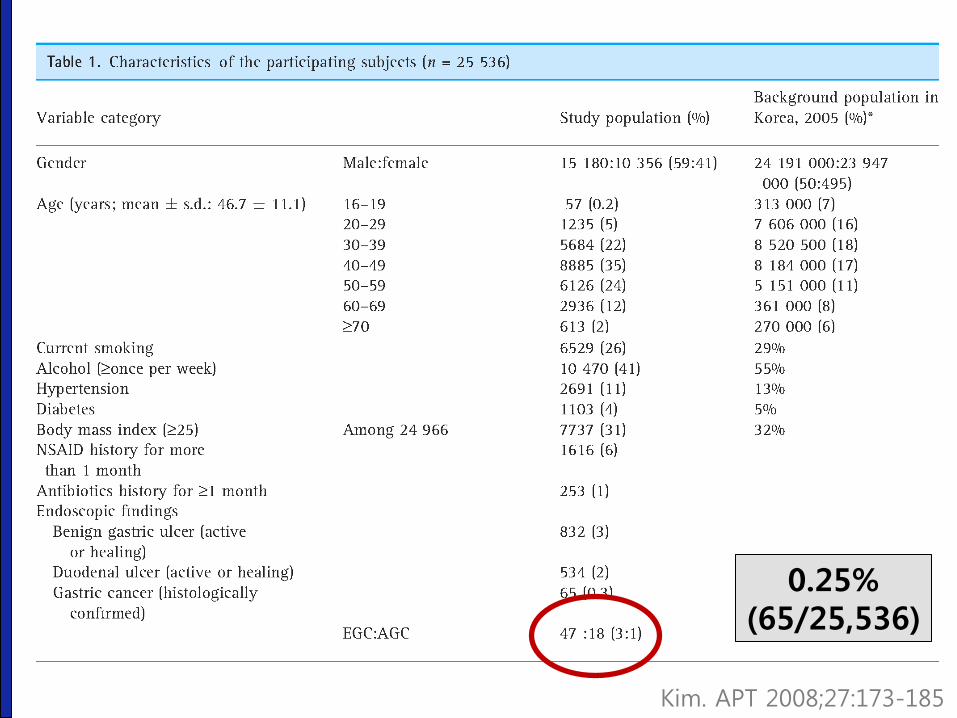
Kim. APT 2008;27:173-185
0.25% (65/25,536)
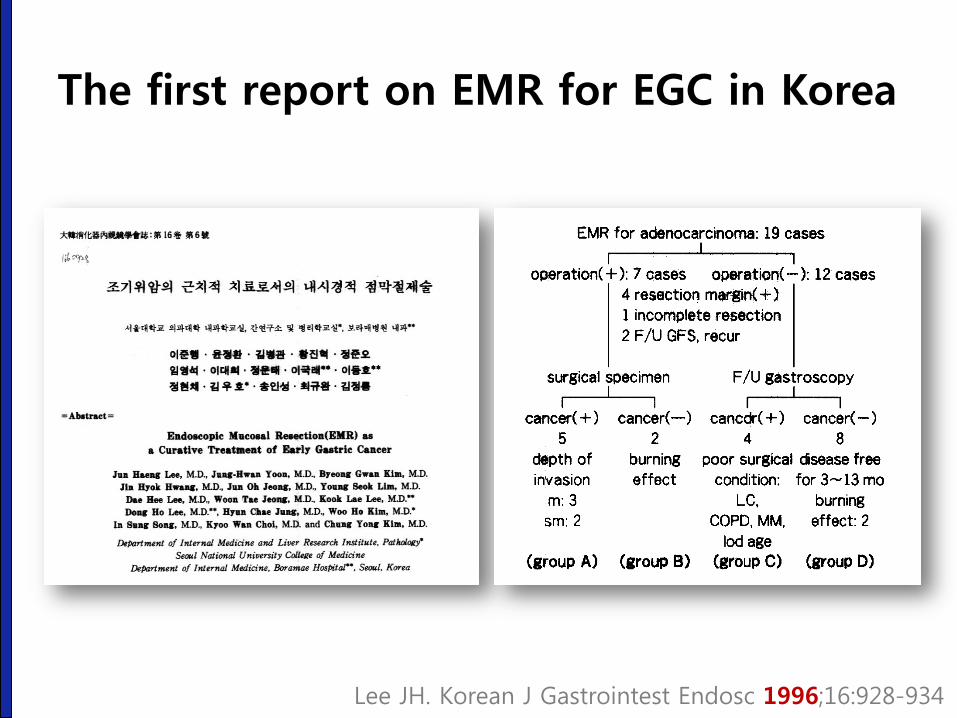
The first report on EMR for EGC in Korea
Lee JH. Korean J Gastrointest Endosc 1996;16:928-934
Symposium and live demonstration
2004 Tokyo
2006 Seoul
Early personal experience of gastric ESD (2005)
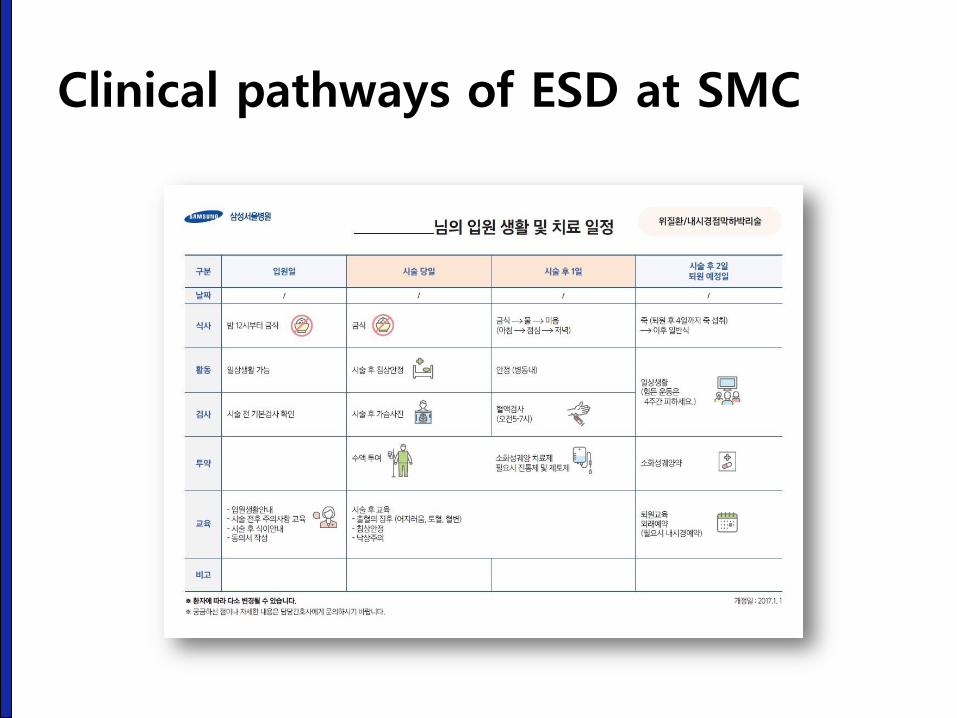
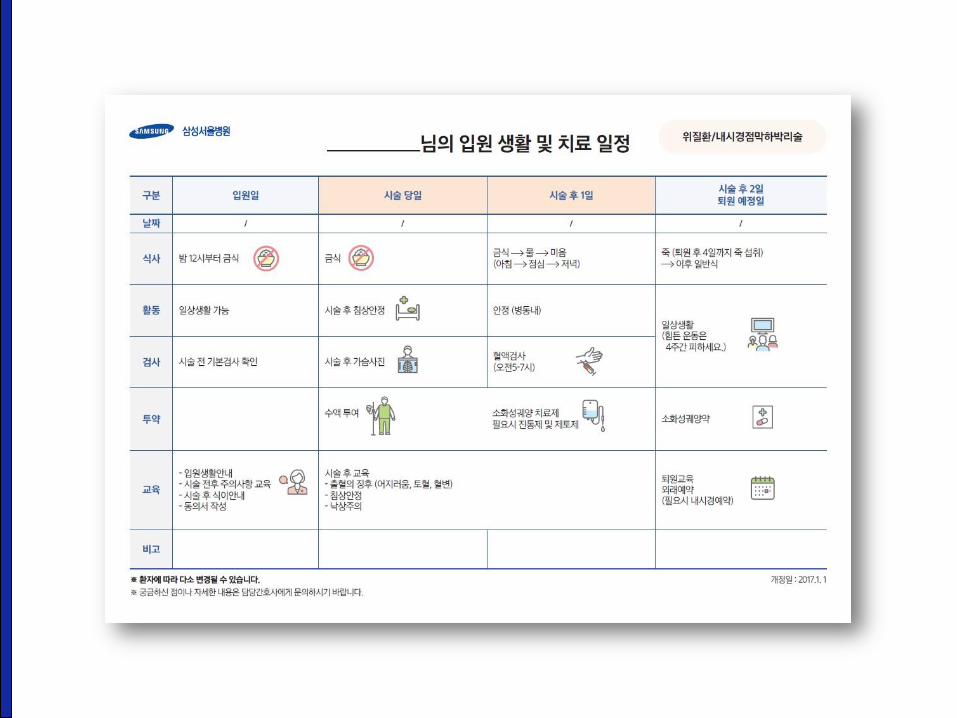
Clinical pathways of ESD at SMC

Insurance coverage for gastric ESD - But, only conventional indications are covered.
