Embed Size (px)
Citation preview

959
like strongyloidiasis, may be devastatingly exacerbated by immuno-suppression, particularly steroid therapy. The recognition andtreatment of these conditions is thus very important.There are still thousands of ex-FEPOWs alive today, mostly in
Britain and other parts of Europe and in Australia and NorthAmerica. Many have not had adequate tropical disease screening,and doctors should be alert to their health problems. Hospitaldoctors should bear in mind that 4-3% of British ex-FEPOWs are
hepatitis B surface antigen (HBsAg) positive, compared with anormal HBsAg carriage rate ofO-1%. Again, this is presumably ahangover from their days of captivity in the tropics.
It is now almost thirty-seven years since these men returned fromimprisonment to their temperate homelands. They have taught usmuch about the amazing longevity of tropically acquired infections.
Department of Tropical Medicine,Liverpool School of Tropical Medicine,Liverpool L3 5QA
GEOFFREY V. GILL*DION R. BELL
* Present address: Department of Medicine, Baragwanath Hospital, Johannesburg, SouthAfrica.
JAUNDICE ASSOCIATED WITH THE USE OFBENOXAPROFEN
SIR,-We have seen three cases of jaundice associated with thenon-steroidal anti-inflammatory drug benoxaprofen (’Opren’).Case .—An 82-year-old woman presented in September, 1981,
with a 1 week history of painless jaundice associated with pale stoolsand dark urine. Apart from osteoarthritis and mild hypertension shehad been in good health. Since February, 1981, her hypertensionhad been controlled by bendrofluazide 5 mg daily. Before July,1981, she had at different times used ibuprofen, fenoprofen, aspirin,and piroxicam for her osteoarthritis without adverse effect. On July13, 1981, benoxaprofen 600 mg at night was started, and 46 dayslater the patient noted jaundice. She also took quinine sulphate fornight cramps and ferrous sulphate had been prescribed in lateAugust, 1981, for an iron-deficiency anaemia. Examinationconfirmed jaundice, with mild hepatomegaly but no signs of liverfailure. Liver function tests are summarised in the table. The
LIVER FUNCTION TESTS ON ADMISSION IN THREE PATIENTS WITH
BENOXAPROFEN RELATED JAUNDICEI I I. I
external biliary passages were normal; there was no serologicalevidence for acute hepatitis A or B, cytomegalovirus (CMV)infection, or Epstein-Barr virus (EBV) infection; and there were nocirculating autoantibodies. On admission to hospital and with-drawal of all medication there was no immediate improvement inliver function, and renal function deteriorated. Urine cultureconfirmed an Escherichia coli infection. With rehydration andprednisolone and co-trimoxazole therapy renal function improvedand bilirubin, transaminase, and alkaline phosphatase values fellgradually. Iron deficiency was confirmed and demonstrated to bedue to a large duodenal ulcer. Steroids were discontinued after 2weeks with continued improvement in liver function thereafter.Case 2.-A 70-year-old woman was admitted in February, 1981,
with a 3 week history of jaundice with pale stools and dark urine.She had had osteoarthritis for many years. She also had exertional
angina pectoris, relieved by glyceryl trinitrate. She had taken
amylobarbitone or diazepam at night for several years.Benoxaprofen 600 mg at night had been started on Nov. 28, 1980,and jaundice was first noted 65 days later. There was no
7 Gill GV, Selkan JB, Mortimer PP Vandervelde EM Hepatitis B infection in formerprisoners of the Japanese Lancet 1980; ii: 918.
8 Wallace J, Milne GR, Barr A. Total screening of blood donations for Australia(hepatitis associated) antigen and its antibody. Br Med J 1972; i: 663-64.
9 Gill GV, Henry L, Reid HA. Chronic cardiac beriberi in a former prisoner of theJapanese. Br J Nutr 1980; 44: 273-74.
hepatomegaly and no clinical signs of liver failure. There wereclinical and radiological signs of an early right lower lobe
bronchopneumonia. Serological studies excluded acute infectionwith HBV, HAV, CMV, and EBV. The patient died from severebronchopneumonia 3 days after admission. At necropsy the
extrahepatic biliary system was normal.Case 3. -A 75-year-old woman was admitted to hospital on Feb. 15
with a history of anorexia and nausea for 4 weeks and jaundice withpale stools and dark urine for a week. She had osteoarthritisfor 6 years and mild congestive cardiac failure for 4 years. Onadmission she was taking amiloride and hydrochlorothiazide(’Moduretic’). She had previously been treated with indomethacin,phenylbutazone, and naproxen, but benoxaprofen 600 mg at nightwas started about 3 months before the onset of jaundice and wasstopped on admission to hospital. She had very occasionally usedquinine sulphate for cramps. There was mild, non-tenderhepatomegaly but no signs of liver failure; serological studies forHBV, HAV, CMV, and EBV infection were negative. Her jaundice
quickly resolved after admission and she was discharged home well.Histological findings (liver biopsy in cases 1 and 3, post mortem in
case 2) were similar. There was a moderately severe cannalicular andhepatocellular cholestasis, especially in the perivenular areas; somefoci of liver cell necrosis; an occasional acidophil body; a mildinflammatory reaction, predominantly lymphocytic and with
Kupffer cell hyperplasia; and the portal tracts contained a lightchronic inflammatory cell infiltrate.To the list of non-steroidal anti-inflammatory drugs associated
with occasional liver damage (aspirin, I phenylbutazone,2 2indomethacin,3 and ibuprofen4), benoxaprofen can probably nowbe added. In all three patients a similar mixed hepatitic/cholestaticlesion developed 1-3 months after they had started takingbenoxaprofen. Although the association remains to be establishedwe believe that caution should be exercised in prescribing thispreparation in the elderly, particularly where there is evidence ofhepatic or renal insufficiency.
