Embed Size (px)
Citation preview

3/11/2015
1
Effects of CV Drugs on Hemodynamics: Which Drug When?
Robin Donohoe Dennison, DNP, APRN, CCNS, CNE
copyright Robin Donohoe Dennison 2015
Objectives
• describe the hemodynamic effects of select CV drugs
• select the appropriate CV drug in a clinical situation
• explain rationale for use of one drug over another drug
To increase:
treatment of cause
parasympatholytics:
atropine
sympathomimetics:
epinephrine
pacemaker
To decrease:
treatment of cause
antidysrhythmics
I: procainamide,
quinidine, lidocaine
II: beta-blockers
III: amiodarone,
ibutilide, dofetilide
IV: calcium channel
blockers
Misc: adenosine,
digoxin
vagal maneuvers
cardioversion
overdrive pacing
defibrillation
Heart RatePalpable Pulse
Herlihy, 2007
by fluids by diuretics, venous vasodilators
by vasopressors by arterial vasodilators, IABP
Volume
Pressure
Optimal preload
Understretched
Normal but suboptimal
Optimal
Overstretched
PreloadRV: RAP
LV: LAP (PAOP)
To decrease:
venous
vasodilators:
morphine; NTG
diuretics
ACE inhibitors or
ARBs
To increase:
crystalloids: NS,
LR
colloids: albumin,
hetastarch,
dextran
blood and blood
products

3/11/2015
2
AfterloadRV: PVRI
LV: SVRI
To decrease:
· arterial vasodilators:
NTP, NTG > 1 mcg/
kg/min; hydralazine
· ACE inhibitors or
ARBs
· IABP
RV specifically
· oxygen
· pulmonary
vasodilators:
aminophylline,
epoprostenol
(Flolan), bosentan
(Tracleer), nitric
oxide
To increase:
· vasopressors:
phenylephrine,
norepinephrine,
dopamine,
vasopressin
ContractilityRV: RVSWI
LV: LVSWI
To increase:
cardiac glycosides:
digoxin
sympathomimetics:
dobutamine
PDE inhibitors:
milrinone
To decrease:
beta-blockers
calcium channel
blockers
Inotropic Agents • Cardiac glycosides: digoxin
• Sympathomimetic (adrenergic) agents
– Epinephrine
– Dopamine
– Dobutamine
• Phosphodiesterase inhibitors
– Inamrinone
– Milrinone
Hemodynamic effects of inotropic agents
Drug CO/CI MAP PAOP SVR Heart rate
Digoxin
Dobutamine or
Dopamine
Inamrinone/
Milrinone
Sympathomimetics Drug Alpha Beta1 Beta2
Phenylephrine ++++ 0 0
Norepinephrine ++++ ++ 0
Epinephrine ++++ ++++ ++
Dopamine +++ +++ +
Dobutamine + ++++ ++
Isoproterenol 0 ++++ ++++
Inotropes
___chronic LVF
___acute LVF
___calcium channel blocker toxicity
___beta-blocker toxicity
___end-stage refractory LVF
a. Dobutamine
b. Milrinone
c. Digoxin
d. Glucagon
e. Calcium

