Embed Size (px)
Citation preview
2/21/2017
1
© 2017 MMIC. All rights reserved
Malpractice Concerns in the New Healthcare World
Robert S. Thompson RT, JD, MBA, LLM, RPLU, CPCU
Director of Education - MMIC
Copyright 2014 MMIC • All rights reserved
Different pic
© 2017 MMIC. All rights reserved
Medical malpractice
• Duty • Breach of duty (standard of care) • Injury caused by breach • Damages • Malpractice plus (x-factor)
– Service lapses – Non-clinical issues – Plaintiff attorney’s dream
© 2017 MMIC. All rights reserved
Today’s environment
• Claims frequency stable • Claims severity
on the rise • 1 in 4 jury verdicts
exceeds $1.2 million • The “x-factor”
will continue the severity trend
© 2017 MMIC. All rights reserved
2/21/2017
2
© 2017 MMIC. All rights reserved
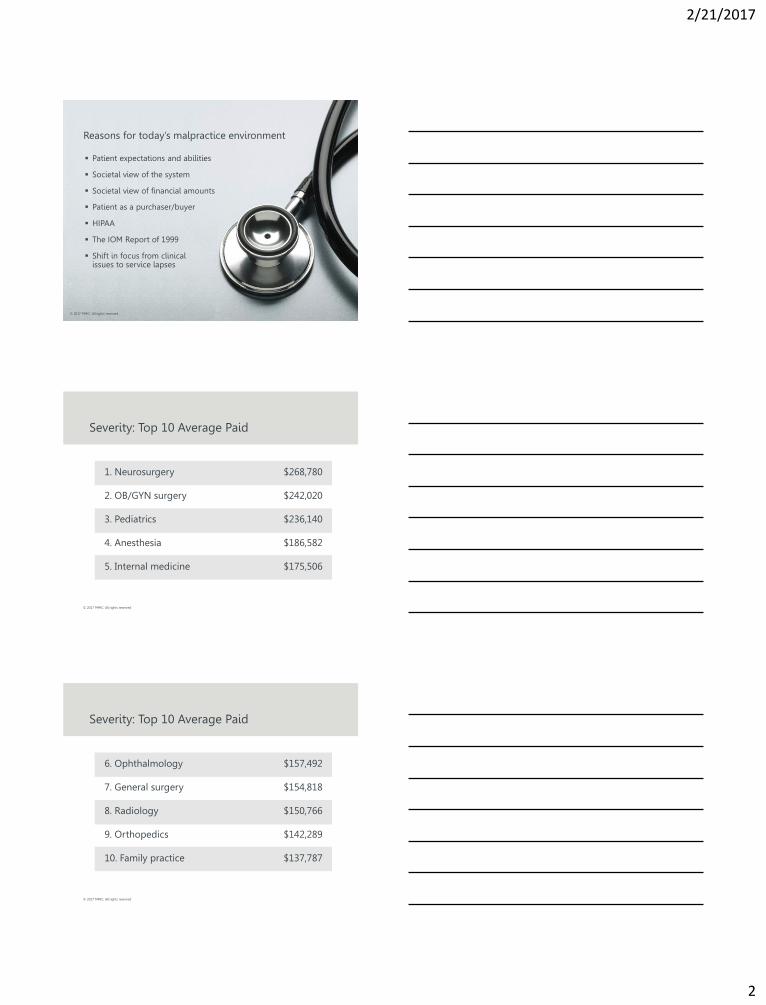
Patient expectations and abilities
Societal view of the system
Societal view of financial amounts
Patient as a purchaser/buyer
HIPAA
The IOM Report of 1999
Shift in focus from clinical issues to service lapses
Reasons for today’s malpractice environment
© 2017 MMIC. All rights reserved
© 2017 MMIC. All rights reserved
Severity: Top 10 Average Paid
1. Neurosurgery $268,780
2. OB/GYN surgery $242,020
3. Pediatrics $236,140
4. Anesthesia $186,582
5. Internal medicine $175,506
© 2017 MMIC. All rights reserved
Severity: Top 10 Average Paid
6. Ophthalmology $157,492
7. General surgery $154,818
8. Radiology $150,766
9. Orthopedics $142,289
10. Family practice $137,787
2/21/2017
3
© 2017 MMIC. All rights reserved
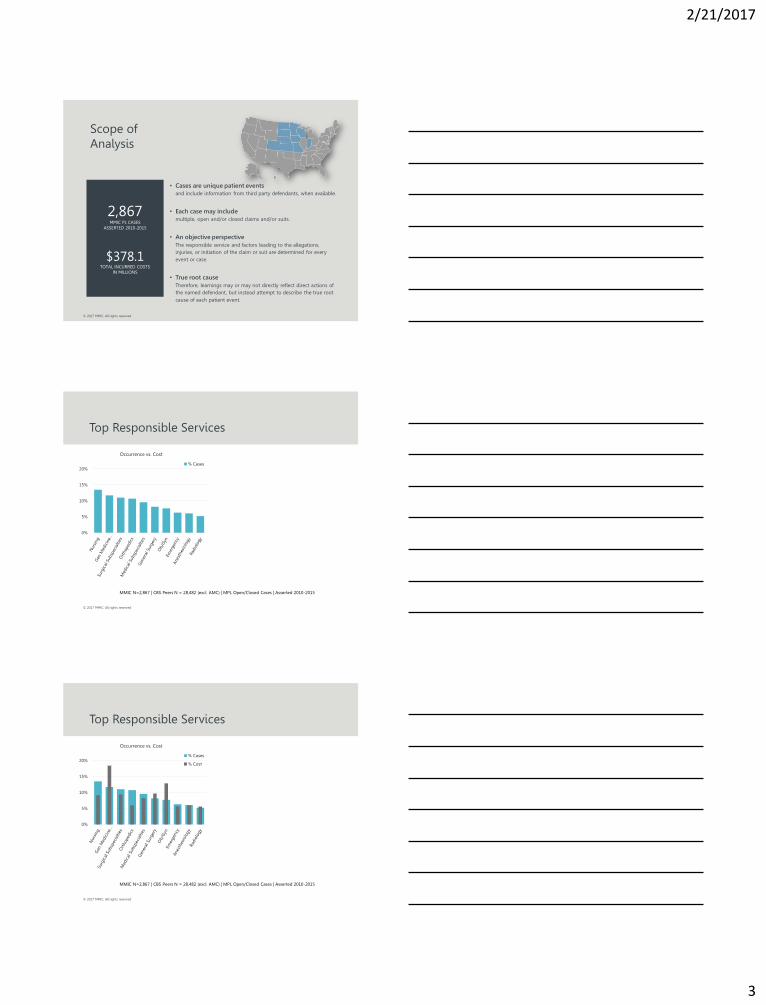
Scope of Analysis
• Cases are unique patient events and include information from third party defendants, when available.
• Each case may include multiple, open and/or closed claims and/or suits.
• An objective perspective The responsible service and factors leading to the allegations, injuries, or initiation of the claim or suit are determined for every event or case.
• True root cause Therefore, learnings may or may not directly reflect direct actions of the named defendant, but instead attempt to describe the true root cause of each patient event.