Western Infirmaryand Gartnavel General Hospital,
Glasgow
Ballochmyle Hospital,Ayrshire
B. M. GOUDIEG. F. BIRNIEG. WATKINSONR. N. M. MACSWEEN
LOIS H. KISSENNANCY E. CUNNINGHAM
GASTRIC JUICE DISSOLVES RAZOR BLADES
SIR,-Mentally ill patients often swallow foreign bodies,including razor blades. Endoscopic removal of sharp objectsrequires a protective sheath outside the endoscope 5,6 and, therefore,considerable dexterity. Three cases where endoscopic removal wasdelayed or not possible have suggested an alternative method ofmanagement.
Case 1. -A 24-year-old schizophrenic who had swallowed a razorblade padded with bread refused endoscopy and spent an uneventfulweek in hospital. By court order, fibreoptic endoscopy was doneunder general anaesthesia on the eighth day. Corroded fragments ofthe blade were found in the stomach, but these crumbled whengrasped. He recovered-and subsequently ate fluorescent bulbs.Case 2.-A 24-year-old schizophrenic snapped a razor blade in
half widthwise. She heard a second snap as she swallowed one of thehalves. At endoscopy we found two pieces of blade in the stomach,
1. Russell AS, Sturge RA, Smith MA. Serum transaminases during salicylate therapy. BrMed J 1971, ii: 428-29.
2 Kuzell WC, Schaffarzick RE, Mangler WE, et al Phenylbutazone: Further clinicalevaluation Arch Intern Med 1953; 92: 646-61
3 Fenech FF, Bannister WH, Green JL. Hepatitis with biliverdinaemia in associationwith indomethacin therapy. Br Med J 1967; iii: 155-56.
4 Stempel DA, Miller JJ. Lymphopenia and hepatic toxicity with ibuprofen J Pediatr1977; 90: 657-58
5. Witzel L, Scheurer U, Muhlemann A, Halter F. Removal of razor blades from stomachwith fibreoptic endoscope Br Med J 1974; ii 539.
6. Martin WC, Jones SA, Nagai N, Texter EC, Jr. Fiberendoscopic removal of longforeign bodies from the stomach using a colon stiffening tube as a protective sheathAm J Gastroenterol 1979; 71: 505-07.

960
but, with the aid of a protective sheath, were able safely to removeonly one. She was put on a high bulk diet, and the other piece passedper rectum in 5 days.
Case 3. -A 34-year-old with a character disorder and suicidalideation broke a razor blade in half and swallowed one piece. Hewould not cooperate for endoscopy. The blade moved through thegastrointestinal tract without complication.These cases indicate that immediate removal of razor blades is not
mandatory and (case 1) that gastric secretions may even destroy.razor blades. I have tested this in vitro.
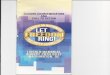
I exposed razor blades to 20 ml ofO 118 mol/1 hydrochloric acid inflasks on a shaking water bath (30 cycles/min, 37°C). After 2, 4, 6,and 8 h I replaced the fluid with 20 ml of fresh acid. At hour 10, Ireplaced the fluid with 50 ml of acid and incubated the blades for 14h more. Gastric juice was collected from three healthy individualsafter subcutaneous injection of pentagastrin. The combinedsecretions contained 0 104 mol/1 hydrochloric acid. I used the sameprotocol to incubate blades with gastric juice as with the acid.Hydrochloric acid damaged razor blades (figure). Gas .
(presumably hydrogen) bubbled from the blades and the pH rose.When blades were exposed to gastric juice the process was not sovigorous but gastric juice did dull the blade surface. After 10 and24 h incubation in gastric juice a ’Gillette Platinum-Plus’ blade hadlost 707o and 18% of its weight; for a ’Gillette Super Blue’ blade thesefigures were 2% and 12%, respectively.An ingested razor blade carries the dangers of gastrointestinal
haemorrhage, perforation or obstruction, and immediate removalby fibreoptic endoscopy is recommended. 7 Poor patientcooperation and the potential for injury as the blade is beingwithdrawn often preclude such treatment, however.
