Embed Size (px)
Citation preview
Kia Mau te Kahu Whakamauru:
Health Literacy in Palliative Care
June 2014 Dr Jacquie Kidd
Susan Reid
Nicola Collins
Dr Veronique Gibbons
Stella Black
Rawiri Blundell
Tamati Peni
Matua Hone Ahu
Te puāwaitanga o te hinengaro mō te tangata
ii
He Mihimihi
Hehōnore,hekorōriakiteAtua
Hemaungarongokitewhenua
Hewhakaaropaikingātāngatakatoa
Tēnārākoutou,eteiwinuitonu,kawhakakorōriatonuiteAtuaKahaRawa.KiatautonuōnamanaakitangamahakirungaiTeArikinuiKīngiTūheitia,meteWhareoteKāhuiAriki.
Kuatangihiakēngia,ngāmateotewā!Nōreira,rātoukiarātou!Tātou,kē,oteaomōrehu,kiatātou!
Kakiteairaronei,hekaupapawhakahirahira,kapākingātāngatakuatinopāngiaengāmomomatepukupuku,mengātūroro,kuatatawhakawhitiatukituaoteārai.Anōhoki,orātouwhānauemōhiopaianakingāāhuatangawhaipāngakitemanaakipaiitetūroro.
Emihianakingāwhānaukuauiuingiamōtetaharangahauotekaupapamerātoungākaimahioteratongamōngātūrorokuatatatewhakawhitikituaoteārai.
MāteRungaRawaetiaki,emanaakitonuiakoutou;ahakoateaha!
ThisreportwaswrittenbyDrJacquieKidd(UniversityofAuckland);SusanReid(WorkbaseEducationTrust);NicolaCollins(UniServices),StellaBlack(UniversityofAuckland),DrVeroniqueGibbons(UniversityofAuckland);RawiriBlundell(MidlandsCancerNetwork);TamatiPeni(UniversityofWaikato)andMatuaHoneAhu(Tainui).Thisstudywassupportedbymanypeopleandweappreciatetheirwisdom,guidanceandtime.
Whānauverygenerouslysharedtheircompellingandmovingstoriesandexperienceswithus.
Wethankthefollowingorganisationsforsupportingus:
o MercyHospice(Auckland) o HospiceWestAucklando WaipunaHospice(Tauranga) o HospiceEasternBayofPlentyo KaitiakiNursingService(Tauranga) o TeWhānauOWaipareirao ADHBPalliativeCareTeam o WesternBayofPlentyPHOo Kimihauora,BayofPlenty o AucklandCancerSociety
WethanktheMinistryofHealth(MOH)andtheHealthResearchCouncilofNewZealand(HRC)forfundingthisstudyandgivingustheopportunitytopreparearesearchagendaforthefuture.
SpecialthankstoProfessorRossLawrensonfromtheSchoolofMedicineandcolleaguesfromtheSchoolofNursingfortheirexpertiseandsupportofthisstudy.
iii
Contents HeMihimihi.....................................................................................................................................................ii
Contents................................................................................................................................................................iii
Tables.......................................................................................................................................................................v
Figures.....................................................................................................................................................................v
Whakarāpopototanga–ExecutiveSummary.......................................................................................vi
Method.............................................................................................................................................................vi
Findings..........................................................................................................................................................vii
NgaKitengaMatua–KeyPoints..................................................................................................................x
Section1:KupuWhakataki‐Introduction.............................................................................................1
1.1 Palliativecare....................................................................................................................................1
1.2 Healthliteracy...................................................................................................................................3
1.3 Literaturereview.............................................................................................................................5
1.4 Thisstudy............................................................................................................................................7
Section2:RautakiMahi–Methodology..................................................................................................9
2.1 Researchdesign................................................................................................................................9
2.2 Recruitment.......................................................................................................................................9
2.3 Datacollection................................................................................................................................10
2.4 Dataanalysis....................................................................................................................................13
2.5 Ethics...................................................................................................................................................16
2.6 Limitations........................................................................................................................................16
Section3:NgaKitenga‐Findings.............................................................................................................18
3.1 Healthprofessionals’conceptsofhealthliteracyinpractice.....................................19
3.2 Writtenresourceanalysis..........................................................................................................20
3.3 Accessingandutilisingpalliativecareservices................................................................22
3.4 Healthliteracydemands.............................................................................................................25
3.5 Healthliteracypractices.............................................................................................................30
iv
3.6 Barriers..............................................................................................................................................35
3.7 Navigatingthepalliativecaresystem...................................................................................41
3.8 Communicationprocesses.........................................................................................................42
3.9 Summary...........................................................................................................................................47
Section4:Hematapakingamehewhakatepe–Discussionandconclusion.........................49
4.1 Access.................................................................................................................................................49
4.2 Healthliteracydemands.............................................................................................................52
4.3 Reducinghealthliteracydemands.........................................................................................53
4.4 Healthliteracypractices.............................................................................................................53
4.5 Communication..............................................................................................................................55
4.6 Systemicororganisationalhealthliteracypractices.....................................................56
4.7 Conclusion........................................................................................................................................57
Section5:ResearchAgenda........................................................................................................................59
Figure 1: Research agenda....................................................................................................................61
References..........................................................................................................................................................63
Glossary...............................................................................................................................................................71
AppendixOne:LiteratureReview............................................................................................................75
AppendixTwo:Listofresourcesanalysed...........................................................................................96
AppendixThree:Healthliteracydemands........................................................................................101
AppendixFour:PatientWhānauInformationLetter,ConsentForm&InterviewSchedule...........................................................................................................................................................106
AppendixFive:HealthProfessionalInformationLetter,ConsentForm&FocusGroupInterviewSchedule,KeyInformantInterviewSchedule.............................................................112
v
Tables Table 1: Health professional participants .................................................................................. 11 Table 2: Key informants ............................................................................................................. 12 Table 3: Individual patient pathways and services accessed ................................................... 23 Table 4: Search #1 Identify barriers that inhibit utilisation of palliative care services for Māori .......................................................................................................................................... 85
Figures Figure 1: Research agenda .......................................................................................................... 61
vi
Whakarāpopototanga – Executive Summary TheNewZealandPalliativeCareStrategy(MinisterofHealth2001)recognisedtheneedfor local and national policies that support the specific needs of Māori, includinglinkages with Māori organisations and care coordinators. While there are increasingnumbersofresearchstudiesaboutaccesstopalliativecareforMāoriandothers(Freyet al 2013; Robinson et al 2013), this is the first to have taken a health literacyperspective.
Health literacy is described as “the degree towhich individuals have the capacity toobtain,processandunderstandbasichealth informationandservicesneededtomakeappropriatehealthdecisions”(Nielsen‐Bohlmanetal2004;MinistryofHealth2010a).For health professionals, health literacy is about their ability to communicate healthinformationandbuildskillsandknowledge.Forhealthorganisations,healthliteracyisabout the appropriateness of the health information and services they provide forpatients and their families as well as the organisational systems and processes tosupporthealthprofessionalstobuildhealthliteracy.
TheHealthResearchCouncilofNewZealand (HRC)and theMinistryofHealthas theMāori Health Joint Venture, contractedUniServices to identify, from a health literacyperspective,issuesforMāoriandtheirwhānauinaccessingpalliativecareservices.FourkeyareasintheRequestforProposalofinterestwereidentified,including:
1. WaysinwhichMāoriaccesspalliativecareservices2. ThecurrentlevelofMāorihealthliteracywithregardstopalliativecare3. ThewayinwhichdifferentfactorswithinwhānauinfluencetheabilityofMāori
toobtain,processandunderstandpalliativecareinformationandservices4. Identification of communication models which are effective in enhancing this
ability.
Method
The study used a qualitative kaupapaMāorimethodology. Following ethics approval,studyparticipantsforthepalliativecareexpertfocusgroupswererecruitedthroughhuiin Auckland and the Bay of Plenty. Patients and whānau were recruited afterapproachesbytheirpalliativecareservicesprovider.
Semistructuredinterviewswereheldwith21patientsandwhānautoidentifyhowtheyaccessedpalliativecareservices, the information theyreceived, theirexperiencesandsuggestions for improvement. All patient andwhānau participantswere in receipt ofspecialistpalliativecare.
Semi structured interviews were completed with six key informants: a medicalspecialist, a service leader involved in developing culturally specific responses topatients, twoMāori servicemanagers, and twoMāori health team leaders. In the key

vii
informant interviews and focus groups, we sought perspectives about palliative careservicesprovidedforMāoripatientsandwhānau;healthliteracyinpalliativecare;thehealth literacy demands of palliative care; and how health professionals take intoaccountthehealthliteracyskillsofpatientsandwhānau.
Focusgroupswereheldwithatotalof54healthprofessionalsprovidingpalliativecareservices.Focusgroupparticipantscame fromarangeofdisciplines:nurses(includingcancer nurses, students, palliative care nurses, clinical nurse specialists, team leadersand nurse practitioners); General Practitioners (GPs) and clinicians; healthpsychologists, counsellors, social workers and chaplains; kaumātua, kaiāwhina,kaitakawaenga, kaiatawhai and navigators; and managers, administrators andcoordinators.
Data analysis The interview transcriptswere analysed to elicit key concepts and recurrent themes,usingageneralinductiveapproach(Thomas2006).Datafromeachparticipantgroup—patientsandwhānau,healthprofessionals,andkeyinformants,wereviewedasequallyauthoritativeduringtheanalyses,withthesameprocessfollowedforall.Asthethemesweredeveloped,itbecameclearthattherewasameasureofgeneralconsistencyacrossallthreegroups.Thetrustworthinessandreliabilityofthegeneralinductiveapproachwas supported by sharing analysis of transcripts among the research team, using aconsistentanalytictemplate,andreviewinganalysedtextsamongstteammembersandat hui on the findings. Member checking or respondent validation was used inpresenting analyses at five huiwith the research communities involved,where therewas participant engagementwith, and agreement on, the categories and themes thathadbeendevelopedfromthedata.
Written resource analysis Palliative care providerswere asked at focus group and key informant interviews tosupplywritteninformationaboutpalliativecareservicesthatprovidersgavetoMāoripatientsandwhānau.Atotalof42writtenresourcesfromparticipatingpalliativecareproviderswere reviewed, in terms of aspects such as purpose, audience, readability,anduseofMāoriconcepts.
Findings
Lateaccesstopalliativecare,includingdifficultieswithaccessandreferralstopalliativecarethatoccurredlateinthelife‐limitingillnessprocesswereidentifiedinthisstudyasissuesfortheparticipants.Theoutcomeofthesewassimilar,withinadequatetimeforpatients,whānau and their service providers to engage, negotiate any health literacydemands,accesssatisfactorysupport,ormakearrangementsforthepatients’preferreddeath experience. Late referrals to palliative care were also reported to increasedistressforhealthprofessionals.
viii
Themechanismsaroundlateaccessandlatereferralvariouslyrelatedtotikanga,lackofknowledgeormisunderstandingsabouttheavailabilityandusesofpalliativecare(lowhealth literacy), lack of availability of services, the clarity and timeliness of ‘hardconversations’ with health professionals about the shift from treatment to palliativecare,andtheculturalcharacterofpalliativecareservices.
Thisstudyfoundthatsomepatientsandwhānauwerereluctanttoacceptpalliativecarebecause they believed that such services were only available as inpatients; that thepurposeofhospicecarewastohastendeath;andthattoacceptpalliativecarewastoacceptthatdeathwasimminent.
This study found that the willingness and ability of health professionals to have the‘hard conversations’ that accompany illness and death had an impact on the healthliteracy of patients andwhānau.Where those conversationswere not held or lackedclarity,whānaureportedfeelingoverwhelmedandunder‐informedabouttheiroptionsandhowtohelptheirfamilymember.
ThisstudyfoundaclearperceptionbyallparticipantsthatHospice,theCancerSociety,andthewiderhealthcaresystemingeneralwerePākehāorganisations.Yet,interestingly,noneofthepatientandwhānauintervieweesidentifiedcultureasabarriertoreceivingpalliativecareoncetheserviceshadbeenaccessed.
Thehealthliteracydemandsonpatientsandwhānauwerefoundtobesubstantialandcomplex,requiringproblemsolvingandresourcefulness.
Threecategoriesofhealthliteracydemandsweredeveloped.Theseincludedthediseasemanagementfocusofmedicinesandpatientcare,andthewiderfocusofnavigatingthepalliativecaresystem.
Theemotionalclimateofpalliativecaremayaddanotherdimensiontohealth literacydemands.Theparticipants acknowledged the additional health literacydifficulties forpatientsandwhānauthatarosebecauseoftheshock,griefandanxietyassociatedwithreceiving palliative care services. These emotions, combined with the health literacydemandsassociatedwithintensivephysicalhealthcareneeds,createdacomplexhealthliteracyenvironment.
Whānaucaregivingwasanother factor that influencedtheemotionalclimate inwhichhealth literacy occurred. Having a single spokesperson for thewhānau increased theresponsibilityandworkloadfor thatperson,andhadthepotential tocreateproblemsfor that person. However, it was the perception of most non‐Māori health careprofessionals that this was the method of communication preferred by patients andtheirwhānau.
This study identified that some health professionals consciously used health literacypractices to ensure that patients and whānau felt able to access information and
ix
support.Thesepracticestendedtohavebeendevelopedbytheindividualandwerenotgenerallyutilisedinasystemicway,orrecognisedatanorganisationallevel.
Patientsandwhānauusedcomplexhealthliteracypractices,whichutilisedarangeofliteracyandnumeracyskillsandincludedcriticalthinkinganddecision‐making.Thesehealthliteracypracticeswereusedinspiteofsignificantbarriersgenerallyrelatedtoalackofeffectivecommunication.Utilisingtheskillsandexpertiseofotherwhānaumemberswasawayof‘workingaround’barriersandobstaclesposedeitherbythesystemitselforbypeopleworkingwithinthesystem.
Patientsandwhānauexperiencedpoorcommunicationonanumberofoccasions.However,whānaualsoidentifiedaspectsofgoodcommunicationpracticesinpalliativecaresettingswhichassistedwhānauinprovidingoptimalsupporttotheirlovedone.Effectivecommunicationgreatlyenhancedthewhānauexperienceofpalliativecare.Generallythewhānauparticipantsidentifiedthatindividualhealthprofessionalswereopenandhonestandtriedtoadvisewhānauoftherealityofthesituation.Patientsandwhānaufoundthefollowingcommunicationprocessesusedbyhealthcareprofessionalseffectiveinsupportingthem:
abilitytocommunicate24/7withhealthprofessionals,toaskquestionsandhavetheirfearsallayed
establishedrespectfulrapportwithpatients practicaltrainingprovidedforwhānaucaregivers opportunity to have regularmeetingswithpeople providing care to patient to
discussprogress whānau and health professionals all using a ‘communication book’ to record
whatwashappening helpwithpredictingfuturecareneeds.
Whānaungatanga, kanohi ki te kanohi, wairuatanga, and the availability of Māorikaimahi (health professionals or allied staff) were all identified as importantcomponentsofaneffectivecommunicationmodelforMāoripatientsandwhānau.
Acommonthemefromthisresearchwastheimportanceofeffectivenavigationand/oradvocacy roles to address some of the health literacy and access barriers. Calledvariously anavigator, kaiāwhina, or simply an extensionof an existing role such as anurseor socialworker,where theyhadbeen involved in the care team, thesepeoplehadmadeabigimpressiononthequalityofcarewhānauexperiencedandreceived.
A research agenda which identifies and prioritises future research directionsaccompanies thisdocument, tobuildon the insights from thisqualitative exploratorystudy.
x
Nga Kitenga Matua – Key Points
This was a qualitative, exploratory study that utilised a relatively smallpurposivesamplethatwasbroadlyaccessedandminimallydefined;itspurposewas todevelop anunderstandingof health literacy inpalliative care forMāoriandtoidentifyfutureresearchpriorities.
Māori patients tend to face barriers to accessing palliative care services forreasons relating to tikanga (customs and traditions, protocol), low healthliteracy, availability of services, health professionals avoiding or mismanagingthe ‘hardconversations’aroundtheshift fromtreatment topalliativecare,andtheculturalcharacterofspecialistpalliativecareservices.
Māori patients andwhānau had a range of health literacy practices thatwereeffectiveandwide‐ranging.However,health literacydemandsareconsiderableand complex for Māori in the palliative care context and more research isrequired.
Health professionals utilise effective individual strategies to help patients andwhānau manage the palliative care environment, but these are not generallyadoptedatanorganisationallevel.
Thisstudyfoundthatpatientsandwhānauexperiencedpoorcommunicationonanumberofoccasions,butaspectsofgoodcommunicationwere identifiedandcouldbebuilton, includingbeingopenandhonestandadvisingwhānauoftherealityofthesituation.
This study found that there is inconsistency aboutwhether palliative care is apositiveexperienceforMāori,withpatients,whānauandhealthprofessionalsallreportingbothpositiveandnegativeexperiences.
This, along with the reality that Māori are a diverse, flexible and changeablepeople (Reid 2005), means that generalisations about culturally effectivehealthcarecannotbemade.
Aresearchagendawhich identifiesandprioritises futureresearchdirections ispresentedinSectionFiveinthisdocument.
Section 1: Kupu Whakataki - Introduction Healthdisparities forMāori have longbeen featured inhealth literature (Davis et al.,2006; Howden‐Chapman, Blakely, Blaiklock, & Kiro, 2000),with strong evidence thatMāorihavedisproportionallyhigh incidencesandmortality fromlife‐limitingdiseasessuch as cancer, cardiovascular, and respiratory diseases (Robson & Harris, 2007).Further, Māori rates for chronic conditions, such as chronic obstructive pulmonarydisease, ischemic heart disease, and complications and deaths from diabetes aresignificantlyhigherthanfornon‐Māori(RobsonandHarris2007).
Notwithstandingthesestatistics,Māorilifeexpectancyisimproving,andanincreasingproportion of Māori are aged 65 years and older (Statistics New Zealand 2012).However the combinationof high life‐limitingdisease rates and thepredictionsof anincreasing agedMāori population suggest thatMāori access to palliative care shouldalsobeincreasing.Thisiscompoundedbytherelativelyrecentdevelopmentofprimarypalliative care services and a change in focus that extends palliative care beyond itspreviousfocusoncancercare(Bellamy&Gott,2013;Freyetal.,2013;Robinson,Gott,&Ingleton,2013).
AddressinginequalitiesinMāoriaccesstopalliativecarehasbeenthefocusofnationalpolicy (Minister of Health, 2001), but recent research has shown that the increasedavailabilityofculturallyappropriateserviceshasnotincreasedaccessandutilisationbyMāori(Moeke‐Maxwell,Nikora,&TeAwekotuku,2010).
The identification of lowMāori health literacy (Ministry ofHealth, 2010) adds a newdimension to questions about Māori access to and utilisation of palliative care,particularly in terms of how such services are presented toMāori, and how they areperceived.
The research focus for thisprojectwas to identify, fromahealth literacyperspective,issues for Māori and their whānau in accessing palliative care services. This sectionprovidesabriefintroductiontohealthliteracyandpalliativecare(seeAppendixOneforafullliteraturereview),andtheset‐upforthestudy.InSection2,themethodologyandresearch design are presented, followed by the research findings in Section 3, anddiscussionandconclusionsinSection4.
1.1 Palliative care
TheWorldHealthOrganization(2011)definespalliativecareasanapproachthataimsto improvethequalityof lifeofpatientsandtheirwhānaufacingproblemsassociatedwith life‐threateningillness. Itdoesthisthroughthepreventionandreliefofsufferingbymeansofearly identificationandapplicableassessmentandtreatmentofpainandotherphysical,psychosocialandspiritualproblems.
2
Palliativecare:
providesrelieffrompainandotherdistressingsymptoms affirmslifeandregardsdyingasanormalprocess intendsneithertohastennorpostponedeath integratesthepsychologicalandspiritualaspectsofpatientcare offersasupportsystemtohelppatientsliveasactivelyaspossibleuntildeath offersasupportsystemtohelpfamily/whānaucopeduringthepatient’sillness
andintheirownbereavement uses a team approach to address the needs of patients and their families,
includingbereavementcounselling,ifindicated willenhancequalityoflife,andmayalsopositivelyinfluencethecourseofillness isapplicableearlyinthecourseoflife‐limitingillness,inconjunctionwithother
therapies that are intended to prolong life, such as chemotherapy or radiationtherapy, and includes those investigations needed to better understand andmanagedistressingclinicalcomplications.
TheNewZealandPalliativeCareStrategy(MinisterofHealth2001)recognisedtheneedfor:
accessibleandappropriateservicesforMāori strategythatbuildsoncurrentservicearrangements moreresponsivesystemstosupportthechoiceofdyingathome care coordinationof services in conjunctionwithMāori providersof culturally
appropriatepalliativecareservices formallinkswithrelevantserviceproviders developmentofplanswithlocalMāoritoensureappropriateaccesstoservices linkagesbetweenpalliativecareprovidersandMāoridevelopmentorganisations workforceplanning.
TheNewZealanddefinitionofpalliativecare(PalliativeCaresubcommittee:NZCancerTreatmentWorkingParty2007)is:
Careforpeopleofallageswithalife‐limitingillnesswhichaimsto:
1. Optimise an individual’s quality of life until death by addressing the person’sphysical,psychosocial,spiritualandculturalneeds.
2. Support the individual’s family, whānau and other caregivers where needed,throughtheillnessandafterdeath.
Palliative care is further defined in termsofwho is providing the care and towhom.Thisfallsintotwocategories(Naylor2012):
1. Primary palliative care (also called generalist palliative care, used in NewZealand since 2012) is care provided by individuals and organisations that

3
deliver palliative care as a component of their services, but their substantiveworkisnotinthecareofpeoplewhoaredying.Thekeycomponentsarethattheindividualhasalife‐limitingorlife‐threateningconditionandtheyarereceivingpalliative care as an integral part of standard clinical care by any healthprofessionalwhoisnotpartofaspecialistpalliativecareteam.
2. Specialistpalliativecare ispalliativecarebythosewhohaveundergonespecifictrainingand/oraccreditationinpalliativecare/medicine,workinginthecontextof an expert interdisciplinary teamof palliative care health professionals. Thiscare is usually provided by hospice or hospital‐based palliative care serviceswherepatientshaveaccess topalliativecarespecialists.Specialistcaremaybedelivered through direct involvement with the individual and whānau orindirectly through advice, support and education to other health professionalsandvolunteerswithintheprimarypalliativecareframework.
Internationally, palliative care has historically focused on the end‐of‐life stage forpeoplewhohavecancer,buthasbeenrevisedtorecognisetheapplicabilityofpalliativecareearlyinthetrajectoryofalllife‐limitingillnesses(Sepúlvedaetal2002).
1.2 Health literacy
Health literacy is defined as “the degree to which individuals have the capacity toobtain,processandunderstandbasichealth informationandservicesneededtomakeappropriatehealthdecisions”(Kickbuschetal2006,p.4).This impliesrightly that theeffects of health literacy relate to how an individual perceives messages. However,individualsdonotoperate in isolation fromthecontext inwhichhealthmessagesaredelivered,receivedandprocessed.Manyskillsarerequiredforindividualstofunctioneffectively in the health care environment and act appropriately on health careinformation. These skills include the ability to interpret documents, read and writeprose (print literacy), use quantitative information (numeracy), and speak and listeneffectively(oralliteracy)(Berkmanetal2011).Bothcontentandcontextareimportant;for example, apersonwith advanced literacy skillsmay, in adifferenthealth context,havepoorhealthliteracy(Nutbeam2009).Theexchangeofhealthinformationhasbeendescribedasacomplexprocessinvolvingtheprovider,thehealthprofessionalandtherecipient, with consumers of health services seen as active receivers and seekers ofinformation who also generate and synthesise information of their own (EuropeanHealthPolicyForum2005).
Healthliteracyhasbeenconceptualisedwithintwodifferentapproaches:seeneitherasa risk factor or as an asset. In the risk model, health literacy is conceptualised as apotential risk factor; for example, that lack of health literacy will act as a barrier topatientsbecomingcompliantwith treatment.Alternatively, it canbeseenasanasset,where improved health literacy is an outcome of personal empowerment in decisionmaking(Nutbeam2008).TheuseoftheriskmodelwasprevalentintheUnitedStates,meaningtherewasanemphasisonmoreassessmentof individualhealth literacy,but
4
recent literaturepertainsmore to theuseofanassetmodelwhichalignscloselywithprinciples of adult education, where the patient’s prior knowledge and experience isrecognised(Workbase2013).
Peoplewithpoorhealthliteracyskillsarethoughttobeatgreaterriskofexperiencingpoorhealthstatusandpoorhealthoutcomes.Conversely,highlevelsofhealthliteracyare likely to enable patients and whānau to take more responsibility for themanagementoftheirhealththroughoutthecontinuumofcare(Nutbeam2000).
In New Zealand, Kōrero Mārama (Ministry of Health 2010a) has provided thebackground data that demonstrates, on a population basis, that Māori have poorerhealthliteracyskillscomparedtonon‐Māoriacrossallsocioeconomicmarkers.
Ashealth care systemsbecomemore complex, thehealth literacydemandsplacedonpatients and whānau also become increasingly complex. The changing face of healthcaremeans that patients are now expected to have amore active role in their care,developnewskillstofindandmanageinformation,understandandmanagetheirrightsand responsibilities and make the best health decisions for themselves (Nielsen‐Bohlmanetal2004).Internationalevidenceshowsthatpatients’knowledgeandskillsare usually below those demanded of themby their health system (Rudd et al 1999;Ruddetal2007).AsKohetal(2012,p.435)state,“awidechasmoftenseparateswhatproviders intend to convey in written and oral communication and what patientsunderstand”.
Thecontentandcontextofhealthmessagesissocomplexthatapersonwithhighhealthliteracyskillsinonecontextmayexperiencemomentsofpoorhealthliteracyinanother.Theseepisodesoccurwhenpatients andwhānau find themselvesdealingwith anewcontext particularly where the patient is in very poor health (Nutbeam 2009). Thephysical and social environmentof health care settings also influences the efficacy ofhealthliteracy(Rudd2013).
ThisstudydrewonRudd’sschemaofhealthliteracy(Ruddetal2004),whichexamines‘health activity’ and ‘focus’ across the health spectrum, from ‘health promotion’ to‘systems navigation’. In her more recent work, Rudd (2013) identified the keycomponents of health literacy as individual skills, health tasks undertaken, healthmaterials used, skills of providers (including the ‘oral exchange’), and the reciprocalphysical and social environment (Rudd 2013). The identification of specific healthliteracy demands in a particular context can require a full evaluation of the range ofactivitiesinvolvedinaccessinginformationandresources,howdecisionsaremadeandactionstaken,howproceduresandprotocolsareimplemented,aswellasassessingthehealthliteracyskill levelsofthepatients,whānau,andhealthprofessionals,andofthehealth service providers systems. This was outside the scope of this study, and alsoethically inappropriate, in relation to the circumstances of people facing life‐limitingillnesses.
5
Instead,thisstudyseekstoprovideanappropriateandmeaningfulexploratoryanalysisof the health literacy context for Māori in the palliative care environment. We havetalked to Māori patients and whānau, health care professionals, and key informantsaboutthelevelofknowledgeofpalliativecareserviceswithinMāoricommunities;thecharacteristics of the communication of palliative carewithMāori patients and theirwhānau; and the key factorswhich affect the ability of thesepatients andwhānau toobtain, process and understand palliative care information and services and makeinformeddecisions.Wewereinterestedinhealthprofessionals’perspectivesonhealthliteracyandpalliativecareforMāoripatientsandwhānau,andwhatthehealthliteracydemandsofpalliativecareareasasnapshotofthosedemands.Wecollectedexamplesof written information provided by different palliative care services providers andanalysedtheseusingahealthliteracyframework.
1.3 Literature review
A literature review was undertaken to address issues related to indigenous healthliteracyandpalliativecare.Thisreviewisbasedonliteraturepertainingtoadultsandutilises a person‐centred, rather than system‐oriented, view. The key findings of thereviewarepresentedhere;thecompleteliteraturereviewisattachedasAppendixOne.
Assumptions
TheMinistryofHealth’sStatementofIntent2010–2013hasakeypriorityareato“workonissuesemergingasaresultofNewZealand’sageingpopulation:improvingthehealthand independence of older New Zealanders” (Ministry of Health 2010b, p.12). Thisreportfocusesmainlyonliteratureintheadultpopulation.
Scopeandmethods
WhileMāoriarereportedfromapopulationbasistohavelowhealthliteracy(Ministryof Health 2010a) and low utilisation of palliative care (Minister of Health 2001), theapproach in the literature review acknowledges the historical shift in health literacyliterature fromaconceptof the individual ‘riskypatient’ toaviewthatacknowledgeshealthprofessionals,healthserviceproviders,andthehealthsystemashavingacriticalroletoplayinbuildinghealthliteracy(Nutbeam2009).
Theliteraturereviewfocusedonthreeaspects:
1. Identify systemic and professional barriers that inhibit utilisation of palliativecareservicesbyMāori
2. Explore how health literacy principles are incorporated into palliative carematerials(includingwrittenresources,suchaspamphlets,andresourcesontheinternet,video,etc)
3. Examine health literacy interventions in palliative care for Māori and theirwhānau.
Thissectionsummarisesthefindingsineacharea.
6
1. Identifysystemicandprofessionalbarriersthat inhibitutilisationofpalliativecareservicesbyMāori
Itisrecognisedthatgenerallyindigenouspeopleswishtodieathomeforanumberofreasons. A home environment is related to the familiarity of being cared for by theirfamilymembers, the ‘circle of life’where they are born and die, gaining energy fromfamilyandcommunityinmovingacrosstotheotherside,andinreceivingsupportforthefamilytoenablecaringtotakeplace(Ngata2005;Kellyetal2009;DeCourtney,etal2010;Hamptonetal2010).Themovetopalliativecareunitsandhospicesisidentifiedasalienintermsofhavingrulesandstructureswhichmaynoteffectivelyaccommodatethe needs of the indigenous patient (McGrath 2008; Hampton et al 2010).Notwithstanding visiting hours, the ability of specialist palliative care services toaddress the needs of indigenous populations is dependent on the knowledge andwillingnessofstaff to ‘allow’caretobeprovidedinaculturallysensitivemanner.Theprovisionofcaregivingbyafamilymemberinahospital‐likeenvironmentmayconflictwithhealthprofessionalswhoarereluctanttorelinquishcareormedicalstaffwhomayfeelasenseoffailureifsupposedlife‐prolongingtreatmentsarediscontinued(BellamyandGott2013). Inaddition, theavailabilityof space for familymemberswhowish toprovide care is limited in some institutional settings. There remains a strong call formore indigenous healthworkers to be available to support health professionalswhocare for indigenous patients. The use ofmembers of the target ethnic community inworkingalongsidepalliativecareserviceshasbeensuccessfullymodelledintheUS(Yeo2009).
2. Explorehowhealthliteracyprinciplesareincorporatedintopalliativecarematerials(including written resources, such as pamphlets, and resources on the internet,videoetc)
Materials in palliative care, although only a small part of the health literacy context,weredeemedtoratepoorlyduetotheoveruseofmedicalterminology.However,whileusing direct explanations and other cues tomake the designmore readable, such asbulletpointsandbold lettering, it isacknowledgedthatreplacingmedical jargonwithplain language alone is not sufficient to improve health literacy (Kehl and McCarty2012;MinistryofHealth2012).Therewerereferencestotheuseofadditionalformsofmedia such as video or the internet (Volandes et al 2011). Videos/DVDs have somehealth literacypotential in theability toviewthemmore thanonceorshareamongstfamily to also view. However, health information may focus primarily on tinana(physical manifestations of illness) and exclude information in relation to wairua(spiritualaspects),hinengaro(thoughtsand feelings)andwhānau(family/communityaspects)whichareofimportancetoindigenouspopulations.Internetuseisincreasingin younger populations andwhile an older personmay not be familiarwith internettechnology, a younger relative may be able to support them. In addition, there isanecdotal evidence that the younger generation are using online communication
7
methods to advocate for olderpeople, although theolderpersonmaybe reluctant tocomplain/comment(MParsons,personalcommunication,April2013).
Depending on health literacy levels, using internet search enginesmay provide userswiththeanswerstotheirquestionsorenablerefinementoftheirquestions.Forhealthprofessionals,theuseoftheinternethasthepotentialtoallowuserstobeinchargeofwhen, howandinwhichformat informationisreceived(Knappetal2011),althoughthe inaccuracyofsome internetmaterialcancreateproblems forhealthprofessionalswhoneedtocorrectmisleadinginformationpatientshavefoundonline(LoandParham2010).
3. ExaminehealthliteracyinterventionsinpalliativecareforMāoriandtheirwhānau
Althoughweintendedtoviewhealthliteracyinterventionsthroughthelensofanassetmodel,noarticlesmeasuredinformationflowasatwo‐wayprocess(EuropeanHealthPolicyForum2005).Therewasa lackofresearchmeasuring theway inwhichhealthinformationwas delivered, apart from some exploration of the usability ofmaterialsprovided. Strategies were measured based on readability or numeracy or on healthliteracylevelsofindividuals.Furtherresearchisrequiredtounderstandtheskillbaseofhealthprofessionalswhentheyconveyhealthmessages.
Indrawingonthefindingsofthisreview,itisevidentthatthestudyofhealthliteracyisstill in its infancy inNewZealand.Theunderstandingofhowtobetteraddresshealthliteracy from a health services perspective has been identified as a practical steptowards improvement. Further studies are required to investigate the capacity andcapability of health professionals and health care providers, and to support thedevelopmentofskillsbasedonadultlearningprinciplesandassessingtheoutcomesofthese.
1.4 This study
In New Zealand, the Ministry of Health’s (2010a) KōreroMārama survey report onMāoriandhealthliteracyarguedthatinsteadofviewinghealthliteracyasanissueforindividuals, with the responsibility on individuals to build their skills, the solutionrequiredaconcertedeffortfromallsectors,includingschools,governmentagenciesandthehealthcaresystem.
TheoverallobjectiveofthisresearchwastoidentifyaccessissuesforMāoriandtheirwhānau to palliative care services, from a health literacy perspective. By identifyingthese issues, this project was designed to contribute to better service delivery ofpalliativecareandimprovedaccesstopalliativecareforMāoriandtheirwhānau.
Keyareasofinterestfortheresearchwere:
1. ThewaysinwhichMāoriaccesspalliativecareservices2. CurrentlevelsofMāorihealthliteracywithregardstopalliativecare