3/11/2015
3
Vasodilators
Vasodilators
Venous dilators to decrease preload
Arterial dilators to decrease afterload
Vasoactive effects of selected drugs DRUG ARTERIES VEINS
Morphine sulfate no yes
Nitroglycerin (Tridil) only if > 1 mcg/kg/min yes
Hydralazine (Apresoline) yes no
Minoxidil (Loniten) yes no
Fenoldopam mesylate (Corlopam) yes no
Clevidipine butyrate (Cleviprex) yes no
Milrinone (Primacor) yes yes
Nicardipine (Cardene) yes yes
Nifedipine (Procardia) yes yes
Nesiritide (Natrecor) yes yes
Nitroprusside (Nipride) yes yes
Phentolamine (Regitine) yes yes
Prazosin (Minipress) yes yes
Effects of calcium channel blockers
Type of Calcium Channel
Blocker
Coronary
Arterial
Dilation
Peripheral
Arterial
Dilation
AV Nodal
Depression
SA Nodal
Depression
Effect on LV
Contractility
Dihydropyridine type
(e.g., nifedipine)
+ +++ 0 0 0
Diphenylalkylamine type
(i.e., diltiazem)
+ ++
Benzothiazepine type
(i.e., verapamil)
+ +
Copyright Dennison, R. D. (2013). Pass CCRN! (4 ed). Philadelphia: Elsevier.
Vasodilators ____eclampsia
___hypertension with neurologic injury
___need for afterload reduction in acute MI
___benign prostatic hypertrophy
___hypertension after vascular surgery
___cerebral vasospasm
___autonomic dysreflexia
___heart failure
___coronary artery spasm
___renal hypoperfusion
a. Nifedipine (Procardia) b. Nitroglycerin (Tridil) c. Labetalol (Normodyne) d. Phentolamine
(Regitine) e. Fenoldopam mesylate
(Corlopam)
f. Hydralazine (Apresoline)
g. Carvedilol (Coreg) h. Clevidipine (Cleviprex) i. Nitroprusside (Nipride) j. Doxazosin (Cardura)

