Embed Size (px)
Citation preview
Normal
Superficial Ulceration
Stomach join has krept up the oesophagus by aprox 7cm. So 2/3 of oesophagus is covered by stomach. This shows Barrett’s Oesophagus
Alimentary Laila Hasan
Gastro-oesophageal Reflux Disease (GORD)
Definitions:
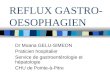
Hiatus hernia: anatomical abnormality with part of stomach in the chest – usually asymptomatic. The stomach normally herniates through the diaphragm into the chest.
Gastro-oesophageal reflux- reflux of gastric contents up into the oesophagus which can occur normally with no symptoms
Gastro-oesophageal reflux disease (GORD) – damage and/or symptoms due to reflux of gastric fluid. It is important to note that presentation of symptoms may not occur!
Also important to note is that A normal endoscopy does not exclude GORD:
– 50-60% of patients with GORD will have no oesophagitis ie a normal endosocpy =‘endoscopy negative refluxers’
This mmeans you may get very bad symptoms but not any results on the endoscopy, so the test and presentation of symptoms and underlying pathology do not correlate well.
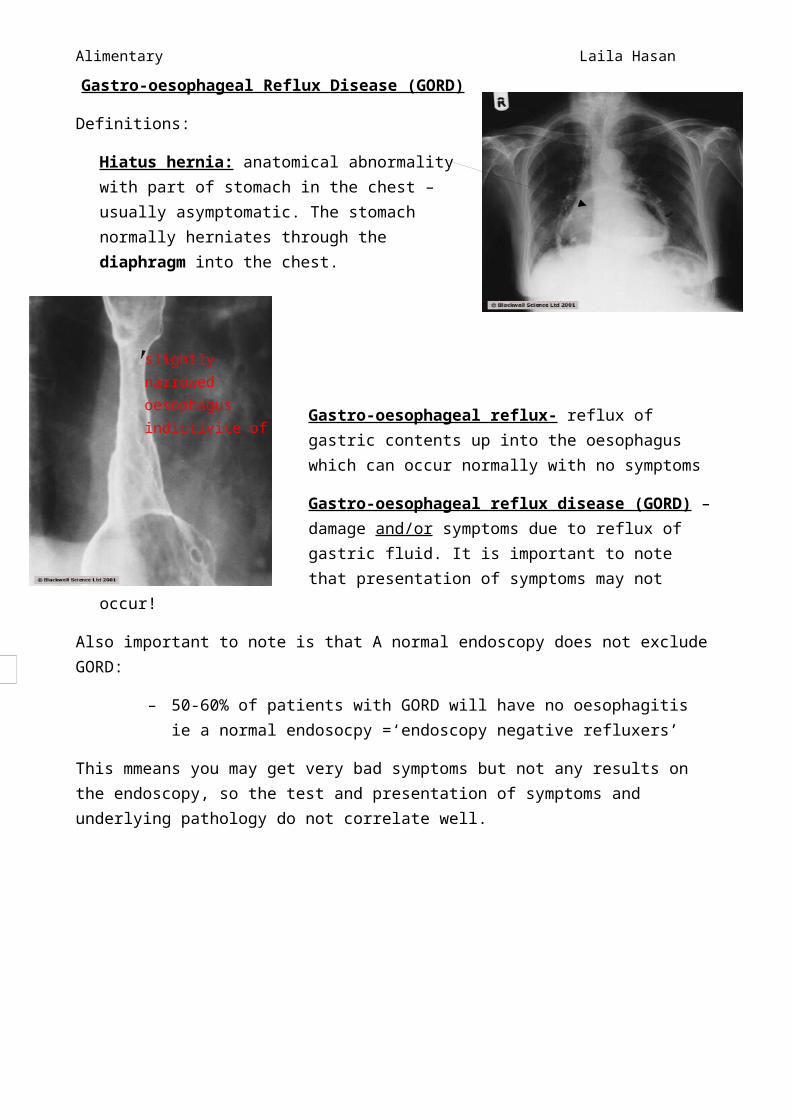
Reflux oesophagitis – inflammation of the lower oesophagus produced by persistent episodes of reflux – may be asymptomatic
slightly narrowed oesophagus indictivite of reflux disease
Reflux oesophagitis