If X-rays show that the blade is in the stomach and if no complica-tions are evident, perhaps non-invasive management should beconsidered. The patient could be positioned on his left side to keepthe blade away from the duodenum and antacids should bewithheld. When X-rays indicate that the blade has left the stomachor has broken up, the patient could be given a high residue, highfibre diet.
This work, was supported by clinical investigator award AM 00927 from theNational Institutes of Health. I thank Dr George Thomas, Dr W. G. M.Hardison, and Dr Henry 0. Wheeler for their suggestions and for theirassistance in managing these patients. Dr H. Juergen Lenz kindly provided thegastric juice.
’
Division of Gastroenterology,Department of Medicine,University of California,San Diego School of Medicine,La Jolla, California 92093, U.S.A. DAVID E. HATOFF
7. Roseman DM Foreign bodies in the gut and upper airway. In: Sleisenger MH,Fordtran JS, eds. Gastrointestinal disease: Pathophysiology, diagnosis,management. Philadelphia. WB Saunders, 1978: 605-11.
Razor blades after incubation in 0 118 molH hydrochloric acid.
Blades were exposed to acid for 10 to 24 h. Con=control; BB = Gillette superblue blade (steel); PP =Gillette platinum-plus blade (stainless steel alloy).
INCORRECT USE OF PAKISTANI AND SIKH FEMALETITLES
SiR,-The incorrect use of the Pakistani titles Bibi and Begum andof the Sikh Kaur can lead to problems in patient identification andwith medical records. Bibi may be simply translated as lady; Begumis the equivalent of wife; and Kaur denotes a Sikh woman. The useof these words as surnames is usually incorrect and leads to misfilingof investigations and even confusion over surgical procedures.Between 1974 and 1981, 154 women with the surname Bibi, 149called Begum, and 158 called Kaur were admitted to hospitals inWales. Most of these admissions were in South Glamorgan andGwent, areas with large immigrant populations. The use of Bibi,Begum, or Kaur as first names is also common, though confusion inthe files is less likely than it is when female titles are written down a;’surnames.
Royal Gwent Hospital,Newport, Gwent
MAHMOOD SHAFI
JOHN MAYBERRY
SALICYLAZOBENZOIC ACID IN ULCERATIVECOLITIS
SIR,-Jewell and Truelove’s experience with disodium
azodisalicylate in the treatment of ulcerative colitis prompts us toreport our results with salicylazobenzoic acid (HB-313). The side-effects of sulphasalazine are mainly due to the sulphapyridinemoiety,2 so salicylazobenzoic acid may cause fewer side-effects.Furthermore, the active metabolite, 5-aminosalicylic acid, wasliberated by bacteria in the colonic lumen faster from this newcompound than from sulphasalazine when both were given tohealthy human volunteers orally or as an enema (unpublished).In our first study seven males and six females (aged 23-78) with
active ulcerative colitis were treated with one retention enema
containing 2 g salicylazobenzoic acid (equivalent to about 3 gsulphasalazine) daily for 8-16 days. No other relevant drugs weregiven, in contrast to the study of Jewell and Truelove where four ofthe five patients took oral sulphasalazine as well as the azodi-salicylate enemas. Patients were assessed clinically and
rectoscopically before and after treatment. Significant clinical
improvement (fewer stools, less blood in stools, and the patients’subjective impression) was found in nine patients, slightimprovement in two, and no change in the remaining two. Thispattern correlated with improvements in rectoscopic appearances.Of three patients examined histologically, two showed marked andthe other slight improvement.Encouraged by these preliminary results we did a crossover study
comparing salicylazobenzoic acid and sulphasalazine enemas in tenpatients whose attacks of ulcerative colitis were usually severe (fivemales, five females, age range 24-68).
In four patients treated with salicylazobenzoic acid for 18-21days followed, after a break of 5-7 days, by sulphasalazine for thesame period, and in two cases treated in reverse order, the new drugwas more effective than sulphasalazine (p<0-05). One patient’scolitis worsened when sulphasalazine followed salicylazobenzoicacid. In one case evaluation was not possible because surgery provednecessary. One patient did not respond to either compound.Sulphasalazine was curative in only two patients whereas in seven itwas not very effective. Salicylazobenzoic acid enemas were welltolerated by all patients and no side-effects were encountered.Our preliminary results suggest that further trials of
salicylazobenzoic acid in the treatment of ulcerative colitis arewarranted.
Department of Surgery,Allgemeine Poliklinikder Stadt Wien,
1090 Vienna, Austria A. BARTALSKY
1. Jewell DP, Truelove SC. Disodium azodisalicylate in ulcerative colitis. Lancet 1981; ii:1168.
2. Azad Khan AK, Piris J, Truelove SC. An experiment to determine the activetherapeutic moiety of sulphasalazine. Lancet 1977; ii: 892-95.