Embed Size (px)
Citation preview

GERIATRIC ASSESSMENT AND QUALITYGERIATRIC ASSESSMENT AND QUALITY OF LIFE AMONG OLDER ADULTS WITH HEMATOLOGIC MALIGNANCIESDaneng Li, MDAssistant Clinical ProfessorMedical Oncology & Therapeutics Research
Erin Kopp M.S.N, A.C.N.P-B.C., N.Popp S , C C ,Nurse PractionerDepartment of Hematology
How the Experts Treat Hematologic MalignanciesLas Vegas, NVMarch 17, 2017
Disclosures
• I do not have anything to disclose.y g
Objectives
• To understand the components of geriatric assessment in p gthe care of older adults with cancer
• To understand potential applications for geriatric t i h t l i li iassessment in hematologic malignancies
Background
• Aging US populationg g p p– Projected 88.5 million > 65yrs by 2050– More than double of 40.2 million in 2010
• Cancer associated with aging– By 2030, ~70% of all cancer diagnosis will occur in patients
age > 65age > 65
Vincent GK et al. www.census.govSmith BD et al. J Clin Oncol 2009
Background
• Older adults significantly underrepresented in clinical trialsg y p– 11% of physicians reported age alone as reason for not enrolling
older adultsL ti f ti i ti i FDA i t ti t i l d t i l– Low proportion of participation in FDA registration trials and trials from National Clinical Trials Network
– Percentage enrolled onto cooperative group trials remained flat at ~20% between 2001-2011
Hutchins et al. N Engl J Med 1999Hurria et al. J Clin Oncol 2015Javid SH et al. Oncologist 2012
For Older Adults:For Older Adults:
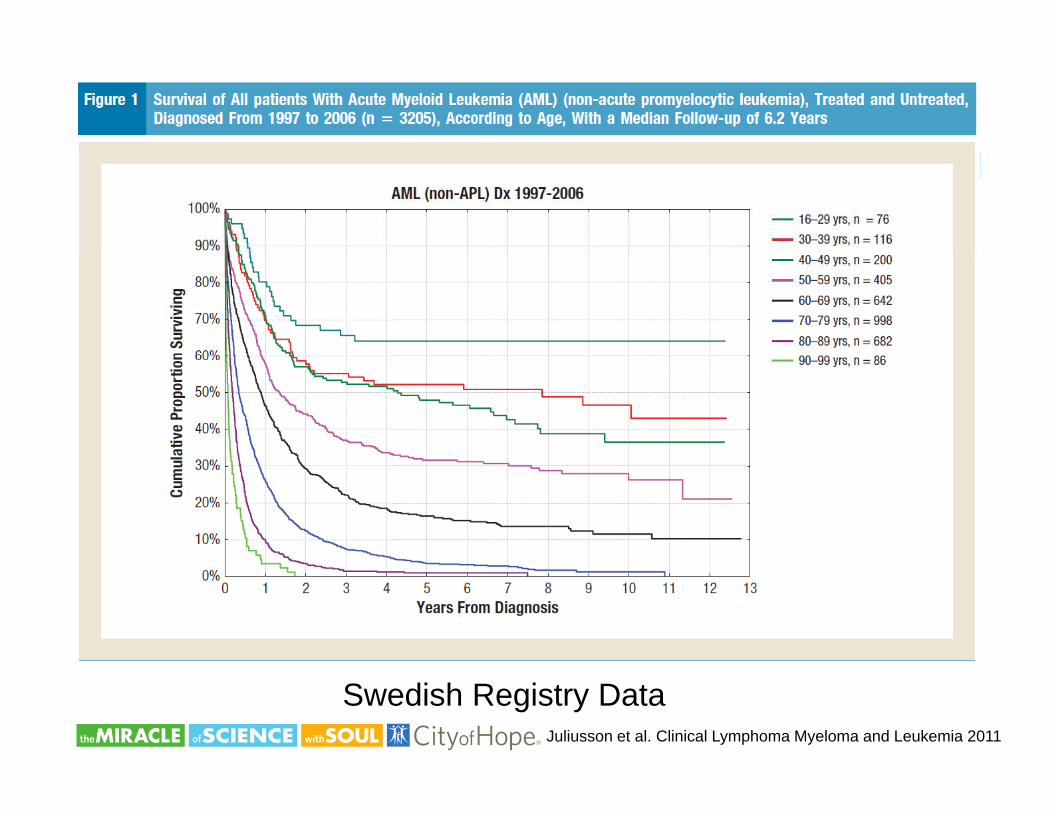
Juliusson et al. Clinical Lymphoma Myeloma and Leukemia 2011
Swedish Registry Data
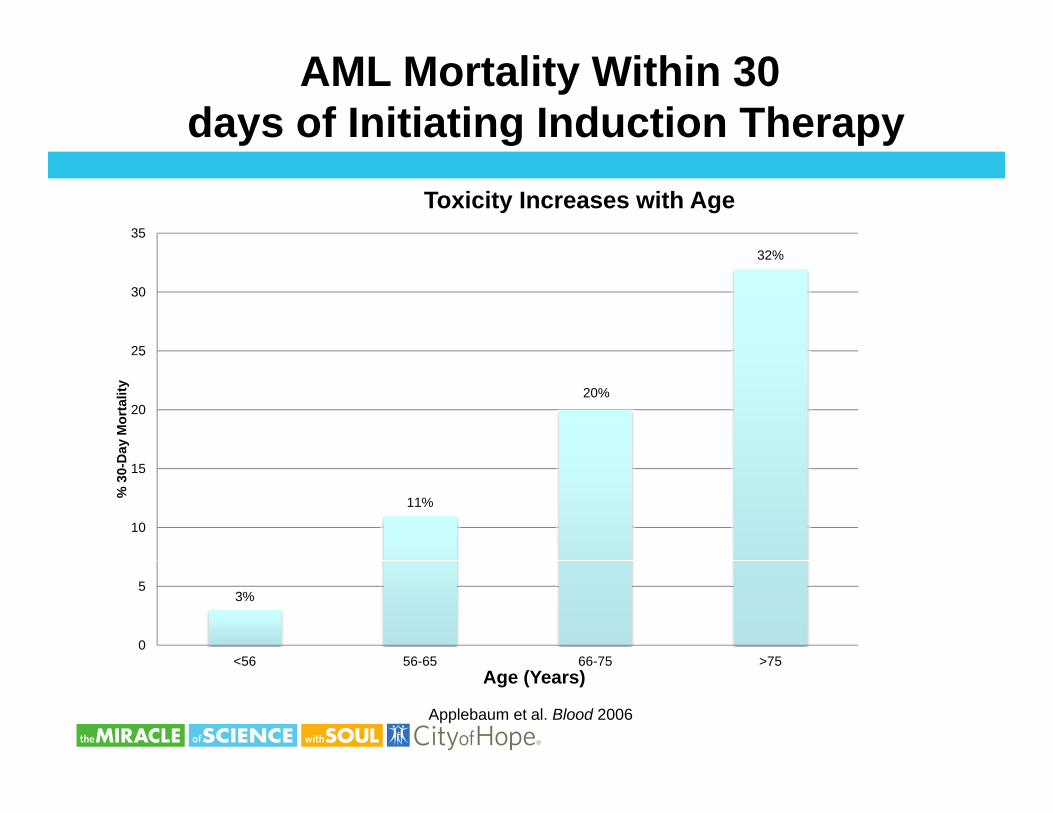
AML Mortality Within 30 days of Initiating Induction Therapy
32%35
Toxicity Increases with Age
32%
25
30
20%20
5
Day
Mor
talit
y
11%
10
15
% 3
0-D
3%
0
5
<56 56-65 66-75 >75<56 56 65 66 75 >75Age (Years)
Applebaum et al. Blood 2006
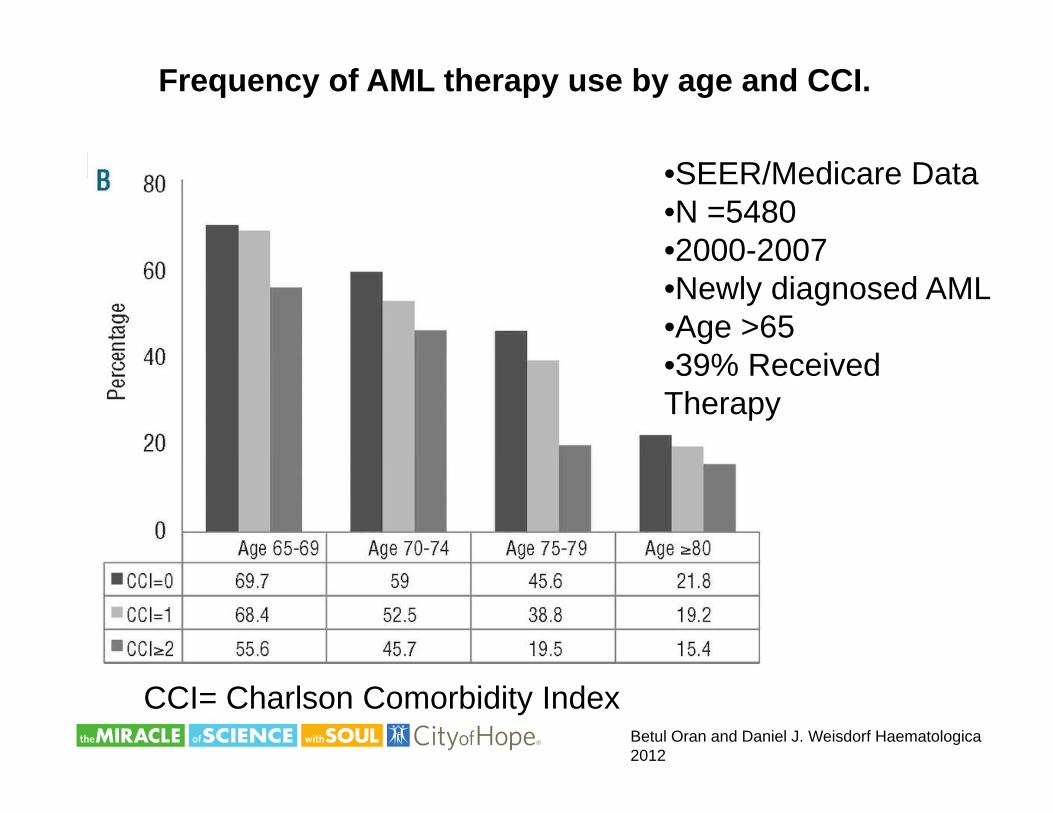
Frequency of AML therapy use by age and CCI.