2,867 MMIC PL CASES
ASSERTED 2010-2015
$378.1 TOTAL INCURRED COSTS
IN MILLIONS
© 2017 MMIC. All rights reserved
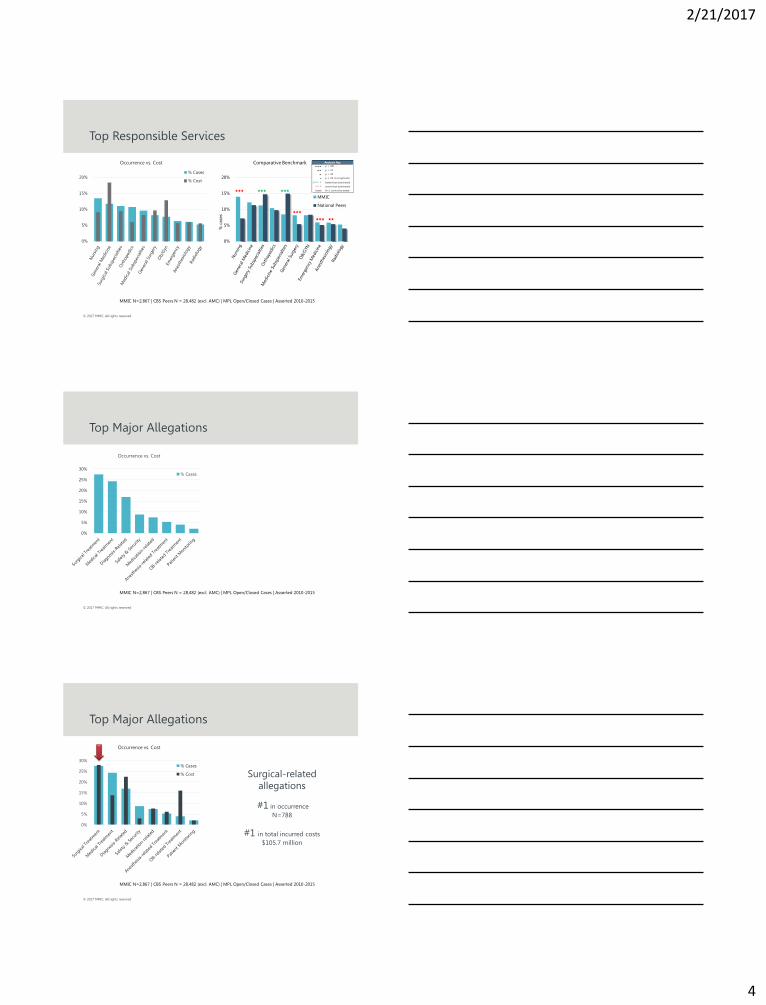
Top Responsible Services
0%
5%
10%
15%
20%
Occurrence vs. Cost
% Cases
% Cost
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
© 2017 MMIC. All rights reserved
Top Responsible Services
0%
5%
10%
15%
20%
Occurrence vs. Cost
% Cases
% Cost
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
2/21/2017
4
© 2017 MMIC. All rights reserved
Top Responsible Services
0%
5%
10%
15%
20%
% c
ase
s
Comparative Benchmark
MMIC
National Peers
0%
5%
10%
15%
20%
Occurrence vs. Cost
% Cases
% Cost
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
p < .001
p < .01
p < .05
p ≥ .05 (not sigificant)
green better than benchmark
red worse than benchmark
blank N<5, cannot be tested
Analysis Key
© 2017 MMIC. All rights reserved
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
0%
5%
10%
15%
20%
25%
30%
Occurrence vs. Cost
% Cases
% Cost
© 2017 MMIC. All rights reserved
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
0%
5%
10%
15%
20%
25%
30%
Occurrence vs. Cost
% Cases
% Cost Surgical-related
allegations
#1 in occurrence
N=788
#1 in total incurred costs
$105.7 million

2/21/2017
5
© 2017 MMIC. All rights reserved
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
0%
5%
10%
15%
20%
25%
30%
Occurrence vs. Cost
% Cases
% Cost Diagnosis-related
allegations
#3 in occurrence
N=484
#2 in total incurred costs
$84.7 million
© 2017 MMIC. All rights reserved
Top Major Allegations
0%
5%
10%
15%
20%
25%
30%
Occurrence with Benchmark
MMIC
National Peers
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
0%
5%
10%
15%
20%
25%
30%
Occurrence vs. Cost
% Cases
% Cost
p < .001
p < .01
p < .05
p ≥ .05 (not sigificant)
green better than benchmark
red worse than benchmark
blank N<5, cannot be tested
Analysis Key
© 2017 MMIC. All rights reserved
Allegations by Claimant Type
MMIC N=2,867 | Asserted 2010-2015 | OP N=1445 | ED N=239 | IP N=1159
0%
10%
20%
30%
40%
50%
Emergency Allegations
N=239
0%
10%
20%
30%
40%
50%
Inpatient Allegations
N=1,159
0%
10%
20%
30%
