Embed Size (px)
Citation preview

MINISTERUL EDUCAŢIEI NAŢIONALE
UNIVERSITATEA „VALAHIA” DIN TÂRGOVIŞTE
IOSUD-ŞCOALA DOCTORALĂ DE ŞTIINŢE ECONOMICE ŞI
UMANISTE
Domeniul: MANAGEMENT
REZUMATUL TEZEI DE DOCTORAT
GUVERNANŢA CLINICĂ:
MIZĂ MAJORĂ PENTRU PERFORMANŢA
SPITALELOR PUBLICE DIN ROMÂNIA
CONDUCĂTOR ŞTIINŢIFIC:
Prof. univ. dr. CONSTANŢA POPESCU
DOCTORAND:
GULAY AVCI (KAKILLIOGLU)
TÂRGOVIŞTE
2019
CUPRINSUL REZUMATULUI TEZEI DE DOCTORAT
CUPRINSUL TEZEI DE DOCTORAT ................................................................................. 3
CUVINTE CHEIE .................................................................................................................... 7
IMPORTANŢA, ACTUALITATEA ŞI NOUTATEA TEMEI ........................................... 7
PROBLEMATICĂ ȘI IPOTEZE............................................................................................ 8
POZIȚIONAREA EPISTEMOLOGICĂ A TEZEI DE DOCTORAT ............................... 9
STRUCTURA TEZEI DE DOCTORAT ............................................................................... 9
CONCLUZII GENERALE .................................................................................................... 18
APORTURILE (CONTRIBUŢIILE) ŞTIINŢIFICE ALE TEZEI DE DOCTORAT .... 23
LIMITELE CERCETĂRII NOASTRE ŞTIINŢIFICE ..................................................... 24
PERSPECTIVE DE CERCETARE...................................................................................... 25
BIBLIOGRAFIE .................................................................................................................... 26
CURRICULUM VITAE ........................................................................................................ 41
LISTA LUCRĂRILOR ȘTIINȚIFICE ................................................................................ 43
CUPRINSUL TEZEI DE DOCTORAT
Listă cadrane..................................................................................................................... 4
Listă figuri......................................................................................................................... 5
Listă tabele ....................................................................................................................... 6
Lista abreverilor ............................................................................................................... 7
Glosar ................................................................................................................................ 9
INTRODUCERE............................................................................................................. 15
CAPITOLUL 1. SERVICIILE DE SĂNĂTATE: TERMENI, CONCEPTE ŞI
ABORDĂRI TEORETICE…………………………………………...
21
1.1. Sănătatea: definire şi modele de abordare…………………………………………… 21
1.2. Sănătatea publică: definire…………………………………………………………... 24
1.3. Determinanţii sociali ai sănătăţii: cadrul theoretic…………………………………… 25
1.4. Economia sănătăţii: fundament teoretic al pieţei serviciilor de sănătate…………… 27
1.5. Sistem de sănătate şi sistem al serviciilor de sănătate: definire şi delimitare………. 31
1.6. Îngrijirile de sănătate primare: definire şi importanţă………………………………... 35
1.7. Sistemele serviciilor de sănătate: evoluţie din perspectivă epistemologică…………. 38
1.8. Sistemul serviciilor de sănătate: sistem organizat de acțiune………………………... 43
Concluziile capitolului ………………………………………………............................. 47
CAPITOLUL 2. SPITALUL PUBLIC: LOC ŞI PROVOVĂRI MAJORE ÎN
CONTEXTUL REFORMEI SISTEMULUI ÎNGRIJIRILOR DE
SĂNĂTATE.............................................................................
51
2.1. Evoluţii ale structurilor de îngrijiri spitaliceşti în Europa şi activitatea lor………... 52
2.1.1. Contextul general care declanşează nevoia reformării sistemelor serviciilor
spitaliceşti în Uniunea Europeană…………………………………………...
52
2.1.2. Organizarea îngrijirilor primare şi orientarea spre spital……………………… 55
2.1.3. Tipologii ale spitalelor regăsite în ţările UE……………………………….... 56
2.1.4. Inovaţii organizaţionale……………………………………………………..... 57
2.2. Convergenţa reformei spitalelor din România cu tendinţele oferite de experienţele
ţărilor din Europa Occidentală……………………………………………………………. 63
2.2.1. Noi structure instituţionale care susţin reforma spitalelor din România…….. 64
2.2.2. Reformarea reţelei spitaliceşti, miză majoră pentru sistemul de sănătate
din România………………………………………………………………………
65
2.3. Indicatorii privind resursele şi activitatea spitalelor publice
din România……………....................................................................................................
70
2.3.1. Resursele……………………………………………………………………… 70
2.3.2. Indicatori de activitate (rezultate)……………………………………………... 76
2.4. Performanţa sistemului de sănătate din România…………………………………… 77
2.5. Principalele elemente definitorii ale stării de sănătate a populaţiei din România…….. 81
Concluziile capitolului …………………………………………......................…………. 86
CAPITOLUL 3. PERFORMANŢA SERVICIILOR DE SĂNĂTATE: ABORDĂRI
TEORETICE ŞI PRACTICE ……………………………………….
87
3.1. Performanţa organizaţională: concept multidimensional……………………………. 88
3.2. Performanţa sistemelor serviciilor de sănătate: cadre de definire…………………… 94
3.3. Principalele cadre de evaluare a performanţeisistemelor de servicii de sănătate……. 103
3.3.1. Cadrul de evaluare a performanţeisistemelor de sănătateelaborat de OMS…. 103
3.3.2.Cadrul de evaluare a performanţei spitalelor elaborat de Biroul
regional european al OMS………………………………………………………...
105
3.3.3. Cadrul de evaluare a calităţii serviciilor de sănătate promovat de OECD…… 107
3.3.4. Cadrele conceptuale de măsurare a performanţelor sistemelor serviciilor
de sănătate în unele ţări cu rezultate notabile……………………………………
112
3.3.4.1. Marea Britanie……………………………………………………… 112
3.3.4.2. Statele Unite ale Americii………………………………………………. 113
3.3.4.3. Canada………………………………………………………………….. 115
3.3.4.4. Noua Zeelandă………………………………………………………….. 116
3.3.4.5. Australia………………………………………………………………… 117
Concluziile capitolului ……………..................……………………………………………. 118
CAPITOLUL 4. GESTIUNEA RESURSELOR UMANE: MIZĂ MAJORĂ PENTRU
PERFORMANȚA SPITALULUI PUBLIC…………………………... 119
4.1. Specificitatea serviciilor spitaliceşti……………………………………………………. 119
4.2. Spitalul public: organizaţie complexă cu o structură divizată şi partajată…………… 120
4.3. Gestiunea strategică a resurselor umane: definire ……………………………………. 123
4.4. Evoluţia conceptelor care operează în domeniul gestiunii resurselor umane
din perspectivă epistemologică…………………………………………………………...
128
4.5. Guvernanţa: un nou spaţiu de control colectiv al activităţilor spitaliceşti……………. 131
Concluziile capitolului ……………………………………………………………........... 135
CAPITOLUL 5. DIMENSIUNILE PERFORMANŢEI SPITALICEŞTI: O
ANCHETĂ ÎN RÂNDUL DIVERŞILOR ACTORI DIN SPITALUL
JUDEŢEAN DE URGENŢĂ BUZĂU....................................................
137
5.1. Contextul teoretic în care se înscrie cercetarea de teren................................................ 137
5.2. Ancheta în rândul personalului Spitalului Judeţean de Urgenţă Buzău……………….. 143
5.2.1. Locul de realizare a anchetei…………………………………………………….. 143
5.2.2. Aspecte metodologice ale anchetei de opinie întreprinse………………………. 144
5.2.3. Rezultatele anchetei de opinie…………………………………………………… 147
5.2.3.1. Caracteristicile eşantionului…………………………………………….. 147
5.2.3.2. Concluzii desprinse din prelucrarea chestionarului…………………….. 148
Concluziile capitolului ………………………………………….......................................... 166
Capitolul 6. GUVERNANŢA CLINICĂ: UN GHID DE BUNE PRACTICI PENTRU
OBŢINEREA PERFORMANŢEI SERVICIILOR DE ÎNGRIJIRI DE
SĂNĂTATE ÎNTR-UN SPITAL PUBLIC..................................................
167
6.1. Provocări ale sistemelor naţionale de sănătate în Statele membre
ale Regiunii europene a OMS…………………………………………………....................
167
6.2.Noi concepe în cadrul managementului spitalelor: deconcentrarea de gestiune
și contractualizarea internă prin crearea polilor de activitate…………………………….......
175
6.3. Elemente definitorii pentru fundamentarea unui demers de trecere
la o guvernanță clinică...............................................................................................
181
6.4. Repere metodologice și practice de abordare a unei noi guvernanțe a spitalului.
Un ghid metodologic…………………………………………………………………........... 186
6.4.1. Prima etapă: Diagnosticul strategic……………………………………………… 187
6.4.2. A doua etapă: Proiectarea demersului de trecere la o nouă guvernanță
a spitalului…………………………………………………………………….................
189
6.4.3. A treia etapă: Implementarea proiectului de trecere la o nouă guvernanță
a spitalului……………………………………………………………………...............
192
Concluziile capitolului ………………………………………………………....................... 195
CONCLUZII GENERALE.................................................................................................. 196
COTRIBUŢIILE ŞTIINŢIFICE .....................................................................................
LIMITELE CERCETĂRII.............................................................................................
PERSPECTIVELE CERCETĂRII..................................................................................
BIBLIOGRAFIE……………………………………………………………………………..
201
202
202
204
ANEXE...................................................................................................................... 222

CUVINTE CHEIE
• Gestiunea resurselor umane
• Gestiunea strategica a resurselor umane
• Guvernanta clinica
• Determinantii sanatatii populatiei
• Economia sanatatii sistemul serviciilor de sanatate
IMPORTANŢA, ACTUALITATEA ŞI NOUTATEA TEMEI
Sănătatea individului reprezintă inevitabil un factor decisiv al dezvoltării socio-
economice a unei țări. Strategiile din domeniul sănătății acoperă unul dintre spațiile de
expresie a calității vieții și a demnității umane, în același timp ca un loc unde se regenerează,
se perpetuează și se reproduce forța de muncă a omului.
Drept consecință a acestui postulat, devine necesară crearea unui sistem național de
sănătate pregătit să satisfacă global nevoile populației. Acest lucru se transpune în practică
printr-un pachet de pârghii care să faciliteze integrarea activităților de îngrijiri preventive și
curative, sectorizarea în intervenții și ierarhizarea îngrijirilor în scopul eficacității și
raționalizării procesului de gestionare a infrastructurii destinată promovării sănătății.
Infrastructura pentru promovarea sănătății cuprinde nu numai resursele umane și
materiale regăsite sub forma structurilor organizaționale și administrative, dar în egală măsură
și structurile de sensibilizare publică și politică la problemele de sănătate și participare la
măsurile vizând rezolvarea acestor probleme.
În cadrul acestei infrastructuri, spitalul public este chemat să joace un rol amplu
care îi conferă poziția de actor principal pentru a răspunde aspirațiilor cetățenilor în
termeni de calitate, transparență, exigență. În fața acestor provocări, managementul
spitalelor are nevoie de un mare efort de modernizare, centrat în prioritate pe una dintre
principalele axe ale sale, și anume resursele umane. Într-adevăr, importanța resurselor
umane ca pârghie de succes al organizațiilor nu mai este de demonstrat. Resursele umane
sunt motorul oricărei organizații și pot să impulsioneze dinamica schimbării și să fie
vectorul de performanțe considerabile. În fapt, performanța managementului resurselor
umane este considerată ca unul din factorii cheie de succes și de dinamizare a schimbării în
favoarea creării valorii pentru întreaga organizație.
În acest context tematic, se integrează cercetarea noastră care se interesează de
conceptul nou al gestiunii resurselor umane pentru domeniul spitalului public în cadrul
sistemului național de sănătate românesc.
Studiul nostru are ca scop general ameliorarea cunoștințelor privind gestiunea
eficace a resurselor umane prin aplicarea adecvată de practici care să permită unui
spital public de a fi mai performant în mediul său aflat sub presiunea schimbărilor
cotidiene. Într-un climat de competitivitate, gestiunea resurselor umane este elementul
fundamental al ecuației strategice.
PROBLEMATICĂ ȘI IPOTEZE
Serviciile spitalicești trebuie să răspundă exigențelor crescute de calitate și de
ameliorare a prestațiilor lor. Bolnavul, client și consumator de îngrijiri, are așteptări precise în
materie de calitate a îngrijirilor, de primire și de informare. Pentru a răspunde acestor cereri,
spitalul public trebuie să se reformeze pe baza unei strategii de ieșire din criză care să
urmărească progrese de ameliorare a evoluțiilor sale pe mai multe niveluri:
- la nivelul organizării interne și a metodelor de muncă;
- la nivelul sistemelor de gestiune, cu o atenție deosebită acordată gestiunii
resurselor umane.
Teza noastră de doctorat este focalizată pe componenta majoră a sistemului de
îngrijiri de sănătate: cea reprezentată de veriga serviciilor de sănătate terțiare – spitalul
public. Problemele științifice la care s-a căutat săse găsească răspunsuri prin demersul
întreprins sunt:
- Cum este percepută performanța activității spitalicești de către personalul
medical?
- Care sunt factorii ce permit personalului medical dintr-un spital să acționeze de
manieră adecvată față de nevoile pacienților săi?
Găsirea răsunsurilor la aceste două probleme științifice se fondează pe trei
ipoteze ce le vom avea în vedere în demersul nostru științific, și anume:
1. Criza financiară a spitalelor publice, în contextul general al deficitului bugetar
cu care se confruntă sistemul național de sănătate românesc, nu este decât una
din formele aparente ale unei crize profunde a modelului spitalicesc tradițional
la nivel structural: în misiunile sale și la nivelul personalului său.
2. Criza personalului spitalicesc dinamizează criza la nivelul spitalelor publice și
punctul de ieșire din criză nu poate să fie găsit doar în modificarea gestiunii
financiare, ci și în modificarea sistemului de management al resurselor umane.
3. Sectorul stabilimentelor spitalicești este un teren favorabil dezvoltării
structurilor de rețea, de exemplu prin crearea polilor de activitate care urmează
să integreze servicii compatibile.
Aceste ipoteze se integrează logic într-o problematică generală sprijinindu-se pe
demonstrația că gestiunea resurselor umane stă în centrul procesului de schimbare și de
modernizare a spitalului public.
POZIȚIONAREA EPISTEMOLOGICĂ A TEZEI DE DOCTORAT
Tema tezei de doctorat se circumscrie, din punct de vedere epistemologic, în sfera
de acoperire a disciplinei managementul resurselor umane. Câmpul științific al
managementului resurselor umane în cadrul spitalului – organizație complexă, cu o structură
organizațională particulară – este larg, transversal, fiind compus din sub-câmpuri
(servicii/poluri de activitate) care se autonomizează.
• Cercetarea științifică care stă la fundamentul tezei noastre de doctorat este
deopotrivă o cercetare :
- exploratorie, în sensul că s-a bazat pe o documentare focusată atât pe confirmarea
unor ipoteze, cât și pe descoperirea de noi tendințe / concepte;
- pozitivă, în măsura în care se formulează o serie de recomandări (Capitolul 6) pentru
a legitima înțelegerea de către practicieni a paradigmelor care stau la baza guvernanței
clinice;
- ipotetico-educativă, bazată pe formularea de ipoteze deduse din teorii validate de
practică și, apoi, făcute generalizări.
• Tipul de cercetare a informațiilor: s-au folosit informații și date din surse publice
(MS, EUROSTAT, OECD, OMS etc), precum și din materialele publicate pe internet,
realizate de către cercetători universitari de notorietate în lumea științifică.
STRUCTURA TEZEI DE DOCTORAT
Teza de doctorat este structurată în șase capitole, la care se adaugă introducerea și o
secțiune finală de concluzii generale și contribuții personale.

Capitolul 1 -,,Serviciile de sănătate: termeni, concepte și abodări teoretice” – a
fost elaborat având ca surse de referință documentară în principal studii și publicații
întreprinse pe plan international, cu un grad ridicat de vizibilitate în mediul științific și
academic, care au constituit fundamentul epistemologic al domeniului investigat. În esență,
acest capitol are scopul de a defini domeniul în care se înscrie obiectul cercetării în cazul
tezei noastre de doctorat – spitalulpublic.Pentru aceasta, primul capitol al tezei noastre de
doctorat abordează conceptele-cheie care definesc un sistem al serviciilorde sănătate,
componentele sale şi legăturile pe care le are cu ansamblul sistemului de sănătate. Astfel, a
fost abordat cadrul teoretic al conceptelor care definesc continutul complex si intgrator al
serviciilor de sanatate: determinantii sociali ai sanatatii; economia sanatatii – fundament
teoretic al pietei serviciilor de sanatate; sistemul de sanatate si sistemul serviciilor de sanatate,
acesta din urma fiind tratat ca un sistem organizat de actiune.
Sistemul serviciilor de sănătate în calitate de sistem organizat de acţiune, având el
însuşi subsisteme organizate de acţiune, nu-şi poate asuma marile funcţii pe care trebuie să
le îndeplinească fără integrarea serviciilor de sănătate, aceasta fiind soluţia potenţială
pentru a contracara eventualele disfuncţionalităţi ce apar atunci când elementele constitutive
ale sistemului acţionează independent unele de altele.
În esenţă, integrarea este procesul care constă în a creea şi a menţine, de-a lungul
timpului, o conducere comună între actori (şi organizaţii) autonomie în scopul de a
coordona interdependenţele lor pentru a permite cooperarea la realizarea unui proiect colectiv.
În domeniul economic, integrarea nu are o conotaţie sistemică, ea urmărind realizarea de
creşteri de productivitate sau de economii de scară. În primul rând, o întreprindere economică
are în vedere o integrare a ciclurilor sale de producţie prin coordonarea cu o serie de activităţi
care se situează în amont sau în aval de activităţile sale proprii (altfel zis, în exteriorul
întreprinderii în cauză). Se vorbeşte în acest caz de integrare verticală. Când este o situaţie de
întreprinderi similare care se grupează, între altele pentru a atinge economii de scară, are loc o
integrare orizontală.
Dimensiunile integrării serviciilor de sănătate vizeazăstabilirea unei coerenţe
între sistemul clinic (constituit din modalităţile de preluare în grijă a pacienţilor şi din
regulile de bune practici, asigurându-se o integrare optimală a îngrijirilor în timp, în spaţiu şi
între cadrele medicale), conducerea (formată dintr-un sistem de gestiune, un sistem de
finanţare şi de un sistem de informaţie) şi sistemul colectiv de interpretări şi de valori
(ansamblul de credinţe, de valori, de scheme interpretative care permit actorilor să comunice
între ei, să-şi coordoneze acţiunile lor şi să coopereze), care structurează spaţiul în care actorii
(organizaţii) interacţionează. Diferitele forme pe care le poate lua procesul de integrare
vizează, în grade diferite, instituţionalizarea relaţiilor de cooperare între toţi actorii
implicaţi în situaţia de interdependenţă în raport cu unul sau mai multe proiecte
comune. Cele cinci dimensiuni ale procesului de integrare trebuie puse în practică de
manieră durabilă în timp: (1) integrarea îngrijirilor; (2) integrarea echipei clinice (integrare
medicală); (3) integrare funcţională; (4) integrare normativă; (5) integrare sistemică.
Capitolul 2 - ,,Spitalul public: loc și provocări majore în contextual reformei
sistemului îngrijirilor de sănătate”– are ca ținte analiza și evaluarea procesului de
reformare a spitalelor din România din perspectiva convergenței acestuia cu tendinețele
de dezvoltare a serviciilor spitalicești manifestate în țări membre ale UE. Acest capitol se
fondează pe analiza unor rapoarte ale două organisme internaționale, OECD și Observatorul
European privind politicile și sistemele de sănătate ale OMS Europa, completate de două
studii referitoare la evaluarea reformei sistemului de sănătate în România, precum și printr-o
analiză a literaturii de specialitate în domeniul sănătății.
Starea spitalelor din România este departe de a putea răspunde cerinţelor de
asigurare a calităţii serviciilor medicale ale populaţiei la standardele europene de înalt
nivel. Sectorul sanitar se bazează pe o infrastructură concepută acum 50-60 de ani, când
nevoia de servicii era diferită faţă de realităţile de astăzi. Existenţa încă a clădirilor vechi
(unele de peste 100 de ani vechime) ale căror soluţii constructive nu permit integrarea
optimală a circuitelor intraspitaliceşti ridică dificultăţi majore în modernizarea funcţionării
spitalelor cu repercusiuni asupra siguranţei pacientului şi a unor cheltuieli evitabile
Eşecurile înregistrate până acum în strategiile de reformă a sistemului de sănătate
românesc impun cu stringenţă un cadru strategic pentru regândirea acestuia. Sunt de reţinut
direcţiile de reformă a sistemului de sănătate formulate în două documente cheie: Strategia
naţională pentru sănătate 2014-2020 şi Planul multi-anual pentru dezvoltarea strategică a
resurselor umane ale sănătăţii 2017-2020. În acest stadiu, niciunul din cele două documente
nu este operaţional, planurile de aplicare în practică fiind încă aşteptate.
Ministerul Sănătăţii a identificat spitalele care fac parte din reţeaua strategică în
care se vor concentra investiţiile necesare de infrastructură, conform viziunii Strategiei
naţionale pentru sănătate 2014-2020. Apreciem ca fiind oportune şi necesare direcţiile de
acţiune înscrise în acest documentP90FP:
- transformarea spitalelor locale, din oraşele mici şi medii, în unităţi care furnizează
servicii în regim ambulatoriu, spitalizare de zi sau servicii pentru îngrijirea pacienţilor
cronici, inclusiv cu contribuţia autorităţilor locale;
- dezvoltarea şi raţionalizarea spitalelor judeţene;
- dezvoltarea şi raţionalizarea spitalelor de nivel regional şi naţional – procesul va
include reducerea numărului de clădiri, pavilioane și spitale monoprofil și integrarea
acestora în clădiri noi sau reabilitate şi modernizate în cadrul spitalelor regionale;
- modernizarea şi dotarea unităţilor sanitare ce vor îndeplini rolul de spitale regionale de
urgenţă;
- construirea a trei spitale regionale de urgenţă: Iaşi, Cluj Napoca, Craiova;
- aducerea la standarde moderne de funcţionare a infrastructurii serviciilor de
radioterapie şi oncologie.
Capitolul 3 -,,Performanța serviciilor de sănătate: abordări teoretice și
practice”sintetizează conceptele teoretice, dezvoltate în timp, care definesc performanța
organizațiilor din domeniul sănătății și au fost validate în practica multor țări care a confirmat
faptul că promovarea și ameliorarea sănătății populației reprezintă obiectivul major (prioritar)
al unui sistem de sănătate, însă analiza performanței sistemelor de sănătate nu se limitează
doar la această dimensiune. Sunt evidențiate, în paginile capitolului, și alte dimensiuni ce
definesc nivelul de performanță a unui sistem de sănătate:
- ameliorarea stării de sănătate atribuită sistemului de îngrijire a sănătății;
- calitatea îngrijirilor;
- capacitatea sistemului de sănătate de a răspunde așteptărilor populației;
- echitatea în accesul la îngrijiri;
- eficiența productivă (productivitatea).
Capitolul 4: - ,,Gestiunea resurselor umane: miză majoră pentru performanța
spitalului public”– reprezintă o sinteză a abordărilor teoretice, desprinse din trecerea în
revistă a surselor documentare de referință, privind dezvoltarea și repoziționarea resurselor
umane ca miză–cheie în reformarea spitalelor publice. Noile concepte de management al
resurselor umane - ,,gestiunea resurselor umane”, ,,gestiunea strategică a resurselor
umane” – sunt abordate în strânsă legătură cu specificitatea serviciilor spitalicești dată de
particularitatea spitalului public ca organizație complexă cu o structură divizată și partajată.
Această divizare organizaţională a spitalului public este generată de repartizarea
puterii în cadrul său. Este vorba de o putere bicefală, existând, pe de o parte, puterea
administrativă, reprezentată de directorul/managerul spitalului şi de care personalul
(exceptând medicii) depinde, directorul fiind garant al condiţiilor de muncă. Pe de altă parte,
puterea medicală care gestionează organizarea muncii personalului implicit legat de
prestarea serviciilor de sănătate. Acestor două entităţi le corespund două structuri de
gestiune: consiliul de administraţie, care determină proiectul de spital, şi comisia medicală
a spitalului (CMS), incluzând medicii, având în sarcină şi stabilirea proiectului medical.
Guvernanţa: un nou spaţiu de control colectiv al activităţilor spitaliceşti
În domeniul sănătăţii, emergenţa conceptului de guvernanţă a unităţilor sanitare
este susţinută de trei argumente solide:
În primul rând, opţiunile legate de prestarea serviciilor de sănătate a căror
coordonare trebuie asigurată acoperă perimetrul de responsabilitate care excede pe cel
al organizaţiilor existente, guvernanţa obligând la o abordare a unui nou spaţiu de
organizare şi control colective.
Acţiunile cărora trebuie să li se asigure coordonarea şi de care trebuie să se ţină seama
au dimensiuni inter-organizaţionale şi interprofesionale care nu se reduc la însumarea
acţiunilor fiecărei organizaţii sau a fiecărui cadru profesional. Guvernanţa obligă la a reflecta
la coordonarea actorilor şi a organizaţiilor care sunt simultan autonome şi interdependente
pentru a asigura un acces echitabil la îngrijiri de sănătate de calitate a unei populaţii definită şi
pentru a contribui la politicile intersectoriale de sănătate.
În prestarea serviciilor de sănătate există patru mari grupe de actori care
interacţionează, fiecare dintre ele având propria lor contribuţie despre logica care ar trebui să
le ghideze deciziile:
1. cadrele medicale (medici, infirmiere, farmacişti, stomatologi ...) care valorizează
logica profesională;
2. gestionării (finanţatori, evaluatori, funcţionari ...) care îşi fondează deciziile pe logica
tehnocratică, pe raţionalitatea formală;
3. lumea comercială (societăţii farmaceutice, de asigurare, grupuri financiare implicate
în oferta de îngrijiri de sănătate ...) şi
4. lumea politică (aleşii, reprezentanţii legitimi de grupuri constituite ...) care revendică
superioritatea logicii democratice.
Guvernanțapoate fi definită ca fiind concepția, conducerea și evaluarea acțiunii
colective pornind de la o poziție de autoritate. Ea se sprijină pe:
1. un sistem de gestiune: ansamblul regulilor care definesc modalitățile de distribuție a
puterii și a responsabilităților;
2. un sistem informațional ansamblul datelor și sistemul lor de exploatare necesar
pentru ca sistemul organizat de acțiune să fie inteligibil și transparent în orice moment
pentru personalul medical, gestionari, planificatori, pacienți și populație;
3. un sistem de finanțare: ansamblul stimulărilor vehiculate prin modalitățile de
finanțare ale sistemului, mecanismele de alocare a bugetelor și mecanismelor de plată
ale actorilor.
Capitolul 5 -,,Dimensiunile performanței spitalicești: o anchetă în rândul
diverșilor actori din Spitalul Județean de Urgență Buzău” - prezintă rezultatele unei
anchete realizată în rândul personalului dintr-un spital județean de urgență (Buzău). Această
anchetă a permis o analiză calitativă, pe baza unui model teoretic al performanței dezvoltat de
către Sicotte și colabP1F
1P. Ancheta a avut două obiective. În primul rând, s-a urmărit cunoașterea
conceptului de performanță pe care o au diverșii actori din cadrul spitalului. În al doilea rând,
pornind de la opinia diferitelor categorii de actori - în funcție de grupa profesională de
apartenență – s-a căutat a se determina eventualele arii de consens sau de divergență. Punerea
în evidență a acestor arii de consens sau de divergență este importantă pentru că un spital nu
poate să fie performant decât dacă actorii săi își unesc forțele pentru a atinge o serie de
obiective comune.
În contextul schemei conceptuale de proiectare a cercetării de teren (punctul 1.), s-a
urmărit obţinerea unor informaţii pertinente (confirmarea ipotezelor modelului integrator al
performanţei organizaţionale de către Sicotte şi colab.) pentru fundamentarea în capitolul al
şaselea al tezei de doctorat a unor recomandări formulate generic sub titlul de„Ghid de bune
practici pentru obţinerea performanţei serviciilor de îngrijiri de sănătate într-un spital
public”.
• Obiectivul central al sondajului de opinie îl constituie explorarea (sondajul fiind
un studiu exploratoriu descriptiv) concepţiilor (percepţiilor) principalilor actori
decizionali ai Spitalului Judeţean de Urgenţă Buzău despre performanţa
serviciilor spitaliceşti şi, apoi, propunerea de pârghii şi instrumente de sprijin al
pilotajului activităţii. Acest tip de studiu (cercetare de teren) este o tehnică adecvată
pentru a explora ceea ce constituie reprezentările performanţei vehiculate în
discursurile actorilor şi pentru a căuta dacă există diferenţe sau similitudini la nivelul
concepţiilor diferitelor categorii de actori, în funcţie de particularităţile lor socio-
profesionale.
• În interpretarea sondajului se au în vedere următoarele ipoteze:
1SICOTTE C., CHAMPAGNE F., CONTANDRIOPOULOS A. C., BARNSELJ J et al (1998), A conceptual
framework for analysis of health care organisations performance, Health Services Management research, 1998,
no 11, pp. 24-48.