•SEER/Medicare Data•N =5480•2000-2007•2000-2007•Newly diagnosed AML•Age >6539% R i d•39% Received
Therapy
Betul Oran and Daniel J. Weisdorf Haematologica 2012
CCI= Charlson Comorbidity Index
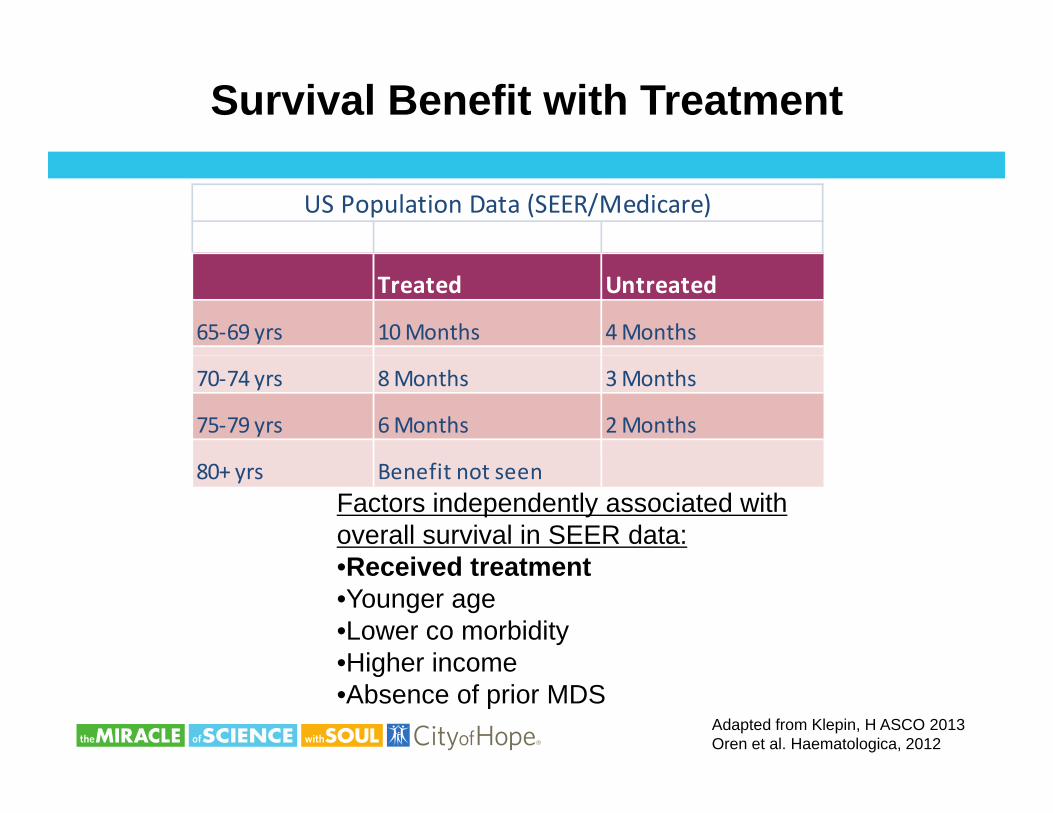
Survival Benefit with Treatment
US Population Data (SEER/Medicare)
Treated Untreated
65‐69 yrs 10 Months 4 Months
70‐74 yrs 8 Months 3 Months
75‐79 yrs 6 Months 2 Months
80+ yrs Benefit not seenFactors independently associated with overall survival in SEER data:R i d t t t•Received treatment
•Younger age•Lower co morbidity•Higher income•Higher income•Absence of prior MDS
Adapted from Klepin, H ASCO 2013Oren et al. Haematologica, 2012
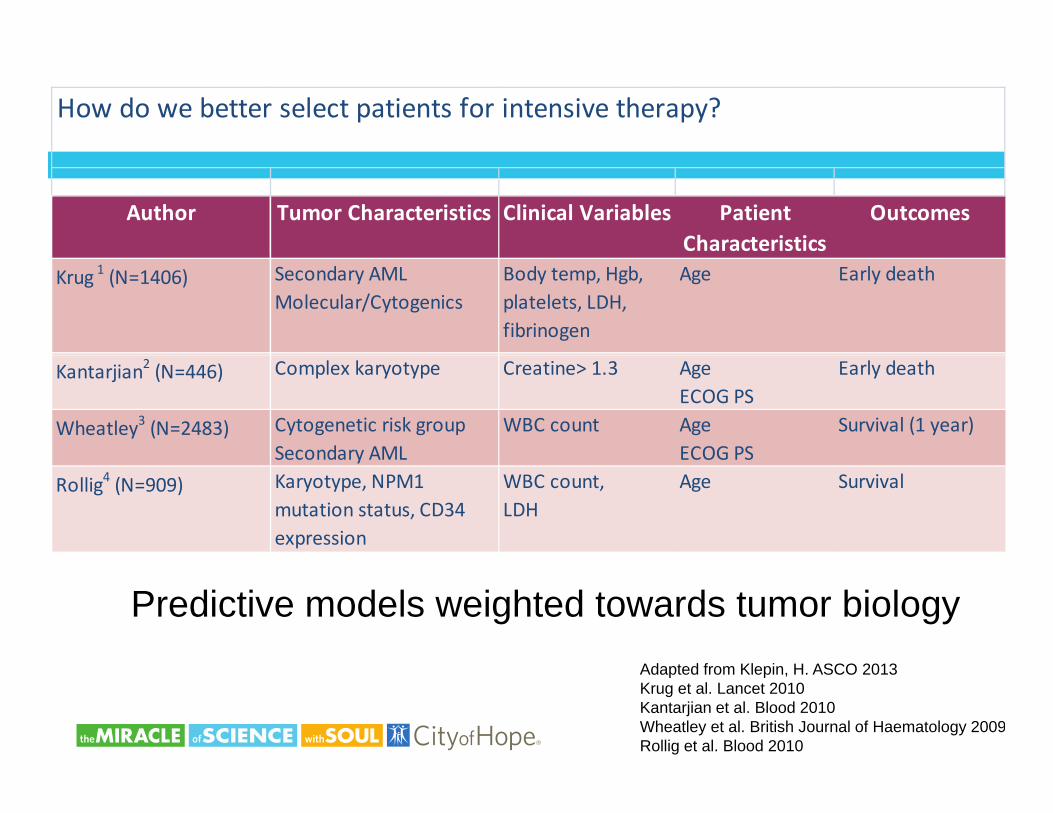
How do we better select patients for intensive therapy?
Author Tumor Characteristics Clinical Variables Patient Characteristics
Outcomes
Krug 1 (N=1406) Secondary AML Molecular/Cytogenics
Body temp, Hgb, platelets, LDH, fibrinogen
Age Early death
Kantarjian2 (N=446) Complex karyotype Creatine> 1.3 Age ECOG PS
Early death
Wheatley3 (N=2483) Cytogenetic risk group Secondary AML
WBC count Age ECOG PS
Survival (1 year)Secondary AML ECOG PS
Rollig4 (N=909) Karyotype, NPM1 mutation status, CD34 expression
WBC count, LDH
Age Survival
Predictive models weighted towards tumor biologyf SCOAdapted from Klepin, H. ASCO 2013
Krug et al. Lancet 2010Kantarjian et al. Blood 2010Wheatley et al. British Journal of Haematology 2009Rollig et al. Blood 2010
Aging is a Heterogeneous Process
Same Chronological Age; Different FunctionalSame Chronological Age; Different Functional Age
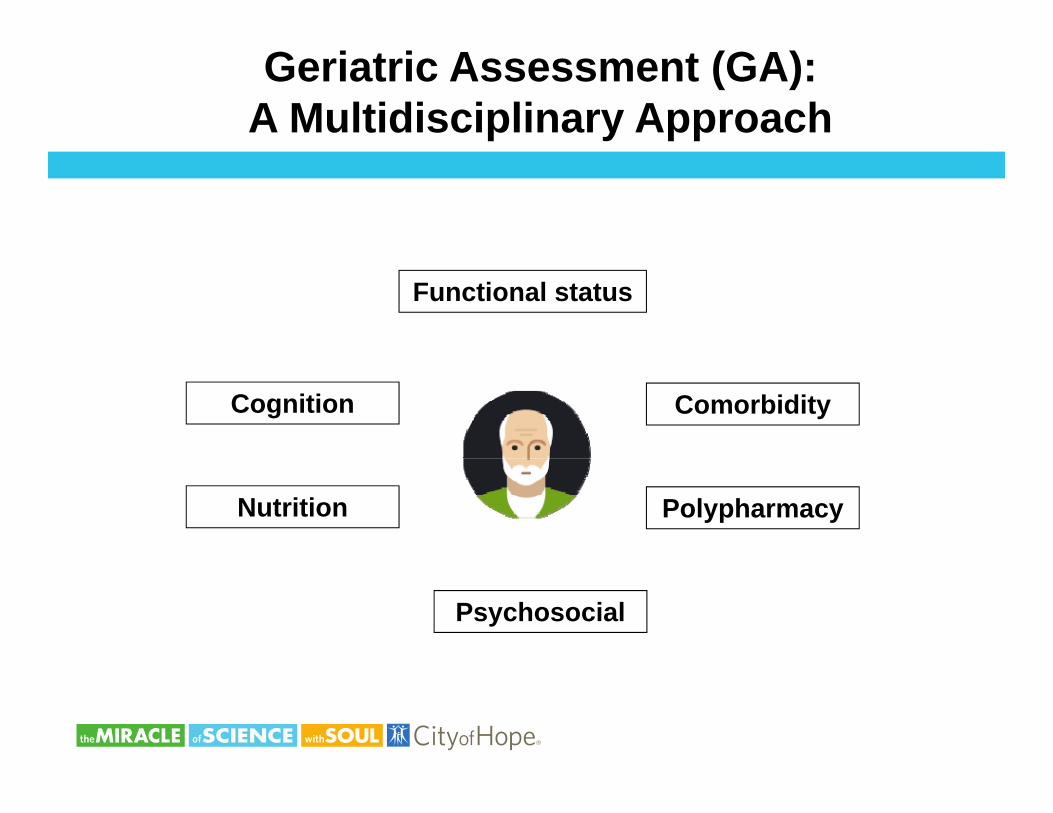
Geriatric Assessment (GA): A Multidisciplinary Approach
Functional status
Cognition Comorbidity
Nutrition Polypharmacy
Psychosocial