http://thestory.chosun.com/site/data/html_dir/2011/09/06/2011090600596.html
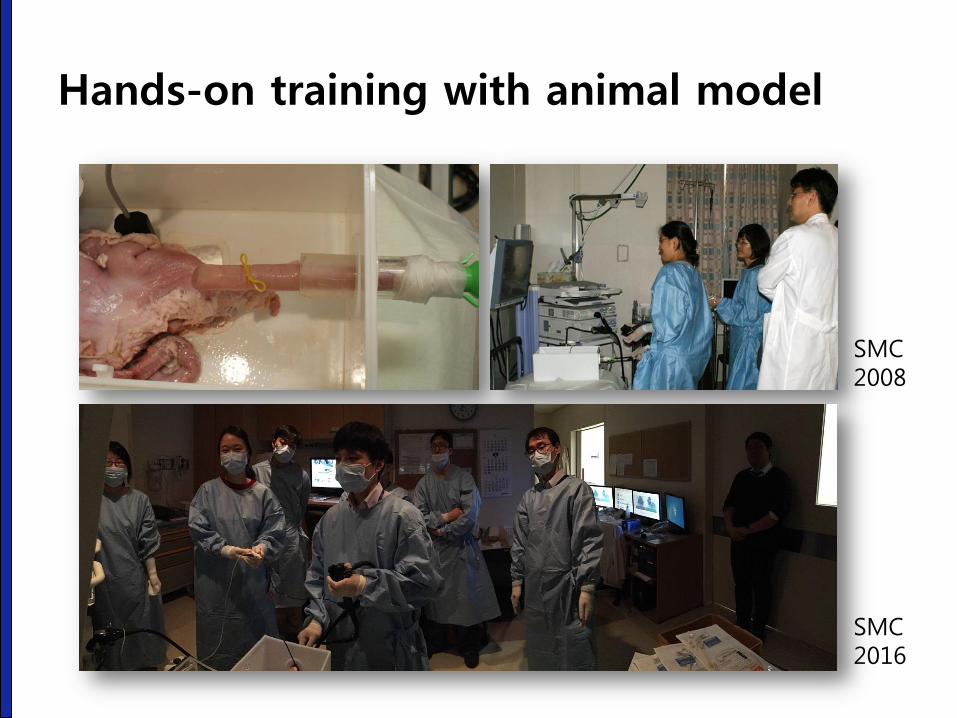
Hands-on training with animal model
SMC 2008
SMC 2016
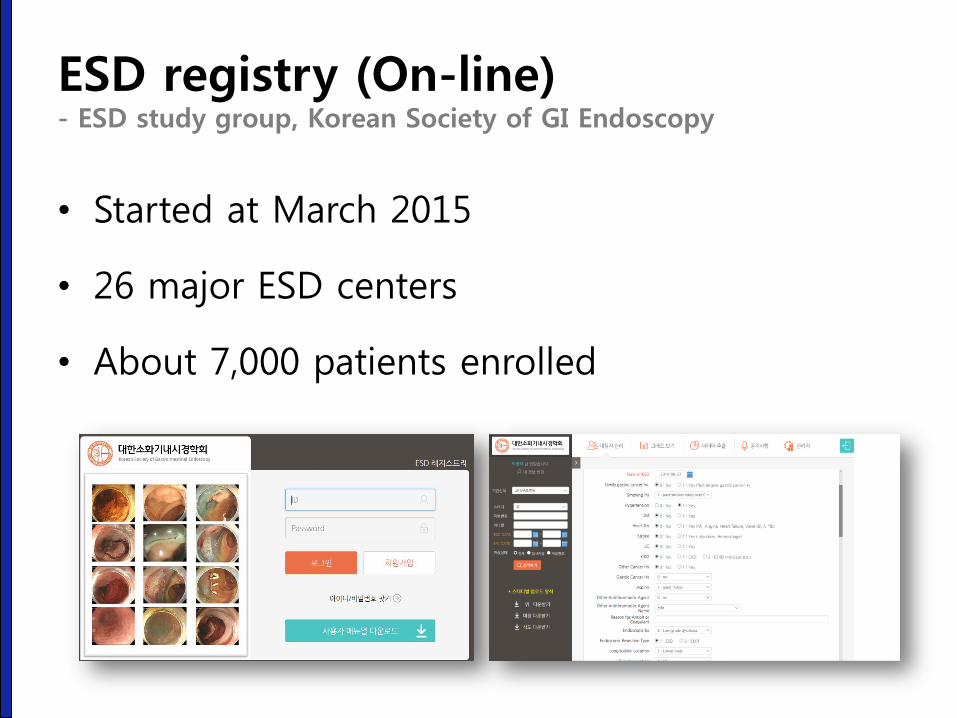
ESD registry (On-line) - ESD study group, Korean Society of GI Endoscopy
• Started at March 2015
• 26 major ESD centers
• About 7,000 patients enrolled
Current status of ESD for EGC in Korea - From Nov 2011 – Dec 2014
• Number of ESD for EGC cases: 23,828
(2012: 6,664 2013:7,499 2014: 7,734)
• Age: 64.9 +/- 9.9 years (median: 66)
• Male: female = 74.2% : 25.8%
• Hospital stay: 5.0 days
• Medical cost in 2014: 1,510,000 won (1,305 US dollars)
• Surgery within 3 months after ESD: 6.6%
Park CM. 24th KCHUGR Annual Scientific Meeting (2016-12-3)
Outcomes of ESD for EGC
Jun Haeng Lee. Department of Medicine
Sungkyunkwanuniversity School of Medicie, Seoul, Korea
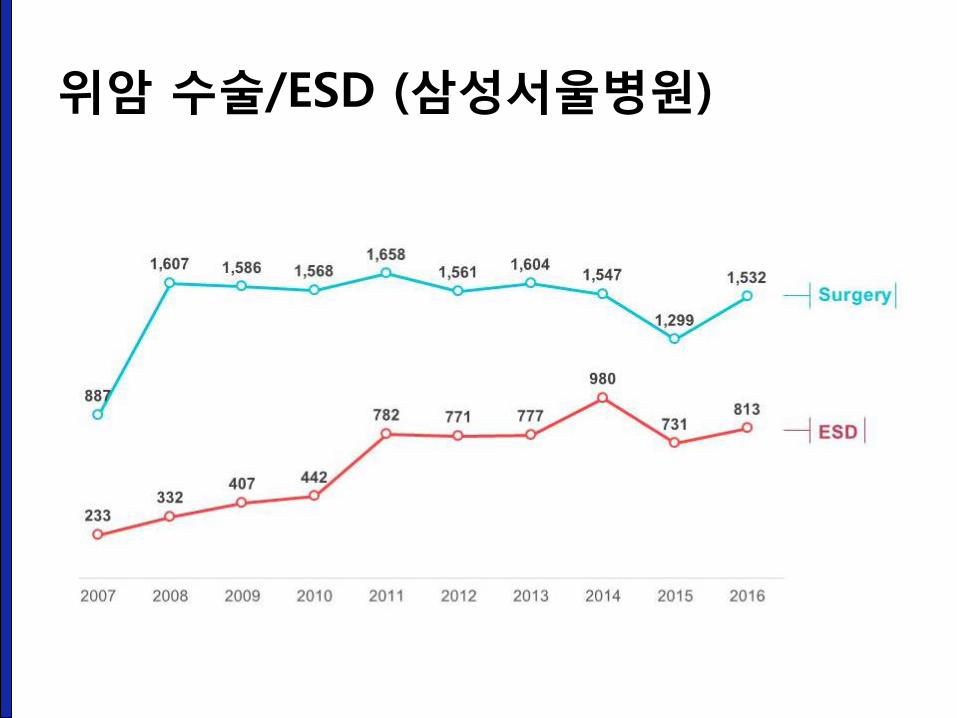
위암 수술/ESD (삼성서울병원)
Outcome of endoscopic treatment of EGC with differentiated histology
1. ITT analysis (both curative and non-curative
resection cases)
• Comparison with surgery (propensity score matched
cohort)
2. PP analysis
1) Curative-resection cases: single-arm long-term data
2) Non-curative resection cases: comparison between
surgery group and observation group
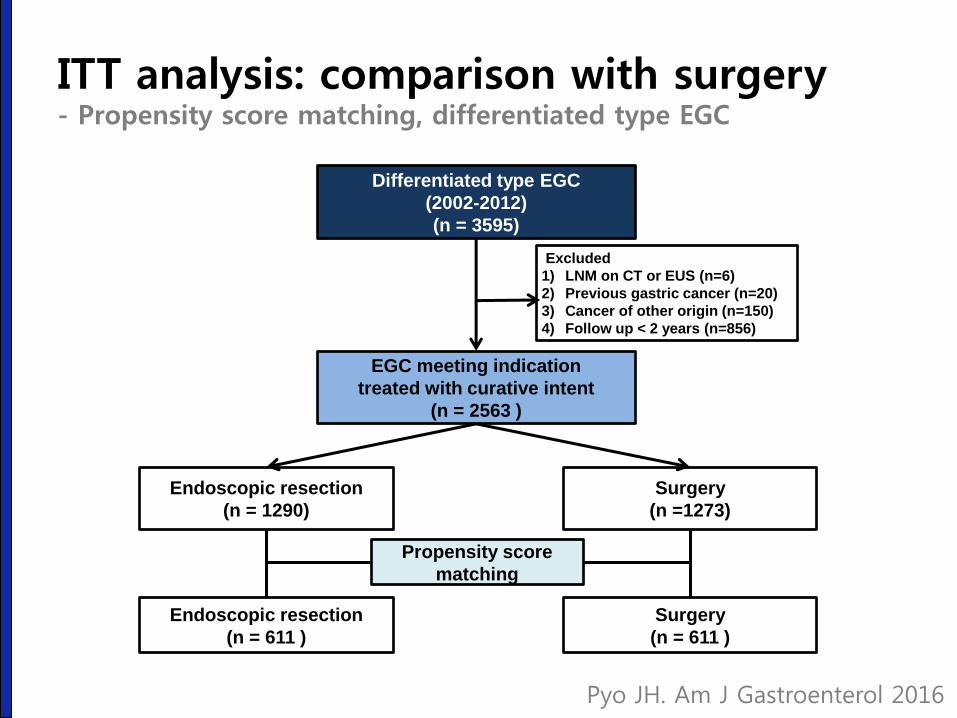
Differentiated type EGC
(2002-2012)
(n = 3595)
Excluded
1) LNM on CT or EUS (n=6)
2) Previous gastric cancer (n=20)
3) Cancer of other origin (n=150)
4) Follow up < 2 years (n=856)
EGC meeting indication
treated with curative intent
(n = 2563 )
Endoscopic resection
(n = 1290)
Surgery
(n =1273)
Endoscopic resection
(n = 611 )
Surgery
(n = 611 )
Propensity score
matching
Pyo JH. Am J Gastroenterol 2016
ITT analysis: comparison with surgery - Propensity score matching, differentiated type EGC
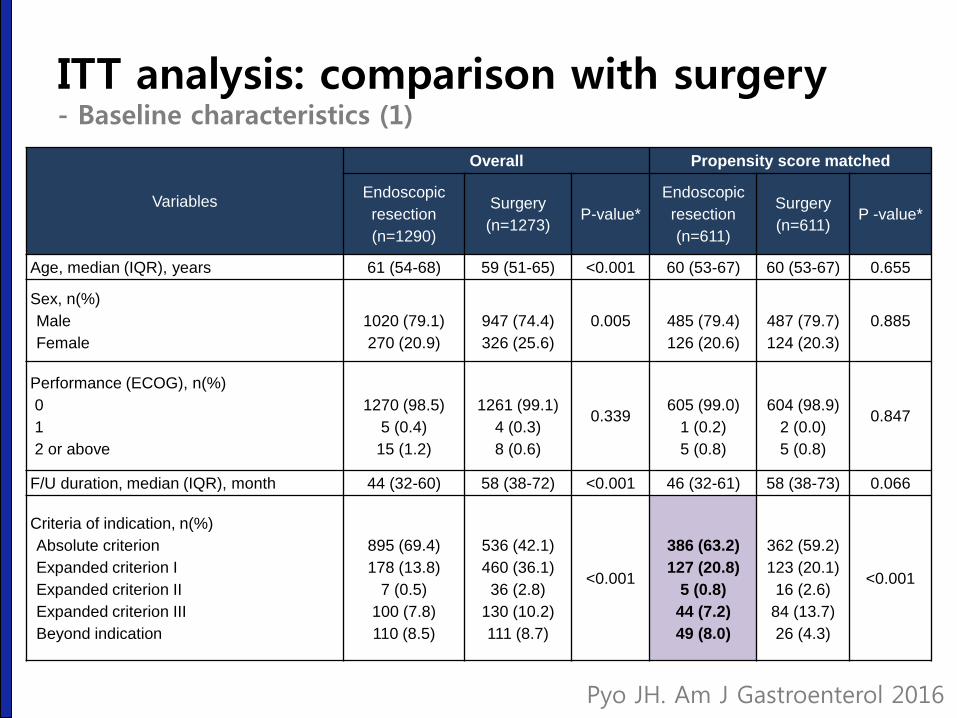
Variables
Overall Propensity score matched
Endoscopic
resection
(n=1290)
Surgery
(n=1273) P-value*
Endoscopic
resection
(n=611)
Surgery
(n=611) P -value*
Age, median (IQR), years 61 (54-68) 59 (51-65) <0.001 60 (53-67) 60 (53-67) 0.655
Sex, n(%)
Male
Female
1020 (79.1)
270 (20.9)
947 (74.4)
326 (25.6)
0.005
485 (79.4)
126 (20.6)
487 (79.7)
124 (20.3)
0.885
Performance (ECOG), n(%)
0
1
2 or above
1270 (98.5)
5 (0.4)
15 (1.2)
1261 (99.1)
4 (0.3)
8 (0.6)
0.339
605 (99.0)
1 (0.2)
5 (0.8)
604 (98.9)
2 (0.0)
5 (0.8)
0.847
F/U duration, median (IQR), month 44 (32-60) 58 (38-72) <0.001 46 (32-61) 58 (38-73) 0.066
Criteria of indication, n(%)
Absolute criterion
Expanded criterion I
Expanded criterion II
Expanded criterion III
Beyond indication
895 (69.4)
178 (13.8)
7 (0.5)
100 (7.8)
110 (8.5)
536 (42.1)
460 (36.1)
36 (2.8)
130 (10.2)
111 (8.7)
<0.001
386 (63.2)
127 (20.8)
5 (0.8)
44 (7.2)
49 (8.0)
362 (59.2)
123 (20.1)
16 (2.6)
84 (13.7)
26 (4.3)
<0.001
Pyo JH. Am J Gastroenterol 2016
ITT analysis: comparison with surgery - Baseline characteristics (1)
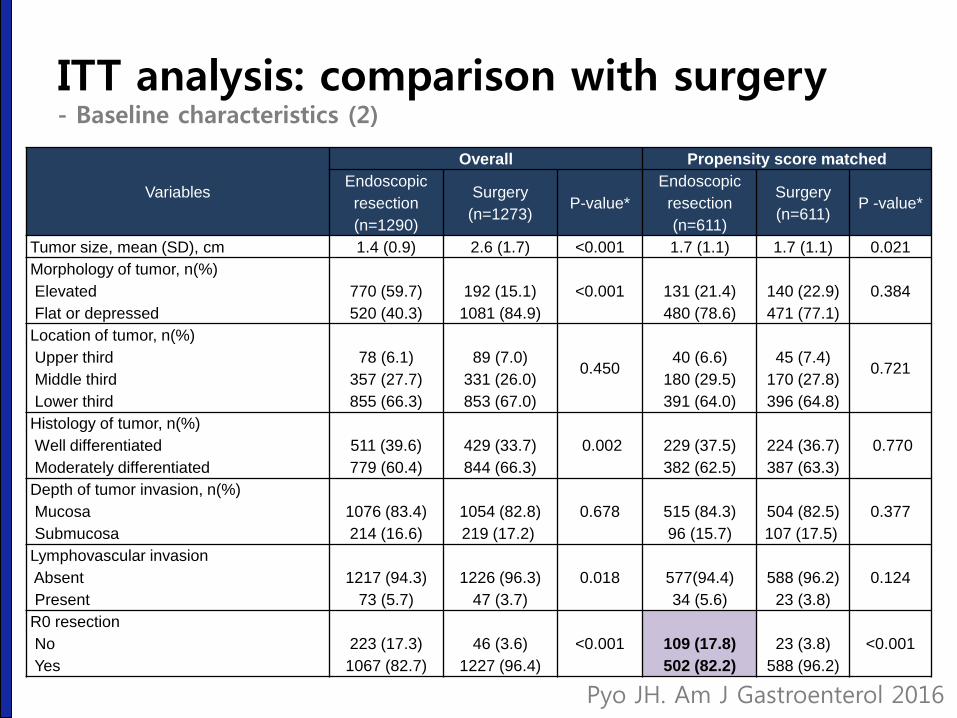
ITT analysis: comparison with surgery - Baseline characteristics (2)
Variables
Overall Propensity score matched
Endoscopic
resection
(n=1290)
Surgery