8
3. How different factors within whānau influence the ability of Māori to obtain,processandunderstandpalliativecareinformationandservices
4. Identification of communication models which are effective in enhancing thisability.
Advisory group AnadvisorygroupofProfessorRossLawrenson,AssociateProfessorMerrynGott,andAssociate Professor Robyn Dixon provided expertise and support for the study,includingfeedbackonthisreport.
Sister project Another Māori health literacy and palliative care research study Hei Manaaki NgāKaumātuawascarriedoutbyRauawaawaKaumātuaCharitableTrustResearchTeam.
BothprojectswerepartofaPalliativeNationalJointWorkProgramme2012forHospiceNewZealand,theMinistryofHealthandPalliativeCareCouncil.
9
Section 2: Rautaki Mahi – Methodology 2.1 Research design
ThisprojectusesaqualitativekaupapaMāorimethodology,amethodologicalapproachthatincorporatesasetofprinciplesthatreflectsthetheoreticalapproachunderpinningand informing theresearchprocess (Bishop2005;Smith2005;Crametal2006).Theprinciplesare:
• locationwithinthewidercontextoftinorangatiratanga(self‐determination).Inthe context of research this principle encompasses control of research andresearch processes, participation in all levels of research, and the delivery ofinformationthatwillcontributetoMāoridevelopmentandautonomy
• connection with Māori philosophy and values and the incorporation of Māoriattitudes,language,andwaysoflivingintheworld
• awareness and critique of the dominant accepted norms, assumptions, andpower relationships and how these serve to maintain the ‘status quo’ thatprivileges the dominant (non‐Māori) community and maintains disparitiesbetweenMāoriandnon‐Māori
• thelegitimacyandvalidityofMāoriworldviewsaretakenforgrantedandseenasthenorm;kaupapaMāoriresearchseekstounderstandMāoriknowledgeandexperienceonitsownterms
• that research moves Māori from the margin to the centre, allowing Māoriconcerns to be addressed, and providing information that addresses our self‐identifiedpriorities.
2.2 Recruitment
In September 2012, huiwere held at theWhakatane Palliative Care Forum,WaipunaHospice (Tauranga), Mercy Hospice (Auckland), Hospice Eastern Bay of Plenty andHospiceWest Auckland to introduce the study and ask for support to identifyMāoripatientsandwhānauwhocouldbeapproachedtoparticipateinthestudy.Atthesametime,weaskedhealthprofessionals toparticipate in focusgroups,andaspartof thatprocesswealsoidentifiedkeyinformantsamongstthehealthprofessionals.Additionalhealthprofessionalswererecruitedthroughformalandinformalworkplacenetworks.Detailsoftheparticipantsfollow.
The two regions of Auckland and Bay of Plenty were chosen as they allowed us toexploreMāorihealth literacyandpalliativecare in largeurban,smallurbanandruralenvironments; in specialised palliative care settings (hospital and community‐basedspecialised hospice services); and in generalist services (including primary careproviders,bothMāoriand‘mainstream’).
10
Patients and whānau, whose details were supplied to us or who indicated to theirpalliative care service provider that they wished to participate in the study, wereindividually contacted by a Māori interviewer to consent to their participation. Theparticipantinformationsheet,andconsentform(inbothEnglishandtereoMāori)areattachedinAppendixFour.
2.3 Data collection
Interview questions for all participants (patients, whānau, focus groups and keyinformants)werebasedon theobjective and fourkeyareasof focus identified in theRequestforProposal.InterviewschedulesareattachedinAppendicesFourandFive.
Patients and whānau Theresearchconducted15interviewswith21people.Twooftheinterviewswerewithpeople discussing the same palliative event. Nineteen of the interviews were withwhānau carers for palliative care patients and twowere patients. All but two of thepatients that whānau carers had been caring for had died before the interview wascarriedout.Tenofinterviewswereconductedonetoone(includingonewithapatient)andtheotherfiveinvolvedmorethanoneperson(oneofwhomwasapatient).
Wherepatientandwhānauquoteshavebeen included in thisreport,eachparticipantwhoparticipatedinthegroupisnamedbytheirrelationshiptothepatient;forexample(wifeanddaughter).Inallcasesthequotereferstoonepalliativeeventaboutwhichthewhānaucarersweretalking.
Interviews were conducted by Māori researchers. The semi‐structured interviewsgenerally tookplace in the homes of participants,whether inAucklandor theBay ofPlenty,andtookbetween30minutesand2hours. Allbutoneoftheinterviewswererecordedandtranscribed.
During thepatient andwhānau interviews,wegathered informationon theway theyusedpalliative care services, how theyobtained informationabout the services,whatthe positive aspects of the palliative care services providedwere andwhat could beimproved.
Theterm‘healthliteracywasnotusedwithpatientsandwhānauasitisanewtermandnotwellknownbythegeneralpublic.Instead,proxytermssuchas‘communication’and‘information’wereused.
Allbutoneoftheinterviewswererecordedandtranscribed.
11
Palliative Care Providers Tenfocusgroupswereheldinvolving54peoplefromorganisationsprovidingpalliativecareservices.FocusgroupswerefacilitatedbybothMāoriandnon‐Māoriresearchers.
Focus groups took place with staff from four hospices, two Māori palliative careproviders, one primary healthcare service, GP practices, the Cancer Society, and onegeneralhospital.Ofthesegroups,sevenprovidedspecialistpalliativecareservicesandthreewereprimarypalliativecareproviders.
Thefocusgroupswerewellattended,with15participantsinonegroup.Generallythefocusgroupsizewasapproximatelyfivepeople.Inallthefocusgroupsexceptone,therewasamixtureofnursesandotherhealthprofessionals.Onefocusgroupwasexclusivelycomprisedofspecialistnursesworkinginasecondarypalliativecareservice.
Themaincriterionforparticipatinginafocusgroupwasthatthehealthprofessionalsparticipatingwereinvolvedinprovidingprimaryorspecialistpalliativecare.
Focus group participantswere asked for their perspectives and understanding aboutMāori access to palliative care services; health literacy and palliative care for Māoripatients and whānau; the health literacy demands of palliative care; and how theyconsidered that services and health professionals took these health literacy demandsintoaccountwhenworkingwithMāoripatientsandwhānau.
Acopyofthefocusgroupinformationletter,consentformandinterviewscheduleareattachedinAppendixFive.
Allfocusgroupinterviewswererecordedandtranscribed.
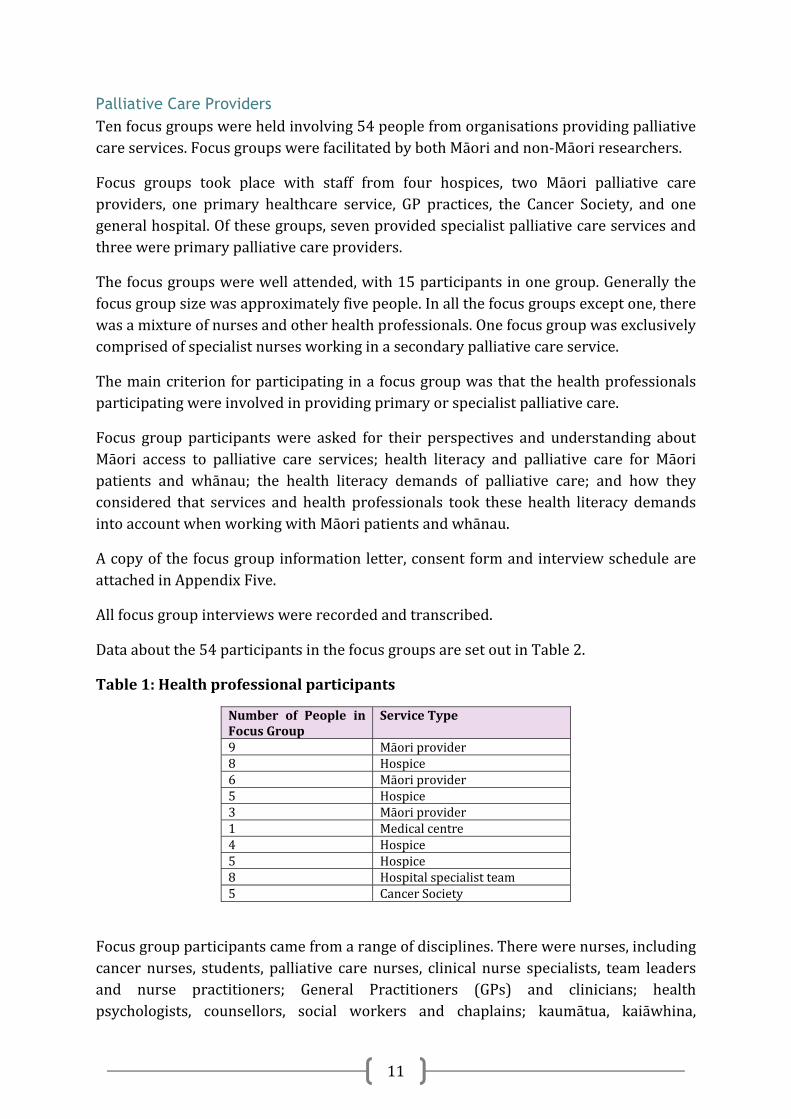
Dataaboutthe54participantsinthefocusgroupsaresetoutinTable2.
Table1:Healthprofessionalparticipants
Number of People inFocusGroup
ServiceType
9 Māoriprovider8 Hospice6 Māoriprovider5 Hospice3 Māoriprovider1 Medical centre4 Hospice5 Hospice8 Hospitalspecialistteam5 CancerSociety
Focusgroupparticipantscamefromarangeofdisciplines.Therewerenurses,includingcancer nurses, students, palliative care nurses, clinical nurse specialists, team leadersand nurse practitioners; General Practitioners (GPs) and clinicians; healthpsychologists, counsellors, social workers and chaplains; kaumātua, kaiāwhina,

12
kaitakawaenga, kaiatawhai and navigators; and managers, administrators andcoordinators.
Duringthefocusgroups,someparticipantswhowerehealthprofessionalsalsospokeoftheir experiences of providing palliative care aswhānau carers rather than as healthprofessionals. From a kaupapa Māori perspective, this reflects that whānau have anumberofroles,includingasprofessionalcarers,membersofawhānauprovidingcareforanotherwhānaumemberwhoisdyingand/orasadvisorstootherwhānaucarersinsimilarsituations.OnepatientattendedaMāoriservicefocusgroupwithhercaregiver.
Key informants Semi structured interviews were completed with six key informants: a medicalspecialist, a service leader involved in developing culturally specific responses topatients, two Māori service managers, and two Māori health team leaders. Theseparticipantswerechosentobringamanagementfocusandabroaderoverviewofthepalliativecareserviceenvironmenttotheresearch.
Thesemi‐structuredinterviewswerecarriedoutbyMāoriandnon‐Māoriresearchers.A copy of the interview schedule is attached in Appendix Five. All key informantinterviews were recorded and transcribed. Key informants were asked similarquestions to the focus groups: perspectives andunderstanding aboutMāori access topalliativecareservices;perspectivesonhealthliteracydemands;andhowservicesandhealth professionals took thesedemands into accountwhendeliveringpalliative careservicestoMāoripatientsandwhānau.
DataaboutthekeyinformantsissetoutinTable3.
Table2:Keyinformants
KeyInformant
Discipline
1 Māoriservicemanager2 Non‐Māoriserviceleader3 Māorihealthteamleader4 Māoriservicemanager5 Māorihealthteamleader6 Non‐Māorimedicalspecialist
KeyinformantscamefromarangeofserviceprovidersincludingDistrictHealthBoards(DHBs),hospicesandcancerservices.
Written resources Writtenresourcesareusedbypalliativecareproviderstoinformpatientsandwhānauof the range of services available. These resources represent a critical health literacy
13
demandplacedonpatientsandwhānau.Palliativecareproviderswereaskedat focusgroups and key informant interviews to supply written information about palliativecareservices thatprovidersgive toMāoripatientsandwhānau.This informationwasusedasasnapshotofthehealthliteracydemandsplacedonpatientsandwhānauwhenaccessingpalliativecareservices.
A total of 42 written resources from palliative care providers located in the Bay ofPlentyandAucklandwerereviewed.Thefollowingprovidedinformation:
4hospiceorganisations 1DHB 1WhānauOraprovider 1nursingservicesprovider.
A listof the resourcesassessed isattachedasAppendixTwo.Theresourcesaimed toexplainpalliativecareservicesandconsumerrightstopatientsandwhānau,andwereevaluated according to criteria such as vocabulary, apparent purpose and audience,inclusion ofMāori concepts, readability and resource type. The evaluation process isoutlinedbelowin‘Writtenresourceanalysis’.
2.4 Data analysis
Interviewsweretranscribedandanonymisedforanalysis.Ageneralinductiveapproachwastakentoanalysingtheinterviewandfocusgroupdata(Thomas2006)toallowthedominantandsignificantthemestobeinterpreted.Thisapproachwaschosenbecauseof its specific focus on analysing exploratory and evaluative data which have beenshapedbyastraightforwardsetofaimsandobjectives.Ouranalysiswasguidedbytheresearch aim of understanding Māori patient and whānau access to primary andspecialistpalliativecareservicesfromahealthliteracyperspective.
The interview transcriptswere analysed to elicit key concepts and recurrent themes.The key concepts and themesweredrawnout by referencing themain objective andkeyareasofinterestofthestudy,aswellasnewissuesthatwerenotedinthedata.Adetailedindexofcodes(categorieswithshorttextdescriptors)wasdevelopedandthetranscripts codedandre‐codedmanuallyuntil all the transcriptshadbeencompletedsatisfactorily. The codeswere then organised into themes reflecting the key areas offocus.
Data fromeachparticipantgroup,patientsandwhānau,healthprofessionals,andkeyinformantsweregivenequalweightduringtheanalysiswiththesameprocessfollowedfor all. As the themes were developed, it became clear that there was generallyconsistency across all three groups. Where differences emerged, this has beenhighlightedinthefindingssection.
14
Asmentionedearlier,duringthefocusgroupssomehealthcareprofessionalsspokeoftheir experiences aswhānau carers and onepatient attended a focus groupwith hercaregiver. Throughout the report, we have identifiedwhether data came fromMāorihealthprofessionalsorMāorihealthserviceswhereverthiswasclearlyidentifiedbytheparticipants,butMāorialsoattended thehospiceandhospital focusgroupssoquotesfromthosesourcescannotbepresumedtobenon‐Māori.
Rigour Trustworthinessandreliabilityofthegeneralinductiveapproachwastestedbysharingtranscripts among the research team, and using an agreed framework of codes anddefinitions to ensure coding consistency.Thiswas further testedby sharing analysedtextsamongsomeoftheresearchteambothindividuallyandthroughtwohuitodiscussthefindings.
Thecategoriesandthemesweretakenbacktotheresearchcommunitiesinaseriesoffive hui for discussion and validation inMarch and April 2013. These hui were wellattended,andgeneratedmorestories,whichwereconsistentwiththecategoriesratherthan producing additional data. None of the categories were challenged by the huiattendees, who generally approved of the themes that had been developed from thedata.
Written resource analysis The42writtenresourcesthathadbeencollectedfrompalliativecareproviderslocatedintheBayofPlentyandAucklandwereanalysedusingcriteriaderivedfromMinistryofHealth(2012)andWorkbase(2013)reportsonaspectsofhealthliteracyandeducation.Thesefocusedonaspectssuchas:
howclear,orimplied,thepurposeoftheresourcewas theaudiencefortheresource,whetherspecifiedorimplied resourcetype thepointinthepalliativecareprocessatwhichtheresourcewasaccessed readability vocabulary language and text features e.g. layout, white space as well as use of visuals
(whichhelpcreatecontextualmeaning) inclusionofMāoriconceptsandvalues,suchasreferringtoTeWhareTapaWhā.
For each resource, therewas an evaluative summary produced onwhatworkedwell(how the resourcemighthelpbuildhealth literacy) anda summaryofwhat couldbeimproved (in terms of purpose and relevance, usability/accessibility/navigation, andoverallbuildingofhealthliteracy).For some resourcewriters, the cornerstoneof resourcedevelopment is readability.AnumberofwritersrefertoadultNewZealandersreadingatthe‘readinglevel’ofa7to10yearold.Thesesortsofgeneralisationsareneitheraccuratenorhelpful.Adultsarenot children and using children’s reading ages to determine how to write patient

15
materialsgivesafalsesenseofsecurity.Thesereadingagesarebasedonvocabulary,forexample what vocabulary a 7 year old might be expected to read. Adults with lowliteracy skills may have smaller reading vocabularies than some children. However,adults have greater life experience than children, and therefore are more likely tounderstandconceptualmatters involvingcomplexvocabulary ifproperlyexplained tothem.
Readabilityformulaeproducereadabilityscoreswhichmeasuretwothings–sentencelength and number of multisyllabic words. Readability formulae are based on thepremise that long sentences and words with multiple syllables are harder tounderstand.Toreducereadabilityscores(thehigherthereadabilityscore,thehardertoread the document is thought to be), short sentences and single syllable words arerecommended.
In health situations, it is not possible to eliminate commonly used multiple syllablewordssuchaspalliative,services,andinformation.Shorteningsentencesandreplacingmultiplesyllablewordswillnotguaranteethatareaderwillmakesenseofthetext.Inahealthcontext, itmaybemoreusefulandrelevant tohavea ‘higher’readabilityscorebecauserequiredterminologyisincludedandexplanationsofthosetermsareprovided.Readabilityhasaplaceinreviewingdocuments.Usingeverydaylanguageandcommonwordswhereappropriateisagoodidea.However,readabilityalonewillnotensurethataresourceiseasiertounderstandorisuseful.
Assessing health literacy The health literacy skills of individual patients and whānau who participated in thisresearchwerenot formallyassessed.However,wedid identifya listofhealth literacydemands(generatedbydatacollectedfrompatients,whānau,focusgroupparticipantsandkeyinformants),whichneedtobeconfirmedwithfurtherresearch.
Thedecisionnot toassess individualhealth literacy levelswasbasedonanumberoffactors.Themostcommonlyusedassessmenttests(RapidEstimateofAdultLiteracyinMedicine andTest of FunctionalHealth LiteracyAssessment) havebeen critiqued forbeing generic, focused on reading only, and for taking a deficit view of patients(Workbase 2013). The deficit model of health literacy, where patients are judged asposing risks to health professionals and health care organisations, has been largelyovertakenbyasystemsapproach,definedasanunderstandingthathealthliteracyis‘aninteraction between the demands of the system and the skills of the individual’(Nielsen‐Bohlman et al 2004) and that health professionals and healthcareorganisationshavearoleinbuildinghealthliteracy,bothbyreducingthehealthliteracydemandsplacedonindividualsandbybuildingindividuals’healthliteracyskills(Kohetal2012).
TheSingle ItemLiteracyScreener (how frequentlypeoplegetassistancewithreadingwritten materials) (Morris et al 2006) was used as part of the patient and whānauinterviews. However, we decided not to use the data collected from this question as
16
palliative care service providers had already advised us that their written materialswerenoteasytoreadandwehadconfirmedthiswhenanalysingthematerialssupplied.
Wealsohadaproxymeasureofhealthliteracyinthat,fromapopulationbasis,75%ofMāori women and 80% of Māori men have low health literacy (Ministry of Health,2010a).
2.5 Ethics
Ethical approval was given to this project by the Multi‐Region Ethics Committee,referenceMEC/12/EXP/050.
2.6 Limitations
Thiswasaqualitative,exploratorystudythatutilisedanappropriatelysmallpurposivesamplethatwasbroadlyaccessedandminimallydefined.Thismeansthat:
There was no assumption of ‘representative’ or ‘population sampling’; theresearch was specifically aimed at in‐depth exploration of the views ofparticipants in thepalliativecaresystem,especially inrelation toMāori,notattrying to make ‘objective’ generalisations. Further research may build on thisqualitativebasetoexplorelargergroupsamples.
The ‘opt‐in’ recruitment strategyused for patient andwhānauparticipants (inthatparticipantschosetorespondtoinformationabouttheresearchandoptintoparticipating)meansthat it ispossible that thewhānauwhorespondedtoarequesttoparticipateinthestudyhadextremeexperiences(eithergoodorbad)ofpalliativecareservices.
Focusgroupparticipantswerenotspecificallyaskedtoidentifytheirethnicityorprofession,soconclusionscannotbedrawnaboutMāori‐specificorprofession‐specificviewpointsamongthehealthprofessionals.Inhindsight,collectingsuchdata would have been useful for the analysis, although transcribing with thislevelofaccuracyabouteachspeakerwouldhavebeenchallenging.
Primaryandspecialisthealthprofessionalswerenotidentifiedseparately,whichhasreducedtheclarityaroundaccessandpracticeissues.
Somefocusgroupparticipantsspokeabouttheirexperiencesaswhānaucarers,but thiswasnotalwaysable tobecapturedseparately.Furthermore,apatientandcaregiverattendedonefocusgroupasparticipants.Thesewerenotcountedinourpatientandwhānaunumbers.
Thisstudydidnot involvedirectobservationof interactionsbetweenpalliativecare providers and patients and whānau. This was not the purpose of theresearch, and would have required very different ethical and logisticalconsiderations,butmayhaveaddedtotherichnessofthefindings.
Recommendationsfromthestudyrequirefurtherresearchtoconfirm.

17
ItshouldbenotedthatitwasbeyondthescopeofthisstudytoinvolveMāoripatientsandwhānauwhohadnotusedhospiceandotherpalliativecareservices.Forexample,wedidnot interviewMāoripatientsandwhānauwhohaddeclinedareferral totheseservices, or were unaware that the services existed, although health professionalsdiscussed some of their experiences of service refusal. It is not known from a directaccountwhatthebarriersforthesetypesofMāoripatientsandwhānaumightbe.
Uniformity of focus group data The interviewerswhomanaged the focus group data collection noted that therewaslittleornodissentduringeachof the focusgroups.Thismayhavebeenbecauseof aperceived risk to the health professionals individually or to the organisation of being‘found’tobe‘culturallyunsafe’,withtheparticipantsdesiringtopresentaunitedfrontof excellent, professional service delivery. In debriefing after each focus group, teammembers frequentlydescribedasenseof initiallybeingtoldwhatwas ‘correct’ratherthanwhathappenedinpractice.Thiswasaddressedinthefocusgroupsbyaskingforexamplesfrompractice,whichtendedtodeepenanddiversifythediscussion.Whenthisoccurred,someofthegroupwouldceasetoparticipate,perhapsindicatingdissent,butnothingwas overtly indicated or said. Therefore, the internal uniformity of the focusgroup data should be regarded as a limitation and further research carried out toconfirmfindings.
18
Section 3: Nga Kitenga - Findings Thefindingsfromthisstudyhavebeenorganisedintothefollowingthemes:accessingandutilisingpalliativecareservices;healthliteracydemands;healthliteracypractices;barriers;andnavigatingthepalliativecaresystem. Inaddition, threeareasof findingswereidentifiedas‘stand‐alone’categories:thediscussionsthattookplaceamonghealthprofessionalsabouttheconceptofhealthliteracyinpractice(section3.1),theanalysisofwrittenresources(3.2),andcommunicationprocesses(3.8).
Verbatim quotes from anonymised transcripts are included to illustrate themes andcategories, fromnumberedpatientandwhānau interviews(denotedwithrelationshipof carer topatient included), focusgroups (denotedwith typeof serviceand locationincluded),orfromkeyinformantinterviews(denotedwithroleandlocation).
ThisstudydidnotseektoevaluateMāorisatisfactionwithpalliativecareservices,andtherewasjustasinglesub‐questionthataskedpatientsandwhānautocommentonthestrengthsoftheirinvolvementwithpalliativecareservices.However,itisinterestingtonote, to set the scene of the findings, thatmost of the patients andwhānau reportedpositiveexperienceswiththeirprovider(s),particularlyinrelationtoparticularhealthprofessionalsandtheprovisionofequipment.
Everythingwasreallygood,actually.Itwas–yeah,thenurses,actually,theywereverymindfulandrespectfulofpeopleingeneral.(Wifeanddaughter)
Thehospicetheyboughteverythingweneeded.Igotahospitalbed...whenIwashaving real trouble and needed to clean her up. I said, “I just can’t handle thisdoublebedthatshe’sin,”andso[hospice]gavemeahospitalbed.(Husband)
But they immediately – itwasalmost like “Well, grab your supermarket trolley,we’re going out the back andwe’re piling everythingwe can fit in your truck.”Everypossible thing thatwe thinkyou’llneedorwillneed,ormightneed,we’regonna put in there and . . . our sun room became the ‘any‐sort‐of‐medical‐equipment‐you‐could‐get room’ for about, it must have only been about threeweeks.(Wife&stepdaughter)
Threewhānaudiscussedverydistressingexperiencesofpoorcare,allofwhichinvolvedgeneralhospitalcareratherthanspecialistpalliativecare.
Ithasbeenhell.Ididn’tknowwhatpalliativecaremeant–Iguesseditmeantdyingbutwhatdoesitmean?Nooneexplainsanything,theygiveyoupamphlets.Butnoone says this iswhat thisonedoesand this iswhat thisonedoes–hospital,GP,publichealthnurses,districtnurses,hospice,chemist...Andmostimportant,whattheydon’tdo–“Oh,wedon’tdothat”.WellwhodoesandhowdoIfindoutaboutthatandwhodoIhavetotalktoaboutthemandwhenandwhere?...Thereissomuchinformationanditissoconfusing.(Wife)
19
Itisnoteworthythatalthoughthepatientsandwhānauidentifiedagenerallypositivepalliativecareexperience,manyofthefindingsindicatethatcarewaslessthanideal.Thisisdiscussedfurtherinthefinalsectionofthisreport,andisidentifiedasatopicrequiringfurtherresearch.
3.1 Health professionals’ concepts of health literacy in practice
During the focus groups and key informant interviews, healthcare professionalsengaged in conversations about their understanding of health literacy. Discussionsincluded health literacy as a component of communication between the health careprofessional and the patient and whānau, and particularly the need to engageeffectively:
. . . engagewhere they’re at or their level of education and understanding andknowledge . . . and that’s different for each person. (Hospital‐based serviceAuckland)
Ithinktoo,it’showyouputthings,notmakeitsoundsoclinical,you’vegottoturnthewordsaroundtotheirunderstandingandgettheirpointaswell,seewhattheythink.(MāorihealthserviceBoP)
It’swalkingthroughthemwiththem,andit’snotaboutgivingthemapamphletonmorphine. It’s saying to them, “This iswhat you’redoing; this iswhatmorphinedoes.Howaboutlet’strygivingherthislittlebitinthismanyhoursandseehowwego?”(MāorihealthprofessionalBoP)
It’sthedifferencebetweenwhatwesay,betweenspokenandwhat iswrittenandwhatisunderstoodandhowpeoplegraspwhatthatactuallymeansforthemandtheirfamily . . .healthliteracyisjust–weliveandbreathethatwhetherwethinkaboutasaconceptornot.(HospiceAuckland)
Some health care professionals reflected on the challenges to their existing practice,particularly:
. . . developing our own ability around communication skills. (Hospital‐basedserviceAuckland)
...learningtolisten,notalwaystalk...(MāorihealthprofessionalAuckland).
...increasingtheculturalawareness,theculturalsensitivityofthepeoplethatareinthepalliativecareteam.(GPBoP).
The participants acknowledged the additional health literacy difficulties for patientsandwhānauthatarisebecauseoftheshock,griefandanxietyassociatedwithreceivingpalliative care services. These emotions, combined with the health literacy demandsassociatedwith intensivephysical health careneeds, create a complexhealth literacyenvironment.