- Ipoteza centrală a cercetării noastre are în vedere că performanţa spitalului nu
poate să fie căutată decât într-o viziune partajată a diferitilor actori cu legături directe
în activitatea spitalului: direcţii judeţene de sănătate, reprezentanţii Statului şi ai
Asigurărilor de Sănătate, sindicatele din domeniul sănătăţii, ansamblul cadrelor medicale şi
pacienţii.
- A doua ipoteză presupune că Spitalul nu poate să amelioreze performanţa sa
atâta timp cât rămâne administrat şi nu gestionat. Această performanţă necesită
angajamentul unui proces de gestiune (guvernanţa) finalizat prin căutarea unei viziuni
partajate a actorilor vizaţi la nivel local şi regional.
Capitolul 6 - ,,Guvernanța clinică: un ghid de bune practici pentru obținerea
performanței serviciilor de sănătate”– are ca tematică generală conceptul nou de
guvernanță clinică care se fondează pe recunoașterea unei interdependențe între practicile
clinice și contextul organizațional în care personalul medical prestează activitatea. În acest
capitol, valorificând o serie de surse documentare de referință, am dezvoltat un demers cu
valențe practice deosebite care oferă pașii de urmat pentru pilotarea de ansamblu a spitalului
(guvernanța de ansamblu) și structurarea muncii actorilor din zona operațională (guvernanța
de proximitate). În esență, capitolul oferă un model managerial care se fondează pe un
leadership partajat conducere/medic, prin căutarea sinergiei între conducere
(stewardship) și corpul medical, cu ținta finală echilibrul guvernanței între direcția
generală și comunitatea medicală. Și totul pornind de la postulatul potrivit căruia spitalul
este o ,,administrație particulară care trebuie să tindă spre o ,,guvernanță adaptată”.
In cursul acestui capitol, intr-o prima sectiune, au fost abordate doua noi concepe
în cadrul managementuluispitalelor: deconcentrarea de gestiune și contractualizarea
internă prin crearea polilor de activitate
Contractualizarea este un răspuns la complexitatea organizației medicale
(spitalul), recunoscându-se un nivel de analiză și de decizie mai descentralizată.
Deconcentrarea de gestiune și contractualizarea sunt factori cheie de reușită în
gestiunea resurselor umane în cadrul spitalului pentru că ele conduc la introducerea unui
management animat de o voință de implicare și de angajament reciproc.
O gestiune deconcentrată pune în discuție organizația ierarhică actuală și structurarea
serviciilor de îngrijiri. Această structurare cere:
✓ trecerea de la o logică de statut, bazată pe o ierarhie piramidală, la o logică de contract
bazată pe competența actorilor și rezultatele lor;
✓ un plus de transversalitate atât în cadrul polului de activitate, cât și între poli.
Constituirea de poli de activitate vizează în mod normal ameliorarea organizării
spitalelor, în special grație punerii în comun a competențelor și a mijloacelor care
permit ajustarea permanentă a resurselor la nevoile pacienților. Acești poli nu
înlocuiesc serviciile. Formează o nouă structură ,,strat” suplimentară în organizarea
spitalelor.
Crearea polilor de activitate se fondează pe patru elemente:
▪ Deconcentrare a gestiunii: sarcinile asumate până acum de către direcția
stabilimentului sunt efectuate de polii clinici și medico-tehnici. În fapt, se atribuie
coordonatorilor de pol o putere de decizie în vaste domenii (finanțe, cumpărare,
organizare a unităților de muncă etc.) sub rezerva respectării strategiei stabilimentului
și bugetului alocat.
▪ Un proiect de pol: elaborat de către responsabilul de pol care asociază în pregătirea
proiectului consiliul de pol. Este un document plurianual, cu un conținut medical și
organizațional, care definește activitatea actuală a polului și dezvoltările sale viitoare,
modalitățile de organizare internă.
▪ Un contract de pol: negociat între directorul centrului spitalicesc și președintele
comisiei medicale a stabilimentului, decanii facultăților de medicină și de farmacie, pe
de o parte, și coordonatorul polului, pe de altă parte, după avizul consiliului executiv;
contractul de pol definește obiectivele de activitate, de calitate și financiare, mijloacele
și indicatorii de urmărit ai polului, modalitățile de obținere de rezultate scontate și
consecințele în caz de neexecutare a contractului.
▪ Contracte inter-poluri
Gestiunea prin poli de activitate corespunde unei evoluții a managementului spitalelor,
deciziile trebuind să fie luate într-un mod colaborativ: polii sunt dirijați de un trio
constituit dintr-un medic, șef de pol, un cadru medical superior și un cadru
administrativ. Astfel, gestiunea polului oferă actorilor managementului spitalicesc
ocazia de a imita (a întrepătrunde) legături între medici, personalul infirmier,
personalul administrativ, forțând unii pe alții să muncească mai degrabă în echipă
decât separat.
Nucleul tematic al capitolului al saselea al tezei, regasit intr-o a doua sectiune, il
formeaza reperele metodologice și practice de abordare a unei noi guvernanțe a
spitaluluicare au constituit fundamentulghidului metodologic propus.

Demersul de punere în practică a noii guvernanțe a unui spital, dintr-o
perspectivă metodologică, se desfășoară în trei etape principale:
➢ Prima etapă: Diagnosticul strategic.Scopul diagnosticului strategic îl constituie
poziționarea spitalului în contextul teritoriului de sănătate și stabilirea mizelor ce
stau în fața lui. Concret, un diagnostic strategic urmărește:
• situarea spitalului într-un context sanitar, politic, social și economic, luând în seamă
oferta concurenței;
• în cadrul spitalului (mediul său intern), identificarea și evaluarea forțelor și
slăbiciunilor, oportunităților și amenințărilor (o analiză SWOT);
• reperarea, în mod obiectiv, a instrumentelor performante, a aporturilor lor, dar și a
limitelor lor;
• identificarea politicii de comunicare.
Un diagnostic strategic se fondează pe găsirea răspunsurilor la următoarele
întrebări:
• Care sunt datele obiective și obiectivabile privind spitalul: număr de paturi, personal,
buget, moduri de contact cu pacienții, activități medicale etc?
• Care este politica sistemului informațional: instrumente de culegere de informații
instituționale, proceduri de gestiune documentare, evaluarea eficienței instrumentelor
de către actori?
• Care sunt indicatorii de resurse, de activități, de rezultate?
• Cum sunt lisibilitatea și coerența datelor culese?
➢ A doua etapă: Proiectarea demersului de trecere la o nouă guvernanță a
spitalului
Această a două etapă trebuie să permită managementului spitalului:
să reflecteze asupra configurației structurilor și să definiească organizarea viitoare;
să găsească logica proprie de conducere a proiectului ce trebuie elaborat.
➢ A treia etapă: Implementarea proiectului de trecerela o nouă guvernanță a
spitalului
În această a treia etapă, se vor concretiza configurația noilor structure și premisele
bunei lor funcționări. Ea trebuie să conducă, prin coordonarea ansamblului actorilor,
la atingerea obiectivelor propuse în a doua etapă. Rolul guvernanței de proximitate
este fundamental pentru poziționarea cadrelor medicale în înterfață cu diferitele logici
decizionale conturate la nivelul guvernanței de ansamblu a spitalului.
Implementarea proiectului de trecere la o nouă guvernanță a spitalului reclama
trei raspunderi delimitate clar:
• Cultura organizațională potrivită. Pentru implementare este nevoie de culturi care
valorizează realizările, disciplina și simțul muncii în echipe pluridisciplinare și/sau
transdisciplinare.
• Leadershipul. Este motorul care propulsează organizația, care trebuie să incite la
acțiuni (practici) care fac o strategie să funcționeze.
• Mecanismele de control, feedback și adaptare. Procesele de implementare a
strategiei susțin schimbarea și adaptarea spitalului. Pentru ca strategia să funcționeze
este nevoie de feedback privind performanța.
Implementarea noii guvernanțe clinice se va traduce prin schimbări structurale,
organizaționale și culturale.
Reperele propuse în acest capitol constituie, pentru actorii implicați, firul conducător
al unui demers care pune în evidență întrebările–problemă ce se pun. Se regăsesc în
propunerile noastre pistele de reflecție asupra practicilor care vor putea să se sprijine –
cu efect sinergetic – pentru reușita implementării proiectului vizat.
Guvernanța clinică constituie o abordare strategică și managerială în care factorul
uman este fundamentul esențial și miza majoră în reușita acestei reforme dorite. Ea
deschide perspectivele unui pilotaj, colectiv și partajat, favorizând, astfel, o calitate de
ascultare reciprocă, o coeziune în demersul unei abordări medicale, de îngrijire,
administrată și tehnică.
CONCLUZII GENERALE
Reforma spitalelor are nevoie de susţinerea unei gestiuni puternice a resurselor
umane. Iar implicarea Direcţiei a resurselor umane va fi amplificată, aceasta fiind chemată să
participe la proiectarea strategiei organizaţionale ( a spitalului).
Problematica de modernizare a politicii resurselor umane în stabilimentele
publice de sănătate se înscrie într-un context general aflat în evoluţie, caracterizat
printr-o serie de provocăriP237F
2P:
2 TOUPILLIER Danielle et ZAHIEL M. (2011), Rapport sur la modernisation de la politique des resources
humaines dans les etablissements publics de santé, Centre National de Gestion des Practiciens Hospitaliers et
des Personnels de Direction de la Fonction Publique Hospitalière, Ministère du travail de l’emploi et de la santé,
p. 3.