(n=1273) P-value*
Endoscopic
resection
(n=611)
Surgery
(n=611) P -value*
Tumor size, mean (SD), cm 1.4 (0.9) 2.6 (1.7) <0.001 1.7 (1.1) 1.7 (1.1) 0.021
Morphology of tumor, n(%)
Elevated
Flat or depressed
770 (59.7)
520 (40.3)
192 (15.1)
1081 (84.9)
<0.001
131 (21.4)
480 (78.6)
140 (22.9)
471 (77.1)
0.384
Location of tumor, n(%)
Upper third
Middle third
Lower third
78 (6.1)
357 (27.7)
855 (66.3)
89 (7.0)
331 (26.0)
853 (67.0)
0.450
40 (6.6)
180 (29.5)
391 (64.0)
45 (7.4)
170 (27.8)
396 (64.8)
0.721
Histology of tumor, n(%)
Well differentiated
Moderately differentiated
511 (39.6)
779 (60.4)
429 (33.7)
844 (66.3)
0.002
229 (37.5)
382 (62.5)
224 (36.7)
387 (63.3)
0.770
Depth of tumor invasion, n(%)
Mucosa
Submucosa
1076 (83.4)
214 (16.6)
1054 (82.8)
219 (17.2)
0.678
515 (84.3)
96 (15.7)
504 (82.5)
107 (17.5)
0.377
Lymphovascular invasion
Absent
Present
1217 (94.3)
73 (5.7)
1226 (96.3)
47 (3.7)
0.018
577(94.4)
34 (5.6)
588 (96.2)
23 (3.8)
0.124
R0 resection
No
Yes
223 (17.3)
1067 (82.7)
46 (3.6)
1227 (96.4)
<0.001
109 (17.8)
502 (82.2)
23 (3.8)
588 (96.2)
<0.001
Pyo JH. Am J Gastroenterol 2016
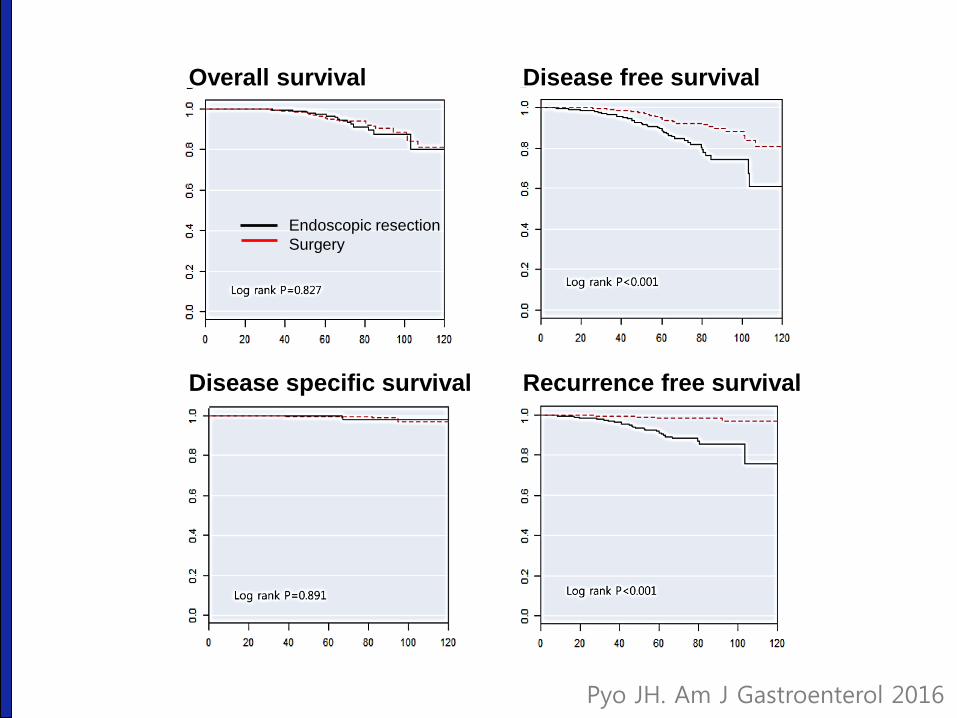
Endoscopic resection
Surgery
Overall survival
Disease specific survival Recurrence free survival
Disease free survival
Pyo JH. Am J Gastroenterol 2016
PP analysis (1): single-arm follow-up - Differentiated, curative (n=1,306)
• EGCs treated by ESD at Samsung Medical Center
• 1,838 patients with 1,889 differentiated-type EGCs
• November 2003 – May 2011
• Censoring date: May 2014
• Differentiated-type EGC
– Well or moderately differentiated or papillary EGC
– According to the quantitatively predominant histologic type
– Differentiated-type EGC > 50%
Min BH. Endoscopy 2015
PP analysis (1): single-arm follow-up - Differentiated, curative (n=1,306)
• Median follow-up: 61 months (range 17-122)
• Local recurrence: 0.08% (1/1,306)
• Metachronous recurrence: 3.6% (47/1,306)
– Definition of metachronous recurrence: at least 12 months after ER
• Extragastric recurrence: 0.15% (2/1,306)
• 5-year overall survival
– Absolute indication: 97.3%
– Expanded indication: 96.4%
Min BH. Endoscopy 2015
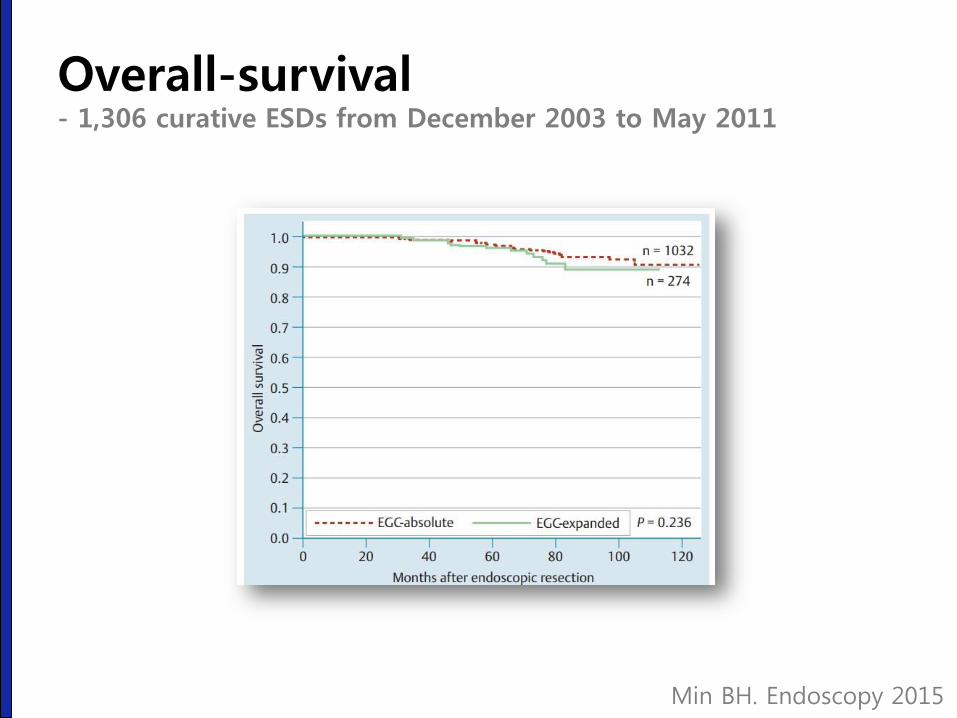
Overall-survival - 1,306 curative ESDs from December 2003 to May 2011
Min BH. Endoscopy 2015
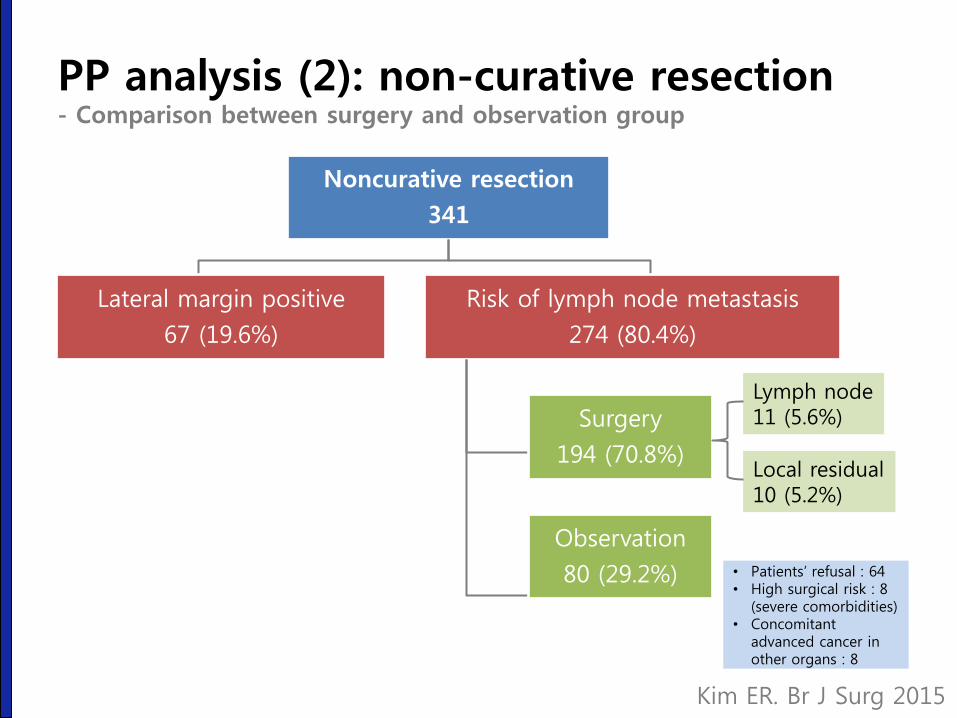
Noncurative resection
341
Lateral margin positive
67 (19.6%)
Risk of lymph node metastasis
274 (80.4%)
Surgery
194 (70.8%)
Observation
80 (29.2%) • Patients’ refusal : 64 • High surgical risk : 8
(severe comorbidities) • Concomitant
advanced cancer in other organs : 8
Lymph node 11 (5.6%)
Local residual 10 (5.2%)
PP analysis (2): non-curative resection - Comparison between surgery and observation group
Kim ER. Br J Surg 2015
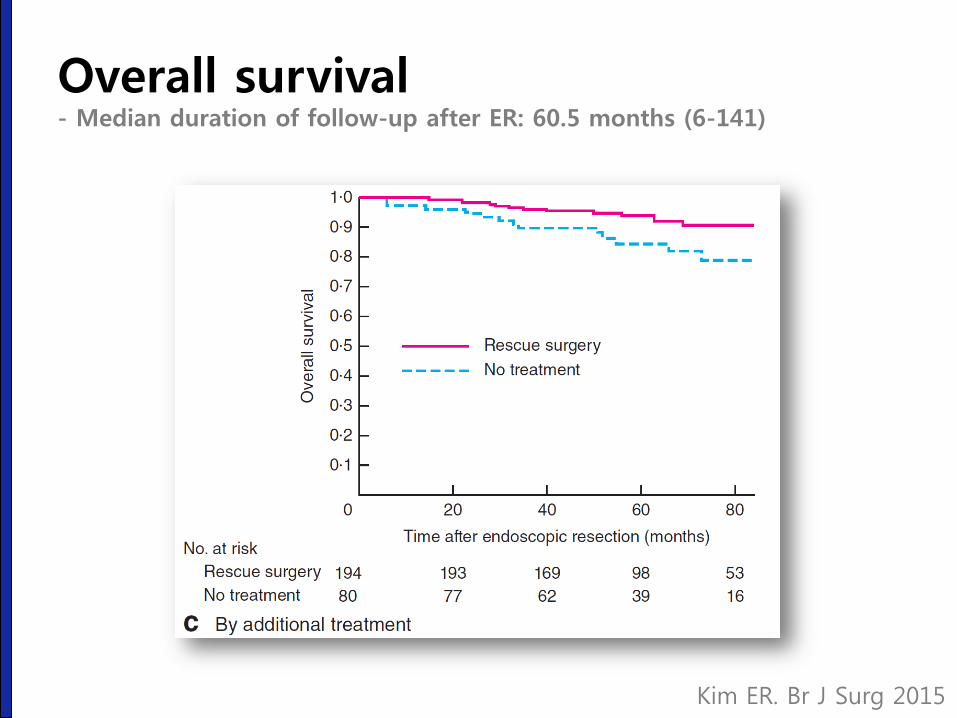
Overall survival - Median duration of follow-up after ER: 60.5 months (6-141)
Kim ER. Br J Surg 2015
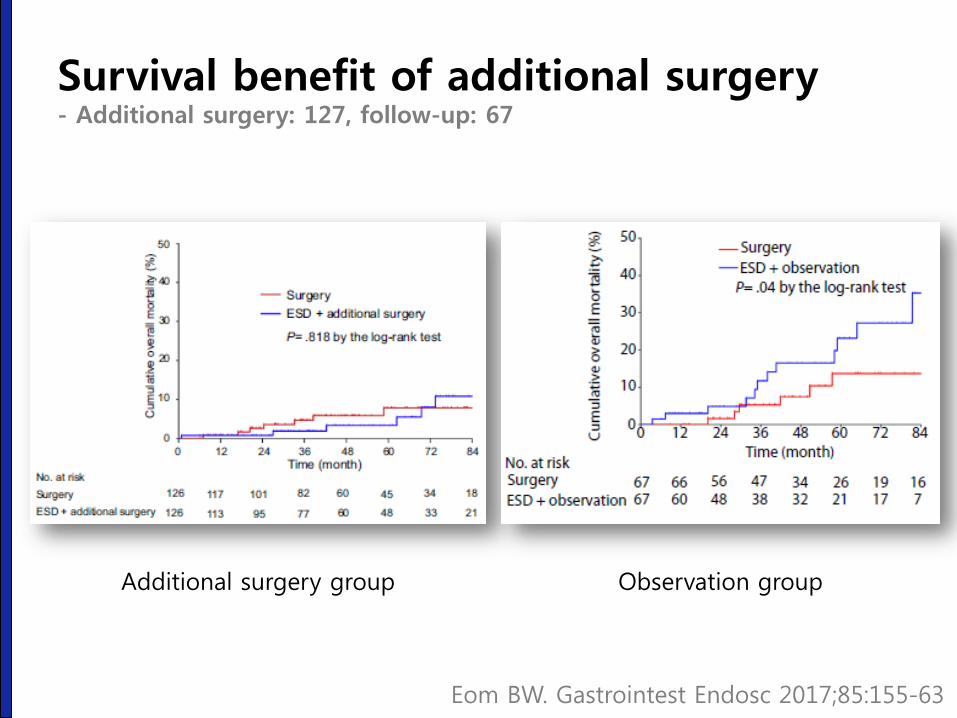
Survival benefit of additional surgery - Additional surgery: 127, follow-up: 67
Observation group Additional surgery group
Eom BW. Gastrointest Endosc 2017;85:155-63
환자에게 어떻게 설명할 것인가?