40%
50%
Outpatient Allegations
N=1,445
Outpatient
50%
ED
[PERCENTAGE]
Inpatient
41%

2/21/2017
6
© 2017 MMIC. All rights reserved
Inpatient vs. Outpatient/ED
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2013 2014 2015
% C
ase
s
Assert Year
MMIC National Peers
Outpatient
+ ED
Inpatient
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
Outpatient
50%
Emergency
8%
Inpatient
41%
Other
1%
Claimant Type
© 2017 MMIC. All rights reserved
Outpatient Cases, N=1,445
MMIC Outpatient Claimants N=1,445 | Asserted 2010-2015
0%
10%
20%
30%
40%
50%
Allegations
Medium
60%
High
22%
Low
18%
Injury Severity
NAIC Clinical Severity Scale
HIGH death, perm grave, perm major/sig
MED perm/temp minor, temp major
LOW temp insignificant, emotional/legal only
Responsible Services % OP
Gen Medicine 17%
Surgical Subspecialties 14%
Medical Subspecialties 13%
Orthopedics 10%
Nursing 8%
Radiology 7%
General Surgery 6%
Anesthesiology 6%
Current Focus:
Diagnostic Error and follow-up
system failures
© 2017 MMIC. All rights reserved
Outpatient Claims
MMIC N=1,455 | MPL Open/Closed Cases | Asserted 2010-2015
• Failure/delay to order dx test and to respond
to repeated patient concerns/symptoms
• Misinterpretation of diagnostic studies
• Narrow diagnostic focus
Clinical Judgment
• Known risks, poor technique, improperly
utilized equipment, inexperience with
procedure
Technical Skill
• Communication with pt and family (21%)
• Communication among providers (10%) Communication
50%
46%
30%

2/21/2017
7
© 2017 MMIC. All rights reserved
Patient communication
In virtually all specialties, communication errors or barriers are the main factors resulting in medical malpractice claims, second only to errors of clinical judgment or technical error (actual malpractice)
© 2017 MMIC. All rights reserved
Patient communication
The major national risk management and patient safety trade organizations (ASHRM, NPSF, NAHQ, AMA) are focusing educational efforts on communication and culture – the “soft sciences” of health care
© 2017 MMIC. All rights reserved
Even in high-risk,
procedure-based
specialties,
communication
is a big factor.