• a răspunde aşteptărilor noi ale pacienţilor legate de transformarea societăţii;
• a respecta pacienţii în sistemul de sănătate;
• a lua în seamă fenomenul de îmbătrânire a populaţiei;
• a observa şi a anticipa problemele legate de sănătatea publică;
• a integra dezvoltarea de patologii cronice şi de polipatologii;
• a se adapta la evoluţiile ştiinţifice şi tehnologice;
• a dezvolta cercetarea şi inovarea.
În aceste condiţii, sistemul spitalicesc trebuie, în acelaşi timp, să acţioneze cu
fermitate în spiritul politicii angajate, să adapteze organizarea serviciilor de îngrijire astfel
încât să atingă indicatorii de performanţă şi de securizare a pacienţilor, să asigure un mediu de
muncă activ pentru ansamblul corpului medical.
Astfel, modernizarea gestiunii resurselor umane a spitalelor decurge din două
imperativeP238F
3P:
➢ a răspunde provocărilor mai sus menţionate;
➢ a lua în seamă şi a susţine mai bine o serie de reforme şi de schimbări probabil fără
precedent, a căror reuşită este condiţionată de mobilizarea tuturor categoriilor de
personal implicate.
Capacitatea spitalelor de a oferi îngrijiri de sănătate de calitate tuturor pacienţilor se
fondează, înainte de toate, pe competenţă, muncă şi angajament. Evoluţiile majore care au
afectat funcţionarea spitalelor în aceste ultime două decenii fac necesară reînnoirea abordării
gestiunii resurselor umane. În particular, trei mize principale sunt de relevatP239F
4P:
1. evoluţia spre o gestiune mai invidualizată a competenţelor şi a susţinerii
parcursurilor profesionale;
2. asigurarea, în permanenţă, a unei abordări între evoluţia constantă a nevoilor de
competenţe în cadrul fiecărui serviciu al spitalului şi competenţele efective
disponibile în alte spitale şi teritorii;
3. savoir faire-ul politicii de gestiune a resurselor umane, un element determinant al
strategiei şi performanţei spitalului, în ansamblul dimensiunilor sale, îndeosebi
calitatea, eficienţa internă şi performanţa economică.
Cu toată importanţa taliei personalului spitalicesc şi având în vedere rolul său central
pentru a impulsiona o reală dinamică a schimbării spre modernizarea guvernanței clinice,
situaţia actuală în spitalele din România denotă existenţa unei oarecare dileme. Într-
3Idem, pp. 3-4. 4Ibidem, p. 64.
adevăr, când spitalele suferă de o slabă eficacitate a resurselor umane şi a insuficienţelor
şi disfuncţionalităţilor pe care ele le prezintă, o slabă conştientizare şi implicare a
managementului sunt constante în cea mai mare parte a spitalelor.
Principalele slăbiciuni care împiedică punerea în practică a unei gestiuni a
resurselor umane performante se situează la următoarele niveluri:
➢ funcţia resurselor umane, ea însăşi, prin organizarea sa actuală, misiunea sa care
rămâne să fie definită în corelaţie cu mijloacele de care ea dispune;
➢ politica de gestiune a resurselor umane care nu este în totalitate definită şi care
rămâne departe de a pilota procesele specifice resurselor umane, precum gestiunea
previzională a locurilor de muncă şi a comptetenţelor, recrutarea, evaluarea
competenţelor şi formarea;
➢ suportul gestiunii resurselor umane prin modul de organizare, stilul de
management, comunicarea, dialogul social, motivarea şi condiţiile de muncă care
nu acţionează pentru toţi în sensul emergenţei unei gestiuni a resurselor umane
eficace.
Recomandările noastre au fost formulate ţinând seama atât de cadrul juridic şi
instituţional al spitalelor din România, cât şi de orientările OMS validate în practica ţărilor
UE, conturate ca tendinţe de promovat şi de către ţări, precum România, aflate încă în
dificultate din perspiectiva atingerii unor indicatori de performanţă a serviciilor de sănătate,
comparabili, competitivi, şi convergenţi cu nivelurile înregistrate de ţările cu sisteme
naţionale de sănătate dezvoltate.
Recomandările propuse în ultimul capitol al tezei noastre de doctorat se vor a fi,
în acelaşi timp, căi de progres, având misiunea de a facilita implementarea principiilor
noii guvernanţe clinice care nu poate fi detaşată de toate dimensiunile – instituţionale,
organizaţionale, tehnice, chiar politice – care traversează ,,viaţa” stabilimentelor spitaliceşti
(aceste dimensiuni/axe strategice sunt prezentate în tabelele 6.1 – 6.3 din ultimul capitol).
Fiecare din aceste recomandări constituie o orientare strategică pentru funcţia
resurselor umane care trebuie declinată, la nivelurile: de ansamblu (total spital),
servicii/departamente, poli de activitate, conform planului de modernizare definit.
Într-o succintă sinteză, am articulat aceste recomandări în jurul a trei serii de
nevoi de gestionare clinică, de natură transversală:
1. Căutare de ,,sens”, ceea ce o aseamănă cu dinamicile constatate în toate
întreprinderile complexe, publice şi private. Prin obiectivele stabilite s-a urmărit,
astfel:
- partajarea mizelor;
- asocierea echipelor;
- poziţionarea cadrelor medicale;
- clasificarea rolurilor pe o bază colaborativă;
- crearea polilor de activitate;
- adoptarea agendelor de lucru ale entităţilor funcţionale (CA, CMS, comisii
specializate) pentru a crea o cultură comună şi a se sprijini pe repere, instrumente şi
metode partajate.
2. Promovarea autonomiei prin:
- cooperare la toate eşaloanele spitalului (crearea unui spaţiu colaborativ organizat între
diferiţii intervenienţi în funcţia resurselor umane şi asigurarea unei delegări de
gestiune şi de putere);
- încurajarea demersului contractual şi partenerial la diferite eşaloane ale spitalului;
- intensificarea activităţii entităţilor funcţionale şi a relaţiei cu partenerii sociali;
- luarea în considerare a (răspuns la) nevoii autorităţilor guvernamentale (crearea unui
reţele profesionale pluridisciplinare în gestiunea resurselor umane).
3. Dotarea şi sprijinirea funcţiei resurselor umane, îndeosebi prin:
- favorizarea difuzăriide instrumente informatice de gestionare a resurselor umane într-o
strategie mai globală, facilitându-se comunicarea internă şi externă;
- dezvoltarea bazelor de date specifice sau în asociere cu alte organisme şi punerea în
practică a unui sistem informativ de întrebări – răspunsuri pentru a asigura fluiditatea
schimburilor de informaţii într-un intranet profesional.
Legat de comunicarea internă trebuie reţinut faptul că ea implică o schimbare –
în particular de practici şi de mentalităţi – care este un obiectiv dificil de atins fără un nou stil
de leadership al spitalului. În acest sens, DUPUY şi RAYNAUD P240F
5P disting, de exemplu, o
serie de principii de comunicare care pot să impulsioneze responsabilizarea şi
angajamentul personalului:
• Luciditatea: Ea constă în a înţelege contingenţa comunicării interne.
• Voinţa reală: Ea se traduce prin formalizarea funcţiei comunicare şi atribuirea
bugetului.
• Transparenţa: Ea se opune maniei secretului.
• Simplicitatea: Ea permite înţelegerea mesajului.
5DUPUY, E. RAYNAUD, I. (1988), La communication interne, vers l’entreprise transparente, Paris: Editions
d’Organisations, p. 52.
• Rapiditatea: Ea permite înlăturarea riscului de ,,rupere” de evenimentul subiect al
comunicării.
• Dezvoltarea comunicării: Trebuie să fie percepută ca o investiţie de durată.
• Adaptarea: Ea exprimă ideea că orice comunicare internă trebuie să se sprijine pe o
cultură de întreprindere şi nu trebuie redusă la o manieră uşoară importată (copiată).
Asta înseamnă că nu este neutră şi că vehiculează intenţii.
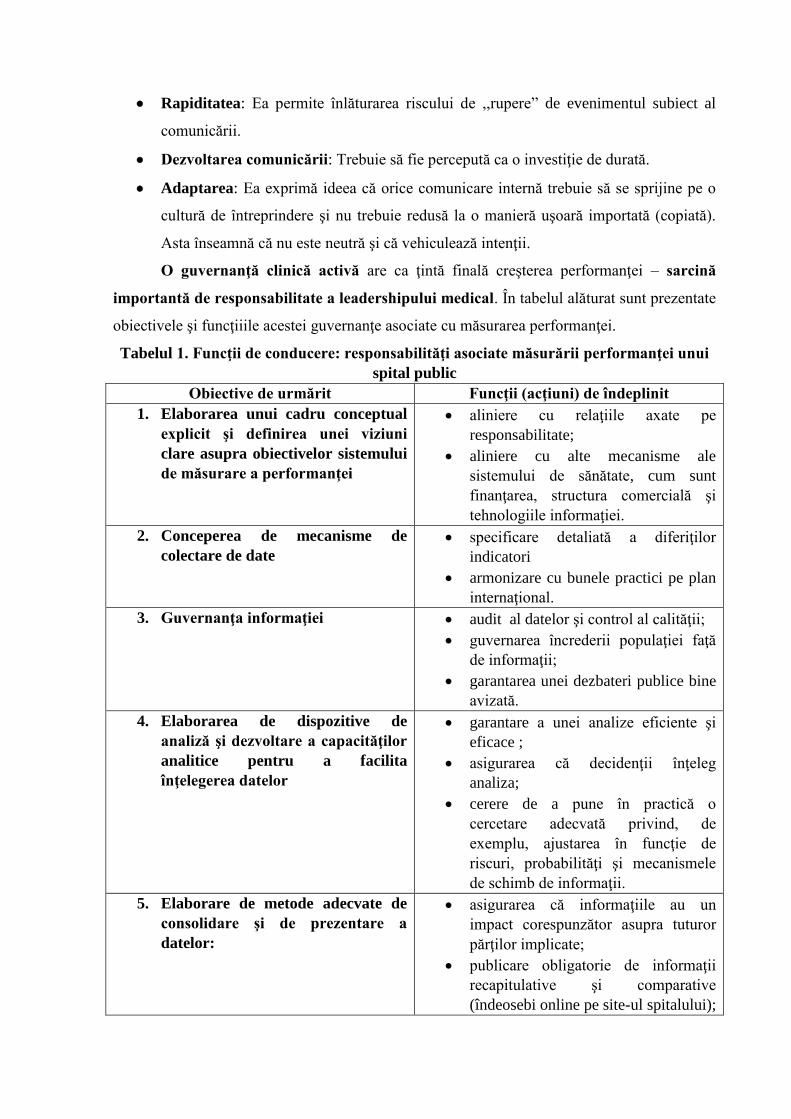
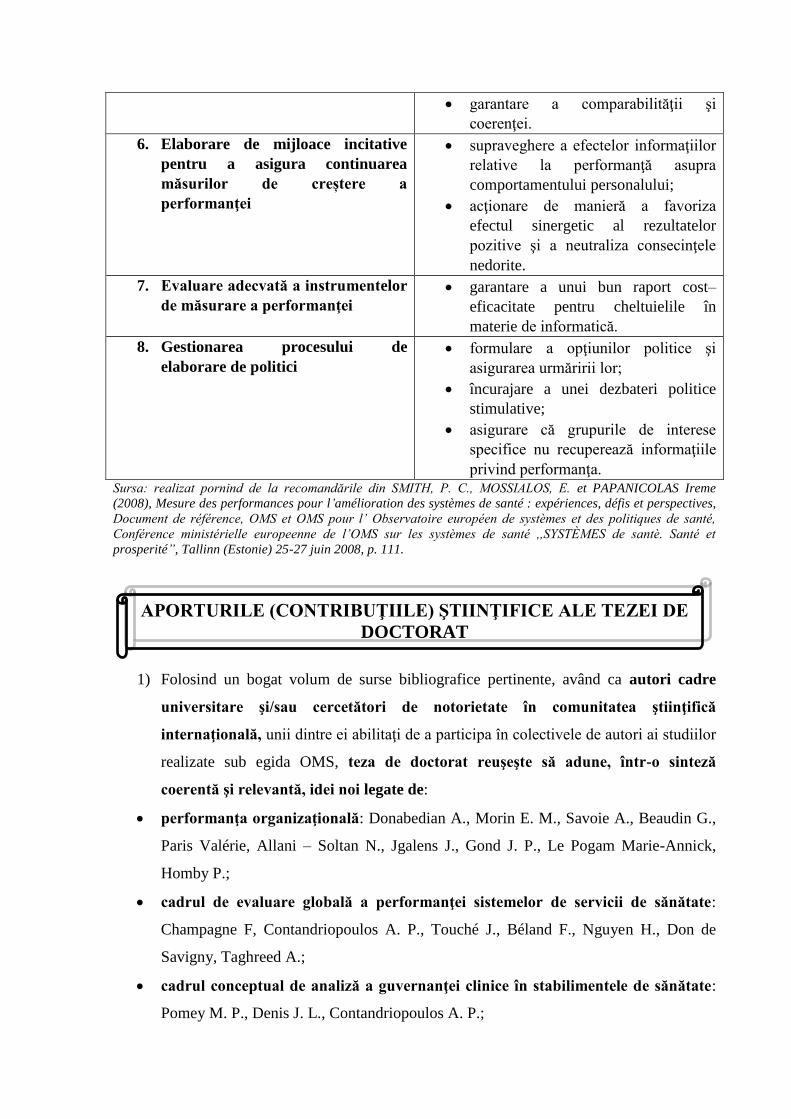
O guvernanţă clinică activă are ca ţintă finală creşterea performanţei – sarcină
importantă de responsabilitate a leadershipului medical. În tabelul alăturat sunt prezentate
obiectivele şi funcţiiile acestei guvernanţe asociate cu măsurarea performanţei.
Tabelul 1. Funcţii de conducere: responsabilităţi asociate măsurării performanţei unui
spital public
Obiective de urmărit Funcţii (acţiuni) de îndeplinit
1. Elaborarea unui cadru conceptual
explicit şi definirea unei viziuni
clare asupra obiectivelor sistemului
de măsurare a performanţei
• aliniere cu relaţiile axate pe
responsabilitate;
• aliniere cu alte mecanisme ale
sistemului de sănătate, cum sunt
finanţarea, structura comercială şi
tehnologiile informaţiei.
2. Conceperea de mecanisme de
colectare de date
• specificare detaliată a diferiţilor
indicatori
• armonizare cu bunele practici pe plan
internaţional.
3. Guvernanţa informaţiei • audit al datelor şi control al calităţii;
• guvernarea încrederii populaţiei faţă
de informaţii;
• garantarea unei dezbateri publice bine
avizată.
4. Elaborarea de dispozitive de
analiză şi dezvoltare a capacităţilor
analitice pentru a facilita
înţelegerea datelor
• garantare a unei analize eficiente şi
eficace ;
• asigurarea că decidenţii înţeleg
analiza;
• cerere de a pune în practică o
cercetare adecvată privind, de
exemplu, ajustarea în funcţie de
riscuri, probabilităţi şi mecanismele
de schimb de informaţii.
5. Elaborare de metode adecvate de
consolidare şi de prezentare a
datelor:
• asigurarea că informaţiile au un
impact corespunzător asupra tuturor
părţilor implicate;
• publicare obligatorie de informaţii
recapitulative şi comparative
(îndeosebi online pe site-ul spitalului);
• garantare a comparabilităţii şi
coerenţei.
6. Elaborare de mijloace incitative
pentru a asigura continuarea
măsurilor de creștere a
performanţei
• supraveghere a efectelor informaţiilor
relative la performanţă asupra
comportamentului personalului;
• acţionare de manieră a favoriza
efectul sinergetic al rezultatelor
pozitive şi a neutraliza consecinţele
nedorite.
7. Evaluare adecvată a instrumentelor
de măsurare a performanţei
• garantare a unui bun raport cost–
eficacitate pentru cheltuielile în
materie de informatică.
8. Gestionarea procesului de
elaborare de politici
• formulare a opţiunilor politice şi
asigurarea urmăririi lor;
• încurajare a unei dezbateri politice
stimulative;
• asigurare că grupurile de interese
specifice nu recuperează informaţiile
privind performanţa. Sursa: realizat pornind de la recomandările din SMITH, P. C., MOSSIALOS, E. et PAPANICOLAS Ireme
(2008), Mesure des performances pour l’amélioration des systèmes de santé : expériences, défis et perspectives,
Document de référence, OMS et OMS pour l’ Observatoire européen de systèmes et des politiques de santé,
Conférence ministérielle europeenne de l’OMS sur les systèmes de santé ,,SYSTÈMES de santè. Santé et
prosperité”, Tallinn (Estonie) 25-27 juin 2008, p. 111.
APORTURILE (CONTRIBUŢIILE) ŞTIINŢIFICE ALE TEZEI DE
DOCTORAT
1) Folosind un bogat volum de surse bibliografice pertinente, având ca autori cadre
universitare şi/sau cercetători de notorietate în comunitatea ştiinţifică
internaţională, unii dintre ei abilitaţi de a participa în colectivele de autori ai studiilor
realizate sub egida OMS, teza de doctorat reuşeşte să adune, într-o sinteză
coerentă şi relevantă, idei noi legate de:
• performanţa organizaţională: Donabedian A., Morin E. M., Savoie A., Beaudin G.,
Paris Valérie, Allani – Soltan N., Jgalens J., Gond J. P., Le Pogam Marie-Annick,
Homby P.;
• cadrul de evaluare globală a performanţei sistemelor de servicii de sănătate:
Champagne F, Contandriopoulos A. P., Touché J., Béland F., Nguyen H., Don de
Savigny, Taghreed A.;
• cadrul conceptual de analiză a guvernanţei clinice în stabilimentele de sănătate:
Pomey M. P., Denis J. L., Contandriopoulos A. P.;
• gestiunea resurselor umane: Vallejo J., Glouberman S., Minzberg H., Bareil Céline,
Guerin G., Wils Th, Storey J., Arcand M., Pigeyre F.
Evident că lista autorilor ce ar fi putut să fie citaţi este foarte extinsă, însă am ţinut să
menţionăm pe cei care, păstrând cerinţele epistemologiei, au definit de manieră originală
termeni şi concepte ale nucleelor paradigmatice circumscrise domeniilor de cercetare reţinute
în preocupările lor.
2) Al doilea aport ştiinţific adus prin teza noastră de doctorat este concretizat
înmaniera de tratare a domeniului investigat în primele patru capitole, care
permit cu uşurinţă cunoaşterea specificităţilor paradigmatice ale domeniului complex
investigat.
3) Al treilea aport al muncii noastre este demonstrat de construcţia persuasivă
acapitolului al şaselea care este focusat pe promovarea unei scheme –
cadru(Ghid)de funcţionare a unui program de modernizare a guvernanţei clinice.
Sistematizând, putem scoate în evidenţă valoarea contribuţiilor tezei noastre de
doctorat pe trei planuri:
• epistemologic: definirea conceptelor paradigmatice ale guvernanţei globale şi
guvernanţei de proximitate ale stabilimentelor clinice;
• operaţional: proiectarea cadrului metodologic de elaborare a strategiei de
modernizare a managementului unui spital;
• formarea resurselor umane: nevoia de formare a gestionarilor competenţi, a liderilor
percepuţi de către echipele lor ca purtători de sens şi capabili să le orienteze spre
obiective precise şi stimulative.
LIMITELE CERCETĂRII NOASTRE ŞTIINŢIFICE
Desigur, munca noastră de cercetare ştiinţifică nu este scutită de limite atât la nivelul
teoriei, al metodologiei, cât şi al concluziilor.
• Astfel, una dintre limitele acestei munci este legată de frontierele cercetării noastre,
care din motive obiective au fost mult restrânse (lipsa de date în special).
• Altă limită se referă la portofoliul nostru de investigaţiepe teren, datorită faptului că
nu am putut avea acces la entităţi de analiza ţintă (spitale). Încercările noastre de
realizare a anchetei pe un număr de spitale publice de referinţă (obiect al capitolului 5)
au eşuat datorită reţinerilor din partea factorilor decizionali ai potenţialelor spitale
vizate (din municipiul Bucuresti).
• altă limită este legată de absenţa cercetătorilor vizând managementul resurselor
umane în stabilimentele de sănătate în România.
• Nu în ultimul rând, o limită se referă la piedicile(obstacolele)care fac imposibil
şi/sau restricţionează analizele şi evaluările ce se impun în găsirea punctelor slabe
în gestiunea resurselor umane: absenţa de date, sistemul limitativ al IT, lipsa de
referinţe şi lucrări de cercetare ştiinţifică privind guvernaţa clinică în România.
PERSPECTIVE DE CERCETARE
Preocupările autoarei pentru tema de cercetare au reprezentat o constantă motivare de
dezvoltare personală care să-i asigure formarea competenţelor profesionale necesare într-o
perspectivă viitoare de implicare în conducerea unui stabiliment de sănătate, eventual creat
prin investiţii proprii.
A pilota un spital (sau o policlinică) necesită fără tăgadă dezvoltarea de competenţe
relative la funcţiile managementului în situaţiile contextuale de azi ale unităţilor sanitare,
pentru a identifica problematicile şi provocările care sunt relevante pe planul managerial. În
acest scop, intenţionez ca printr-o aprofundare a cercetării pe care am iniţiat-o cu ocazia
elaborării tezei de doctorat, să realizez un studiu exploratoriu pornind de la evoluţia şi
progresele reţelei de spitale din Turcia (îndeosebi cele private) pentru a repera soluţiile ce se
pot aplica în practică și în România.
BIBLIOGRAFIE
1. ABBAD, J. (2001), Organisation et management hospitalier, Paris: Berger –
Levrault.
2. ACADEMIA ROMANA, Institutul de lingvistică „Iorgu Iordan”, Dicţionarul
explicativ al limbii române (DEX), (1998), Bucureşti: Editura Universul
enciclopedic.
3. ALTER, N. (1998), Organisation et innovation: une rencontre conflictuelle,
Sciences Humaines, No 20, mars /avril 1998, pp. 56-59.
4. ANHOURY, P. et VIENS, G. (coord.), (1994), Gérer la qualité et les risques à
l’hôpital, Paris: ESF Éditeurs.
5. ALLANI-SOLTAN, N. (2003), L’effet des pratiques de gestion des ressources
humaines sur la performance des entreprises française, Thèse de doctorat,
Université Nancy 2, sursa citată în BERNARD Manon (2009).
6. ARAH, O.A., KLAZINGA, N.S., DELNOIJ, D.M.J., TEN ASBROEK, A.H.A.,
CUSTER, T. (2003), Conceptual frameworks for health systems performance: a
quest for effectiveness, quality, and improvement, International jornal for quality in
health care, vol.15, no 5.
7. ARCAND, M. (2000), L’effet des pratiques de gestion des ressources humaines sur
l’efficacitéde caisses populaires Desjardins du Québec, Thése de doctorat,
Université de Metz.
8. ARNAUD, J-O et BARSACQ, G. (1989), La dynamisation des ressources
humaines à l’hôpital, Paris, Gérer la santé, Edition ESF.
9. ARROW, K.J. (1963), Uncertainty and the Welfare Economics of Medical Care,
American Economic Review, 53 (5), pp.941-973.
10. BANCA MONDIALĂ ȘI GUVERNUL ROMÂNIEI (2011-2012), Analiza
Funcţională a Sectorului Sănătate în România, proiect cofinanţat din Fondul Social
European, prin Programul Operaţional Dezvoltarea Capacităţii Administrative,
sgg.gov.ro/File/UPP/doc/rapoarte-finale-bm/.../MS-RO-FR-Health-Sector-ROM.
11. BAREIL Céline et al., (2002), Les pratiques renouvelées de gestion des ressources
humaines dans le réseau montréalais de la santé et des services sociaux, Gestion,
2002/3 vol.27, pp.64-73.
12. BATAL, C. (2000), La gestion des ressources humaines dans le secteur public,
tome I, Paris : Edition Organisation.
13. BAYAD, M., ARCAND, G., ARCAND, M., ALLANI, N. (2004), Gestion
stratégique des ressources humaines : fondaments et modèles, Revue international
des relations de travail, janvier, vol. 2, no 1, pp. 76-77.
14. BEAUBEAU, D. et PEREIRA, C., (2003), Mesure de la performance dans le
domain de la santé, Présentation au 10-ième Colloque de compatibilé Nationale,
Paris: 22 janvier 2004.
15. BENAMOUZIG, D. (2005), La santé au miroir de l’économie, Paris: PUF.
16. BENETT, S., FRANCO, L.M. (1999), Public sector health worker motivation and
health sector reform: a conceptual framework, Bethesda, Maryland (SUA), Abt
Associates Inc. for Partnerships for health Reform Project (Major Applied Research
5, Technical Paper 1).
17. BERNARD Manon, (2009), L’effet des pratiques de ressources humaines sur la
performance sociale des employés dans le context de culture national, Thése de
doctorat en Science de Gestion, Université de Strasbourg, scd-these.u-
strasbg.fr/view/name/Bernard_Manon.html.
18. BJÖRNBERG, A. (2018), Health Consumer Powerhouse (HCP), Euro Health
Consumers Index 2017, Report, 1TUwww.heathpowerhouse.com/publications/euro-
health-index-2016/U1T.
19. BLUM, H.L.(1981), Planning for Health, generis for the Eighties, Londre: Human
sciences press.
20. BOLAND, T. and FOWLER, A. (2000), A Systems Perspective of Performance
management in Public Sector Organisations, Int J Public Sector Manag 13, pp.417-
446.
21. BOURDIEU, P., WACQUANT, L.J.D.(1992), Réponses pour une anthropologie
réflexive, Paris: Seuil.
22. BOURGUEIL, Y., MAREK, A., MOUSQUES, J. (2009), Trois modèles types
dîorganisation des soins primaires en Europe, au Canada, en Australie et en
Nouvelle Zélande, Questions d’économie de la Santé no 141-Avril 2009, IRDES
(Institut de Recherche et de Documentation en Economie de la Santé),
1TUhttp://www.irdes.fr/Publications/Qes/Qes141.pdfU
23. BOUSSARD Valérie (2013), Travail d’organisation gestionnaire des cadres et
mutation des entreprise publiques, La nouvelle revue du travail, 2013/2.
24. BUDET, J-M. (2001), Contractualisation interne: le cadre juridique, Gestion
Hospitalières. août – septembre 2001, No 167.
25. CANADIAN INSTITUTE FOR HEALTH INFORMATION, STATISTICS
CANADA (2000), Canadian Health Information Roadmap Initiative Indicators
Framework, Otawa: Canadian Institute for Health Information.
26. CANGUILHEM, G. (1966), Le normal et le pathologique, Paris, Quadrige, PUF.
27. CEBOLLA Beatriz (director de proiect), Etude menée par l’UE sur les maladies du
coeur (2016), Communiqué de presse: Euro Heart Index 2016,
1TUwww.healthpowerhouse.com/publications/euro/heart-index--2016U1T.
28. CERTO, S. C. (2002), Management modern, Diversitatea, calitatea, etica și mediul
global, București : Editura Teora.
29. CHAMBARETAUD Sandrine et HARTMANN Laurence (2004), Économie de la
santé : avancées théoretique et opérationnelles, Revue l’OFCE.
30. CHAMPAGNE, F., CONTANDRIOPOULOS, A.P., PICOT-TOUCHÉ JULIE,
BÉLAND, F. et NGUYEN, H. (2005), Un cadre d’évaluation de la performance des
systèmes de service de santé: le modèle EGIPSS (Évaluation globale et intégrée de
la performance des systèmes de santé), Université de Montréal, p.28.
31. CHAMPAGNE, F., CONTANDRIOPOULOS, A-P., DENIS, JL, LAMOTHE, L.,
(2002) Les centres universitaires de santé. La gouverne d’organisations complexe
aux contours flours. Document de travail préparé par la Département
d’Administration de la santé et le Groupe de recherche interdisciplinaire en santé,
Montréal, Université de Montréal.
32. CHAMPAGNE, F., CONTANDRIOPOULOS, A-P., TOUCHÉ, J., BÉLAND, F. et
NGUYEN, H. (2005), Un cadre d’évaluation globale de la performance des
systèmes de services de santé: Le modèle EGIPSS, Rapport de recherche, Group de
recherche interdisciplinaire en santé, Université de Montréal,
1TUhttp://www.csbe.gouv.qc.ca/.../Conseil SanteBienEntre/.../200U1T...
33. CIOCOUREL, A. (2002), Le raisonnement médical, une approche socio-cognitive,
Paris, Seuil.
34. CONTANDRIOPOULOS, S, A.-P. (2008), La gouvernance dans le domaine de la
santé: une régulaton orientée par la performance, Santé Publique, 2008/2, Vol. 20,
pp. 191-199, 1TUhttps://www.cairn.info/revue-sante-publique-2008-2-page-191.htmU1T
35. CONTANDRIOPOULOS, A.-P. & SOUTEYRAND, Y., éds (1996), L’hôpital
stratège: dinamiques locales et offre de soins, Paris: John Libbey Eurotext.
36. CONTANDRIOPOULOS, A.-P., CHAMPAGNE, F., DENIS, J.-L., AVERGUES,
M.C. (2000), L’évaluation dans le domaine de santé: concepts et méthodes, Revue
d’épidemologie et de santé publiques 2000, nov.48 (6), pp.517-539.
37. CONTANDRIOPOULOS, A.P., DENIS, J.L., TOUATI NASSERE, RODRIGUES,
R., (2001) Intégration des soins: Ruptures, revue transdisciplinaire en santé, vol. 8,
no2, 2001.
38. CONSILIUL JUDEŢEAN BUZĂU, (2016), Planul strategic al Spitalului Judeţean
de Urgenţă Buzău pentru perioada 2016-2020
39. CROZET, P., KAANICHE Asma et LIENARD J. (2008), Nouvelle gouvernance à
l’hôpital: recomposition de l’organisation et gestion des ressources humaines, revue
Politiques et management public, Vol. 26/2/2008.
40. CROZIER, M., SERIEYX, H., (1994), Du management panique à l’entreprise du
21ème siècle, Maxima.
41. CUCU Maria Alexandra (coord.), (2016), Raportul naţional al stării de sănătate a
populaţiei, Ministerul Sănătăţii, Institutul Naţional de Sănătate Publică, Centrul
Naţional de Evaluare şi Promovare a Stării de Sănătate.
42. DAHLGREN, G. & WHITEHEAD, M. (1991), What can we do about inequalities
in health, The lancet, no 338, pp.1059-1063
43. DAVIES, P. (2001), Stewardship: wat is it and kow can measure it? Presentation to
meeting on Health economics in developing and transitional countries: the
changing role of the state, Departament for International Development, York United
Kingdom, 26 July 2001.
44. DELOITTE, (2010), L’hôpital au coeur des réformes du système de santé. Réussir
sa transformation, Health Workforce Department World Health Organization,
Geneva 1TUwww.who.int/hrh.
45. DERVAUX Amélie, PICHAULT, Fr. și RENIERNathalie (2011), L’apport de la
théorie de l’acteur-réseau à la professionnalisation de la GRH en milieu hospitalier,
Journal d’Economie Médicale, nP
oP 1-2, vol. 29, pp. 62-73, Eska, Paris.
46. DESMIDT, S. and HEENE, A. (2006), Strategie en Organisatie van Publieke
Organisaties, Lannoo : Tielt.
47. DEVER, CHAMPAGNE, F. (1984), Epidemiology in Health Services Management,
Germantown, Maryland.
48. DIETRICH, A., PIGEYRE, F. (2005), La gestion des Ressources Humaines, Paris:
La Découverte, Coll. Repères.
49. DON DE SAVIGNY et TAGHREED, A. (ed) (2009), Pour une approche
systémique du renforcement des systèmes de santé, Alliance pour la recherche de
santé-OMS, 1TUhttp://www.who.int/alliance-hpsrU1T.
50. DONABEDIAN, A. (1966), Evaluating the Quality of Medical Care, The Milbank
Quaterly 44, pp. 166-203.
51. DONABEDIAN, A. (1978), The quality of medical care, Science 200 (4344),
pp.856-864.
52. DONABEDIAN, A. (1980), The definition of quality and approaches to its
assessment, Health Administration Press.
53. DORÉ Anne-Marie (coord) (2006), Encadrement et nouvelle gouvernance à
l’hôpital. Guide méthodologique, Ministère de la Santé et des Solidarités (France).
54. EVANS, R.G., BARER, M., MARMOR, T. (Eds) (1996), Être ou ne pas être en
bonne santé: biologie et déterminants sociaux de la maladie, Paris: John Libby
Eurotext.
55. FORUM NATIONAL sur la SANTÉ (1997), La santé au Canada: un héritage à
faire fructifier, Ottawa: Gouvernement du Canada.
56. FREIDBERG, E. (1993), Le pouvoir et la règle , Paris: Seuil.
57. FRIEDMAN, D. J., HUNTER, E. L. and PARRSH, R. G., (2002), Shaping a Health
Statistics Vision for the 21 st Century, Final Report November, 2002, [s.l], Centers
for sisease Control and Prevention, National Committee on Vital and Health
Statistics.
58. GALAMBAUD, B., LEON, E. (2008), Le sens de la mesure, le cas de la
performance en gestion des ressources humaines, Revue Gestion, Vol. 33, no.2.
59. GHEORGHE, A. (2012), Reforma spitalelor publice – evidenţe din spaţiul
european, Seria „Policy reports”, pp.8-12, Bucureşti: Observatorul Român de
Sănătate.
60. GHRISSI, M. L. (2011/2012), Le management des ressources humaines dans
l’hôpital public, CAS:CHU D’Oran, Thèse de doctorate en science, Faculté des
science économiques, des sciences de gestion et dans sciences commerciales.
61. GIRAUD Françoise, SAULPIC, O., BONNIER Carole, FOURCADE, F. (2008),
Contrôle de Gestion et Pilotage de la Performance, Paris : Gualino éditeur.
62. GIRAUD, F., SAULPIC, O., NAULLEAU, G., DELMOND, M-H., BESCOS, P-L.
(2004), Contrôle de gestion et pilotage de la performance, 2e édition, Collection
Business, Paris: Gualino éditeur.
63. GLOUBERMAN, S et MINZBERG, H. (2001), Managing the care health and the
cure of disease-PartI: Differentiation, Health care Management Review, vol. 26, no
1, pp.56-69.
64. GUERIN, G. et WILS, TH., (2002), La gestion stratégique de ressources humaines,
Gestion, 2002/2 vol..27, pp.14-23.
65. GUISSET Ann-Lise, SICOTTE, C., LECLERCQ, P., D’HOORE, W., (2002),
Définition de la performance hospitalière: une enquěte auprès des divers acteurs
stratégiques au sein hôpitaux, Sciences sociales et santé, 2002, Volume 20, numero
2, pp. 65-104.
66. HALL, T.L., MEJIA, A. (1979), La planification des personnels de santé: principes,
méthodes, problèmes, Genève, Organisation mondiale de la santé, sursă citată în
OMS (2006).
67. HAS (Haute Autorité de Santé-Franţa) (2009), Rapport d’évaluation. Le recours à
l’hôpital en Europe. Argumentaire, HAS/Service évaluation économique et santé
publique, Mars 2009, 1TUwww.has-sante.frU1T
68. HATCHUEL, A. (2000), Perspective et gouvernance: quelle théorie de l’action
collective?, en HEURGON, E.,, LANDRIEU, J. (sous la direction de), Perspective
pour une gouvernance démocratique, Paris, Éditions Aube, 2000.
69. HEALY, J&MCKEE, M (2002), Implementing hospital reform in central and
eastern Europe, Health Policy, vol. 61.no.1, pp.1-19;
70. HERREROS, G., (1996), Changements, pouvoirs et logiques d’action à l’hôpital,
Gestions hospitalières, Décembre 1996.
71. HOWLET, M. et. al. (2009), Studying Public Policy, New York, Oxford University
Press.
72. 1THOOD, Ch. (1991), A Public Management for All Seasons, Public Administration,
69 (1), pp. 3-19.
73. 1THOMBY, P., FORTE, P. (2002), Human resource indicators health service
performance, Keele (Royaume –Uni), Keele University, Centre for Health Planning
and Management.
74. HOLDEN, R.R., MAGRUDER, C.D., STEIN, S.J., SITARENIOS, G., SHELDON,
S. (1999), The effects of anonymity on the Holden Psychological Screening
Inventory, Personality and Individual Differences, 27, pp. 737-742.
75. 1THREBINIAK, L. G. (2009), Strategia în afaceri. Implementarea și executarea
eficientă, traducere CRISTEA Gabriela Camelia, bucurești, Editura ALL.
76. HURST, J., JEE-HUGHES, M. (2001), Performance Measurement and
Performance Management in OECD Health Systems, OECD, Labour market and
social policy, occasional papers nP
oP 47.
77. IGALENS, J., GOND, J.P., (2003), La mesure de la performance sociale de
l’entreprise: une analyse critique et empirique des données. Arese, Revue de Gestion
des ressources humaines, no 50, oct.-déc., pp. 111-129.
78. IGALENS, J., ROUSSEL, P. (1998), Méthodes de recherche en Gestion des
Ressources Humaines, Paris: Editions Economica, Collection Recherche en Gestion.
79. INSTITUTE OF MANAGEMENT ACCOUNTANTS AND ANDERSEN, A.
(1998), Tools and Techniques for Implementing Integrated Performance
Measurement Systems: Statement pn Management Accounting 4DD. Montvale, NJ.
80. IREF (Institut de recherches économique et la concurrence fiscale) (2017),
L’efficacité des systèmes publiques de santé europeens. Mieux vaut la concurrence
que le monopole, 1TUhttp://fr.irefeurope.org/Publications/INDEX-de-l-efficacite-de-la-
depense-publique/L-efficacite-des-systemes-publique-desante-europeensU1T
81. JAQUES, Jessica., (2012-2013), Indicateurs de performance clinique
hospitalière.Etudes empiriques basée sur les données medico-administratives
belges, Thèse présentée en vue de l’obtention du grade de docteur en sciences de la
santé publique, Université de Liege.
82. JUILLIARD – FOURNIER Nadine (2002), L’Hôpital organisé en pôles d’activités.
Perspectives et enjeux pour le directeur des soins, Mèmoire de l’École Nationale de
la Santé Publique, École Nationale de la Santé Publique (ENSP), Rennes.
83. KADDAR, M., (2004), Economie de la santé: brève
introduction,1TUwww.santemaghreb.com/algerie/comptes_/_rendus/jnp_200411/jour1_
1_kaddar.pdfU 1T
84. KESLEY, T. (2001), Améliorer la qualité des soins, în L’observateur de l’OCDE,
nr.229, Royaume Uni, Novembre, 2001.
85. KRIEGER, N. (2008), Ladders, pyramids and champagne: the iconography of
health inequities, Journal of Epidemiology and Community Health, 62 (12),
pp.1098-1104
86. LALONDE, M. (1981), Nouvelle perspective de la santé des Canadiens,
Gouvernement du Canada.
87. LAWRENCE, P.R., LORSCH, J.W. (1989), Adapter les structures de l’entreprise,
intégration au différenciation, Paris: Les éditions d’organisation.
88. LE POGAM Marrie-Annick, LUANGSAY-Catelin, NOTEBAERT, J.-F., (2009),
La performance hospitaliére : à la recherche d’un modèle multidimensionnel
cohérent, Management&Avenir 2009/5 (nP
oP 25), https://www.cairininfo/revue-
management-et-avenir-2009-5-page-116.htm.
89. LEATHERMAN, S. (2001), Être à la hauteur: mesurer et améliorer la performance
des systèmes de la santé dans les pays de l’OCDE, Extrait de la conférance
organisée par l’OCDE et le Canada-OCDE, Novembre.
90. LEATHERMAN, S. (2002), Utiliser les indicateurs de performance pour améliorer
les systèmes de santé dans les pays de l’OCDE, chapitre 15 en Smith, P. (éditeur)
(2002), Être à la hauteur. Mesurer et améliorer la performance des systémes de santé
dans les pays de l’OCDE, OCDE: Santé Canada,
https://books.google.ro/books?/slow=9266429595X..
91. LEGUELINEL Géraldine (2017), Initiation à l’économie de la santé, CHU Nimes,
Université de Montpellier,
1TUhttps://moodle.umontpellier.fr./.../DFGSP2_UE6_Initiation_P U1T...
92. LEVESQUE, J.F. et BERGERON, P. (2003), De l’individuel au collectif: une vision
décloisonnée de la santé publique et des soins, Ruptures, 9:2, pp.73-89.
93. LETHIELLEUX, L. (2014), L’essentiel de la gestion des ressources humaines
2014-2015, 8P
eP édition, Paris : Gualino Éditeur.
94. LOMBRAIL, P., NAIDITCH, D. and CUNEO, P. (1999), Les éléments de la
performance hospitatalière. Les conditions d’une comparaison, Etudes et résultats,
DREES 42, pp.1-8.
95. MACINKO, J., STARFIELD, B., SHI, L. (2003), The contribution of primary care
systems to health outcomes within Organization for Economic Cooperation and
development (OECD) countries, 1970-1998, Health Services Research, 2003; 38, 3,
pp. 831-865.
96. MARABET, M. (2018), Définitions, approches et concepts en santé publique, Notes
de cours santé publique Master USSAE.
Ufmp.um5.ac.ma/.../Définition%2C20concept%2C20approches%20en%20santé.pdf.
97. MARTY, C. et MERLIN, H, (2007), Mesurer la performance des hôpiteaux public
en France. Fundements méthodologique d’un modèle d’evaluation, enjeux, HEC
Paris, Observatoire du Manangement Alternatif, Cahier de resherche,
1TUhttp://creativecommons.org./licenses/by/2.0/frU1T.
98. MELIS, R.J., OLDE RIKKERT, M.G., PARKER, S.G., VAN EIJKEN, M.I.,
(2004), What is intermediate care?, BMJ 2004, 329 (7462).
99. MINISTERE DE LA SANTÉ ET DES SERVICES SOCIAUX (2007), Cadre
d’orientation por le développement et l’évolution de la fonction de surveillance au
Québec, Gouvernement de Québec.
100. MINISTERE DE LA SANTÉ ET DES SERVICES SOCIAUX DU QUEBEC
(2010), Cadre conceptuel de la santé et ses déterminants. Résultat d’une réflexion
commune, version mars 2010, 1TUhttp://intranetreseau.rtss.qc.caU
101. MINISTERE DE LA SANTÉ ET DES SERVICES SOCIAUX ET INSTITUT
NATIONAL DE SANTE PUBLIQUE DU QUEBEC (2005), Plan commun de
surveillance de l’état de santé de la population et de ses déterminants 2004-207,
Parte I: Cadre de référence, Québec, Gouvernement de Québec. février.
102. MINISTERUL SĂNĂTĂŢII (2014), Strategia Naţională de Sănătate 2014-2020.
Sănătate pentru prosperitate, Ministerul Sănătăţii, Bucureşti,
1TUhttp://www.ro/documente/Anexă%201%20-
%20Strategia%Naţională%20de%20Sănătate_886_1761.pdfU
103. MINISTERUL SĂNĂTĂŢII (2011), Ordin metodologic al ministrului sănătăţii.
104. MINISTERUL SĂNĂTĂȚII, Legea nr. 95 din 14 aprilie 2006 privind reforma din
domeniul sănătății, Republicată în temeiul ar. VI din Legea 184/2015 privind
aprobarea Ordonanței de urgență a Guvernului (OUG) nr. 77/2011 privind stabilirea
unor contribuții pentru finanțarea unor cheltuieli în domeniul sănătății precum și
pentru modificarea și completarea Legii nr. 95/2006 privind reforma în domeniul
sănătății. Cu modificările aduse de: Legea nr. 2 din 12 ianuarie 2017 pentru
modificarea Legii nr 95/2006 privind reforma în domeniul sănătății; Legea nr. 185
din 24 iulie 2017 privind asigurarea calității sistemului de sănătate.
105. MINTZBERG, H. (2008), Ascensiunea și declinul planificării strategice, București,
Editura Publică.
106. MINVIELLE, E. (2000), Réconcillier standardisation et singularité: les enjeux de
l’organisation de la prise en charge des malades, Rupture, revue trandisciplinaire en
santé, 2000, (7), pp. 8-22.
107. MOISDON. J. C. (2008), Gouvernance clinique et organisation des processus de
soins : un chrainon manquant ?
108. MOISDON, J. C., TONNEAU, D. (1999), La démarche gestionnaire à l’hôpital,
tome 1 recherche sur la gestion interne, Seli Arshan.
109. MORIN, E.M., SAVOIE, A., BEAUDIN, G. (1994), L’efficacité de
l’organisation.Théorie, représentations et mesures,Gaétan Morin Éditeur.
110. MORIN, M. (2006), Nouvelles définitions de la santé: un regard psychosocial,
Spirale 2006/1, (no 37), 1TUhttps://www.cairn.info/revue_spirale/2006/1/page/29.htmU1T
111. MORISSON, V., GAGNON, F., MORESTIN FLORENCE et KEELING, M.
(2014), Mots-clés du domaine des politiques publiques favorables à la santé,
Rapport Centre de Collaboration nationale sur les politiques publiques et la santé,
Institut national de santé publique Québec, 1TUwww.ccnpps.ca.
112. MORTEN BALLE, H et al., (2013), la nouveau management public, les marchés
bureau critiques et les problèmes de coordination interdépartamentale : analyse
comparative de la haute fonction publique dans l’administration de l’Etat, Revue
Internationale des sciences Administratives, 2013/I, Vol. 79, pp. 31-51.
113. NICOLESCU, O., VERBONCU, I. (1996), Management, București, Editura
Economică.
114. New Zealand Ministry of Health (2003), Improving Quality (IQ): A systems
approach for the New Zealand Health and Disability Sector.
115. NOBRE, Th. (1999), L’hôpital:le modéle de la bureucratie professionnelle revisté à
partir de l’analyse du coût des dysfoncyionnements, Manuscrit auteur, publié dans
20ÉME CONGRES DE L’AFC, France, 1999, (halshs-00587813, version 1-21 Apr
2011).
116. NUTLEY, S. et SMITH, P.C. (1998), League Tables for performance improvement
in health care, Journal of Health Serv, Res. Policy, vol.3, no.1, pp.50-57, Janvier.
117. OCDE (1990), Les systèmes de santé, Paris: OCDE.
118. OECD (2010), Améliorer la performance des soins de santé: comment mesurer leur
qualité, Forum sur la qualité des soins, Paris, 7.8 octobre 2010.
119. OECD (2010), Systèmes de santé. Efficacité et politiques, Paris: OECD
120. OECD/European Observatory on Health Systems and Policies (2017), România:
Profilul Sănătăţii în 2017, State of Health in the EU,
1TUhttp://dx.doi.org/101787/9789264285392-roU1T
121. OGIEN, A. (2000), Médecine, santé et gestion, in Cresson et F. – X., SCHWEYER
(sous la direction de )Professions et institutions de santé face à l’organisation du
travail. Aspects sociologiques, Éditions de l’ENSP, Revues, 2000, pp. 133-148.
122. OMS, Préambule à la Constitution de l’Organisation mondiale de la Santé,
adoptată de Conférance internationale sur la santé, New York, 19 juin-22 juillet
1946, et entré en vigueur de 7 avril 1948, http//www.who.int.
123. OMS, Bureau régional pour l’Europe, (1984), Health Promotion:A discussion
document on the concept and principtes, Copenhague, http//www.who.int.
124. OMS (1998), Glossaire de la promotion de la santé, Division de la promotion de la
communication pour la santé, service éducation sanitaire et promotion de la santé,
Genève, 1TUhttp://whqlibdoc.who.int/hq(1998)/WHO_MPR_HEP_98.1_fre.pdfU1T
125. OMS (2000), Le rapport sur la santé dans le monde, 2000, Genève,
http//www.who.int
126. OMS (2000), The World Health Report 2000, Health systems: Improving
performance, Geneva, http//www.who.int.
127. OMS (2003), Health Systems Performance Assessment Debates, Methods and
Empiricism, http//www.who.int.
128. OMS - Bureau régional de l’OMS de l'Europe, (2005), Des systèmes de santé
renforces sauvent plus vies: un aperçu de la stratégie européenne de l’ OMS en
matière de systèmes de santé, Copenhague, http//www.euro.who.int.
129. OMS (2006), Rapport sur la santé dans le monde 2006: travailler ensemble pour la
santé, [email protected].
130. OMS (2007), Everybody’s Business: Strengthening Health Systems to Improve
Health Outcomes: Who’s Framework for Action, Genève, OMS, http//www.who.int.
131. OMS (2008), La Charte de Tallin: des systèmes de la santé pour la santé et la
prospérité, Copenhague,
1TUhttp://www.euro.who.int/_data/assets/pdf_file/0008/88604/E91439.pdfU1T
132. OMS (2008), Les soins de santé primaires – Maintenant plus que jamais, Rapport
sur la santé dans le monde, Uhttp:www.who.int/whr/2008/fr/index.html
133. OMS – Bureau régional de l”OMS de l”Europe, (2008), Direction et guvernance des
systèmes de santé dans la Région européenne de l”OMS, Comité régional de
l”Europe, Cinquante–hutième session, Tibilisi (Géorge), 15-18 septembre 2008, p.
4, 1TUhttp://www.euro.who.intU1T.
134. OMS (Bureau régional de l’Europe), (2010), Relever les principaux défi de la santé
publique et de la politique sanitaire en Europe: Progresser dans la recherche de
l’amélioration de la santé dans la Région européenne de l’OMS, Comité régional de
l’Europe, Soixantième session, Moscov, 13-16 septembre 2010,
http :Uwww.euro.who.int
135. OMS-Bureau régional de l’Europe (2011), Renforcement des capacités et services
de santé publique en Europe: cadre d’action, Comité régional de l’Europe,
Soixante et unième session, Bakou (Azerbaidjan), 12-15 septembre,
1TUhttp://www.euro.who.int/fr/who-we-are/gouvernanceU1T
136. OMS-Commission sur les déterminants sociaux de la santé,
1TUhttp://www.who.int/social_determinants/fr/U1T.
137. Ordinul Ministerului Sănătății 914 din 26 iulie 2006 pentru aprobarea normelor
privind condițiile pe care trebuie să le îndeplinească un spital în vederea obținerii
autorizației sanitare de funcționare, Anexa 3.
138. PARIS Valérie (2012), Le performances comparées des systèmes de santé, Les
Tribunes de la santé 2012/2(nP
oP35), https://www.cairn.info/revue-les-tribunes-de-la-
sante-2012-2-page-43.htm
139. PARSONS, T. (1977), Social systems and the evolution of action theory, New York,
NY: Free Press.
140. PAULHUS, D.L., (1991), measurement and control response bias, In: Robinson J.P.
141. PELJAK, D. (1997), Le management de subsidiarité au service de hôpitaux in
Gestions Hospitalièrea, juin-juillet.
142. PERETTI, J. M. (2012), Gestion des ressources humaines, 18P
eP édition, Paris :
Vuibert.
143. PETRELLA, R. (1996), Le bien commun, Brusselle: Labor.
144. PETRESCU I. (2003), Managementul personalului organizației, București : Editura
Expert.
145. PETRESCU M., STEGĂROIU, I., NĂBÂRJOIU N., DUICĂ A., DUICĂ M. C.,
POPA E., (2010), Managementul schimbării și riscului, Târgoviște : Editura
Bibliotheca.
146. PICHAULT, Fr. et NIZET, J. (2000), Les pratiques de gestion des ressources
humaines, Coll. Point/Inédit/Essais, editions du Seuil, Paris.
147. PIGEYRE, F., (2006), Les modèles d’analyse de la GRH, en Ministère Éducation
Nationale Enseignement Supérieur Recherche, Éduscol, les actes de la DGESCO,
Management et gestion des ressources humaines: stratégies, acteurs et pratiques,
Actes du séminaire national 23-26 août 2005, Cité internationale universitaire, Paris,
pp.7-16., eduscol.education.fr./D0033/, p.14.
148. POMEY, M. P., DENIS, J. L., CONTANDRIOPOULOS, A. P. (2008), Un cadre
conceptuel de l’analyse de la gouvernance clinique dans les établissements de santé,
Pratiques et Organisation des Soins, Revue trimestrielle, vol. 39 – no 3/, juilet –
september 2008.
149. RECHEL, B., McKee., (2009), Health reform in central and eastern Europe and the
former Soviet Union, The Lancet, vol. 374, no. 9696, pp. 1186-1195
150. RÉFIPS (Réseau francophone international pour la promotion de la santé), section
des Amériques (le „site web”) (2012), Déterminants sociaux de la santé. Cadres
théoriques.
151. REICH M.R. (2002) Reshaping the state from above, from within, from below:
Implications for public health,Social Science and Medicine 54, pp. 1669-1675.
152. RENAUT, L. (1999), Etude de la satisfaction des usages: De la mesure de
satisfaction...A l’amélioration de la qualité au Centre Hospitalier de Sens, Memoire
de l’Ecôle National de la Santé Publique,
1TUhttp://documentation.ehesp.fr/memoires/1999/edh/renant.pdfU
153. RISTEA Ana-Lucia, IOAN-FRANC, V., POPESCU Constanța, (2017), Metodică în
cercetarea științifică, Ediția a doua revizuită și adăugită, București : Editura Expert.
154. ROCHER, G. (1972), Talcott Parsons et la sociologie américaine, Paris: P.U.F.
155. SAINSAULIEU, I. (2006), La communanté de soins en question. Le travail
hospitalier face aux enjeux de la societé, Paris: Éditions Lamarre.
156. SALTMAN R.B., FERROUSSIER-DAVIS O., (2000), The concept of stewardship
in health policy. Bulletin of the World Health Organization 78 (6), pp. 732-739.
157. SHAVER, P.T., WRIGHTSMAN, L.S., eds., Measures of personality and social
psychological attitudes, San Diego, Academic Press, pp. 17-59.
158. SEGADE, J. P. (2000), La contractualisation à l’hôpital, Paris : Ed.
Elsevier/Masson.
159. SICOTTE, C., CHAMPAGNE, F., CONTANDRIOPOULOS, A.C. (1999), La
performance organisationnelle des organismes publics de santé, Rupture-Revue
trandisciplinaire en santé, vol.6, no 1, pp.34-36.
160. SICOTTE, C., CHAMPAGNE, F., CONTANDRIOPOULOS, A.P., BARNSLEY,
J. et al., (1998), A conceptual framework for analysis of health care organizations
performance, Health Services Management research, 1998, 11, pp. 24-48.
161. SOLAR, O., IRVIN A. (2011), A conceptual framework for action on the social
determinants of health. Social determinants of Health, Discussion Paper 2 (Pollicy
and practice), 1TUhttp://www.who.int/social determinants/fr/index.htmlU1T
162. STEINER, A. (2001), Intermediate care ...a good thing? Age Ageing 2001; 30
(Suppl 3).
163. ST-ONGE, S., AUDET, M., HAINES, V.et PETIT, A. (2004), Relever les défis de
la gestion des ressources humaines, 2ème édition, Montréal: Gaëtan Morin Editeur.
164. STOREY, J. (2003), La légitimité stratégique de la GRH, Encyclopédie des
ressources humaines, Vuibert, Paris.
165. TEIL ALICE (2000), Qu’appelle-t-on système de soins?, în Organization, decision
et financement du système de soins, revue Actualité et dossier en santé publique
(adsp) no 33, revue du Haut Conseil de la Santé Publique,
1TUhttps://www.hcsp.fr/explore.cgi/adsp?chef=62U1T
166. TILMONT, B., ALCARAZ, I. (2012), Concepts en Santé publique, D.U. Santé
Précarité, Lille 11-13-01-2012, p.17, 1TUwww.infectio-lille.com/.../2013-DU-Sante-
precarite-Tilmont_Alcaraz.pdf
167. 1TTOUPILLIER Danielle et YAHIEL, M. (2011), Rapport sur la modenisation de la
politique des ressources humaines dans les etablissements publics de santé, Centre
National de Gestion des Practiciens Hospitaliers et des Personnels de Direction de la
Fonction Publique Hospitalière, Ministère du travail de l’emploi et de la santé.
168. UNESCO-IIEP, (2015), Concepts de la gestion des resources humaines et
planification prèvisionnelle, Gestion des enseignant, Unité 2, [email protected]
169. VALLEJO J. (2013), La modernisation du services RH hospitaliers: un enjeu
stratégique?, Gestion et management, 2013, p.17, 1TUhttps://dumas.ccsd.cnrs.fr/dumas-
00933484U1T
170. VALLET, G. (1997), L’hôpital citoyen, D. H. La Revue des directeurs d’hôpitaux,
Mars 1997, p. 47.
171. VAGU, P., STEGĂROIU, I. (1998), Management general, Târgoviște : Editura
Macarie.
172. VAGU, P. și STEGĂROIU, I. (coordonatori), CROITORU G., DUICĂ Anișoara,
Duică, M. (2013), Tratat de management general, Vol. 1, Școlile de management,
Târgoviște : Editura Bibliotheca.
173. VINCENT Catherine et VOLOVITCH P. (2003), Les Syndicats face au
restructurations hospitalières, Revue française des affaires sociales, 2003/3, no 3,
pp. 121-140.
174. WINSLOW, C., (1920), The untilled fields of public health, Science, 51 (1306), pp.
23-33.
175. WONCA Europe (World Organization of Family Doctors) (2002), La définition
européenne de la médecine générale- médecine de famille,
1TUhttp://www.woncaeurope.org/web%20documents/European%20Definition%20of%
20family%20medicine/WONCA%20definition%20French%20version.pdfU1T
176. WORLD HEALTH ORGANISATION, Regional Office for Europe (2003),
Measuring hospitals performance to improuve the qualitz of care in Europe: a need
for clarifying the concepts and defining the main dimentions, Raport on a WHO
Workshop Barcelona, Spain, 10-11 January 2003.
177. Zaghdoudi, T. (2004), L’intervention de d’Etat dans le domaine sanitaire: l’hôspital
public, 1TUhttps://www.memoireonline.com>BiologieU1T et Médicine.
178. *** Quels principaux axes de réforme pour le système de santé en Roumaine?
Ambasade de France en Roumaine, Service economique,
https://www.tresor.economie.gouv.fr/Ressources/File/439310
179. ***SINTEZA – Profilul stării de sănătate 2016, Uinsp.gov.ro/sites/cnepss/wp-
content/uploads/2014/11/SSPR-2016.pdf
180. 1TUhttp://publications.msss.gouv.qc.ca/acrobat/f/documentation/2010/10-202-02.pdf
181. 1TUhttps://fr.wikipedia.org/wiki/Diagnosis_related_groupU 1T accesat 30,05,2018.
182. www.Public health in England, The report of the Committee of Inquiry into the
Future Development of the Public Health Function, London, HMSO, 1988.
183. xxx L’ordonance no 2005-406 du 2 mai 2005 prévoyant la simplification du régime
juridique des établissements de santé,France,
1TUhttp://www.legifrance.gouv.fr/wAspad/UntexteDeJorf?numjo=SANX0500028R U1T.
CURRICULUM VITAE
INFORMAŢII PERSONALE KAKİLLİOĞLU (AVCİ) GÜLAY
Şoseaua İancului Strada Floarea-Soarelui, Nr.45, Vila 19 Voluntari İlfov
Romania
-------------------- 0722.234.505
---------------------
--------------------
Sexul Feminin | Data naşterii 29.05.1971 | Naţionalitatea Turcă (cetățean turc şi român însă)
EXPERIENŢA PROFESIONALĂ
Perioada 2008 – 2012:
Perioada 1994 – 2008:
Perioada 1999 – 2008:
Perioada 1992 – 1994:
Director General şi Administrator al societatii NOVELLA HOME SRL, din Romania.
Director General al societatii PATRİAPLAST SRL, din Romania.
- Activitati de dezvoltare şi punere in aplicare de planuri, politici şi proceduri generale de
administare
- Urmarirea procesului de certificare İSO 9001
- Responsabil cu planning-ul resureselor umae, angajari şi desemnari in functii
- Responsabil cu intocmirea planurilor şi politicilor de administrare şi conducere a societatii
- Coordonarea activitatilor specifice unei societati cu obiect de activitate productia de bubnuri de uz
casnic din PVC.
- Activitati de coordonare a departamentului financiar contabil din punct de vedere al evidentei
contabile.
- Activitati de identificare a nevoilor de pregatire profesionala a personalului.
- Administrarea intalnirilor bilaterale referitoare la cererilor de concediu sau de demisie.
Director General şi Asociat al societatii PRESTİGE MOB SRL, din Romania.
- Activitati de dezvoltare şi punere in aplicare de planuri, politici şi proceduri generale de
administare
- Urmarirea procesului de certificare İSO 9001
- Responsabil cu planning-ul resureselor umae, angajari şi desemnari in functii
- Responsabil cu intocmirea planurilor şi politicilor de administrare şi conducere a societatii
- Coordonarea activitatilor specifice unei societati cu obiect de activitate productia de bubnuri de uz
casnic din PVC.
- Activitati de coordonare a departamentului financiar contabil din punct de vedere al evidentei
contabile.
- Activitati de identificare a nevoilor de pregatire profesionala a personalului.
- Administrarea intalnirilor bilaterale referitoare la cererilor de concediu sau de demisie.
Director Economic al societatii ASFEM İthalat Sanayi ve Ticaret Limited Şirketi, din Turcia.
- Stabilirearea şi continuarea relatiilor cu clientii.
- Administrarea legaturilor dintre clienti şi societate.
- Activitati de evidenta şi supervizare a platilor lunare ale clientilor
- Administrarea informatilor
LOCUL DE MUNCA ACTUAL
C.E.O. la SC BURAK TOYS İNTERNATİONAL SRL - Buftea / Romania
COMPETENΤE PERSONALE Experienta Conducere şi Administrare İnstitutii şi İntreprinderi
EDUCAŢIE ŞI FORMARE
1987 – 1991
2011 - 2012
2013 - 2014
2013 - prezent
Facultatea de İnginerie Chimică
Universitatea Yıldız din İstanbul
Academia de Studii Economice din Bucureşti
Diploma de Masterat
Administrarea Afacerilor (cursuri cu predare în limba română şi engleză)
Universitatea „Dimitrie Cantemir” din Romania
Facultatea de Ştiinte ale Educatiei
Pedagogia İnvatamantului
Universitatea Valahia din Targovişte / Romania
IOSUD – Şcoala Doctorală de Ştiinţe Economice şi Umaniste
Domeniul Management - doctorand
Limba(i) maternă(e) Turca
Alte limbi străine cunoscute
ΙNΤELEGERE VORBIRE SCRIERE
Ascultare Citire Participare la
conversaţie Discurs oral
Specificaţi limba străină: ROMANA B1/B2 B1/B2 B1/B2 B1/B2 B1/B2
Scrieţi denumirea certificatului. Scrieţi nivelul, dacă îl cunoaşteţi.
Specificaţi limba străină: ENGLEZA B1/B2 B1/B2 B1/B2 B1/B2 B1/B2
Scrieţi denumirea certificatului. Scrieţi nivelul, dacă îl cunoaşteţi.
Niveluri: A1/A2: Utilizator elementar - B1/B2: Utilizator independent - C1/C2: Utilizator experimentat
Competenţe de comunicare Bune competenţe de comunicare dobândite prin experienţa proprie de manager de spatii de productie.
Competenţe
organizaţionale/manageriale ▪ Leadership
Dobandita prin anii de exprienta in administrarea societatilor.
Competenţe dobândite la locul de
muncă ▪ O bună cunoaştere a resurselor umane
Dobandita prin anii de experinta in care am condus angajati din toate departamantele.
Competenţe digitale AUTOEVALUARE
Procesarea
informaţiei Comunicare
Creare de
conţinut Securitate
Rezolvarea de
probleme
Utilizator
Independent
Utilizator
Independent
Utilizator
Independent
Utilizator
Independent
Utilizator
Independent
▪ o bună stăpânire a suită de programe de birou (procesor de text, calcul tabelar, software pentru
prezentări)
Alte competenţe
Permis de conducere Categoria B
ANEXE
Universitatea „Valahia” din Târgovişte
IOSUD Valahia- Şcoala Doctorală de Ştiinţe Economice şi Umaniste
Facultatea de Ştiinţe Economice
Domeniul Management
Drd. Gulay (Avci) Kakillioglu
LISTA LUCRĂRILOR ȘTIINȚIFICE
ARTICOLE PUBLICATE ÎN
REVISTE ȘTIINȚIFICE
2016
Gulay (Kakillioglu) Avci,Analysis of Correlation Between Changes in Health
Spending per Capita and Gross Domestic Product on an Inhabitant of Romania
During 2000-2014, Internal Auditing and Risk Management, Athenaeum
University of Bucharest, vol. 42(1), pp. 35-42, June.
https://ideas.repec.org/a/ath/journl/v42y2016i1p35-42.html.
2018 ConstanţaPopescu, GulayKakillioglu, Milestones for the Development and
Repositioning of the Human Resources Division in a Hospital,Vol. 3, Nr. 2/2018,
pp. 48-52. ISSN 2537 – 4222, ISSN-L 2537 – 4222,
https://ceeol.com/search/article-detail?id=702740.
2018
Constanta Popescu, Gulay (Avci) Kakillioglu,Strategiile de reformă a sistemului
de sănătate din Româniaîn contextual tendințelordin țările U.E. , Procedia of
International Multidisciplinary Conference ICM 2018 Innovation , Creativity and
Management in the 21 st century Perspectives in Education,Academia Publishing-
AEPEEC, 2018, pp.60-65. ISBN 978-1-9998738-7-5.
2018
ConstanţaPopescu, KakilliogluGulay(Avci),Public Hospitals Performance
Theoretical Foundations and Challenges, International Conference,Globalization,
Innovation and Development.Trends and Prospects,, (G.I.D.T.P.), MAY 16-17,
2018, Alexandria, România, Lumen, (în curs de publicare).
2018 ConstanţaPopescu, KakilliogluGulay(Avci),The Need for an Integrative Approach
of the Healthcare System, International Conference « Global Interferences of
Knowledge Society » 2nd Edition, 16 - 17 November 2018, Târgovişte-Romania,
Lumen (în curs de publicare).
2018 Constanţa Popescu, KakilliogluGulay(Avci),Analyse comparative des indicateurs
de performance du système de santé en roumanie avec ceux des systèmes de santé
nationaux des pays européens,Congrès International d’Izmir des Sciences
Economiques et Administratives Izmir Turcia 05-08.12.2018, se publica in
volumul de conferinta(încurs de publicare).