20
In this next quote, a participant describes very well the complex health literacydemandsplacedonpatientsandwhānauandtheroleofthehealthprofessional:
Theyhave toprocessa lotof information froma lotofhealthprofessionals,andsometimes the information that they’re processing is conflicting . . . our role isactually trying to orchestrate some consistency in the information that’s beingprovidedtothefamilyandtothepatient.(Hospital‐basedserviceAuckland)
3.2 Written resource analysis
Thereviewofthewrittenresourcessuppliedbypalliativecareprovidersfoundthattheresources reviewed used formal language and structures (e.g. did not use directlanguage such as ‘you’ or ‘we’),were passive in tone, included unfamiliar vocabularywithout explanations, had high readability scores and contained large blocks of text.Sometimestheaudienceandthepurposeoftheresourcewereclear.Inotherresources,theywereimpliedorabsent.
Sometextshadgoodheadingsandsubheadingswhichassistedinnavigatingthetexttofind particular information. However, in some cases, the lack ofwhite space and thedifficultvocabularymadetheresourcedifficulttoread,notwithstandinggoodheadings.
Anumberofterms,suchas‘complementarytherapies’,wereusedinmaterialswithoutexplanation.Othertermswereconceptualorrequiredwhānautoinferwhatthetermsmightmean—forexample,integrity,respect,‘circlesofsupport’,and‘practicalmatters’.
FewpublicationsreferredtoMāorivaluesandconcepts.Thosethatdidwereresourcesdevelopedby twoorganisations, one aMāori provider and theother apalliative careservicesproviderwhichhadaMāoristaffmember.
Anumberofhospicesprovided ‘communicationbooks’,whichwere supposed tohelpfacilitate clear communication processes by enabling all health care professionals,patientsandtheirwhānauwritenotesandquestionsintheoneplace.Onehadastickeron the front coverwith the24hour contactnumbers for the staff.Noneof thebooksincludedexamplesofhowwhānaucouldusethecommunicationbook.
Some services provide a lot of information towhānau all at one time (in a folder orenvelope)anditishardforwhānautoseetherelevanceofmuchofthisinformation,e.g.aWorkandIncomepamphletwhere the firstserviceoffered is toassistpeople togetintowork, or a pamphlet about eye donation.One hospice had awelcome letter thatexplained towhānauhow they could use the information in the folder. Although thislettercouldbeimproved,itwasagoodexampleofhelpingareadertounderstandothermaterialtheyaregiven.Otherservicesalsohadlettersbutthesedidnotprovideaguidetothecontentofothermaterialsowereevaluatedasbeingredundant.
21
Butallthehandoutsandeverything,thebookletandthatcamewellbeforehewasdiagnosed.Yeah,sothatwhentheyfirstcameouttoassesshim,whentheyfirstgotthecall,that’swhenalltheinformationcame.(Wife&daughter)
Oftendifferent typesofdocuments(e.g. informationand instructions)werecombinedwithoutmaking it clearwhen therewas a transition from one type to the other. Forexample, a text might start off providing information and then move to givinginstructions.
Consentformswereevaluatedasbeingparticularlydifficulttounderstand.Someoftheforms contained information about services the hospice did not provide, includinginformationaboutsocialservicesandenduringpowerofattorney.
Participantsgenerallyagreedthattheefficacyofwrittenresourcesreliedonthequalityoftherelationshipbetweenthepatientandwhānauandthehealthprofessional,whichneedstobecharacterisedbyeffectivecommunication(discussedfurtherinsection3.8).
Health professional and key informant interviews suggested that providing anopportunitytodiscussresourcesattimesmightbequitedifficult.
Wedon’thavethetimeIguess.Andatthetimewegive[information]tothemwedon’thavethetimetogothroughit,soit’softenjustleftthere;whethertheyreaditevenisdebatable.(HospiceBoP)
Yeah Imeaneducation isahugecomponentofourwork. . . .thereforeonecouldassume thatwe should be spending themajority of our time educating, but theclinicaldemands[aretoohigh]...(Hospital‐basedserviceAuckland)
Therewereoftenconflictingneedstoengagewiththepatientandwhānau,conductaninitial assessment, and providemandatory information such as Health and Disabilityliterature,aswellasanagreementtoreceivecare.Someparticipantsidentifiedthehighhealthliteracydemandsthatformedbarrierstoachievingeffectiveengagement.
The nurse does the initial visit and she will give the patient and whānau aninformationbooklet,orfolderwithlotsofdifferent–Itwillhavetheagreementtocareinitanditwillhaveinformationabouttheserviceandtheywilltalkaboutallthe different aspects of the service and do an initial assessment. (SocialworkerAuckland)
Whenyougo to the initialassessmentyouhaveabigenvelope thathasgotstuffaboutthehospiceandthenrightsandeverythingyoucanimagineandIhavesometimereadingit,butIdon’tthinkitgetsread.(HospiceAuckland)
Oftenyougivepeoplelotsofstufftoread,butwhenyougobackthenexttime,notonlycantheynotfind it,theydon’tevenknowthatthey’vehad itandIdofeelasthoughit’saburdenforthemoften.It’sareallybigaskforthemtogetthrougha

22
whole lotofwrittenmaterialwhen they’re strugglingwith complexityandoftensuddenbadnews.(HospiceBoP)
Thefindingsfromthesetwocategoriesarerevisitedthroughoutthefollowingthemes,andareparticularlyusefulinunderstandingthecontextofhealthliteracydemandsandpatientandwhānauresponsestothese.
3.3 Accessing and utilising palliative care services
Thisthemeincludesthepathwaysexperiencedbyourpatientandwhānauparticipants,the timelinessof their referral topalliativecare,health literacydemands,anddiseasemanagement literacy. This latter term refers to the specific knowledge and skillsrequiredtocarryoutassessmentsandtasksrelatedtothepatient’smedicalneeds.
Access pathways Asalreadynoted,theNewZealanddefinitionofpalliativecareis:
Careforpeopleofallageswithalife‐limitingillnesswhichaimsto:
1. Optimise an individual’s quality of life until death by addressing the person’sphysical,psychosocial,spiritualandculturalneeds.
2. Support the individual’s family, whānau and other caregivers where needed,through the illness and after death. (Palliative Care subcommittee: NZ CancerTreatmentWorkingParty2007)
Achievingtheseaspirationsreliesonanumberoffactors,includingaccesstopalliativecare and the timeliness of referrals, aswell as the overall provision of palliative careservices.Thispartofthereportlooksataccessandtimelinessofreferrals.
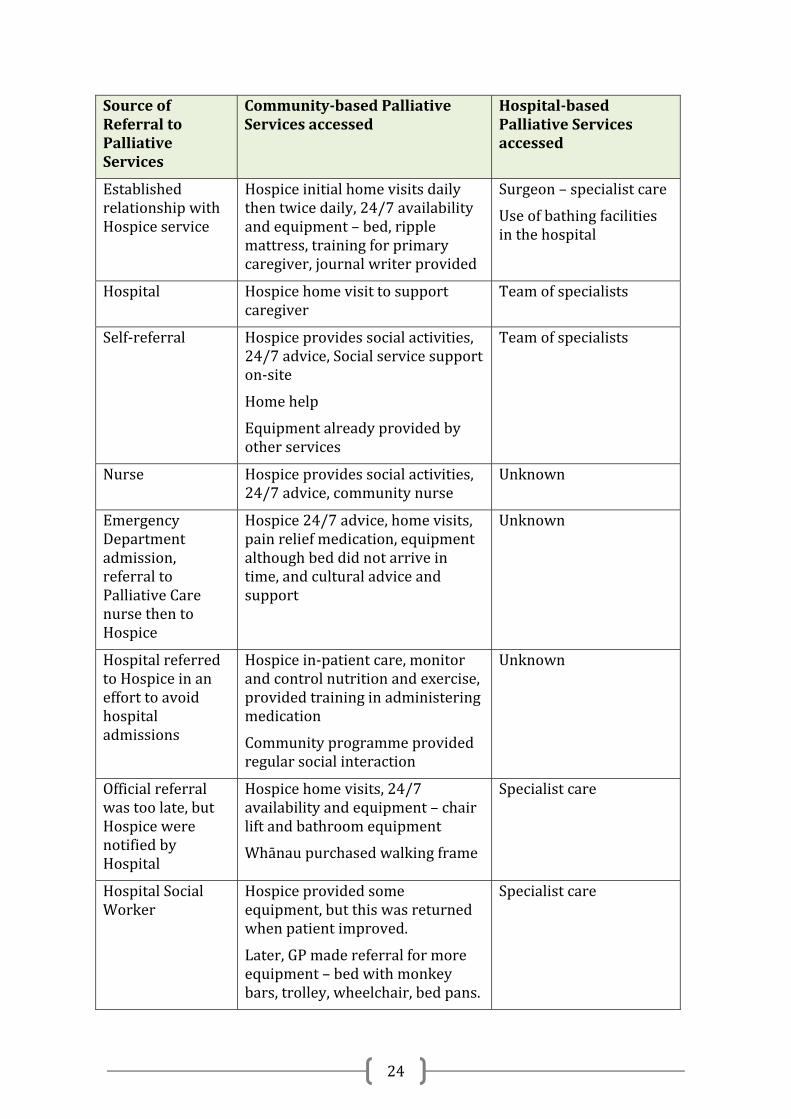
Anoverviewofthedetailsofreferralsandservicesaccessedby15oftheparticipantsisset out in Table 4. Not all participants wanted to discuss access pathways, and theinterviewersdidnotinsistontheinformation.

23
Table3:Individualpatientpathwaysandservicesaccessed
SourceofReferraltoPalliativeServices
Community‐basedPalliativeServicesaccessed
Hospital‐basedPalliativeServicesaccessed
Hospital Hospicehomevisits
Patientalreadyhadequipment
Specialistcare
Self‐referral Hospicehomevisits,respite,24/7availabilityandequipment
Pastoralcommunitynursinginhospice
Specialistcare
Hospital Limitedhospicecare,asineligiblewhilstunderspecialistcare
PastoralCommunitynursing
Specialistcare,noreferralforhomefollow‐upafterdischargefromhospital
Hospital Hospiceinitialhomevisits,24/7availabilityandequipment–bed,wheelchair,andwalkingframe
Ambulance–24/7availability
Resthomeforfinalmonthoflife
Oncologist
Chemotherapy
GeneralPractitioner(GP)/Hospital
GPconsultationandadvice
Hospicehomevisits,24/7availabilityandequipment
Homehelp
Specialistcare
Chemotherapy
Cancernavigator GPconsultationbutpooradvice
Chiropractoradvice
Nebuliser(AsthmaFoundation)Hospiceprovidedsomeequipment,andmade2homevisits
Otherequipmenthiredbywhānau
Specialistcare
Whānaumemberahealthprofessional
Hospicedailyhomevisits–painreliefinjections,2hourdaystayandlongerrespiteoptionsoffered
Equipment:chair,mattress,personalcareitemprovided,showerrailprocuredfromotherwhānau
Physiotherapisthomevisit,exercisesbutnohomeassessment.
Specialistcare
24
SourceofReferraltoPalliativeServices
Community‐basedPalliativeServicesaccessed
Hospital‐basedPalliativeServicesaccessed
EstablishedrelationshipwithHospiceservice
Hospiceinitialhomevisitsdailythentwicedaily,24/7availabilityandequipment–bed,ripplemattress,trainingforprimarycaregiver,journalwriterprovided
Surgeon–specialistcare
Useofbathingfacilitiesinthehospital
Hospital Hospicehomevisittosupportcaregiver
Teamofspecialists
Self‐referral Hospiceprovidessocialactivities,24/7advice,Socialservicesupporton‐site
Homehelp
Equipmentalreadyprovidedbyotherservices
Teamofspecialists
Nurse Hospiceprovidessocialactivities,24/7advice,communitynurse
Unknown
EmergencyDepartmentadmission,referraltoPalliativeCarenursethentoHospice
Hospice24/7advice,homevisits,painreliefmedication,equipmentalthoughbeddidnotarriveintime,andculturaladviceandsupport
Unknown
HospitalreferredtoHospiceinanefforttoavoidhospitaladmissions
Hospicein‐patientcare,monitorandcontrolnutritionandexercise,providedtraininginadministeringmedication
Communityprogrammeprovidedregularsocialinteraction
Unknown
Officialreferralwastoolate,butHospicewerenotifiedbyHospital
Hospicehomevisits,24/7availabilityandequipment–chairliftandbathroomequipment
Whānaupurchasedwalkingframe
Specialistcare
HospitalSocialWorker
Hospiceprovidedsomeequipment,butthiswasreturnedwhenpatientimproved.
Later,GPmadereferralformoreequipment–bedwithmonkeybars,trolley,wheelchair,bedpans.
Specialistcare
25
Timeliness of referral Mostwhānauandhealthcareprofessionalsexpressedfrustrationandgriefatthelackoftimeliness of patient engagement with palliative care services. Some whānau werereferredvery late topalliative care servicesand thepatientoftendiedwithina shortperiodoftimefollowingthereferral.Thisoccurredinonecasenotwithstandingthefactthat the patient had a long term condition and was frequently hospitalised. Thefollowingquotes illustrate threedifferent scenarios related to lateaccess topalliativecare.Thefirstrelatestoadelayintheinitialdiagnosisoflife‐limitingillness,thesecondquotereferstoalackofreferralfromatertiarymedicalservice,andthethirdreferstowhānauresistancetoreceivingpalliativecare.
WeweretoldontheMonday,IbroughthimhomeontheWednesdayandhepassedontheFriday.(Daughter)
YesterdayaMāoripatient Iwent to see,hashad cancer formonthsand shehasbeenknowntobepalliativeformonths,but[weare]justgoinginnowandthatisprobablywhyitissoawful,becauseIhaven’thadmonthstobuilduparapportandthenyouaregoinginandsayingmum’sgotdays,justbringthisweddingforward,or,yeah,becauseitissolate.(HospiceAuckland)
The other thing that I’ve found is that often families don’twant us.They’re thefamiliesthatwereceivereallylateandthey’rethepatientswhoareliterallydyingandwemight–there’saheckofalotofhardworkgoesoninthatinitialtime,buttheirresistancetousisverystrong.Sowehavetotryandbreakdownthatbarrierandindoingso,Imeanbythetimewedoit,thepatient’sdied.(HospiceAuckland)
Thereasonsforthesedelayswerenotdiscussedwithinthisstudy,butindicatetheneedforfurtherresearchintothepointswheretimelinessisaffected.
This finding of late referral is consistentwith the literature (Davis 2006;Ministry ofHealth 2013), but requires further analysis to ascertain the systemic, organisational,individualandwhānauinfluencesonlackoftimelyaccesstohealthservicesforMāori.Someofthesearediscussedlaterinthereportasinternalfactorsthatactasbarriersforwhānau.
3.4 Health literacy demands
Wedidnotdirectlyaskpatientsandwhānauwhathealthliteracydemandswereplacedonpatientsandwhānaubecause the term is relativelyunknown.Wedidaskpatientsand whānau what they had to do to find out information. We directly asked healthprofessionalsaboutthehealthliteracydemandsplacedonpatientsandwhānau.Threecategories of health literacy demands, based onRudd and colleagues (2004) schema,were developed from both explicit statementsmade by patients andwhānau, healthprofessionalsandpalliativecareserviceproviders,aswellas implicit references from

26
patientsandwhānau.Thecategoriesweremedicines,providingcaretothepatient,andnavigatingthepalliativecaresystem.
Each category was divided into knowledge and tasks. The knowledge component iswhere patients and whānau had to “obtain, process and understand information”(Ministry of Health 2010a) about palliative care, either from health professionals,palliativecareservicesprovidersorothersources.Thetaskcomponentswerethetasksthatpatientsandwhānaureportedtheyhadtodotomeetthehealthliteracydemandsofpalliativecareservices.
The health literacy demands were found to be substantial and complex, requiringproblemsolvingandresourcefulnesson thepartofpatientsandwhānau.A full list isprovidedinAppendixThree.
The emotional climate Theemotional climateofpalliative care creates anadditionaldemanding layer for analreadycomplexhealthliteracyenvironment.Theparticipantsdescribedtheadditionalhealthliteracydifficultiesforpatientsandwhānauthatarisebecauseoftheshock,griefand anxiety associated with the knowledge that a whānau member is dying, thetimeframesaroundreceivingthatinformation,andreceivingpalliativecareservices.
You get the: “Ohwell,we can’t do anythingmore.Do you have any questions?”You’vejustbeentoldthatyourlovedoneisgoingtopassawayshortly.Doyouhaveanyquestions?Well–youknow?Allwithinthatfiveminutes.(Daughter)
Iwastryingnottocry.TherewasastageIsaid,“It’snotthenurses’fault.I’mnotblamingthem.”I’mexhaustedandamstrugglingtolookatthenurse.I’vebecometeary.I’vetriedsohardnottocryinfrontofmybeautifulfather.(Daughter)
Ithink italsoshowswhatbigdemandspeopleandtheirwhānauhavewhentheygetadiagnosislikethat.Theyhavetotakeonboardsomuchinformationandtheknowledgeoftheir lovedonestimebeing limitedand I justthink it is justahugethingforanywhānautocometotermswithandthenontopofthatwehavegotallthehealthprofessionals,different environments,and the jargon,differentpeoplethat come in, learninghow todowound care,ormaybe stoma careoryou, it ismindbogglingwhen you thinkofwhatpeoplehave todo. (Māorihealth serviceBoP)
Howthewhānauchoosetoapproachtheresponsibilitiesofcaregivingisanotherfactorthatinfluencestheemotionalclimateinwhichhealthliteracyoccurs.Thisisparticularlyimportant during communication with health professionals about the care andtreatment of the patient. Having a single spokesperson for thewhānau increases theresponsibilityandworkload for thatperson,andhas thepotential tocreateproblemsforthatperson.However,itistheperceptionofsomehealthcareprofessionalsthatthisisthemethodofcommunicationpreferredbypatientsandtheirwhānau.
27
AndIsaidtoher,“Reallyyoucannotdoitonyourown.Youneedthewholelotofya...I’vebeenthroughthere.I’vebeenthroughit.I’vedoneit,andI’mtellingyou,involveasmanyasyoucan.Don’ttakeitonyourself.”Yeah,butit’sahardyakka.(Daughter)
Yeahwell Iwould personally askwho’s the spokesperson and try and find thatperson each time . . . and I’ve spoken to the wrong person inadvertently. Andbecausethatpersonidentifiedthemselvesasaspokespersonbuttheactualwhānauhadn’t,sothat’sachallengeaswell.Yeah.(HospiceAuckland)
Veryrecentlywehadthiswomanwhowasthespokespersonforthewhānauwhowasanin‐lawandshefeltreallyresponsibleandshehadtomakeadecisionandIcan’trememberwhatitwas,butwesaidtoher,“Ourrolehereistosupportyou.Ifyoufeel–youcouldblameus,youcouldblameus–thatwhateverwasdecided,youcouldbring itback to thehospitalas theoutlet.”Butshewasreallyrelievedandyoucouldalmostseethetensiononherface,particularlybeinganin‐law.(HospiceBoP)
Ididthinkaboutwhatyouweresayingbeforeaboutinformationfilteringthroughthe familyandIthinkoften forus inthe largerwhānauespeciallythatwedotryand identify one spokesperson to then filter that information through to others.Andobviouslywe’reonly speaking tooneperson,but identifying theperson thatthewhānau identifying theperson that is tobe themain spokespersonand themgivingthemalotofinformation,butthenencouragingthemtotalkwiththerestofthewhānau(HospiceBoP)
...whenitcomestoyourownfamily...youdoityourself....yes,okay,who’sgoingtopayforthis,who’sgoingtopayforthat?Where’shegoing?Andwho’sgoingtobe responsible for all the different things, you know? And that’s all donebeforehand.Becauseyouknowyou’regonna losehim– it’snogood leaving it forthelastminute,yeah.Andwho’sgoingtobethepersonthat’sgoingtodothisanddo that.Youknow, it’saboutallocatingdifferent things todifferentones,withinyourlittlegroupoffamily,andthenyousenditouttotheextendedwhānau,dotherestthere...(wife)
In the whānau context, all members are potential caregivers. This first quote belowrefers toamokopunahelping thewhānau tocome to termswith thenewrealityofakuia with cancer, while the second quote refers to practical care provided by amokopunatoakorouainhospital.
Intermsofthetreatmentandwhat‐have‐you,itwasthedialogue,itwasthelittlekōrerothatthemokopunahadwithhernanny.Thatwasthemedicine.Intermsofimportance,itwasthemokosthatwasthemostimportantthatcouldactuallyhelpnavigateandmovethepathway.(MāorihealthserviceAuckland)

28
Healways looked forward tohavinghis feet [massaged]–hemusthavehad thetidiest feetandnails, thehospitalused to say.But thatwas just sharingwithhismokopuna.Yeah.(wife&daughter)
Thesenextquotesprovidesomeinformationaboutthechallengesfacedbywhānauandthelevelsofresiliencythatareneededwhenrespondingtohealthliteracydemands.
Itwasjustsohard...beingatthehospitalandtalkingtothedoctorsandnursesallthetimeandtakingcareofthekids.Theolderoneshadtomovehometolookaftertheyoungerones.Andtheyoungeronesweresoangryandconfused...Ineededtostaywithhimwhen theyneededme tobeathome.And the schooldidn’t reallyunderstandandweregiving themahard time fornotgoing toclass. Itwasveryhard.(Wife)
Hard as. Hard, hard, hard. Andwhen I think back in the dayswhenwe did it[caregiving]10yearsagoorso–wehadthebigwhānauthatwouldcomeandgiveyouaday.Everyonewasaround.Noweverybody’ssobusytryingtoworkandkeeptheir jobs, I find that thewhānauare smallernow, so that support isnot there.(MāorihealthprofessionalBoP)
Itryandgotosleepbutthenpeoplecomeinandthenespeciallyyou’vegottokeepaneyeonfortheonesthatshe...Cosshe’sonethatwouldn’tletanyonejusttouchher,evenherhand,andso ifcertainpeoplevisited,youhavetostayup.Andthentheyhadtocomeandgetmecosthefamilygottoastagetheywouldn’tgivehermedication,cosshewassaying,“No,no,”rejectingallofthem.SoIsays,“Ohwell,I’lljustdoit.”Sotheyleftthattomeandwhenshegotinpainquiteabit,soIhadtokindofstayup.(Cousin)
The tension around whānau caregiving in the home, and wanting support but alsoneeding to respect the patient’s desire to remain independent is highlighted by thiscomment:
Those[hospice]nursesaremylifelinebut[husband]won’tlettheminthehouse.Hesaysiftheycomeinthatmeansheisdyingandheisn’tdying.SothenursesandImeetonthelawnorthefrontstepsandtheygivemethedrugsheneeds.Theyalsogivemeequipmenttohelpwithshoweringandsoon.TheyarealsoavailableonthephoneanytimeifIneedthem.(Wife)
Reducing health literacy demands Most of the health professional discussions included ways that individuals hadattemptedtoreducehealthliteracydemandsonpatientsandwhānau.
We’regenerallyprettymindfulofwhether it’s the right timeand the rightplaceandrightpeopleare there.So therewouldbe someenquiryas to: “Is itokay foryou?” . . . “Is thereanyone else youwould likeherebeforeweproceed further?”(Hospital‐basedserviceAuckland)
29
Sometimes you can get a bit engrossed in your paperwork and not be sort oflooking . . .butIthinkitisreallyimportanttojustbeawareofhowthey’refeelingandknowwhentopushonandwhentodrawbackreally.(HospiceBoP)
Theysayinhospicethatyouhavetobereallycareful,youcan’t justthrowalltheinformationatpeople...Ournursesarereallygoodatnotforcinginformationthattheydon’twant.(HospiceAuckland)
Manyofthehealthprofessionals,Māoriandnon‐Māori,describedindividuallyadaptingtheir practice in a culturally competent way to help patients and whānau achievegreaterconfidenceintheirserviceproviderandgreaterskillinutilisingtheservice.
Ithink,tome,thattranslatesintoslowingdownandacknowledgingtomyselfthatthereisgoingtobemoretimerequiredtogettoknow.Thethingsthatarealreadyknownanddon’tneedtobespokenwhenyoushareaculture,yetyouneedtohavethe time to develop some stuff and it is about us getting to know and aboutstandingstillquietlyandyouknow,beingknown.(HospiceAuckland)
Ithinkactuallywhenwedoitwellandyouspendthattimemakingarapportinthefirstplace,theamountoftimethat ittakesfromthenonwardandtheabsenceofmisunderstanding of the mistake, that should make up for it. It is efficient todevelopa relationshipwherepeopleare confident toaskquestions theyarenotsureabout...IsawthesamepatientyesterdayandIspent,itwouldhavebeenlikefourhoursattheirhouseandgettingthisrapportandthentodayIwasthere fortenminutes.Theyfiguredoutthedriver,mostpatientsIhavetodothateveryweek,theywere just likemanagingandbecausetherewas justsomuchwhānau, itwasfullofwomen,beautifulwomenandtheyjustallwanttoknowhowtoworkitandit seems that once the trust is there, you are fast and efficient . . .you create alearningenvironment.(HospiceAuckland)
Health professionals and key informants discussed their understanding of the healthliteracydemandsonpatientsandwhānau,with someactivelymakingefforts tobuildhealthliteracy.
Wehavethiscommunicationcardsystem,andweactivelyencouragepatientsandtheir family to take thiswith them to every appointment . . .it’s a handwrittenoverview. . .we work very hard in the inpatient unit to put it in user‐friendlylanguage.Eventhedosagesaswell:ifit’s3mgofdexamethasonewe’regoingtobeputting that there’s a 1mg pill and they’ve got to take three of them and inabsolutelysimplewords . . .“thisoneistostopyoufeelingsick”or“thisoneisforconstipation”. So that gets talked through with the patient going home andparticularly with their carer as well. Often our patients aren’t going to be apositiontobeabsorbingallthatormanagingtoretainallthat,butaspartofourcheck‐listonthatcardit’salsosignedthatthecarerhasreceiveditandthatwe’vetalkedourwaythroughit.(HospiceBoP)

30
Reducinghealth literacydemandsneedstobeanactive,purposefulprocessdrivenbythe health care organisation (Rudd 2013). These health care professionals havedemonstrated ways in which they worked as individuals, but there were only a fewexamples in this research todemonstrate that thebuildingofhealth literacy skillsbyhealthprofessionalswassupportedbytheirhealthcareorganisations.
3.5 Health literacy practices
Health literacy practices are the actions that patients and whānau take to meet thehealthliteracydemands.Healthliteracypracticesinvolvetheuseofhealthliteracyskillssuchas reading,writing, speaking, listeningandnumeracyaswell as critical thinkinganddecision‐making.
Patients and whānau reported the use of a wide range of health literacy practicesrequiredinordertomeetthehealthliteracydemandsplacedontheminthecontextofpalliative care services. These health literacy practices were identified from explicitstatementsmadebypatientsandwhānau.Thehealthliteracypracticesmostcommonlyusedbypatientsandwhānauinthisstudywerethattheysoughtsupportfromwhānauand friends, maintained written records, researched information, read writteninformation, dispensed medicines, advocated on behalf of patients, and interpretedunspokenmessages.Eachwillnowbeoutlinedinmoredetail..
Seeking support from whānau and friends Manyofthepatientsandwhānauusedwhānaumembersandfriendswhohadpreviousexperiencewithpalliativecare,werehealthprofessionals,orwhowereworkinginrolessuchassocialworkers,toprovideadviceandassistanceparticularlywithnavigatingthepalliative care system. In some cases, this involved thewhānaumemberwith healthcareexperiencestepping inanddirectlyadvocatingonbehalfof thewhānaucarer. Inother situations, it involved the experiencedwhānaumember coachingor supportingthewhānaucarertoaccessthesystemtoachievetheoutcometheyneededtoachieve.
Iwasjustfullon,24hours,andIendedupsleepingrightthroughtoabouthalfpastnineIthinkitwasandmumneededtogotoiletandIwasn’tup,shecouldn’twakemeup.SoitwasprettymuchthenIcalledoneofmymates...Shewasanex‐nurseataMedicalCentre...shecomeoverandshebroughtasocialworkerovertohaveaninterviewwithmeandthenIwastellingherandsharingwithher,thisiswhatIdo,andIhadn’tsleptandIendedupsleepingandmymumneededtobecaredforand she couldn’twakeme up. And thenwe had ameeting and they ended upbringinginanotherperson.(Daughter)
Therewassomeevidenceinthisstudytoshowthatwhānaumemberswereusedinthiswaybecausewhānaucarers feltmorecomfortable talking tosomeone theyknewandwho they perceived was more knowledgeable about the system. There was also
31
evidencethatpatientsandwhānauusedotherwhānaumembersforadvicebecausethepatientsandwhānauwerenotprovidedwithinformationtoenablethemtounderstandhowthedifferentpartsandplayersinthepalliativecaresystemworkedtogether.
There’salwayssomebodythatknowssomebodywho’sjustbeenthroughit.It’sthatsortofkorero,andyoulookaftereachother.Andthere’ssometime . . .they’llfindoftenit’sthenursesinthewhānauoranadvocateinthewhānau.“Ah,yeah,I’llringuptheblahblah–she’llknowwhattodo.”...andtheysay,“Oh,no,no,no,no,”youknow,“wedidthis.Yougottogotrythis,thisandthis.”“Yeah,we’lldothat,”andthey’re talking to each other and they’re looking after each other.Ourwhānauhavebeen through it. Ifyou’vebeen through it,you’vegotall the information toshare.Andweallknowwho’sdoingwhatatthemarae.They’llsay,“Whatdidyoudowhen this happened?” Sowe are talking to each other now and giving eachotheradvice, sharing– sharing the love, sharing the resources, sharing the care.(MāorihealthprofessionalBoP)
Utilising the skills and expertise of other whānau members was a way of ‘workingaround’barriersandobstaclesposedeitherbythesystemitselforbypeopleworkingwithinthesystem.
Iwasbackandforthonthephonetomyaunty...she’sasocialworker.SoIhadtoringherupandsay,“Lookthey’renotgonnaletherin,”andshegoes,“No,yougetback on the phone and you get . . .” you know. So yeah, I just kept on doing it.(Daughter)
Maintained written records Oneofthekeyhealthliteracypracticesusedbypatientsandwhānauwasthekeepingofwrittenrecordsornotesabout theday todayexperiencesof thepatientandwhānaucarers.Participantsidentifiedmultiplereasonsforkeepingtheserecords:
toinformotherwhānaumemberswhowerelivingatadistanceandsowerenotintimatelyinvolvedincaringforthepatient
tomakesenseofthedifferentinformationthatwasbeingprovidedtowhānau
Ikeptadiaryeverydayofwhatthedoctorsandnursessaid.Ineededtodothattomakesenseformeandmyfamily.(Wife)
tokeeprecordsofmedicationsandothertreatments
Yeah, somebody taught me how to – it was my sister‐in‐law again, this iswhat . . . And because everything had to be, before the blister packs . . .Everythinghadtobewrittendownsoyouknewwhatpillitwas,which–howmany,yeah.(Daughter)
32
We had a red big folder, bag thing,where if you asked us for anymedicalrecords,anything,prescriptionslips,wegotitallorganisedintabs.Sowhatdoyouwant?Okay,we’llfindyouthoseresults.IfHstudiesanything,hestudiesitto down to the point where he could perform surgery on himself. (Wife &daughter)
topreventhealthprofessionalsfromgivingincorrectmedicines
Becausetheygottoreaditandnotewhowascomingintoseemumandwhatwere they saying aboutmum and how shewas reacting.Evenwriting downwhat she looked like. [laughs] . . . They’d switch the nurses. Yeah. The staffnurseshadbeenswitched.Soanewlotwouldcomeinandtheyweretryingtogivehersomethingelse,someothermedication,butitwasn’tforher–itwasn’tfor that time, itwas for later on. So I could say, “Oh no no, that’s not hermedication.That’snotwhatshe’ssupposedtobehavingrightnow.(Daughter)
asawhānauresourceforotherswhomighttakeonacarerrole
Iendeduphavingadiary,sothe firstday Istartedwritingdownandstartednotingdownanythingtheyhadsaid.Andthenmysisterswouldjustreadit.Sothat’showwekeptup...AndIwasabletodothesamethingformybrother‐in‐lawandhisfamilytoo,soitsortofquitepaidoff.(Daughter)Whenmymumpassedaway,mymum’ssisterendedupgettingcancertoo,soIpassedthebook[diary]ontomycousinsaying,“Takenotesfromherecousin,sothatyouknow...”(Wife)
Thesewritten recordswere apowerful andpractical tool forwhānau in ahealthcaresystem which privileges written information. One whānau noted that their recordkeepingwasasourceofdiscomfortforhealthprofessionals.
WhenDad’sfistulapoppedopen,wewenttotheAandEandwaiting . . .Waiting,waiting,andtheregistrarcomes in.Andhesaid,“OhDrR’sinameeting.I’ve justcomehereto justcheck . . .Allthesurgeonshavegotameetingrightnow.I’llbebackinanhour”.Andwesaid,“IsDadgoingtobeokay?”...Hegoes,“Oh,look,I’vegotmymeetingandI’vegottogo.Heshouldbeokay”.Andsomysister,Imean,wewere exhausted and here she’s like, “Should be okay?What does thatmean? Issomebodygoingtohelpushereatthehospitalorwhat?”SoIstartedwritingdownandIthinkIlookedatthetimeandIwrotedownthetimeandhegoes,“Oh,whatareyouwritingfromme?Youmakepeoplenervouswhenyouwrite.”AndactuallyIhadthatsaidtomebyaboutthreepeopleatthehospital.Andhegoesoutandhecomebackinandhegoes,“Oh,it’s2o’clocknow.I’mhavingmylunch.Doyouwanttowritethatdowntoo?”(Daughter)
33
Researched information Some participants described feeling frustrated at the lack of clear explanations fromhealthprofessionals,andturnedtotheinternettofindtheinformationtheyneeded.
Theyusedlongwordsanddidn’texplainandsoIwouldtryandrememberwhatitwasandwrite itdownandthen look ituponGoogleonthe laptoptheolderkidsgavemeeverynight.(Wife)
Butthat’sanotherthingtheinternetwasgoodfor,isthemedication,andthesideeffects,yeah,andhowallhermedications,allthestuffshewastaking,wouldaffectyeahwhateverelseshewastaking.Soitwaseasiertofigureoutwhatwaswrongorwhatmedicinesweregoodforherandwhatwasn’t.(Daughter)
Thereisthepotentialforsuchinternetinformationtoleadtomoreinformeddialoguebetweenpatientsanddoctors(Knappetal2011),howevertheliteraturealsosuggeststhatdoctorshaveconcernsabouttheaccuracyofinformationgleanedfromtheinternet,which can change consultations to include debunking inaccurate or misleadinginformation(LoandParham2010).
Read written information Most of the patient and whānau participants did not report that they receivedinformation from thewritten resources. This health literacy practicewas specificallymentioned by only two whānau, and the second whānau read the information inretrospect.
Ipickedup[pamphlets] inthehospitalwhileIwascaring formum.I juststartedreadingthem.Yeah,mostoftheservicesthatwehad,Ihadgottenfrompamphletsorhadasked...(Daughter)
It'squitefunny,becauseacoupleofweeksagomysisteraskedmetocomeover–she didn't know whether we needed to keep all this information [after Mum’sdeath]andtherewasafiletherefromhospice.WewerelookingatitandIactuallystartedtoreaditthereandthen,butIdidn'treaditatthetime.(Daughter)
Dispensed medicines and used medical equipment Whānaualsotalkedaboutthedemandsplacedonthemaroundspecialistcare.Thefirstquote illustrates theproblem‐solvingabilitiesofonewhānauwhen thehealth systemdid not provide the support required. The second highlights how whānau could beoverwhelmedwiththelevelofcaretheyneededtoprovidebutwiththerightsupportthiscouldbeachieved.
Hedevelopedachestinfectionanditgotsobadhewouldbeinagonyandwe’dbecalling[theGP]onthephonesaying,“Shouldwebecallingtheambulance,shouldwedosomething?”andhe’slike“Wellgivesomeparacetamol,”...Intheendwegottheambulance...Wetookhimuptothehospitalandduringthatprocesswegotincontact with the Asthma Foundation and got him a nebuliser . . .we did this
34
ourselves.Notthroughthehospital,or[theGP],notthroughanyone.(Wife&stepdaughter)
ItoldherIwasreallynervousaboutitcos . . .Ididn’tknowwhatIwasdoingandthenallofasuddenI’vegotthisbigresponsibilityonhermeds.AndIdidn’twantto–butshe [nurse] taughtmeand thenshegotme todo itand Idid it . . . Ididn’tknowifitwasstillgoingtobeeasywhenIhadtodoitoncewewerehome.ButIseemedtoknowwhatIwasdoingplusItalkedtootherpeopleplusthenurse,soIobviouslyknew...itwaslikefiveminutestraining,butIaskedtostayinthereforthedayjusttosee,justtowatchandmakesure.(Daughter)
Advocated on behalf of patient, with health professionals and healthcare providers Whānau also reported on some occasions it was necessary to act as an advocate.Sometimes this was because the patient was too sick or too afraid to advocate forthemselvesinothersadvocacywasrequiredtonegotiatethehealthcaresystem.
Ihadtostaywith[her]inhospital,cosshedidn’ttrustanydoctorsornurses.Andthenonedayshejustdidn’twanttohavebloodsandtheytookitthatshegaveuponallhermedication,butitwasjustatthatonetimeshedidn’twantthem...sowehadtokindofnegotiatetimesandstufflikethat,yeah....Wetriednegotiatingwithdieticianstoo,wayback,totryandgetamenudevelopedforourfamiliesthatrunswithinthebudget–butnoonewouldreallycometotheparty...(Cousin)
Interpreted unspoken messages Anaspectofhealthliteracythatisnotdiscussedintheliteratureistheabilityofpatientsandwhānautodrawinferencesfromeventsandactionstakenbyhealthprofessionals.In this firstquote, thewhānauusedtheproposedappointmentasan indicationof lifeexpectancywhentheyfeltotherwiseuninformedaboutwhendeathmightoccur.
She [allied health worker] said she was gonna come and see mum on theWednesday and I thought, oh, you must think she's still gonna be alive onWednesday,geezthat'spromising.(Daughter)
Itwasmorewhattheyweren’tsayingasopposedtowhattheyweresaying.(Wife&daughter)
Health care professionals discussed their understanding of non‐verbal cues frompatientsandwhānau,andhowtheyadaptedtheirresponsesaccordingly.
Youhavepatientswhoarereluctanttotakeanymedicationatall.Icertainlyhavethatconversationwithpatientsaboutpainandhowitmakesthemfeelalive...I’llaskifthey’veusedthemedicationandifit’sstillsittingtherenotbeingused,thenIexplore reallywhy it’s not being used and if there are anxieties about actuallypickingupthebottleandusingit.(GPBoP)
35
Inthefollowingexchange,adaughterillustratestheimportanceofunderstandingnon‐verbalcues:
Int:Howdoyouknowwhenshedidn’tunderstandstufforwhendidyouknowyouhadtoexplainthings?
Participant:Becauseshe justusedtositthereandsmile.[laughs]Andagree.Cosshedidn’tknow.(Daughter)
Thesequotesindicatetheimportanceofhealthprofessionalsunderstandingthepowerand uses of non‐verbal communication, and the interpretations patients andwhānaucanplaceonapparentlyroutineactionssuchasarrangingafutureappointment.Thisisanareawhichrequiresfurtherresearchtounderstand.
Some of the patients and whānau used these health literacy practices in spite ofsignificant barriers put in their way by both individual health professionals andhealthcare providers. Generally these barriers related to failing to communicate fullywith whānau and failing to acknowledge the considerable knowledge and expertiseaboutthepatientwhichwhānauhaddevelopedthroughprovidingcontinuousintimatecaretothepatient.
3.6 Barriers
This study identified barriers experienced by patients and whānau, and reported byhealth professionals,while navigating the palliative care system. These barriersweregenerally grounded in poor health literacy and had the effect of restricting access orutilisationofpalliativecare.
Access barriers for whānau Previouslywedescribedthewayspatientsandwhānauaccesspalliativecareservices.Thisstudyalsoexploredpotentialbarrierstoaccessingtheseservices.
AsdemonstratedinTable4,accesstopalliativecareservicesoccurredthroughavarietyofmeansforthissample.Furthertothesepathways,participantsnotedthatpatientandwhānau perceptions of palliative care and hospice impacted on their ability andwillingnesstoaccessservices.Thesetwowhānauhadtheirconcernsallayedoncetheyhadagreedtoaccesshospicecare:
He reluctantly went to the hospice. And they were wonderful in there. It’s abeautifulplace.(Daughter)
Andwehaveabigfamily,likelotsofgrandchildrenandstuff–liketheydidn’tmindusallbeing there. . .Youdidn’t feel like that,oh,you’renotallowed togoupyetbecauseit’sblah,blah,blahtime.(Daughter)
It was very common to hear that patients and whānau refused to access inpatienthospicecare.
36
Theywantedhertogotohospice,andforherinhermindwasno,hospiceisthelastplacethatyou’rereadytogoout.Soshe’dnevergothere.(Cousin)
Buttotakethemintohospice,theyprefernotto.Theyprefertolookafterthemathome.That iswhat I'm tryingtosayhere.Ninetimesoutof10 . . .[thewhānau]wouldprefertotakethemhomeandlookafterthem,notgointohospice.(MāorihealthprofessionalAuckland)
Reasonsforthereluctanceincludedthe“misconceptionthatpalliativecareisverymuchinside a hospice or inside a hospital – not something that can be delivered in thecommunity”(MāorihealthserviceBoP),andthattoacceptpalliativecarewastoacceptthatdeathwasimminent.
Māori lookat it in thatway, that this is the last stopanduntilonecanget thatmessageacross,thatisnotthelaststopbutit’saplacewhereonecanbesortof–inMāoriwecallitmanaaki–onecanbehelped.(Hospice,KaumātuaAuckland)
Severalparticipantsdescribedpatientandwhānaubeliefs that thepurposeofhospicecare was to hasten death. This was particularly the case when morphine was beingadministeredorthedosageincreasedthroughasyringedriverforthefirsttime.
Youareveryblessed ifyoucanspeaktothemandtellthemthatthemorphine inthesyringedriver is just takingover fromwhat thepatienthasbeen taking,andwe’re not trying to increase it and we’re not certainly trying to hurry theprocedure,butthatthecancerortheillnessisjustprogressing...Iguessunpackingsomeof their thoughtsandbeliefs,and trying toreframe it,but sometimes thosebeliefsaresodeeplyset...(HospiceBoP)
Other perceived reasons for avoiding palliative care included stigma and a lack ofaccurateinformationaboutwhatwasinvolved.
Ithinkthere’smoreofthatstigmaattachedtopalliativecareservicesthanthereisaGP,andaGP isaverynormalthingtogoandseeversuspalliativecare.You’reautomaticallyidentifyingyourselfasbeingsomeonewho’sdyingorsomeonewho’sinadifferentzonetoeveryoneelse.(MāorihealthserviceBoP)
I don’t think people realise that it is a free service and people living in povertywould be thinking, like, I can’t go there because it is going to costmemoney.(HospiceAuckland)
Ithinkthathospiceitself,regardlessofculture,isnotwelladvertised,itisnot[onTV]...That[awareness]reallyneedstobeaddressedbecauseanybodycancometous. . .Iftheyknowaboutourservices longbeforetheyareneeded,theywillknowwhere to comewhen they are needed and they don’t need to get aGP referral.(HospiceAuckland)

