Embed Size (px)
Citation preview

Gastroscopy per gastrostomyAnother indication for the use of a small diameterflexible fiberoptic endoscope
Wallace A. Gleason, Jr., MDRichard K. Danis, MD
St. Louis, Missouri
Seven fiberoptic examinations of the upper gastrointestinal tract wereperformed through gastrostomies in 5 patients. In 3 of 4 attempts, astring was recovered from the stomach, allowing guided esophagealdilation. The technique permits limited examination of the gastricmucosa with a minimum of anesthesia. Disadvantages include inabilityto examine the esophagus and difficulty in advancing the instrument tothe pylorus. Complications were limited to minor fissures at the stoma."Gastroscopy per gastrostomy" is another indication for the use of smallcaliber fiberoptic endoscopes.
The use of specially designed, small caliber, flexible, fiberoptic endoscopes has been the subject of a number of recentreports.1-8 This paper describes a novel indication for the use
of the small endoscopes: examination of the upper gastrointestinal tract through a gastrostomy.
In 1975, 5 patients were examined a total of 7 times usingthis method. (Table I). Two had esophageal strictures resultingfrom lye ingestion. Three had tracheosophageal fistula andesophageal atresia. Their ages ranged from 2 months to 3years. Indications for examination included recovery of the
distal end of a string passed to guide an esophageal dilator (4examinations,3 patients), gastric outlet obstruction (2 examinations, 2 patients) and upper gastrointestinal bleeding (1examination).
METHODS Five of the 7 examinations were done with seda
tion only. Preparation for these examinations consisted of a 4to 6 hour fast, administration of atropine sulfate (0.01 mglkg)
intramuscularly 15 to 30 minutes before examination, and asmall intravenous dose of diazepam (1 mg to 5 mg) just
preceding the examination. Two children were studied
through gastrostomies while under general anesthesia foresophagoscopy and passage of a guide string through a
nonflexible esophagoscope.
A recently developed pediatric endoscope (Olympus GIF-P)was used in all cases. The tip of the endoscope (diameter 7.2mm) was usually easily passed into the stoma. Two casesrequired dilation of the gastrostomy stoma with Hegar di lators.In 1 case, adequate dilation of the stoma was achieved by
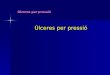
Table I.Summary of patients studied "per gastrostomy"
patient age diagnosis indication findings
1 (MC) 3 months TEF* gastric outlet antralobstruction ulceration
2 (PS) 3 years lye ingestion, stri ng recoverystricture stri ng recovery
3 (EH) 17 months TEF, colonic gastric outlet normal mucosainterposition obstruction extrinsic
obstruction
18 months stricture at altempt to pass unable tocologastric string for enter colonicanastomosis dilation segment
4 (SP) 3 years lye ingestion, bleeding no abnormalitiesstricture
5 (CH) 2 months TEF string removed
*TEF = tracheoesophageal fistula with esophageal atresia
76
From the Departments of Pediatrics and Surgery, St. Louis University School of Medicine andCardinal Glennon Memorial Hospital, SI. Louis, Missouri. Reprint requests: Wallace A.Gleason, Jr., MD, Department of Pediatrics, SI. Louis University School of Medicine, 1465 S.
Grand Blvd., SI. Louis, Missouri 63104.
GASTROINTESTINAL ENDOSCOPY

progressively increasing the size of the gastrostomy tube overthe course of a week before study.
In the 4 examinations done to recover the distal end of astring from the stomach, the string was located and graspedwith the biopsy forceps. The endoscope was then withdrawnfrom the stomach and the string thus delivered to the exterior.Rotating the endoscope and winding the string around thebiopsy forceps before its withdrawal prevented loss of thestring.RESULTS Good visualization of most of the gastric mucosawas obtained in all cases. However, complete examination ofthe stomach, particu larly of those areas closest to the gastrostomy site, was not always accomplished. Three of 4 procedures performed for string recovery were successful. In 2patients studied because of gastric outlet obstruction, 1 hadantral ulceration and 1 had extrinsic obstruction, later founddue to adhesions. One patient with a long esophageal stricturecaused by lye ingestion presented because of gastrointestinalbleeding and was found to have normal antral and duodenalmucosa. The esophagus was entered from below demonstrating severe deformity and stricture formation but no bleedinglesions. An attempt to enter the esophagus from below inanother patient was unsuccessful because of the proximity ofthe gastrostomy to the gastroesophageal junction. Leakage ofinsufflated air through the gastrostomy was considerable butdid not prevent adequate distention of the stomach.