3/11/2015
4
Blood pressure =
Vasopressors
Sympathomimetics Drug Alpha Beta1 Beta2
Phenylephrine ++++ 0 0
Norepinephrine ++++ ++ 0
Epinephrine ++++ ++++ ++
Dopamine +++ +++ +
Dobutamine + ++++ ++
Isoproterenol 0 ++++ ++++
Hormone: Vasopressin
Antidysrhythmics Antidysrhythmics
___blocks potassium channel
___blocks beta receptors
___blocks calcium channel
___blocks sodium channel
___blocks reentry
a. Class I
b. Class II
c. Class III
d. Class IV
e. Miscellaneous
3/11/2015
5
Diuretics
Diuretics
___heart failure
___hypertension
___oliguria
___rhabdomyolysis
___glaucoma
___metabolic alkalosis
___intracranial hypertension
___cirrhosis
a. Thiazide
b. Loop
c. Osmotic
d. Aldosterone antagonists
e. Carbonic anhydrase
___Digoxin ___Dobutamine ___Dopamine 3-5 mcg/kg/min ___Dopamine 5-10 mcg/kg/min ___Dopamine >10 mcg/kg/min ___Fluid challenge ___Furosemide ___Milrinone ___Nesiritide ___Nitroglycerin ___Nitroprusside ___Phenylephrine ___Propranolol ___Vasopressin
a. Increased heart rate b. Decreased heart rate c. Increased preload d. Decreased preload e. Increased afterload f. Decreased afterload g. Increased contractility h. Decreased contractility
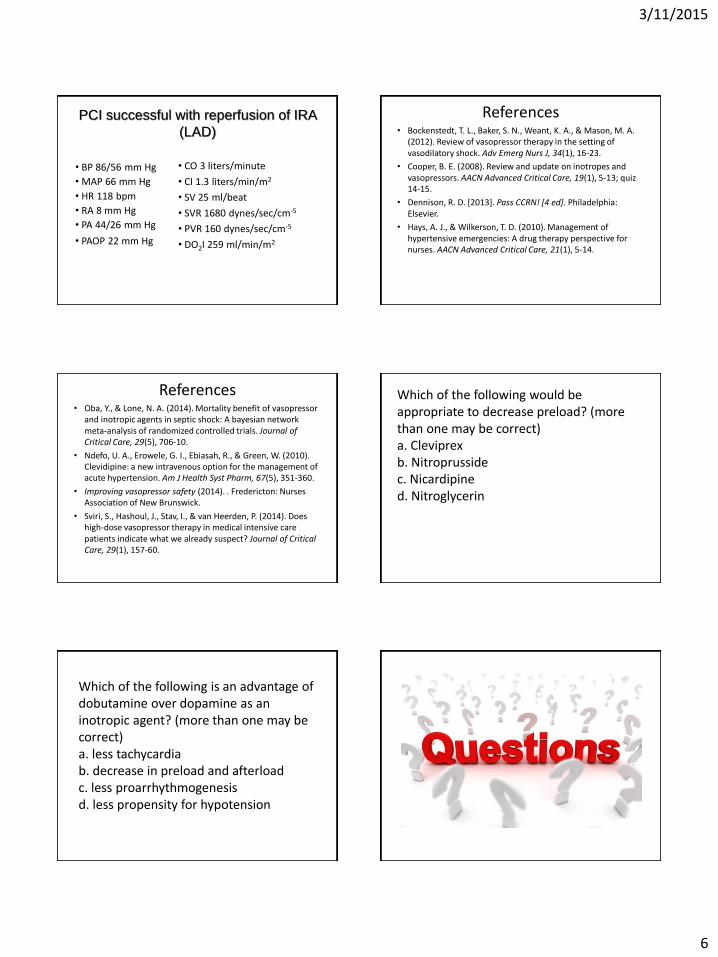
Case Study
ST
segment
elevation
in V1 =
septal
injury
Pathologic Q waves and ST segment
elevation in V2 through V5 =
acute anterior MI
ST
segment
elevation
in V6 =
lateral
injury
3/11/2015
6
• BP 86/56 mm Hg
• MAP 66 mm Hg
• HR 118 bpm
• RA 8 mm Hg
• PA 44/26 mm Hg
• PAOP 22 mm Hg
• CO 3 liters/minute
• CI 1.3 liters/min/m2
• SV 25 ml/beat
• SVR 1680 dynes/sec/cm-5
• PVR 160 dynes/sec/cm-5
• DO2I 259 ml/min/m2
PCI successful with reperfusion of IRA
(LAD)
References • Bockenstedt, T. L., Baker, S. N., Weant, K. A., & Mason, M. A.
(2012). Review of vasopressor therapy in the setting of vasodilatory shock. Adv Emerg Nurs J, 34(1), 16-23.
• Cooper, B. E. (2008). Review and update on inotropes and vasopressors. AACN Advanced Critical Care, 19(1), 5-13; quiz 14-15.
• Dennison, R. D. [2013]. Pass CCRN! [4 ed]. Philadelphia: Elsevier.
• Hays, A. J., & Wilkerson, T. D. (2010). Management of hypertensive emergencies: A drug therapy perspective for nurses. AACN Advanced Critical Care, 21(1), 5-14.
References • Oba, Y., & Lone, N. A. (2014). Mortality benefit of vasopressor
and inotropic agents in septic shock: A bayesian network meta-analysis of randomized controlled trials. Journal of Critical Care, 29(5), 706-10.
• Ndefo, U. A., Erowele, G. I., Ebiasah, R., & Green, W. (2010). Clevidipine: a new intravenous option for the management of acute hypertension. Am J Health Syst Pharm, 67(5), 351-360.
• Improving vasopressor safety (2014). . Fredericton: Nurses Association of New Brunswick.
• Sviri, S., Hashoul, J., Stav, I., & van Heerden, P. (2014). Does high-dose vasopressor therapy in medical intensive care patients indicate what we already suspect? Journal of Critical Care, 29(1), 157-60.
Which of the following would be appropriate to decrease preload? (more than one may be correct) a. Cleviprex b. Nitroprusside c. Nicardipine d. Nitroglycerin
Which of the following is an advantage of dobutamine over dopamine as an inotropic agent? (more than one may be correct) a. less tachycardia b. decrease in preload and afterload c. less proarrhythmogenesis d. less propensity for hypotension

















![[Gokigenyou] Eart Grls v.1 C.05](https://img.pdfslide.tips/doc/110x75/577ca6d41a28abea748c0c34/gokigenyou-eart-grls-v1-c05.jpg)
![[Gokigenyou] Eart Grls v.1 C.03](https://img.pdfslide.tips/doc/110x75/577ca7a01a28abea748c7baf/gokigenyou-eart-grls-v1-c03.jpg)

![[Gokigenyou] Eart Grls v.1 C.04](https://img.pdfslide.tips/doc/110x75/577ca7531a28abea748c5849/gokigenyou-eart-grls-v1-c04.jpg)