Alimentary Laila Hasan
Barrett’s oesophagus – presence of intestinal metaplastic columnar epithelium which has replaced squamous epithelium due to acid reflux (or repetitive acid contact). This is a premetaplasmic state.
Epidemiology
GORD = 5-8% in the British PublicHeartburn = 30-60%
The findings when dyspepsia(bad digestion with complex symptoms such as bloating, epigastric pain, chest pain and nausea) is diagnosed by Rapid access endoscopy are:20% oesophagitis, 7-10% duodenal ulcer, 5% gastric ulcer.
PATHOPHYSIOLOGY:Reflux of small amounts of gastric contents is normal BUT in GORD = there are frequent, prolonged, large amounts and / or damage because anti-reflux mechanisms fail
In the normal physiology there are a number of different mechanisms to prevent reflux. These are:1. Lower oesophageal sphincter (LOS) –intra-abdominal and thoracic portion which is 4cm
segment of smooth muscle (there is one in the upper oesophagus but this is less utilised). It is a high pressure zone of muscle contraction which normally relaxes on swallowing to allow food through and regains tone to prevent reflux. It can increase in tone in response to rises in gastric and abdominal pressure.
2. Intra-abdominal segment acts as flap valve3. Mucosal rosette formed by gastric folds occlude gastro-oesophageal junction4. Contraction of crural diaphragm has a pinchcock-like action at LOS5. Rapid clearance of content from oesophagus by peristalsis that makes acid go distally to the
stomach.
The Proposed mechanisms that lead to GORD are:
1. Transient LOS relaxation episodes (This can be spontaneous and more susceptible at daytime)
2. Low resting tone in LOS which fails to increase when patient lies flat which it would normally (Patients often sleep with many pillows to relieve the reflux as the intra abdo pressure increases)
3. LOS tone fails to increase when gastric or abdo pressure increases 4. Increased oesophageal mucosal sensitivity to acid5. Delayed gastric emptying eg. in diabetes6. Prolonged episodes of GOR which occur at night and postprandially 7. Reduced oesophageal clearance of acid due to poor peristalsis or ‘trapping’ acid in hiatus
hernia8. A large hiatus hernia can impair crural diaphragm pinchcock effect as it prevents the
diaphragm from pinching LOS.
Exacerbating factors Smoking

Alimentary Laila Hasan
Alcohol Pregnancy Obesity Exertion Posture – stooping or lying flat Drugs : NSAIDS (directly irritate the oesophagus mucosa), nitrates (relax the smooth
muscle of oesophagus so reflux is no longer inhibited) and muscle relaxants Large meals, fat, chocolate, coffee Hiatus hernia Systemic sclerosis
Most diagnostics are based on gaining a good history and not by clinical tests:
as abdo pressure increases
This can occur as acid can cause trouble higher up the oesoph, causing irritation.

There are squamous islands still residing as the normal oesophagus lining but the mass has been replaced by columnar epithelium.
Alimentary Laila Hasan
Achalasia: Lower chest discomfort and chest pain. The oesophagus does not relax, which is different from GORD
The complications of GORD are: Reflux oesophagitis = 60% Of those with oesophagitis: Barrett’s = 10% (adenocancer risk 40-
100x) Stricture = 4-20% Ulceration = 5% Bleeding = <2%
What is Barrett’s oesophagus?• Columnar epithelium with intestinal metaplasia transformation of squamous lining of lower
oesophagus due to reflux. It is important to note that the reflux could be bile or pancreatic in nature and not just acid reflux.
• Premalignant• Most people with it will die of other diseases• Surveillance endoscopy to detect dysplasia?
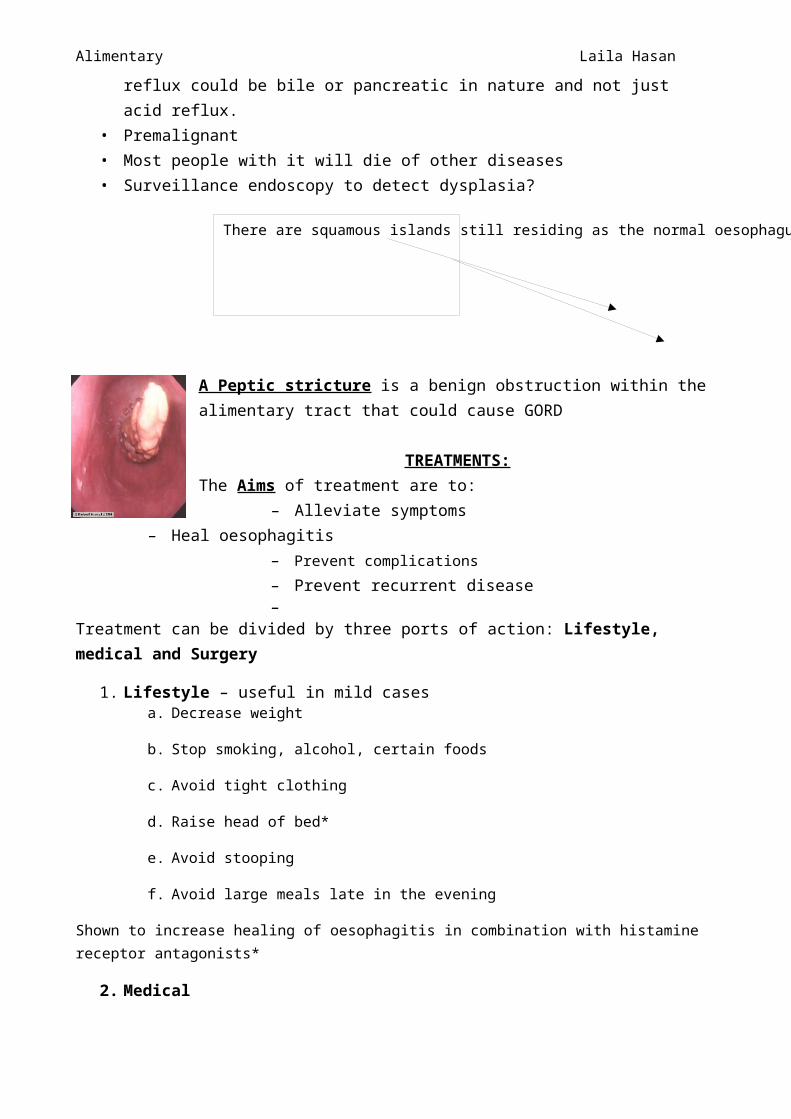
Barrett’s complicated by adenocarcinoma