2/21/2017
8
© 2017 MMIC. All rights reserved
• Substandard judgment 77%
• Miscommunication 36%
• Technical error 26%
• Inadequate
documentation 26%
• Administrative failures 23%
Biggest contributors to OB claims
© 2017 MMIC. All rights reserved
• Technical skill 67%
• Clinical judgment 62%
• Communication 33%
Biggest contributors to surgical claims
© 2017 MMIC. All rights reserved
Communication and teamwork issues
are named as a root cause in nearly
of all sentinel events. 70%
2/21/2017
9
© 2017 MMIC. All rights reserved
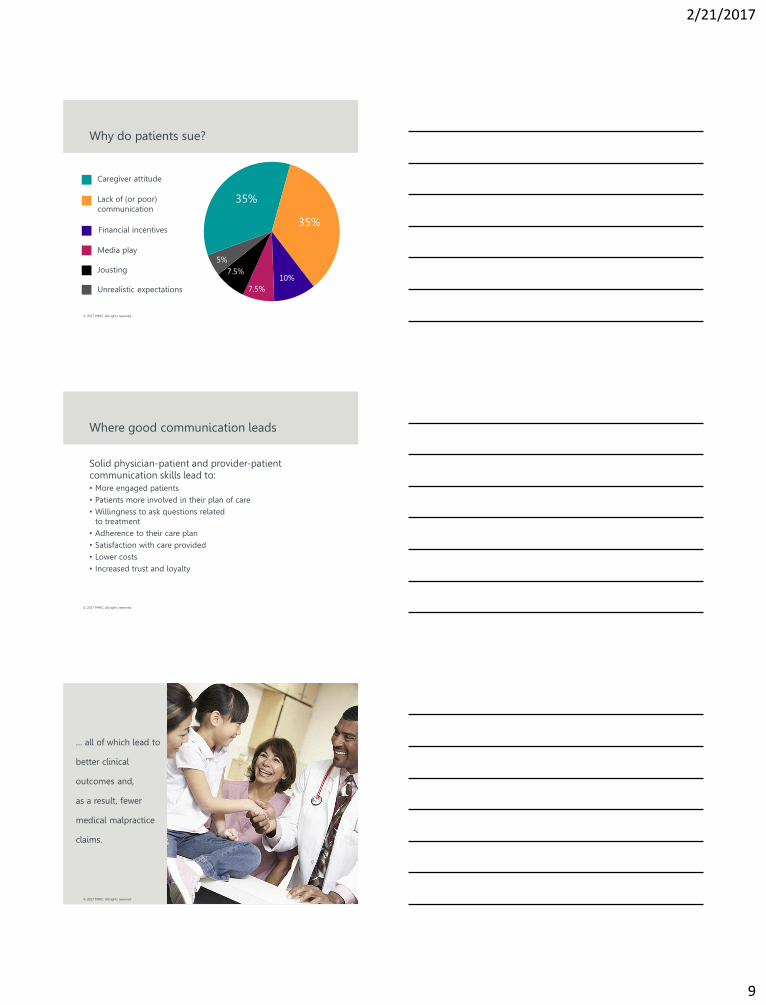
Why do patients sue?
Caregiver attitude
Lack of (or poor)
communication
Financial incentives
Media play
Jousting
Unrealistic expectations
35%
35%
10%
7.5%
7.5%
5%
© 2017 MMIC. All rights reserved
Where good communication leads
Solid physician-patient and provider-patient communication skills lead to: • More engaged patients • Patients more involved in their plan of care • Willingness to ask questions related
to treatment • Adherence to their care plan • Satisfaction with care provided • Lower costs • Increased trust and loyalty
© 2017 MMIC. All rights reserved
… all of which lead to
better clinical
outcomes and,
as a result, fewer
medical malpractice
claims.