www.mycarg.org
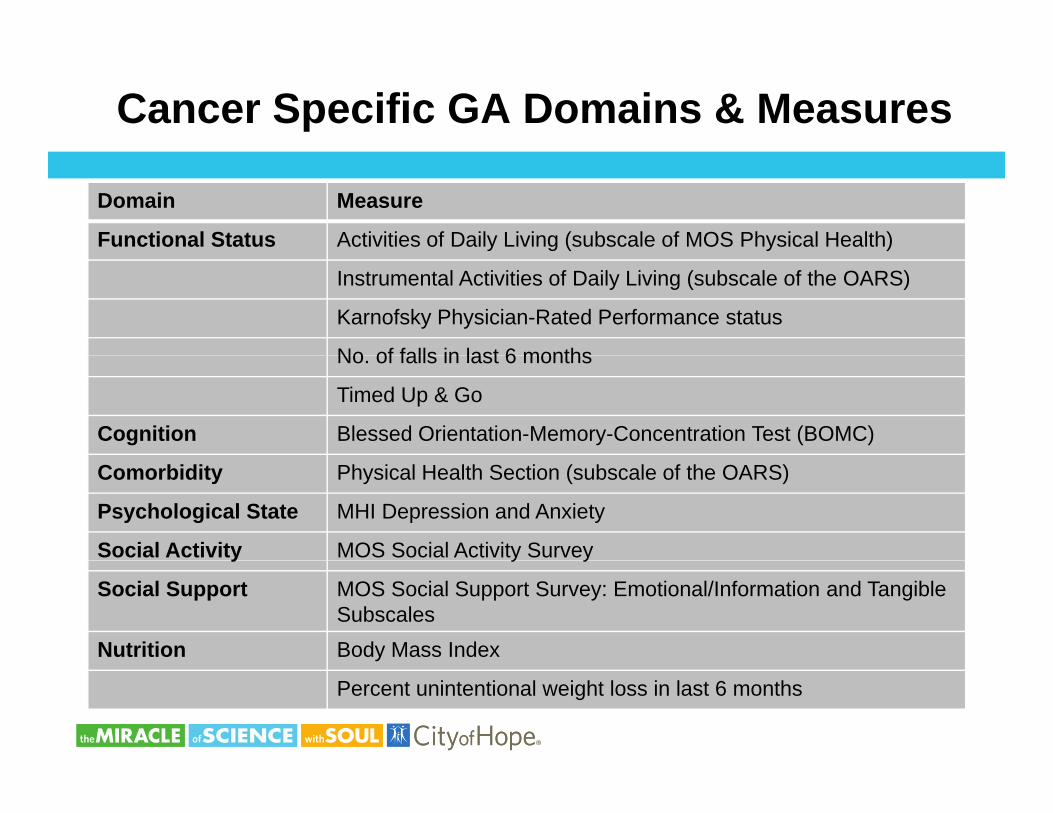
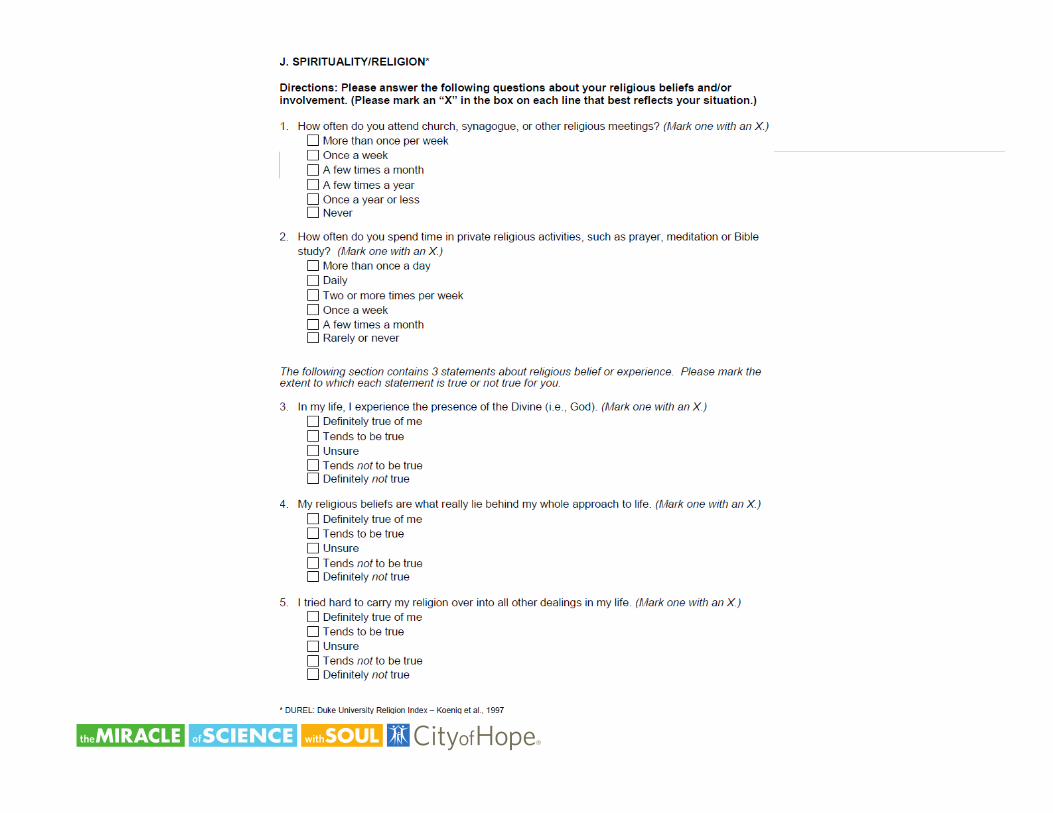
Cancer Specific GA Domains & Measures
Domain Measure
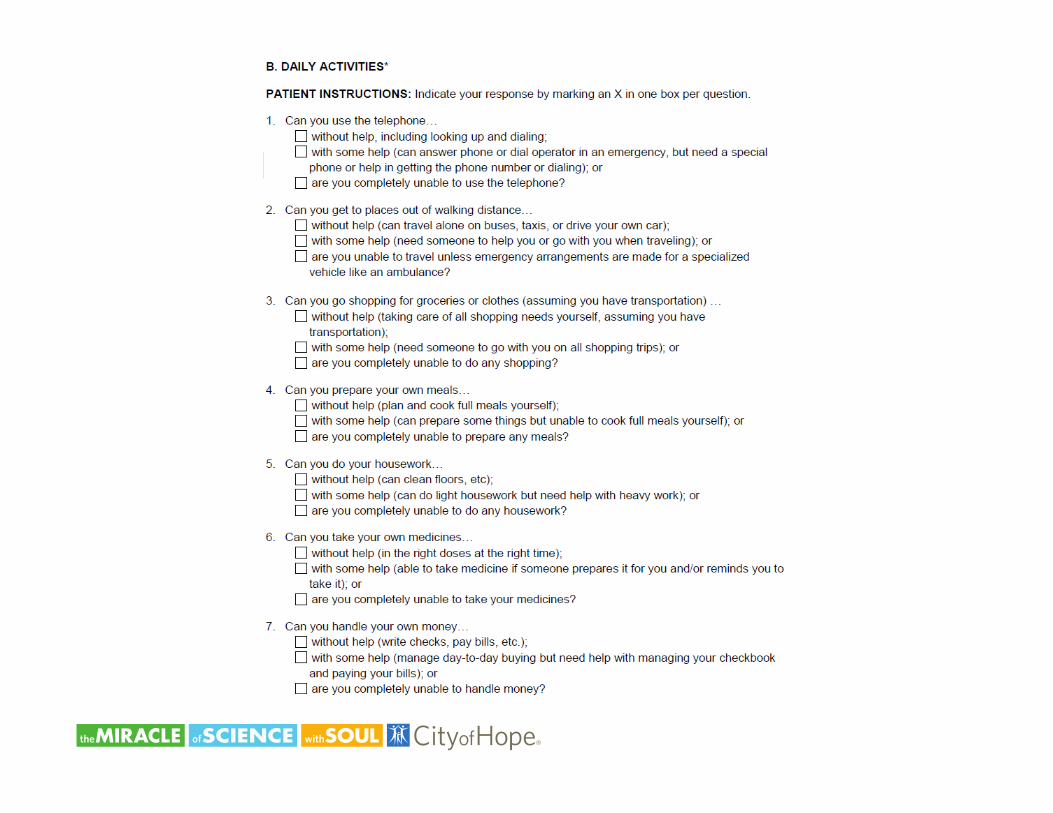
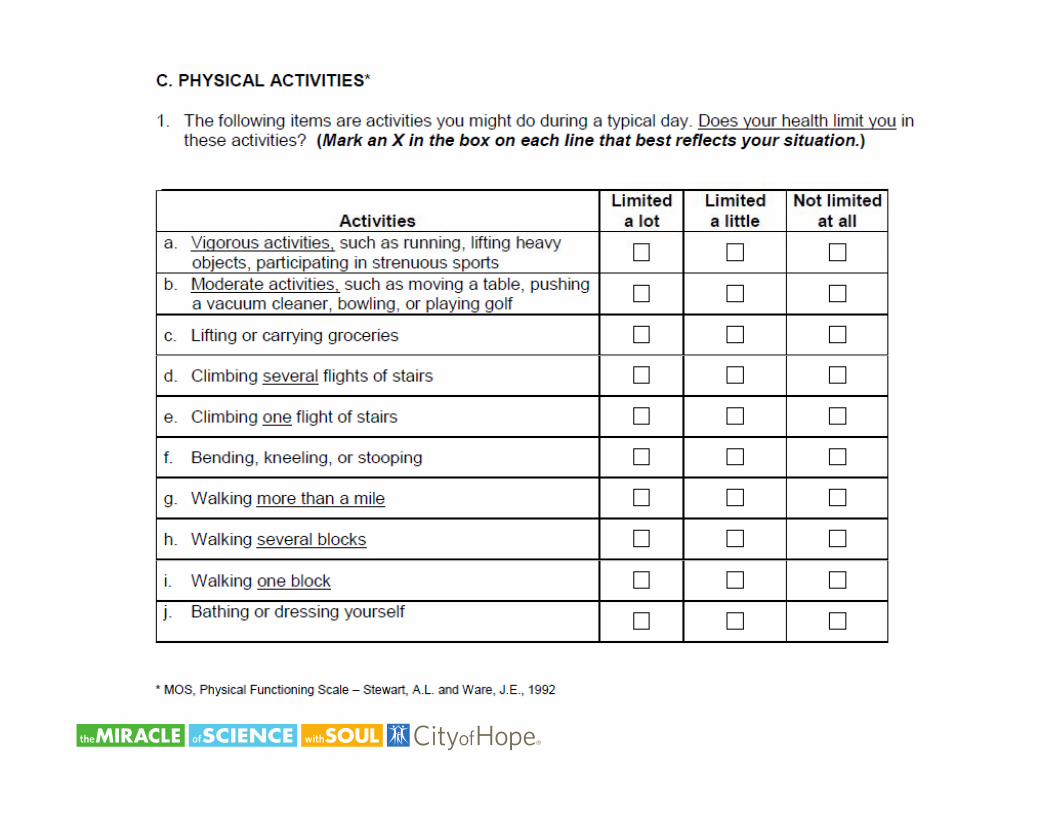
Functional Status Activities of Daily Living (subscale of MOS Physical Health)
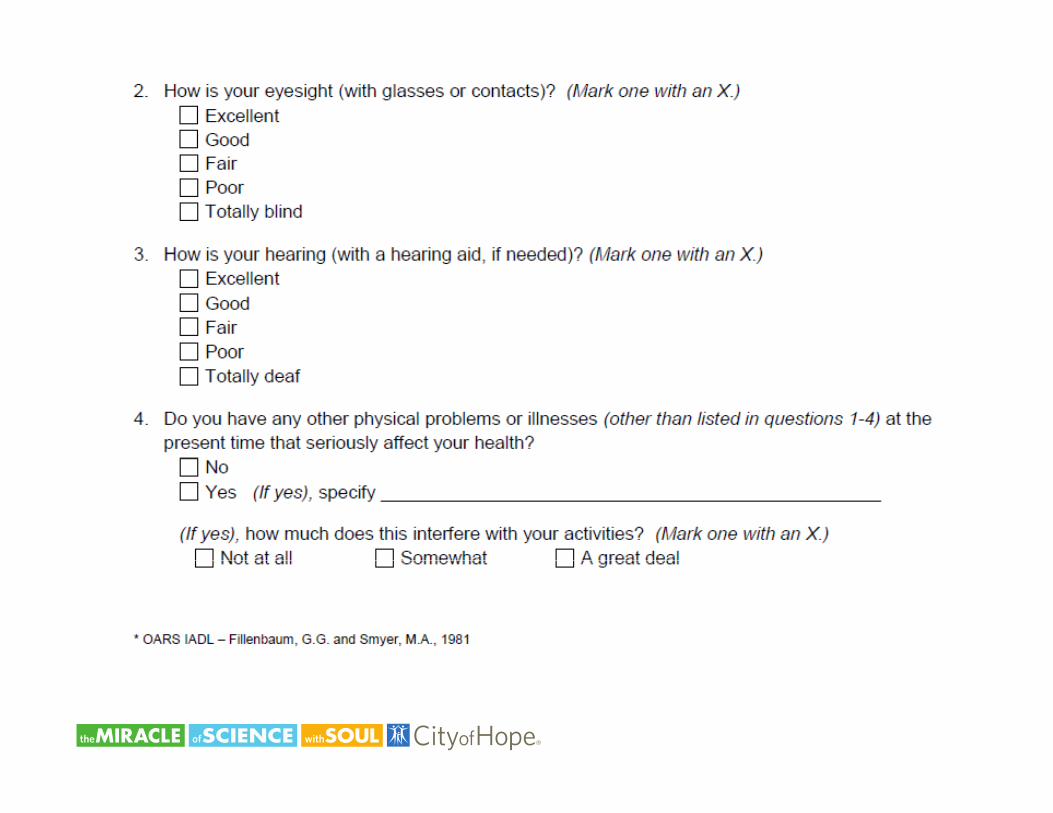
Instrumental Activities of Daily Living (subscale of the OARS)
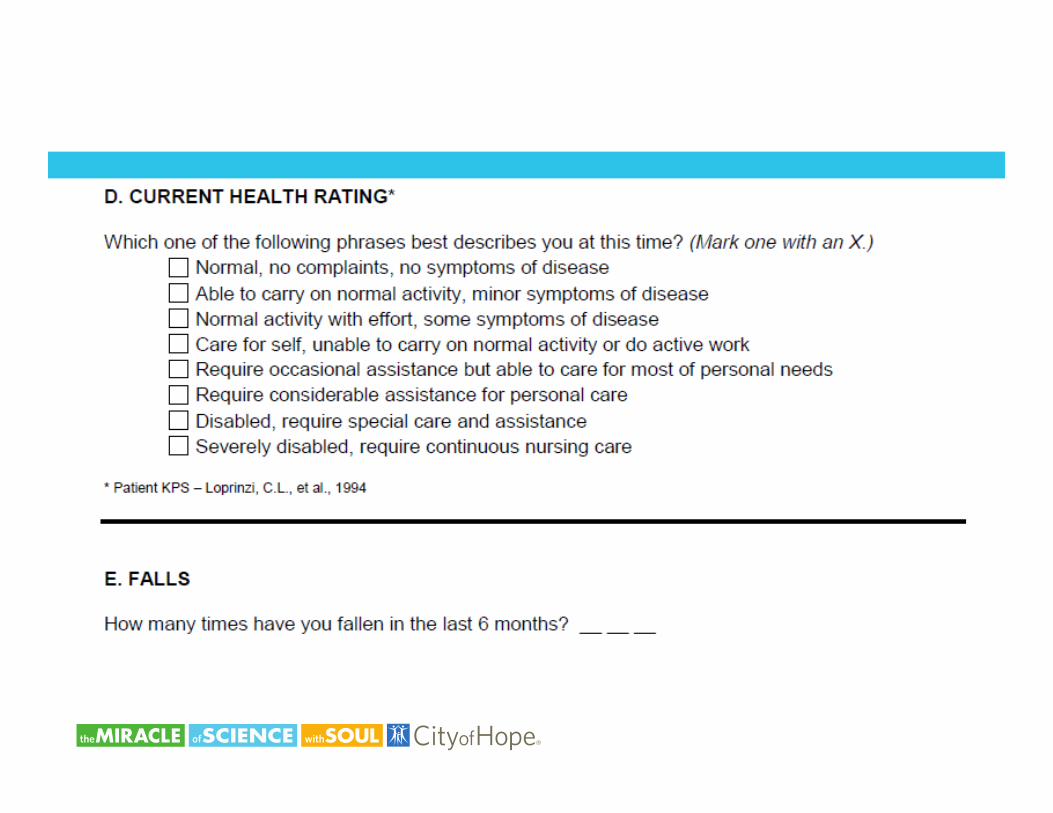
Karnofsky Physician-Rated Performance status
No of falls in last 6 monthsNo. of falls in last 6 months
Timed Up & Go
Cognition Blessed Orientation-Memory-Concentration Test (BOMC)
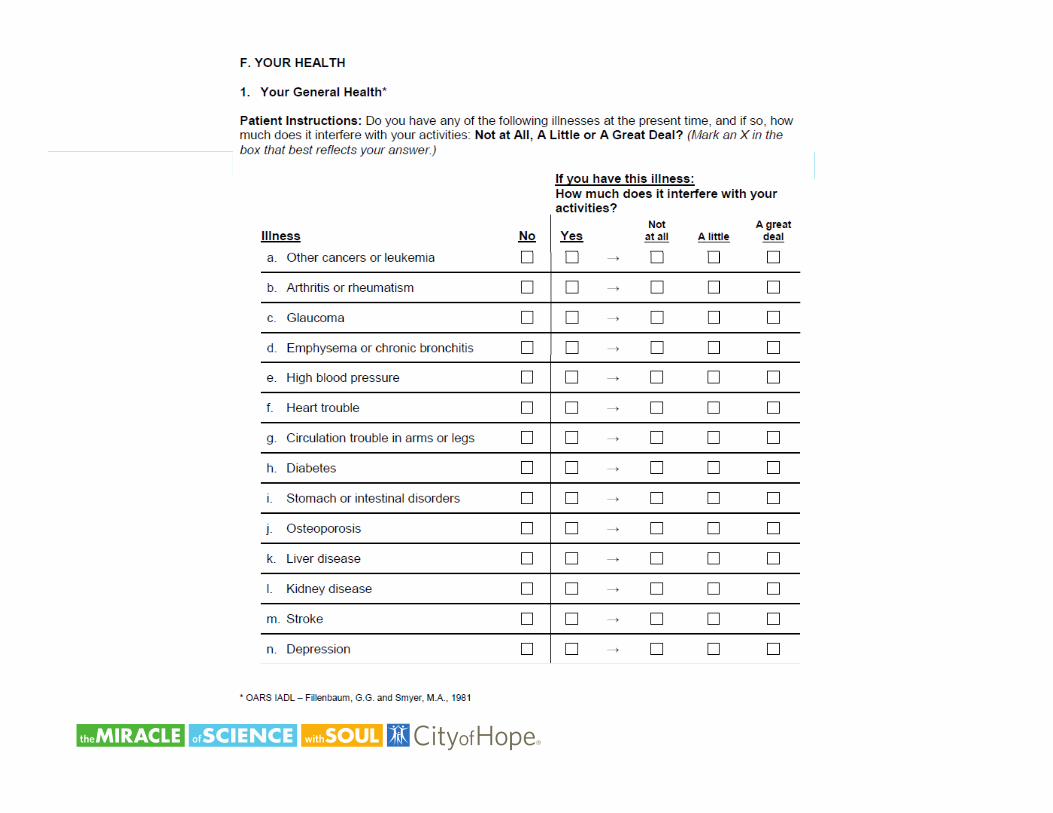
Comorbidity Physical Health Section (subscale of the OARS)
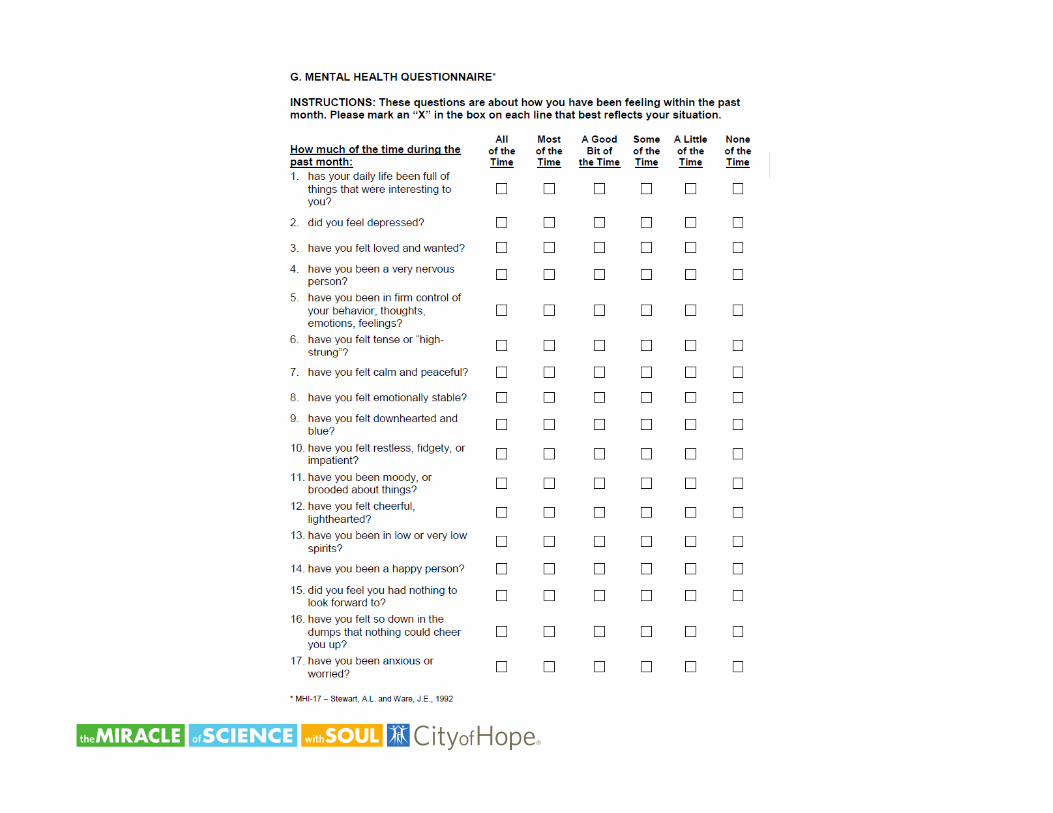
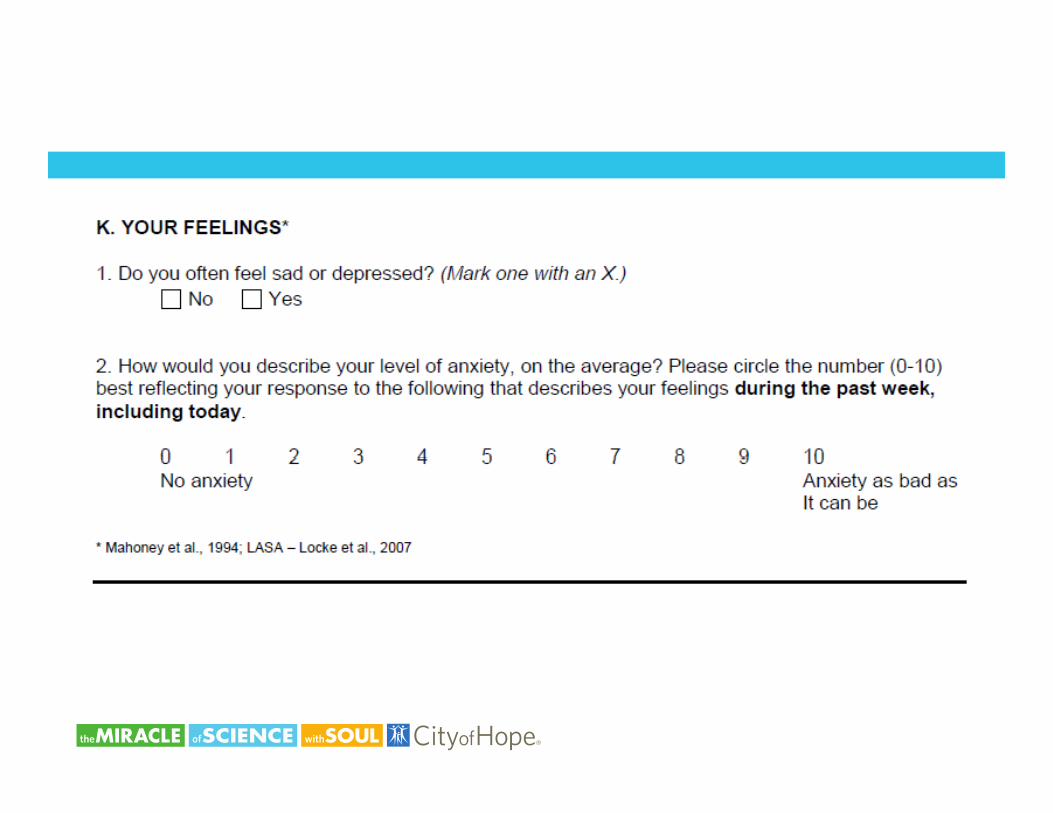
Psychological State MHI Depression and Anxiety
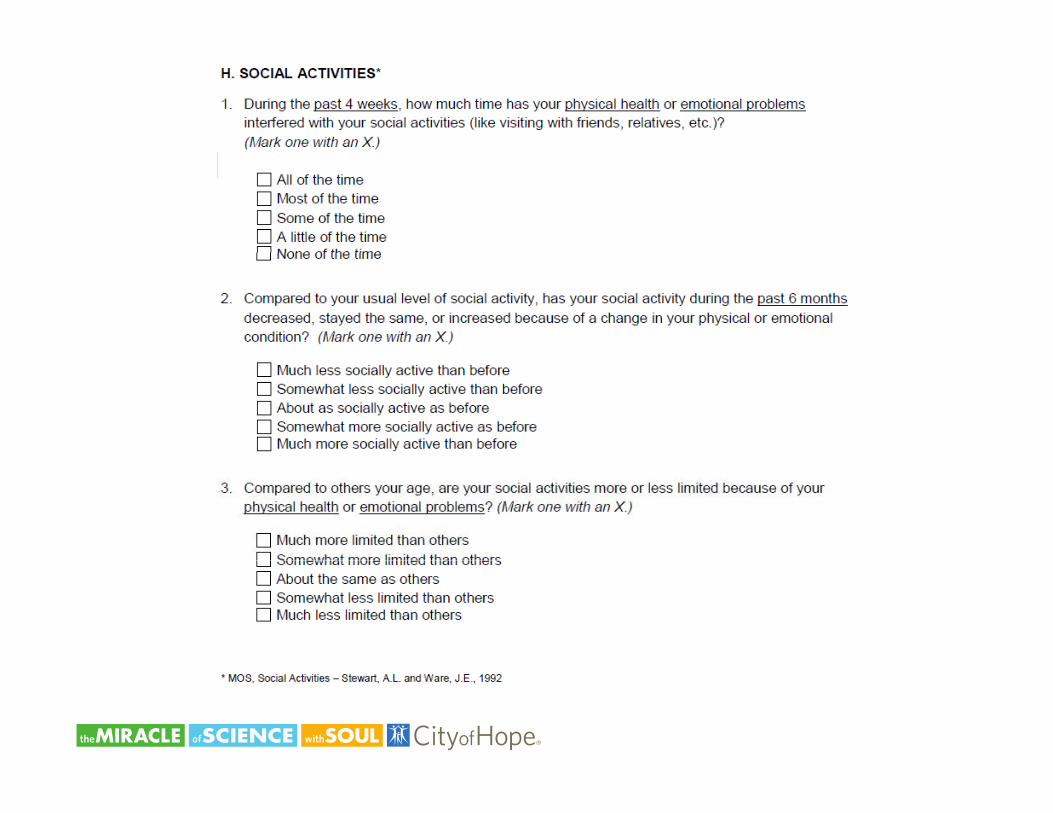
Social Activity MOS Social Activity Surveyy y y
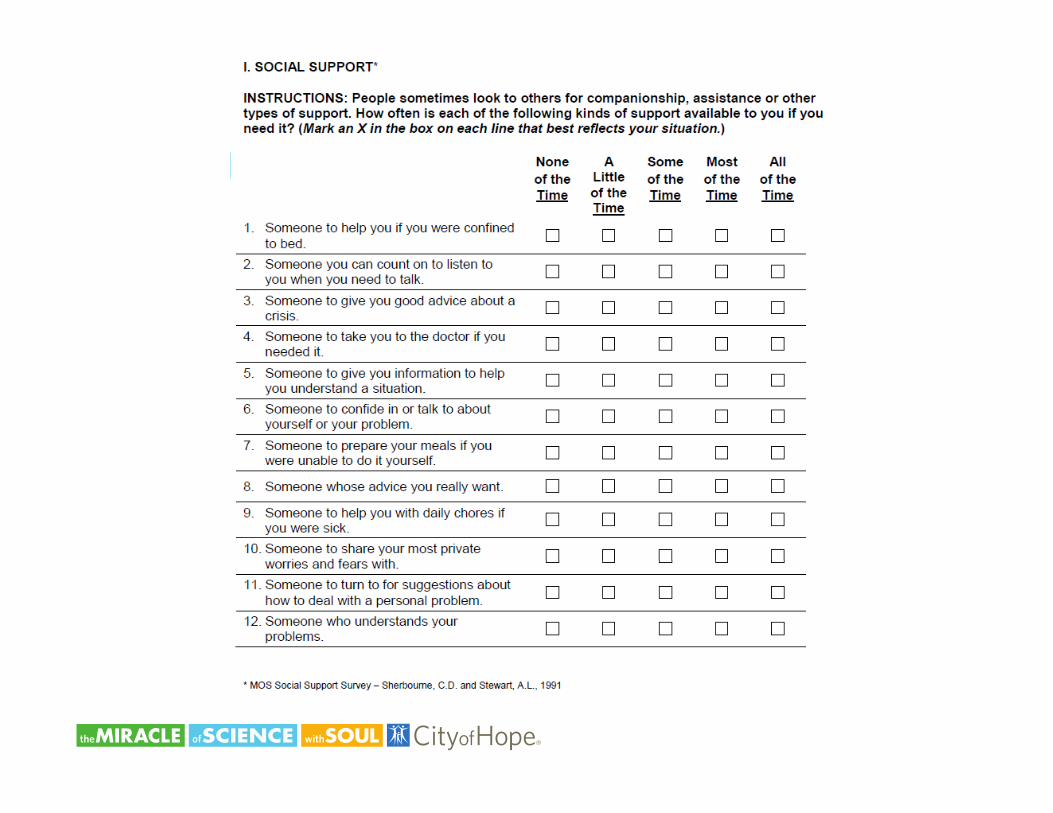
Social Support MOS Social Support Survey: Emotional/Information and Tangible Subscales
Nutrition Body Mass Index
Percent unintentional weight loss in last 6 months
Geriatric Assessment in Older Adults with Cancer
• Predict toxicity to cancer treatment• Predict survival for older cancer patients• Uncover problems not detected by routine H&P• Improves mental health and well-being• Improves pain control
Feyer et al. Ann Oncol 2005 Maione et al. JCO 2005Repetto et al JCO 2002 Chen et al Cancer 2003Repetto et al. JCO 2002 Chen et al. Cancer 2003Rao et al. J Gerontol A Biol Sci 2005 Extermann et al. CROH 2004
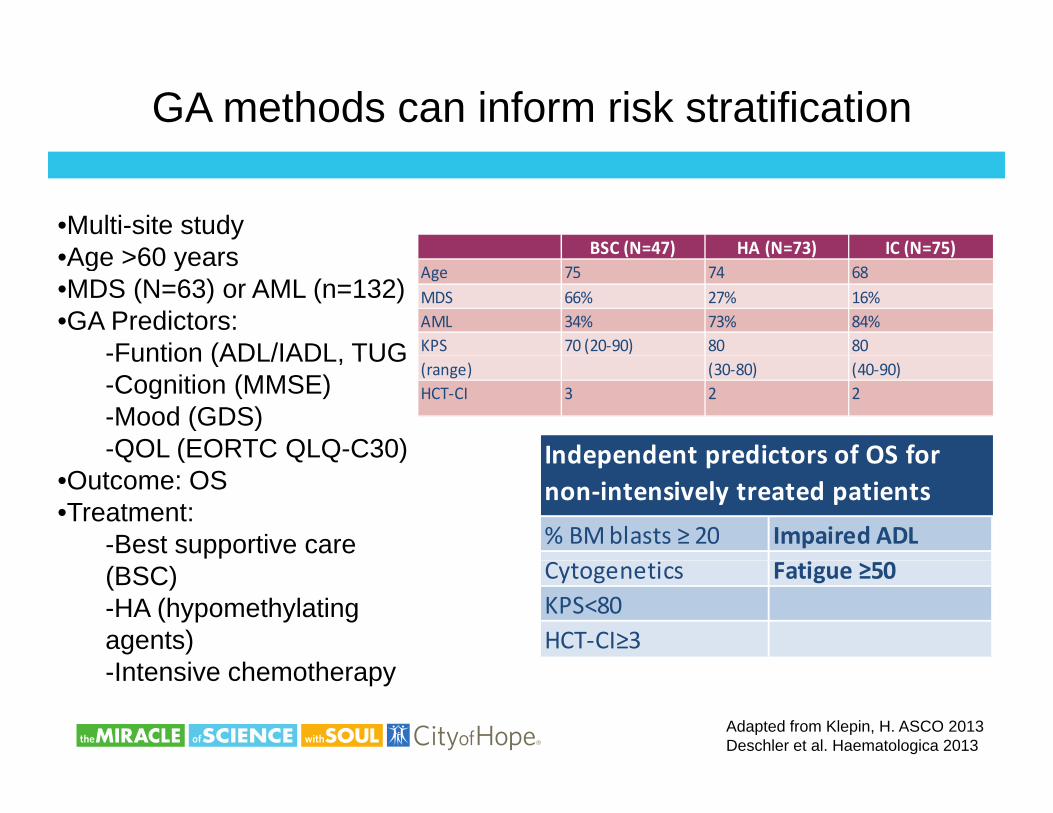
GA methods can inform risk stratification
•Multi-site studyAge >60 years BSC (N=47) HA (N=73) IC (N=75)•Age >60 years