37
Sometimesgoingtopalliativecarewasjusttoocomplicated;patientswereconfusedbyincreasing amounts of information that was often inconsistent or incomprehensible,andweretooilltohavetheenergytodosomethingnew.
Ifyou’vegonetothesameGPyourwholelife,tosuddenlychangeandtrustanewmedicalprofessionaltakesalongtime.Youseethatwiththeoncologist.Ittakesalongtimetobuilduparelationshipwithanoncologist.(MāorihealthserviceBoP)
Itdidn’thelpthatthephysioscameinbeforethatandtheOTdepartmentcameinafterthattoputsomethings inhishouse.Hewasbuggeredandhegotmixedupaboutwhowaswho...theprocessofthatwastoomuch;hedidn’tevenunderstandthelanguage.(MāorihealthserviceBoP)
Interviews with health professionals explored perceptions of what might make itdifficultforMāoripatientsandwhānautoaccesspalliativecareservices.Someofthesewere based on personal and/or work experiences, and others were put forward asperceivedbarriersgiventhecomplexitiesofworkinginthisfieldandwiththiscohort.Acommonthemewasthattheircolleaguesinnon‐palliativecaresettingssuchashospitalwards,specialists,andprimarycareavoidedhaving‘hardconversations’withpatientsand whānau about the change in focus from treatment to palliation. This createdsituationswherepatientsandwhānauwerepoorlypreparedforpalliativecare.
Many of the nurses who participated in the focus groups had stories about helpingpatientstoovercomeafearofhospiceas‘theplacetodie’.
I rememberwheeling in aMāori lady one day . . . shewas so frightened, reallyfrightened...Istoppedthewheelchairandwhippedroundthefrontandsaid,“Areyoureallyfrightenedasyoulook?”andshesaid,“YesIam;thisisaplaceyoucometodie”.Shebroughttheconversationupagainwhenshesawmethenexttimeandsaid,“...Thisisthebestthingthatweeverdid.Ireallydidthinkthiswasaplacetocomeanddieandnow Iknowbetter.” . . .youknow sometimes it’sbreaking thatinitialperception.(HospiceBoP)
Icanthinkofacoupleofstoriesorincidenceswherepeoplehavecomeinandsaid,“Wow,thisismuchbetterthanIthoughtitwasgoingtobe,I’lltelltherestofmyfamilynow.”Oryoucanseethewiderfamilycomingtousandsaying,“Thisiswaydifferent.Yes,nowthatwe’veseenitwithourowneyeswecantelltherestofourwhānau,”andwegetthatkindofcommentallthetime.(HospiceBoP)
Cultural barriers During discussions about the cultural identity of services among all the healthprofessionalsandkeyinformants,therewasaclearperceptionthatHospice,theCancerSociety,andthewiderhealthcaresystemingeneralarePākehāorganisations; ‘white,femaleandmiddle‐class’.Althoughthisperceptionisdemonstratedtobeinaccurateinsomeaspectsofthisreport,thestatementwasclearlyarticulatedinallthehospicefocus

38
groups,theCancerSocietyandtheGPfocusgroup.ItwasalsodiscussedasabarriertoaccessintheMāoriservicefocusgroupsandamongthekeyinformants.
I can understand some seeing hospice as very sort of Europeanmiddle‐classed‐focused,andIstronglybelievethatwehavetobreakthatdown,notonlyintermsofinpatienthospicebutrightthroughthecommunity.(MedicalspecialistBoP)
Weareverywhitemiddleclass.Yougoaroundthewholestaff,everydepartment;that’swhoweare.(HospiceAuckland)
There’s a perception that – the Cancer Society’s a very good example of this. Awhite middle class organisation who won’t understand me, who won’t try tounderstandme,whodon’twanttounderstandme.(MāorihealthserviceBoP)
Comingintothisbuilding,itisnotverywelcoming.Thereisnothingthattheycanrecognisethatmakesthemfeelthatthis isaplacewheretheycangetthepropercarethattheirculture,theirwayofthinkinganddoingthings;itdoesn’tlookliketheyaregoingtogetitinthisbuilding.(HospiceAuckland)
Inanysituationlikedying,respectisaparamountthing,wellwithanybodyIthink,andwithMāori they simply think thatunless they [hospice]areMāoriand theyknowMāoriprotocolandprocedures,thattheyjustarenotawareofhowMāoridothings.(HospiceAuckland)
The perceptions of Māori communities andwhānau about the ability of hospice andotherpalliativecareserviceproviderstodelivercarewhichisculturallycompetentandappropriateforMāoriwasalsoindoubt.
[Hospiceisa]Pākehāservice.There’salwaysthatreluctancetogetinvolvedinthefirst instance. ...That imbalance thatwillalwaysbe there Iguessuntilyou seeaMāorifacetothatorganisation...(MāorihealthprofessionalBoP)
ProcessesandenvironmentsthatacknowledgeaMāoriworldviewwereseenaslargelyabsentfrommanypalliativecareservices.Forexampletherewaslittlereciprocityintherelationship,andattendanceatgroupswascontrolledbytheserviceprovider.
Likeyousay,whenMāoricome intoasituation likethis,theyareverymindfulofthefactthatthisis,well,beinginaPākehāworldwherehospiceisconcernedandMāorihavetheirownprotocols,sowhenhospicecomesintoplaywithMāoriinthissortofway,Māoritendtotakeabackstepandsortofnutthingsoutbeforetheycommitthemselvestodoinganything.(Kaiatawhai,HospiceAuckland)
Ithinkifitwasanopenhousetypething,andletpeopleknowthat,thenyoucanjustdropinforacupoftea,insteadofhavingtobelongtoagroup...Andyouseehospicegetseverything.Theygetbakingdoneforthem . . .Wellyouknow,whenIwasgrowingup,wehadtotakeaplate,whether itbeabreadandabutter,andthat’sthething.Ithinkhospicehasgottoletthembringwhattheywanttobring,
39
insteadofsaying,“Ohnono,it'salright,they’vegotitallhere.”That’snottheissue.Theissueis,thisissomethingIbroughttoshare.(Patient&husband)
Manyof thehealthprofessionalsdemonstrateda levelofhelplessnessabouteffectingchanges thatwould benefitMāori. This extended to service‐level issueswhereMāoristaff were either not recruited or were not viewed as intrinsically important to theservice.
Interestinglyenough,wehaveaprocesswherewehaveaChinese liaisonpersonwhomeetsallChinesepatients.Wedon’taskthem[thepatients],thenursecomesasasharedvisit.AndwehavelookedatwhyisitthatwedothatwithallChinesepatients, but we don’t do that with other cultures. Perhaps the nurses aren’tintroducing [thekaiāwhina]–wellbecause it isveryhard to introduce someonewhothey’venevermetbefore.(HospiceAuckland)
Welldefinitely forus itwouldbe lovely to someone thatworked forus thatwasMāori.ItwouldbenicetohaveaMāorinurse...We’vebeenaskingforitforaverylongtimeandobviouslyitalljustcomesbacktomoney.(HospiceBoP)
Ithinkoneofthebarriersisthatourworkforceisnotculturallydiverseenoughinpalliativecare,andyeah,I’vespokentoa fewnursing leadersaboutthisovertheyears and I think thatwe should be doing some sort of purposeful recruitment,because I think our workforce lacks cultural diversity. (Hospital‐based serviceAuckland)
Some of the focus group discussions demonstrated a lack of empathy that could beconsideredstructuralracism.Allofthefollowingquotesoriginatedfromdifferentfocusgroupparticipants.
Ithinkpartofitiswebelievewehavealovelyplaceherebutforthemit’snotliketheirhome, it’s tooclean, it’s too– they sometimesgetembarrassedcoming toaplacethattheydon’tperceive,Idon’tliketosayworthyof,butit’sdifferentandweseeit,andwehaveitsetoutnicelyandtheyfindsometimesMāoripeople,untiltheygethereandoncethey’reheretheyloveit,butit’sjustdifferentforthem.(HospiceBoP)
On one level you could argue that [hospice is] designed for neat, tidy little tinymodularfamiliesratherthangreatwhānauandsoforth,andthat’ssomethingthatwe’vetalkedabouthere.Westruggle.Wedon’treallyhavethe facilities,wedon’thavethewhānauhouse,wedon’thavethewhānauroom,wedon’thaveshoweringand toileting facilitiesat thishospice. . .Someofmy colleagues find itextremelydifficulttomanagethose–thenumbersoffolksthatcanhappen.(HospiceBoP)
IthinkthereisadifferenceforMāori...Ithinkhealthliteracyforeveryone’sreallyimportant,it’saboutensuringtheotherpersonunderstands,it’sabouttalkinginasimple language . . .But forMāorisometimes Ithink it’s ignoranceofwantingto

40
know,bynotgoing to thedoctorhence latepresentations– the fearofwhat is,yeah.(HospiceBoP)
Itwas also clear that somepalliative care organisationswere not collecting ethnicitydataaspercensusguidelineswhichwasabarriertoprovisionofculturallycompetentcare.
That isanother thing to take into consideration,workingwithwhānau.Youaregoingtogetblueeyed,blondheadedMāoriandthatisthewayitisnow,soneverunderestimatethewhānauvalues.(MāorihealthserviceBoP)
Forme it’s very, very limited because I can’t identify sometimeswhether thesepeople areMāori ornot . . . Idon’tget that informationbecause it’snot in ouraccesssheet.(HospiceAuckland)
Interestingly,noneofthepatientandwhānauinterviewsidentifiedcultureasabarriertoreceivingpalliativecareoncetheserviceshadbeenaccessed.Thisisdiscussedfurtherinthenextsection.
External barriers to health literacy Earlier sections in this report focused on factors within (internal to) whānau whichinfluenced their health literacy skills around palliative care. However, this study alsoidentifiedthattherewereanumberoffactorsexternaltowhānau(eithergeneratedbyhealth professionals, palliative care service providers or the palliative care systemitself) which directly interfered with and acted as barriers to whānau building theirhealth literacy skills around palliative care. Of key importance were communicationbarriers:
Soweweretryingtoget[thedoctor]to–don’ttalktouslikewe’reidiots–talktousandexplaintouswhatyou’relookingat.(Wife&stepdaughter)
He[specialistdoctor]alwaysjusttoldus.There’snoconversation.(Daughter)
Whenwe [moved toanotherhospital]myunderstandingwas thathewasgoingintothe intensivecareunit. Ididn’trealise itatthetimebut Idonowknowthatbecause he had a superbug my husband was never going to be admitted tointensivecare.Butnoone toldme that–noone toldmeanything. . .Itwasonlylater I realised that . . .because they thoughthewasgoing todie theydidn’tdoanythingabout[hisinfection].(Wife)
In summary, the findings from this study suggest that patients andwhānauwho aremotivatedforarangeofreasonswilldevelophealth literacy inparticularcontexts(inthiscasepalliativecare)whicharerelevantandimportanttothem.Thesefindingsareconsistentwithbothadulteducationprinciples(Knowlesetal2005)andadultliteracystudies(Stichtetal1987)
41
Wedidnotspecificallyaskpatientsandwhānauwhethertheywerealreadyusingthesepractices in other contexts before transferring the practices to the palliative carecontext. Nor did we ask patients and whānau whether they had transferred thesepractices into other health care contexts e.g. optimal use of asthma medication anddevices.
3.7 Navigating the palliative care system
A common theme from this research was the importance of effectiveadvocacy/navigationtoaddresssomeof thehealth literacyandaccessbarriers.Whileadvocacywasdiscussedaboveasahealth literacypractice involvingutilisingwhānauand friends, this section relates to a specific function provided by palliative careservices.Calledvariouslyanavigator,kaiāwhina,orsimplyanextensionofanexistingrole such as a nurse or social worker, these people act as advocates and systemnavigatorsandappearedtohavemadeabigimpressiononthequalityofcarewhānauexperienced and received. The following quotes illustrate the range of perspectivesfrom whānau experiencing a navigator role, to a health professional observing anavigator,anavigatorservicedescribingwhattheydo,andanotherhealthprofessionalnotingthefullextentofwhatthenavigatoroffers.
[Thenavigator] took– like Iwas trying to takenotesand then she just tookmybook and she just – so I could listen, she did all the notes for us and I reallyappreciated that. And by the time I got my book back she had all the phonenumbersinit,shehadeverythingIneeded,yeah...alwayslikekeepingastepaheadofus.Likesheknewwhatquestionswedidn’tknowtoask,andsheknewthatsoonwewouldbeneedingcertainservices,andshewouldmakesurethatcontacteitherhadbeenmadebyherselftosetupcontact–sothattheywouldcontactusorshewouldgiveusthe informationandwewouldcontactthem. . .Shewassaying,“Dothisnow,don’twaittillitgetsworse,sothatyou’vegotarapportwiththesepeoplebeforeyouneedthem”.(Wife&stepdaughter)
[Thenavigator]wasactuallytalkingtotherestoftheteamanddocumentingthat[thetreatmentplan]issomethingthatisdistressingtothefamily.(Hospital‐basedserviceAuckland)
Wesupportwhānau intermsofnavigatingtheiroptions inawaythatmaintainstheirmana.Andinawaythatprovidesanopportunitytowhānautoactuallylookatwhatarethechoicesthattheymake.Andpartofthat...isactuallyensuringthatinformation isdelivered insuchaway that theycancomprehend, theycanapplythoseoptionstotheirworldview,andtotheirwhānaucontextandwhat’sactuallyhappening.(MāorihealthserviceAuckland)
Theroleofthenavigatorinvolvesbeingcalledathomeat8o'clockatnightorat10 o'clock at night and being toldwe're having trouble and being expected toaccesscare.(MedicalspecialistBoP)
42
Attending appointments with patients and whānau formed a key part of advocacy,ensuring that information was effectively communicated because “people feeloverwhelmingly intimidatedbyhealthprofessionalsand the language that’sbeingusedandmaynotreallyunderstandwhat’sgoingon”(Hospital‐basedserviceAuckland).
Sometimes you go with them to their appointments, to their GP, oncologist orwhoeverand it’sabout translating the information for them,generallywhat thediagnosisisandwhattheprognosisis.(MāorihealthserviceBoP)
Theyliketoreada[pamphlet]sowetaketheminformationonthat[chemotherapyandradiotherapy]andImeanthatisprettyhardtounderstandsowesitthereandgothroughitwiththem.Theyareterrifiedofgoingtotheirfirsttreatment,sowegowith them.Wemeet thembefore theywalk in thedoor. (Māorihealth serviceBoP)
Advocacy was extended to accessing social support such as Work and Incomeappointments,andinterveningwhenschoolsbecameconcernedaboutachild’sabsenceduringthefinalstagesoflifeforaparentorgrandparent.
3.8 Communication processes
Many aspects of the themes above have some relationship to the topic ofcommunication. It is an important topic, so is included as a separate theme here.Patientsandwhānaufoundthefollowingcommunicationprocessesusedbyhealthcareprofessionalswereeffectiveinsupportingthem:
abilitytocommunicate24/7withhealthprofessionals,toaskquestionsandhavetheirfearsallayed
Thegoodthingaboutitisthattheyhadthiswhiteboardandittoldyouwhowason,andlikefromthesocialworkerrightdown...wecouldtalktoanyofthemaboutifwehadlikeaquestionoranything.Theywerenice. . .Andthethingaboutthemwasthattheywerequitestraightupwithyou,whichwasevenbetter.That’swhatyousortofneedwhenyou–soyoucansortofprepare yourselfandall of that sort of stuff so yeah.Even though itwasscary,itwasstillgood.(Daughter)
TherewerecertaintimesthatIneeded[thenurse]toexplaintothefamily.Andtheywereprettymuchtherewithinhalfanhour.(Cousin)
establishedrespectfulrapportwithpatientsOh theway she spoke, theway she interactedwithus . . . shewas reallylovely,reallyinformative...Hewashappywithher.Shewentrightthroughthemedication . . .sayingthathecan increasethatwhenever;therewon’tbeanyproblemswithit.(Wife&daughter)
43
trainingprovidedforcarersSo thenurses taughtTwhat todo [morphine],which isreallygood,cos itwasoneononesoitwaseasyforhertounderstandaswell.(Daughter)
The people from hospice came out and explained [to thewhānau]whatneeded tobedoneandwhat I foundwas the fact that they showed themhowtohandlethepatient,whattodo,andhowtheyshouldbetreatedandevenhowtowashthem,andtheytookallthatinandthathelpedmyfamilyheaps,itwasfantastic.(HospiceAucklandkaumātua)
opportunity to have regularmeetingswithpeople providing care to patient todiscussprogress
Onceaweek you could callameetingwith everybodywho’s lookedaftermumandthenwecanallgrouptogetherandseewhat’sgoingonandhow’sitallgoing?(Daughter)
communicationbooktorecordwhatwashappeningBecause theygot to read itandnotewhowascoming in to seemumandwhatweretheysayingaboutmumandhowshewasreacting.Evenwritingdownwhatshelookedlike[laughs].(Daughter)
helpwithpredictingfuturecareneeds...alwayslikekeepingastepaheadofus.Likesheknewwhatquestionswedidn’tknow toask,and sheknew that soonwewouldbeneeding certainservices,and shewouldmake sure that contact eitherhadbeenmadebyherselftosetupcontact–sothattheywouldcontactusorshewouldgiveustheinformationandwewouldcontactthem...Shewassaying,“Dothisnow,don’twaittill itgetsworse,sothatyou’vegotarapportwiththesepeoplebeforeyouneedthem”.(Wife&stepdaughter)
Generally the whānau participants identified that individual nurses were open andhonest and tried to advise whānau of the reality of the situation. Most healthcareprofessionals said they would answer questions if asked, but somewere not alwaysproactive in giving information, particularly if they assessed the patient andwhānauwerenotreadytohearit.
Iwouldonlyevertellsomeonewhattheywanted,iftheywereaskingaboutit.Theysay in hospice that you have to be really careful, you can’t just throw all theinformationatpeople...Ournursesarereallygoodatnotforcinginformationthattheydon’twant.Lotsofpeopledon’twanttoknoweverythingabout it.They justwanttoknowwhattheywanttoknow.(HospiceAuckland)
Some health professionals described their process for ensuring patients andwhānauwouldfeelabletoaccessinformationandsupport.
44
Iwantthemtofeelthatthere’sanopendoorandthattheywillusethephone. . .Iwill follow thatupa fewdays laterwithaphonecall just to sayhoware thingsgoing,wemettheotherday,againjusttomakesurethattheyknowthatI’mreallyopentothatlevelofcommunication.Themostimportantthinginadoctor/patientrelationship is that you can communicate and let people know that there’s anabilitytocommunicate.(GPBoP)
I always explain . . . “Come with your questions, don't hesitate. If you're toowhakamāgivethemtomeandI'llaskthem.”...We’llstayafterwardsbecausethewhānau usually come, “Nowwhat did that doctormean?”Or they usually comeback asking me questions. And that's good too, because that's what we want.(MāorihealthprofessionalAuckland)
Duringthediscussionsanddescriptionsrelatedtocommunicationprocessestherewasconsiderableoverlapamongaccountsfrompatientsandwhānau,andhealthprofessionals.TherewasgeneralagreementthatfindingwaystoeffectivelycommunicatewithineachextendedcareteamwasakeypartofhavingagoodpalliativecareexperienceforMāori.
Culturally appropriate communication Māorihealthprofessionalsandsomeofthepatientsandwhānauparticipantsidentifieddimensions of culturally appropriate communication and care that were criticallyimportantforMāori.Itisinterestingtonotethatfewpatientsandwhānaudiscussedthedetailof culturallyappropriate communication; their attention remainedon themoreclinically focusedpointsdescribedabove. It is the impressionof the interviewers thattheculturalcomponentofwhānau‐healthprofessionalcommunicationwasinherentinthe successful processes described above. This impression could be tested in futureresearch.ThedimensionsofculturallyappropriatecommunicationthatwereidentifiedbyMāorihealthprofessionalsareoutlinedinthefollowingsection.
Whānaungatanga
Whānaungatangacontainsmanyaspects;ourparticipantsparticularlydiscussedtwoofthem. The first was the process of becoming known to one another, which wasdiscussedasakeyfactorintheacceptabilityandculturalsafetyofservicedelivery.Thesecond aspect of whānaungatanga mentioned was the development of an ongoingrelationshipbetweenthepatient,whānau,andhealthprofessionals.
When we meet, it’s whānaungatanga – whakawhānaungatanga is the mostimportantthing.(MāorihealthprofessionalAuckland)
Onceyouareinwiththemfromtheheartyouarebondingwiththem...itisfromhearttoheart...youtakeintoaccounttheprotocol.Theirpracticesneedtothinkaboutthefamilyingeneral,ifyoungeryouthinkabouttheparents,knowhowwehavetolivethroughthiswiththatpersonandthenonceyoucangetthattrust,youknow,getthemtotrustyou.(MāorihealthserviceBoP)
45
Wegoalongandintroduceourselvesandtalkaboutthem,wheretheycomefrom,wherewecomefrom,sothatwecangetatrustformedandthenwetake it fromthere . . .That can be two or three visits before they talk about cancer. (MāorihealthserviceBoP)
Youcan’t,withanewreferralgoinandtalkcancerstraightawayinthefirstthing.Itmightnotbeuntil the thirdoreven the fourthvisit thatyoucan start talkingabout thecancer.Youhave todevelop that trustandrespect firstbeforeyoucanstart talking about theirmamae, their hurt, before you can talk about it. (KI1:MāorimanagerBoP)
Kanohi ki te kanohi
Themost commonmeans of communicating among all the participants was throughkanohikitekanohi(face‐to‐faceconversation).Thiswasidentifiedasbeingparticularlyimportantforwhānau.
It[kanohikitekanohi]takesmoretime,itdoestakemoreeffort . . .buttherearebetter outcomes. It addsmore to the quality of the information – it just does.(MāorihealthprofessionalsBoP)
Kanohikitekanohi...sovitalforMāori.Itisreallyimportantthatyousitandtalktosomeone.(MāorihealthprofessionalAuckland)
Te hora o te whānau i te māramatanga – Whānau sharing knowledge
Participants acknowledged the strength to be found in sharing knowledge andexperiences.
There’salwayssomebodythatknowssomebodywho’sjustbeenthroughit.It’sthatsortofkōrero,andyoulookaftereachother.Andthere’ssometime . . .they’llfindoftenit’sthenursesinthewhānauoranadvocateinthewhānau.“I’llringupblahblah–she’llknowwhattodo.”...Ourwhānauhavebeenthroughit.Ifyou’vebeenthrough it,you’vegotall the information to share.Andweallknowwho’sdoingwhatatthemarae.They’llsay,“Whatdidyoudowhenthishappened?”Sowearetalkingtoeachothernowandgivingeachotheradvice,sharing–sharingthelove,sharingtheresources,sharingthecare.(MāorihealthprofessionalBoP)
Oranga wairua – Spiritual care
Spiritualcareorwairuatangaisadimensionofcarethatwasincludedbywhānauaskeytotheirengagementinhealthcare.
When[thechaplain]came,dadhadbeenfightingdeath,fightingforeverybreath,notgivingin.Thechaplainaskedwhattypeofkarakiadidwewant?Iknewtherewould be nomiracle. I asked for a karakia to givemy father a safe journey toheaven.Thekarakiaorprayerbeganand I feltmy father’sbody ease. I felthimrelax. Ibelieved thiskarakiahelpedmydadpassoverand Iamgrateful for this.(Daughter)
46
It’sacompletelydifferentpointofview,andaspecificperspectivethatI’mthinkinghere, but I think that it’s very bound up in Christianity. Dealingwith pain, forinstance,youareobligedtoputupwiththatpain,becauseit’sbeengiventoyoubyGodandtryingtocircumventthatbytakingpainreliefistryingtocircumventGodand thereforewe don’t do that. And that’s just something that from a spiritualpointofviewandahealthpracticalpointofview–that’saveryhardconceptforus[nurses]togoalongwith,orevenunderstand.Sothereyou’vegotaspiritualdivide.Andyou’reaskingthemtounderstand information fromapracticalpointofviewand scientificpointofview,and that’s justnotwhere they’recoming fromatall.(MāorihealthserviceBoP)
ThespiritualaspectsofMāorihealth,Māorideath,andofpalliativecarehavebeenwelladdressed in the literature(forexample,seeDurie1994;Fairbairn2002;Paley2008;Moeke‐Maxwelletal2010).Therelevanceofspiritualitytothehealth literacycontexthasnotyetbeenresearched.Rudd(2013)callsforcarefulexaminationofimpactofthesocial environment on health literacy; this research and the literature suggests thatwairuatanga should be viewed as an area of potential impact on health literacy forMāori.
Nā Māori, mā Māori – By Māori, for Māori
Palliative care provided by Māori afforded patients and whānau a different level ofengagement.Participantsagreedthattherewasa“culturaldividethere...careisbettermanagedbyMāoriforMāori...Somuchofwhatwedoisaboutrelationships,andifyou’vegotarelationshipwithsomebody, ifthey’vegottherelationshipwith[Māori],you’vegotthatconduit.”(GPBoP)
ThereissomethingthatMāorinurseshaveforMāorianditissomethingwefinditreallydifficulttoarticulate. It is Isuppose justanX‐factor– it isaculturalthingand ourMāori patients feel this too, like they always say tome,where are youfrom?Thereissomethingthatnon‐Māorinurses,theydon’thavethatX‐factor...itiswonderfultobeabletospeakMāoritoaMāorinursefluentlyandtheylovethat.(MāorimanagerBoP)
There’sawairuainthereothatyoucanfeel,andevenifyou’renotconversinginitbutlookingattwopeopleconversing,youcanstillfeelthat.Whenpeoplefeelthat,theymovebecausetheycanfeelit.Soyoucanseeorhearthings,butit’sdifferentwhenyoufeeliteh.(MāorihealthprofessionalsBoP)
Sometimes youhear, “Iwish thereweremoreMāorinurses”, “Iwish therewereMāori...”...forMāorisometimesthere’sjustalookandit’sanunderstandingthatwordscannotsayandyoujust,Idon’tknow,havethatconnection.I’mnotsayingithappens inallcases.ImeanevenIgetchallenged,even fromkuias,theold,yeah.But I think ifyourheart’s in the rightplaceandyouknowwhyyou’re there . . .(MāorihealthprofessionalataHospicefocusgroupBoP)
47
Sowehaveconventionalmedicineand treatment,rongoa, tohunga,karakiaandmirimiri.Ithinkthenursesknowthatwhenitcomestothatpalliativecaretimefortheirpatients,thattheyaretheretositandkarakiawiththem,providethemwhattheywantandtoknowwhat it istheywantandtounderstandtheprocessand IthinkthatiswhereitisMāoriforMāori.(MāorimanagerBoP)
Māori care did provide challenges, however, in terms of the close connections ofwhānau.
FormyselfasMāori,some [patients]are familyand I’vehad tosay several timesthatwhat’ssaidbetweenyouandIstayshere.YesIknowthatyoumightberelatedtomyfamily,butI’mworkinghereandwhatwesaystayshereunlessthere’ssomesafetythingforyou,thenIneedtotalktosomebody.AndthatconversationIhavetohavequiteoften...that’stheothersideofMāori.(Hospice,MāorinurseBoP)
ThecommunicationprocessesidentifiedbytheseparticipantsisconsistentwithmuchoftheliteraturethatexaminesculturallyappropriatehealthcareforMāori(Durie1998;Crametal2003;Cormacketal2005;Jansenetal2008;Kiddetal2013).
3.9 Summary
Māoriaccesstopalliativecaretookmanyforms,fromself‐referralthroughtohighlevelspecialist referrals. Some whānau experienced significant difficulties with access toappropriate care. Whānau and health professionals reported that when referralsoccurredverylateintheillnessprocess,thepatients,whānauandserviceprovidersdidnot have time to engage, negotiate the health literacy demands, access satisfactorysupport,ormakearrangements for theirpreferreddeathexperience.Latereferrals topalliativecarewerealsoreportedtoincreasedistressforhealthprofessionals.
Reasons for late access and/or late referrals included individual patient andwhānauperceptions that accepting palliative care was synonymous with accepting imminentdeath,andthathospicemighthastendeath.
Patientsandwhānaudemonstratedawiderangeofhealthliteracypracticesinordertomeet the health literacy demands placed on them in the context of palliative careservices.Someofthepatientsandwhānauusedthesehealthliteracypracticesinspiteofsignificantbarriersputintheirwaybyindividualhealthprofessionals,palliativecareproviders, and referring services. Practices which improved health literacy includedthose categorised as internal to the whānau, such as accessing friends and resourcepeoplewhocouldassistwithnavigatingthepalliativecareenvironment,andinitiatingand maintaining written information records that were passed on to healthprofessionalsandextendedwhānau.
Thehealth literacydemandsassociatedwithpalliative carewereacknowledged tobewiderangingandcomplex.Whānauwerenegotiatingtheacquisitionofnewknowledgeandskillswithinacontextofshock,griefandloss.Whilerecentresearchsuggeststhat

