Embed Size (px)
Citation preview
GI bleedingGI bleeding
Mackay Memorial Hospital
Department of Internal Medicine
Division of Gastroenterology
R4 陳泓達
97/6/22
GI BleedingGI Bleeding UGI bleedingUGI bleeding
Peptic ulcer diseasePeptic ulcer disease Variceal bleedingVariceal bleeding
LGI bleedingLGI bleeding
UGI bleeding: 5 times more common than LGI UGI bleeding: 5 times more common than LGI bleeding. bleeding.
Men > WomenMen > Women
Elderly persons.Elderly persons. Despite ongoing advances, fundamental Despite ongoing advances, fundamental
principles are the same !!!!principles are the same !!!!
immediate assessment and stabilization of immediate assessment and stabilization of
hemodynamic statushemodynamic status
Determine the source of bleedingDetermine the source of bleeding Stop active bleedingStop active bleeding Treat underlying abnormalityTreat underlying abnormality Prevent recurrent bleedingPrevent recurrent bleeding
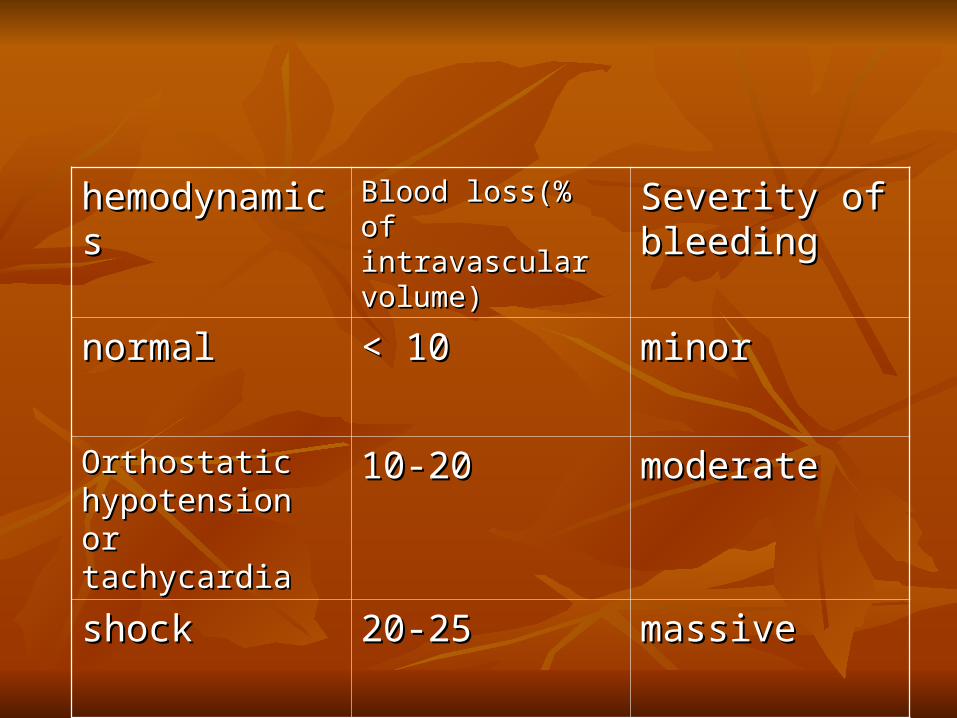
hemodynamicshemodynamics Blood loss(% of Blood loss(% of intravascular volume)intravascular volume)
Severity of Severity of bleedingbleeding
normalnormal < 10< 10 minorminor
Orthostatic Orthostatic hypotension or hypotension or tachycardiatachycardia
10-2010-20 moderatemoderate
shockshock 20-2520-25 massivemassive
ResuscitationResuscitation
In hemodynamically unstable…In hemodynamically unstable…
Set up two large-bore IV catheterSet up two large-bore IV catheter
Colloid solution (NS or lactated Ringer’s) Colloid solution (NS or lactated Ringer’s) To restore vital sign !!To restore vital sign !!
ICU monitor is indicatedICU monitor is indicated
Central venous monitoringCentral venous monitoring
F/U vital sign and urine output F/U vital sign and urine output
History taking and physical examinationHistory taking and physical examination
UGI or LGI ?UGI or LGI ?
UGI UGI peptic ulcer disease or portal peptic ulcer disease or portal hypertension related (EV or GV)?hypertension related (EV or GV)?
Differentiate LGI and UGIDifferentiate LGI and UGIMelena – upper GI cause in 90%Melena – upper GI cause in 90%Hematochezia – upper GI cause in 10%Hematochezia – upper GI cause in 10%
The intermediate patientThe intermediate patient
Take more time….Take more time….
Re-examine,Re-examine,
Monitor vital signs,Monitor vital signs,
Re-check CBC, BUNRe-check CBC, BUN
Transfusion ?Transfusion ? In hemodynamic unstable, any sign of poor In hemodynamic unstable, any sign of poor
tissue oxygenation, continued bleeding, tissue oxygenation, continued bleeding, persistent low Ht level(20-25%)persistent low Ht level(20-25%)
Maintain adequate perfusionMaintain adequate perfusion Target ?Target ?
Other Blood tests on the Other Blood tests on the bleeding patient…bleeding patient…
INR, PTTINR, PTT
– coagulopathy anyone?
““There is no single value of There is no single value of hemoglobin concentration that hemoglobin concentration that
justifies or requires transfusion; justifies or requires transfusion; an evaluation of the patient’s an evaluation of the patient’s
clinical situation should also be a clinical situation should also be a factor in the decision.”factor in the decision.”
Capital Health Guide to Blood TransfusionCapital Health Guide to Blood Transfusion
You’ve decided to give You’ve decided to give blood…blood…
Options?Options?
O neg O neg Type Specific Type Specific Full Cross MatchFull Cross Match
– immediately available – 10 – 15 min. – 30 – 60 min.
What is in a unit of What is in a unit of packed cells?packed cells?