•MDS (N=63) or AML (n=132)•GA Predictors:
-Funtion (ADL/IADL TUG
BSC (N 47) HA (N 73) IC (N 75)Age 75 74 68MDS 66% 27% 16%AML 34% 73% 84%KPS 70 (20‐90) 80 80 -Funtion (ADL/IADL, TUG
-Cognition (MMSE)-Mood (GDS)-QOL (EORTC QLQ-C30)
(range) (30‐80) (40‐90)HCT‐CI 3 2 2
Independent predictors of OS forQ ( Q Q )•Outcome: OS•Treatment:
-Best supportive care % BM blasts ≥ 20 Impaired ADL
Independent predictors of OS for non‐intensively treated patients
(BSC)-HA (hypomethylating agents)I t i h th
Cytogenetics Fatigue ≥50KPS<80HCT‐CI≥3
Adapted from Klepin, H. ASCO 2013Deschler et al. Haematologica 2013
-Intensive chemotherapy
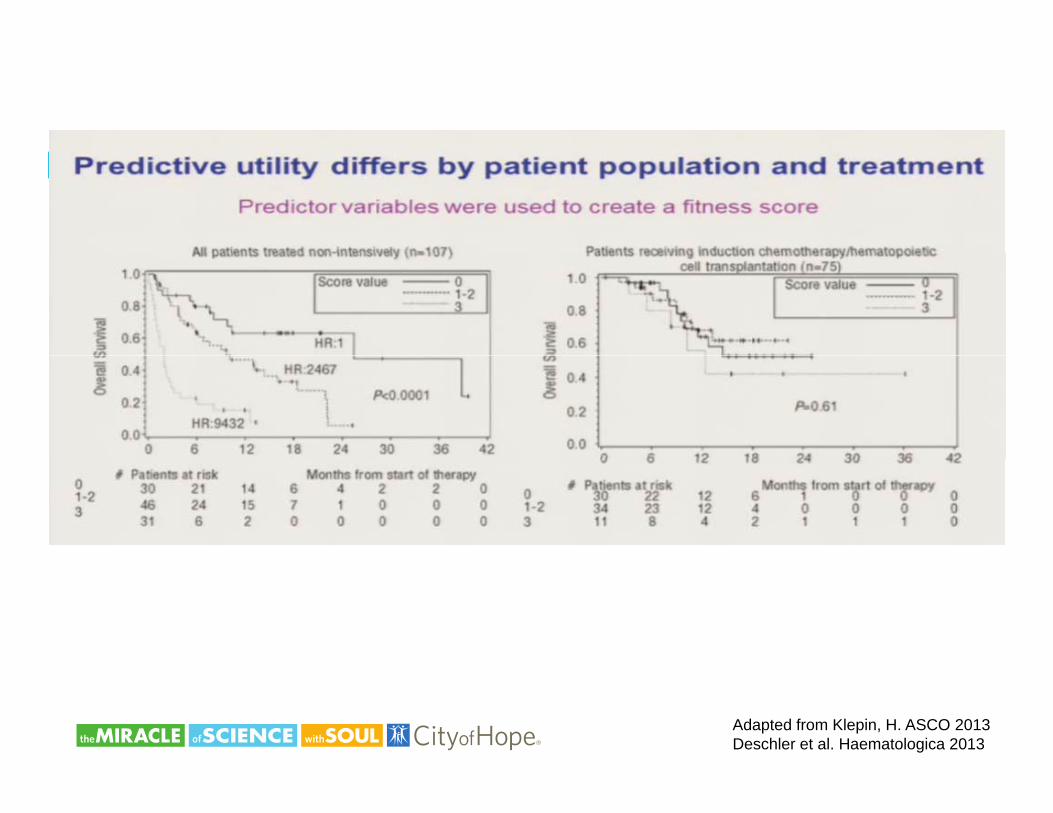
Adapted from Klepin, H. ASCO 2013Deschler et al. Haematologica 2013
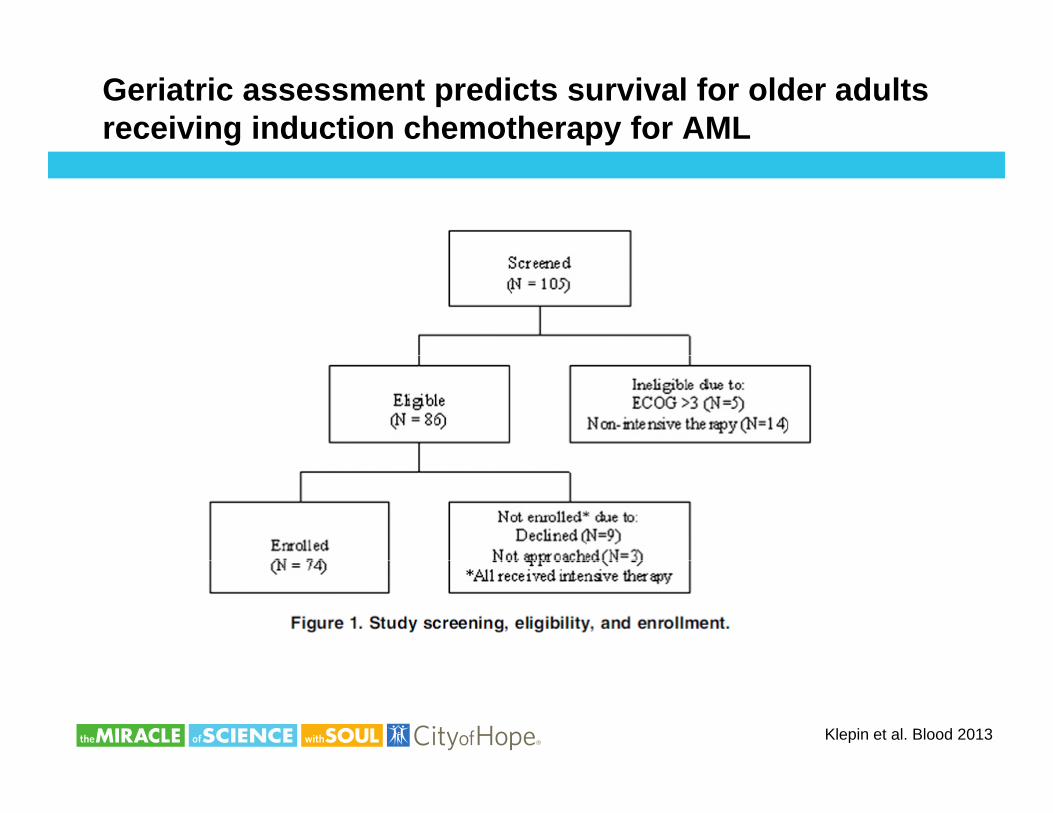
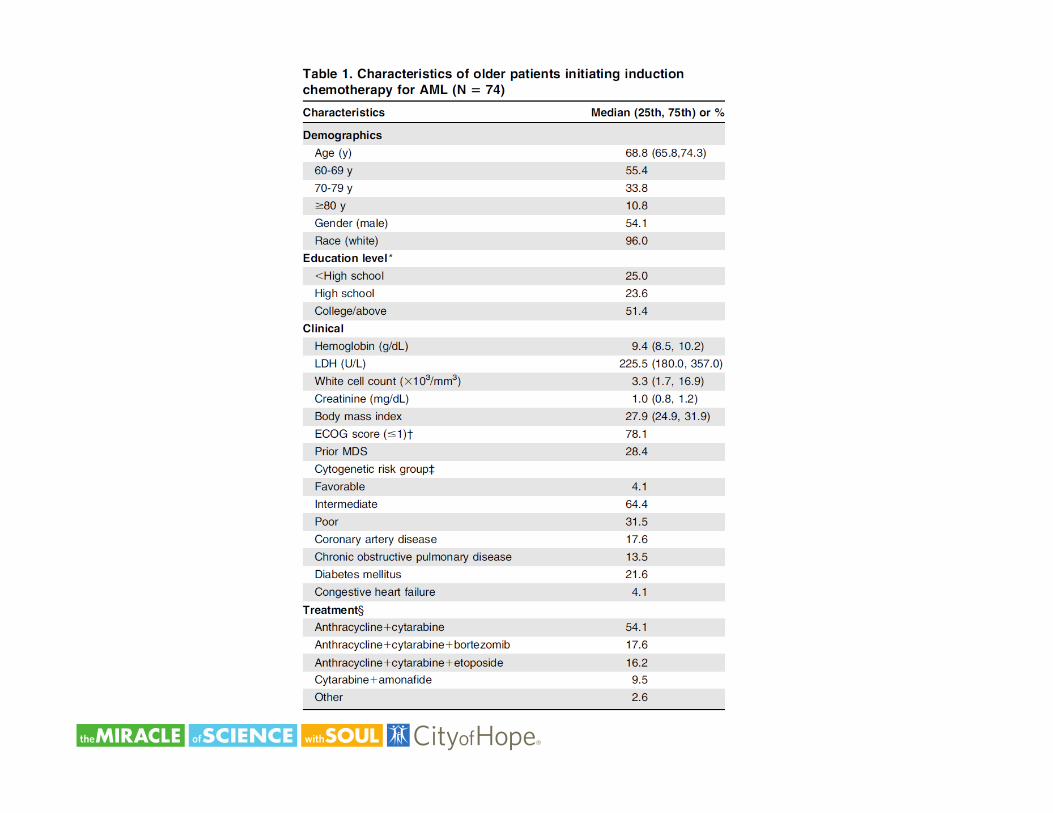
Geriatric assessment predicts survival for older adults receiving induction chemotherapy for AML
Klepin et al. Blood 2013
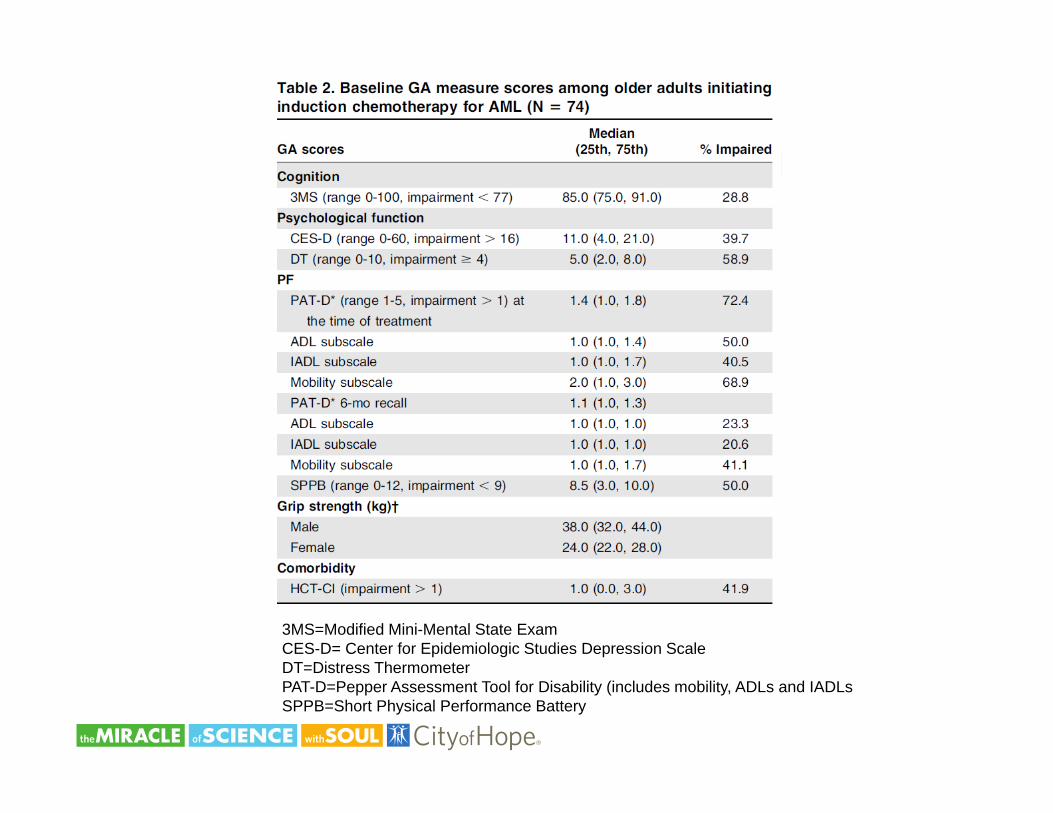
3MS=Modified Mini-Mental State ExamCES-D= Center for Epidemiologic Studies Depression ScaleDT Di t Th tDT=Distress ThermometerPAT-D=Pepper Assessment Tool for Disability (includes mobility, ADLs and IADLsSPPB=Short Physical Performance Battery
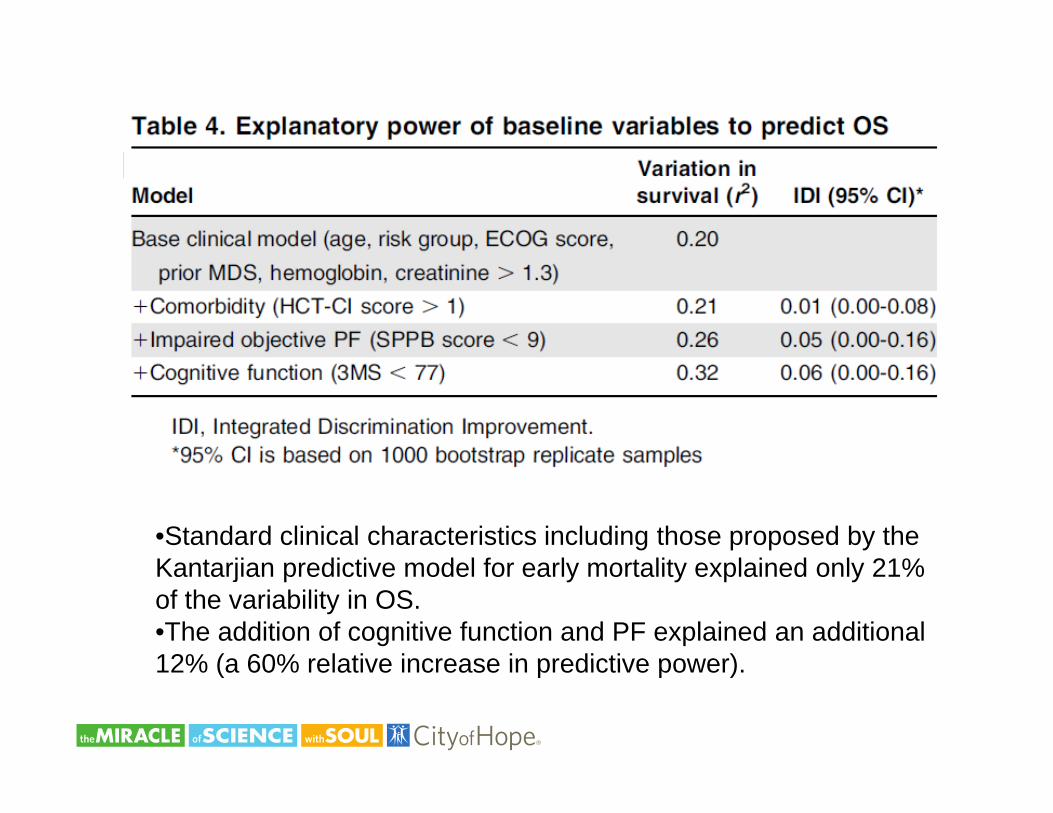
•Standard clinical characteristics including those proposed by the K t ji di ti d l f l t lit l i d l 21%Kantarjian predictive model for early mortality explained only 21% of the variability in OS.•The addition of cognitive function and PF explained an additional 12% (a 60% relative increase in predictive power)12% (a 60% relative increase in predictive power).
Summary
• Limited patient characteristics currently exist to guide treatment p y gof hematologic malignancies such as AML