성균관대학교 의과대학 내과 이준행
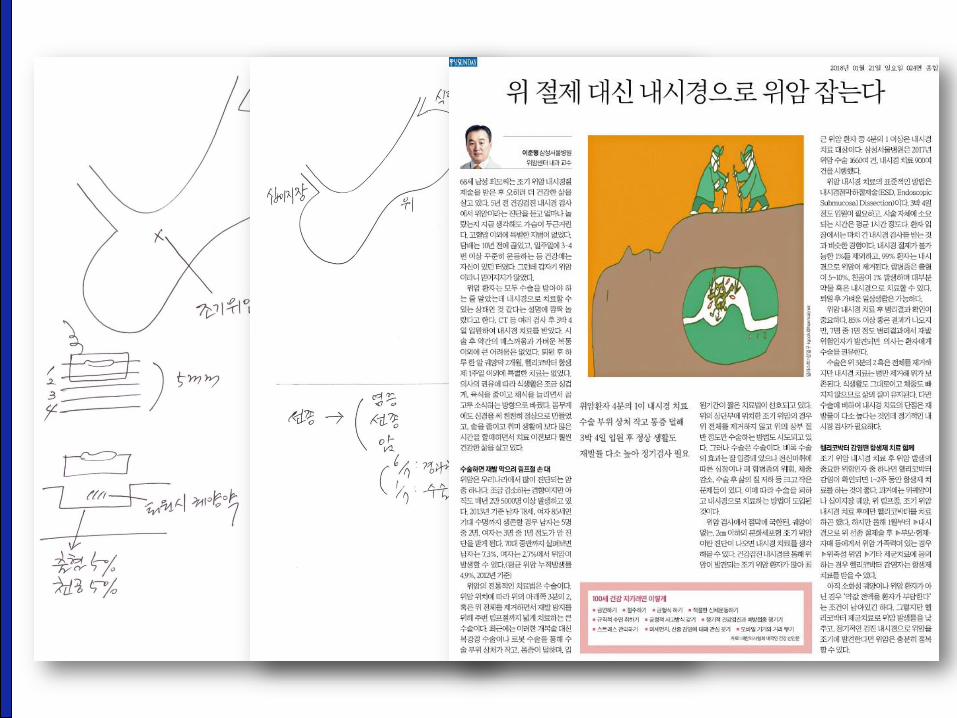
수기 차트를 이용한 설명 (2005)
수기 차트를 이용한 설명 (2005)
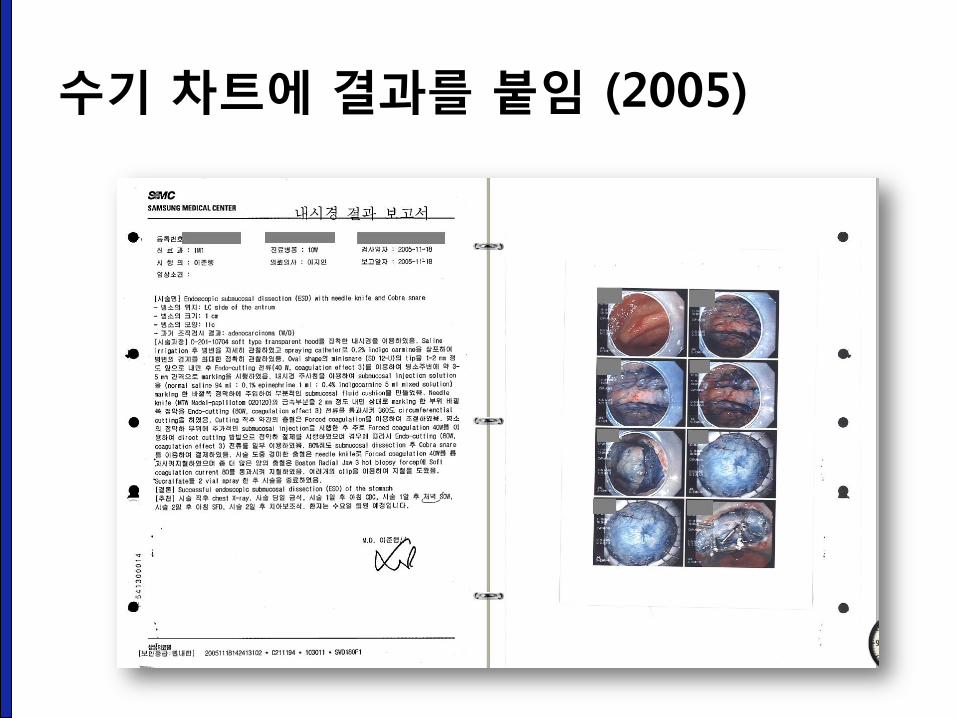
수기 차트에 결과를 붙임 (2005)
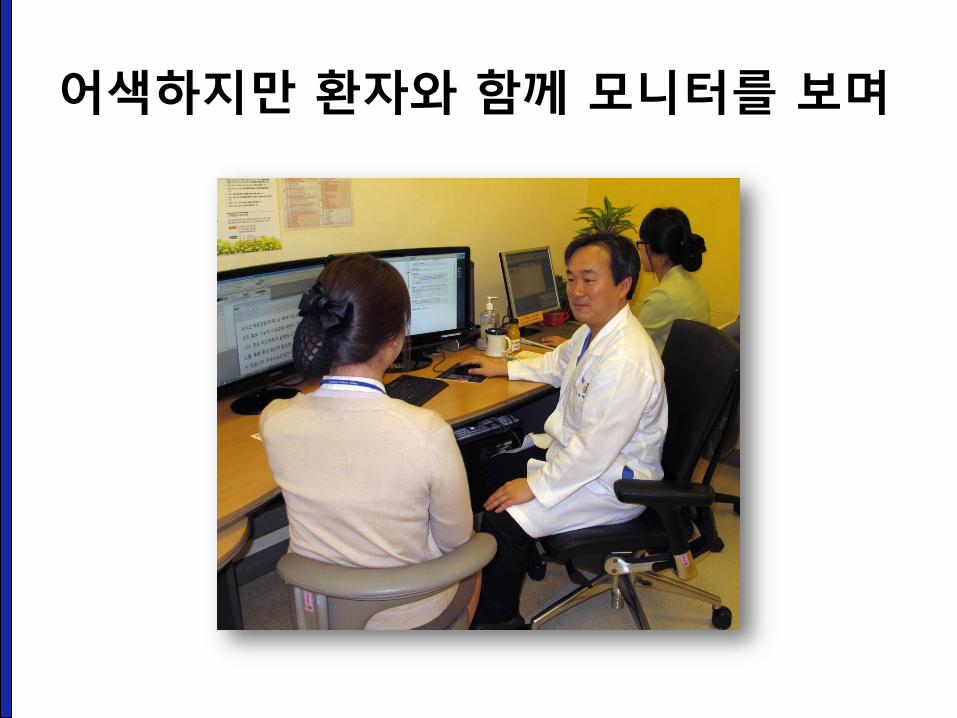
어색하지만 환자와 함께 모니터를 보며
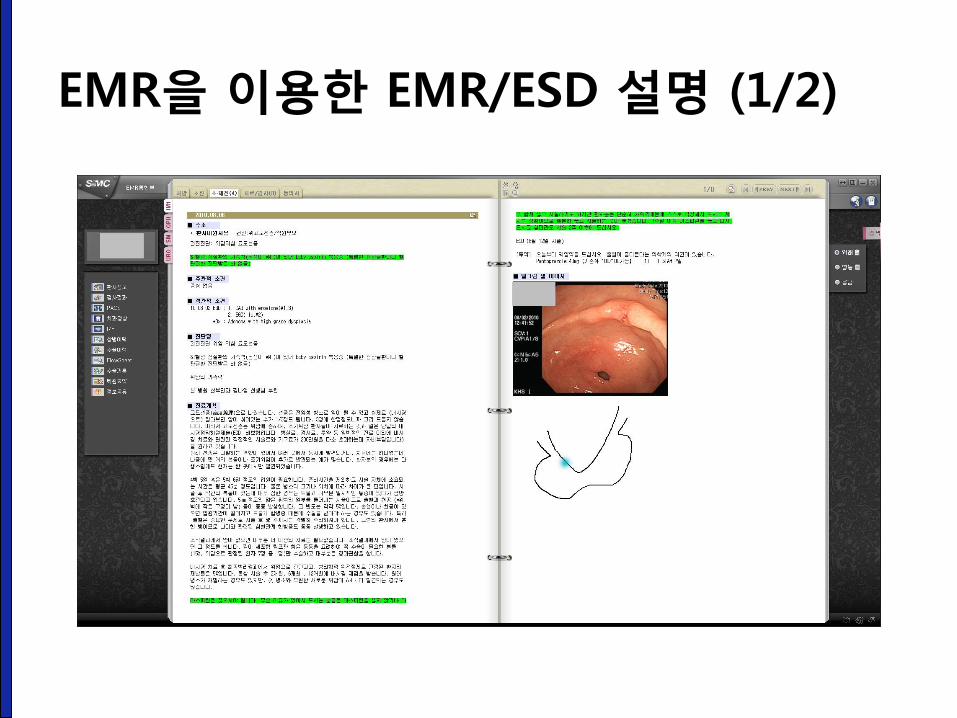
EMR을 이용한 EMR/ESD 설명 (1/2)
EMR을 이용한 EMR/ESD 설명 (2/2)
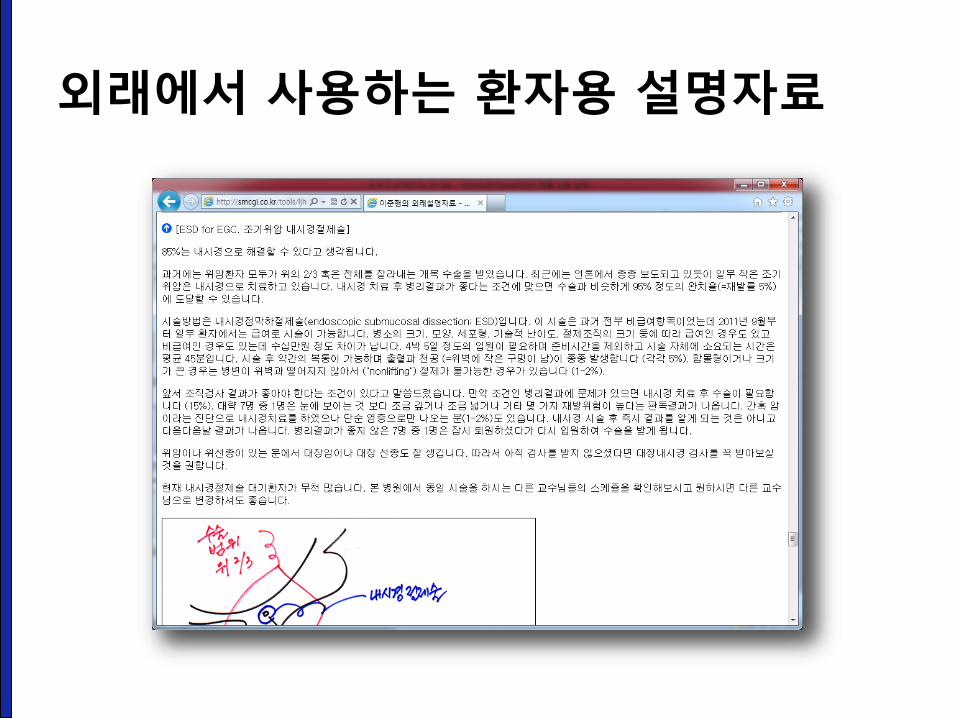
외래에서 사용하는 환자용 설명자료
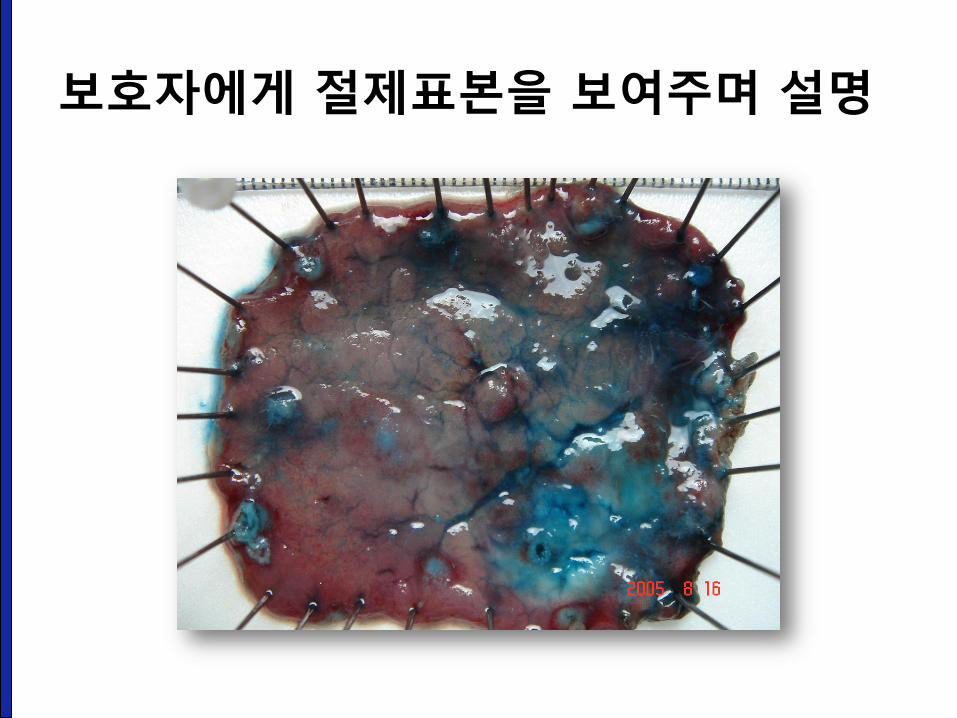
보호자에게 절제표본을 보여주며 설명
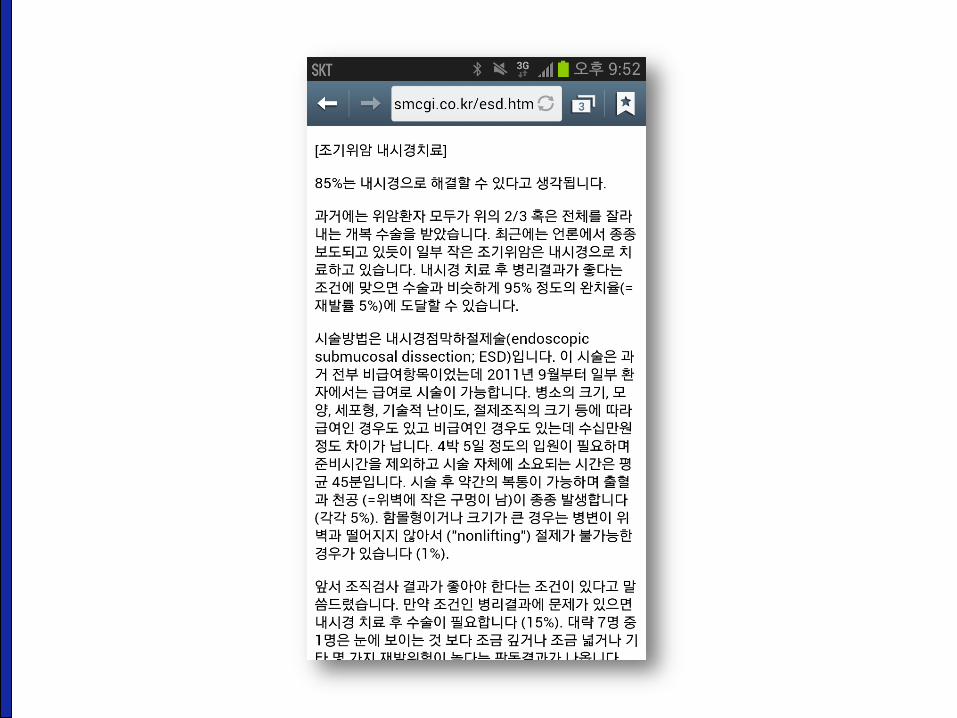
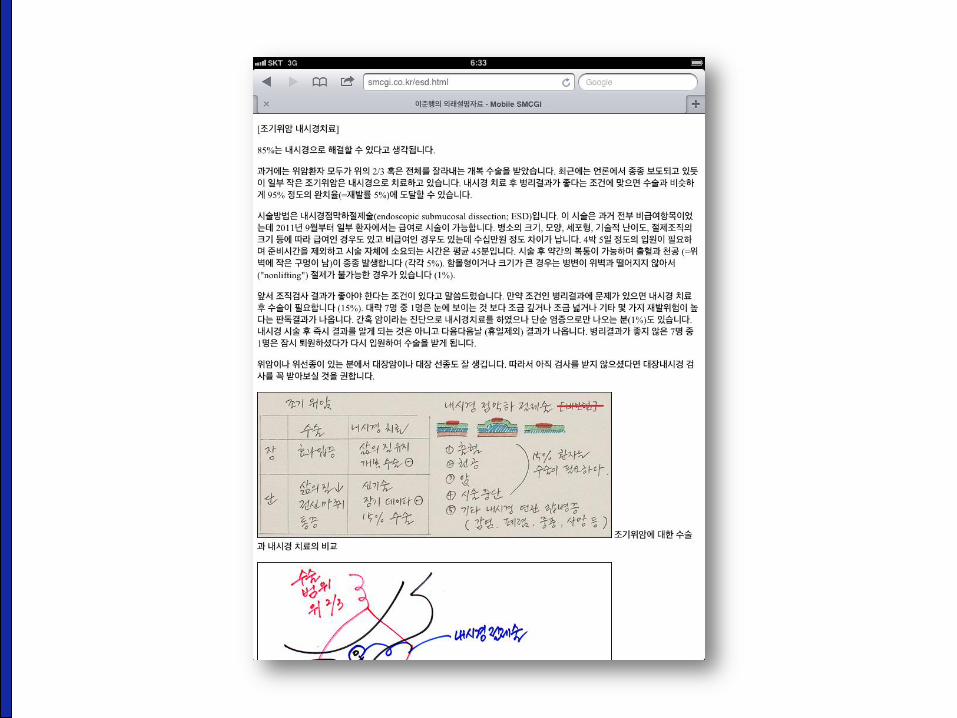
Smartphone을 이용하여 회진시 설명

Technical Aspects
성균관대학교 의과대학 내과 이준행
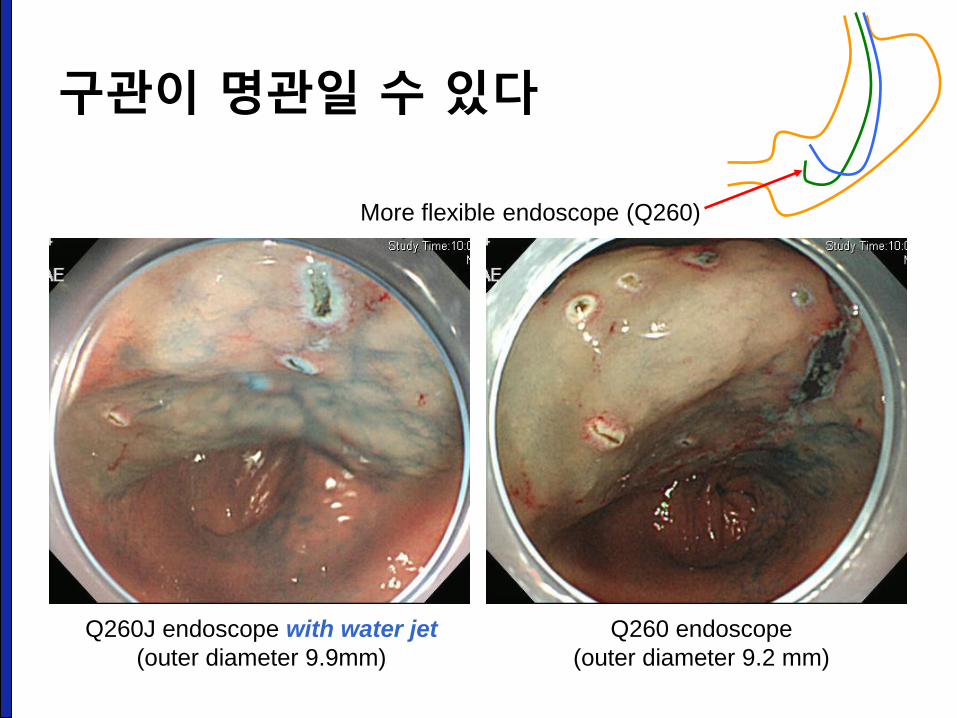
Q260 endoscope