250 mL volume250 mL volumeContains citrate (anticoagulant), and preservContains citrate (anticoagulant), and preserv
ative.ative.1 unit packed cells will increase the Hb conc1 unit packed cells will increase the Hb conc
entration by approx. --?entration by approx. --? 0.5mg/dL
Massive TransfusionMassive Transfusion
Greater than 1 blood volume( or 10 units ) Greater than 1 blood volume( or 10 units ) transfused within 24 hourstransfused within 24 hours
May dilute platelets and clotting factorsMay dilute platelets and clotting factors
Dilution coagulopathyDilution coagulopathy
Monitor the patient for coagulopathyMonitor the patient for coagulopathyFollow the resuscitation (CBC, INR, PTT)Follow the resuscitation (CBC, INR, PTT)
Treatment of dilution coaTreatment of dilution coagulopathygulopathy
Plasma /FFPPlasma /FFP 10 – 15 mL / kg 10 – 15 mL / kg
Usual adult dose 2 units.Usual adult dose 2 units.
5 –8 mL / kg dose for warfarin revers5 –8 mL / kg dose for warfarin reversalal
Treatment of dilution coagulTreatment of dilution coagulopathyopathyPlateletsPlatelets
Keep the count greater than 50 ,000 in the Keep the count greater than 50 ,000 in the bleeding patientbleeding patient