PARTICIPĂRI LA
CONFERINȚE ȘI CERCURI
ȘTIINȚIFICE
2018 ConstanţaPopescu, GulayKakillioglu, Milestones for the Development and
Repositioning of the Human Resources Division in a Hospital,International
Scientific Conference Accounting and Finance – The Global Languages in
Business - 3nd Edition, Universitatea Constantin Brâncoveanu, Piteşti, 23 Martie
2018.
2018
Constanta Popescu, Gulay (Avci) Kakillioglu,Strategiile de reformă asistemului
de sănătate din Româniaîncontextultendințelor din țările U.E., International
Multidisciplinary Conference ICM 2018 „Innovation, Creativity and Management
in the 21st century. Perspectives in Education”, Istanbul, Turcia,mar.2018.
2018
ConstanţaPopescu, KakilliogluGulay(Avci),Public Hospitals Performance
Theoretical Foundations and Challenges, International Conference, Globalization,
Innovation and Development.Trends and Prospects,, (G.I.D.T.P.), May 16-17,
2018, Alexandria, România.
2018 ConstanţaPopescu, KakilliogluGulay(Avci),The Need for an Integrative Approach
of the Healthcare System, International Conference « Global Interferences of
Knowledge Society » 2nd Edition, 16 - 17 November 2018, Târgovişte-Romania.
2018 Constanţa Popescu, KakilliogluGulay(Avci),Analyse comparative des indicateurs
de performance du système de santé en roumanie avec ceux des systèmes de santé
nationaux des pays européens, Congrès International d’Izmir des Sciences
Economiques et Administratives Izmir Turcia 05-08.12.2018.
MINISTRY OF EDUCATION
„VALAHIA” UNIVERSITY, TÂRGOVIŞTE
IOSUD-DOCTORAL SCHOOL OF ECONOMIC AND HUMANISTIC
SCIENCES
Domain: MANAGEMENT
SUMMARY OF DOCTORAL THESIS
CLINICAL GOVERNANCE:
A MAJOR STAKE FOR THE PERFORMANCE
OF PUBLIC HOSPITALS IN ROMANIA
SCIENTIFIC SUPERVISOR:
Professor CONSTANŢA POPESCU, M.D.
CANDIDATE:
GULAY AVCI (KAKILLIOGLU)
TÂRGOVIŞTE
2019
DOCTORAL THESIS SUMMARY –TABLE OF CONTENTS
DOCTORAL THESIS - CONTENTS ...................................... Error! Bookmark not defined.
KEYWORDS .............................................................................. Error! Bookmark not defined.
IMPORTANCE, TOPICALITY AND NOVELTY OF THE THEME ..... Error! Bookmark
not defined.
SUBJECTS AND HYPOTHESES ............................................ Error! Bookmark not defined.
EPISTEMOLOGICAL POSITIONING OF THE PHD THESIS ....... Error! Bookmark not
defined.
STRUCTURE OF THE PHD THESIS ..................................... Error! Bookmark not defined.
GENERAL CONCLUSIONS .................................................... Error! Bookmark not defined.
THE SCIENTIFIC CONTRIBUTIONS OF THE PHD THESIS ....... Error! Bookmark not
defined.
THE LIMITATIONS OF OUR SCIENTIFIC RESEARCH . Error! Bookmark not defined.
RESEARCH PERSPECTIVES ................................................. Error! Bookmark not defined.
BIBLIOGRAPHY ....................................................................... Error! Bookmark not defined.
CURRICULUM VITAE ............................................................ Error! Bookmark not defined.
LIST OF SCIENTIFIC PAPERS .............................................. Error! Bookmark not defined.
DOCTORAL THESIS - CONTENTS
List of quadrans................................................................................................................... 4
List of figures......................................................................................................................... 5
List of tables ....................................................................................................................... 6
List of abbreviations ........................................................................................................ 7
Glossary ................................................................................................................................ 9
INTRODUCTION............................................................................................................. 15
CHAPTER 1. HEALTH SERVICES: THEORETICAL TERMS, CONCEPTS AND
APPROACHES ……………………….....................................................
21
1.1. Health: definition and approaching methods…………………………………………… 21
1.2. Public health: definition…………………………………………………………............ 24
1.3. Social determinants of health: theoretical frame………………………………………... 25
1.4. Healthcare economy: theoretical foundation of health services market……………….... 27
1.5.Healthcare system and health service system: definition and delimitation………………. 31
1.6. Primary health: definition and importance………………………………........................ 35
1.7. Health service system: evolution from an epistemological perspective ………………… 38
1.8. Health service system: a system organized on action ……………………………............ 43
The conclusions of the chapter ……………………………………........................…………. 47
CHAPTER 2. THE PUBLIC HOSPITAL: A PLACE OF MAJOR CHALLENGES IN
THE CONTEXT OF THE HEALTHCARE SYSTEM
REFORM......................................................................................................
51
2.1. Evolution of the hospital healthcare structures in Europe and their activity ………....... 52
2.1.1. General context that triggers the need of reforming the hospital service system
in the European Union ………………………...…………………..........................
52
2.1.2. Organising primary healthcare and hospital ………..…………………………….. 55
2.1.3. Hospital typologies found in EU countries………………………..………............. 56
2.1.4. Organisational innovations………………………………………..……………..... 57
2.2. The convergence of Romanian hospital reform with the tendencies in Western European
countries …………………..……………………………........................................................
63
2.2.1. New institutional structures that support the hospital reform in Romania ……….. 64
2.2.2. Hospital network reform, a major stake for the healthcare system in Romania….. 65
2.3. Indicators of the resources and activity of public
hospitals……………..................................................................................................................
70
2.3.1. Resources…………………………………………………………..……………… 70
2.3.2. Activity indicators (results)………………………………………..……................. 76
2.4. Healthcare system performance in Romania …………..………………………………… 77
2.5. Main defining elements of health status of the population in Romania ……………….. 81
The conclusions of the chapter ……………………………………………………………….. 86
CHAPTER 3. HEALTH SERVICE PERFORMANCE: THEORETICAL AND
PRACTICAL APPROACHES …………………………………………….
87
3.1. Organisational performance: multidimensional concept ……………………………….. 88
3.2. Health service performance: defining frameworks………………………………………. 94
3.3. Main evaluation frameworks of health service system performance …………………… 103
3.3.1. Evaluation framework of healthcare system performance drawn up by WHO … 103
3.3.2.Evaluation framework of hospital performance drawn up by the WHO Regional
Office for Europe …………………………………………...……………........................
105
3.3.3. Evaluation framework of health service quality promoted by OECD……….…… 107
3.3.4. Conceptual frameworks of measuring the health service performance in some
countries with notable results …………………………………...……………………….
112
3.3.4.1. UK…………………………………………………...…………………… 112
3.3.4.2. United States of America……………………...…………………………. 113
3.3.4.3. Canada…………………………………………………………..……….. 115
3.3.4.4. New Zealand……………………………………………….…………….. 116
3.3.4.5. Australia…………………………………………………..……………… 117
The conclusions of the chapter ……………………………………………..………………. 118
CHAPTER 4. HUMAN RESOURCE MANAGEMENT: A MAJOR STAKE IN
PUBLIC HOSPITAL PERFORMANCE ……………..…………….......
119
4.1. Specificity of hospital services …………………………………………………………. 119
4.2. Public hospital: complex organisation with a divided and shared structure ………..…… 120
4.3. Strategic human resource management: definition ……………………………..………. 123
4.4. Evolution of concepts that operate in the human resource management domain from an
epistemological perspective ………………………………….……………………………...
128
4.5. Governance: a new space of collective control of hospital activities ………………….. 131
The conclusions of the chapter ………………………….…………………………………. 135
CAPITOLUL 5. HOSPITAL PERFORMANCE DIMENSIONS: A SURVEY AMONG
THE VARIOUS STAKEHOLDERS AT THE BUZAU EMERGENCY
COUNTY HOSPITAL.................................................................................
137
5.1. Theoretical context of field research................................................................................... 137
5.2. Survey carried out among the staff of the Buzau Emergency County Hospital ……..…. 143
5.2.1. Place of survey…………………………………………………………………….. 143
5.2.2. Methodological aspects of the survey ………………………………..…………… 144
5.2.3. Results of the survey………………….……………………..……………………. 147
5.2.3.1. Survey characteristics……………………………………………………. 147
5.2.3.2. Conclusions of the survey ………………………………………………. 148
The conclusions of the chapter ……………………………………………………………... 166
Chapter 6. CLINICAL GOVERNANCE: GUIDELINES OF GOOD PRACTICE FOR
ACHIEVING THE PERFORMANCE OF HEALTH
SERVICES............................................................................................................
167
6.1. Challenges of national healthcare systems in Member States of the European Region of
WHO …………………………………………………..........................................................
167
6.2.New concepts of hospital management: management deconcentration and internal
contractualisation through the creation of activity poles …………………………………….
175
6.3. Defining the elements for a move towards a clinical
governance................................................................................................................................
181
6.4. Methodological and practical benchmarks for approaching a new hospital governance.
A methodological guideline ………………………………………………………………….
186
6.4.1. First stage: Strategic diagnosis …………………………………………………... 187
6.4.2. Second stage: Designing the move towards a new hospital governance
…………………………………………………………………….....................................
189
6.4.3. Third stage: Implementation of the project of moving towards a new hospital
governance ……..……………………………………………………………..…………
192
The conclusions of the chapter ………………………………………………………............ 195
GENERAL CONCLUSIONS....................................................................................................
SCIENTIFIC CONTRIBUTIONS.....................................................................................
RESEARCH LIMITS....................................................................................................
RESEARCH PERSPECTIVES..................................................................................
196
201
202
202
BIBLIOGRAPHY…………………………………………………………………………….. 204
ADDENDA................................................................................................................ 222