(outer diameter 9.2 mm)
Q260J endoscope with water jet
(outer diameter 9.9mm)
More flexible endoscope (Q260)
구관이 명관일 수 있다
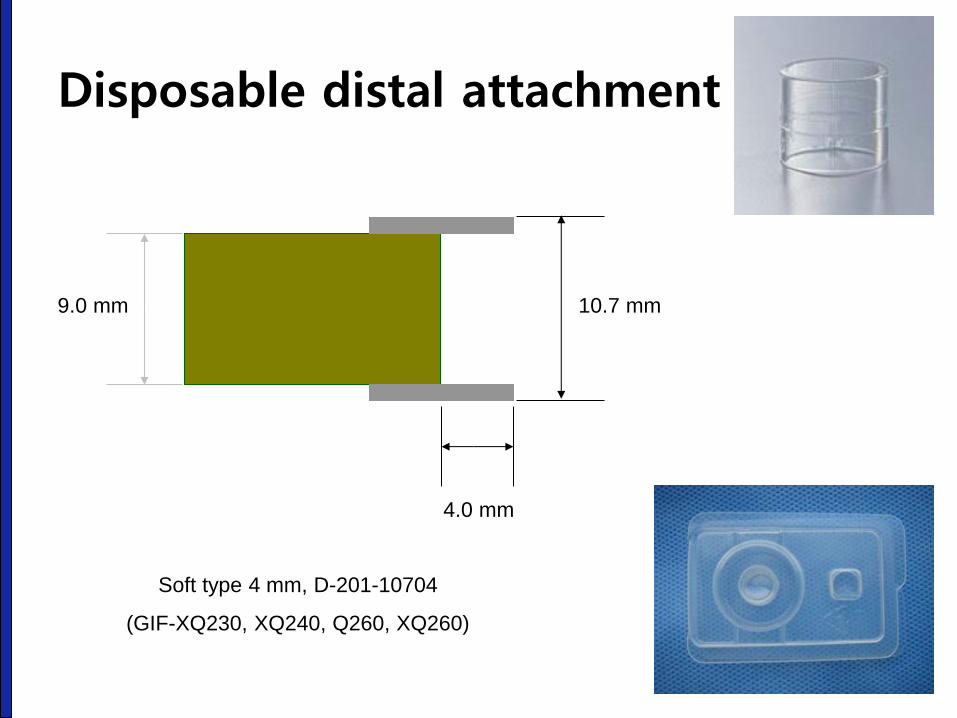
Disposable distal attachment
9.0 mm 10.7 mm
4.0 mm
Soft type 4 mm, D-201-10704
(GIF-XQ230, XQ240, Q260, XQ260)
Presentation title Page 46
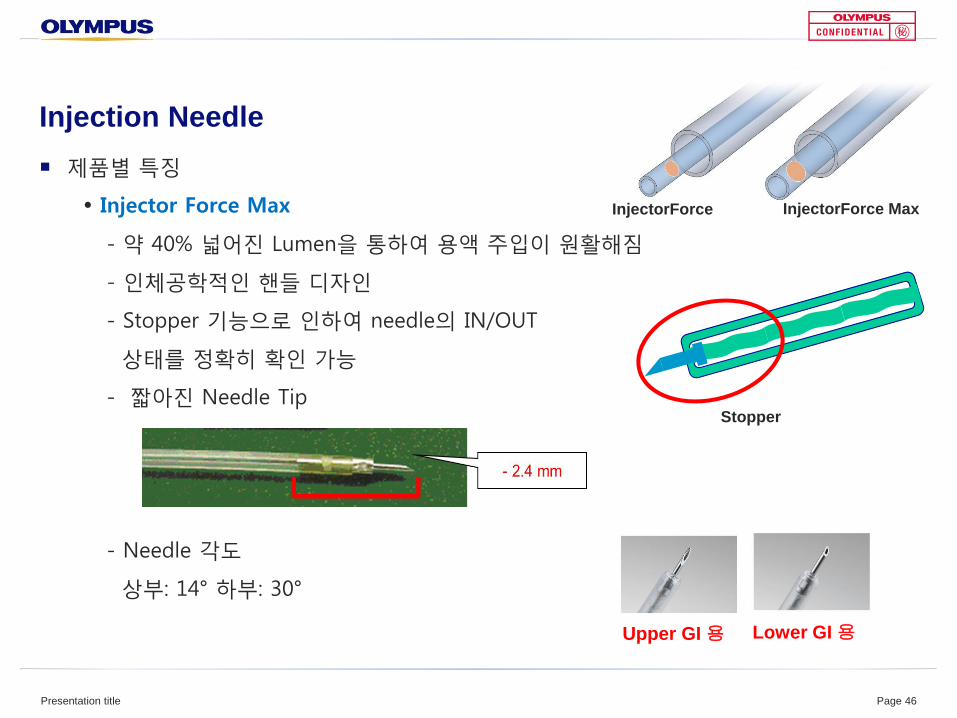
Injection Needle
제품별 특징
Injector Force Max
- 약 40% 넓어진 Lumen을 통하여 용액 주입이 원활해짐
- 인체공학적인 핸들 디자인
- Stopper 기능으로 인하여 needle의 IN/OUT
상태를 정확히 확인 가능
- 짧아진 Needle Tip
- Needle 각도
상부: 14° 하부: 30°
InjectorForce InjectorForce Max
Upper GI 용 Lower GI 용
Stopper
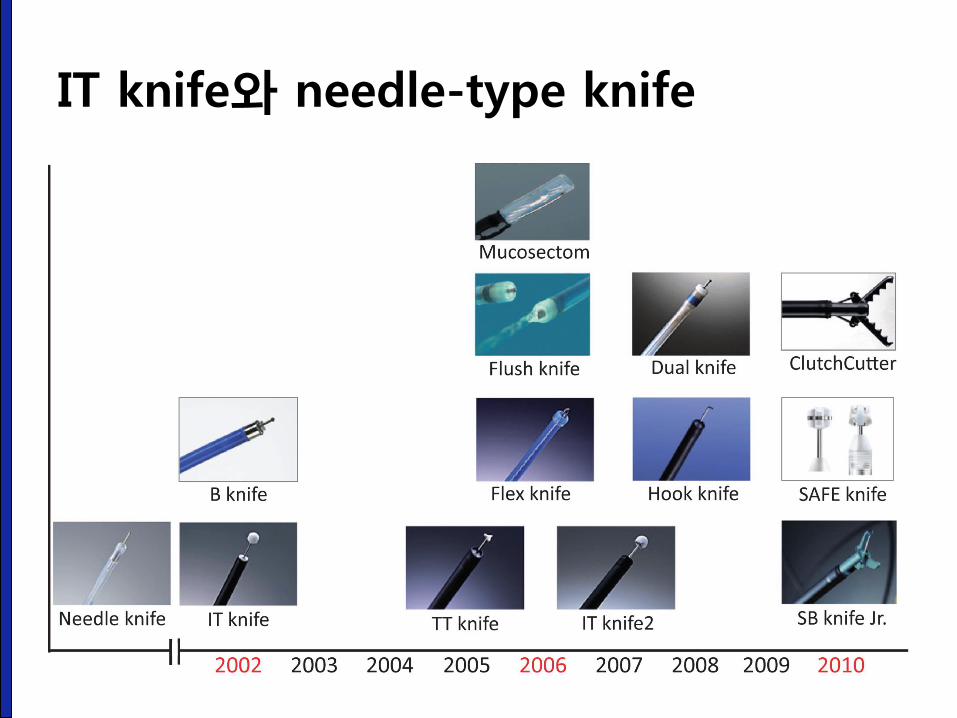