1 unit should increase platelet count by 1 unit should increase platelet count by 5 ,000– 10, 000 / L5 ,000– 10, 000 / L
Dose: 6 packDose: 6 pack
Massive TransfusionMassive TransfusionWhat else can go wrong?What else can go wrong?
HypothermiaHypothermia
PotassiumPotassium
Citrate toxicity (hypocalcemia)Citrate toxicity (hypocalcemia)
Vomiting BloodVomiting BloodHematemesisHematemesis
Upper GI BleedingUpper GI Bleeding
EtiologyEtiology
Peptic Ulcer 50 %Peptic Ulcer 50 %Gastritis 20%Gastritis 20%Esophageal varices 10%Esophageal varices 10%The rest: Tears, AVM, CA,etc 20%The rest: Tears, AVM, CA,etc 20%
More about bleeds….More about bleeds….
80 % of Non – variceal upper GI ble80 % of Non – variceal upper GI bleeds will stop spontaneouslyeds will stop spontaneously
60 % of variceal bleeds will stop spo60 % of variceal bleeds will stop spontaneouslyntaneously
What else can I do for GI bleeding, What else can I do for GI bleeding, before endoscopybefore endoscopy
NG lavageNG lavage
DrugDrug
ABCABC
Patient and family AgreePatient and family Agree
( Sign permit first)( Sign permit first)