KEYWORDS
• Human resource management
• Strategic human resource management
• Clinical governance
• Social determinants of population health
• Healthcare economy, health service system
IMPORTANCE, TOPICALITY AND NOVELTY OF THE THEME
The individual's health is inevitably a decisive stakeholder in the socio-economic
development of a country. Health strategies cover one of the spaces of expression of quality
of life and human dignity, at the same time as a place where work capacity is regenerated,
perpetuated and reproduced.
As a consequence of this postulate, it becomes necessary to create a national health
system prepared to meet the global needs of the population. This is put into practice through a
package of levers that facilitate the integration of prevention and cure activities, the
classification according to interventions and creation of a care hierarchy in order to streamline
and rationalize the management process of the health infrastructure.
Health infrastructure covers not only the human and material resources found in the
form of organizational and administrative structures, and also structures for public and
political awareness of health problems and participation in measures to address these issues.
Within this infrastructure, the public hospital is called upon to play a large role
that gives it the position of a lead stakeholder in meeting citizens' aspirations in terms of
quality, transparency, and exigency. Faced with these challenges, hospital management
needs a major modernization effort focusing on one of its main axes, namely human
resources. Indeed, the importance of human resources as a success generator for
organizations no longer needs to be demonstrated. Human resources are the engine of any
organization and can boost the dynamics of change and be the vector of considerable
performance. In fact, the performance of human resource management is considered as one
of the key stakeholders for success and dynamization of change in favour of value creation for
the entire organization.
In this thematic context, we integrate our research focusing on the new concept of
human resource management for public hospitals belonging to the Romanian national
health system.
Our study aims to improve knowledge on effective human resource management
through appropriate implementation of practices that enable a public hospital to be
more efficient in its environment under the pressure of day-to-day changes. In a competitive
environment, human resource management is the fundamental element of the strategic
equation.
SUBJECTS AND HYPOTHESES
Hospital services should meet the high requirements regarding quality and
improvement of their performance. The patient, the customer and the consumer of healthcare
have precise expectations regarding the quality of care, reception and information. In order to
respond to these demands, the public hospital needs to undergo reform on the basis of a
crisis exit strategy monitoring the progress in its improvement on several levels:
- at the level of internal organization and work methods;
- at the level of management systems, with a special focus on human resource
management.
Our PhD thesis focuses on the major component of the healthcare system: the
tertiary care service link – the public hospital. The scientific questions for which
answers have been sought through our approach are:
- - How is the performance of hospital activity perceived by the medical staff?
- What are the stakeholders that make it possible for the medical staff of a
hospital to act in a manner that is adequate for the needs of their patients?
Finding answers to these two scientific questions is based on three hypotheses
that we will take into account in our scientific approach, namely:
4. The financial crisis of public hospitals in the general context of the budget
deficit faced by the Romanian national health system is only one of the clear
forms of a profound crisis of the traditional hospital model at a structural level:
in its missions and staffing.
5. The crisis of hospital staff increases the crisis of public hospitals and the exit
from the crisis can be found both in the modification of the financial
management, and in the modification of the human resource management
system.
6. The hospital sector is a territory favourable for the development of network
structures, for example by creating activity poles that will integrate compatible
services.
These assumptions logically integrate in a general theme by relying on the
demonstration that human resource management is at the heart of the process of change
and modernization of the public hospital.
EPISTEMOLOGICAL POSITIONING OF THE PHD THESIS
The theme of the PhD thesis is, from an epistemological perspective, covered by the
sphere of human resource management discipline. The scientific field of human resource
management within the hospital – a complex organization with a particular organizational
structure - is broad, transversal, and composed of sub-fields (services / activity poles) that are
autonomous.
• The scientific research underlying our PhD thesis is at the same time:
- an exploratory research, in that it was based on a documentary focusing on the
confirmation of assumptions and discovery of new trends/concepts;
- a positive research, meaning that a series of recommendations are made (Chapter 6)
to legitimize practitioners' understanding of the paradigms underpinning clinical governance;
- a hypothetical-educational research, based on the formulation of hypotheses
deduced from theories validated by practice and subsequently turned into generalizations.
• Type of information research: we used information and data from public sources
(Ministry of Health, EUROSTAT, OECD, WHO, etc.), and from materials published on the
Internet, prepared by well-known university researchers from the scientific world.
STRUCTURE OF THE PHD THESIS
The PhD thesis is structured into six chapters, plus an introduction and a final
section of general conclusions and personal contributions.
Chapter 1 - "Health Services: Theoretical Terms, Concepts and Approaches" –
has been prepared having documentary reference sources mainly consisting of international