• GA can provide additional information to help to risk stratify ti t d i t t t f h t l i li ipatients undergoing treatment for hematologic malignancies
• Increased incorporation of GA into hematologic malignancy clinical trials can help to inform its use in routine practiceclinical trials can help to inform its use in routine practice
Erin Kopp M.S.N, A.C.N.P-B.C., N.P.

Disclosures
• No disclosures
Objectives
• Review common hematologic malignancies seen in the older adult
• Identify factors unique to the older adult that contribute to prognosisprognosis
• Discuss quality of life findings for older adults with hematologic malignancies
• Discuss methods to improve quality of life in the older adult with a hematologic malignancy
Hematologic malignancy Median age of diagnosis
• 30% of patients newly diagnosed with hematologic malignancy p y g g g yare over age 75
• Lymphoma– Non-Hodgkin lymphoma-83% of patients diagnosed after the
age of 50• Leukemia• Leukemia
– CLL- age 71; AML- age 67; CML-age 64• Multiple Myeloma, MDS, Hodgkin Lymphoma, ALLp y , , g y p ,
Factors contributing to prognosis in the older adult undergoing treatment for hematologic malignancy
• Type of hematologic malignancy/treatmentyp g g y• Functional age• Increased numbers of comorbidities• Decreased organ reserve• Polypharmacy
f• Performance status prior to diagnosis and treatment• Development of geriatric syndromes• USE of GERIATRIC ASSESSMENT KEY• USE of GERIATRIC ASSESSMENT KEY
Treatment approaches and lifelong effects
• Surgery g y• Radiation- skin damage, organ damage, loss of function• Chemotherapy-cardiotoxicity, pulmonary toxicity, neuropathy,
cognitive changes• Immunotherapy-infection risk, PML, CRS, unknowns
Decreased organ reserve