2/21/2017
10
© 2017 MMIC. All rights reserved
Patients are changing
More prepared through research
More medically savvy
More challenging of medical opinions
More “consumer” than patient
© 2017 MMIC. All rights reserved
Build rapport/set the tone
• Be prepared • Greet the patient • Make eye contact • Shake hands • Introduce yourself (to everyone in the room) • Use the patient’s (parent’s) name • Learn everyone’s role • Smile and be pleasant • Make small talk
© 2017 MMIC. All rights reserved
Build rapport/set the tone
• Attend to the patient’s comfort • Acknowledge the wait, if any • Convey knowledge of patient history • Sit down (it makes a difference!) • Maintain eye contact • Explain need to enter information in EHR
2/21/2017
11
© 2017 MMIC. All rights reserved
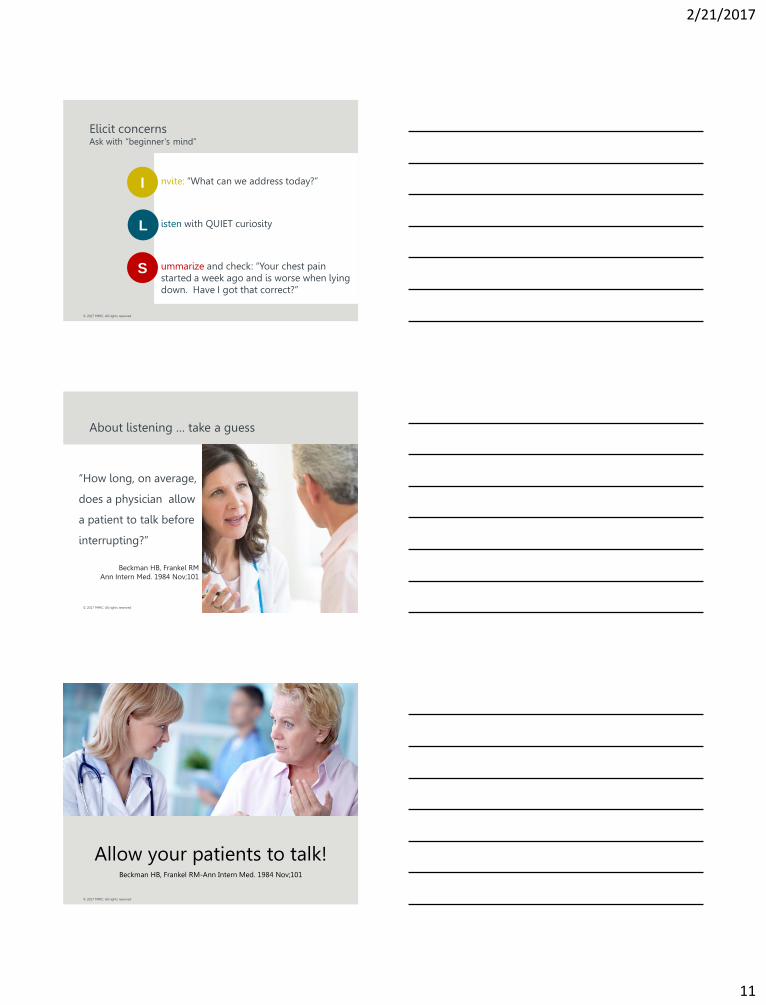
nvite: “What can we address today?” isten with QUIET curiosity ummarize and check: “Your chest pain started a week ago and is worse when lying down. Have I got that correct?”
Elicit concerns Ask with “beginner’s mind”
I
L
S
© 2017 MMIC. All rights reserved
About listening … take a guess
“How long, on average,
does a physician allow
a patient to talk before
interrupting?”
Beckman HB, Frankel RM
Ann Intern Med. 1984 Nov;101
© 2017 MMIC. All rights reserved
Allow your patients to talk! Beckman HB, Frankel RM-Ann Intern Med. 1984 Nov;101
2/21/2017
12
© 2017 MMIC. All rights reserved
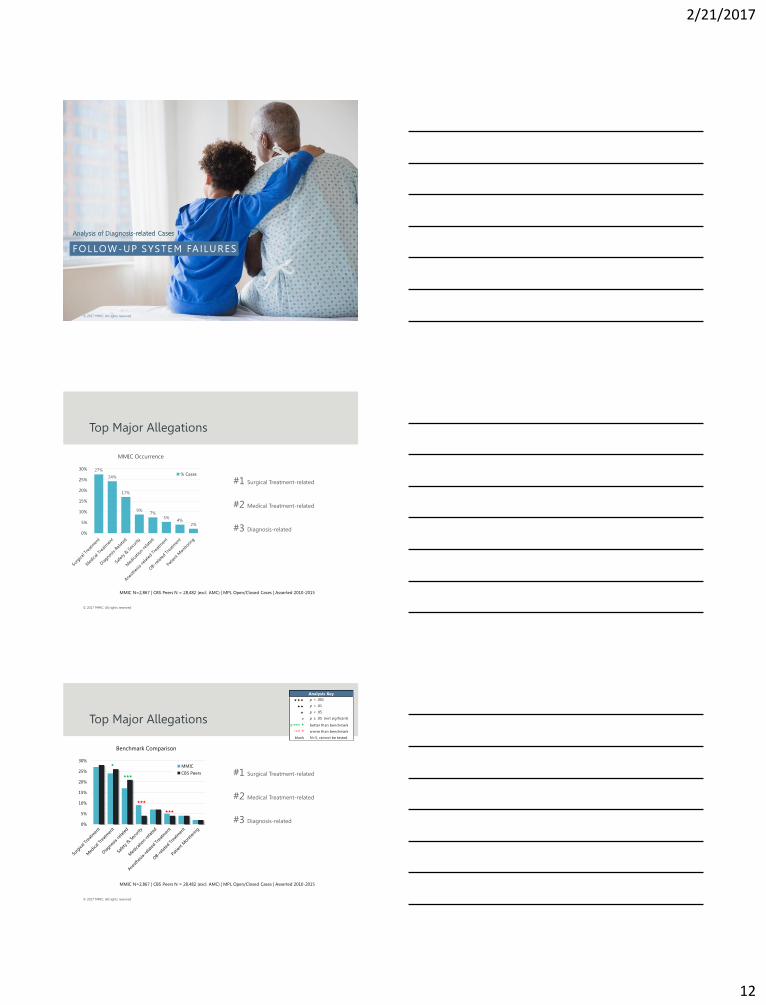
FOLLOW-UP SYSTEM FA ILURES
34
Analysis of Diagnosis-related Cases
© 2017 MMIC. All rights reserved
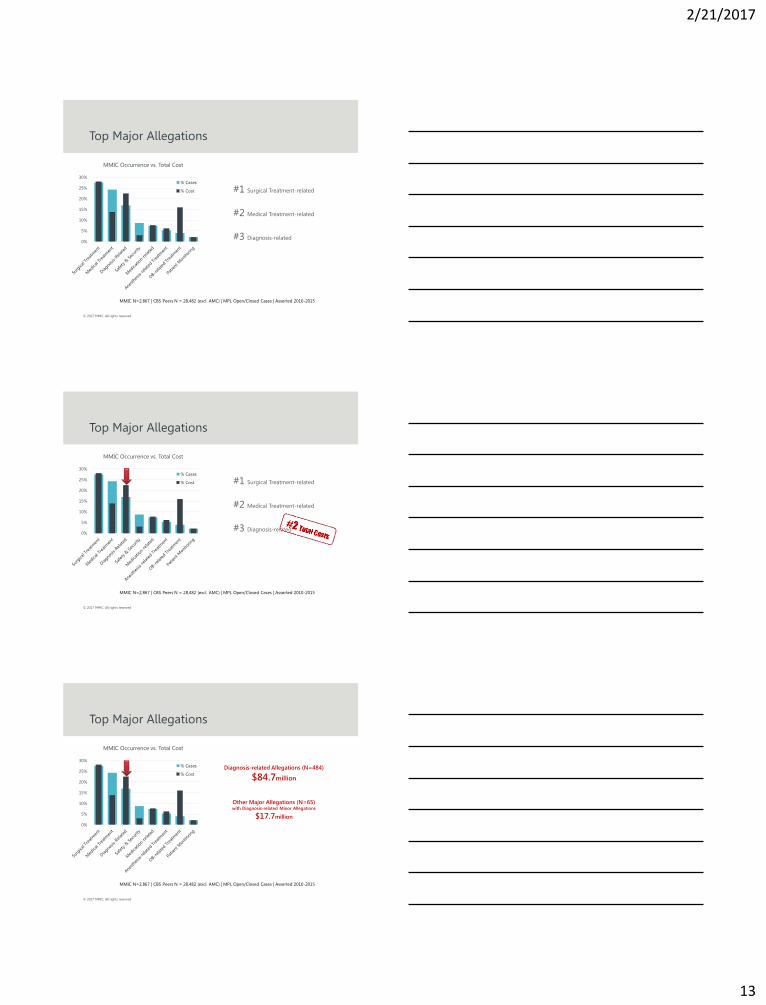
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
27%
24%
17%
9% 7%
5% 4%
2%
0%
5%
10%
15%
20%
25%
30%
MMIC Occurrence
% Cases
% Cost #1 Surgical Treatment-related
#2 Medical Treatment-related
#3 Diagnosis-related
© 2017 MMIC. All rights reserved
0%
5%
10%
15%
20%
25%
30%
Benchmark Comparison
MMIC
CBS Peers
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
#1 Surgical Treatment-related
#2 Medical Treatment-related
#3 Diagnosis-related
p < .001
p < .01
p < .05
p ≥ .05 (not sigificant)
green better than benchmark
red worse than benchmark
blank N<5, cannot be tested
Analysis Key
2/21/2017
13
© 2017 MMIC. All rights reserved