IT knife와 needle-type knife
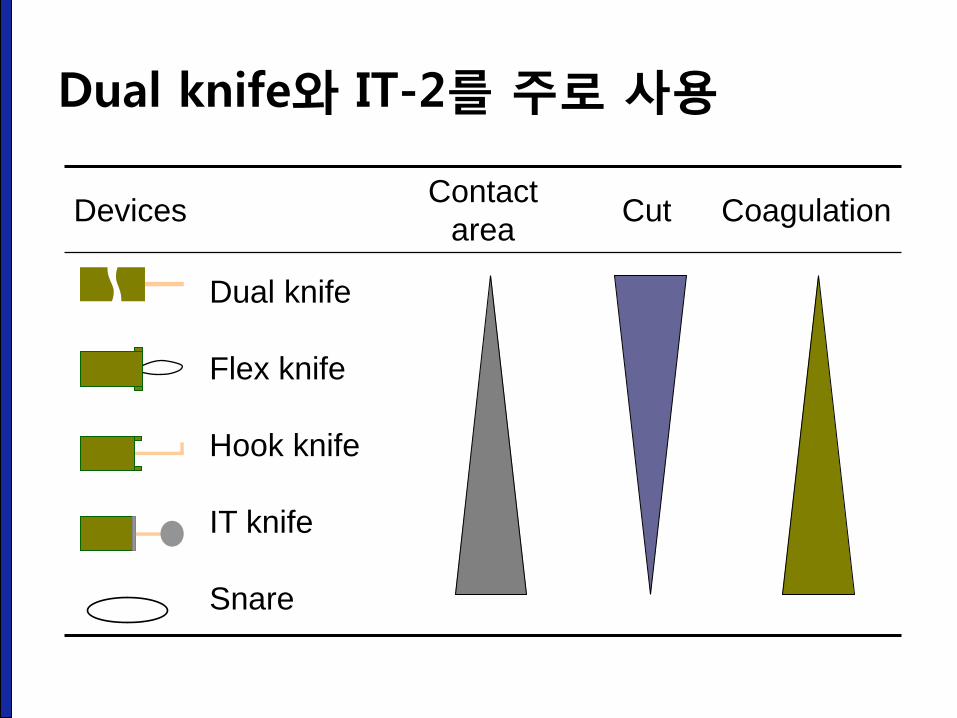
Devices Contact
area Cut Coagulation
Dual knife
Flex knife
Hook knife
IT knife
Snare
Dual knife와 IT-2를 주로 사용
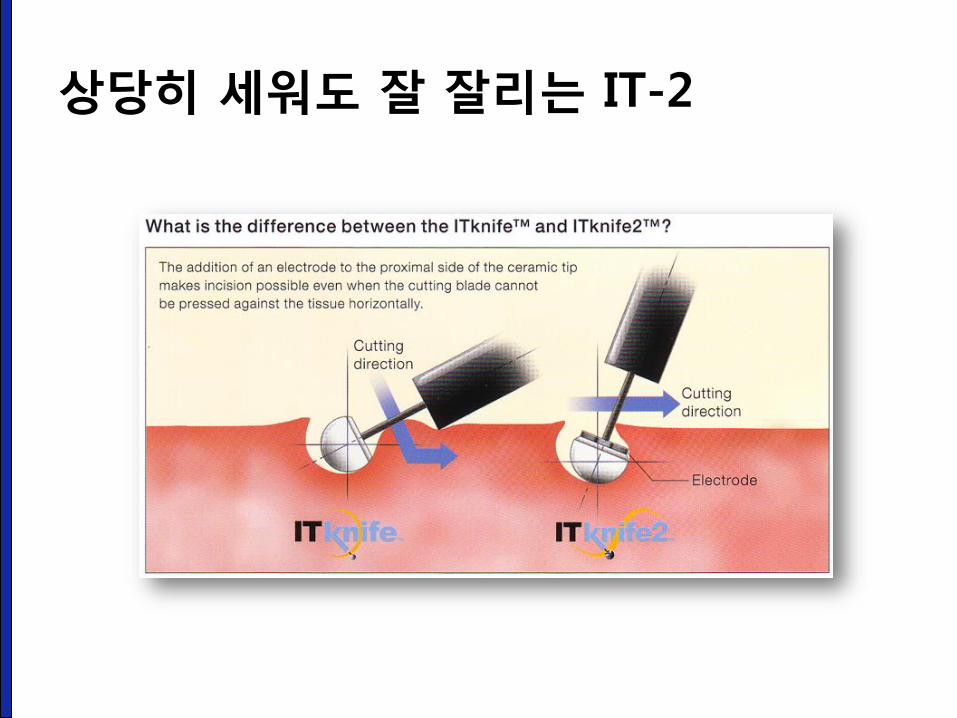
상당히 세워도 잘 잘리는 IT-2
Presentation title Page 50
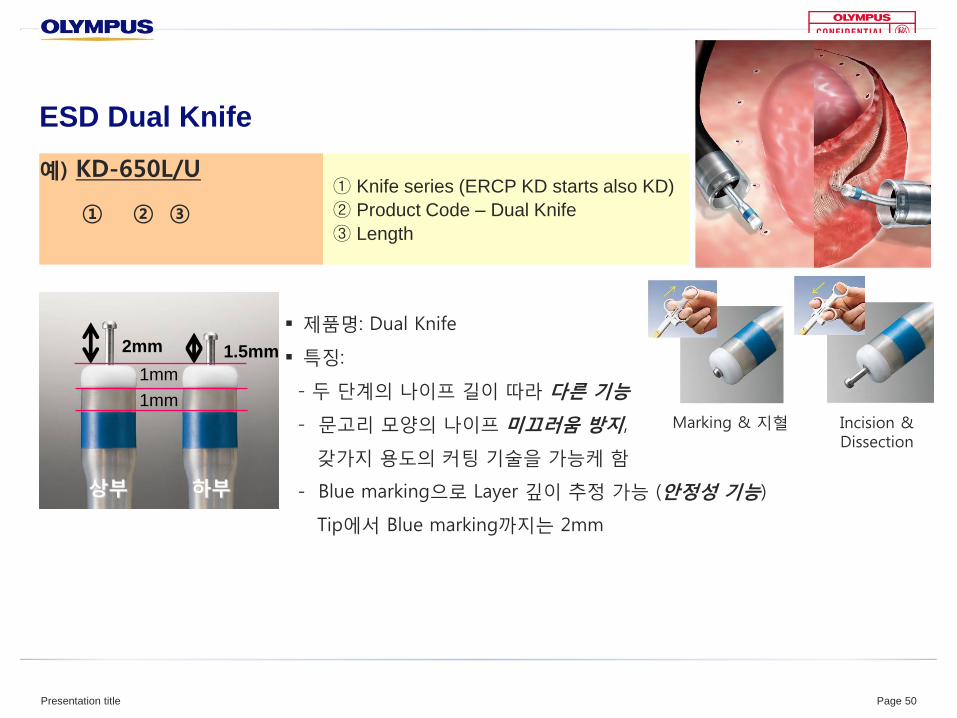
ESD Dual Knife
예) KD-650L/U
① ② ③
① Knife series (ERCP KD starts also KD)
② Product Code – Dual Knife
③ Length
제품명: Dual Knife
특징:
- 두 단계의 나이프 길이 따라 다른 기능
- 문고리 모양의 나이프 미끄러움 방지,
갖가지 용도의 커팅 기술을 가능케 함
- Blue marking으로 Layer 깊이 추정 가능 (안정성 기능)
Tip에서 Blue marking까지는 2mm
Marking & 지혈 Incision & Dissection
2mm 1.5mm
상부 하부
1mm
1mm

국산도 활발히 개발되고 있습니다.