• Pre-treatment- diagnostic testing, supportive medications, g g, pp ,medications for cormorbidities, nutrititional status, fluid/electrolyte balanceT t t id ff t t iti l t t di ti t• Treatment-side effects, nutritional status, medications to manage symptoms
• Post-treatment-immunosuppression, anti-infectives,Post treatment immunosuppression, anti infectives, fluid/electrolyte balance
• Orthostatic hypotension, anticholinergics, opiates
Polypharmacy
• Many patients are on multiple medications prior to cancer y p p pdiagnosis
• Medications required to manage toxicity are often dangerous in th ld d ltthe older adult
• Beers Criteria for potentially inappropriate drugs– AGS website *AGS website
How to Use AGS 2015 Beers Criteria
Key Principles to Guide Optimal Use of theAmerican Geriatrics Society (AGS) 2015 Beers Criteria
• Patients- review current meds if concerned about interactions at
• 1 Medications in the AGS 2015 Beers Criteria are potentially• inappropriate, not definitely inappropriate.• 2 Read the rationale and recommendations statements for each• criterion. The caveats and guidance listed there are important.• 3 Understand why medications are included in the AGS 2015
B C it i d dj t h t th di ti
www.nlm.nih.gov/medlineplus/druginformation.html• Clinicians- use Beers criteria as a warning sign to do an in
depth review of the medication and potential interactions– Use criteria as a tool to decide on whether to adjust
prescriptions with patient• Beers Criteria and adjust your approach to those medications• accordingly.• 4 Optimal application of the AGS 2015 Beers Criteria involves• identifying potentially inappropriate medications and where• appropriate offering safer nonpharmacological and
pharmacological