#1 Surgical Treatment-related
#2 Medical Treatment-related
#3 Diagnosis-related
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
0%
5%
10%
15%
20%
25%
30%
MMIC Occurrence vs. Total Cost
% Cases
% Cost
© 2017 MMIC. All rights reserved
0%
5%
10%
15%
20%
25%
30%
MMIC Occurrence vs. Total Cost
% Cases
% Cost #1 Surgical Treatment-related
#2 Medical Treatment-related
#3 Diagnosis-related
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
© 2017 MMIC. All rights reserved
0%
5%
10%
15%
20%
25%
30%
MMIC Occurrence vs. Total Cost
% Cases
% Cost
Top Major Allegations
MMIC N=2,867 | CBS Peers N = 28,482 (excl. AMC) | MPL Open/Closed Cases | Asserted 2010-2015
Diagnosis-related Allegations (N=484)
$84.7million
Other Major Allegations (N=65) with Diagnosis-related Minor Allegations
$17.7million
2/21/2017
14
© 2017 MMIC. All rights reserved 40
Drilling Down to Diagnosis
© 2017 MMIC. All rights reserved
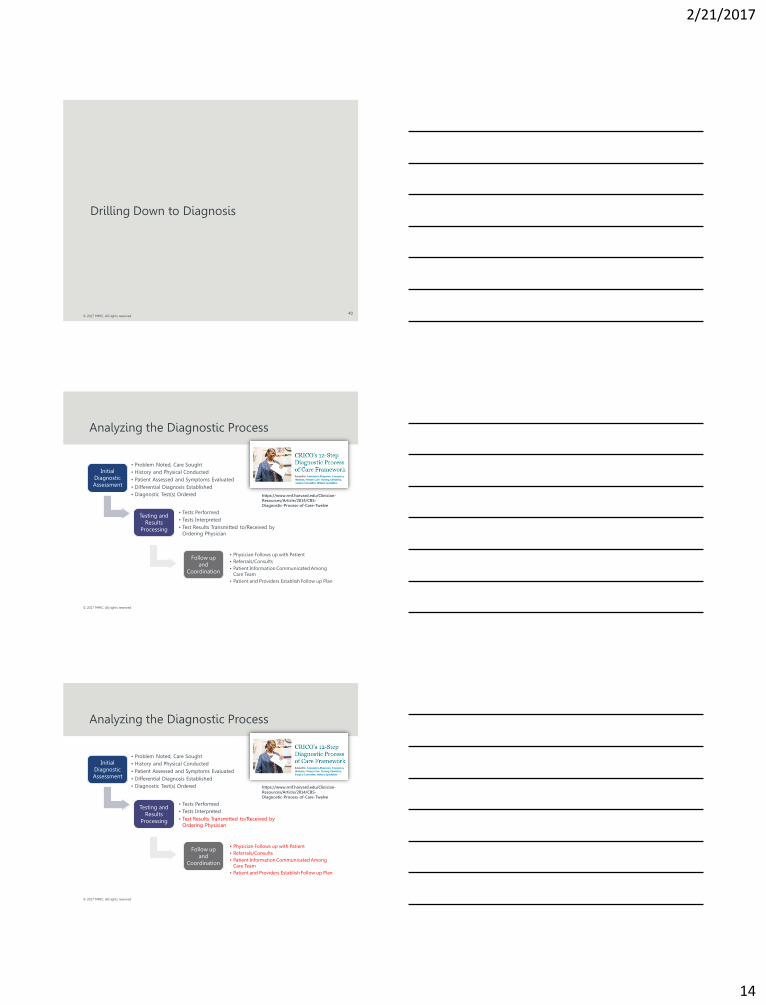
Initial
Diagnostic
Assessment
• Problem Noted, Care Sought
• History and Physical Conducted
• Patient Assessed and Symptoms Evaluated
• Differential Diagnosis Established
• Diagnostic Test(s) Ordered
Testing and
Results
Processing
• Tests Performed
• Tests Interpreted
• Test Results Transmitted to/Received by
Ordering Physician
Follow up
and
Coordination
• Physician Follows up with Patient
• Referrals/Consults
• Patient Information Communicated Among
Care Team
• Patient and Providers Establish Follow up Plan
Analyzing the Diagnostic Process
https://www.rmf.harvard.edu/Clinician-
Resources/Article/2014/CBS-
Diagnostic-Process-of-Care-Twelve
© 2017 MMIC. All rights reserved
Initial
Diagnostic
Assessment
• Problem Noted, Care Sought
• History and Physical Conducted
• Patient Assessed and Symptoms Evaluated
• Differential Diagnosis Established
• Diagnostic Test(s) Ordered
Testing and
Results
Processing
• Tests Performed
• Tests Interpreted
• Test Results Transmitted to/Received by
Ordering Physician
Follow up
and
Coordination
• Physician Follows up with Patient
• Referrals/Consults
• Patient Information Communicated Among
Care Team
• Patient and Providers Establish Follow up Plan
Analyzing the Diagnostic Process
https://www.rmf.harvard.edu/Clinician-