Alimentary Laila Hasan
A Peptic stricture is a benign obstruction within the alimentary tract that could cause GORD
TREATMENTS:The Aims of treatment are to:
– Alleviate symptoms– Heal oesophagitis – Prevent complications– Prevent recurrent disease –
Treatment can be divided by three ports of action: Lifestyle, medical and Surgery
1. Lifestyle – useful in mild cases a. Decrease weight
b. Stop smoking, alcohol, certain foods
c. Avoid tight clothing
d. Raise head of bed*
e. Avoid stooping
f. Avoid large meals late in the evening
Shown to increase healing of oesophagitis in combination with histamine receptor antagonists*
2. Medicala. Antacids and alginates : good for relief of reflux symptoms: magnesium trisilicate and
aluminium hydroxide or gaviscon
i. Little evidence that they are better than placebo
ii. No evidence of oesophagitis healing
b. H2RA: reflux symptoms are controlled in 80% after 6-8 weeks. (cimetidine, ranitidine)
c. Healing depends on dose, frequency and grade (I-V)
i. Overall 50% healed after 6-8 weeks
ii. Grade I = 80%, Grade III = 20% at 8 weeks
iii. Control of symptoms doesn’t = healing
d. Prokinetics: help emptying and clearing of oesophagus
i. eg. metoclopramide,
ii. domperidone
iii. cisapride)They have been found to be better than placebo in controlling symptoms, BUT there is little evidence that they heal oesophagitis
Alimentary Laila Hasan
e. Protein Pump Inhibitos (PPIs) – omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole – all inhibit gastric hydrogen pump which stops gastric acid production.
i. Most effective medical treatment (healing rates >80% over 8weeks)ii. Excellent symptom relief
iii. Relief of symptoms good predictor of endoscopic healingiv. Effective for all grade of oesophagitis v. Effective for resistant oesophagitis
vi. Prevents complicationsvii. Safe, few adverse side effects
3. Surgicala. Endoscopic (induce a ‘controlled’ stricture)
i. Stitch (sewing maching device)ii. Radiofrequency damage of LOS
iii. Injection of compounds into LOS1. All to be evaluated longterm
b. Surgicali. Laproscopic or open WRAP (Nissen fundoplication) This is the tightening of
the lower valve and are for those people who have low oesophagus sphincter tone and don’t want to be on PPIs.
1. As good as longterm PPI and prevent complications?2. Cheaper than longterm PPI?
Initial Managment
Typical symptoms – no sinister symptoms and patient <45years oldTrial of treatment without initial investigation – step up or step down approach
Step up : lifestyle, antacids/alginates, H2RA, prokinetics, PPIsStep down : lifestyle + PPIs and decrease according to response
Patient assessed at 6-8 weeks- success of Rx based on symptom relief. If still symptomatic consider investigation
Who to Investigate?
• Sinister symptoms• Diagnosis unclear• Fails to respond to treatment after 6-8wks• Relapses quickly• >45 years of age with recent onset symptoms?
Post endoscopy managementIf the Endoscopy shows:
• Oesophagitis + grade – commence medical treatment • Complications :
• stricture – dilate (medical Rx increase or surgical)

Alimentary Laila Hasan
• Barrett’s – medical, endoscopic, surgical treatment – consider surveillance until 75 years of age
• Consider surgery in certain circumstances for long term problems or failure to improve on medical treatment but always need pH and manometry before proceeding. (Manometry is when a tube with pressure sensors goes through the nose down to the stomach. The patient is asked to swallow causing peristalsis occurs and a reading is obtained of the pressure on the valves which is then projected into a graph).
If the Endoscopy shows:• Normal – no oesophagitis but story good for reflux (endoscopy negative refluxer?)• then undergo a Manometry and 24 pH studies. (A pH study involves the same sort of tubing
down the oesophagus into the stomach but instead of pressure sensors the acid content is measured over a 24 hour period. At the same time the patient is asked to note down any symptoms they feel and note the date and time of those symptoms. Once the study is complete you can correlate whether the symptoms correspond to increased gastric pH at that time or the symptoms were not due to increased pH. You can therefore define whether a patient needs to be treated just for the symptoms and not the cause of increased gastric secretion.)