Urgent Endoscopy ?Urgent Endoscopy ?Initial evaluation: Initial evaluation: 初始出血量是否大量 初始出血量是否大量 ??出血量大者出血量大者 ,rebleeding ,rebleeding 機會也大機會也大觀察重點觀察重點 : vital sign (tachycardia, orthost: vital sign (tachycardia, orthost
atic atic hypotension resting hypotension, shock),hypotension resting hypotension, shock),
吐血或吐血或血便黑便的頻次與量血便黑便的頻次與量 , NG lavage, NG lavage 的結果的結果
NG lavage NG lavage
15 – 20 % of upper GI bleeds have a n15 – 20 % of upper GI bleeds have a negative aspirate egative aspirate
Sensitivity 79%, Specificity 55%Sensitivity 79%, Specificity 55%Cuellar et al, Arch of Int Med Jul 1990Cuellar et al, Arch of Int Med Jul 1990
•For endoscopic preparation( not contraindicated in patients with varices)
EndoscopyEndoscopy
DiagnosticDiagnosticTherapeuticTherapeuticPrognosticPrognostic
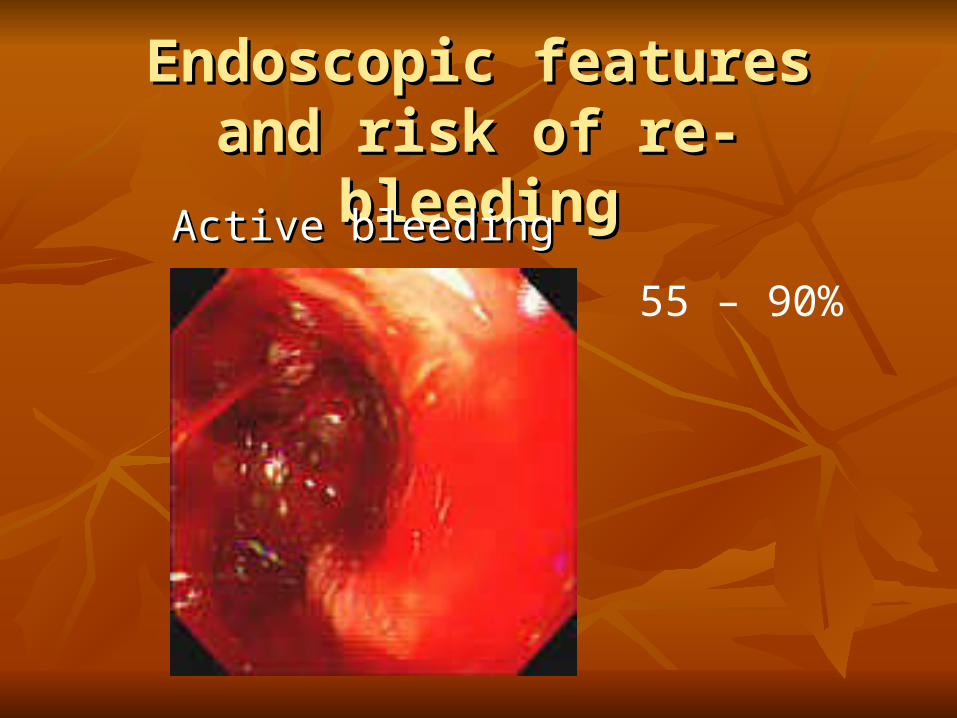
Endoscopic features and risk of Endoscopic features and risk of re-bleedingre-bleeding
Active bleedingActive bleeding
55 – 90%
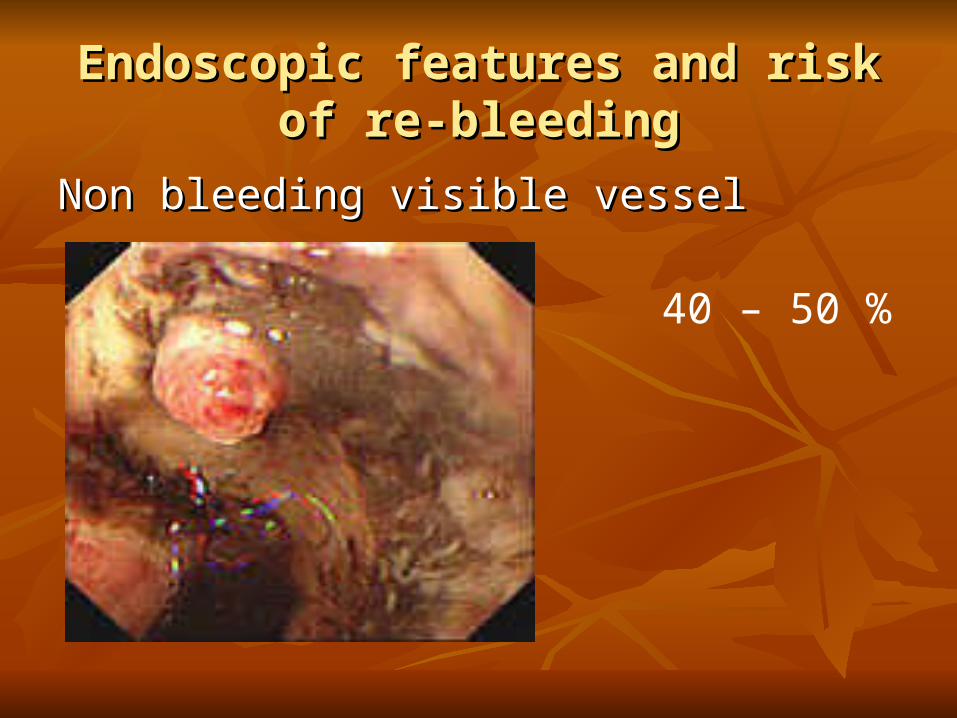
Endoscopic features and risk of re-Endoscopic features and risk of re-bleedingbleeding
Non bleeding visible vesselNon bleeding visible vessel
40 – 50 %
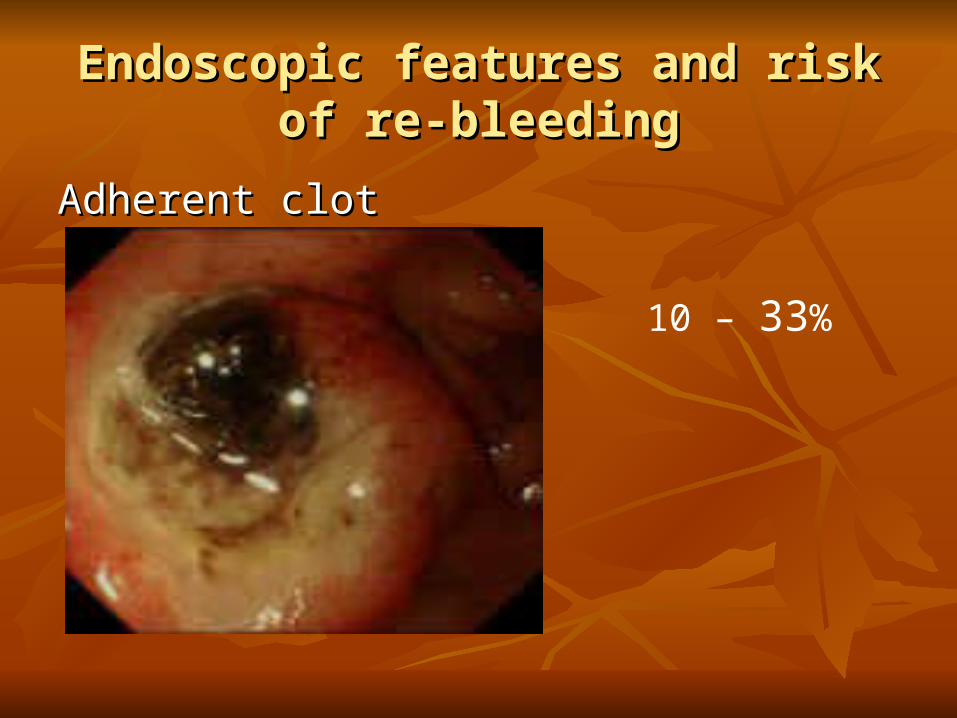
Endoscopic features and risk of re-Endoscopic features and risk of re-bleedingbleeding