http://www.finemedix.com
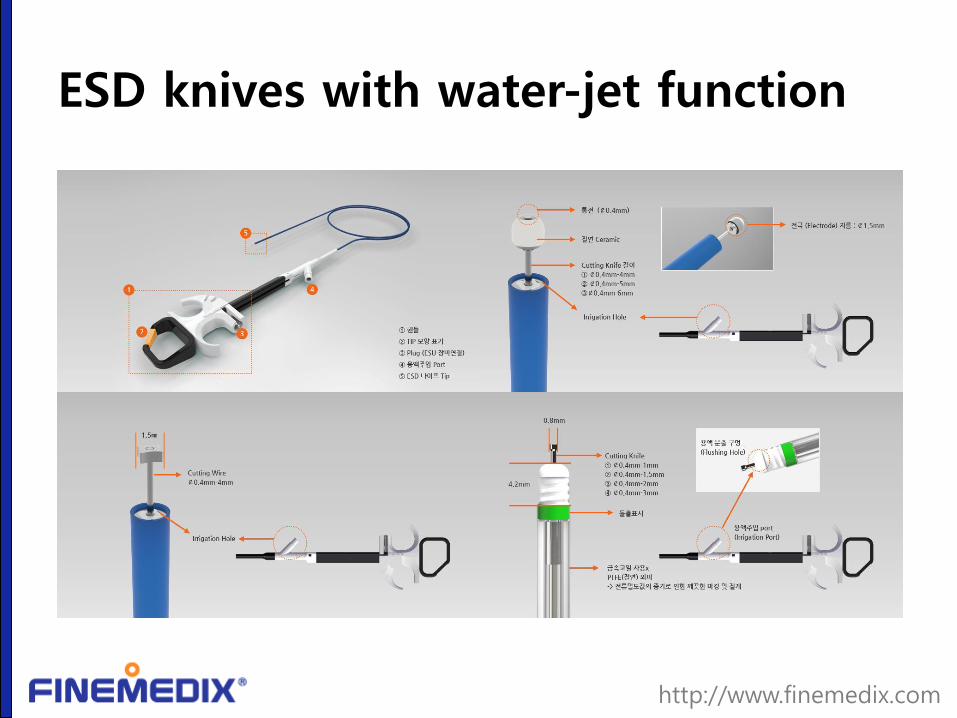
ESD knives with water-jet function
http://www.finemedix.com
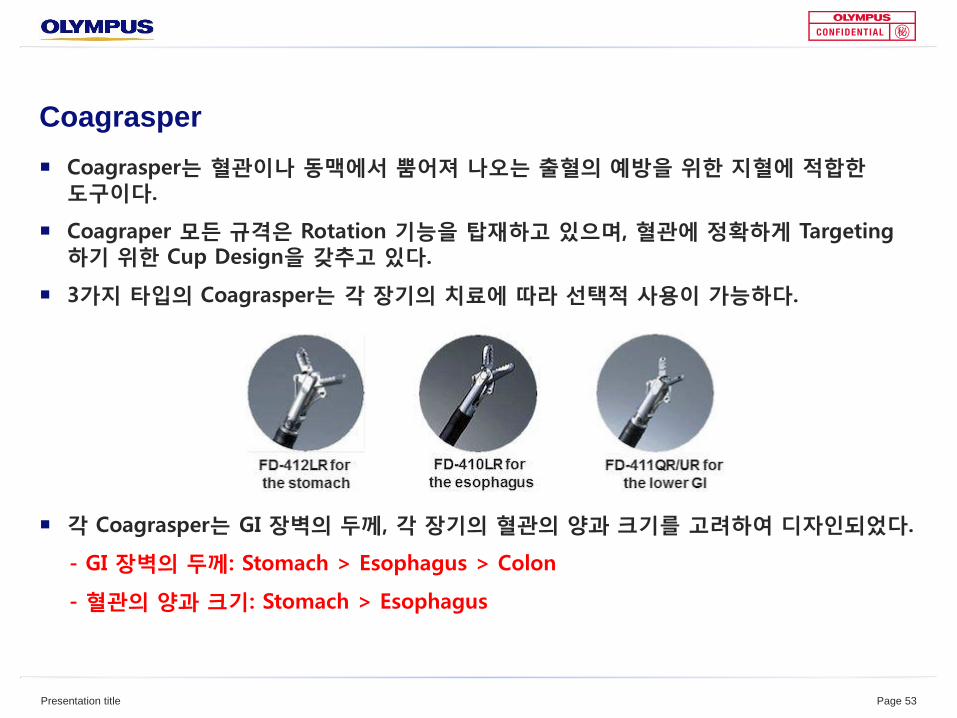
Coagrasper
Coagrasper는 혈관이나 동맥에서 뿜어져 나오는 출혈의 예방을 위한 지혈에 적합한 도구이다.
Coagraper 모든 규격은 Rotation 기능을 탑재하고 있으며, 혈관에 정확하게 Targeting 하기 위한 Cup Design을 갖추고 있다.
3가지 타입의 Coagrasper는 각 장기의 치료에 따라 선택적 사용이 가능하다.
각 Coagrasper는 GI 장벽의 두께, 각 장기의 혈관의 양과 크기를 고려하여 디자인되었다.
- GI 장벽의 두께: Stomach > Esophagus > Colon
- 혈관의 양과 크기: Stomach > Esophagus
Presentation title Page 53
Submucosal Injection
• 과거: normal saline 493 ml +epinephrine 5
ml + 0.8% indigocarmine 2ml
• 현재: normal saline 100 ml + epinephrine 1
ml + 0.8% indigocarmine 0.1 ml
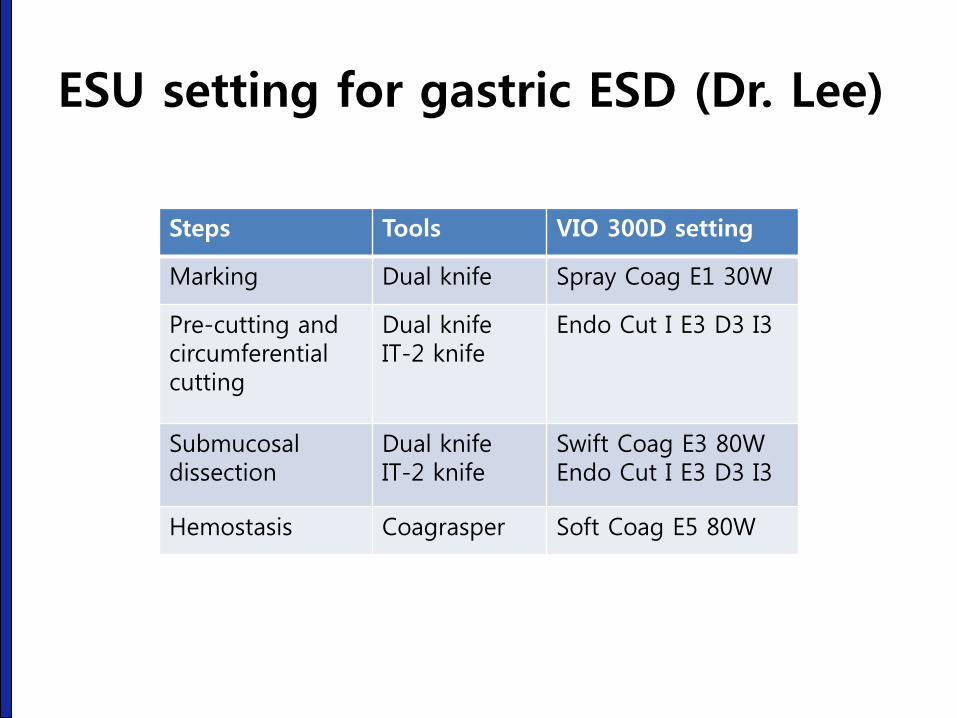
ESU setting for gastric ESD (Dr. Lee)
Steps Tools VIO 300D setting
Marking Dual knife Spray Coag E1 30W
Pre-cutting and circumferential cutting
Dual knife IT-2 knife
Endo Cut I E3 D3 I3
Submucosal dissection
Dual knife IT-2 knife
Swift Coag E3 80W Endo Cut I E3 D3 I3
Hemostasis Coagrasper Soft Coag E5 80W
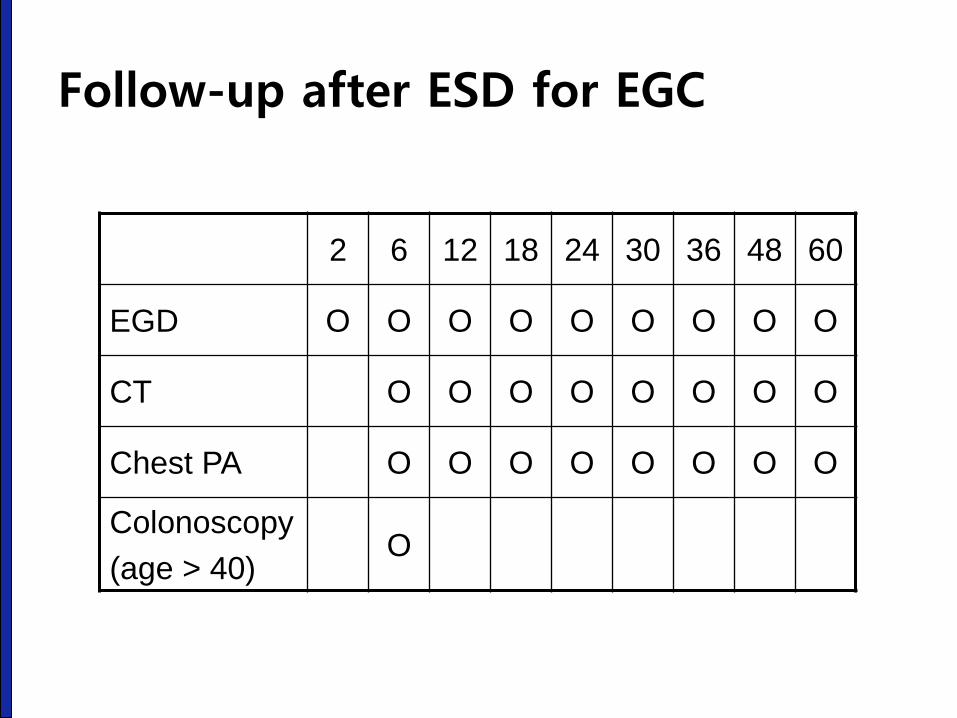
Follow-up after ESD for EGC
2 6 12 18 24 30 36 48 60
EGD O O O O O O O O O
CT O O O O O O O O
Chest PA O O O O O O O O
Colonoscopy