48
Māori have low health literacy,whānauwho participated in this study demonstratedhigh level health literacy practices including finding and understanding information,navigating the health care system by utilising resource people, and keeping writtenrecords of their experiences. Whānau were often faced with complex health caresystemsandbarrierswithhealthprofessionals,whichmayhaveat timesunderminedtheeffectivenessoftheirhealthliteracypractices.
Manyhealthcareprofessionalsdemonstratedanunderstandingofwhatwasrequiredto achieve health literacy and reduce health literacy demands, but there was littleevidence of organisations taking a systematic approach to such achievements. Healthcareprofessionalsalsoexperiencedsystemsbarrierstoimprovingtheirpracticeintheareaofhealthliteracy.
External barriers influencing health literacy in palliative care settings included thequality and context of information transmitted by health professionals, culturalconsiderationsincludingtheperceptionofhospiceandtheCancerSocietyasnon‐Māoriorganisations,andthepresenceorabsenceofadvocatesornavigators.
Effectivecommunicationforwhānauparticipantsinvolvedrespectfortheknowledgeheldbywhānau,plainspeech,andawillingnesstohavethe‘hardconversations’thataccompaniedthemovefromtreatmentfocusedcaretopalliativecare.
Whānaungatanga,kanohikitekanohi,wairuatanga,andMāoriserviceproviderswereallidentifiedasimportantcomponentsofaneffectivecommunicationmodelforMāoripatientsandwhānau.

49
Section 4: He matapakinga me he whakatepe – Discussion and conclusion Healthliteracyisafunctionofthedemandsandexpectationsplacedonthepatientbythehealthcaresystemaswellasbythepatient’sdiseaseprocesses(Sudoreetal2009),and has been described as an interactive practice rather than an individual skill set(Workbase2013).Healthprofessionalsandhealthserviceprovidershaveacriticalroletoplay inhealth literacy. In thissectionwediscuss the findingswithreference to theliterature,maintainingabroad focusonpatient andwhānau,healthprofessional, andorganisationalorsystemicviews.
4.1 Access
Lateaccess,difficultieswithaccess,andlatereferraltopalliativecarewereallidentifiedin this study as issues for the participants. The outcome of these was similar, withinadequate time for patients and whānau and their service provider to engage,negotiate the health literacy demands, access satisfactory support, or makearrangements for thepatients’ preferreddeath experience. Late referrals topalliativecarewerealsoreportedtoincreasedistressforhealthprofessionals.
Themechanisms around late access and late referralmay variously relate to tikanga,lack of knowledge ormisunderstandings about the availability and uses of palliativecare (low health literacy), availability of services, the clarity and timeliness of ‘hardconversations’ with health professionals about the shift from treatment to palliativecare,andtheculturalcharacterofpalliativecareservices.
Tikanga Tikanga(culturalvalues)suchasrestrictionsonwhomayphysicallytouchthebodycanlead toMāori patients andwhānau to resist or refuse health care (Kidd et al 2013).AlthoughthereisnolargescaleorgeneralisableresearchintoMāoripreferencesaboutdyingathome,theseparticipantsandinternationalliteraturetendtosuggestagreementwiththeviewthatdyingathomeisapreferredoptionforMāori.Forexample,Canadianand Alaskan research identified that indigenous people prefer to be cared for byrelatives(Kellyetal2009;DeCourtneyetal2010),andaNewZealandstudyhighlightedthenecessityforspiritual,emotional,moralandphysicalsupportforthedyingpersonandtheirfamily(Ngata2005).TheoddsofMāoridyingathospicearelowerthanforNZEuropeans(Freyetal2012),but theexactreasons for thisarenotclear.Theplaceoftikanga inhealthcare,andthepreferences forplaceofdeath forMāoriareareas thatrequirefurtherresearch.
Attributes of blame for having a terminal illness are attributed to self or ancestralwrongdoings–asortofpayback(Ngata2005)whichmay inhibit family fromseekingpalliativecare.Thismayleadtoadditionalstressonthepatientwhomaybeunwillingto talk about their disease for fear of bringing shame to the family and community

50
(Shahid and Thompson 2009). Furthermore, refusing care may be as a result ofacceptance; that they are bearing the pain to protect their families from furthersufferingcausedbya‘curse’orpayback.
The extent ofMāori refusing or avoiding palliative care for reasons of tikanga is notknown; culturally appropriate research is required to increase understanding and toenableservicestoadapttheircareaccordingly.
Low health literacy Thisstudyfoundthatsomepatientsandwhānauwerereluctanttoacceptpalliativecarebecause they understood that such services were only available as an inpatient;believed that the purpose of hospice care was to hasten death; and believed that toaccept palliative care was to accept that death was imminent. Many of the healthprofessionalshadstoriesabouthelpingpatients toovercomea fearofhospiceas ‘theplacetodie’,whichwereconsistentwithNewZealandresearch(Freyetal2012).Thisperceptionmaybeabarriertoutilisingtheservicesprovided,especiallywherefamiliesarestillwishingtoremainpositive(BellamyandGott2013).
Thestudyalsofoundthatsomepatientsandwhānaudidnotknowoftheexistenceofsuchservicesuntil theywereconfrontedwithareferral.The levelofhealth literacy islikelytobeafactorinwhetherareferraltopalliativecareisaccepted,withpeoplewhohavelowormarginalhealthliteracymorelikelytoprefertreatmentfocusedcarethanpalliative care (Volandes et al 2008). A recent New Zealand study confirms that thisfinding occurs across other cultures in addition to Māori, and recommends publicprofilingofhospicewitheducationandinformationprovisiontostrengthencommunityinvolvement(BrayandGoodyear‐Smith2013).
Service availability All our patient and whānau participants were in receipt of specialist palliative care,eventhosewholivedinrelativelyremoteareasoftheBayofPlenty,largelybecauseofthemobilityofhospicecareintheregion.GPandMāoriprimarycareprovidersinbothregionswerealsoinvolvedincaredelivery.However,accesstospecialistpalliativecareservicesinruralareashasbeenacknowledgedasaconcern(MinisterofHealth2001).Many Māori live in rural areas of NZ or return to their ancestral/tribal home whenterminallyill,meaningtheymaybedisadvantagedintheiraccesstospecialistpalliativecareservices(Lawrensonetal2010).
ThefullextentoftheimpactofregionalgapsinpalliativecareforMāoriisnotknown.
‘Hard conversations’ This study found that the willingness and ability of health professionals to have the‘hard conversations’ that accompany illness and death had an impact on the healthliteracy of patients andwhānau.Where those conversationswere not held or lackedclarity,whānaureportedfeelingoverwhelmedandunder‐informedabouttheiroptionsand how to help their family member. This also had an impact on their access to
51
services,with somewhānaunot realising that choiceswerebeingoffered, andothersresistingpalliativecarereferralsbecauseofpreconceivedideas.
Themovefromactivetreatmenttopalliativecarehasbeendescribedas transitioningfromaspaceofclosedawareness,toonefocusingontreatmentandsideeffectsonly,toopen awareness where the limits of medicine are acknowledged and end‐of‐lifeplanningisopenlydiscussed(Wittenberg‐Lylesetal2011).
Thisstudydidnotexplorewhetherthesehardconversationsoccur(ordonotoccur)inthesamewayinprimary,specialistorgeneral(pre‐referral)healthcaresettings.
AlthoughaNZstudyfoundthatatraditionalMāoribeliefsystemabouttheinevitabilityofdeathmadeconversationsaboutend‐of‐lifecare lessdifficult forstaff(BellamyandGott2013),healthprofessionalscanstrugglewithdecisionstochangethedirectionofcarefromactivemanagementtopalliativecare(Moritaetal.2005;Wittenberg‐Lylesetal 2011; Bellamy and Gott 2013). An Australian study suggested that GPs lackconfidence in talkingaboutdeathanddying (Burgesset al2004),whileanotherNewZealandstudyfoundalackofknowledgeamongacutehospitalstaffabouthowtocareforadyingpatient(Shewardetal2011).
Forhealthprofessionals, caring forapersonof adifferent culture canbringabout itsown anxiety (McGrath 2000). A lack of physician and nurse awareness of traditionalbeliefs held by the community regarding death was a barrier to care in a study ofremotecommunitiesinCanada(WestlakeVanWinkle2000;Hotsonetal2004).
This finding highlights the need to understand how to teach and support healthprofessionals toworkwith peoplewho have life‐limiting illnesses, particularly at thepointwhereactivetreatmentchangestopalliativecare.
Cultural character ThisstudyfoundaclearperceptionbyallparticipantsthatHospice,theCancerSociety,andthewiderhealthcaresystemingeneralwerePākehāorganisations;‘white,femaleand middle‐class’. The perceptions of Māori communities (reported by Māori healthprofessionalsandkey informants)andwhānauabout theabilityofhospiceandotherpalliative care service providers to deliver care which was culturally competent andappropriateforMāoriwasalsoindoubt.
Some of the focus group discussions demonstrated a lack of empathy that could beconsidered structural racism (Jones 2000), while many of the health professionalsdemonstratedalevelofhelplessnessabouteffectingchangesthatwouldbenefitMāori.
Certainruleswereevidentinsomehospitalorhospicesettingswhichmayconflictwiththeculturalrequirementstowardstheendoflife.Forexample,visitinghoursandpolicyaroundwhomandhowmanycanvisit couldbeatoddswith this concept.ForMāori,seeingpeoplewhiletheyarestillaliveisimportant:extendedfamilybringswiththemtheirspirit,lifespark,collectiveconcern,loveandsympathy(Ngata2005).Whilenone
52
oftheorganisationsinthisstudyimposedvisitinghoursforpeoplereceivingpalliativecare,most of the participants from inpatient settings reported difficultieswith spaceandresourcesforextendedwhānauovertime.
Interestingly,noneofthepatientandwhānauinterviewsidentifiedcultureasabarriertoreceivingpalliativecareoncetheserviceshadbeenaccessed.Thismayreflectabiasin our sample because all the patient and whānau participants were identified byhospices.However,theperceptionsandimportanceofcultureforpatientsandwhānauwho either choose to engage or avoid engaging with palliative care services is notknownandrequiresfurtherresearchtounderstand.
Theoverallfindingoflatereferralorlatepresentationisconsistentwiththeliterature(Davisetal2006;MinistryofHealth2013),but requires furtheranalysis toascertainthe systemic, organisational, individual, whānau and cultural influences on timelyaccesstohealthservicesforMāori.
4.2 Health literacy demands
The health literacy demands were found to be substantial and complex, requiringproblemsolvingandresourcefulnessonthepartofpatientsandwhānau.
Three categories of health literacy demands, based on Rudd and colleagues (2004)schema,weredeveloped.Thesearetheknowledgeandtaskcomponentsofthediseasemanagement focus of medicines, patient care, and the wider focus of navigating thepalliative care system. A larger, more targeted study is required to confirm thesecategories.
Theemotionalclimateofpalliativecaremayaddanotherdimensiontohealth literacydemands.Theparticipants acknowledged the additional health literacydifficulties forpatientsandwhānauthatarosebecauseoftheshock,griefandanxietyassociatedwithreceiving palliative care services. These emotions, combined with the health literacydemandsassociatedwithintensivephysicalhealthcareneeds,createdacomplexhealthliteracyenvironment.
Whānaucaregivingwasanother factor that influencedtheemotionalclimate inwhichhealth literacy occurred. Having a single spokesperson for thewhānau increased theresponsibilityandworkloadfor thatperson,andhadthepotential tocreateproblemsfor that person. However, it was the perception of most non‐Māori health careprofessionals that this was the method of communication preferred by patients andtheirwhānau.
AsurveyofNewZealandGPsidentifiedtheneedtoinvolvewhānauinthemanagementofMāoripatientsneedingpalliativecarebyidentifyingthekeypeoplewithinthefamily(Lawrensonetal2010).Insomecases,identifyingthedecision‐makerinthefamilyisamatter of health professionals simply asking who it is (DeCourtney et al 2010). Incontrast,whānaucaregiversdiscussedhowstressfulanddifficult itcouldbetobethe
53
‘identifiedperson’. Largermulti‐dimensional studiesmayhelp to identify appropriatewaysforhealthprofessionalstoworkwithwhānau.
4.3 Reducing health literacy demands
Thisstudyidentifiedthatsomehealthprofessionalsusedindividualprocessestoensurethat patients and whānau would feel able to access information and support. Inparticular, theydescribed ‘front‐loading’ time to ensure thatwhenpatientswere firstreferred, relationships were actively created to support an effective learningenvironmentwhenpatientswerefirstreferred.
Theperceptionsofsomehealthprofessionalswerethatdecisionmakingwaseasierandmoreeffectivewhenpatientsandwhānaualreadyhadsomeknowledgeaboutpalliativecare.
Providing education is a fundamental health professional intervention that is ideallybothempoweringandculturallysensitiveforthoseinhospiceandotherend‐of‐lifecaresettings(CagleandKovacs2009).However,manyhealthprofessionalsarelikelytohavebeen taught toprovideeducation ina ‘top‐down’ fashion (withhealthprofessional aspowerful expert) that bears little resemblance to the principles of adult education(includingsharedcollaborativeknowledge)thatformthefoundationofhealthliteracy(Nutbeam2008).
Studies of current health literacy content in professional training programmes andassessment of their efficacy would ensure that future generations of healthprofessionals are competent at recognising and reducing health literacy demands forpatientsandwhānau.
4.4 Health literacy practices
Health literacy practices are the actions that patients and whānau take to meet thehealthliteracydemands.Healthliteracypracticesinvolvetheuseofhealthliteracyskillssuchas reading,writing, speaking, listeningandnumeracyaswell as critical thinkinganddecision‐making(Nutbeam2009).
This study found evidence of patients and whānau using complex health literacypractices,which utilised a range of literacy and numeracy skills and included criticalthinkinganddecision‐making.Theseincluded:
Seeking out and utilising whānau and friends for information, support andadvocacy
Researchinginformation,especiallyontheinternet Readingwritteninformation Maintainingwrittenrecords Dispensingmedicines(includingusingsyringedriversandnaso‐gastrictubes)

54
Advocating on behalf of patient with health professionals and healthcareproviders
These health literacy practices were used in spite of significant barriers generallyrelated toa lackofeffectivecommunication.Utilising theskillsandexpertiseofotherwhānaumemberswasawayof‘workingaround’barriersandobstaclesposedeitherbythesystemitselforbypeopleworkingwithinthesystem.
Some participants described feeling frustrated at the lack of clear explanations fromhealth professionals, and turned to the internet to find the information they needed.Thereisthepotentialforsuchinternetinformationtoleadtomoreinformeddialoguebetweenpatientsanddoctors(Knappetal.2011),howevertheliteraturealsosuggeststhatdoctorshaveconcernsabouttheaccuracyofinformationgleanedfromtheinternet,which can change consultations to include debunking inaccurate or misleadinginformation (Lo and Parham 2010). Research shows a positive correlation betweeninternetsearchingandhealthliteracyforolderpeople(LamandLam2012),soitwouldbe useful to understand how the internet is changing the health professional‐patientdynamicandhowhealthprofessionalscantakeadvantageoftheincreasingavailabilityofhealthinformation.ItisnotknownhowtheinternetcouldaffectMāorihealthliteracyin palliative care, but clearly a number of whānau participants in this study wereaccomplishedinternetusers.
Thesepalliativehealthcareliteracypracticescouldbeviewedasbeingincontrasttothefinding of low levels of general health literacy for Māori found in Kōrero Marama(MinistryofHealth2010a).Explanationsforthiscouldincludethatpeoplereceivingorcaring for people in palliative care may be more motivated by the presence of life‐limiting illness to develop health literacy; that the motivation of these particularparticipants had resulted in high levels of health literacy and would have beenmeasuredassuch(samplebias);oralternativelythattherearesystemicbarriersinthehealth care system that prevent the translation of health literacy practices into highlevelsofmeasureablehealthliteracy,sonomatterhowmanyhealthliteracypracticesthewhānauemploythereisabarriertoachievingmeasurablehealthliteracyforMāori.
Thesuggestionthatpatientsandwhānauaremotivatedtoimprovetheirhealthliteracybytheimportantdiagnosisoflife‐limitingillnessisconsistentwithbothadulteducationprinciples (Knowles et al 2005) andadult literacy studies (Sticht et al 1987).Furtherstudies are required to engage health professionals and health care providers indeveloping skills based on adult learning principles and assessing the outcomes ofthese.
It is not knownwhether patients andwhānauwere already using these practices inothercontextsbeforetransferringthepracticestothepalliativecarecontext.Nordoweknow whether they subsequently transferred these practices into other health carecontexts,althoughgiventhevalueplacedoninformationfromotherwhānaumembersorfriendswhohadbeenthroughpalliativecaresituations,wemightassumetheywere
55
also transferring information and health literacy practices to others facing palliativecare.
Asystematicreviewofhealthliteracyidentifiedthathealthliteracycanbeamediatorofracialdisparitiesinhealthoutcomes(Berkmanetal2011).Despiteaplethoraofhealthliteracy literature emerging in the past decade, this area remains emergent in NewZealandandrequiresfurtherresearch.
Nopatientsandwhānaureportedusinganadvancedcareplanningdirectiveor livingwill,nordidhealthprofessionalsdiscuss these.This isanarea for furtherresearch toestablishtheusefulnessofsuchdevices.
4.5 Communication
This study found that patients and whānau did not always experience goodcommunicationand,infact,experiencedpoorcommunicationonanumberofoccasions.A recentNew Zealand study identified patients’ and families’ dissatisfactionwith thequality and type of information provided; understanding of language used; ways ofbeing informed about patient’s condition; poor communication of ‘bad news’; stafflacking the skills to have these difficult conversations; staff not available to provideupdates;andalwaysbeingreactiveratherthanproactivearoundprovidinginformation(Robinson et al 2013). The experiences of patients and whānau in this study wereconsistentwithalltheseexamplesofpoorcommunication.
However,whānaualsoidentifiedaspectsofgoodcommunicationpracticesinpalliativecare settingswhich assistedwhānau in providing optimal support to their loved one.Effective communication greatly enhanced the whānau experience of palliative care.Generally,thewhānauparticipantsidentifiedthatindividualhealthprofessionalswereopenandhonestandtriedtoadvisewhānauoftherealityofthesituation.
Patientsandwhānaufoundthefollowingcommunicationprocessesusedbyhealthcareprofessionalswereeffectiveinsupportingthem:
abilitytocommunicate24/7withhealthprofessionals,toaskquestionsandhavetheirfearsallayed
establishedrespectfulrapportwithpatients practicaltrainingprovidedforwhānaucaregivers opportunity to have regularmeetingswithpeople providing care to patient to
discussprogress communicationbooktorecordwhatwashappening helpwithpredictingfuturecareneeds.
Whānaungatanga, kanohi ki te kanohi, wairuatanga, and the availability of Māorikaimahi (health professionals or allied staff) were all identified as importantcomponentsofaneffectivecommunicationmodelforMāoripatientsandwhānau.The

56
spiritual aspects of Māori health, Māori death, and of palliative care have been welladdressed in the literature(forexample,seeDurie1994;Fairbairn2002;Paley2008;Moeke‐Maxwelletal2010).Therelevanceofspiritualitytothehealth literacycontexthasnotyetbeenresearched.Rudd(2013)callsforcarefulexaminationofimpactofthesocial environment on health literacy; this research and the literature suggests thatwairuatangashouldalsobeviewedasanareaofpotentialimpactonhealthliteracyforMāori.
The communication processes identified by these participants was consistent withmuchoftheliteraturethatexaminesculturallyappropriatehealthcareforMāori(Durie1998;Crametal2003;Cormacketal2005;Jansenetal2008;Kiddetal2013).
Written resources Thereviewofthewrittenresourcessuppliedbypalliativecareprovidersfoundmultipleproblems. For example, they tended to use formal language and structures, werepassive in tone, included unfamiliar vocabulary without explanations, had highreadabilityscoresandcontainedlargeblocksoftext.FewpublicationsreferredtoMāorivaluesandconcepts.
Someservicesprovideda lotof information towhānauall atone time (ina folderorenvelope), and often different types of documents (e.g. information and instructions)werecombinedwithoutmaking itclearwhentherewasa transition fromonetypetotheother.
Health professional and key informant interviews suggested that there were oftenconflictingneedstoengagewiththepatientandwhānau,conductaninitialassessment,andprovidemandatory informationsuchasHealthandDisability literatureaswellasan agreement to receive care. Finding an opportunity to discuss resources at timescouldbequitedifficult.Asystematicreviewthatfocusedonsingleormultipleliteracy‐directed interventions (Sheridan et al 2011) reported that presenting only essentialinformation improved comprehension in individuals with low literacy and numeracycomparedwithprovidingessentialandnon‐essentialinformation.
Inthisstudy,thecombinationofeffective,culturallyrelevantcommunicationprocessesalongwithwrittenmaterialswas found to be themost valuablemeans of improvinghealthliteracy,althoughfurtherresearchisrecommendedtoconfirmthisfinding.
4.6 Systemic or organisational health literacy practices
This study found that some health professionals were individually building healthliteracy with their patients, but there was little evidence of palliative care serviceprovidersusingsystemicapproachestoreducinghealthliteracyproblems(DeWaltetal2011).

57
Thereisagrowingappreciationthathealthliteracydoesnotfocussolelyonindividualskill(Nielsen‐Bohlmanetal2004),soreducinghealthliteracydemandsneedstobeanactive,purposefulprocessdrivenbythehealthcareorganisation(Rudd2013).
Researchershavearguedthattheinterventionsrequiredtoensureorganisationshavetheattributestobehealthliterateinclude:havinghealthliteracyintegraltocorevalues;integrating health literacy into planning, evaluation, and quality improvement;workforcepreparedness;allowingandintegratingpopulationinput;meetingtheneedsofthepopulation;usinghealth literacystrategies incommunicationandconfirmation;providing easy access to navigate health information and services; utilising easy tounderstand design and distribution of materials; prior identification of high risksituationsforhealthliteracy;andcommunicatingclearlyaboutcosts(Brachetal2012).
Individual practices to build health literacy could be systematised and applied on anorganisational level, although further research would be required to evaluate theirefficacyforpatientsandwhānau.
Navigators Acommonthemefromthisresearchwastheimportanceofeffectivenavigationand/oradvocacytoaddresssomeofthehealthliteracyandaccessbarriers,whetherbywhānauand friends or as a specific palliative care services function, provided by navigators,kaiāwhina,oroutofexistingrolesasnursesorsocialworkers.Thesystemicprovisionof a navigator role has the potential to improve health literacy and reduce healthliteracydemands forpatientsandwhānau.Variationsof thenavigator rolehavebeensuccessfully implemented in a range ofNewZealandhealth care settings (Dohan andSchrag 2005; Freeman 2006; Doolan‐Noble et al 2013). A trial of such a role wouldprovide evidence of efficacy and satisfaction levels for Māori in the palliative carecontext.
4.7 Conclusion
This was a qualitative, exploratory study that utilised a purposive sample that wasbroadlyaccessedandminimallydefined;itspurposewastodevelopanunderstandingofhealthliteracyinpalliativecareforMāoriandtoidentifyfutureresearchpriorities.
Māori patients tend to struggle with access to palliative care services for reasonsrelating to the importance of maintaining tikanga whilst accepting health care, lowhealth literacy, availability of services, health professionals avoiding ormismanagingthe ‘hard conversations’ around the shift from treatment to palliative care, and the(sometimesmisperceived)culturalcharacterofspecialistpalliativecareservices.
HealthliteracyforMāoriinthepalliativecarecontextisacomplextopicwhichcanbemore effectively understood with further research. Health literacy demands areconsiderable,withpatientsandwhānauutilisingvariedhealthliteracypracticestomeetthe demands. Health professionals utilise individual strategies to help patients and