Resources/Article/2014/CBS-
Diagnostic-Process-of-Care-Twelve

2/21/2017
15
© 2017 MMIC. All rights reserved
Mining Factors Indicating Follow-up System Failures (FUSF)
Follow up Systems Failures (FUSF)
N=229 PL Cases Asserted 2010-2015
with a Major or Minor Dx-related Allegation
FUSF factors
…
FUSF factors
…
FUSF factors
…
19 Contributing Factors from CRICO Strategies’
Clinical Coding Taxonomy
© 2017 MMIC. All rights reserved
Scope of FUSF
Other 81% N=2,318
No FUSF 11%
N=320
FUSF 8% N=229
Cases with Dx-related Major or Minor Allegation with Follow up System Failures (FUSF)
Dx-related 19% N=549
Cases with a major or minor diagnosis-related allegation
MMIC N=2,867 PL Open/Closed Cases Asserted 2010-2015
© 2017 MMIC. All rights reserved
Scope of FUSF
Other 81% N=2,318
No FUSF 11%
N=320
42% of MMIC cases with
a major or minor dx-related allegation
involves an FUSF factor
FUSF 8% N=229
Cases with Dx-related Major or Minor Allegation with Follow up System Failures (FUSF)
Dx-related 19% N=484
Cases with a major or minor diagnosis-related allegation
MMIC N=2,867 PL Open/Closed Cases Asserted 2010-2015
Scope of FUSF within Diagnosis-related Cases
FUSF 42%
N=229
No FUSF 58%
N=320

2/21/2017
16
© 2017 MMIC. All rights reserved
Scope of FUSF
Other 81% N=2,318
No FUSF 11%
N=320
42% of MMIC cases with
a major or minor dx-related allegation
involves an FUSF factor
FUSF 8% N=229
Cases with Dx-related Major or Minor Allegation with Follow up System Failures (FUSF)
Dx-related 19% N=484
Cases with a major or minor diagnosis-related allegation
MMIC N=2,867 PL Open/Closed Cases Asserted 2010-2015
Scope of FUSF within Diagnosis-related Cases
FUSF 42%
N=229
No FUSF 58%
N=320
Even if physicians diagnosed accurately 100%
of the time, we’d still have diagnostic error.
© 2017 MMIC. All rights reserved
Scope of FUSF
Other 81% N=2,318
No FUSF 11%
N=320
FUSF 8% N=229
Cases with Dx-related Major or Minor Allegation with Follow up System Failures (FUSF)
Dx-related 19% N=484
Cases with a major or minor diagnosis-related allegation
MMIC N=2,867 PL Open/Closed Cases Asserted 2010-2015
Scope of FUSF within Diagnosis-related Cases
FUSF 42%
N=229
No FUSF 58%
N=320
The cost of FUSF…
$43.7million
229 MMIC cases over 6 years