studies and publications with a high degree of visibility in the scientific and academic
environment, which have built the epistemological foundation of the investigated field. In
essence, this chapter aims at defining the scope of the research for our PhD thesis – the
public hospital. For this, the first chapter of our PhD thesis addresses the key concepts that
define the health services system, its components and its links with the healthcare system as a
whole. Thus, we have approached the theoretical framework of concepts defining the complex
and inclusive content of health services: the social determining stakeholders of health; health
economics – the theoretical foundation of the health services market; the healthcare system
and the health services system, the latter being treated as an organized action system.
The health services system as an organized action system, with organized
subsystems, cannot assume the major functions that it needs to fulfil without the
integration of health services, this being the potential solution to fight potential
malfunctions that occur when the components of the system act independently of one another.
Essentially, integration is the process of creating and maintaining, over time, a
joint leadership between autonomous stakeholders (and organizations) in order to
coordinate their interdependencies to allow for co-operation in carrying out a collective
project. In the economic field, integration does not have a systemic connotation, as it aims at
achieving higher productivity or important savings. Firstly, a business company considers
integrating its production cycles by coordination with a number of activities that are located
upstream or downstream of its own activities (i.e., outside the company in question). We are
talking here about vertical integration. When there is a situation of similar companies merging
to achieve important savings, a horizontal integration takes place.
The dimensions of integration of health services aim at establishing a coherence
between the clinical system (consisting of the modalities of accepting patients for care and
the good practice rules, ensuring optimal integration of healthcare in terms of time, space and
between health professionals), the management (consisting of a management system, a
financing system and an information system) and the collective system of interpretations
and values (the set of beliefs, values, interpretation schemes that allow stakeholders to
communicate with each other, coordinate their actions and cooperate) that structure the space
in which stakeholders (organizations) interact. The various forms that the integration process
can take aim, in varying degrees, to institutionalize the cooperation relations among all
stakeholders involved in the situation of interdependence in relation to one or several
joint projects. The five dimensions of the integration process should be implemented in a
sustainable manner over time: (1) integration of care; (2) integration of the clinical team
(medical integration); (3) functional integration; (4) normative integration; (5) system
integration.
Chapter 2 - "The Public Hospital: a place of major challenges in the context of
the healthcare system reform" - aims at analysing and evaluating the process of
reforming hospitals in Romania from the perspective of its convergence with the trends
of hospital services development in EU Member States. This chapter is based on the
analysis of reports by two international bodies, the OECD and The European Observatory on
Health Systems and Policies, supplemented by two studies on the assessment of the healthcare
system reform in Romania, and by a review of health literature.
The state of hospitals in Romania is far from being able to meet the requirements
of the population for quality medical services at the highest European standards. The
healthcare sector is based on an infrastructure that was designed 50-60 years ago, when the
need for services was different from today's realities. The existence of old buildings (some
over 100 years old) whose constructive solutions do not allow the optimum integration of
intrahospital circuits raises major difficulties in modernizing hospital functions with
repercussions on patient safety and avoidable expenses.
The previous failure of the reform strategies of the Romanian healthcare system
stringently requires a strategic framework for rethinking the system. It is important to note the
healthcare system reform directives included in two key documents: The 2014-2020 National
Health Strategy and the 2017-2020 Multi-Annual Plan for the Strategic Development of
Human Health Resources. At this stage, none of the two documents is operational, and the
implementation plans are still not ready.
The Ministry of Health has identified the hospitals belonging to the strategic
network where the necessary infrastructure investments will be targeted, in line with the
vision of the 2014-2020 National Health Strategy. We appreciate that the directions of
action outlined in this document are pertinent and necessary:
- transformation of local hospitals located in small and medium-sized towns into
institutions that provide outpatient services, day care or care services for chronic
patients, with the contribution of local authorities;
- development and rationalization of county hospitals;
- development and rationalization of regional and national hospitals – the process will
include the reduction of the number of buildings, pavilions and single specialty
hospitals and their integration into new or rehabilitated and modernized buildings
within the regional hospitals;
- modernization and endowment of healthcare institutions that will fulfil the role of
regional emergency hospitals;
- construction of three regional emergency hospitals: Iasi, Cluj Napoca, Craiova;
- bringing the infrastructure of radiotherapy and oncology services to modern standards
of operation.
Chapter 3 - "Health Service Performance: Theoretical and Practical
Approaches" synthesizes theoretical concepts developed over time that define the
performance of healthcare organizations and have been validated in the practice of many
countries that has confirmed that the promotion and improvement of public health is the major
objective (priority) of a health system, but the performance analysis of healthcare systems is
not limited to this factor. Other factors that define the performance level of a healthcare
system are highlighted in this chapter:
- the improvement of the health status generated by the healthcare system;
- the quality of care;
- the capacity of the healthcare system to meet the expectations of the population;
- the equity of access to healthcare;
- the productive efficiency (productivity).
Chapter 4: "Human Resource Management: A Major Stake in Public Hospital
Performance" - is a synthesis of theoretical approaches taken from the review of reference
documentary sources on the development and repositioning of human resources as a key stake
in public hospital reform . The new concepts of human resource management – "human
resource management", "strategic human resource management" – are approached in
close connection with the specificity of hospital services given by the particularity of the
public hospital as a complex organization with a divided and shared structure.
This organizational split of the public hospital is generated by the distribution of
power within it. It is a bicephalic power, on the one hand the administrative power
represented by the director/manager of the hospital on whom the staff (except the doctors) is
dependent, the director being the person in charge of the working conditions. On the other
hand, the medical power in charge of the organization of work of the staff providing health
services. Two management structures correspond to these two entities: the board of
directors, which determines the hospital activity, and the hospital medical committee
(HMC), made of doctors, in charge of the medical activity.
Governance: a new space for collective control of hospital activities
In the field of health, the emergence of the concept of governance of healthcare
institutions is supported by three solid arguments:
First of all, the options for the provision of health services that need to be
coordinated cover the perimeter of responsibility that goes beyond that of existing
organizations, while governance requires the approach of a new space for collective
organization and control.
The actions to be coordinated and to be taken into account have inter-organizational
and inter-professional dimensions that are not reduced to summing up the actions of each
organization or each professional framework. Governance requires us to reflect on the
coordination of stakeholders and organizations that are simultaneously autonomous and
interdependent to ensure fair access to quality healthcare for a defined population and to
contribute to cross-sectoral health policies.
In the provision of health services there are four large groups of stakeholders who
interact, each with its own contribution concerning the logic that should guide their
decisions:
5. medical professionals (doctors, nurses, pharmacists, dentists...) who value
professional logic;
6. management (donors, evaluators, officials...) who base their decisions on technocratic
logic and formal rationality;
7. commercial world (pharmaceutical companies, insurance companies, financial
groups involved in the supply of healthcare...) and
8. political world (elected representatives, legitimate representatives of constituted
groups...) who claim the superiority of democratic logic.
Governance can be defined as the conception, management and evaluation of
collective action based on a position of authority. It relies on:
4. a management system: the set of rules defining how power and responsibilities are to
be distributed;
5. an information system: the set of data and their operating system necessary for the
organized system of action to be intelligible and transparent at all times for healthcare
professionals, managers, planners, patients and population;
6. a funding system: all the financing provided through various modalities, the budget
allocation mechanisms and the stakeholder’s payment mechanisms.
Chapter 5 - "Hospital Performance Dimensions: a survey among the various
stakeholders at the Buzau Emergency County Hospital" - presents the results of an
investigation carried out among the staff of a county emergency hospital (Buzau). This survey
allowed a qualitative analysis based on a theoretical performance model developed by Sicotte
et al.6P. The survey had two objectives. First of all, it was intended to discover the performance
concept of the various stakeholders within the hospital. Secondly, based on the opinion of the
different categories of stakeholders – depending on the professional group of membership – it
was sought to determine possible areas of consensus or divergence. Highlighting these areas
of consensus or divergence is important because a hospital can only be efficient if its
stakeholders are joining forces to achieve a number of common goals.
In the context of the conceptual design of field research (point 1.), it was sought to
obtain relevant information (confirming the assumptions of the inclusive model of
organizational performance by Sicotte et al.) for the substantiation in chapter 6 of the PhD
thesis of some general recommendations under the title "Guidelines of Good Practice for
Achieving the Performance of Health Services in a Public Hospital".
• The central objective of the survey is to explore (the survey being a descriptive
exploratory study) the conceptions (perceptions) of the key decision-makers of the
Buzau Emergency County Hospital on the performance of hospital services and
then to propose levers and tools to support the steering of the activity. This type of
survey (field research) is an appropriate technique to explore the representations of
performance in the stakeholders' speeches and to look for differences or similarities in
the conceptions of various categories of stakeholders, depending on their socio-
professional peculiarities.
• The following hypotheses are considered in the interpretation of the survey:
- The central hypothesis of our research is that hospital performance can only be
sought in a shared vision of different stakeholders with direct links to hospital activity:
county health directorates, State and Health Insurance representatives, health unions, medical
staff and patients.
- The second hypothesis assumes that the Hospital cannot improve its
performance as long as it is administered and not managed. This performance requires the
commitment of a management process (governance) that is completed by seeking a shared
vision of local and regional stakeholders involved.
6SICOTTE C., CHAMPAGNE F., CONTANDRIOPOULOS A. C., BARNSELJ J et al (1998), A conceptual
framework for analysis of healthcare organisations performance, Health Services Management research, 1998,
no 11, pp. 24-48.
Chapter 6 - "Clinical Governance: Guidelines of Good Practice for Achieving the
Performance of Health Services" – has as a general theme the new concept of clinical
governance based on the recognition of an interdependence between the clinical practices and
the organizational context in which healthcare professionals work. In this chapter, we used a
series of reference documentary sources to develop a special practical approach that provides
the steps to be followed for general hospital steering (overall governance) and structuring the
stakeholders’ work in the operational area (proximity governance). In essence, the chapter
provides a management model that builds on a shared management/physician
leadership by seeking synergy between the management (stewardship) and the medical
staff, with the ultimate goal of balancing governance between the general direction and
the medical community. All this starts from the postulate that the hospital is a "private
administration that has to aim for an <adapted governance>".
The first section of this chapter approaches two new concepts of hospital
management: management deconcentration and internal contractualisation through the
creation of activity poles.
Contractualisation is a response to the complexity of the medical organization
(the hospital), recognizing a more decentralized analysis and decision-making level.
Management deconcentration and contractualisation are key success factors in
human resource management within a hospital because they lead to the introduction of a
management animated by a willingness towards involvement and mutual engagement.
A deconcentrated management calls into question the current hierarchical organization
and the structuring of health services. This structuring requires:
✓ moving from a status logic, based on a pyramid hierarchy, to a contract logic based on
the competence of the stakeholders and their results;
✓ additional transversality both within the activity pole and between poles.
The establishment of activity poles normally aims at improving the organization of
hospitals, in particular by pooling competences and means a constant adjustment of
resources to patients' needs. These poles do not replace services. They form a new
"extra layer" structure in the organization of hospitals.
✓ The creation of activity poles is based on four elements:
▪ Deconcentration of management: the tasks undertaken so far by the management of
the institution are performed by the clinical and medical-technical poles. In fact, pole
coordinators are given a decision-making power in a wide range of areas (finance,

acquisition, organization of work units, etc.) subject to compliance with the
institution’s strategy and budget.
▪ A pole project: elaborated by the pole officer who associates with the pole council for
project preparation. It is a pluriannual document with medical and organizational
content that defines the current activity of the pole and its future development and
types of internal organization.
▪ A pole contract: negotiated between the director of the hospital and the chair of the
medical commission of the institution, the deans of the faculties of medicine and
pharmacy, on the one hand, and the pole coordinator, on the other hand, after the
approval of the Executive Council; the pole contract defines the activity, quality and
financial objectives, the means and indicators of the pole, the methods of obtaining the
expected results and the consequences in case of contract default.
▪ Inter-pole contracts
The management through activity poles corresponds to an evolution of hospital
management, the decisions being made in a collaborative way: the poles are led by a
trio consisting of a physician, head of the pole, a senior medical professional and an
administrative employee. Thus, pole management gives hospital management
stakeholders the opportunity to imitate (intertwine) links between doctors, nursing
staff, administrative staff, forcing them to work in a team rather than separately.
The thematic core of the sixth chapter of the thesis, which is found in a second
section, is formed by the methodological and practical benchmarks for
approaching a new hospital governance, which formed the basis of the proposed
methodological guidelines.
From a methodological perspective, the approach of implementing a new hospital
governance takes place in three main stages:
➢ First stage: Strategic diagnosis. The purpose of the strategic diagnosis is to
position the hospital in the context of the health territory and establish the
challenges it faces. Specifically, a strategic diagnosis aims at the following:
• placing the hospital in a sanitary, political, social and economic context, taking into
account the offer of the competition;
• identifying and evaluating strengths and weaknesses, opportunities and threats (a
SWOT analysis) of the hospital (its internal environment);
• objectively identifying the performance tools, their contributions and their limits;
• identifying the communication policy.
A strategic diagnosis is based on finding answers to the following questions:
• What are the objective and objectifiable data of the hospital: number of beds, staff,
budget, contact with patients, medical activities, etc?
• What is the information system policy: tools for collecting institutional information,
documentary management procedures, assessment of the effectiveness of the
instruments by the stakeholders?
• What are the indicators of resources, activities, results?
• How comprehensive and coherent are the gathered data?
➢ Second stage: Designing the move towards a new hospital governance
This second stage should allow hospital management:
to reflect on the configuration of the structures and to define the future organization;
to find its own project management logic for the project that needs to be elaborated.
➢ Third stage: Implementing the project to move towards a new hospital
governance
In this third stage, the configuration of the new structures and the premises of
their proper functioning will materialize. It should lead, through the coordination of
all stakeholders, to achieving the objectives proposed in the second stage. The role
of proximity governance is fundamental for the positioning of health professionals in
an interface with various decision logics outlined in the hospital's overall governance.
The implementation of the project to move towards a new hospital governance
requires three clearly outlined responsibilities:
• Appropriate organizational culture. Implementation requires a culture that values
achievements, discipline and workmanship in multidisciplinary and/or
transdisciplinary teams.
• Leadership. It is the engine that drives the organization, which must call to actions
(practices) that make a strategy work.
• Control, feedback and adjustment mechanisms. Strategy implementation processes
support the change and adjustment of the hospital. A functioning strategy needs
performance feedback.
The implementation of the new clinical governance will translate into structural,
organizational and cultural changes.
The benchmarks proposed in this chapter are, for the stakeholders involved, the silver
lining of an approach that highlights the problem questions that are being asked. Our
proposals include the paths of reflection on practices –that could be relied on, in a
synergy, for the success of project implementation.
Clinical governance is a strategic and management approach where the human factor
is the essential building block and major challenge in the success of this desired
reform. It opens up the perspectives of a collective and shared steering, thus fostering
the quality of listening to each other, a cohesion in the attempt of a medical,
healthcare, management, and technical approach.
GENERAL CONCLUSIONS
Hospital reform needs the support of a strong human resource management. And the
involvement of the Human Resources Division will be amplified, as this is called upon to
participate in the design of the organizational strategy (of the hospital).
The subject of modernizing the human resources policy in public health
institutions is part of an evolving general context characterized by a series of
challenges7P:
• to respond to new patient expectations related to the transformation of society;
• to respect patients in the health system;
• to take into account the population aging phenomenon;
• to notice and anticipate public health issues;
• to integrate the development of chronic pathologies and polypathologies;
• to adapt to scientific and technological developments;
• to develop research and innovation.
Under these circumstances, the hospital system should, at the same time, act firmly in
the spirit of a committed policy, adapt the organization of health services to reach
performance and patient safety indicators, provide an active work environment for the whole
medical staff.
Thus, the modernization of human resource management of hospitals results
from two requirements8P:
➢ to respond to the above-mentioned challenges;
7 TOUPILLIER Danielle et ZAHIEL M. (2011), Rapport sur la modernisation de la politique des resources
humaines dans les etablissements publics de santé, Centre National de Gestion des Practiciens Hospitaliers et
des Personnels de Direction de la Fonction Publique Hospitalière, Ministère du travail de l’emploi et de la santé,
p. 3. 8 Idem, pp. 3-4.
➢ to take into account and better support a series of probably unprecedented reforms and
changes, the success of which is conditioned by the mobilization of all the categories
of staff involved.
Hospitals' capacity to provide quality healthcare to all patients is primarily based on
competence, work and commitment. Major developments that have affected the functioning
of hospitals over the past two decades require a renewed approach to human resource
management. In particular, three main stakes are revealed9P:
4. evolution towards a more individualized management of skills and support for
professional pathways;
5. an approach between the constant evolution of skill needs within each hospital
department and the actual skills available in other hospitals and territories;
6. the savoir faire of human resource management policy, a key factor of the strategy
and performance of the hospital, as a whole, in particular its quality, internal
efficiency and economic performance.
With all the importance of the quality of hospital staff and in view of its central role in
stimulating a real dynamic of change towards the modernization of clinical governance, the
current situation of hospitals in Romania shows the existence of a certain dilemma.
Indeed, hospitals suffer from poor human resource efficiency and various shortcomings
and malfunctions, while poor management awareness and involvement are consistent
across most hospitals.
The main weaknesses that prevent the implementation of an efficient human
resource management are at the following levels:
➢ the human resource function, itself, through its current organization, its mission,
which is to be defined in correlation with the means available to it;
➢ the human resource management policy that is not entirely defined and remains far
from driving human resource specific processes, such as job and skill management,
recruitment, skills assessment and training;
➢ the support of human resource management through the manner of organization,
the management style, the communication, the social dialogue, the motivation
and the working conditions that do not act for all in the sense of emergence of an
efficient human resource management.
We drafted our recommendations taking into account both the legal and the
institutional framework of hospitals in Romania and the WHO guidelines validated in the
9 Ibidem, p. 64.
practice of EU countries, outlined as trends that need to be followed by countries such as
Romania, that are still in difficulty from the perspective of achieving various performance
indicators of health services that are comparable, competitive, and convergent with the levels
of countries with developed national healthcare systems.
The recommendations proposed in the last chapter of our PhD thesis are also
intended as paths to progress, having the mission to facilitate the implementation of the
principles of new clinical governance that cannot be detached from all the factors -
institutional, organizational, technical, even political - influencing the "lives" of the hospitals
(these dimensions/strategic axes are presented in Tables 6.1 - 6.3 of the last chapter).
Each of these recommendations is a strategic orientation for the function of
human resources, which needs to be revealed at the following levels: overall (the entire
hospital), services/departments, activity poles, according to the defined modernization
plan.
In a short synthesis, we structured these recommendations around three sets of
transversal clinical management needs:
4. Searching for "meaning", thus resembling the dynamics found in all complex,
public and private enterprises. The established objectives were as follows
- stakes sharing;
- association of teams;
- positioning of medical staff;
- classification of roles on a collaborative basis;
- creation of activity poles;
- adoption of work agenda of functional entities (BDs, HMCs, specialized commissions)
to create a common culture and build on shared benchmarks, tools and methods.
5. Promoting autonomy through:
- cooperation at all hospital levels (creating a collaborative space between the various
interveners in the function of human resources and ensuring a delegation of
management and power);
- encouraging the contractual and partnership approach at the various levels of the
hospital;
- intensifying the work of the functional entities and the relationship with the social
partners;
- taking into account (the response to) the need of government authorities (creating a
multidisciplinary professional network in human resource management).
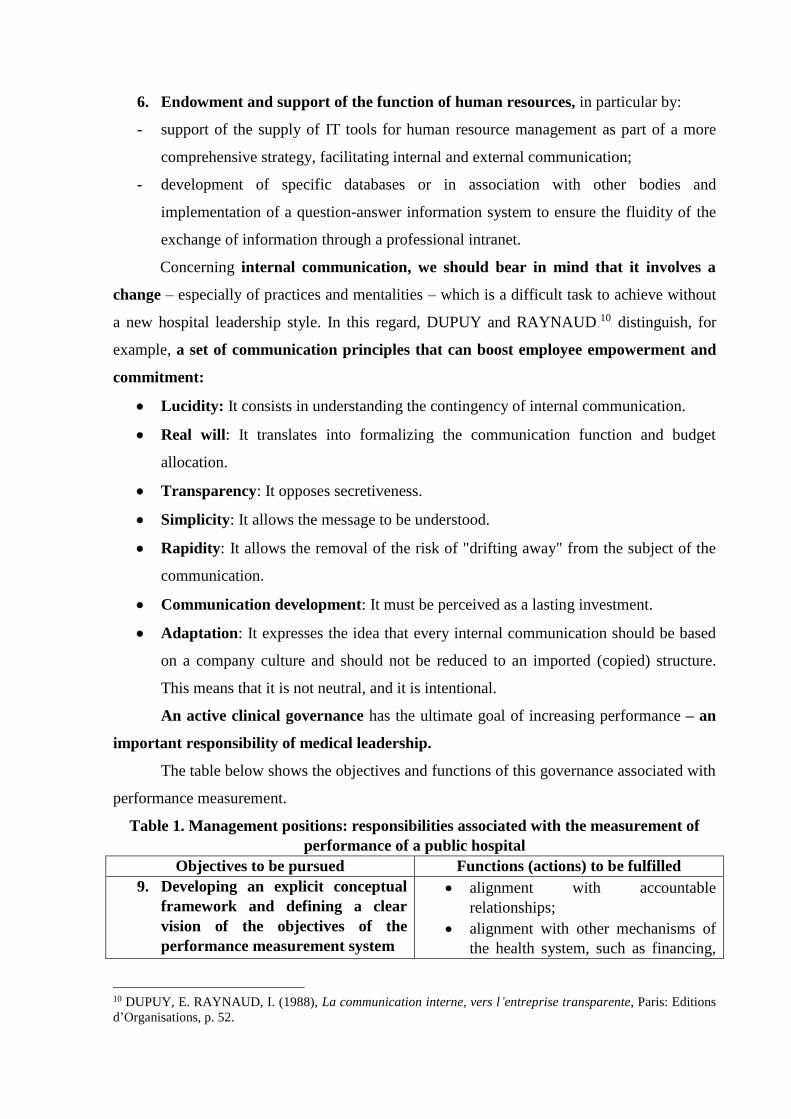
6. Endowment and support of the function of human resources, in particular by:
- support of the supply of IT tools for human resource management as part of a more
comprehensive strategy, facilitating internal and external communication;
- development of specific databases or in association with other bodies and
implementation of a question-answer information system to ensure the fluidity of the
exchange of information through a professional intranet.
Concerning internal communication, we should bear in mind that it involves a
change – especially of practices and mentalities – which is a difficult task to achieve without
a new hospital leadership style. In this regard, DUPUY and RAYNAUD P240F
10P distinguish, for
example, a set of communication principles that can boost employee empowerment and
commitment:
• Lucidity: It consists in understanding the contingency of internal communication.
• Real will: It translates into formalizing the communication function and budget
allocation.
• Transparency: It opposes secretiveness.
• Simplicity: It allows the message to be understood.
• Rapidity: It allows the removal of the risk of "drifting away" from the subject of the
communication.
• Communication development: It must be perceived as a lasting investment.
• Adaptation: It expresses the idea that every internal communication should be based
on a company culture and should not be reduced to an imported (copied) structure.
This means that it is not neutral, and it is intentional.
An active clinical governance has the ultimate goal of increasing performance – an
important responsibility of medical leadership.
The table below shows the objectives and functions of this governance associated with
performance measurement.
Table 1. Management positions: responsibilities associated with the measurement of
performance of a public hospital
Objectives to be pursued Functions (actions) to be fulfilled
9. Developing an explicit conceptual
framework and defining a clear
vision of the objectives of the
performance measurement system
• alignment with accountable
relationships;
• alignment with other mechanisms of
the health system, such as financing,
10 DUPUY, E. RAYNAUD, I. (1988), La communication interne, vers l’entreprise transparente, Paris: Editions
d’Organisations, p. 52.

trade structure and information
technologies.
10. Designing data collection
mechanisms
• detailed specification of different
indicators
• harmonization with international best
practices.
11. Information governance • data audit and quality control;
• governing people's trust in
information;
• guaranteeing a well-informed public
debate.
12. Elaboration of analysis tools and
development of analytical
capabilities to facilitate the
understanding of the data
• guaranteeing an efficient and effective
analysis;
• ensuring that decision makers
understand the analysis;
• request to put in place an appropriate
research on, for example, risk-based
adjustment, probabilities and
mechanisms for the exchange of
information.
13. Elaboration of appropriate methods
of data consolidation and
presentation:
• ensuring that information has an
appropriate impact on all
stakeholders;
• mandatory publication of
recapitulative and comparative
information (especially online on the
hospital website);
• ensuring comparability and
consistency.
14. Elaboration of incentives to ensure
continuity of performance increase
measures
• supervising the effects of
performance-related information on
staff behaviour;
• acting in a manner that favours the
synergy effect of positive results and
neutralizes unwanted consequences.
15. Adequate assessment of
performance measurement tools
• Guaranteeing a good cost-
effectiveness ratio for IT-related
expenses.
16. Management of the policy-making
process
• formulating policy choices and
ensuring their follow-up;
• encouraging a stimulating policy
debate;
• ensuring that specific interest groups
do not recover performance
information.
Source: carried out starting from the recommendations in SMITH, P. C., MOSSIALOS, E. et PAPANICOLAS
Ireme (2008), Mesure des performances pour l’amélioration des systèmes de santé : expériences, défis et
perspectives, Document de référence, OMS et OMS pour l’ Observatoire européen de systèmes et des politiques
de santé, Conférence ministérielle europeenne de l’OMS sur les systèmes de santé ,,SYSTÈMES de santè. Santé
et prosperité”, Tallinn (Estonie) 25-27 juin 2008, p. 111.
The Scientific Contributions of the PhD Thesis
1) Using a rich volume of relevant bibliographic sources authored by academic
professionals and/or notorious scholars in the international scientific community,
some of them authorized to participate in the teams of authors of studies performed
under the aegis of the WHO, the PhD thesis succeeds in putting together, in a
coherent and relevant synthesis, new ideas related to:
• organizational performance: Donabedian A., Morin E. M., Savoie A., Beaudin G.,
Paris Valérie, Allani – Soltan N., Jgalens J., Gond J. P., Le Pogam Marie-Annick,
Homby P.;
• global performance assessment framework for health services systems:
Champagne F, Contandriopoulos A. P., Touché J., Béland F., Nguyen H., Don de
Savigny, Taghreed A.;
• conceptual framework for the analysis of clinical governance in healthcare
institutions: Pomey M. P., Denis J. L., Contandriopoulos A. P.;
• human resource management: Vallejo J., Glouberman S., Minzberg H., Bareil
Céline, Guerin G., Wils Th, Storey J., Arcand M., Pigeyre F.
Obviously, the list of authors that could have been quoted is very extensive, but we
wanted to mention those who, while maintaining the requirements of epistemology, defined in
an original manner the terms and concepts of paradigm nuclei circumscribed to the research
fields they were preoccupied with.
2) The second scientific contribution brought by our PhD thesis is materializes in
the manner of dealing with the field investigated in the first four chapters, which
provide knowledge of the paradigmatic specificities of the complex field under
investigation.
3) The third contribution of our work is demonstrated by the persuasive construction
of the sixth chapter, which focuses on promoting a framework layout (Guide) for
the operation of a clinical governance modernization program.
As a synthesis, we can highlight the value of the contributions of our PhD thesis on
three levels:
• epistemological: defining the paradigm concepts of global governance and proximity
governance of clinical establishments;
• operational: designing the methodological framework for the elaboration of a hospital
management modernization strategy;
• human resource training: the need to train competent managers, leaders perceived
by their teams as carriers of meaning capable to direct them towards clear and
stimulating goals.
THE LIMITATIONS OF OUR SCIENTIFIC RESEARCH
Of course, our scientific research paper has its limits both in terms of theory and
methodology, and in terms of conclusions.
• Thus, one such limitation relates to the boundaries of our research, which for
objective reasons have been reduced a lot (lack of data in particular).
• Another limitation refers to our field investigation portfolio because we could not
have access to target analysis entities (hospitals). Our attempts to carry out the survey
in a number of public hospitals (object of chapter 5) failed due to the reservations of
the decision-makers of the potential hospitals concerned (in the city of Bucharest).
• Another limitation is related to the absence of researchers targeting human
resource management in the healthcare institutions in Romania.
• Last but not least, one limitation concerns the impediments (obstacles) that render
impossible and/or restrict the analyses and assessments that are required in
finding the weaknesses in human resource management: the lack of data, the
limiting IT system, the lack of references and scientific research papers on clinical
governance in Romania.
RESEARCH PERSPECTIVES
The author's preoccupations with the research theme were a constant motivation for
personal development intended to provide her with the necessary professional skills in a
future perspective of involvement in the management of a healthcare facility, possibly created
through her own investments.