– Make sure to taper medication when switching– Assess for interactions/symptoms in individual
patient
g• therapies.• 5 The AGS 2015 Beers Criteria should be a starting point for a• comprehensive process of identifying and improving medication• appropriateness and safety.• 6 Access to medications included in the AGS 2015 Beers Criteria• should not be excessively restricted by prior authorization• and/or health plan coverage policies.• 7 The AGS 2015 Beers Criteria are not equally applicable to all
• Patients- review meds at www.nlm.nih.gov/medlineplus/druginformation.htmlg p g
• Clinicians-
Functional Status Beyond ECOG and KPS
Activities Daily Living Instrumental ADLy g• Bathing • Dressing
• Use telephone• Shopping
• Toileting• Transferring
C
• Food preparation • Housekeeping
• Continence• Feeding
• Laundry• Transportation (drives or
takes public transport)takes public transport)• Take own meds• Handle finances
Functional Status and Quality of Life
• Inability to return to previous level of activity is associated with y p ydecreased quality of life
• Geriatric assessment can identify deficits overlooked otherwise• Utilization of PT/OT
– Physical therapy improves gait and physical functionOT focuses on participation in activities cognitive function– OT focuses on participation in activities, cognitive function, IADL
Study by Pergolotti et al showed that age, comorbidities and y y g g ,level of education increased odds of functional limitations that are modifiable
Geriatric Syndromes
• Older adults are prone to having geriatric syndromesp g g y• Health related conditions that do not follow a specific diagnosis • Are prevalent in older adults, especially the frail elderly• Can impact patient quality of life and poor outcomes• What are geriatric syndromes?........