58
whānaumanagethepalliativecareenvironment,butthesearenotgenerallyadoptedatanorganisationallevel.
This study found that patients and whānau experienced poor communication on anumberofoccasions.However,whānaualsoidentifiedaspectsofgoodcommunicationpracticesinpalliativecaresettingswhichassistedwhānauinprovidingoptimalsupporttotheirlovedone.Effectivecommunicationgreatlyenhancedthewhānauexperienceofpalliativecare.Generallythewhānauparticipantsidentifiedthatindividualnurseswereopenandhonestandtriedtoadvisewhānauoftherealityofthesituationstheyfaced.
This study found that there was inconsistency about whether palliative care was apositive experience for Māori, with patients, whānau and health professionals allreportingbothpositiveandnegativeexperiences.This,alongwiththerealitythatMāoriareadiverse, flexibleandchangeablepeople (Reid2005),means thatgeneralisationsaboutculturallyeffectivehealthcarecannotbemade.
A research agenda which identifies and prioritises future research directions ispresentedinthenextsection.
59
Section 5: Research Agenda Life‐limitingillnessesdonothavetomeantheendofbeinginvolvedwithwhānauandenjoyingday to day life. Palliative care services exist to improve the quality of life ofpatients andwhānau facing theproblems associatedwith life‐limiting illnesses. Theirfocusisonaffirminglifeandprovidingrelieffrompainandotherdistressingsymptoms.Palliative care is provided according to an individual’s need, and may be suitablewhetherdeathisdays,weeks,monthsoroccasionallyevenyearsaway.
Palliativecareaimstooptimiseanindividual’squalityoflifeuntildeathbyaddressingthe person’s physical, psychosocial, spiritual and cultural needs, and support theindividual’sfamily,whānauandothercaregiverswhereneeded,throughtheillnessandafterdeath(PalliativeCaresubcommiteee:NZCancerTreatmentWorkingParty,2007).
Māorilifeexpectancyisimproving,andanincreasingproportionofMāoriareaged65years and older (Statistics New Zealand 2012). This, combined with high rates ofchronicandlife‐limitingillnesses(RobsonandHarris2007),lowlevelsofhealthliteracy(Ministry ofHealth 2010a), and inequalities aroundhealthcare access (Cormack et al2005; Crengle, et al 2005), means there is a growing need to understand access topalliativecareprovisionforMāori.
Experiencing a life‐limiting illness does not remove the patient from the nationalstrategic aim for improved wellbeing for Māori (Minister of Health and AssociateMinisterofHealth,2002),or fromtheneedto involvepatientsandwhānau inservicedeliveryplanning.
Two projectswere commissioned by theMinistry of Health and theHealth ResearchCouncilofNewZealandMāoriHealthJointVentureprogrammetoexploretheissueofMāori,palliativecareandhealthliteracy,andtodeterminethehealthresearchprioritiesthat will contribute to improved access for Māori to palliative care services and toimprovedpalliativecarehealthliteracy.
This project was led by the University of Auckland in partnership with UniServices,Workbase, and the Māori and palliative care communities in the Bay of Plenty andAuckland. Organisations that supported and contributed to the research includedWaipunaHospice,KaitiakiNursingService,HospiceEasternBayofPlenty,Kimihauora,Western Bay of Plenty PHO, Mercy Hospice, Hospice West Auckland, Te Whānau OWaipareira,AucklandDHBPalliativeCareTeam,andtheAucklandCancerSociety.
The two regions of Auckland and Bay of Plenty were chosen as they allowed us toexploreMāorihealth literacyandpalliativecare in largeurban,smallurbanandruralenvironments; in specialised palliative care settings (hospital and community‐basedspecialised hospice services); and in generalist services (including primary careproviders,bothMāoriand‘mainstream’).
60
Thevisionthatinformedtheresearchwasofpatientsandwhānaureceivingtimelyandeffective palliative care in a way that suits their needs and feels safe to access.Principles underpinning the research included 1) an integrative approach to theproblem of low health literacy for Māori that views health organisations, healthprofessionals,whānauandpatientsascontributorstothehealthliteracycontext,and2)a strengths‐based focus that assumes that Māori have successful strategies fornegotiatinghealthcareandseekstohighlightandworkwiththosestrategies.
The sister project was conducted by Rauawaawa Kaumātua Charitable Trust inpartnership with Waikato University. Organisations that contributed to the studyincluded HospiceWaikatoandthePalliativeCareUnitatWaikatoHospital,TeRūnangaoKirikiriroa, WaikatoDistrictHealthBoard, and theUniversityofAucklandWaikatoClinicalSchool.
The central focus of that studywas to identify access issues for kaumātua and theirwhānauinpalliativecareservices,usingahealthliteracyperspective.Healthliteracyisconceptualised as a multidimensional construct involving functional, technical,interactive, cultural, and critical/advocacy aspects. The vision for the study was todevelopappropriatemodelsofcommunicationthatcanbeutilisedwithinpalliativecareservices, including practices and interventions that enhance kaumātua and whānauknowledgeandexperienceofpalliativecare,andimprovedeliveryofthoseservicesbyclinicians and community health kaimahi (workers). The aim was to identify keycommunication practices that contribute to Māori health literacy and kaumātua andwhānau experiences of end‐of‐life planning and care, as well as clinicians’ andcommunitykaimahideliveryoftheseservices.
Theresearchdesignincludedtheestablishmentofanadvisorygroupandastakeholderend users group, a systematic review of New Zealand and international literature,interviews kaumātua, whānau hui (focus groups) and focus groups with palliativehealthcarekaimahi(workers),ananalysisofpromotionalbrochuresfromprovidersofpalliative care services, and a document audit of palliative care patients’ use ofEmergencyDepartmentswithinWaikatoDistrictHealthBoard(RauawaawaKaumātuaCharitableTrustResearchProjectTeam,2013).
Keyareasofinterestforbothprojectsresearchwere:
1. ThewaysinwhichMāoriaccesspalliativecareservices2. CurrentlevelsofMāorihealthliteracywithregardstopalliativecare3. How different factors within whānau influence the ability of Māori to obtain,
processandunderstandpalliativecareinformationandservices4. Identification of communication models which are effective in enhancing this
ability
The research agenda aims to prioritise translational research that can change orinfluencepalliativecareprovisionandhealthliteracyforMāori.
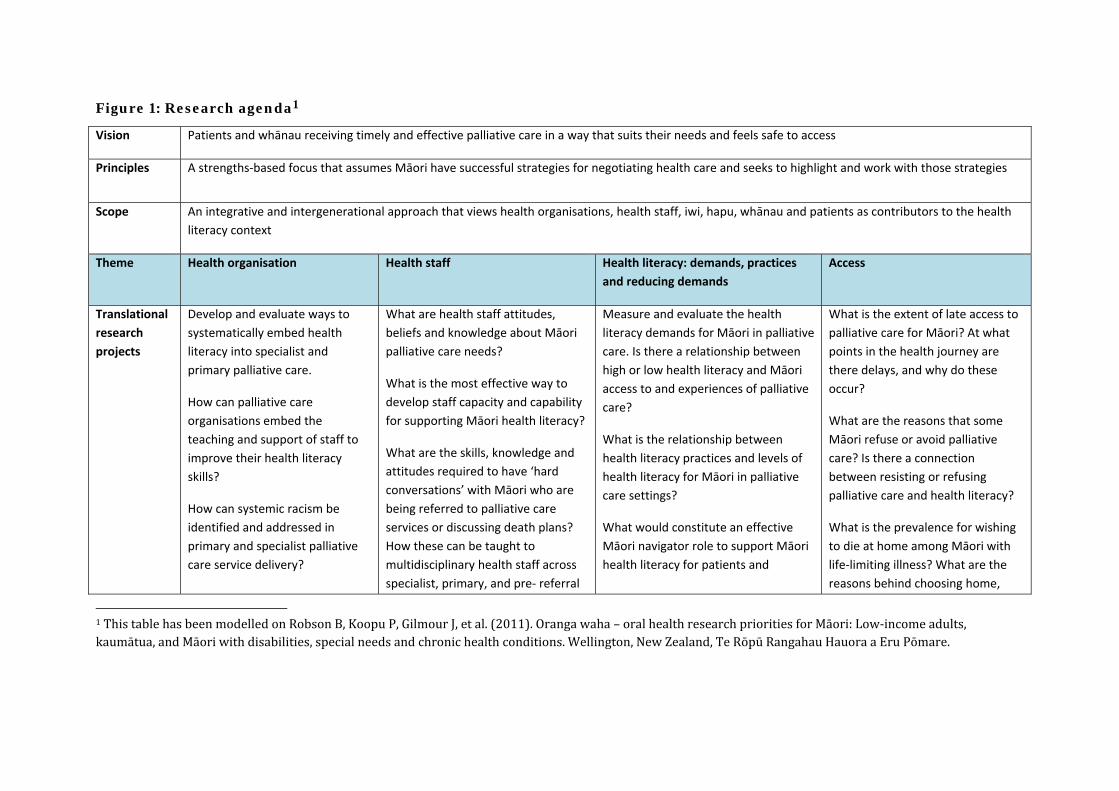
Figure 1: Research agenda1
Vision Patients and whānau receiving timely and effective palliative care in a way that suits their needs and feels safe to access
Principles A strengths‐based focus that assumes Māori have successful strategies for negotiating health care and seeks to highlight and work with those strategies
Scope An integrative and intergenerational approach that views health organisations, health staff, iwi, hapu, whānau and patients as contributors to the health
literacy context
Theme Health organisation Health staff Health literacy: demands, practices
and reducing demands
Access
Translational
research
projects
Develop and evaluate ways to
systematically embed health
literacy into specialist and
primary palliative care.
How can palliative care
organisations embed the
teaching and support of staff to
improve their health literacy
skills?
How can systemic racism be
identified and addressed in
primary and specialist palliative
care service delivery?
What are health staff attitudes,
beliefs and knowledge about Māori
palliative care needs?
What is the most effective way to
develop staff capacity and capability
for supporting Māori health literacy?
What are the skills, knowledge and
attitudes required to have ‘hard
conversations’ with Māori who are
being referred to palliative care
services or discussing death plans?
How these can be taught to
multidisciplinary health staff across
specialist, primary, and pre‐ referral
Measure and evaluate the health
literacy demands for Māori in palliative
care. Is there a relationship between
high or low health literacy and Māori
access to and experiences of palliative
care?
What is the relationship between
health literacy practices and levels of
health literacy for Māori in palliative
care settings?
What would constitute an effective
Māori navigator role to support Māori
health literacy for patients and
What is the extent of late access to
palliative care for Māori? At what
points in the health journey are
there delays, and why do these
occur?
What are the reasons that some
Māori refuse or avoid palliative
care? Is there a connection
between resisting or refusing
palliative care and health literacy?
What is the prevalence for wishing
to die at home among Māori with
life‐limiting illness? What are the
reasons behind choosing home,
1ThistablehasbeenmodelledonRobsonB,KoopuP,GilmourJ,etal.(2011).Orangawaha–oralhealthresearchprioritiesforMāori:Low‐incomeadults,kaumātua,andMāoriwithdisabilities,specialneedsandchronichealthconditions.Wellington,NewZealand,TeRōpūRangahauHauoraaEruPōmare.
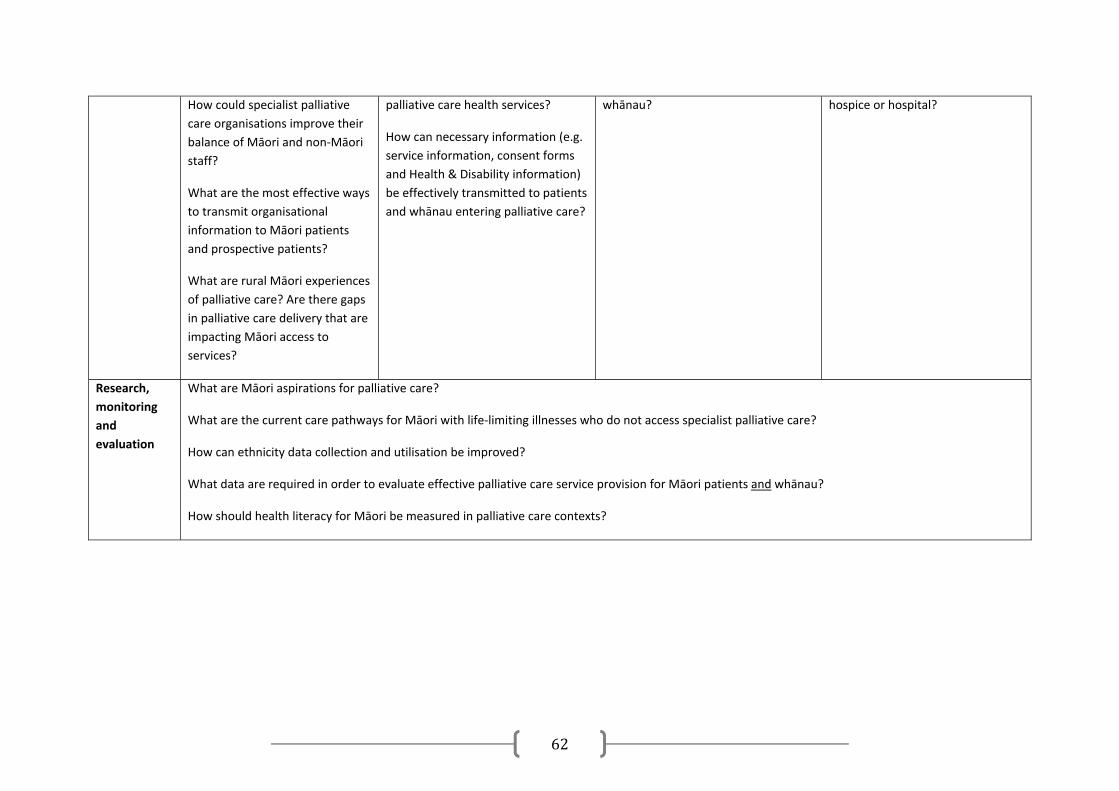
62
How could specialist palliative
care organisations improve their
balance of Māori and non‐Māori
staff?
What are the most effective ways
to transmit organisational
information to Māori patients
and prospective patients?
What are rural Māori experiences
of palliative care? Are there gaps
in palliative care delivery that are
impacting Māori access to
services?
palliative care health services?
How can necessary information (e.g.
service information, consent forms
and Health & Disability information)
be effectively transmitted to patients
and whānau entering palliative care?
whānau? hospice or hospital?
Research,
monitoring
and
evaluation
What are Māori aspirations for palliative care?
What are the current care pathways for Māori with life‐limiting illnesses who do not access specialist palliative care?
How can ethnicity data collection and utilisation be improved?
What data are required in order to evaluate effective palliative care service provision for Māori patients and whānau?
How should health literacy for Māori be measured in palliative care contexts?
References
BasuA,BrinsonD,WasanA,etal.2010.InterventionstoMitigatetheEffectsofLowHealthLiteracy:ASystematicReviewoftheLiterature.UniversityofCanterbury:HealthServicesAssessmentCollaboration.
BellamyG,GottM.2013.Whataretheprioritiesfordevelopingculturallyappropriatepalliativeandend‐of‐lifecareforolderpeople?TheviewsofhealthcarestaffworkinginNewZealand.Health&SocialCareintheCommunity21(1):26–34.
BerkmanN,SheridanS,DonahueK,etal.2011.HealthLiteracyInterventionsandOutcomes:AnUpdatedSystematicReview.Rockville,MD:AgencyforHealthcareResearchandQuality.
Bishop,R.2005.FreeingOurselvesfromNeocolonialDominationinResearch:AKaupapaMāoriApproachtoCreatingKnowledge.In:NKDenzinandYLincoln(eds.),TheSageHandbookofQualitativeResearch(pp.109–38).ThousandOaks,CA:Sage.
BrachC,KellerD,HernandezCB,etal.2012.TenAttributesofHealthLiterateHealthCareOrganizations.WashingtonDC:InstituteofMedicine,NationalAcademyofSciences.
Bray,Y,Goodyear‐Smith,F.2013.Patientandfamilyperceptionsofhospiceservices:‘Iknewtheyweren’tlikehospitals’.JournalofPrimaryHealthCare5(3):206–13.
BurgessTA,BrooksbankM,etal.2004.Talkingtopatientsaboutdeathanddying.AustralianFamilyPhysician33(1–2):85–6.
CagleJG,KovacsPJ.2009.Education:Acomplexandempoweringsocialworkinterventionattheendoflife.HealthandSocialWork34(1):17–27.
CastledenH,CrooksVA,HanlonN,etal.2010.Providers’perceptionsofAboriginalpalliativecareinBritishColumbia’sruralinterior.HealthandSocialCareintheCommunity18(5):483–91.
CormackD,RobsonB,PurdieG,etal.2005.AccesstoCancerServicesforMāori:AReportPreparedfortheMinistryofHealth.Wellington:WellingtonSchoolofMedicineandHealthSciences.
CramF,McCreanorT,SmithLT,etal.2006.KaupapaMāoriresearchandPakehasocialscience:EpistemologicaltensionsinastudyofMāorihealth.Hulili3(1):41–66.
CramF,SmithLT,JohnstoneW.2003.MappingthethemesofMāoritalkabouthealth.NewZealandMedicalJournal116(1170):1‐7.
CrengleS,Lay‐YeeR,DavisP,etal.2005.AComparisonofMāoriandNon‐MāoriPatientVisitstoDoctors:TheNationalPrimaryMedicalCareSurvey(NatMedCa):2001/02.Report6.Wellington:MinistryofHealth.
64
D’EathM,Barry,MM,SixsmithJ.2012.ARapidEvidenceReviewofInterventionsforImprovingHealthLiteracy.Stockholm:ECDC.
DavisP,Lay‐YeeR,DyallL,etal.2006.QualityofhospitalcareforMāoripatientsinNewZealand:Retrospectivecross‐sectionalassessment.Lancet367(9526):1920–25.
DeCourtneyCA,BranchPK,MorganKM.2010.GatheringinformationtodeveloppalliativecareprogramsforAlaska’sAboriginalpeoples.JournalofPalliativeCare26(1):22–31.
DeWaltDA,BroucksouKA,HawkV,etal.2011.Developingandtestingthehealthliteracyuniversalprecautionstoolkit.NursOutlook59(2):85–94.
DohanD,SchragD.2005.Usingnavigatorstoimprovecareofunderservedpatients:Currentpracticesandapproaches.Cancer104(4):848–55.
Doolan‐NobleF,SmithD,GauldR,etal.2013.Evolutionofahealthnavigatormodelofcarewithinaprimarycaresetting:Acasestudy.AustHealthRev37(4):523–28.
Durie,M.H.1994.Whaiora:MāoriHealthDevelopment.Auckland,OxfordUniversityPress.
Durie,M.H.1998.Whaiora:MāoriHealthDevelopment.Auckland,OxfordUniversityPress.
EuropeanHealthPolicyForum.2005.RecommendationsonHealthInformation.Brussels:EUHealthPolicyForum.
FairbairnG.2002.Agooddeath:Onthevalueofdeathanddying.NursingPhilosophy3(3):274–75.
FerrellBR.2005.Latereferralstopalliativecare.JournalofClinicalOncology23(12):2588–89.
FreemanHP.2006.Patientnavigation:Acommunitybasedstrategytoreducecancerdisparities.JUrbanHealth83(2):139–41.
FreyR,GottM,RaphaelD,etal.2013.‘WheredoIgofromhere’?Aculturalperspectiveonchallengestotheuseofhospiceservices.Health&SocialCareintheCommunity21(5):519–29.
FreyR,GottM,BellamyG.2012.UnderstandingBarriersandFacilitatorstoHospiceCareServicesAccessintheTotaraHospiceSouthAuckland.FinalReporttotheTotaraHospiceSouthAucklandandCMDHB.Auckland:UniversityofAuckland.
HamptonM,BaydalaA,BourassaC,etal.2010.Completingthecircle:Eldersspeakaboutend‐of‐lifecarewithAboriginalfamiliesinCanada.JournalofPalliativeCare26(1):6–14.
HotsonKE,MacdonaldSM,MartinBD,etal.2004.UnderstandingdeathanddyinginselectfirstnationscommunitiesinnorthernManitoba:Issuesofcultureand
65
remoteservicedeliveryinpalliativecare.InternationalJournalofCircumpolarHealth63(1):25–38.
Howden‐Chapman,B.,Blakely,T.,Blaiklock,A.,&Kiro,C.(2000).Closingthehealthgap.NewZealandMedicalJournal,113(1114),301.302.
JansenP,BacalK,CrengleS.2008.HeRitengaWhakaaro:MāoriExperiencesofHealthServices.Auckland:MauriOraAssociates.
JonesCP.2000.Levelsofracism:Atheoreticframeworkandagardener’stale.AmericanJournalofPublicHealth90(8):1212–15.
KehlKA,McCartyKN.2012.Readabilityofhospicematerialstopreparefamiliesforcaregivingatthetimeofdeath.ResearchinNursingandHealth35(3):242–49.
KellyL,LinkewichB,CromartyH,etal.2009.PalliativecareofFirstNationspeople:Aqualitativestudyofbereavedfamilymembers.CanadianFamilyPhysician55(4):394–95.
KickbuschI,WaitS,MaagD.2006.NavigatingHealth:TheRoleofHealthLiteracy.AllianceforHealthandtheFuture.London:AllianceforHealthandtheFuture,InternationalLongevityCentre.
KiddJ,GibbonsV,KaraE,etal.2013.OrangaTaneMāori:AwhānauorajourneyofMāorimenwithchronicillness:ATeKorowaianalysis.AlterNative:AnInternationalJournalofIndigenousPeoples9(2):125–41.
KnappC,MaddenV,MarcuM,etal.2011.Informationseekingbehaviorsofparentswhosechildrenhavelife‐threateningillnesses.PediatricBloodandCancer56(5):805–11.
KohHK,BerwickDM,ClancyCM,etal.2012.Newfederalpolicyinitiativestoboosthealthliteracycanhelpthenationmovebeyondthecycleofcostly‘crisiscare’.HealthAffairs31(2):434–43.
KripalaniS,WeissB.2006.Teachingabouthealthliteracyandclearcommunication.JournalofGeneralInternalMedicine21(8):888–90.
LamMK,LamLT.2012.Healthinformation‐seekingbehaviourontheinternetandhealthliteracyamongolderAustralians.electronicJournalofHealthInformatics7(2):e15.
LawrensonR,SmythD,KaraE,etal.2010.RuralgeneralpractitionerperspectivesoftheneedsofMāoripatientsrequiringpalliativecare.NewZealandMedicalJournal123(1315):30–6.
LoB,ParhamL.2010.Theimpactofweb2.0onthedoctor‐patientrelationship.JournalofLawandMedicalEthics38(1):17–26.
MaddalenaV,O’SheaF,MurphyM.2012.Palliativeandend‐of‐lifecareinNewfoundland’sdeafcommunity.JournalofPalliativeCare28(2):105–12.
66
MaddocksI,RaynerRG.2003.Issuesinpalliativecareforindigenouscommunities.MedicalJournalofAustralia179(6):S17–9.
McGrathCL.2000.IssuesinfluencingtheprovisionofpalliativecareservicestoremoteaboriginalcommunitiesintheNorthernTerritory.AustralianJournalofRuralHealth8(1):47–51.
McGrathP.2007.‘Idon'twanttobeinthatbigcity;thisismycountryhere’:ResearchfindingsonAboriginalpeoples’preferencetodieathome.AustralianJournalofRuralHealth15(4):264–68.
McGrathP.2008.FamilycaregivingforAboriginalpeoplesduringend‐of‐life:FindingsintheNorthernTerritory.JournalofRuralandTropicalPublicHealth7:1–10.
McGrathP,HolewaH,Kail‐BuckleyS.2007.“Theyshouldcomeouthere...”:ResearchfindingsonlackoflocalpalliativecareservicesforAustralianaboriginalpeople.AmericanJournalofHospice&PalliativeMedicine24(2):105–13.
McGrathP,HolewaH,OgiliveK,etal.2006.InsightsonAboriginalpeoples’viewsofcancerinAustralia.ContemporaryNurse22(2):240–54.
MelhadoL,BushyA.2011.ExploringuncertaintyinadvancecareplanninginAfricanAmericans:Doeslowhealthliteracyinfluencedecisionmakingpreferenceatendoflife.AmericanJournalofHospiceandPalliativeMedicine28(7):495–500.
MinisterofHealth2001.TheNewZealandPalliativeCareStrategy.Wellington:MinistryofHealth.
MinisterofHealthandAssociateMinisterofHealth2002.HeKorowaiOranga:MaoriHealthstrategy.Wellington:MinistryofHealth.
MinistryofHealth.2009.GapAnalysisofSpecialistPalliativeCareinNewZealand.ProvidingaNationalOverviewofHospiceandHospital‐basedServices.Wellington:MinistryofHealth.
MinistryofHealth.2010a.KoreroMarama:HealthLiteracyandMāori.Resultsfromthe2006AdultLiteracyandLifeSkillsSurvey.Wellington:MinistryofHealth.
MinistryofHealth.2010b.StatementofIntent2010–2013.Wellington:MinistryofHealth.
MinistryofHealth.2012.RauemiAtawhai:AGuidetoDevelopingHealthEducationResourcesinNewZealand.Wellington:MinistryofHealth.
MinistryofHealth.2013.TheHealthofMāoriAdultsandChildren.Wellington:MinistryofHealth.
Moeke‐MaxwellT,NikoraLW,TeAwekotukuN.2010.DyingtoResearch:AnAutoethnographicExplorationofResearchingMāoriandWhānauExperiencesofEndofLifeCare.4thInternationalTraditionalKnowledgeConference:KeiMuriiTeKāpar,Auckland:NgāPaeoteMāramatanga.

67
MoritaT,AkechiT,IkenagaM,etal.2005.LatereferralstospecializedpalliativecareserviceinJapan.JournalofClinicalOncology23(12):2637–44.
MorrisN,MacLeanC,ChewL,etal.2006.TheSingleItemLiteracyScreener:EvaluationofaBriefInstrumenttoIdentifyLimitedReadingAbility.BMCFamilyPractice7(26).DOI:10.1186/1471‐2296‐7‐21(accessed27October2012).
MuircroftW,McKimmJ,WilliamL,etal.2010.ANewZealandperspectiveonpalliativecareforMāori.JournalofPalliativeCare26(1):54–8.
NaylorW.2010.PositioningPalliativeCareinNewZealand.Wellington:PalliativeCareCouncilofNewZealand.
NaylorW.2012.NewZealandPalliativeCareGlossary.Wellington:PalliativeCareCouncilofNewZealand,HospiceNewZealand&MinistryofHealth.
NgataP.2005.Death,Dying,andGrief.In:MSchwass(ed),LastWords.ApproachestoDeathinNewZealand’sCulturesandFaiths(pp.29–40).Wellington:BridgetWilliamsBooksLimitedandTheFuneralDirectorsAssociationofNewZealand.
Nielsen‐BohlmanL,PanzerAM,KindigDA(eds).2004.HealthLiteracy:APrescriptiontoEndConfusion.CommitteeonHealthLiteracyBoardonNeuroscienceandBehavioralHealth.Washington,D.C:TheNationalAcademiesPress.
NutbeamD.2000.Healthliteracyasapublichealthgoal:Achallengeforcontemporaryhealtheducationandcommunicationstrategiesintothe21stcentury.HealthPromotionInternational15(3):259–67.
NutbeamD.2008.Theevolvingconceptofhealthliteracy.SocialScience&Medicine67(12):2072–78.
NutbeamD.2009.TheEvolvingConceptofHealthLiteracy:FarewellSpeechtotheUniversityofSydney.URL:http://notes.med.unsw.edu.au/CPHCEWeb.nsf/resources/Don+Nutbeam+farewell/$file/Nutbeam+Health+literacy+‐+Sydney+May+2009.pdf(accessed15September2012).
PaleyJ.2008.Philosophyandpalliativecare.NursingPhilosophy9(2):75–6.
PalliativeCareSubcommittee:NZCancerTreatmentWorkingParty.2007.NewZealandPalliativeCare:AWorkingDefinition.Wellington:NZCancerTreatmentWorkingParty.
RauawaawaKaumātuaCharitableTrustResearchProjectTeam.(2013).Māorihealthliteracyandcommunicationinpalliativecare:Kaumātua‐ledmodels.Hamilton,NewZealand:MinistryofHealth.
Reid,P.2005.ContemporaryPerspectives.In:MSchwass(ed),LastWords.ApproachestoDeathinNewZealand’sCulturesandFaiths(pp.45–7).Wellington:BridgetWilliamsBooksandTheFuneralDirectorsAssociationofNewZealand.

68
RobinsonJD,GottM,IngletonC,etal.2013.Patientandfamilyexperiencesofpalliativecareinhospital: Whatdoweknow?Anintegrativereview.PalliativeMedicine.DOI:10.1177/0269216313487568(accessed14July2013).
RobsonB,HarrisR(eds).2007.Hauora:MāoriStandardsofHealthIV.AStudyoftheYears2000–2005.Wellington:TeRōpūRangahauHauoraaEruPōmare.
RuddR,AndersonJE,OppenheimerS,etal.2007.HealthLiteracy:AnUpdateofPublicHealthandMedicalLiterature.In:JPComings,BGarner,CSmith(eds),ReviewofAdultLearningandLiteracy(pp.175–203).Mahwah,NJ:LawrenceErlbaumAssociates.
RuddR,MoeykensB,Colton,C.1999.HealthandLiteracy:AReviewoftheMedicalandPublicHealthLiterature.In:JPComings,BGarner,CSmith(eds),AnnualReviewofAdultLearningandLiteracy(pp.158–99).SanFrancisco,CA:Jossey‐Bass.
RuddR.2013.Neededactioninhealthliteracy.JournalofHealthPsychology18(8):1004–10.
RuddRE,KirschIS,YamamotoK.2004.LiteracyandHealthinAmerica.Princeton,NJ:ETSPolicyInformationCenter.
SepúlvedaC,MarlinA,YoshidaT,etal.2002.Palliativecare:TheWorldHealthOrganization’sglobalperspective.JournalofPainandSymptomManagement24(2):91–6.
ShahidS,ThompsonS.2009.AnoverviewofcancerandbeliefsaboutthediseaseinindigenouspeopleofAustralia,Canada,NewZealandandtheUS.AustralianandNewZealandJournalofPublicHealth33(2):109–18.
ShawS,HuebnerC,ArminJ,etal.2009.Theroleofcultureinhealthliteracyandchronicdiseasescreeningandmanagement.JournalofImmigrantMinorityHealth11:460–67.
SheridanS,HalpernD,VieraA,etal.2011.Interventionsforindividualswithlowhealthliteracy:Asystematicreview.JournalofHealthCommunication16:30–54.
ShewardK,ClarkJ,MarshallB,etal.2011.Staffperceptionsofend‐of‐lifecareintheacutecaresetting:ANewZealandperspective.JournalofPalliativeMedicine14(5):623–30.
SmithLT.2005.OnTrickyGround:ResearchingtheNativeintheAgeofUncertainty.In:NKDenzinandYLincoln(eds.),TheSageHandbookofQualitativeResearch(pp.85–108).ThousandOaks,CA:Sage.
StatisticsNewZealand.2012.NewZealandPeriodLifeTables:2010–12.URL:www.stats.govt.nz/browse_for_stats/health/life_expectancy/NZLifeTables_HOTP10‐12.aspx(accessed14January2013).
69
SudoreRL,LandefeldCS,Perez‐StableEJ,etal.Unravelingtherelationshipbetweenliteracy,languageproficiency,andpatient‐physiciancommunication.PatientEducationandCounselling,75(3):398‐402.
SudoreRL,SchillingerD.2009.Interventionstoimprovecareforpatientswithlimitedhealthliteracy.JournalofClinicalOutcomesManagement16(1):20‐9.
TaylorA,BoxM.1999.MulticulturalPalliativeCareGuidelines.URL:www.palliativecare.org.au/Portals/46/resources/MulticulturalGuidelines.pdf(accessed17February2013).
ThomasDR.2006.Ageneralinductiveapproachforanalyzingqualitativeevaluationdata.AmericanJournalofEvaluation27(2):237–46.
TiemanJ,RawlingsD.2008.Exploringnursesattitudesto,anduseof,anonlinepalliativecareresource.InternationalJournalofPalliativeNursing14(2):587–94.
TreloarC,GrayR,BrenerL,etal.2013.Healthliteracyinrelationtocancer:AddressingthesilenceaboutandabsenceofcancerdiscussionamongAboriginalpeople,communitiesandhealthservices[Epubaheadofprint].HealthandSocialCareintheCommunity.DOI:10.1111/hsc.12054(accessed17February2013).
UnitedNations.2008.UnitedNationsDeclarationontheRightsofIndigenousPeoples.NewYork,UnitedNations.
VolandesAE,BarryMJ,ChangY,etal.2010.Improvingdecisionmakingattheendoflifewithvideoimages.MedicalDecisionMaking30(1):29–34.
VolandesAE,FergusonLA,DavisAD,etal.2011.Assessingend‐of‐lifepreferencesforadvanceddementiainruralpatientsusinganeducationalvideo:Arandomizedcontrolledtrial.JournalofPalliativeMedicine14(2):169–77.
VolandesAE,Paasche‐OrlowM,GillickMR,etal.2008.Healthliteracynotracepredictsend‐of‐lifecarepreferences.JournalofPalliativeMedicine11(5):754–62.
WeeramanthriT.1997.“PaintingaLeonardowithfingerpaint”:MedicalpractitionerscommunicatingaboutdeathwithAboriginalpeople.SocialScience&Medicine45(7):1005–15.
WestlakeVanWinkleN.2000.End‐of‐LifeDecisionMakinginAmericanIndianandAlaskaNativeCultures.In:KBraun,JPietsch,PBlanchette(eds.),CulturalIssuesinEnd‐of‐LifeDecisionMaking(pp.127–44).ThousandOaks,CA,Sage.
Wittenberg‐LylesE,GoldsmithJ,RaganS.2011.Theshifttoearlypalliativecare:Atypologyofillnessjourneysandtheroleofnursing.ClinicalJournalofOncologyNursing15(3):304–10.
Workbase.2013.Literaturereviewofhealthliteracyeducation,trainingtoolsandresourcesforhealthproviders.Auckland:Workbase.
70
WorldHealthOrganization.2011.WHOdefinitionofpalliativecare.URL:www.who.int/cancer/palliative/definition/en/(accessed25April2012).
YeoG.2009.HowwilltheU.S.healthcaresystemmeetthechallengeoftheethnogeriatricimperative?JournaloftheAmericanGeriatricsSociety57(7):1278–85.
71
Glossary2 AdvanceDirective:Instructionsthatconsentto,orrefuse,specifiedmedicaltreatmentorprocedureinthefuture.
AdvancedirectivesaredefinedintheCodeofHealthandDisabilityServicesConsumers’Rights(theCode)aswrittenororaldirectivesinwhichthepatientmakesachoiceaboutapossiblefuturehealthcareprocedure,andthischoiceisintendedtobeeffectiveonlywhenthepatient isno longercompetent.For thisreason,advancedirectivesarealso,thoughlessfrequently,referredtoas‘livingwills’.
Right7(5)oftheCodegiveseveryconsumerthelegalrighttouseanadvancedirectiveinaccordancewithcommonlaw.
Death: The cessation of all vital functions of the body, including the heartbeat,breathingandbrainactivity(includingthebrainstem).
Dying:Apersonisconsideredtobedyingwhentheyareintheprocessofpassingfromlife to death. It is characterised by a gradual failing of vital functions including thecardiac,respiratoryandcentralnervoussystems,followedbyanabsenceofcriteriathatdefine life (spontaneous heartbeat, breathing and brain function). The dying phase isgenerally considered to beminutes to hours in duration, but can occasionally be justseconds.
End‐of‐LifeCare:End‐of‐lifecare is theprovisionofsupportiveandpalliativecare inresponsetotheassessedneedsofthepatientandfamily/whānauduringtheend‐of‐lifephase.Itfocusesonpreparingforananticipateddeathandmanagingtheendstageofalife‐limitingorlife‐threateningcondition.Thisincludescareduringandaroundthetimeof death, and immediately afterwards. It enables the supportive and palliative careneedsofboth thepersonandthe family/whānautobe identifiedandmet throughoutthe lastphaseof lifeandintobereavement. It includesmanagementofpainandothersymptoms and provision of psychological, social, spiritual and practical support andsupportforthefamily.
GeneralistPalliativeCare:Referto‘PrimaryPalliativeCare’.
Hinengaro:Mind,thinkingprocess.
Hospice:Hospice isnotonlyabuilding; it isaphilosophyofcare.Thegoalofhospicecareistohelppeoplewithlife‐limitingandlife‐threateningconditionsmakethemostoftheirlivesbyprovidinghighqualitypalliativeandsupportivecare.
Hospicesprovidecareforthewholeperson,notjusttheirphysicalneedsbutalsotheiremotional, spiritual, and social needs. They also care for families and friends, both
2ThisglossaryhasbeenadaptedfromtheNewZealandPalliativeCareGlossary(2013)publishedbytheNewZealandPalliativeCareCouncil,HospiceNewZealand&theMinistryofHealth,andKidd,Gibbons,etal.(2013).
72
beforeandafteradeath. Irrespectiveofwhereahospiceservice is, thisphilosophyofcaredoesnotchange. InNewZealandallaspectsofhospicecareareprovided freeofcharge.
Hui:Meeting.
Kaumātua: Elders. In some areas, including Waikato, this term refers to male andfemaleelders.
KaupapaMāori:Māoriideology.
Life‐Limiting Condition: A life‐limiting condition is one for which there is noreasonablehopeofcureandfromwhichthepersonwilldie.Someoftheseconditionscauseprogressivedeteriorationrenderingthepersonincreasinglydependentonfamilyandcarers.
Liverpool Care Pathway (LCP): The LCP is an evidence‐based, integrated carepathway that was developed to transfer the hospice model of care into other caresettings.TheLCPguideshealthcareprofessionalstodeliverbest‐practicecaretodyingpatients and their families/whānau in the last days and hours of life, irrespective ofdiagnosisorcaresetting.
Mirimiri:Massage.
Mokopuna:Grandchildren(sometimesabbreviatedtomoko).
PalliativeCare:TheWorldHealthOrganization (2011)definespalliative careas: “anapproach that improves the quality of life of patients and their families facing theproblems associated with life‐limiting or life‐threatening conditions, through theprevention and relief of suffering by means of early identification and impeccableassessment and treatment of pain and other problems, physical, psychosocial andspiritual.Palliativecare:
providesrelieffrompainandotherdistressingsymptoms; affirmslifeandregardsdyingasanormalprocess; intendsneithertohastennorpostponedeath; integratesthepsychologicalandspiritualaspectsofpatientcare; offersasupportsystemtohelppatientsliveasactivelyaspossibleuntildeath; offersasupportsystemtohelpthefamilycopeduringthepatient’sillnessandin
theirownbereavement; uses a team approach to address the needs of patients and their families,
includingbereavementcounselling,ifindicated; will enhance quality of life, and may also positively influence the course of
illness; is applicable early in the course of illness, in conjunctionwith other therapies
thatareintendedtoprolonglife,suchaschemotherapyorradiationtherapy,andincludes those investigations needed to better understand and managedistressingclinicalcomplications.”
73
ANewZealand‐specificdefinitionofpalliativecare is:Careforpeopleofallageswithalife‐limitingorlife‐threateningconditionwhichaimsto:
1. Optimise an individual’s quality of life until death by addressing the person’sphysical,psychosocial,spiritualandculturalneeds.
2. Support the individual’s family, whānau, and other caregivers where needed,throughtheillnessandafterdeath.
Palliative care is provided according to an individual’s need, and may be suitablewhether death is days, weeks, months or occasionally even years away. It may besuitable sometimeswhen treatments are being given aimed at improving quantity oflife.
Itshouldbeavailablewhereverthepersonmaybe.
It should beprovidedby all heath care professionals supported,wherenecessary, byspecialistpalliativecareservices.
Palliative care should be provided in such a way as to meet the unique needs ofindividuals fromparticularcommunitiesorgroups.These includeMāori, childrenandyoungpeople,immigrants,refugees,andthoseinisolatedcommunities.
Palliative Care Services: This term refers to any individual, team or organisationwhosecoreworkfocusesondeliveringpalliativecare,forexampleahospiceorhospitalpalliativecareteam.
PalliativeCareSystem:Thisrefers topalliativecareservices,primarypalliativecareproviders and the other factors that enable them to deliver palliative care, such ascommunication and coordination between providers. Without these ‘other factors’palliativecareproviderscannotfunctionaspartofa‘system’.
It is not simply the existence of primary palliative care providers and palliative careservicesthatcomprisesthepalliativecaresystem;itisthelinksthatexistbetweenthemthattietogether‘asystem’.
Patient:Apatientistheprimaryrecipientofcare.Inthepracticeofpalliativecare,thepatienttogetherwiththeirfamilyandcarersarethefocusofcare.
Primary Palliative Care: Primary palliative care is provided by all individuals andorganisations that deliver palliative care as a component of their service, but theirsubstantiveworkisnotinthecareofpeoplewhoaredying.Itispalliativecareprovidedfor thoseaffectedbya life‐limitingor life‐threatening conditionasan integralpartofstandardclinicalpracticebyanyhealthcareprofessionalwhoisnotpartofaspecialistpalliativecareteam.
In the context of end‐of‐life care, a primary palliative care provider is the principalmedical, nursing or allied health professionalwho undertakes an ongoing role in thecare of patientswith a life‐limiting or life‐threatening condition. A primary palliativecareprovidermayhave abroadhealth focusorbe specialised in aparticular field ofmedicine. It is provided in the community by general practice teams, Māori health
74
providers, allied health teams, district nurses, and residential care staff etc. It isprovided in hospitals by general ward staff, as well as disease‐specific teams – forinstanceoncology,respiratory,renalandcardiacteams.
Primarypalliativecareprovidersassessandreferpatients tospecialistpalliativecareserviceswhenthepatient’sneedsexceedtheirservicescapability.
Qualitycareattheendoflifeisrealisedwhenstrongnetworksexistbetweenspecialistpalliativecareproviders,primarypalliativecareproviders,supportcareprovidersandthecommunity–workingtogethertomeettheneedsofallpeople.
SpecialistPalliativeCare:Specialistpalliativecareispalliativecareprovidedbythosewhohaveundergonespecifictrainingand/oraccreditationinpalliativecare/medicine,working in the context of an expert interdisciplinary team of palliative care healthprofessionals. Specialist palliative caremaybeprovidedbyhospiceor hospital basedpalliative care services where patients have access to at least medical and nursingpalliativecarespecialists.
Specialist palliative care is delivered in two key ways in accordance with the NewZealanddefinitionofpalliativecare.
Directly – to provide direct management and support of patients andfamilies/whānau where more complex palliative care need exceeds theresources of the primary provider. Specialist palliative care involvement withanypatientandthefamily/whānaucanbecontinuousorepisodicdependingonthechangingneed.Complex need in this context is defined as a level of need that exceeds theresources of the primary team – thismay be in any of the domains of care –physical,psychological,spiritual,etc.
Indirectly – to provide advice, support, education and training of other healthprofessionalsandvolunteerstosupporttheprimaryprovisionofpalliativecareprovision.
Tikanga:Customsandtraditions,protocols.
Tinana:Physicalself,body.
Wairua:Spirit,soul,spiritofaperson.Wairuatangareferstothespiritualwellbeingoftheindividual.
Whānau:Whānaumeanstheextendedfamily,familygroup,afamiliartermofaddresstoanumberofpeople—inthemoderncontext the termissometimesusedto includefriendswhomaynothaveanykinshiptiestoothermembers.
Whānaungatanga:Formingconnections,relationships.
75
Appendix One: Literature Review ReviewTeam
ThisreportwasauthoredbyDrVeroniqueGibbons,ResearchFellowatWaikatoClinicalSchool,TheUniversityofAuckland,whodevelopedandundertooktheliteraturesearch,extractedthedata,conductedthecriticalappraisalsandpreparedthereport.
Acknowledgements
This reviewwas conductedunder the auspices of a contract co‐fundedby theHealthResearchCouncilofNewZealand(HRC)andtheMinistryofHealth(MoH)partnership,theMāoriHealthJointVenture,tojointlyfundMāorihealthresearchtopromotehealthoutcomesforMāori,ledbyDrJacquieKidd.
Purpose
Thepurposeofthis literaturereviewistosupportbetterservicedeliveryofpalliativecare and improved access to palliative care forMāori and theirwhānau. The reviewneeds to identify access issues for Māori and their whānau from a health literacyperspective.
AMāoriHealth JointVenturerequest forproposalsought toestablishaprojectwhichfocused broadly within the context of health literacy in palliative care. The SteeringCommitteeidentifiedfourkeyareasofinterest:
1. ThewaysinwhichMāoriaccesspalliativecareservices;2. ThecurrentlevelofMāorihealthliteracywithregardstopalliativecare;3. ThewayinwhichdifferentfactorswithinwhānauinfluencetheabilityofMāori
toobtain,processandunderstandpalliativecareinformationandservices;and,4. Theidentificationofcommunicationmodelswhichareeffectiveinenhancingthis
ability.
This literature review informs the accompanying research agenda to include gaps incurrentknowledgeandpolicyimplicationsacrosspalliativecarefromahealthliteracyandMāoricontext.
Assumptions
TheMinistryofHealthStatementofIntent2010–2013hasakeypriorityareato ‘workonissuesemergingasaresultofNewZealand’sageingpopulation:improvingthehealthand independence of older New Zealanders’ (p12) (Ministry of Health 2010). Thisreportfocusesmainlyonliteratureintheadultpopulation.
Scopeandmethods
WhileMāoriarereportedfromapopulationbasistohavelowhealthliteracy(Ministryof Health 2010) and low utilisation of palliative care (Minister of Health 2001), this

