-
8/3/2019 Health Economics- Lecture Ch13
1/39
Nonprofit Firms
Dr. Katherine SauerMetropolitan State College of Denver
Health Economics
-
8/3/2019 Health Economics- Lecture Ch13
2/39
Overview:I. Why Nonprofit Firms Exist
II. Models of Nonprofit Hospital BehaviorIII. Efficiency of
Nonprofit vs For Profit Firms
-
8/3/2019 Health Economics- Lecture Ch13
3/39
Nonprofit firms account for only 5 percent of GDP, butthey make
up a significant portion of the health caresector.
The 60 percent of community hospitals that arenonprofit provide
nearly 70 percent of the beds and treata similar proportion of the
nations hospital patients.
-
8/3/2019 Health Economics- Lecture Ch13
4/39
Distinctions between for-profit and nonprofit firms:
Nonprofits:- nondistribution constraint
- no one has a claim on the residual
- exempt from corporate income taxes- often sales tax and
property tax, too
- donations to nonprofits receive favorable tax
treatment
-
8/3/2019 Health Economics- Lecture Ch13
5/39
I. Why Nonprofit Firms Exist
A. market failure
Externalities:- free markets underproduce goods/services
with
external benefits
Public Goods:- non-excludable and non-rival
- free rider problem
-
8/3/2019 Health Economics- Lecture Ch13
6/39
B. Weisbrod Model (nonprofits arise becausegovernment fails to
provide the level of the good desired
by the people)
Suppose there are 5 voters (A, B, C, D, and E) withdifferent
marginal benefits associated with a particular
public good.
The government must choose how much of the publicgood to
provide.
All voters will pay the same marginal tax for theprovision of
the good.
-
8/3/2019 Health Economics- Lecture Ch13
7/39
$
Quantity of the Public Good
MarginalTax
D(A) D(B)D(C) D(D) D(E)
QA QB QC QD QE
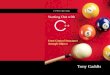
Given the same marginal tax, but different marginalbenefits,
each voter will have a different optimal levelof the public
good.
-
8/3/2019 Health Economics- Lecture Ch13
8/39
If the government opts for level QA of the good:- 4 voters would
have preferred more- 1 voter is happy
If the government opts for level QB of the good:- 3 voters would
have preferred more- 1 voter would have preferred less- 1 voter is
happy
If the government opts for level QC of the good:- 2 voters would
have preferred more- 2 voters would have preferred less- 1 voter is
happy
-
8/3/2019 Health Economics- Lecture Ch13
9/39
-
8/3/2019 Health Economics- Lecture Ch13
10/39
C. Contract Failure (Hansmann)
Nonprofits arise in situations where it is hard to verify
that the contract has been fulfilled (esp. when quality ishard
to observe).
- nursing homes often have contract failure
- physicians help abate contract failure in hospitals
-
8/3/2019 Health Economics- Lecture Ch13
11/39
II. Models of nonprofit hospital behavior
A. Quality-Quantity Theory (Newhouse)
Think of the hospital as a utility maximizer.- max the utility
of decision makers
- board of trustees- administrator/CEO- physician staff
The hospital has preferences over quality and quantity.-
quantity is # of cases (treat as one type)- assume one measure of
quality
-
8/3/2019 Health Economics- Lecture Ch13
12/39
The hospital has a budget constraint.- must pay its bills (no
negative net revenue)- nondistribution constraint (no positive
netrevenue)
Let all the revenue sources be summarized in the averagerevenue
curve (demand curve).
- depends on level of quality q
- higher quality means a higher demand curve
-
8/3/2019 Health Economics- Lecture Ch13
13/39
-
8/3/2019 Health Economics- Lecture Ch13
14/39
$
Quantity
AC(q3)
AC(q2)
AC(q1)
D(q1) D(q3)D(q2)
Q1 Q2 Q3
-
8/3/2019 Health Economics- Lecture Ch13
15/39
For each level of quality, the firm chooses the quantitywhere
AR=AC.
If we plot each quality-quantity point, we can see
theQuality-Quantity Frontier.
Quality
quality
-
8/3/2019 Health Economics- Lecture Ch13
16/39
The tangency between the QQF and the indifferencecurve yields
the optimal combination of quality and
quantity for the firm.
Quantity
quality
U
U (firm prefers quantity)
U (firm prefers quality)
-
8/3/2019 Health Economics- Lecture Ch13
17/39
B. The Profit-Deviating Nonprofit Hospital(Lakdawalla and
Philipson )
This model views a nonprofit as a mix of altruism and
profit motives.
This model explores the entry and exit responses ofnonprofits to
changes in market conditions and
government regulation.
-
8/3/2019 Health Economics- Lecture Ch13
18/39
A nonprofit has an advantage over pure for-profit firms
because it can receive donations.
The operating constraint of for-profit firms:profits must be
> zero
The operating constraint of nonprofit firms:profits + donations
must be > zero
-
8/3/2019 Health Economics- Lecture Ch13
19/39
C. The hospital as a physicians cooperative (Pauly
andRedisch)
This view focuses on the full price of the hospital care.-
hospital charges- physician charges
The hospital maximizes pecuniary gains for the
decisionmakers.
Physicians run the hospital to maximize their incomes.
-
8/3/2019 Health Economics- Lecture Ch13
20/39
The hospital maximizes net revenues (NR) per physician (M): NR
/M
NR = all revenues - payments for other labor- payments for
capital
-
8/3/2019 Health Economics- Lecture Ch13
21/39
Physicianincome
$
Number ofphysicians
Supply of physicians
Net average revenue
S
M* Mo
From the physicians standpoint, M* is the optimalnumber.