Managing a hospital (or a polyclinic) undoubtedly requires the development of skills
related to the management functions in today's contextual settings of healthcare facilities in
order to identify the issues and challenges that are relevant to the management plan. To this
end, by deepening the research initiated during the drafting of my PhD thesis, I intend to
conduct an exploratory study on the evolution and progress of the Turkish hospital network
(especially the private one) to identify the solutions which can be implemented in Romania.
BIBLIOGRAPHY
1. ABBAD, J. (2001), Organisation et management hospitalier, Paris: Berger –
Levrault.
2. ACADEMIA ROMANA, Institutul de lingvistică „Iorgu Iordan”, Dicţionarul
explicativ al limbii române (DEX), (1998), Bucureşti: Editura Universul
enciclopedic.
3. ALTER, N. (1998), Organisation et innovation: une rencontre conflictuelle,
Sciences Humaines, No 20, mars /avril 1998, pp. 56-59.
4. ANHOURY, P. et VIENS, G. (coord.), (1994), Gérer la qualité et les risques à
l’hôpital, Paris: ESF Éditeurs.
5. ALLANI-SOLTAN, N. (2003), L’effet des pratiques de gestion des ressources
humaines sur la performance des entreprises française, Thèse de doctorat,
Université Nancy 2, sursa citată în BERNARD Manon (2009).
6. ARAH, O.A., KLAZINGA, N.S., DELNOIJ, D.M.J., TEN ASBROEK, A.H.A.,
CUSTER, T. (2003), Conceptual frameworks for health systems performance: a
quest for effectiveness, quality, and improvement, International jornal for quality in
health care, vol.15, no 5.
7. ARCAND, M. (2000), L’effet des pratiques de gestion des ressources humaines sur
l’efficacitéde caisses populaires Desjardins du Québec, Thése de doctorat,
Université de Metz.
8. ARNAUD, J-O et BARSACQ, G. (1989), La dynamisation des ressources
humaines à l’hôpital, Paris, Gérer la santé, Edition ESF.
9. ARROW, K.J. (1963), Uncertainty and the Welfare Economics of Medical Care,
American Economic Review, 53 (5), pp.941-973.
10. BANCA MONDIALĂ ȘI GUVERNUL ROMÂNIEI (2011-2012), Analiza
Funcţională a Sectorului Sănătate în România, proiect cofinanţat din Fondul Social
European, prin Programul Operaţional Dezvoltarea Capacităţii Administrative,
sgg.gov.ro/File/UPP/doc/rapoarte-finale-bm/.../MS-RO-FR-Health-Sector-ROM.
11. BAREIL Céline et al., (2002), Les pratiques renouvelées de gestion des ressources
humaines dans le réseau montréalais de la santé et des services sociaux, Gestion,
2002/3 vol.27, pp.64-73.
12. BATAL, C. (2000), La gestion des ressources humaines dans le secteur public,
tome I, Paris : Edition Organisation.
13. BAYAD, M., ARCAND, G., ARCAND, M., ALLANI, N. (2004), Gestion
stratégique des ressources humaines : fondaments et modèles, Revue international
des relations de travail, janvier, vol. 2, no 1, pp. 76-77.
14. BEAUBEAU, D. et PEREIRA, C., (2003), Mesure de la performance dans le
domain de la santé, Présentation au 10-ième Colloque de compatibilé Nationale,
Paris: 22 janvier 2004.
15. BENAMOUZIG, D. (2005), La santé au miroir de l’économie, Paris: PUF.
16. BENETT, S., FRANCO, L.M. (1999), Public sector health worker motivation and
health sector reform: a conceptual framework, Bethesda, Maryland (SUA), Abt
Associates Inc. for Partnerships for health Reform Project (Major Applied Research
5, Technical Paper 1).
17. BERNARD Manon, (2009), L’effet des pratiques de ressources humaines sur la
performance sociale des employés dans le context de culture national, Thése de
doctorat en Science de Gestion, Université de Strasbourg, scd-these.u-
strasbg.fr/view/name/Bernard_Manon.html.
18. BJÖRNBERG, A. (2018), Health Consumer Powerhouse (HCP), Euro Health
Consumers Index 2017, Report, 1TUwww.heathpowerhouse.com/publications/euro-
health-index-2016/U1T.
19. BLUM, H.L.(1981), Planning for Health, generis for the Eighties, Londre: Human
sciences press.
20. BOLAND, T. and FOWLER, A. (2000), A Systems Perspective of Performance
management in Public Sector Organisations, Int J Public Sector Manag 13, pp.417-
446.
21. BOURDIEU, P., WACQUANT, L.J.D.(1992), Réponses pour une anthropologie
réflexive, Paris: Seuil.
22. BOURGUEIL, Y., MAREK, A., MOUSQUES, J. (2009), Trois modèles types
dîorganisation des soins primaires en Europe, au Canada, en Australie et en
Nouvelle Zélande, Questions d’économie de la Santé no 141-Avril 2009, IRDES
(Institut de Recherche et de Documentation en Economie de la Santé),
1TUhttp://www.irdes.fr/Publications/Qes/Qes141.pdfU
23. BOUSSARD Valérie (2013), Travail d’organisation gestionnaire des cadres et
mutation des entreprise publiques, La nouvelle revue du travail, 2013/2.
24. BUDET, J-M. (2001), Contractualisation interne: le cadre juridique, Gestion
Hospitalières. août – septembre 2001, No 167.
25. CANADIAN INSTITUTE FOR HEALTH INFORMATION, STATISTICS
CANADA (2000), Canadian Health Information Roadmap Initiative Indicators
Framework, Otawa: Canadian Institute for Health Information.
26. CANGUILHEM, G. (1966), Le normal et le pathologique, Paris, Quadrige, PUF.
27. CEBOLLA Beatriz (director de proiect), Etude menée par l’UE sur les maladies du
coeur (2016), Communiqué de presse: Euro Heart Index 2016,
1TUwww.healthpowerhouse.com/publications/euro/heart-index--2016U1T.
28. CERTO, S. C. (2002), Management modern, Diversitatea, calitatea, etica și mediul
global, București : Editura Teora.
29. CHAMBARETAUD Sandrine et HARTMANN Laurence (2004), Économie de la
santé : avancées théoretique et opérationnelles, Revue l’OFCE.
30. CHAMPAGNE, F., CONTANDRIOPOULOS, A.P., PICOT-TOUCHÉ JULIE,
BÉLAND, F. et NGUYEN, H. (2005), Un cadre d’évaluation de la performance des
systèmes de service de santé: le modèle EGIPSS (Évaluation globale et intégrée de
la performance des systèmes de santé), Université de Montréal, p.28.
31. CHAMPAGNE, F., CONTANDRIOPOULOS, A-P., DENIS, JL, LAMOTHE, L.,
(2002) Les centres universitaires de santé. La gouverne d’organisations complexe
aux contours flours. Document de travail préparé par la Département
d’Administration de la santé et le Groupe de recherche interdisciplinaire en santé,
Montréal, Université de Montréal.
32. CHAMPAGNE, F., CONTANDRIOPOULOS, A-P., TOUCHÉ, J., BÉLAND, F. et
NGUYEN, H. (2005), Un cadre d’évaluation globale de la performance des
systèmes de services de santé: Le modèle EGIPSS, Rapport de recherche, Group de
recherche interdisciplinaire en santé, Université de Montréal,
1TUhttp://www.csbe.gouv.qc.ca/.../Conseil SanteBienEntre/.../200U1T...
33. CIOCOUREL, A. (2002), Le raisonnement médical, une approche socio-cognitive,
Paris, Seuil.
34. CONTANDRIOPOULOS, S, A.-P. (2008), La gouvernance dans le domaine de la
santé: une régulaton orientée par la performance, Santé Publique, 2008/2, Vol. 20,
pp. 191-199, 1TUhttps://www.cairn.info/revue-sante-publique-2008-2-page-191.htmU1T
35. CONTANDRIOPOULOS, A.-P. & SOUTEYRAND, Y., éds (1996), L’hôpital
stratège: dinamiques locales et offre de soins, Paris: John Libbey Eurotext.
36. CONTANDRIOPOULOS, A.-P., CHAMPAGNE, F., DENIS, J.-L., AVERGUES,
M.C. (2000), L’évaluation dans le domaine de santé: concepts et méthodes, Revue
d’épidemologie et de santé publiques 2000, nov.48 (6), pp.517-539.
37. CONTANDRIOPOULOS, A.P., DENIS, J.L., TOUATI NASSERE, RODRIGUES,
R., (2001) Intégration des soins: Ruptures, revue transdisciplinaire en santé, vol. 8,
no2, 2001.
38. CONSILIUL JUDEŢEAN BUZĂU, (2016), Planul strategic al Spitalului Judeţean
de Urgenţă Buzău pentru perioada 2016-2020
39. CROZET, P., KAANICHE Asma et LIENARD J. (2008), Nouvelle gouvernance à
l’hôpital: recomposition de l’organisation et gestion des ressources humaines, revue
Politiques et management public, Vol. 26/2/2008.
40. CROZIER, M., SERIEYX, H., (1994), Du management panique à l’entreprise du
21ème siècle, Maxima.
41. CUCU Maria Alexandra (coord.), (2016), Raportul naţional al stării de sănătate a
populaţiei, Ministerul Sănătăţii, Institutul Naţional de Sănătate Publică, Centrul
Naţional de Evaluare şi Promovare a Stării de Sănătate.
42. DAHLGREN, G. & WHITEHEAD, M. (1991), What can we do about inequalities
in health, The lancet, no 338, pp.1059-1063
43. DAVIES, P. (2001), Stewardship: wat is it and kow can measure it? Presentation to
meeting on Health economics in developing and transitional countries: the
changing role of the state, Departament for International Development, York United
Kingdom, 26 July 2001.
44. DELOITTE, (2010), L’hôpital au coeur des réformes du système de santé. Réussir
sa transformation, Health Workforce Department World Health Organization,
Geneva 1TUwww.who.int/hrh.
45. DERVAUX Amélie, PICHAULT, Fr. și RENIERNathalie (2011), L’apport de la
théorie de l’acteur-réseau à la professionnalisation de la GRH en milieu hospitalier,
Journal d’Economie Médicale, nP
oP 1-2, vol. 29, pp. 62-73, Eska, Paris.
46. DESMIDT, S. and HEENE, A. (2006), Strategie en Organisatie van Publieke
Organisaties, Lannoo : Tielt.
47. DEVER, CHAMPAGNE, F. (1984), Epidemiology in Health Services Management,
Germantown, Maryland.
48. DIETRICH, A., PIGEYRE, F. (2005), La gestion des Ressources Humaines, Paris:
La Découverte, Coll. Repères.
49. DON DE SAVIGNY et TAGHREED, A. (ed) (2009), Pour une approche
systémique du renforcement des systèmes de santé, Alliance pour la recherche de
santé-OMS, 1TUhttp://www.who.int/alliance-hpsrU1T.
50. DONABEDIAN, A. (1966), Evaluating the Quality of Medical Care, The Milbank
Quaterly 44, pp. 166-203.
51. DONABEDIAN, A. (1978), The quality of medical care, Science 200 (4344),
pp.856-864.
52. DONABEDIAN, A. (1980), The definition of quality and approaches to its
assessment, Health Administration Press.
53. DORÉ Anne-Marie (coord) (2006), Encadrement et nouvelle gouvernance à
l’hôpital. Guide méthodologique, Ministère de la Santé et des Solidarités (France).
54. EVANS, R.G., BARER, M., MARMOR, T. (Eds) (1996), Être ou ne pas être en
bonne santé: biologie et déterminants sociaux de la maladie, Paris: John Libby
Eurotext.
55. FORUM NATIONAL sur la SANTÉ (1997), La santé au Canada: un héritage à
faire fructifier, Ottawa: Gouvernement du Canada.
56. FREIDBERG, E. (1993), Le pouvoir et la règle , Paris: Seuil.
57. FRIEDMAN, D. J., HUNTER, E. L. and PARRSH, R. G., (2002), Shaping a Health
Statistics Vision for the 21 st Century, Final Report November, 2002, [s.l], Centers
for sisease Control and Prevention, National Committee on Vital and Health
Statistics.
58. GALAMBAUD, B., LEON, E. (2008), Le sens de la mesure, le cas de la
performance en gestion des ressources humaines, Revue Gestion, Vol. 33, no.2.
59. GHEORGHE, A. (2012), Reforma spitalelor publice – evidenţe din spaţiul
european, Seria „Policy reports”, pp.8-12, Bucureşti: Observatorul Român de
Sănătate.
60. GHRISSI, M. L. (2011/2012), Le management des ressources humaines dans
l’hôpital public, CAS:CHU D’Oran, Thèse de doctorate en science, Faculté des
science économiques, des sciences de gestion et dans sciences commerciales.
61. GIRAUD Françoise, SAULPIC, O., BONNIER Carole, FOURCADE, F. (2008),
Contrôle de Gestion et Pilotage de la Performance, Paris : Gualino éditeur.
62. GIRAUD, F., SAULPIC, O., NAULLEAU, G., DELMOND, M-H., BESCOS, P-L.
(2004), Contrôle de gestion et pilotage de la performance, 2e édition, Collection
Business, Paris: Gualino éditeur.
63. GLOUBERMAN, S et MINZBERG, H. (2001), Managing the care health and the
cure of disease-PartI: Differentiation, Health care Management Review, vol. 26, no
1, pp.56-69.
64. GUERIN, G. et WILS, TH., (2002), La gestion stratégique de ressources humaines,
Gestion, 2002/2 vol..27, pp.14-23.
65. GUISSET Ann-Lise, SICOTTE, C., LECLERCQ, P., D’HOORE, W., (2002),
Définition de la performance hospitalière: une enquěte auprès des divers acteurs
stratégiques au sein hôpitaux, Sciences sociales et santé, 2002, Volume 20, numero
2, pp. 65-104.
66. HALL, T.L., MEJIA, A. (1979), La planification des personnels de santé: principes,
méthodes, problèmes, Genève, Organisation mondiale de la santé, sursă citată în
OMS (2006).
67. HAS (Haute Autorité de Santé-Franţa) (2009), Rapport d’évaluation. Le recours à
l’hôpital en Europe. Argumentaire, HAS/Service évaluation économique et santé
publique, Mars 2009, 1TUwww.has-sante.frU1T
68. HATCHUEL, A. (2000), Perspective et gouvernance: quelle théorie de l’action
collective?, en HEURGON, E.,, LANDRIEU, J. (sous la direction de), Perspective
pour une gouvernance démocratique, Paris, Éditions Aube, 2000.
69. HEALY, J&MCKEE, M (2002), Implementing hospital reform in central and
eastern Europe, Health Policy, vol. 61.no.1, pp.1-19;
70. HERREROS, G., (1996), Changements, pouvoirs et logiques d’action à l’hôpital,
Gestions hospitalières, Décembre 1996.
71. HOWLET, M. et. al. (2009), Studying Public Policy, New York, Oxford University
Press.
72. 1THOOD, Ch. (1991), A Public Management for All Seasons, Public Administration,
69 (1), pp. 3-19.
73. 1THOMBY, P., FORTE, P. (2002), Human resource indicators health service
performance, Keele (Royaume –Uni), Keele University, Centre for Health Planning
and Management.
74. HOLDEN, R.R., MAGRUDER, C.D., STEIN, S.J., SITARENIOS, G., SHELDON,
S. (1999), The effects of anonymity on the Holden Psychological Screening
Inventory, Personality and Individual Differences, 27, pp. 737-742.
75. 1THREBINIAK, L. G. (2009), Strategia în afaceri. Implementarea și executarea
eficientă, traducere CRISTEA Gabriela Camelia, bucurești, Editura ALL.
76. HURST, J., JEE-HUGHES, M. (2001), Performance Measurement and
Performance Management in OECD Health Systems, OECD, Labour market and
social policy, occasional papers nP
oP 47.
77. IGALENS, J., GOND, J.P., (2003), La mesure de la performance sociale de
l’entreprise: une analyse critique et empirique des données. Arese, Revue de Gestion
des ressources humaines, no 50, oct.-déc., pp. 111-129.
78. IGALENS, J., ROUSSEL, P. (1998), Méthodes de recherche en Gestion des
Ressources Humaines, Paris: Editions Economica, Collection Recherche en Gestion.
79. INSTITUTE OF MANAGEMENT ACCOUNTANTS AND ANDERSEN, A.
(1998), Tools and Techniques for Implementing Integrated Performance
Measurement Systems: Statement pn Management Accounting 4DD. Montvale, NJ.
80. IREF (Institut de recherches économique et la concurrence fiscale) (2017),
L’efficacité des systèmes publiques de santé europeens. Mieux vaut la concurrence
que le monopole, 1TUhttp://fr.irefeurope.org/Publications/INDEX-de-l-efficacite-de-la-
depense-publique/L-efficacite-des-systemes-publique-desante-europeensU1T
81. JAQUES, Jessica., (2012-2013), Indicateurs de performance clinique
hospitalière.Etudes empiriques basée sur les données medico-administratives
belges, Thèse présentée en vue de l’obtention du grade de docteur en sciences de la
santé publique, Université de Liege.
82. JUILLIARD – FOURNIER Nadine (2002), L’Hôpital organisé en pôles d’activités.
Perspectives et enjeux pour le directeur des soins, Mèmoire de l’École Nationale de
la Santé Publique, École Nationale de la Santé Publique (ENSP), Rennes.
83. KADDAR, M., (2004), Economie de la santé: brève introduction,
1TUwww.santemaghreb.com/algerie/comptes_/_rendus/jnp_200411/jour1_1_kaddar.pdfU1T
84. KESLEY, T. (2001), Améliorer la qualité des soins, în L’observateur de l’OCDE,
nr.229, Royaume Uni, Novembre, 2001.
85. KRIEGER, N. (2008), Ladders, pyramids and champagne: the iconography of
health inequities, Journal of Epidemiology and Community Health, 62 (12),
pp.1098-1104
86. LALONDE, M. (1981), Nouvelle perspective de la santé des Canadiens,
Gouvernement du Canada.
87. LAWRENCE, P.R., LORSCH, J.W. (1989), Adapter les structures de l’entreprise,
intégration au différenciation, Paris: Les éditions d’organisation.