Adherent clotAdherent clot
10 – 33%

Endoscopic features and risk of re-Endoscopic features and risk of re-bleedingbleeding
Flat spotFlat spot
7 – 10 %
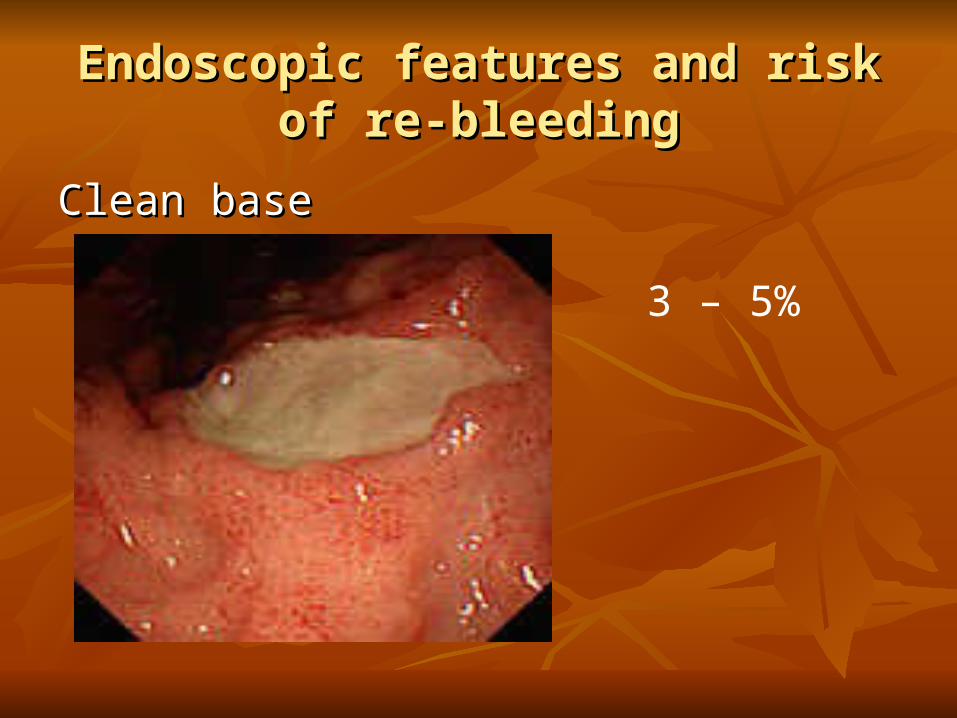
Endoscopic features and risk of re-Endoscopic features and risk of re-bleedingbleeding
Clean baseClean base
3 – 5%
Variceal bleedingVariceal bleeding
Non-variceal bleedingNon-variceal bleeding
Drugs: Peptic ulcer bleedingDrugs: Peptic ulcer bleeding
Manipulation of gastric pH Manipulation of gastric pH
Use of PPI’sUse of PPI’s
Theory : raise gastric pHTheory : raise gastric pHBetter platelet activityBetter platelet activity
Pepsinogen requires acid to become Pepsinogen requires acid to become activated to pepsinactivated to pepsin
Clots will form, clots not digestedClots will form, clots not digested
High Risk PatientsHigh Risk PatientsElderlyElderly
Co – MorbidityCo – MorbidityMore severe bleeding (hemo-dynamically uMore severe bleeding (hemo-dynamically u
nstable, ongoing bleedingnstable, ongoing bleeding
Other helpful medication Other helpful medication
somatostatin / octreotide somatostatin / octreotide associated with a reduced risk of contassociated with a reduced risk of continued bleeding and rebleeding in PUinued bleeding and rebleeding in PUD D