From the hospitals standpoint, Mo is
the optimal number.
-
8/3/2019 Health Economics- Lecture Ch13
22/39
D. Comparison of Q-Q model and Physicians Coop. model
Hospital Residual (HR) = R(K, L, Mo) - wL - rK +D +G
R(.) is all revenuesD is donationsG is government subsidies
-
8/3/2019 Health Economics- Lecture Ch13
23/39
-
8/3/2019 Health Economics- Lecture Ch13
24/39
E. The Evidence
Sloan and colleagues (1998)conclude that there is not a
difference. They base theirconclusion on studies of quality, cost,
and efficiency of
hospitals by ownership type.
Ballou (2008)finds public hospitals are first to serve areas of
poverty.
-
8/3/2019 Health Economics- Lecture Ch13
25/39
McClellan and Staiger (1999)find higher mortality rates for the
elderly in for-profithospitals overall, but the small difference on
averagemasked substantial variation with a number of marketsshowing
quality superiority in the for-profit hospitals.
Grabowski and Hirth (2003)find that competition from nonprofits
tends to providespillover effects so as to improve the quality of
the for-
profits .
-
8/3/2019 Health Economics- Lecture Ch13
26/39
Norton and Staiger (1994)found that hospitals in the same market
area tend to serve
the same number of uninsured.
Ballou and Weisbrod (2003)find substantial differences among
religious, secular
nonprofit, and government hospitals in patterns of
CEOcompensation.
Brickley and van Horn (2002)
find for a large sample of nonprofit hospitals thatcompensation
incentives for CEOs are significantlyrelated to financial
performance.
-
8/3/2019 Health Economics- Lecture Ch13
27/39
Hansmann et al. (2002)found the for-profit to be quicker in
adjusting to marketdemand changes.
Chakvarty et al. (2005)find the for-profits to be more nimble in
adjusting tonew economic conditions.
-
8/3/2019 Health Economics- Lecture Ch13
28/39
-
8/3/2019 Health Economics- Lecture Ch13
29/39
Implications:1. expect that hospital preferences for new
technology will be driven by the physiciandemanders- quality
enhancing
2. any hospital regulation aimed at the trusteesor
administration may have little effect
3. re-organizing hospitals along product linesmay make them more
efficient
- ex: cardiology department
-
8/3/2019 Health Economics- Lecture Ch13
30/39
III. Efficiency of nonprofit firms vs for profit firms
A. Property Rights Theory
An essential economic problem comes about because of
the non-distribution constraint.- non-pecuniary benefits become
more important
Employees in for-profit and nonprofit firms both face a
tradeoff between monetary wealth and non-pecuniarybenefits.
-
8/3/2019 Health Economics- Lecture Ch13
31/39
Non-pecuniary benefits
wealthWealth-Benefits Frontier
Profit maximizing firms will
try to achieve the highestutility that the WB
frontierallows.
Uprofit
-
8/3/2019 Health Economics- Lecture Ch13
32/39
Non-pecuniary benefits
wealthNonprofits often have limits(L) on the level of
wealth.
Uprofit
LU non-profit
-
8/3/2019 Health Economics- Lecture Ch13
33/39
Non-pecuniary benefits
wealthEven if firms have similar
preferences between wealthand non-pecuniary benefits,
the nonprofit will choose ahigher level of non-pecuniary
benefits.
Uprofit
LU non-profit
-
8/3/2019 Health Economics- Lecture Ch13
34/39
B. Evidence
Nonfrontier studies(matched hospitals pair-wise or compared
selectedgroups of hospitals) usually found little, if any,
costefficiency differences between the nonprofits and the
for-profits.
Kessler and McClellan (2001)find the for-profit hospitals could
treat elderly heart
attack patients at somewhat less expense (2.4 percentless)
without reduction in quality of care.
-
8/3/2019 Health Economics- Lecture Ch13
35/39
Wilson and Jadlow (1982)compared nuclear medicine services in
nonprofit and
for-profit hospitals and found for-profits more efficient.
Ozcan et al. (1992)used DEA and found small differences
Burgess and Wilson (1998)conclude that no significant difference
in efficiency can
be found between nonprofit and for-profit hospitals.
-
8/3/2019 Health Economics- Lecture Ch13
36/39
Concluding Thoughts:
Nonprofit firms exist in health care for two
possiblereasons:provide public goods that are neglected by
theprivate markets and the government
reduce or eliminate a contract failure that arisesbecause
consumers may not trust the profit-motivated firm
-
8/3/2019 Health Economics- Lecture Ch13
37/39
Three analytical models of nonprofit hospital behavior:The
Newhouse hospital model is motivated by the
desire to provide service to the community.
The Lakdawalla-Philipson model exploits a middleground to
explain the entry and exit behaviors of
nonprofits.
The Pauly-Redisch hospital model is really under thephysicians
control, who use it to maximize the
average physicians income.
-
8/3/2019 Health Economics- Lecture Ch13
38/39
The data from recent efficiency studies offer littlesupport
regarding hospitals, which have shown little, if
any, difference between the ownership types.
-
8/3/2019 Health Economics- Lecture Ch13
39/39
Discussion Questions:
1. If the delivery and quality of health care could becheaply
and accurately monitored by an agency, wouldthere be any contract
failure in health care remaining?Would there be any need for
nonprofits?
2. Under which of the models of hospital behavior doesthe
tax-exempt status of nonprofit hospitals make the
most sense? The least sense?