76
literaturereviewseekstomoveawayfromasolefocusonpatientsandacknowledgeshealth professionals and health service providers as having a critical role to play inhealthliteracy.
Thisliteraturereviewsoughtto:
1. Identify systemic and professional barriers that inhibit utilisation of palliativecareservicesforMāori
2. Explorehowhealth literacyprinciplesare incorporated intomaterials (writtenresourcessuchaspamphlets,internet,videosetc)inpalliativecare
3. Examine health literacy interventions in palliative care for Māori and theirwhānau.
Searches were carried out using Scopus which is the largest abstract and citationdatabaseofpeer‐reviewedresearchliteraturewithmorethan20,500titlesfrommorethan5,000internationalpublishers.Inaddition,itcoversPubMed(includesMEDLINE)andEmbase.
Freetextsearcheswereusedtoidentifykeywordsinthetitle,abstractandkeywords.Asearchofallfieldswastooresourceintensiveand,asanexample,pickedupwordsthatmayonlyappearinthereferencetitlesratherthaninthebodyofthetext.Inaddition,onlyarticlesorreviewarticleswererequested.Inrelationtothechoiceofsearchterms,Scopus relies on free text rounded by quotationmarks and therefore does not relatethese to Medical Subject Headings (MESH) as would be found in a database likeMEDLINE.However,viewingthesetermsinMEDLINEwecouldascertaintheusefulnessofeachcriterion.
This reviewdidnot seek towrite a comprehensive reviewof the literatureonhealthliteracyorpalliativecareassinglesearchterms.Thesehavebeendoneelsewhereandhavebeenusedutilisedinpolicydocuments(Nutbeam2000;MinisterofHealth2001;Nutbeam2008;Ministry ofHealth 2009;Ministry ofHealth 2010;Naylor 2010). Thefollowingstepswereusedtoconductthisreview.
Identifyingsearchterms
This section identifieshoweachgroupof terms relating topalliative care, indigenouspeoplesandhealthliteracywasdeveloped.
#1. Forpalliativecare:palliativecareorhospicecareorterminalcareorend‐of‐lifecare(26,913articles);
Palliative care became a search term on MEDLINE in 1996; prior to this, palliativetreatmentwasthetermused(1964–1995).Thischangerelatedtotheconceptofcarealleviating symptoms without curing the underlying disease (Stedman, 25th edition,quotedbyMEDLINE).Terminalcarerelatestomedicalandnursingcareofpatientsintheterminalstageofanillnessandhasbeenasearchtermsince1968.Hospicecareisamorebroadtermrelatingtospecialisedhealthcare,supportiveinnature,providedtoa
77
dying person. This concept has been a MEDLINE term since 1992 and includesbereavementcareforthefamily.
#2. ForIndigenouspopulations:NativeAmericanorAmericanIndianorIndigenousorFirstNationsorAlaskaNativeorCanadianIndianorCanadianNativeorInuitorAboriginalorMāoriorTorresStraitIslandorMetís)(50,603articles);
Indigenous peoples were identified using the United Nations modern understandingwhich includes: self‐identification as indigenous peoples at the individual level andacceptance by the community as their member; historical continuity or commonancestrywith pre‐colonial and/or pre‐settler societies; strong links to territories andsurrounding natural resources (primordial); distinct social, economic or politicalsystems;distinctlanguage,cultureandbeliefs;formernon‐dominantgroupsofsociety;and, resolve tomaintain and reproduce their ancestral environments and systems asdistinctivepeoplesandcommunities(UnitedNations2008).Weutilisedarticlesforthisreview from specific countries whose colonisation histories are similar to NewZealand’s:Canada,NorthAmericaandAustralia.
#3. Healthliteracy:Healthliteracyorliteracy(19,516articles).
The term Health Literacy has been in existence in the United States since the early1970s; however, it is identified as a newer search term onMEDLINE, as recently as2010. Inaddition, theMESHterms ‘PatientEducationasTopic’and ‘ConsumerHealthinformation’wereadded in2008.These latter terms relate to theprovisionofhealthinformation toconsumersorpatients concerning theirownhealthneedsand/orwithanemphasisonself‐careandpreventiveapproaches.InScopus,usingtheterm‘healthliteracy’ alone identified 2,763 articles, probably reflecting this relatively newterminology.Thesearchwasextendedto includehealthandliteracywherethewordsappearedwithin15wordsofeachother;thisaddedmorepublicationswhichsoughttoaddressthisarea(3,896articles).
Searchresults
The initial searches revolved around the three search strands of palliative care (#1),IndigenousPeoples (#2) andhealth literacy (#3).The combined searchesyielded thefollowingnumberofarticles:
Searchstrategy No.ofarticlesSCOPUS#1AND#2AND#3 1#1AND#2 96#1AND#3 39#2AND#3 330
Thenumbersofarticleswasanindicationoftheworkloadrequiredtoeffectivelysort,reviewandsynthesisetheliteraturereviewinthegiventimeframe.
78
Inclusioncriteria
All articles were restricted to the English language, published from 2000 until May2013.Inaddition,weidentifiedsecondaryreferencesfromreferencelistsofpublishedliterature.UnpublishedliteraturewassourcedfromtheNZPalliativeCareCouncilandHospice NZ, and through word of mouth from palliative care and health literacycolleagues.
Potentiallyrelevantstudieswereidentifiedbyreviewingtitlesandabstractsretrievedfromthebibliographicdatabases.Studiesthatwerepotentiallyrelevantwereretrievedinfulltextandscreenedforinclusion.
Focus
Thisliteraturereviewisfocusedonthethreequestionsasoutlinedinthescope.Theseare:
1. Identify systemic and professional barriers that inhibit utilisation ofpalliativecareservicesforMāori
The terms that reflected barriers were defined from identifyingMESH terms for theword‘barriers’andcapturingcommonwordsusedintitlesandabstractsinMEDLINE.ThisstrategyfoundthreeMESHheadingswhichwerefitforpurpose.ThesearchtermsinMEDLINEincludedCommunicationBarriers/orPatientAcceptanceofHealthCare/orHealth Services Accessibility/ or Attitude toHealth. In Scopus, the free text termsusedwere:barriersoracceptanceoraccessibilityorattitude(1,051,884).Thissearchwaslabelled#4.
Atotalof22full‐textarticleswereretrievedforfurtherreviewfromtheScopussearch.Afurtherfivearticleswereidentifiedfromreferencelistswhichmayhavebeenoutsidethe timeperiodbutprovided information referred to inprimaryarticles.Reasons forexcluding articles included not meeting our definition of indigenous populations,focusingonquantitativeoutcomes,commentariestoalreadyidentifiedfull‐textarticles,service evaluation, end‐of‐life in relation to critical care rather than palliative care,opinionpieces andpolicydirectives. Themajority of studieswerequalitative studies,the methodology of which lends itself to studies on palliation due to its socialphenomenon,non‐quantifiableoutcomesandalimitednumberofparticipants(Hotsonetal2004).
Dyingathomeisacommonthreadforindigenouspeoplesforanumberofreasons.Ofthosewhodiedfromcancerin1996,Māoriweremorelikelytodieathomethannon‐Māori (53.2% and 30.8% respectively) (Minister of Health 2001). Often identified inliteraturewasthedesiretobecaredforbyrelatives(Kellyetal2009;DeCourtneyetal
Searchstrategy No.ofarticlesSCOPUS#1AND#2AND#4 51Fulltextretrieved 22
79
2010).ResearchonAboriginalpeoplesofCanadahighlightedthetraditionofcaringforthepersonwhoraisedthemtotheendoftheirlifeandtheviewsheldthatbynotdoingthisyouwereappearingungrateful(DeCourtneyetal2010).Thiscircleoflifeanddeathwaspartof theexpectation that familymemberswould care for eldersathome.Thiscaringprocessidentifiedtherolethatcarersplayedinhelpingthedyingpersonandalsoinsupportingfamilymembersbyproviding ‘energy’ tohelpthepersonpassfromthisworldtothenext(Hamptonetal2010).Notonlyissupportneededinprovidingenergyforthedyingperson’stransition,carersneededemotionalaswellaspracticalsupport(McGrath2008).ForMāori,likewise,relativesandfriendsarereportedasgatheringatthebedsideofMāoritoprovidespiritual,emotional,moralandphysicalsupportforthedyingpersonandtheirfamily(Ngata2005).AswithCanadianAboriginalpeoples,Māori‘energies’, both unseen and unspoken, are describedwhich connect the physical andspiritualenvironments(Muircroftetal2010).Thecentralityof familyandcommunitywasdemonstratedstronglyintheliterature(Ngata2005;Kellyetal2009;DeCourtneyetal2010).
Dyingathomewasalsorelatedtoculturalfactors.Thegeographicalconceptof‘Home’reflectstheAustralianAboriginal’s‘deathcountry’,wherethesoulandspiritaretiedtothe land (McGrath2007).Geographic isolationpresented itsown issues in relation toprovision of community‐based palliative care (Hotson et al 2004). These includedlimitedspecialistmedical treatment, theabsenceofacommittedprimarycaregiver inan isolated location,and the lackof inpatient care forpatients requiringadmissionattheterminalphaseofillness.
Whiletheliteratureappearstobeinclusiveintheviewthatindigenouspeopleswouldrejecthospitalpalliativecareservicesduetothewish(and/orexpectation)forfamilytobepartofthecaregiving,therewereoccasionsinliteraturewhichdescribedsituationswhereserviceshavenotbeenrejected.Firstly,inonecommunity,therewasabeliefthatdyingathomewouldbenegativeforthefamilyduetopartofthedyingperson’sspiritbeingleftbehind(Hotsonetal2004).Inanotherstudy,therewasstigmaattachedtoaperson dying at home; the family did not want to be held responsible for the death(blame)(McGrath2008).Secondly,palliativecareserviceswereanecessity, toenablefamily to have ‘time off’ (respite). However, a barrier to this was that for familieswanting temporary relief from caring there was confusion around the utilisation ofhospice care concerning its availability for respite or its use during an acute episode(Freyetal2012).
Alackofresourcesinthecommunity,oftencitedinruralandremotecommunities,wasa barrier for families in not being able to look after a familymember. Serviceswerecommonlylocatedinthecity,oftenquitefarfromtheirhome(McGrath2008).
Finally,thebreakdownofthefamilystructureimpactedontheuseofhospice/hospitalpalliativecareservices(Weeramanthri1997).

80
Overathree‐yearperiod(2008–2010),anincreasehadbeenreportedinthenumbersofMāoridyingatonehospicewhencomparedtothelocalhospital,suggestinganincreaseinhospiceasaplaceofdeathforMāori.However,onfurtheranalysis,theoddsofMāoridying at hospice remained lower than for NZ Europeans and was not statisticallysignificant (p = .744) (Frey et al 2012). Larger studies would be needed to test thisfindingandtomodelfuturebehaviour.
Researchhaslookedatcertainrulesevidentinsomehospitalorhospicesettingswhichmay conflictwith the cultural requirements towards the endof life. For example, theconceptofvisitinghoursastheyareimposedinsomesettingswasdescribedasalientopeoplewho,duringthefinaldays,wantedtoensuretheenvironmentremainedupbeatsothattheenergytopasstothenextworldwasdonepositively(Hamptonetal2010).Thenumberofvisitors,asapersonisdying,dependedonextendedkinshipnetworksofpeoplewhocametopaytheirlastrespectsbeforedeath(McGrath2008).Visitinghoursandpolicyaroundwhoandhowmanycanvisitcouldbeatoddswiththisconcept.ForMāori,seeingpeoplewhiletheywerestillalivewasreportedtobeimportant:extendedfamilybroughtwiththemtheirspirit,lifespark,collectiveconcern,loveandsympathytopromotehealingandrecovery(Ngata2005).Atdeath,Māorihavebeenreportedasidentifying the need to ensure the deceased “is kept warm and comforted by thepresence of kinfolk to calm the soul and assist it on its journey to the spirit world”(Ngata 2005, p.33). A lack of primary palliative care services and respite facilities inruralandremotelocationshasbeencitedasabarriertoprovidingsupportattheendoflife for those who wish to remain with their communities (McGrath et al 2007;Lawrensonetal2010).Culturallysensitivecarerequiredaccesstofamilysupportsandtraditionalservicesifrequested(Hotsonetal2004).
Beliefsaboutthecausesof illnessareoftencitedwhenthemechanismsofdiseasearegivenwithoutthemeaningastowhyapersonhadaparticulardisease(McGrathetal2006). Attributes of blame for having a terminal illness were reported as beingattributedtoselforancestralwrongdoings–asortofpayback(MaddocksandRayner2003; McGrath 2008) and thismight inhibit family from seeking palliative care. Theconceptof‘blame’inAboriginalAustralianswasstronglyrelatedtothereasonsfortheillnessand links tokinship tiesandtraditional law(Weeramanthri1997).The ideaofpaybackwasalsoafeatureofMāoriculture(Ngata2005).Researchershaveidentifiedthatthismayleadtoadditionalstressonthepatientwhomaybeunwillingtotalkabouttheir disease for fear of bringing shame to the family and community (Shahid andThompson2009).Furthermore,refusingcaremaybeasaresultofacceptance;thattheyarebearingthepaintoprotecttheirfamiliesfromfurthersufferingcausedbya‘curse’orpayback.
In researchwithhealthprofessionals, itwaspointedout that caring forapersonofadifferentculturecouldbringaboutitsownanxiety(McGrath2000).AlackofphysicianandnurseawarenessoftraditionalbeliefsheldbythecommunityregardingdeathwasabarriertocareinastudyofremotecommunitiesinCanada(WestlakeVanWinkle2000;
81
Hotson et al 2004). It was recommended that health professionals who providepalliative care inmulticultural societiesmust “set aside our own beliefs and seek tounderstandtheneedsoftheotherperson”(TaylorandBox1999,p.13).Itwasarguedthattherewasaneedforhealthprofessionalstorecognisethateachpersonwasuniqueandthatpartoffollowingprotocolswasrecognisingthateachindividualwasdifferent,“becausetheCreatormadeussouniquethateventhatwayofgoingisunique.Sothere’snot one way of doing it. Everyone will have their own” (Hampton et al 2010, p.12).Thesedifferenceswerealsoattributedto‘traditional,acculturatedorreligiouspractice’(WestlakeVanWinkle2000;Hotson,etal2004).Inaddition,foragroupsuchasMāori,whoweredescribedbyReid(2005)asbeingdiverse,flexibleandchangeable,therewasa danger inmaking generalisations about cultural identity based onwhatReid called“museumexhibitsofpastbehaviours”(Reid2005,p.47).
The construct of death was highlighted in research as different within westernmedicine‐oriented models (where death is the enemy) and Canadian Aboriginalunderstandings of death as a transition fromMother Earth (Hampton et al 2010). Inaddition,itwasarguedthatitmustberecognisedthategalitarianprinciplestoprovidequalitycaretoallpeoplemightcauseharmtocultureswhoseneedsandexpectationsdifferfromthedominantculture(McGrath2000).
Five articles focused solely on the perspectives of health professionals who providepalliativecare,asopposedtoincludingtheviewsofpatientsortheirfamilies/whānau.The articles were identified specifically for their inclusion of discussion aboutindigenouspopulations.Threearticleswere fromNewZealand,one fromCanadaandonefromAustralia.
GPfocusgroupsinAustraliasuggestedthatGPsneededtodevelopconfidenceintalkingaboutdeathanddying,withoneGPnotingthatthereluctanceofGPstoworkwithdyingpatientsmayreflect theirown fearofdeath (Burgessetal2004).These focusgroupswere made up of GPs who had an interest in palliative care; however, GPs wereparticularlyconcernedwithhavingaccesstosupport[forthemselves]whencaringfordyingpatientsfrom‘othercultures’,acommentwhichstronglyidentifiedthattheGPswere from the ‘dominant’ culture. This study might have been strengthened withdiscussion of different views about the needs of indigenous peoples, not solely onmedicalneeds.
A surveyof hospital staff perceptionsof current end‐of‐life carewas conducted in anacute hospital setting to gather a baseline understanding of challenges facing NZpalliative care services (Sheward et al 2011).Nurses described assessment, advocacyand a form of brokerage on behalf of patients, even though at times differentperceptions led to conflict with medical staff. A barrier to achieving good symptomcontrol forpatients, identifiedpredominantlybynursingrespondents,was the lackofknowledge among health professionals about how to care for a dying patient. Otherbarrierswhich contributed to challengingdynamics includedprofessionaldifferences,

82
staffculturalbackgroundsandpersonalvaluesandbeliefsstemmingfromattitudestodeathanddying.
Access tospecialistpalliativecareservices inruralareashasbeenacknowledgedasaconcern (Minister ofHealth 2001).ManyMāori live in rural areas ofNZ or return totheir ancestral/tribal home when terminally ill; researchers have argued this meanstheyaredisadvantagedintheiraccesstospecialistpalliativecareservices(Lawrenson,etal2010).Asurveyof186ruralNewZealandGPsaimedtoidentifytheirperspectivesoftheneedsofMāoripatientsreceivingpalliativecareandtodiscoverwhatGPsdidtomeettheseneeds(Lawrensonetal2010).ThestrongestthemefromGPswastheneedto involve whānau in the management of Māori patients needing palliative care,includingtheneedformoretimeforinteractionandcommunicationandtoidentifythekey people within the family. Identifying the decision‐maker in the family washighlightedasbeingimportant.Insomecasesitisamatterforhealthprofessionalstosimply ask who it is (DeCourtney et al 2010); in others, kinship ties may makeidentifying the ‘kinship network’more difficult but holding familymeetings has beensuggestedasameanstoensureawayof ‘sharingthestory’about theperson’s illnesswiththemostappropriatefamilymembers(McGrath2000).
A New Zealand study exploring the views of primary and specialist palliative careproviders regarding the provisions of culturally appropriate palliative and end‐of‐lifecare for older non‐Pākehā people demonstrated a number of identified barriers(BellamyandGott2013).Inagreementwithotherstudies,itwasacknowledgedthattheinvolvementoffamilywasfundamentaltotheprovisionofpalliativecareandforMāori,allowing family members to provide ‘hands‐on’ care. Again, the lack of space toaccommodatefamilymemberswhowereprovidingcareorwhoweretheretosupportthefamilyspirituallyimpactedonadifficultbutpotentiallyrewardingtime.Inresponse,the hospice setting provided adjoining rooms where families could be close to andprovide care to their sick relative, while the residential setting housed groups awayfrom the other residents but were close enough at hand to provide support but notintrudeonotherpatientswhomaybepresent.
Discord around heath professionals’ decisions to change the direction of care fromactive management to palliative care appeared to cause a ‘sense of struggle’ with areluctance to ‘abandon’ treatment being perceived as failure by some medicalrespondents(Moritaetal2005;Wittenberg‐Lylesetal2011;BellamyandGott2013).Health professionals experienced ethical dilemmas associated with continuingtreatmentsthatwereperceivedtonotbeinthebestinterestofthepatient.Thefamiliesreported that they received insufficient preparation from health professionals forchanging the treatment focus fromactivemanagement topalliative care (Morita et al2005).Thismovefromactivetreatmenttopalliativecarewasdescribedastransitioningfrom a space of closed awareness (isolated journey), focusing on treatment and sideeffectsonly, toopenawareness (rescued journey),where the limitsofmedicinewere

83
acknowledged and end‐of‐life planning was openly discussed (Wittenberg‐Lyles et al2011).
ANZstudyaddressingthedevelopmentofprioritiesforculturallyappropriatepalliativecare and end‐of‐life care for older Māori, Pacific and Chinese people in AucklandreportedthatcaringforMāori(andPacific)peoplesinahospicesettingwaseasierthanproviding thesameservice toChinesepeople,due toMāoriandPacificbeliefsystemsaboutbeingmoreable to talkaboutdeathanddyingwhichreducedbarriers for staff(BellamyandGott2013).TheresearchersreportedthatsomeChinesefamilieswishedtokeeptheprognosisfromapatient,whichcomprisedarisktostaffofbeinginbreachof the Health and Disability Commissioner (Code of Health and Disability ServicesConsumers'Rights)Regulations1996.Itwasrecognisedthatamoreproactiveapproachwouldbea‘comfortedjourney’whichsituatedpalliativecareatthepointofdiagnosis;thereinsupportingpatientsandfamiliesthroughdiagnosisandsideeffectsoftreatmentby focusingcareonqualityof lifeandpatientgoals(Ferrell2005). Ithasbeenarguedthat Māori patients and familiesmay, therefore, bemore receptive to the comfortedjourney at an early stage (Wittenberg‐Lyles et al 2011). In identifying palliative carejourneys, therewere limitationsof placing the research in the settingof a hospiceorhospital palliative care service and it is not known whether these journeys from‘isolation’ to ‘rescued’occurredinthesamewayinacommunitysetting.Ahospitalorhospicewasseenasaplacetogotodie(Freyetal2012)andthisperceptionmaybeabarrier to utilising the services provided there especially where families were stillwishingtoremainpositive(BellamyandGott2013)orwishedtoremainclosetotheircommunities(McGrath2007).
Aqualitativecasestudytoexplorechallengesofdeliveringculturallysensitiveandsafepalliative care was undertaken with a small minority Aboriginal population in ruralBritishColumbiawheretherewasalackofformalpalliativecareservices(Castledenetal 2010). Participants included nurses, doctors, health care administrators, hospicevolunteersandemployees,alliedhealthcareworkersandafamilycaregiver.MuchwasdiscussedonwhethertherewasanAboriginalpopulationinthatareatothepointthatasservicesbecameincreasinglydifficulttoaccess,‘theyjustreturntotheplacefamiliartothem’.Oneparticipantdescribedserviceprovisiononanindividualbasisyetthiswascontradictedbyanotherwhostatedthatculturaldifferencesweresetasidesopatientsreceived equal access and care. However, an example of observed racism wasexpressed.Talkinginamannerthatconveyedageneralistview,apersonwasreportedassaying, ‘Youpeoplearealways. . .’ inanelevatedvoice,which left thepatient(withadditionalchronicdiseaseneeds)scared,distrustfulandwithoutdignity–likelynevertoreturn formuchneededcare.For thisstudy, the lackofvisibilityof the indigenouspopulation and their traditions was a barrier to addressing cultural and conceptualdifferencesandinprovidingculturallysensitivecarepracticestothispopulation.
Insummary, in identifyingbarriers that inhibitedutilisationofpalliativecareservicesforMāori, itwasrecognisedthatgenerally indigenouspeopleswish todieathome.A