When endoscopic / pharmacological treatment When endoscopic / pharmacological treatment fail…fail…
◎ ◎ angiography angiography to localize bleeder and to localize bleeder and hemostasishemostasisgenerally reserved for patient: generally reserved for patient: poor surgical candidatespoor surgical candidates control of bleeding in an unstable patient control of bleeding in an unstable patient awaiting surgeryawaiting surgery
SurgerySurgery
Hemodynamic instability despite Hemodynamic instability despite vigorous resuvigorous resuscitationscitation (more than a three unit transfusion) (more than a three unit transfusion)
Recurrent hemorrhage after initial stabilization Recurrent hemorrhage after initial stabilization (attempts at obtaining (attempts at obtaining endoscopic hemostasisendoscopic hemostasis) )
ShockShock associated with recurrent hemorrhage associated with recurrent hemorrhage Continued slow bleeding with a transfusion reContinued slow bleeding with a transfusion re
quirement exceeding three units per day.quirement exceeding three units per day.
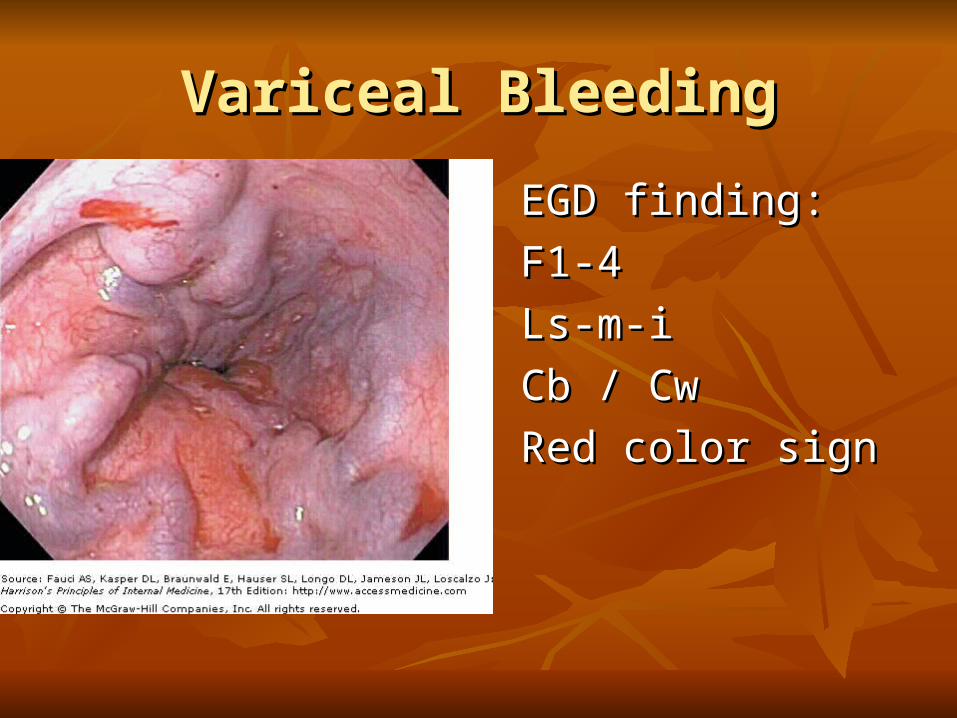
Variceal BleedingVariceal Bleeding