© 2017 MMIC. All rights reserved
Follow-Up Systems Errors
• One of the major focuses of plaintiff attorneys when
pursuing service-lapse type claims • In a study performed by one of the nations largest
malpractice insurance providers assessing risks leading to patient injury in the medical office setting, the single greatest concern was ineffective tracking for diagnostic tests/consults (follow-up systems)

2/21/2017
17
© 2017 MMIC. All rights reserved
Follow-Up Systems Errors
• Most frequent issue is test results being transmitted to/received by physician/clinic
• Most often seen with lab and radiology reports
• Unrelated to clinical practice-deals with procedure and process (service lapse)
• Patient education/orientation on test results delivery methodology is necessary
© 2017 MMIC. All rights reserved
Follow-Up Systems Errors
• Define then convey your policy on delivery of test results
• No news is “NO NEWS”
• Utilize your patient as a last line of defense
• “If you haven’t heard from us by…..”
• Staff engagement and responsibility is imperative
© 2017 MMIC. All rights reserved
The Key Steps: Follow-up System Cycle
Test
ORDERED
Patient
RETURNS
for follow-up
Appointment
Follow-Up
APPOINTMENT
scheduled
DOCUMENTATION of
notification and instructions to
patient
Results
REVIEWED
For clinical decision
Results RECEIVED
Test DONE Patient
ASSESSED
Patient NOTIFIED
and given
instructions

2/21/2017
18
© 2017 MMIC. All rights reserved
The Key Steps: Follow-Up System Cycle
• The effectiveness of a follow-up system depends on
the integrity of each step • A weakness at any point in the process may end up
in a patient injury and subsequent malpractice claim
© 2017 MMIC. All rights reserved
Focus Should Be On The Main Components
• Receipt of test results
• Review of test results
• Notification to patient
• Missed appointment cancellation tracking
© 2017 MMIC. All rights reserved
2/21/2017
19
© 2017 MMIC. All rights reserved
© 2017 MMIC. All rights reserved
Questions?
56
© 2017 MMIC. All rights reserved
Contact us
Robert.Thompson
@MMICgroup.com

2/21/2017
20
© 2017 MMIC. All rights reserved 58















![Follow Up[1.0]](https://img.pdfslide.tips/doc/110x75/5561462bd8b42a857d8b460a/follow-up10.jpg)