(age > 40) O
ESD training
성균관대학교 의과대학 내과 이준행
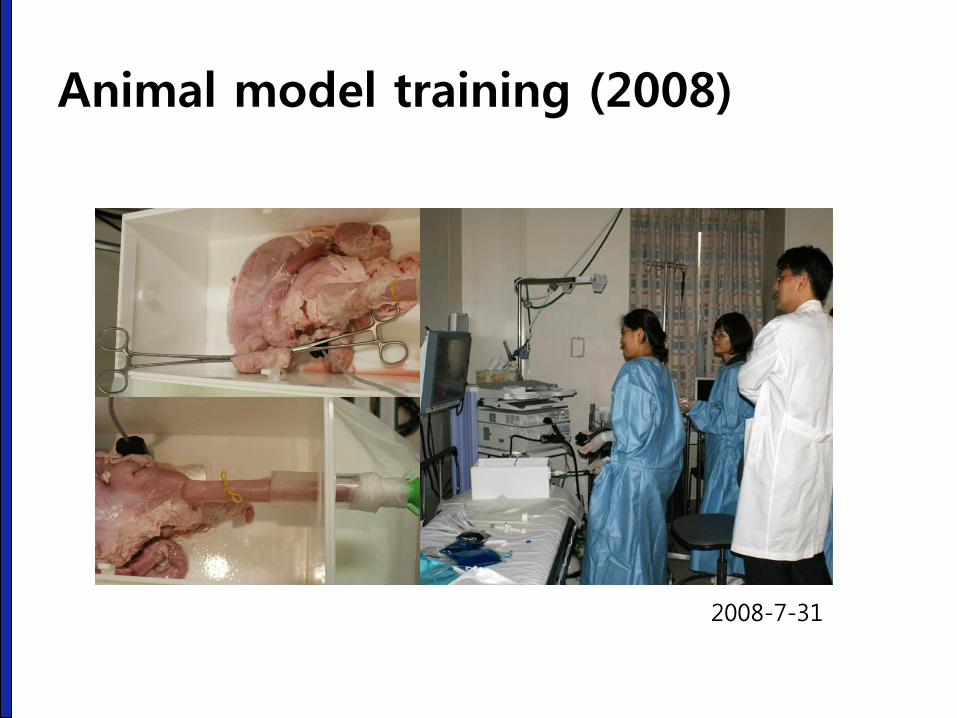
Animal model training (2008)
2008-7-31
적출 장기를 이용한 animal model 훈련도 동물실험실을 이용하도록 제도 변경
2017-4-21. ESD hands-on training (SMC)
2015 JDDW ESD hands-on training

2016 JSGE ESD hands-on training
2016 JSGE ESD hands-on training for women doctors
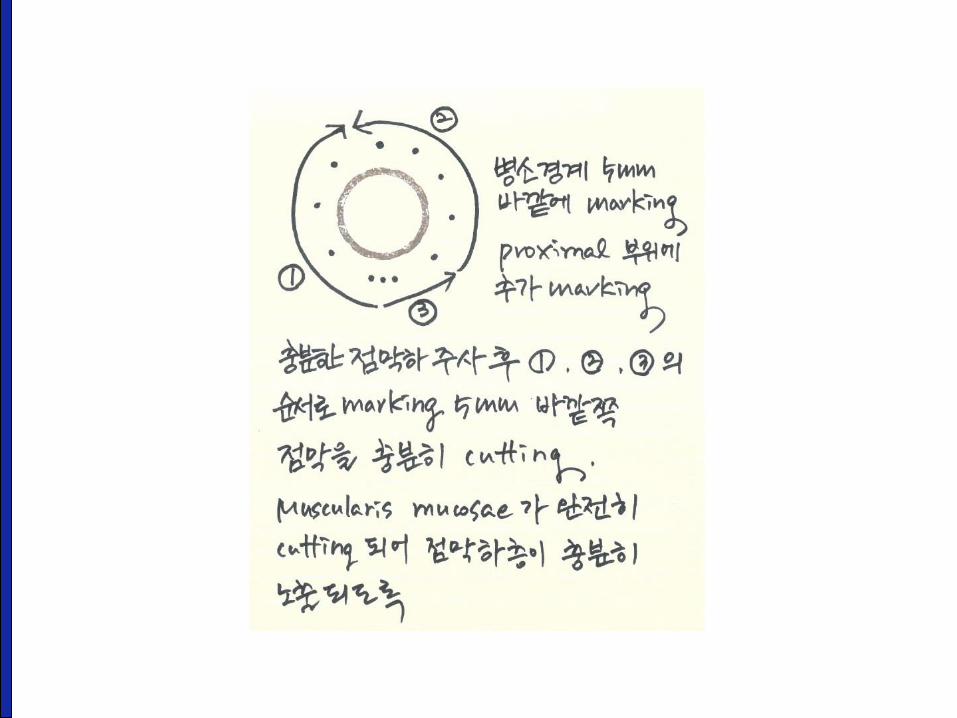
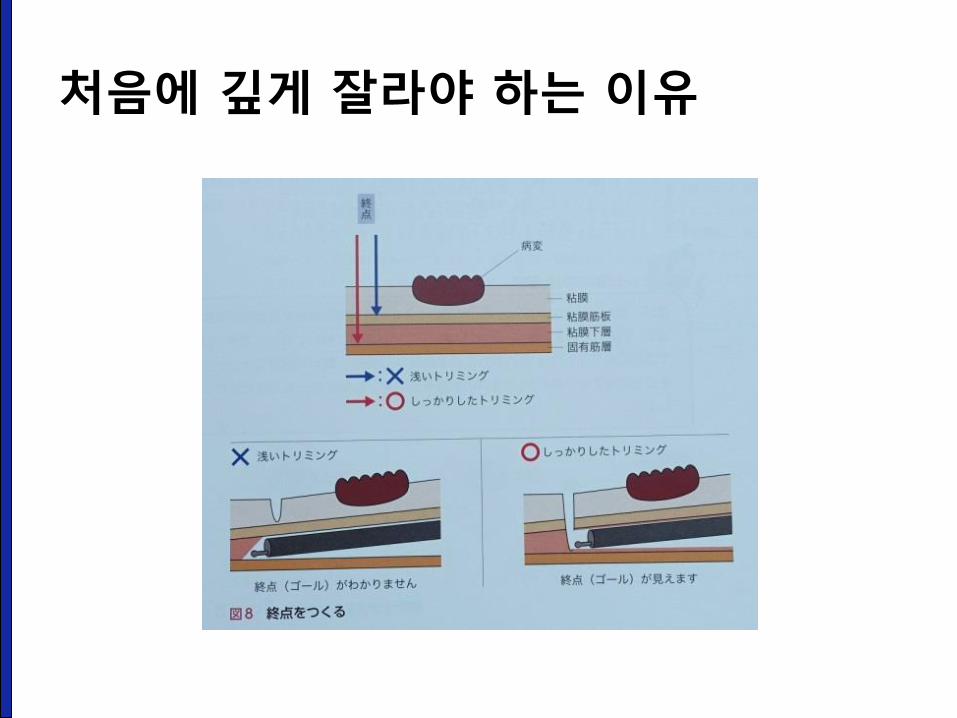
처음에 깊게 잘라야 하는 이유
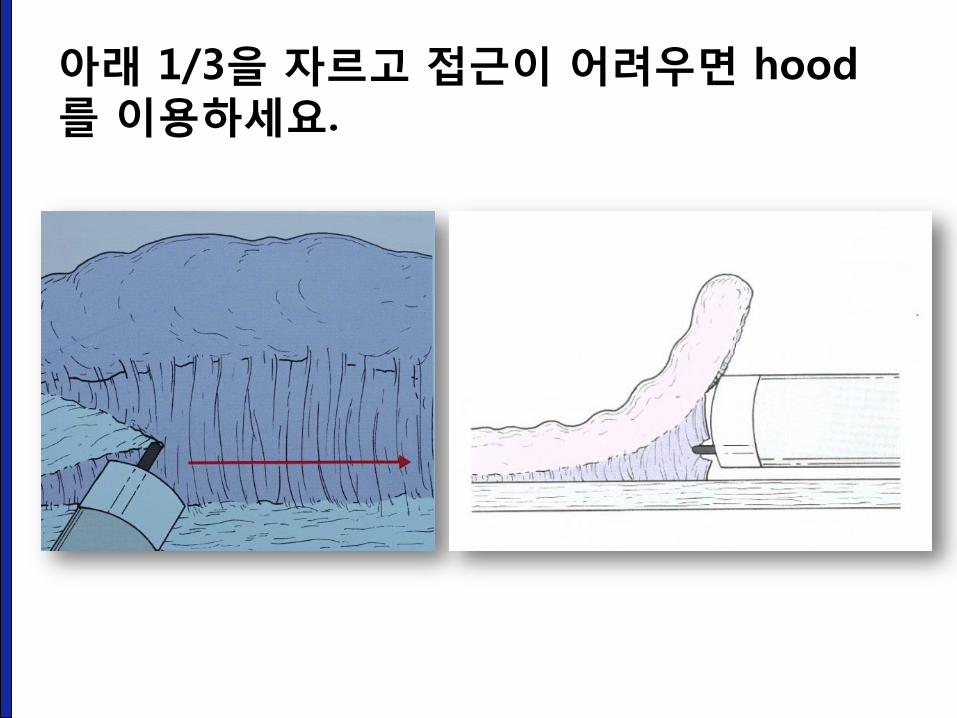
아래 1/3을 자르고 접근이 어려우면 hood를 이용하세요.
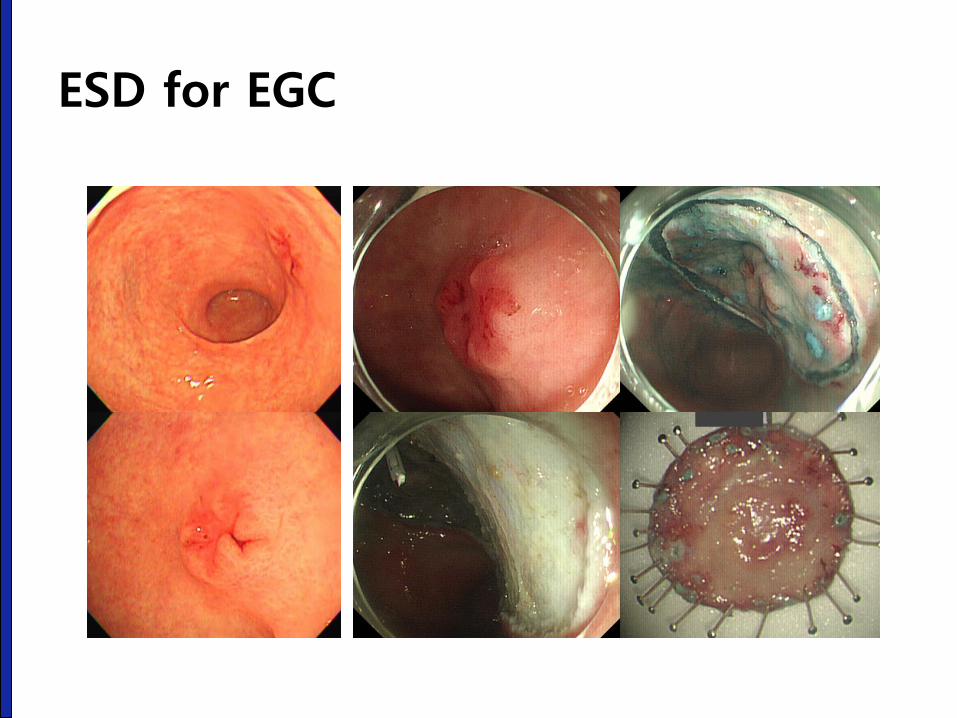
ESD for EGC
Final comments
• 뒤에서 PK mode로 보고 있다가 갑자기 ESD를
하기는 어렵습니다. First assistant로 몇 개월 함
께 ESD를 하다 보면 저절로 배우게 될 것입니다.
• 혼자 익히지 마십시오. 동영상으로 촬영하여
feedback을 받으시기 바랍니다.
• 자신의 data를 관리하십시오.
동영상으로 촬영하여 feedback을 받자
Current status of ESD for EGC in Korea - From Nov 2011 – Dec 2014
• Number of ESD for EGC cases: 23,828
(2012: 6,664 2013:7,499 2014: 7,734)
• Age: 64.9 +/- 9.9 years (median: 66)
• Male: female = 74.2% : 25.8%
• Hospital stay: 5.0 days
• Medical cost in 2014: 1,510,000 won (1,305 US dollars)
• Surgery within 3 months after ESD: 6.6%
Park CM. 24th KCHUGR Annual Scientific Meeting (2016-12-3)

Thank you for your attention.





