EGD finding:EGD finding:
F1-4F1-4
Ls-m-iLs-m-i
Cb / CwCb / Cw
Red color signRed color sign
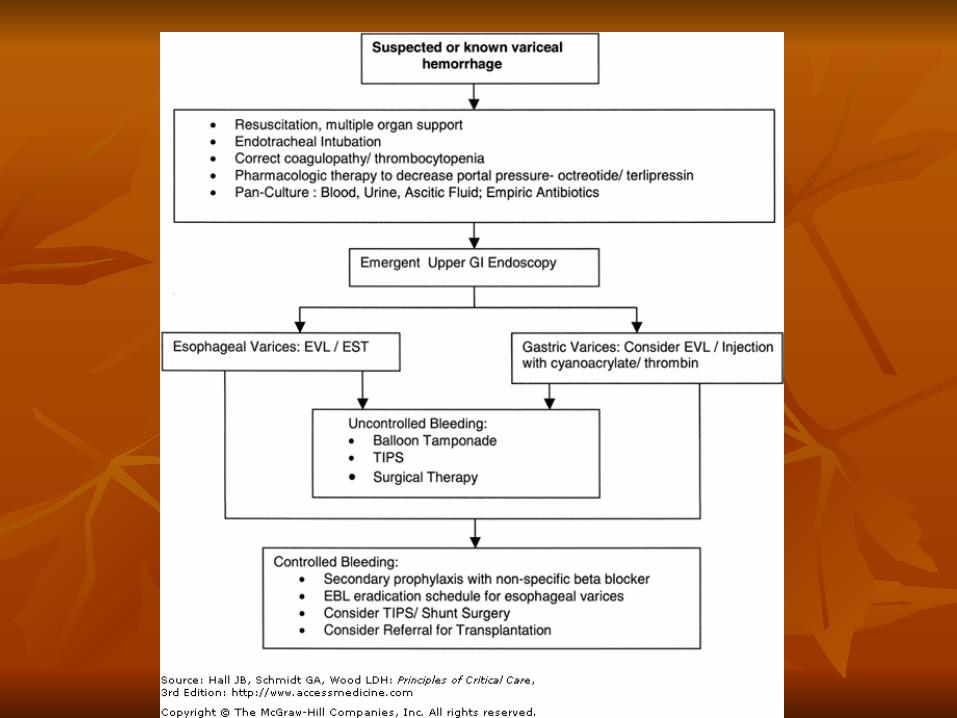
After endoscopic treatment…After endoscopic treatment…
Fail to achieve hemostasis or rebleeding Fail to achieve hemostasis or rebleeding
Balloon tamponadeBalloon tamponade Transjugular Intrahepatic Portosystemic Shunt Transjugular Intrahepatic Portosystemic Shunt
(TIPS)(TIPS) Surgery for shuntSurgery for shunt

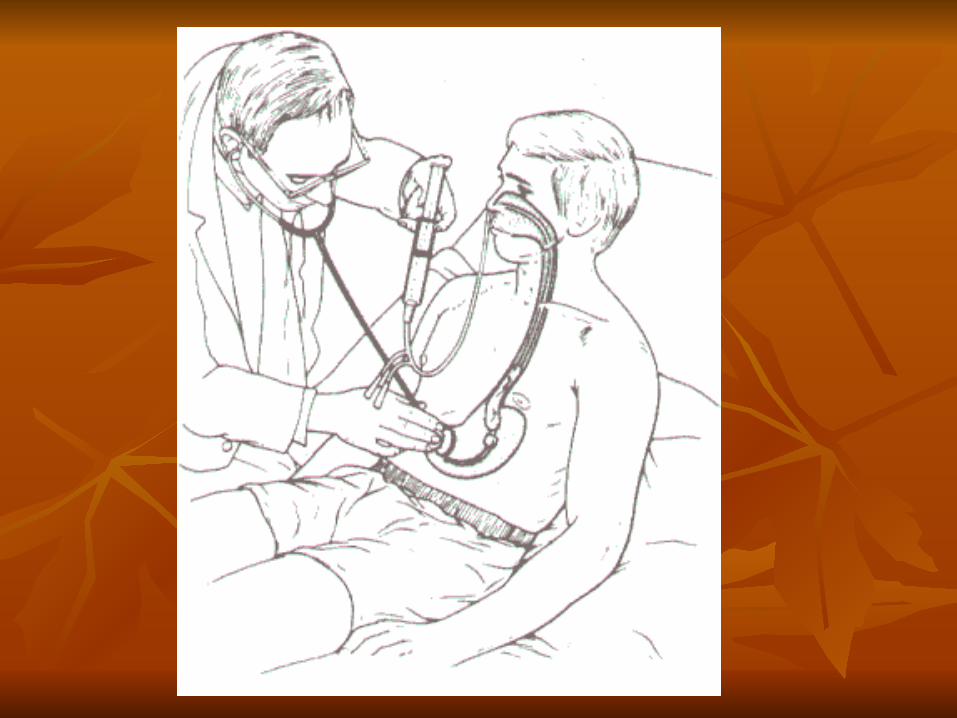
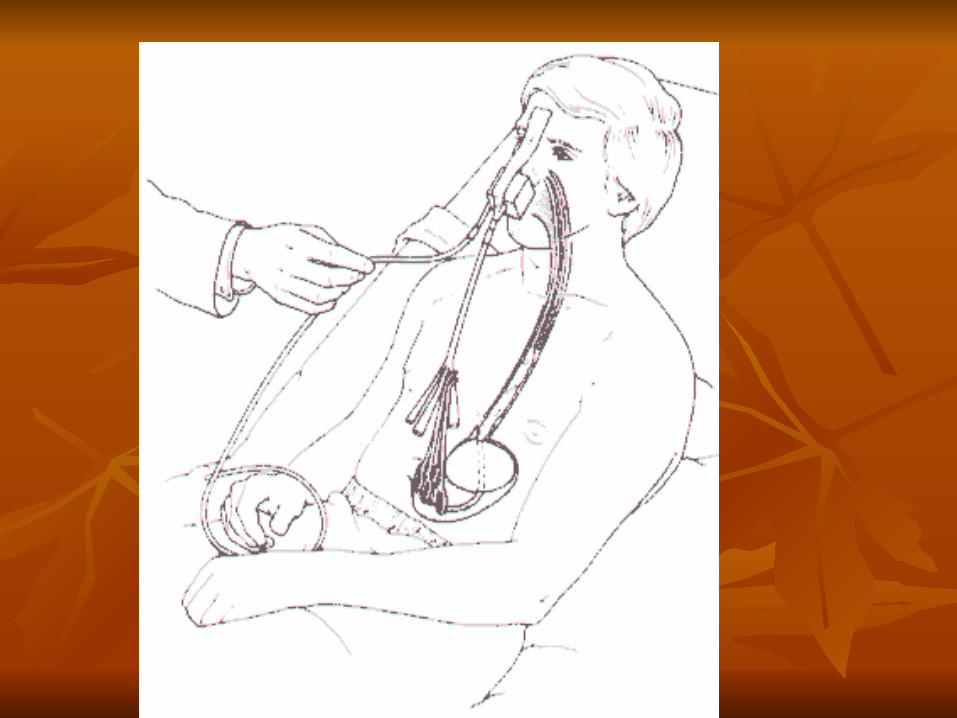
Balloon TamponadeBalloon Tamponade-Buy time-Buy timeAvailable in MMHAvailable in MMH
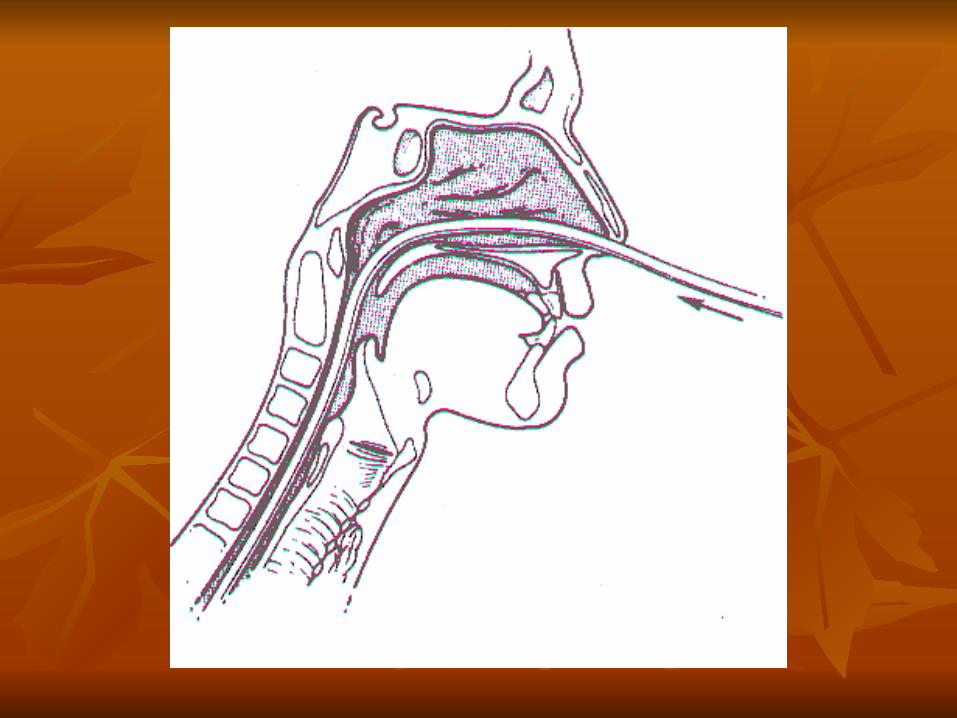
S-B tube S-B tube
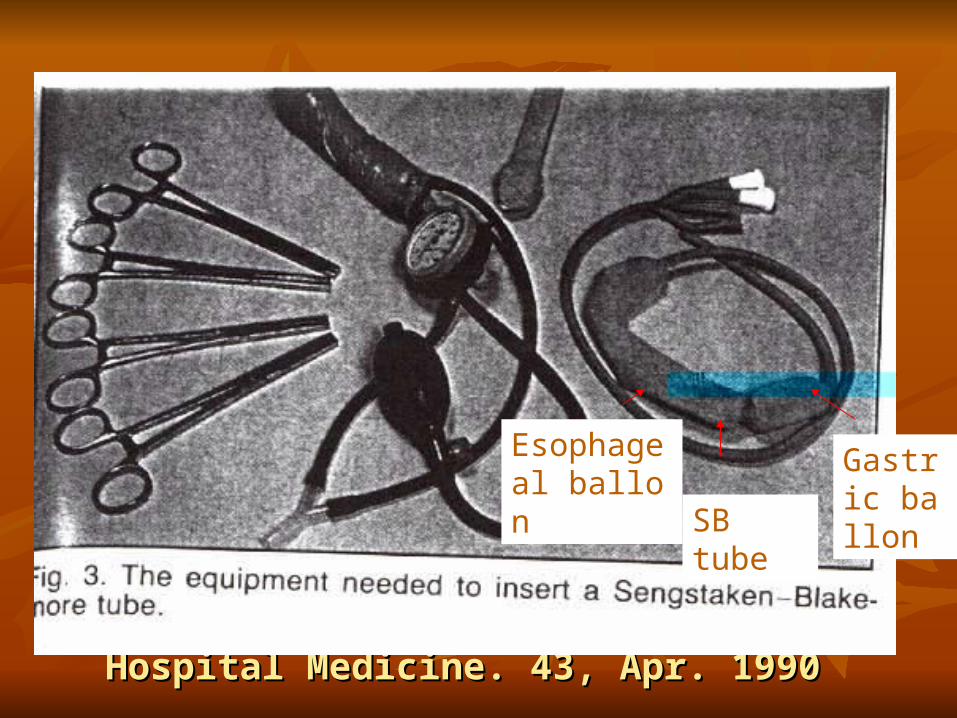
McCormick. British Journal of Hospital McCormick. British Journal of Hospital Medicine. 43, Apr. 1990Medicine. 43, Apr. 1990
SB tube
Gastric ballon
Esophageal ballon
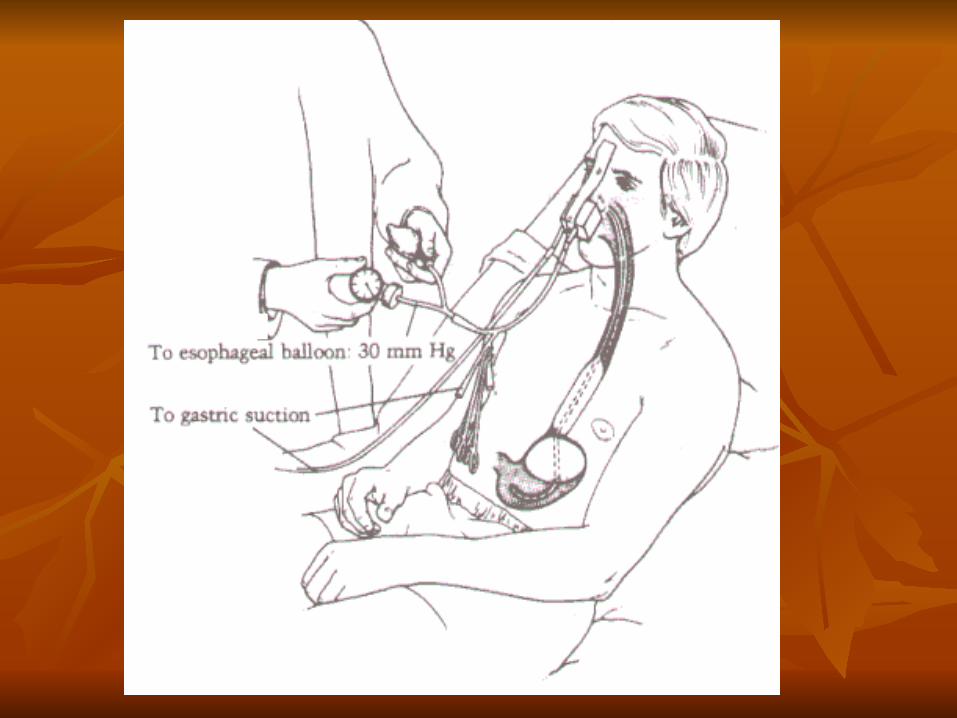
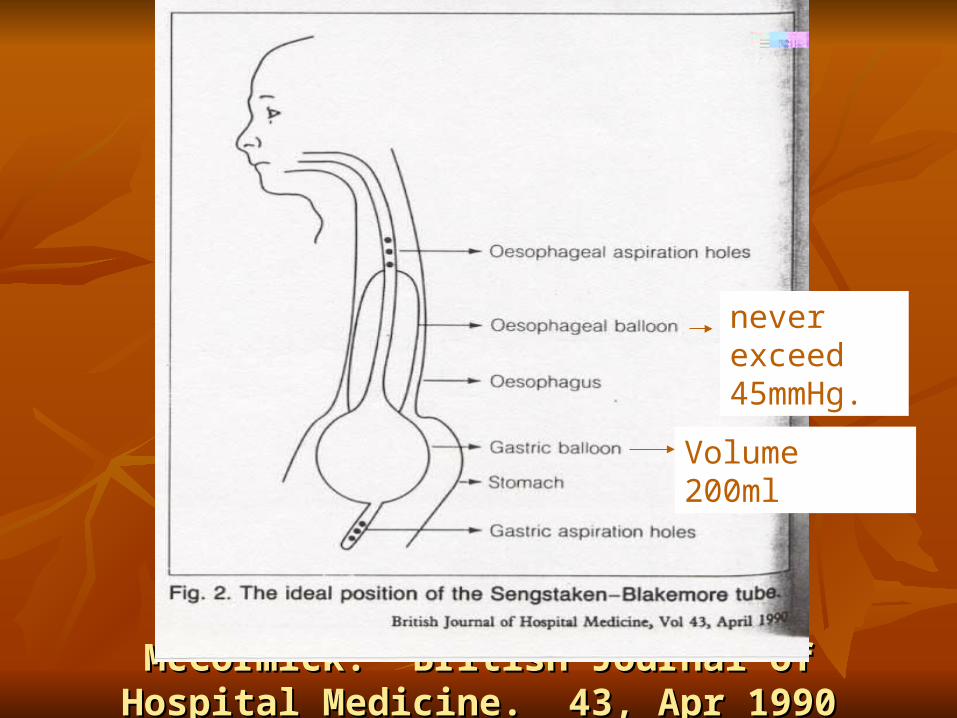
McCormick. British Journal of Hospital McCormick. British Journal of Hospital Medicine. 43, Apr 1990Medicine. 43, Apr 1990
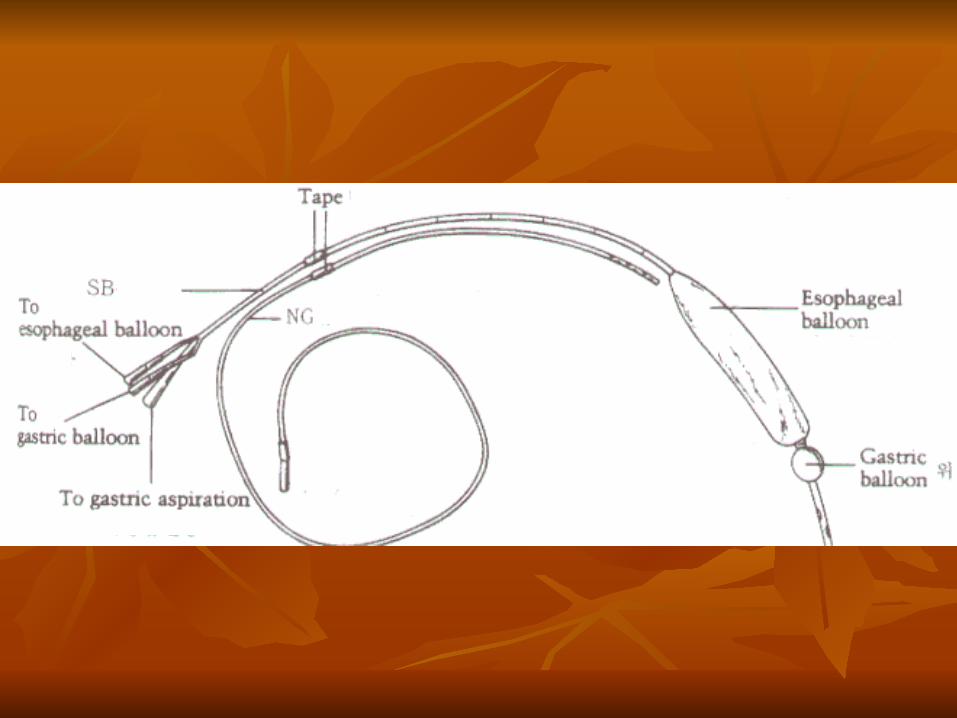
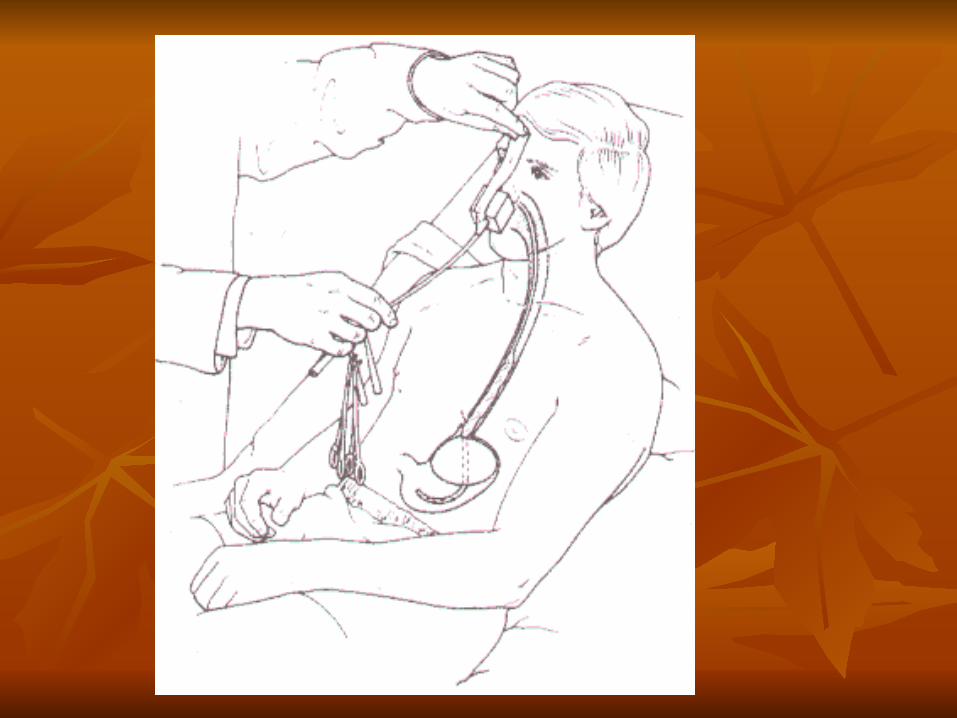
never exceed 45mmHg.