Considerations in Geriatric Syndrome
• Multiple morbiditiesp• Polypharmacy• Cognitive impairment• Frailty• Disabilty
S• Sarcopenia• Malnutrition
SPICES Framework for Assessment
• Systematic screening tool • Signals need for more specific assessment
• Acronym of six common marker conditions• Acronym of six common marker conditions– S is for sleep disorders– P is for problems with eating or feeding
f– I is for incontinence– C is for confusion– E is for evidence of fallsE is for evidence of falls– S is for skin breakdown
Used with permission www.nicheprograms.org
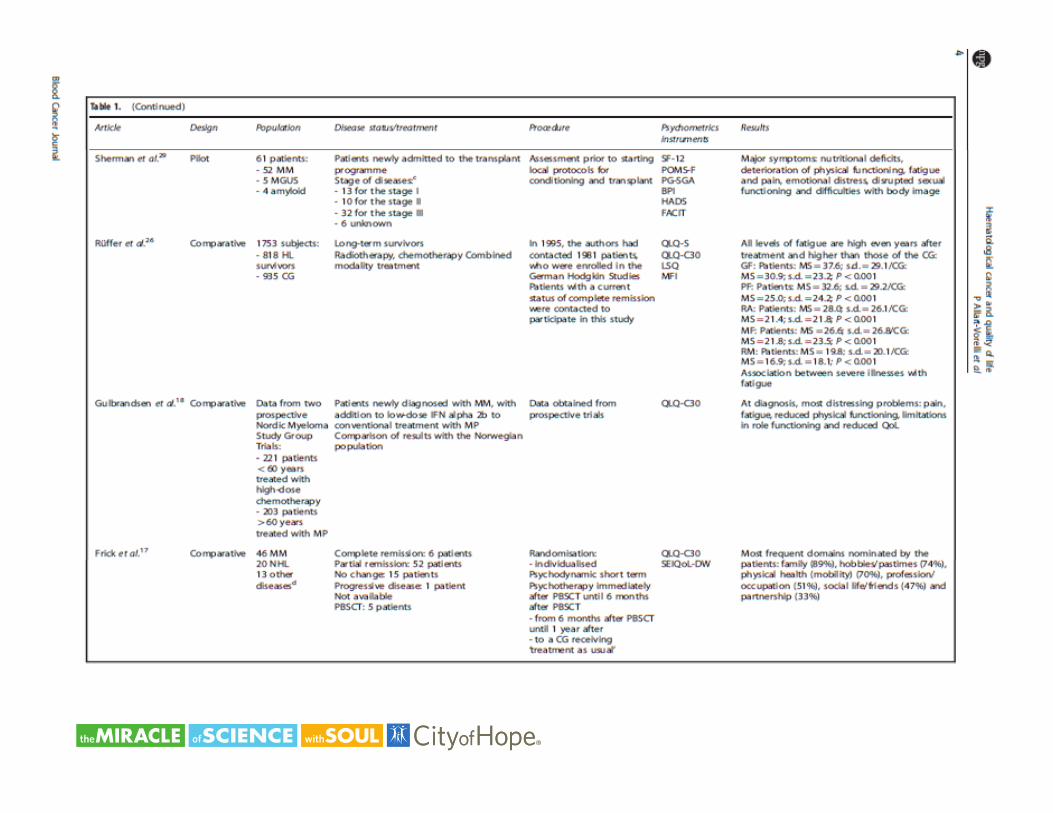
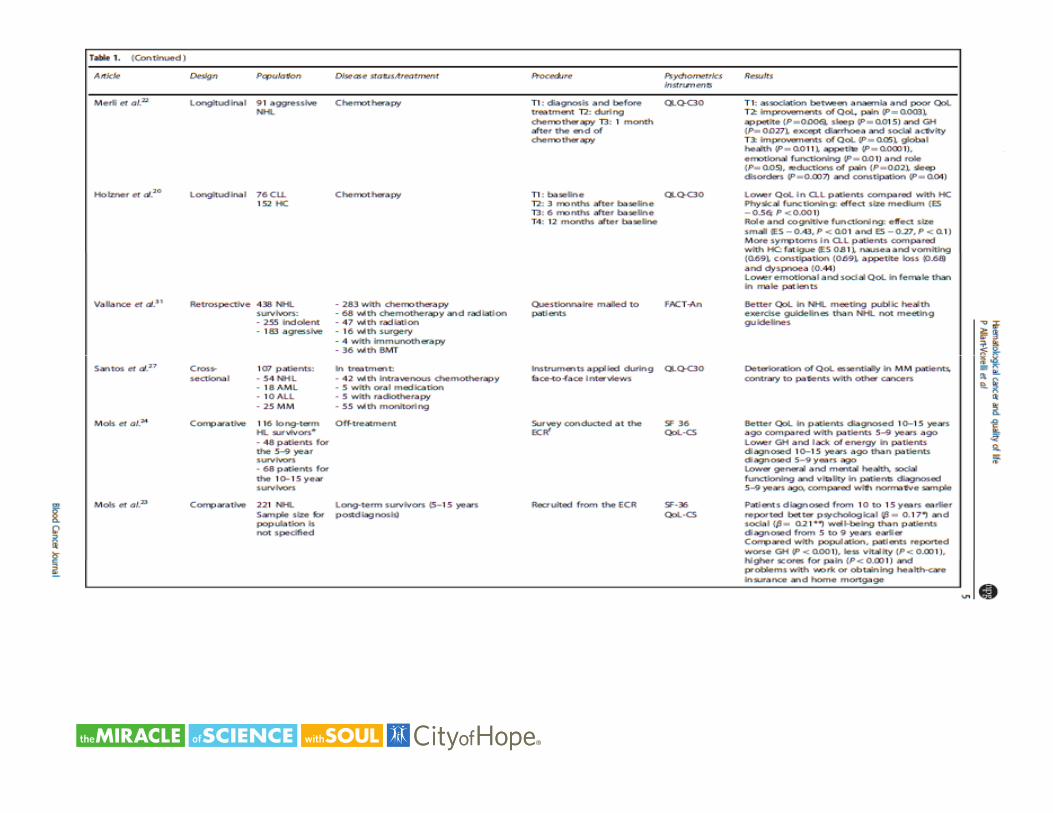
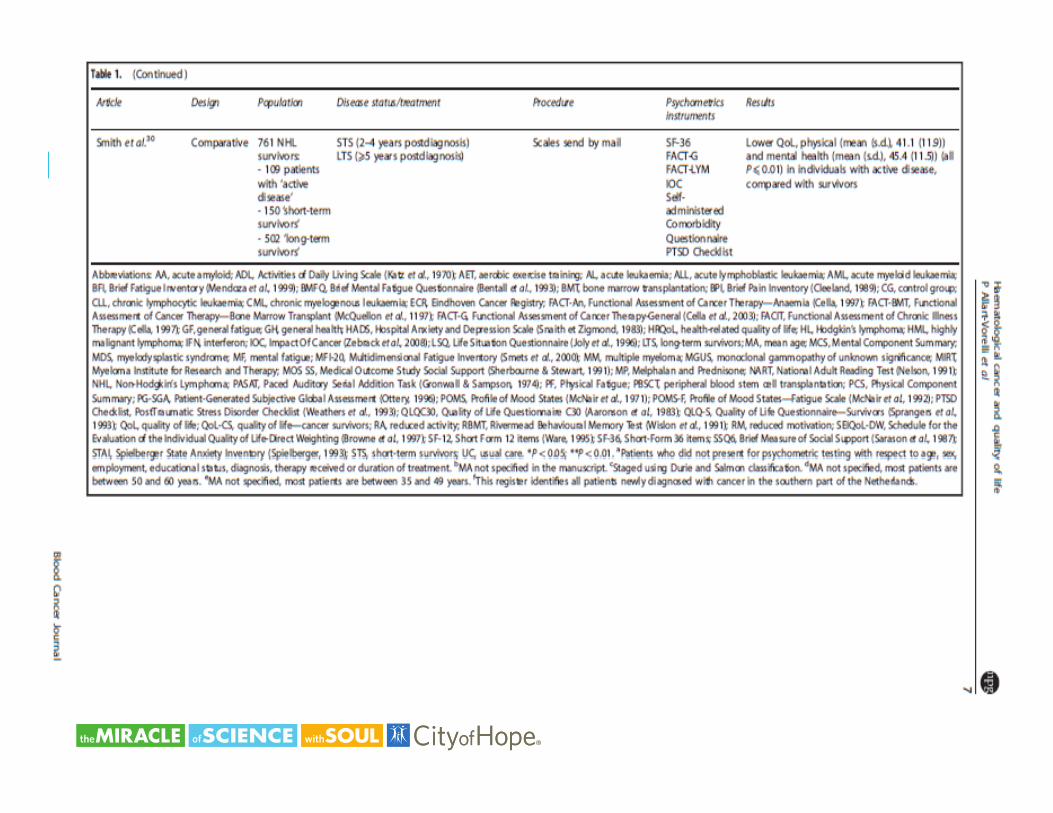
Quality of life for patients with hematologic malignancies
• Quality of life associated with different factors by individualQ y y• Multiple studies show the importance of baseline Quality of Life
parameters as independent prognostic factors in this population • How to accurately predict effects of disease and selected
treatment on future QOL– Deeg & Steuten show that QOL in patients post transplant withDeeg & Steuten show that QOL in patients post transplant with
AML have decreasing scores correlated with age

Decrease in QOL consistent among hematologic malignancy sufferers

Recommendations
• Ask patient what factors contribute to individual perception of p p pgood QOL
• Identify and intervene early for modifiable factors that may di i i h QOL d i th l tdiminish QOL now and in the long term
• Utilize geriatric assessment approaches throughout the treatment continuumtreatment continuum
• Assemble multidisciplinary team to address challenges from a multi-pronged approach
• Reevaluate QOL at multiple time points along care continuum
Case Study
• AR- 70y/o male with • Lives with elderly wife that yhistory of myelodysplastic syndromeP i t AML
ysuffers from early dementiaR ibl f ll• Progression to AML
• Presented with severe fatigue, anemia, and
• Responsible for all instrumental ADLs
• Med HX- Diabetes, HTN,fatigue, anemia, and epistaxis
• Currently hospitalized for k d t t t
Med HX Diabetes, HTN, CKD Stage II
• Expresses high level of i t di dworkup and treatment anxiety re: disease and
treatment
References
• Steinman, M.A. etal (2015). How to use the american geriatrics society 2015 Beers criteria- a guide for patients, clinicians, health systems and payors. JAGS 63(1-7)
• Pergolotti, M. et al. (2015). The prevalence of potentially modifiable functional deficits and the subsequent use of occupational and physical therapy by older adults with cancer. Science Direct,6 (194-201)
• Allart-Vorelli, P, et al. (2015). Haematological cancer and quality of life: a systematic literatureAllart Vorelli, P, et al. (2015). Haematological cancer and quality of life: a systematic literature review. Blood 305 (10)
• Sekeres, MA et al. (2004) Decision-making and quality of life in older adults with acute myeloid leukemia or advanced myelodysplastic syndrome. Leukemia18, (809-816)D hl B t l (2013) P t d t t d b i t i d lit f lif t i 195• Deschler, B. et al (2013). Parameters detected by geriatric and quality of life assessment in 195 older patients with myelodysplastic syndromes and acute myeloid leukemia are highly predictive for outcome. Haematologica 98 (2)
• DeSantis, C.E. et al. (2014). Cancer treatment and survivorship and statistics, 2014. CA: A journal for clinicians. 64 (4)
• Maggior, R.J. et al (2014). Polypharmacy and potentially inappropriate medication use in older adults with cancer undergoing chemotherapy: effect on chemotherapy-related toxicity and hospitalization during treatment. JAGS 62 (8)