88. LE POGAM Marrie-Annick, LUANGSAY-Catelin, NOTEBAERT, J.-F., (2009),
La performance hospitaliére : à la recherche d’un modèle multidimensionnel
cohérent, Management&Avenir 2009/5 (nP
oP 25), https://www.cairininfo/revue-
management-et-avenir-2009-5-page-116.htm.
89. LEATHERMAN, S. (2001), Être à la hauteur: mesurer et améliorer la performance
des systèmes de la santé dans les pays de l’OCDE, Extrait de la conférance
organisée par l’OCDE et le Canada-OCDE, Novembre.
90. LEATHERMAN, S. (2002), Utiliser les indicateurs de performance pour améliorer
les systèmes de santé dans les pays de l’OCDE, chapitre 15 en Smith, P. (éditeur)
(2002), Être à la hauteur. Mesurer et améliorer la performance des systémes de santé
dans les pays de l’OCDE, OCDE: Santé Canada,
https://books.google.ro/books?/slow=9266429595X..
91. LEGUELINEL Géraldine (2017), Initiation à l’économie de la santé, CHU Nimes,
Université de Montpellier,
1TUhttps://moodle.umontpellier.fr./.../DFGSP2_UE6_Initiation_P U1T...
92. LEVESQUE, J.F. et BERGERON, P. (2003), De l’individuel au collectif: une vision
décloisonnée de la santé publique et des soins, Ruptures, 9:2, pp.73-89.
93. LETHIELLEUX, L. (2014), L’essentiel de la gestion des ressources humaines
2014-2015, 8P
eP édition, Paris : Gualino Éditeur.
94. LOMBRAIL, P., NAIDITCH, D. and CUNEO, P. (1999), Les éléments de la
performance hospitatalière. Les conditions d’une comparaison, Etudes et résultats,
DREES 42, pp.1-8.
95. MACINKO, J., STARFIELD, B., SHI, L. (2003), The contribution of primary care
systems to health outcomes within Organization for Economic Cooperation and
development (OECD) countries, 1970-1998, Health Services Research, 2003; 38, 3,
pp. 831-865.
96. MARABET, M. (2018), Définitions, approches et concepts en santé publique, Notes
de cours santé publique Master USSAE.
Ufmp.um5.ac.ma/.../Définition%2C20concept%2C20approches%20en%20santé.pdf.
97. MARTY, C. et MERLIN, H, (2007), Mesurer la performance des hôpiteaux public
en France. Fundements méthodologique d’un modèle d’evaluation, enjeux, HEC
Paris, Observatoire du Manangement Alternatif, Cahier de resherche,
1TUhttp://creativecommons.org./licenses/by/2.0/frU1T.
98. MELIS, R.J., OLDE RIKKERT, M.G., PARKER, S.G., VAN EIJKEN, M.I.,
(2004), What is intermediate care?, BMJ 2004, 329 (7462).
99. MINISTERE DE LA SANTÉ ET DES SERVICES SOCIAUX (2007), Cadre
d’orientation por le développement et l’évolution de la fonction de surveillance au
Québec, Gouvernement de Québec.
100. MINISTERE DE LA SANTÉ ET DES SERVICES SOCIAUX DU QUEBEC
(2010), Cadre conceptuel de la santé et ses déterminants. Résultat d’une réflexion
commune, version mars 2010, 1TUhttp://intranetreseau.rtss.qc.caU
101. MINISTERE DE LA SANTÉ ET DES SERVICES SOCIAUX ET INSTITUT
NATIONAL DE SANTE PUBLIQUE DU QUEBEC (2005), Plan commun de
surveillance de l’état de santé de la population et de ses déterminants 2004-207,
Parte I: Cadre de référence, Québec, Gouvernement de Québec. février.
102. MINISTERUL SĂNĂTĂŢII (2014), Strategia Naţională de Sănătate 2014-2020.
Sănătate pentru prosperitate, Ministerul Sănătăţii, Bucureşti,
1TUhttp://www.ro/documente/Anexă%201%20-
%20Strategia%Naţională%20de%20Sănătate_886_1761.pdfU
103. MINISTERUL SĂNĂTĂŢII (2011), Ordin metodologic al ministrului sănătăţii.
104. MINISTERUL SĂNĂTĂȚII, Legea nr. 95 din 14 aprilie 2006 privind reforma din
domeniul sănătății, Republicată în temeiul ar. VI din Legea 184/2015 privind
aprobarea Ordonanței de urgență a Guvernului (OUG) nr. 77/2011 privind stabilirea
unor contribuții pentru finanțarea unor cheltuieli în domeniul sănătății precum și
pentru modificarea și completarea Legii nr. 95/2006 privind reforma în domeniul
sănătății. Cu modificările aduse de: Legea nr. 2 din 12 ianuarie 2017 pentru
modificarea Legii nr 95/2006 privind reforma în domeniul sănătății; Legea nr. 185
din 24 iulie 2017 privind asigurarea calității sistemului de sănătate.
105. MINTZBERG, H. (2008), Ascensiunea și declinul planificării strategice, București,
Editura Publică.
106. MINVIELLE, E. (2000), Réconcillier standardisation et singularité: les enjeux de
l’organisation de la prise en charge des malades, Rupture, revue trandisciplinaire en
santé, 2000, (7), pp. 8-22.
107. MOISDON. J. C. (2008), Gouvernance clinique et organisation des processus de
soins : un chrainon manquant ?
108. MOISDON, J. C., TONNEAU, D. (1999), La démarche gestionnaire à l’hôpital,
tome 1 recherche sur la gestion interne, Seli Arshan.
109. MORIN, E.M., SAVOIE, A., BEAUDIN, G. (1994), L’efficacité de
l’organisation.Théorie, représentations et mesures,Gaétan Morin Éditeur.
110. MORIN, M. (2006), Nouvelles définitions de la santé: un regard psychosocial,
Spirale 2006/1, (no 37), 1TUhttps://www.cairn.info/revue_spirale/2006/1/page/29.htmU1T
111. MORISSON, V., GAGNON, F., MORESTIN FLORENCE et KEELING, M.
(2014), Mots-clés du domaine des politiques publiques favorables à la santé,
Rapport Centre de Collaboration nationale sur les politiques publiques et la santé,
Institut national de santé publique Québec, 1TUwww.ccnpps.ca.
112. MORTEN BALLE, H et al., (2013), la nouveau management public, les marchés
bureau critiques et les problèmes de coordination interdépartamentale : analyse
comparative de la haute fonction publique dans l’administration de l’Etat, Revue
Internationale des sciences Administratives, 2013/I, Vol. 79, pp. 31-51.
113. NICOLESCU, O., VERBONCU, I. (1996), Management, București, Editura
Economică.
114. New Zealand Ministry of Health (2003), Improving Quality (IQ): A systems
approach for the New Zealand Health and Disability Sector.
115. NOBRE, Th. (1999), L’hôpital:le modéle de la bureucratie professionnelle revisté à
partir de l’analyse du coût des dysfoncyionnements, Manuscrit auteur, publié dans
20ÉME CONGRES DE L’AFC, France, 1999, (halshs-00587813, version 1-21 Apr
2011).
116. NUTLEY, S. et SMITH, P.C. (1998), League Tables for performance improvement
in health care, Journal of Health Serv, Res. Policy, vol.3, no.1, pp.50-57, Janvier.
117. OCDE (1990), Les systèmes de santé, Paris: OCDE.
118. OECD (2010), Améliorer la performance des soins de santé: comment mesurer leur
qualité, Forum sur la qualité des soins, Paris, 7.8 octobre 2010.
119. OECD (2010), Systèmes de santé. Efficacité et politiques, Paris: OECD
120. OECD/European Observatory on Health Systems and Policies (2017), România:
Profilul Sănătăţii în 2017, State of Health in the EU,
1TUhttp://dx.doi.org/101787/9789264285392-roU1T
121. OGIEN, A. (2000), Médecine, santé et gestion, in Cresson et F. – X., SCHWEYER
(sous la direction de ) Professions et institutions de santé face à l’organisation du
travail. Aspects sociologiques, Éditions de l’ENSP, Revues, 2000, pp. 133-148.

122. OMS, Préambule à la Constitution de l’Organisation mondiale de la Santé,
adoptată de Conférance internationale sur la santé, New York, 19 juin-22 juillet
1946, et entré en vigueur de 7 avril 1948, http//www.who.int.
123. OMS, Bureau régional pour l’Europe, (1984), Health Promotion:A discussion
document on the concept and principtes, Copenhague, http//www.who.int.
124. OMS (1998), Glossaire de la promotion de la santé, Division de la promotion de la
communication pour la santé, service éducation sanitaire et promotion de la santé,
Genève, 1TUhttp://whqlibdoc.who.int/hq(1998)/WHO_MPR_HEP_98.1_fre.pdfU1T
125. OMS (2000), Le rapport sur la santé dans le monde, 2000, Genève,
http//www.who.int
126. OMS (2000), The World Health Report 2000, Health systems: Improving
performance, Geneva, http//www.who.int.
127. OMS (2003), Health Systems Performance Assessment Debates, Methods and
Empiricism, http//www.who.int.
128. OMS - Bureau régional de l’OMS de l'Europe, (2005), Des systèmes de santé
renforces sauvent plus vies: un aperçu de la stratégie européenne de l’ OMS en
matière de systèmes de santé, Copenhague, http//www.euro.who.int.
129. OMS (2006), Rapport sur la santé dans le monde 2006: travailler ensemble pour la
santé, [email protected].
130. OMS (2007), Everybody’s Business: Strengthening Health Systems to Improve
Health Outcomes: Who’s Framework for Action, Genève, OMS, http//www.who.int.
131. OMS (2008), La Charte de Tallin: des systèmes de la santé pour la santé et la
prospérité, Copenhague,
1TUhttp://www.euro.who.int/_data/assets/pdf_file/0008/88604/E91439.pdfU1T
132. OMS (2008), Les soins de santé primaires – Maintenant plus que jamais,
Rapport sur la santé dans le monde, Uhttp:www.who.int/whr/2008/fr/index.html
133. OMS – Bureau régional de l”OMS de l”Europe, (2008), Direction et
guvernance des systèmes de santé dans la Région européenne de l”OMS, Comité
régional de l”Europe, Cinquante–hutième session, Tibilisi (Géorge), 15-18
septembre 2008, p. 4, 1TUhttp://www.euro.who.intU1T.
134. OMS (Bureau régional de l’Europe), (2010), Relever les principaux défi de la santé
publique et de la politique sanitaire en Europe: Progresser dans la recherche de
l’amélioration de la santé dans la Région européenne de l’OMS, Comité régional de
l’Europe, Soixantième session, Moscov, 13-16 septembre 2010,
http :Uwww.euro.who.int
135. OMS-Bureau régional de l’Europe (2011), Renforcement des capacités et services
de santé publique en Europe: cadre d’action, Comité régional de l’Europe,
Soixante et unième session, Bakou (Azerbaidjan), 12-15 septembre,
1TUhttp://www.euro.who.int/fr/who-we-are/gouvernanceU1T
136. OMS-Commission sur les déterminants sociaux de la santé,
1TUhttp://www.who.int/social_determinants/fr/U1T.
137. Ordinul Ministerului Sănătății 914 din 26 iulie 2006 pentru aprobarea normelor
privind condițiile pe care trebuie să le îndeplinească un spital în vederea obținerii
autorizației sanitare de funcționare, Anexa 3.
138. PARIS Valérie (2012), Le performances comparées des systèmes de santé, Les
Tribunes de la santé 2012/2(nP
oP35), https://www.cairn.info/revue-les-tribunes-de-la-
sante-2012-2-page-43.htm
139. PARSONS, T. (1977), Social systems and the evolution of action theory, New York,
NY: Free Press.
140. PAULHUS, D.L., (1991), measurement and control response bias, In: Robinson J.P.
141. PELJAK, D. (1997), Le management de subsidiarité au service de hôpitaux in
Gestions Hospitalièrea, juin-juillet.
142. PERETTI, J. M. (2012), Gestion des ressources humaines, 18P
eP édition, Paris :
Vuibert.
143. PETRELLA, R. (1996), Le bien commun, Brusselle: Labor.
144. PETRESCU I. (2003), Managementul personalului organizației, București : Editura
Expert.
145. PETRESCU M., STEGĂROIU, I., NĂBÂRJOIU N., DUICĂ A., DUICĂ M. C.,
POPA E., (2010), Managementul schimbării și riscului, Târgoviște : Editura
Bibliotheca.
146. PICHAULT, Fr. et NIZET, J. (2000), Les pratiques de gestion des ressources
humaines, Coll. Point/Inédit/Essais, editions du Seuil, Paris.
147. PIGEYRE, F., (2006), Les modèles d’analyse de la GRH, en Ministère Éducation
Nationale Enseignement Supérieur Recherche, Éduscol, les actes de la DGESCO,
Management et gestion des ressources humaines: stratégies, acteurs et pratiques,
Actes du séminaire national 23-26 août 2005, Cité internationale universitaire, Paris,
pp.7-16., eduscol.education.fr./D0033/, p.14.
148. POMEY, M. P., DENIS, J. L., CONTANDRIOPOULOS, A. P. (2008), Un cadre
conceptuel de l’analyse de la gouvernance clinique dans les établissements de santé,
Pratiques et Organisation des Soins, Revue trimestrielle, vol. 39 – no 3/, juilet –
september 2008.
149. RECHEL, B., McKee., (2009), Health reform in central and eastern Europe and the
former Soviet Union, The Lancet, vol. 374, no. 9696, pp. 1186-1195
150. RÉFIPS (Réseau francophone international pour la promotion de la santé), section
des Amériques (le „site web”) (2012), Déterminants sociaux de la santé. Cadres
théoriques.
151. REICH M.R. (2002) Reshaping the state from above, from within, from below:
Implications for public health, Social Science and Medicine 54, pp. 1669-1675.
152. RENAUT, L. (1999), Etude de la satisfaction des usages: De la mesure de
satisfaction...A l’amélioration de la qualité au Centre Hospitalier de Sens, Memoire
de l’Ecôle National de la Santé Publique,
1TUhttp://documentation.ehesp.fr/memoires/1999/edh/renant.pdfU
153. RISTEA Ana-Lucia, IOAN-FRANC, V., POPESCU Constanța, (2017), Metodică în
cercetarea științifică, Ediția a doua revizuită și adăugită, București : Editura Expert.
154. ROCHER, G. (1972), Talcott Parsons et la sociologie américaine, Paris: P.U.F.
155. SAINSAULIEU, I. (2006), La communanté de soins en question. Le travail
hospitalier face aux enjeux de la societé, Paris: Éditions Lamarre.
156. SALTMAN R.B., FERROUSSIER-DAVIS O., (2000), The concept of stewardship
in health policy. Bulletin of the World Health Organization 78 (6), pp. 732-739.
157. SHAVER, P.T., WRIGHTSMAN, L.S., eds., Measures of personality and social
psychological attitudes, San Diego, Academic Press, pp. 17-59.
158. SEGADE, J. P. (2000), La contractualisation à l’hôpital, Paris : Ed.
Elsevier/Masson.
159. SICOTTE, C., CHAMPAGNE, F., CONTANDRIOPOULOS, A.C. (1999), La
performance organisationnelle des organismes publics de santé, Rupture-Revue
trandisciplinaire en santé, vol.6, no 1, pp.34-36.
160. SICOTTE, C., CHAMPAGNE, F., CONTANDRIOPOULOS, A.P., BARNSLEY,
J. et al., (1998), A conceptual framework for analysis of health care organizations
performance, Health Services Management research, 1998, 11, pp. 24-48.
161. SOLAR, O., IRVIN A. (2011), A conceptual framework for action on the social
determinants of health. Social determinants of Health, Discussion Paper 2 (Pollicy
and practice), 1TUhttp://www.who.int/social determinants/fr/index.htmlU1T
162. STEINER, A. (2001), Intermediate care ...a good thing? Age Ageing 2001; 30
(Suppl 3).
163. ST-ONGE, S., AUDET, M., HAINES, V.et PETIT, A. (2004), Relever les défis de
la gestion des ressources humaines, 2ème édition, Montréal: Gaëtan Morin Editeur.
164. STOREY, J. (2003), La légitimité stratégique de la GRH, Encyclopédie des
ressources humaines, Vuibert, Paris.
165. TEIL ALICE (2000), Qu’appelle-t-on système de soins?, în Organization, decision
et financement du système de soins, revue Actualité et dossier en santé publique
(adsp) no 33, revue du Haut Conseil de la Santé Publique,
1TUhttps://www.hcsp.fr/explore.cgi/adsp?chef=62U1T
166. TILMONT, B., ALCARAZ, I. (2012), Concepts en Santé publique, D.U. Santé
Précarité, Lille 11-13-01-2012, p.17, 1TUwww.infectio-lille.com/.../2013-DU-Sante-
precarite-Tilmont_Alcaraz.pdf
167. 1TTOUPILLIER Danielle et YAHIEL, M. (2011), Rapport sur la modenisation de la
politique des ressources humaines dans les etablissements publics de santé, Centre
National de Gestion des Practiciens Hospitaliers et des Personnels de Direction de la
Fonction Publique Hospitalière, Ministère du travail de l’emploi et de la santé.
168. UNESCO-IIEP, (2015), Concepts de la gestion des resources humaines et
planification prèvisionnelle, Gestion des enseignant, Unité 2, [email protected]
169. VALLEJO J. (2013), La modernisation du services RH hospitaliers: un enjeu
stratégique?, Gestion et management, 2013, p.17, 1TUhttps://dumas.ccsd.cnrs.fr/dumas-
00933484U1T
170. VALLET, G. (1997), L’hôpital citoyen, D. H. La Revue des directeurs d’hôpitaux,
Mars 1997, p. 47.
171. VAGU, P., STEGĂROIU, I. (1998), Management general, Târgoviște : Editura
Macarie.
172. VAGU, P. și STEGĂROIU, I. (coordonatori), CROITORU G., DUICĂ Anișoara,
Duică, M. (2013), Tratat de management general, Vol. 1, Școlile de management,
Târgoviște : Editura Bibliotheca.
173. VINCENT Catherine et VOLOVITCH P. (2003), Les Syndicats face au
restructurations hospitalières, Revue française des affaires sociales, 2003/3, no 3,
pp. 121-140.
174. WINSLOW, C., (1920), The untilled fields of public health, Science, 51 (1306), pp.
23-33.
175. WONCA Europe (World Organization of Family Doctors) (2002), La définition
européenne de la médecine générale- médecine de famille,
1TUhttp://www.woncaeurope.org/web%20documents/European%20Definition%20of%
20family%20medicine/WONCA%20definition%20French%20version.pdfU1T
176. WORLD HEALTH ORGANISATION, Regional Office for Europe (2003),
Measuring hospitals performance to improuve the qualitz of care in Europe: a need
for clarifying the concepts and defining the main dimentions, Raport on a WHO
Workshop Barcelona, Spain, 10-11 January 2003.
177. Zaghdoudi, T. (2004), L’intervention de d’Etat dans le domaine sanitaire: l’hôspital
public, 1TUhttps://www.memoireonline.com>BiologieU1T et Médicine.
178. *** Quels principaux axes de réforme pour le système de santé en Roumaine?
Ambasade de France en Roumaine, Service economique,
https://www.tresor.economie.gouv.fr/Ressources/File/439310
179. ***SINTEZA – Profilul stării de sănătate 2016, Uinsp.gov.ro/sites/cnepss/wp-
content/uploads/2014/11/SSPR-2016.pdf
180. 1TUhttp://publications.msss.gouv.qc.ca/acrobat/f/documentation/2010/10-202-02.pdf
181. 1TUhttps://fr.wikipedia.org/wiki/Diagnosis_related_groupU 1T accesat 30,05,2018.
182. www.Public health in England, The report of the Committee of Inquiry into the
Future Development of the Public Health Function, London, HMSO, 1988.
183. xxx L’ordonance no 2005-406 du 2 mai 2005 prévoyant la simplification du régime
juridique des établissements de santé,France,
1TUhttp://www.legifrance.gouv.fr/wAspad/UntexteDeJorf?numjo=SANX0500028R U1T.
CURRICULUM VITAE
PERSONAL INFORMATION KAKİLLİOĞLU (AVCİ) GÜLAY
Şoseaua İancului, 45, Floarea-Soarelui, Street, Villa 19, Voluntari, İlfov, Romania
-------------------- 0722.234.505
---------------------
--------------------
Sex Female | Date of birth 29/05/1971 | Nationality Turkish (Turkish and Romanian citizen)
WORK EXPERIENCE
From 2008 to 2012:
From 1994 to 2008:
From 1999 to 2008:
From 1992 to 1994:
General Manager and Director of S.C. NOVELLA HOME SRL, a Romanian company. General Manager of S.C. PATRİAPLAST SRL, a Romanian company. - Activities pertaining to the development and implementation of general administration and management plans, policies and procedures - Follow-up of the İSO 9001 certification process - Responsible for HR planning, employment and appointment in various positions - Responsible for drawing up the company’s management and administration plans and policies - Coordinate the activities specific of a company whose object of activity is represented by PVC household products - Activities pertaining to the coordination of the financial – accounting department in terms of the accounting records - Activities pertaining to the identification of the personnel’s need for professional training - Manage bilateral meetings concerning requests for leave of absence or resignation General Manager and Shareholder of S.C. PRESTİGE MOB SRL, a Romanian company. - Activities pertaining to the development and implementation of general administration plans, policies and procedures - Follow-up of the İSO 9001 certification process - Responsible for HR planning, employment and appointment in various positions - Responsible for drawing up the company’s management and administration plans and policies - Coordinate the activities specific of a company whose object of activity is represented by PVC household products - Activities pertaining to the coordination of the financial – accounting department in terms of the accounting records - Activities pertaining to the identification of the personnel’s need for professional training - Manage bilateral meetings concerning requests for leave of absence or resignation Economic Manager of ASFEM İthalat Sanayi ve Ticaret Limited Şirketi, a Turkish company. - Establish and continue customer relations - Manage the company’s relationships with its customers - Record and supervise the monthly payments made by customers - Manage information
CURRENT JOB
C.E.O. at SC BURAK TOYS İNTERNATİONAL SRL - Buftea / Romania
PERSONAL SKILLS Experience in the Management and Administration of İnstitutions and Enterprises
EDUCATION AND TRAINING
1987 – 1991
2011-2012
2013 -2014
2013 - present
Faculty of Chemical Engineering Yıldız University from İstanbul Academy of Economic Studies in Bucharest Master’s Degree Business Administration (courses taught in Romanian and English) “Dimitrie Cantemir” University in Romania Faculty of Educational Sciences Pedagogy of Education
“Valahia” University of Targovişte / Romania IOSUD-DOCTORAL SCHOOL OF ECONOMIC AND HUMANISTIC SCIENCES
Domain: MANAGEMENT - PhD
Mother tongue(s) Turkish
Other language(s)
UNDERSTANDING SPEAKING WRITING
Listening Reading Spoken interaction Spoken production
Specify the language: ROMANIAN B1/B2 B1/B2 B1/B2 B1/B2 B1/B2
Specify the name of the certificate. Enter the level, if known.
Specify the language: ENGLISH B1/B2 B1/B2 B1/B2 B1/B2 B1/B2
Specify the name of the certificate. Enter the level, if known.
Levels: A1/A2: Basic user - B1/B2: Independent user - C1/C2: Experienced user
Communication skills Good communication skills gained through my experience as production facilities manager.
Organisational / managerial skills ▪ Leadership Gained during my first years of experience in company administration.
Job-related skills ▪ Good knowledge of human resources Gained during my first years of experience leading employees across all departments.
Digital skills SELF-ASSESSMENT
Information processing
Communication
Content creation
Safety Problem solving
Independent user Independent user Independent user Independent user Independent user
▪ good command of office suite (word processor, spread sheet, presentation software)
Other skills
Driving license Category B
ANNEXES
87
„Valahia” University ofTârgovişte
IOSUD Valahia- Doctoral School of Economic and Human Sciences
Faculty of Economic Sciences
Field Management
PhD. StudentGulay (Avci) Kakillioglu
LIST OF SCIENTIFIC PAPERS
ARTICLES PUBLISHED IN
SCIENTIFIC MAGAZINES
2016
Gulay (Kakillioglu) AVCI,Analysis of Correlation Between Changes in
Health Spending Per Capita and Gross Domestic Product on an Inhabitant of
Romania During 2000-2014, Internal Auditing and Risk Management,
Athenaeum University of Bucharest, vol. 42(1), pp. 35-42, June.
https://ideas.repec.org/a/ath/journl/v42y2016i1p35-42.html.
2018 ConstanţaPopescu, GulayKakillioglu,Milestones for the Development and
Repositioning of the Human Resources Division in a Hospital, The Journal
Contemporary Economy ,Vol. 3, Nr. 2/2018, pp. 48-52. ISSN 2537 – 4222,
ISSN-L 2537 – 4222,https://ceeol.com/search/article-detail?id=702740.
2018
Constanta Popescu, Gulay (Avci) Kakillioglu,Strategies for reforming the
health system in Romania in the context of trends in E.U., Procedia of
International Multidisciplinary Conference ICM 2018 Innovation , Creativity
and Management in the 21 st century Perspectives in Education,Academia
Publishing-AEPEEC, 2018, pp.60-65. ISBN 978-1-9998738-7-5.
2018
ConstanţaPopescu, KakilliogluGulay(Avci),Public Hospitals Performance
Theoretical Foundations and Challenges, International
Conference,Globalization, Innovation and Development.Trends and Prospects,,
(G.I.D.T.P.), May 16-17, 2018, Alexandria, România, Lumen, (pending
publication).
2018 ConstanţaPopescu, KakilliogluGulay(Avci),The Need for an Integrative
Approach of the Healthcare System, International Conference « Global
Interferences of Knowledge Society » 2nd Edition, 16 - 17 November, 2018,
Târgovişte-Romania, Lumen (pending publication).
2018 Constanţa Popescu, KakilliogluGulay(Avci),Analyse comparative des
indicateurs de performance du système de santé en roumanie avec ceux des
systèmes de santé nationaux des pays européens,Congrès International d’Izmir
des Sciences Economiques et Administratives Izmir Turcia 05-
08.12.2018,ispublished in the conference volume (pending publication).
88
PARTICIPATION IN
SCIENTIFIC
CONFERENCES AND
CIRCLES
2018 ConstanţaPopescu, GulayKakillioglu, Milestones for the Development and
Repositioning of the Human Resources Division in a Hospital,International
Scientific Conference Accounting and Finance – The Global Languages in
Business - 3nd Edition, Universitatea Constantin Brâncoveanu, Piteşti, 23
Martie 2018.
2018
Constanta Popescu, Gulay (Avci) Kakillioglu,Strategies for reforming the
health system in Romania in the context of trends in E.U. , International
Multidisciplinary Conference ICM 2018 „Innovation, Creativity and
Management in the 21st century. Perspectives in Education”, Istanbul,
Turcia,mar.2018.
2018
ConstanţaPopescu, KakilliogluGulay(Avci),Public Hospitals Performance
Theoretical Foundations and Challenges, International Conference,
Globalization, Innovation and Development.Trends and Prospects,,
(G.I.D.T.P.), May 16-17, 2018, Alexandria, România.
2018 ConstanţaPopescu, KakilliogluGulay(Avci),The Need for an Integrative
Approach of the Healthcare System, International Conference « Global
Interferences of Knowledge Society » 2nd Edition, 16 - 17 November 2018,
Târgovişte-Romania.
2018 Constanţa Popescu, KakilliogluGulay(Avci),Analyse comparative des
indicateurs de performance du système de santé en roumanie avec ceux des
systèmes de santé nationaux des pays européens, Congrès International
d’Izmir des Sciences Economiques et Administratives Izmir Turcia 05-
08.12.2018.






![Serviciile de Sanatate si Romii Evaluarea Sistemului …Serviciile de sanatate si romii. Evaluarea sistemului de mediere sanitara [ 15 ] Sistemul de sanatate publica in Romania Date](https://img.pdfslide.tips/doc/110x75/5e493cb9407fe522fb0e6126/serviciile-de-sanatate-si-romii-evaluarea-sistemului-serviciile-de-sanatate-si-romii.jpg)






