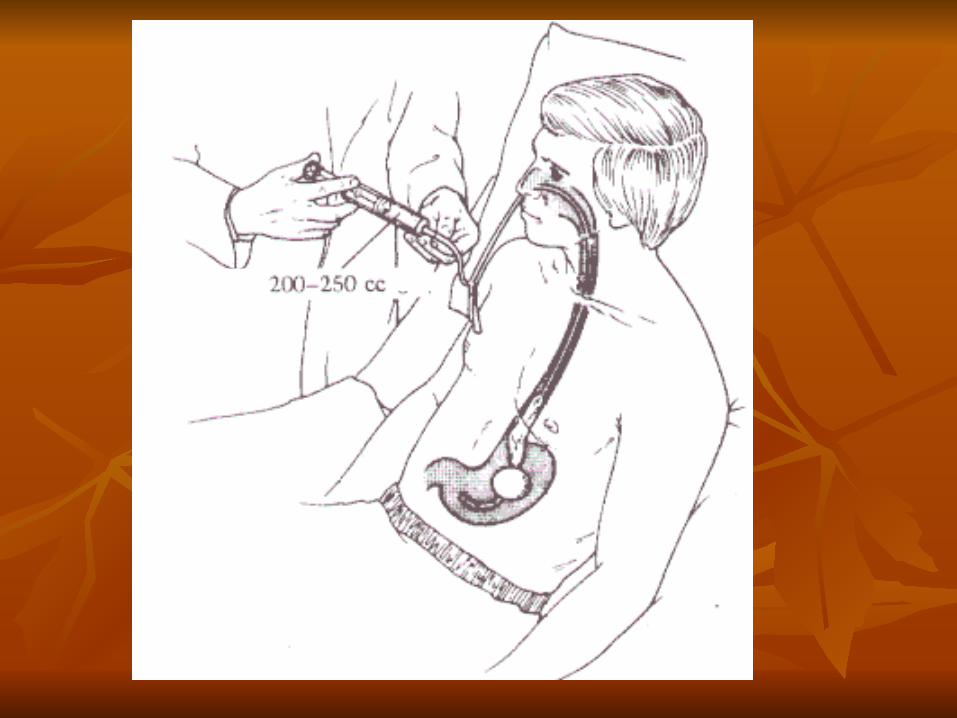
Volume 200ml

Tamponade Tube Tamponade Tube Sengstaken-Blakemore (S-B) tubeSengstaken-Blakemore (S-B) tube
Radiographic confirmation of the gastric balRadiographic confirmation of the gastric balloon’s position -- 30cc air inflate the gastric loon’s position -- 30cc air inflate the gastric balloonballoon
Insufflation of the esophageal balloon to 35Insufflation of the esophageal balloon to 35mmHgmmHg
Compression of varices for not excess 48 Compression of varices for not excess 48 hourshours
Deflate the esophageal balloon for about 3Deflate the esophageal balloon for about 30 mins every 12 hours0 mins every 12 hours
Major complications -- aspiration and esoMajor complications -- aspiration and esophageal perforation phageal perforation
Control hemorrhage >90%, but it is tempoControl hemorrhage >90%, but it is temporaryrary
Bridging procedureBridging procedure buy time buy time
Definite therapeutic management must be Definite therapeutic management must be performed.performed.
Lower GI BleedingLower GI Bleeding
Hematochezia 90%Hematochezia 90%
Melena 10%Melena 10%
EtiologyEtiology
Most blood passed per rectum is from Most blood passed per rectum is from the upper GI tract.the upper GI tract.
Lower GI BleedsLower GI Bleeds
Diverticulosis, angiodysplasia, CA, cDiverticulosis, angiodysplasia, CA, colitis, ischemia, hemorrhoidsolitis, ischemia, hemorrhoids
More about Lower GI More about Lower GI BleedsBleeds
80% resolve spontaneously80% resolve spontaneously25 % will re–bleed25 % will re–bleedUsually painlessUsually painlessIf painful, r/o mesenteric ischemiaIf painful, r/o mesenteric ischemia
Investigation of the lower Investigation of the lower GI bleedGI bleed
The usual suspects: CBC, BUN, CreThe usual suspects: CBC, BUN, Creatinine, INR, PTT, T/Satinine, INR, PTT, T/S
Investigation of the lower Investigation of the lower GI bleedGI bleed
Plain X-rays and abd. CT – not much help Plain X-rays and abd. CT – not much help unless you clinically suspect perforation, ounless you clinically suspect perforation, o
bstruction, ischemia (PAIN)bstruction, ischemia (PAIN)
Diagnostic procedureDiagnostic procedureEndoscopyEndoscopy : 80% accuracy : 80% accuracy
Poor visibility with heavy bleedingPoor visibility with heavy bleeding
•Angiography : 40–80% accuracy Requires heavy bleeding Able to perform embolization or vasopressin infusion
Diagnostic procedureDiagnostic procedure
RBC scans RBC scans 25–90% accurate25–90% accurateAble to do with lower bleeding ratesAble to do with lower bleeding rates
What if the patient is What if the patient is really bleeding?really bleeding?
Involve your consultants early. Involve your consultants early.
Radiologist for angiographyRadiologist for angiography
Procto. If tumor or ischemic bowelProcto. If tumor or ischemic bowel





