The procedure was well tolerated by all patients. In 1 casefissures of the stoma were noted secondary to dilation of thegastrostomy.
DISCUSSION Retent advances in the design of endoscopicinstruments have resulted in the availability of small caliberfiberoptic endoscopes which have been used successfully forgastrointestinal endoscopy in infants and children8 and inadults for situations requiring small instruments, e.g.,esophageal or pyloric strictures, partially obstructi ng masses. 9
Our experience indicates that "gastroscopy per gastrostomy"is another indication for the use of such instruments. Previous
REFERENCES1. FREEMAN NV: Clinical evaluation ofthe fiberoptic bronchoscope (Olympus
BF5B) for pediatric endoscopy.! Pediat Surg. 8:213, 19732. GRAHAM DY, SCHWARTZjT: Endoscopic removal of a knotted feed ing tu be
from an infant. Gastrointestinal Endoscopy 21 :32, 19743. CREMER M, PEETERS jP, EMONTS P, RODESCH P, CADRANEL 5: Hberendos
copy of the gastrointestinal tract in children; experience with newly designed fiberscope. Endoscopy 6: 186, 1974
4. ARMSTRONG MAM, MINTZ AA: Method for removing a knotted nasogastric feeding tube in an infnnt.! Pediat 85:732, 1974
5. GLEASON WA, TEDESCO F], KEATING jP, GOLDSTEIN PD: Fiberopticgastrointestinal endoscopy in infants and children.! Pediat 85:810,1974
6. GANS SL, AMENT M, CHRISTIE DL, LEIBMAN WM: Pediatric endoscopywith flexible fiberscopes.! Pediat Surg 10:375, 1975
VOLUME 23, NO.2, 1976
gastroscopic examinations through gastrostomies have usedfiberoptic bronchoscopes,'o requiring air insufflation througha syringe to achieve gastric distention, or larger diameter (10mm) endoscopes, necessitating dilation of the stoma toachieve passage of the endoscope.,,·12 The use of the newthinner panendoscope avoids both problems in most cases.
Although our patients were children, the technique isequally applicable to adults. As the instrument does not haveto be passed through the oropharynx, minimal anesthesia orsedation is required.
Limitations of the method are largely mechanical. Thegastrostomy, of course, must be patulous enough to accommodate the endoscope (7.2 mm, 22 French). The greaterlength of the instrument that remains outside the patient issometimes unwieldy. The proximity of the gastrostomy to thegastroesophageal junction, especially in small children, frequently prevents entry into the esophagus. Examination of theantrum and more distal structures requires extreme deflectionof the tip of the endoscope after entering the gastrostomy.Advancement towards the pylorus under such conditions isdifficult. Gastric mucosa closest to the gastrostomy site isseldom seen with this technique. Because of these limitations,this technique is not well suited to diagnostic examinations inthe absence of esophageal obstruction.
The technique offers the most promise in the managementof esophageal strictures caused by lye ingestion, peptic disease, or as a resu It of surgical operation for tracheoesophagealfistula associated with esophageal atresia. On 3 occasions, wewere able to bring a string, passed to guide esophagealdilators, through the gastrostomy to be anchored on theanterior abdominal wall.
Our observations suggest that further refinements in instrumentation and technique will be worthwhile in increasingthe usefulness of "gastroscopy per gastrostomy."
ACKNOWLEDGEMENTThe authors are grateful to Mrs. Catherine Camp for assistance in preparation
of this manuscript.
7. GiLAT T, ROZEN P: Fiberoptic endoscopic diagnosis and treatment of acongenital esophageal diaphragm. Am! Dig Dis 20:781, 1975
8. TEDESCO F], GOLDSTEIN PD, GLEASON WA, KEATING jP: Upper gastrointestinal endoscopy in the pediatric patient. Gastroenterology 70:492, 1976
9. COTTON PB: A thinner panendoscope (Olympus PDF) (Abstract).Gastrointestinal Endoscopy 20:177, 1974
10. lIGHTDALE C], POSNER G, SHERLOCK P, WINAWER 51: Fiberoptic stomoscopy. Gastrointestinal Endoscopy 19:198, 1973
11. SCHAPIRA L, FALKENSTEIN DB, ZIMMON DS: Endoscopy and retrogradecholangiography via gastrostomy. Gastrointestinal Endoscopy 22:103,1976
12. HENTSCHEL E, DITTRICH H, WEISS W: Retrograde oesophagoscopy viagastrostomy. Endoscopy 8:38, 1976
77