84
home environment was related to the familiarity of being cared for by their familymembers,the ‘circleof life’wheretheywerebornanddie,gainingenergyfromfamilyand community inmoving across to the other side, and in receiving support for thefamilytoenablecaringtotakeplace.Duetoalackofspecialistpalliativecareservicesinmany rural areas and the limitations of primary palliative care services, themove tospecialistpalliativecareserviceswasoftenawayfromthecommunity,thusisolatingthepatient from their support structures of family and community at an important timetowards the end of their life. The move to palliative care units and hospices wasidentifiedasalien—in termsofhaving rulesandstructureswhichmaynoteffectivelyaccommodatetheneedsofthe indigenouspatient.Notwithstandingvisitinghours, theability of specialist palliative care services to address the needs of indigenouspopulationswasreportedasbeingdependentontheknowledgeandwillingnessofstaffto ‘allow’ care to be provided in a culturally sensitive manner. The provision ofcaregivingbyafamilymemberinahospital‐likeenvironmentwasarguedaspotentiallyin conflictwithhealthprofessionalswhowere reluctant to relinquishcareormedicalstaff who may feel a sense of failure if supposed life‐prolonging treatments werediscontinued. In addition, the availability of space for family members, who wish toprovidecare,wasreportedtobelimited.Theabilitytoprovidecomprehensivecarewascalled to questionwhen health professionalswithin specialist palliative care servicessupportthenotionthatsomestaffmaybebetteratcaringforpatientstowardstheend‐of‐life thanothers. It isworthconsidering the turnoverofworkforcewithinpalliativecareserviceswhichmay impacton the relationshipbetween familiesand theservice.Furthermore, there remained a strong call formore indigenous healthworkers to beavailable tosupporthealthprofessionalswhocare for indigenouspatients.Theuseofmembersof thetargetethniccommunity inworkingalongsidepalliativecareserviceswassuccessfullymodelledintheUS(Yeo2009).
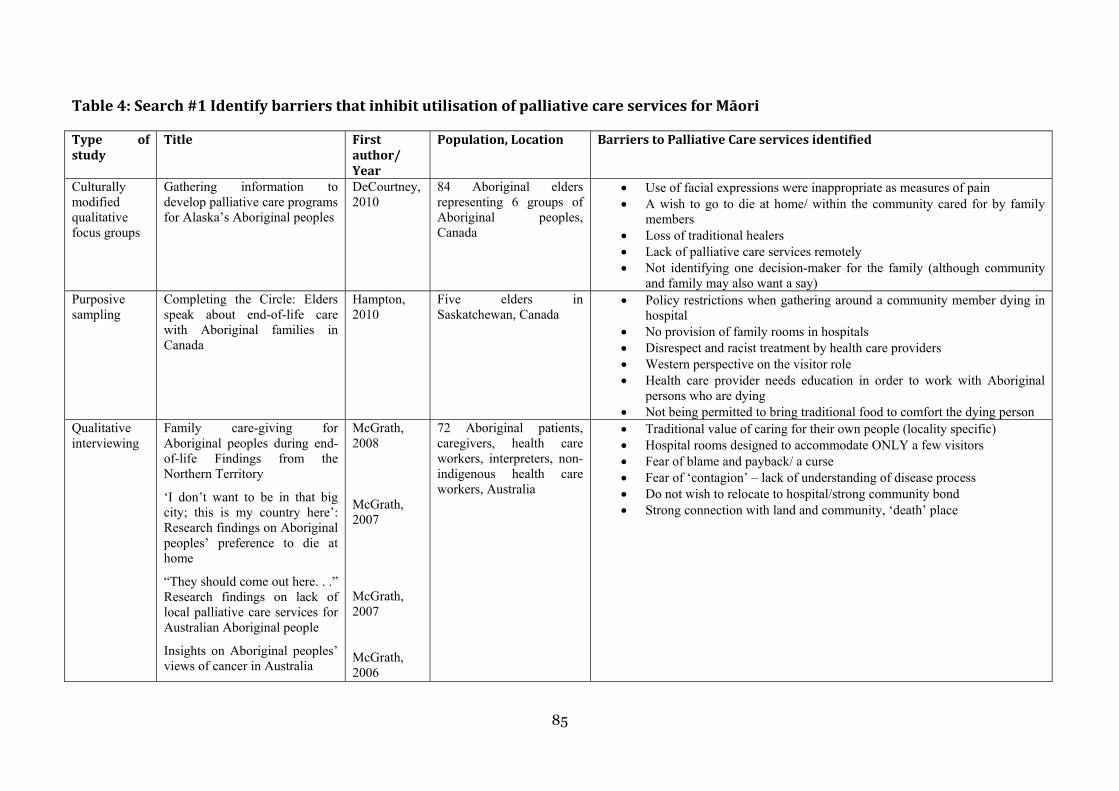
85
Table4:Search#1IdentifybarriersthatinhibitutilisationofpalliativecareservicesforMāori
Type ofstudy
Title Firstauthor/Year
Population,Location BarrierstoPalliativeCareservicesidentified
Culturally modified qualitative focus groups
Gathering information to develop palliative care programs for Alaska’s Aboriginal peoples
DeCourtney, 2010
84 Aboriginal elders representing 6 groups of Aboriginal peoples, Canada
Use of facial expressions were inappropriate as measures of pain A wish to go to die at home/ within the community cared for by family
members Loss of traditional healers Lack of palliative care services remotely Not identifying one decision-maker for the family (although community
and family may also want a say) Purposive sampling
Completing the Circle: Elders speak about end-of-life care with Aboriginal families in Canada
Hampton, 2010
Five elders in Saskatchewan, Canada
Policy restrictions when gathering around a community member dying in hospital
No provision of family rooms in hospitals Disrespect and racist treatment by health care providers Western perspective on the visitor role Health care provider needs education in order to work with Aboriginal
persons who are dying Not being permitted to bring traditional food to comfort the dying person
Qualitative interviewing
Family care-giving for Aboriginal peoples during end-of-life Findings from the Northern Territory
‘I don’t want to be in that big city; this is my country here’: Research findings on Aboriginal peoples’ preference to die at home
“They should come out here. . .” Research findings on lack of local palliative care services for Australian Aboriginal people
Insights on Aboriginal peoples’ views of cancer in Australia
McGrath, 2008 McGrath, 2007 McGrath, 2007 McGrath, 2006
72 Aboriginal patients, caregivers, health care workers, interpreters, non-indigenous health care workers, Australia
Traditional value of caring for their own people (locality specific) Hospital rooms designed to accommodate ONLY a few visitors Fear of blame and payback/ a curse Fear of ‘contagion’ – lack of understanding of disease process Do not wish to relocate to hospital/strong community bond Strong connection with land and community, ‘death’ place
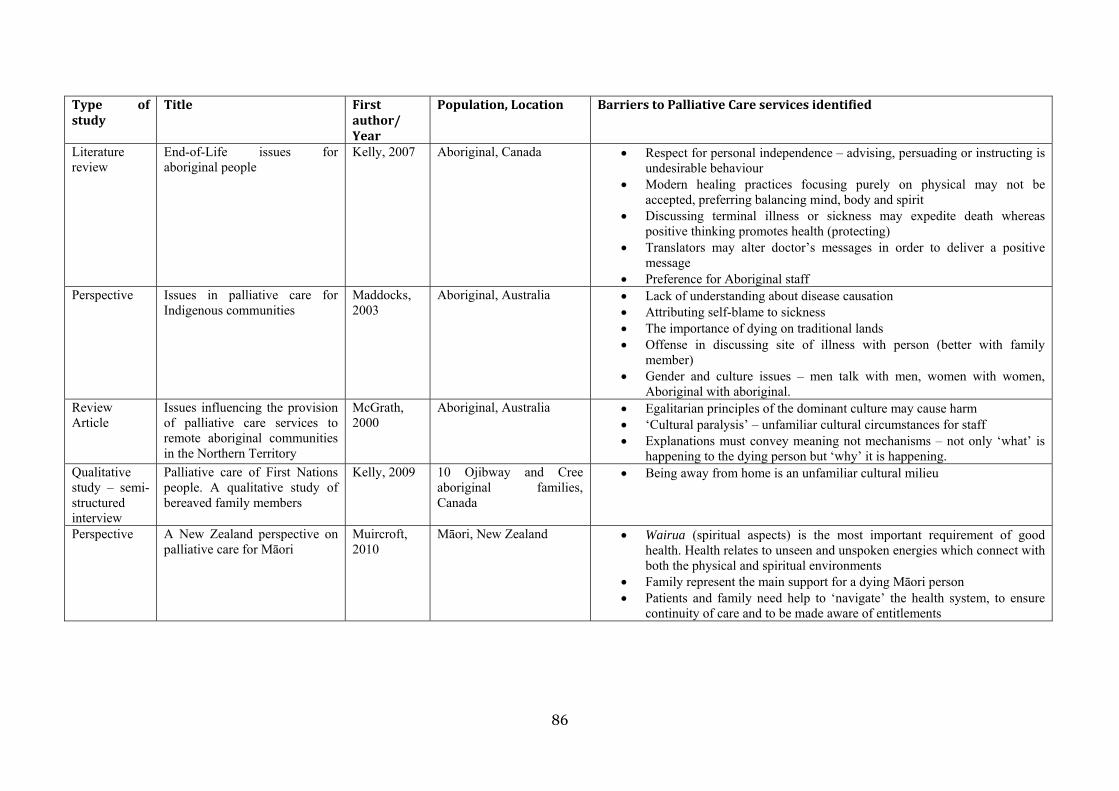
86
Type ofstudy
Title Firstauthor/Year
Population,Location BarrierstoPalliativeCareservicesidentified
Literature review
End-of-Life issues for aboriginal people
Kelly, 2007 Aboriginal, Canada Respect for personal independence – advising, persuading or instructing is undesirable behaviour
Modern healing practices focusing purely on physical may not be accepted, preferring balancing mind, body and spirit
Discussing terminal illness or sickness may expedite death whereas positive thinking promotes health (protecting)
Translators may alter doctor’s messages in order to deliver a positive message
Preference for Aboriginal staff Perspective Issues in palliative care for
Indigenous communities Maddocks, 2003
Aboriginal, Australia Lack of understanding about disease causation Attributing self-blame to sickness The importance of dying on traditional lands Offense in discussing site of illness with person (better with family
member) Gender and culture issues – men talk with men, women with women,
Aboriginal with aboriginal. Review Article
Issues influencing the provision of palliative care services to remote aboriginal communities in the Northern Territory
McGrath, 2000
Aboriginal, Australia Egalitarian principles of the dominant culture may cause harm ‘Cultural paralysis’ – unfamiliar cultural circumstances for staff Explanations must convey meaning not mechanisms – not only ‘what’ is
happening to the dying person but ‘why’ it is happening. Qualitative study – semi-structured interview
Palliative care of First Nations people. A qualitative study of bereaved family members
Kelly, 2009 10 Ojibway and Cree aboriginal families, Canada
Being away from home is an unfamiliar cultural milieu
Perspective A New Zealand perspective on palliative care for Māori
Muircroft, 2010
Māori, New Zealand Wairua (spiritual aspects) is the most important requirement of good health. Health relates to unseen and unspoken energies which connect with both the physical and spiritual environments
Family represent the main support for a dying Māori person Patients and family need help to ‘navigate’ the health system, to ensure
continuity of care and to be made aware of entitlements
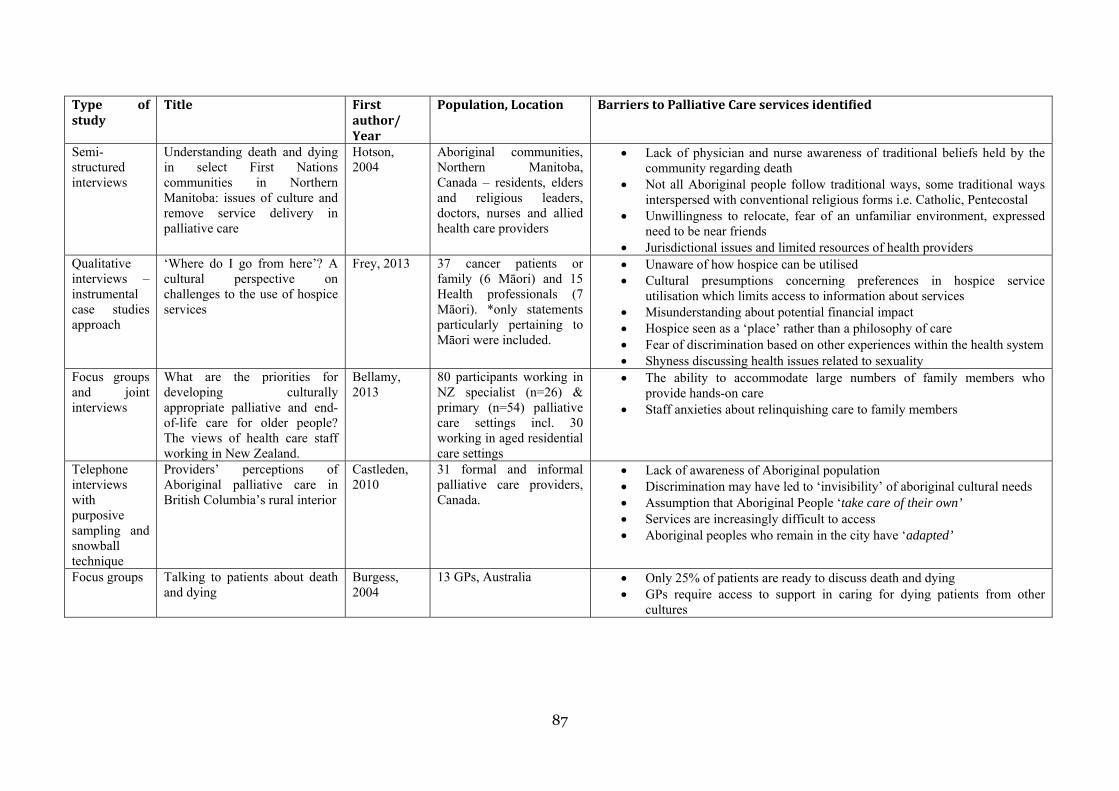
87
Type ofstudy
Title Firstauthor/Year
Population,Location BarrierstoPalliativeCareservicesidentified
Semi-structured interviews
Understanding death and dying in select First Nations communities in Northern Manitoba: issues of culture and remove service delivery in palliative care
Hotson, 2004
Aboriginal communities, Northern Manitoba, Canada – residents, elders and religious leaders, doctors, nurses and allied health care providers
Lack of physician and nurse awareness of traditional beliefs held by the community regarding death
Not all Aboriginal people follow traditional ways, some traditional ways interspersed with conventional religious forms i.e. Catholic, Pentecostal
Unwillingness to relocate, fear of an unfamiliar environment, expressed need to be near friends
Jurisdictional issues and limited resources of health providers Qualitative interviews – instrumental case studies approach
‘Where do I go from here’? A cultural perspective on challenges to the use of hospice services
Frey, 2013 37 cancer patients or family (6 Māori) and 15 Health professionals (7 Māori). *only statements particularly pertaining to Māori were included.
Unaware of how hospice can be utilised Cultural presumptions concerning preferences in hospice service
utilisation which limits access to information about services Misunderstanding about potential financial impact Hospice seen as a ‘place’ rather than a philosophy of care Fear of discrimination based on other experiences within the health system Shyness discussing health issues related to sexuality
Focus groups and joint interviews
What are the priorities for developing culturally appropriate palliative and end-of-life care for older people? The views of health care staff working in New Zealand.
Bellamy, 2013
80 participants working in NZ specialist (n=26) & primary (n=54) palliative care settings incl. 30 working in aged residential care settings
The ability to accommodate large numbers of family members who provide hands-on care
Staff anxieties about relinquishing care to family members
Telephone interviews with purposive sampling and snowball technique
Providers’ perceptions of Aboriginal palliative care in British Columbia’s rural interior
Castleden, 2010
31 formal and informal palliative care providers, Canada.
Lack of awareness of Aboriginal population Discrimination may have led to ‘invisibility’ of aboriginal cultural needs Assumption that Aboriginal People ‘take care of their own’ Services are increasingly difficult to access Aboriginal peoples who remain in the city have ‘adapted’
Focus groups Talking to patients about death and dying
Burgess, 2004
13 GPs, Australia Only 25% of patients are ready to discuss death and dying GPs require access to support in caring for dying patients from other
cultures
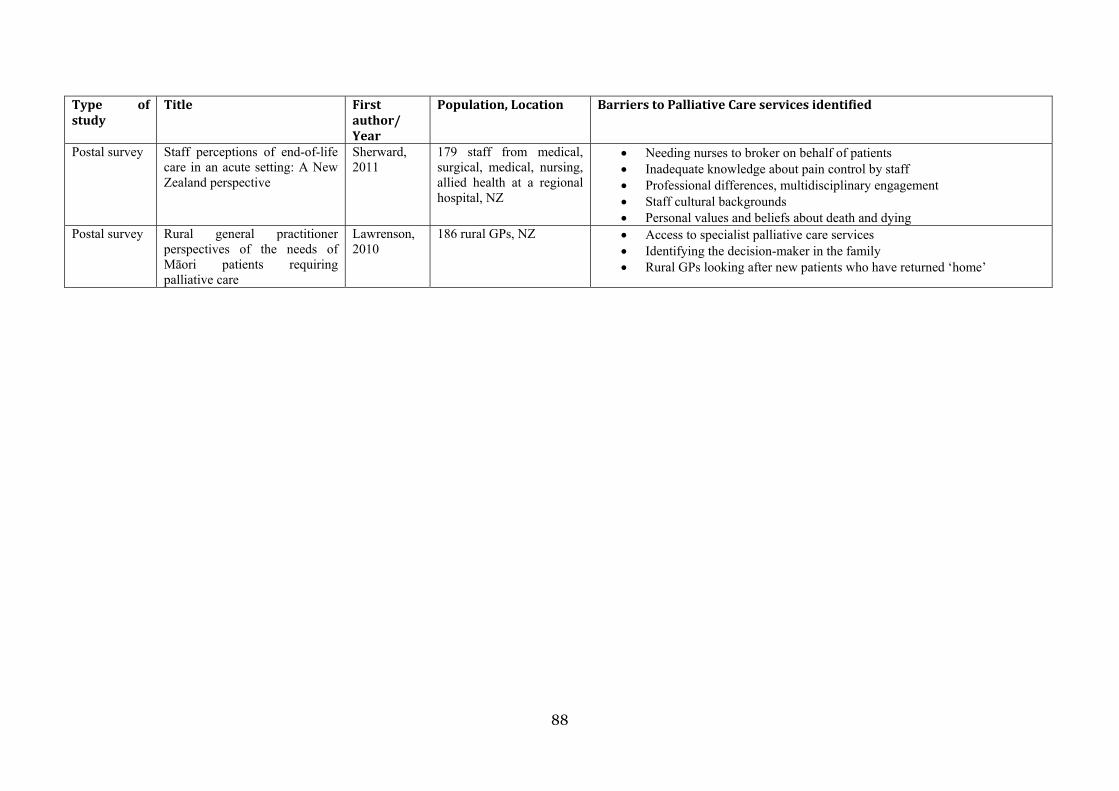
88
Type ofstudy
Title Firstauthor/Year
Population,Location BarrierstoPalliativeCareservicesidentified
Postal survey Staff perceptions of end-of-life care in an acute setting: A New Zealand perspective
Sherward, 2011
179 staff from medical, surgical, medical, nursing, allied health at a regional hospital, NZ
Needing nurses to broker on behalf of patients Inadequate knowledge about pain control by staff Professional differences, multidisciplinary engagement Staff cultural backgrounds Personal values and beliefs about death and dying
Postal survey Rural general practitioner perspectives of the needs of Māori patients requiring palliative care
Lawrenson, 2010
186 rural GPs, NZ Access to specialist palliative care services Identifying the decision-maker in the family Rural GPs looking after new patients who have returned ‘home’
2. Explorehowhealthliteracyprinciplesareincorporatedwithmaterials(writtenresourcessuchaspamphlets,internet,videosetc)inpalliativecare
This search strategy utilised the combination of #1 (Palliative care) and #3 (HealthLiteracy)
Searchstrategy No.ofarticlesSCOPUS#1AND#3 39Fulltextretrieved 9
Atotalof39articleswereidentifiedusingacombinationofthesearchterms,palliativecareand health literacy. On examination of titles, abstracts and keywords, only nine articlesfittedthecriteriaconcerningmaterialsinpalliativecarewhichrelatedtohealthliteracy.Ofthese, six articles were suitable for inclusion. The removed articles related to advancedcaredirectives(MelhadoandBushy2011),culturaldeficitsbasedonagroupofpeoplewithasensorydisability(asaculturalidentification)(Maddalenaetal2012)andoneusingthesamecohortandinformationasanalreadydescribedarticle(Volandesetal2010).
Researchers argued that education could be conceptualised as a fundamental healthprofessional intervention in providing information that was both empowering andculturally sensitive for those in hospice and other end‐of‐life care settings (Cagle andKovacs2009).Therewereseveraleducationalcomplexitiesthatimpactedontheabilitytoeffectivelyhelppatientsandfamiliestoaccesstheinformationtheyneeded.Healthliteracydrewonprinciplesofadulteducationandrequirededucatorstodrawonthepatient'spriorknowledgeandexperience(Nutbeam2008).
Health professionals are seen as relying heavily on spoken and written forms ofcommunication(Workbase2013);however,theuseofplainlanguageinreplacingmedicaljargonwasnotseenin itselfassufficienttoguaranteereadabilityhadbeenachievedandhealthmessageshadbeenunderstood(MinistryofHealth2012).Inaddition,itwasarguedthat caregivers themselvesmayhaveco‐morbidities thatmayreduce their literacy levels(Kehl andMcCarty 2012) impacting on their ability to advocate for patients. AUS studyexaminedwrittendocumentsusedby170hospicestopreparefamiliesforcaregivingatthetimeofdeath lookingat the languagesof thematerials,whatmaterialswereofferedandhowmaterialsweredistributedand reviewed (KehlandMcCarty2012).Resourceswereanalysed for readability using three health literacy tools, the Flesch‐Kincaid ReadabilityFormula(F‐K),theSimpleMeasureofGobbledygook(SMOG),andtheColorsLabelEaseforAdultReadersInstrument(CLEAR).Hospicesprovidedfromonetosevendocumentsfromproviders forreview.Fewdocumentswerereportedasmeeting therecommendedgradelevel for adequate comprehension. The number of medical terms ranged from 0 to 20.

90
Overallitwasfoundthatthemainreasonforpoorratingsonliteracytestswastheuseofmedicalterminologywithoutadequateandeffectiveexplanations.Implicationsforpracticeincluded: highlighting medical terms coupled with the use of direct explanations,improving document design through the use of bullet points, appropriate use ofillustrationsandappropriatelylargefontsize.
Other articles referred to types and presentation of information. The format in whichinformation is provided may have an effect on how it is received, processed and actedupon. A US study of parents who had children with life‐threatening illnesses comparedwhether they weremore likely to use the internet as a primary information source forhealthqueriescomparedwithusingthedoctorasaprimaryinformationsource,basedontheir self‐identified internet usage. It found that greater internet use was positivelyassociated with an increase in e‐health literacy (Knapp et al 2011). Despite parents ofHispanicoriginhavinglesseraccesstotheinternetingeneral,forthosethatdidaccesstheinternet, usingmultivariate analysis, the researchers identified that e‐health literacy didnotdiffer byethnicity.Theuseof visual content in e‐health literacywas seenashelpingparentstounderstandthe informationprovidedonthe internet.Eventhoseparentswhowerenotabletodecipherthecontentwerepromptedtofollowupwhattheyfoundontheinternetwith thedoctor, thus leading tonewdialoguebetweenparents and their healthprofessional.A furthersearchwouldbe required tounderstand theconsequencesof thisforpatientsandhealthprofessionals.
Aninterventionaltrialassessinghealthliteracyandend‐of‐lifepreferencesbetweengroupsin a rural community compared verbal information about dementia against having theverbalinformationplusavideodecisionaid(Volandesetal2011).Thegroupthatreceivedthevideodecision‐makingaidalongsidetheverbalinformationweremorelikelytoprefercomfort care compared with the verbal information alone (91% c.f. 72%). Those withhigher health literacy also had a greater propensity towards comfort care. In an earlierstudybythesameauthorwhichaddressedhealthliteracyasavariableindecisionmaking,itwas found that thosewith low ormarginal health literacyweremore likely to preferaggressive care than comfort care after verbal description, but afterwatching the videodecision‐makingaidtherewerenosignificantdifferencesinthedistributionofpreferencesbyraceorhealthliteracy(Volandesetal2008).
An internet survey exploring nurses’ attitudes to and use of an online palliative careresourcewas conductedwith staffworking in specialist palliative care services (TiemanandRawlings2008).Whilethecontentwasfoundtobecredible,specialistpalliativecarenursesweremoreawareoftheresourcethanothernurses.
91
A systematic review that focused on single or multiple literacy‐directed interventions(Sheridan et al 2011) reported that presenting only essential information improvedcomprehension in individualswith lownumeracycomparedwithprovidingessentialandnon‐essential information. However, when quality information was presented that putessentialinformationfirst,comprehensionwasimprovedforthosewithlownumeracy.
Itisknownthatthereishighcorrelationbetweenmeasuresofhealthliteracy,printliteracyandnumeracy(Berkmanetal2011).Studiesusingintensiveself‐managementinterventiontoimproveheartfailureoutcomesfailedtoimprovequalityoflifescoresorhealthliteracyscores.Inpalliativecare,self‐managementrecognisesstagesofillnessandinformspatientsand families ofwhere symptomcontrol ormore intense intervention is required. In thisreview,theyfoundfewstudiesthatstratifiedanalysisbyhealthliteracylevels.Nonewereethnicityspecificandnonerelatedtopalliativecare.
Insummary, inaddressinghowhealthliteracyis incorporatedintomaterials inpalliativecare, althoughonly part of the overall health literacy context,materialsweredeemed torate poorly due to the overuse of medical terminology. However, while using directexplanationsandothercuessuchasbulletpointsandboldletteringwasarguedaspossiblymakingthedesignmorereadable,itwasacknowledgedthatfocusingonreadabilityaloneby replacing medical jargon with plain language was not sufficient in improving healthliteracy.Otherliteraturereferredtotheuseofadditionalformsofmediasuchasvideoorinternet use. Videos hadpotential in their capacity tobe viewedagain at a laterdate orsharedamongstfamilytoalsoview.Internetuseisincreasinginyoungerpopulationsandanecdotallytheyoungergenerationareadvocatingmoreforolderpeoplewheretheolderpersonmaybereluctanttocomplain/comment(MParsons,personalcommunication,April2013). Therefore, while an older personmay not be au fait with internet technology, ayoungerrelativemaybeable tosupport them.Dependingonhealth literacy levels,usinginternetsearchenginesmayprovideuserswith theanswersto theirquestionsorenablerefinementoftheirquestions.
3. Examinehealth literacy interventions inpalliative care forMāoriandtheirwhānau
Usinga combinationof#1 (Palliative care),#2 (IndigenousPopulations) and#3 (HealthLiteracy), this search strategy provided one article in Scopus which considered thechallengesofethnogeriatricsintheUS(Yeo2009).SeveraladditionalarticlesappearedtomeetthecriteriawhichwerenotfoundusingtheScopussearch,aswellasnon‐publishedliterature (book, reports). Itwas important tokeep the focuson thehealthoutcomes forMāoriandthereforethisfinalstrategymovestoanarrativesynthesistogarneracompletepictureoftheinterventionsidentifiedthatresearchindicatedmightsupportbetterserviceoutcomes for tāngatamāuiui and theirwhānau. Furthermore, theassetmodel (Nutbeam
92
2008)wasthelensinwhichthisreviewwassited.Theassetmodeluseshealtheducationasaleverwithwhichpersonalempowermentindecisionmakingcanoccur.
Beginning with the one identified article, the authors cited several challenges to high‐quality ethnogeriatric care which included disparities in health status and health care,differencesofacculturationlevelandothercharacteristicswithinthepopulations,languageand limited English proficiency, health literacy, culturally defined health beliefs andsyndromes,andspecificbeliefsandpreferencesaboutlong‐termandend‐of‐lifecare(Yeo2009). While this article did not focus solely on indigenous populations, therecommendations for ethnically diverse populations appeared to correspond with thebarrierstopalliativecareservicesidentifiedinthefirstsectionofthisreview.
An Australian study examined individual, social and cultural aspects of health literacyrelevant to cancer among Aboriginal patients, carers and their health workers in NewSouth Wales (Treloar et al 2013). It was recognised that differing views of health andillness in indigenous populations were not aligned with western biomedical models(Hampton et al 2010). This qualitative study identified the silence of cancer in whichAboriginalpeopledidnotbelievetheywouldgetcancerduetoitsportrayal inthemediawheretherewasanabsenceofAboriginalpeopleinpubliccampaigns;hencethecampaignlacked meaning to indigenous people. In addition, priorities were discussed in whichcancermay take a back seat to other health issues. Recommendations to address theseaspects of health literacy included facilitated communitymembers’ awareness of cancerandforcancereducationprogrammesatanumberoflevels.
A systematic review of interventions to mitigate the effects of low health literacy wasperformedaddressingthreefactors: improvinghealth literacy forpatientsandproviders,improving utilisation of appropriate services and improving health outcomes comparedwithusualcare(Basuetal2010).Foursystematicreviewsand30primarystudies,thathadnotbeenincludedinanyofthepreviously identifiedsystematicreviews,metthecriteria.Twenty‐two out of the 30 studies were randomised controlled trials. Five generalprinciples for organising health literacy related interventions were identified ascontributingtosuccessfuloutcomes,howevertwooftheseprinciples(visualmaterialsandreadabilitylevels,andmulti‐componentandmulti‐media)overlappedwithoneoftheotherthreethemes.Therefore,thethreemainprinciplesincluded:complexinterventions(thosethatengagedintwoormodalitiessuchascombinationsofface‐to‐faceinteractions,useofmultimedia or videotape instruction and the use of textual data); interventions thatrecognisedpeoples’differentlearningstyles(recognisingthatpeopleprocessinformationindifferentways, and therefore including text‐basedmaterials, soundbytes, visualisation(pictorials), debates and verbal exchanges of ideas); and interventions that werepersonalisedandtailoredtospecificindividualsorgroupsandwereoutcomesfocused.One
93
keyideawasforhealthprofessionalsandothercaregiverstocheckforunderstandingbyensuring that ‘message sent = the message received’. The teach‐back method, wherepatients and families can restate in their own words what has been told, was onerecommended way to ensure the message was understood and remembered, and forpractical training, a dummy run was another technique to check for understanding(KripalaniandWeiss2006).
A rapid evidence review of interventions for improving health literacy relating tocommunicable diseases found that a diversity in the range of outcomes limited theconclusions inmost studies (D’Eath et al 2012).More importantly, the authors reportedlittleevidenceofspecificinclusionofdisadvantagedorhard‐to‐reachgroups.Noneofthestudies focused on palliative care and there was a lack of research which consideredinterventionsbasedonethnicity,cultureorage.Asthisreportwasareviewofreviews,itsqualitywas constrained by the quality of reviews.Most literature onhealth literacy andpatient adherence does not seek to investigate culture or ethnicity as variables, despitecommonlyobservedoutcomesthatlowhealthliteracyismoreprevalentinethnicminority,low‐incomeandelderlypopulations(Shawetal2009).
An updated systematic review of health literacy interventions and outcomes that wasconducted in theUS allowed for increased recognitionof numeracy in relation to healthliteracy,andoforalskillsofparticipants,aswellasknowledge,asoutcomes(Berkmanetal2011). Variables on the causal pathway between health literacy and health outcomesincludedknowledge,self‐efficacyandsocialstigma.Inthisupdatedreview,itwasidentifiedthathealthliteracycouldbeamediatorofracialdisparitiesinhealthoutcomes.Despiteaplethora of health literacy literature emerging in the past decade, this area remainsemergent in New Zealand. Small sample sizeswere reported asmaking it impossible todeterminetrueeffectandinconsistentapproachestocreatinghealthliteracyandnumeracylevelsorthresholdsinanalysishamperedcomparisons.
Asystematicreviewwhichreviewedinterventionsforindividualswithlowhealthliteracyrecognised several discrete design features that improved patient comprehension(Sheridanetal2011).Theauthorsconcludedthatintensiveself‐managementinterventionsreducedemergencydepartmentvisitsandhospitalisations,andintensiveself‐anddisease‐management interventions reduced disease severity. They also reported that multipleinterventionsshowedpromiseformitigatingtheeffectsoflowhealthliteracy.
Aframeworkhasbeenproposedbasedonbest‐practiceprinciplesforimprovingcarewithpatientswith limitedhealth literacy(Sudoreetal2009).Within it, limitedhealth literacywasdescribedasafunctionofthedemandsandexpectationsplacedonthepatientbythehealth care system, as well as by the patient’s disease processes. Three main areas of
94
intervention were identified: Clinical‐Patient Level Interventions, focusing oncommunication, presentation, reinforcement, reconciliation and confirmation ofunderstanding; System‐Patient Level Interventions, around materials, labelling, diseasemanagement programmes, empowering environments and clinical communicationtraining; and Community‐Patient Level Interventions, including adult education andliteracyprogrammes,useoflayhealtheducatorsandhealthnavigatorsandharnessingthemedia. This comprehensive framework cited limitations in the use of some of theseinterventions as not having been tested in limited health literacy populations. Strategiessuchastheuseofcomputerkioskswithtouchscreenshavebeenreportedasbeingusedmoreinlargehealthcareorganisationsandhavebeenshowntobeusefulandacceptableinwell‐educatedpopulations;howevertheiruseinlimitedhealthliteracypopulationshasnotbeen tested. Themessagewas not a ‘one‐size fits all’ approach as other factors such aslanguage barriers, the use of interpreters, learning disabilities and dementia sufferersfurther inhibited health literacy. The key is for further research to examine how client‐patient communication can increase health literacy thereby reducing health disparities(SudoreandSchillinger2009).
A list of ten attributes of health literate health care organisationswere identified by theInstituteofMedicine(Nielsen‐Bohlmanetal2004).Iforganisationshavetheseattributesitisarguedthatitwillmakeiteasierfortheorganisations’patientstonavigate,understandanduseinformationandservicestotakecareoftheirhealth(Brachetal2012).Thereisagrowingappreciationthathealthliteracydoesnotfocussolelyonindividualskill(Nielsen‐Bohlmanetal2004).Accordingtoresearchthusfar,theinterventionswhichorganisationsneedtoensuretheyhavetogaintheattributesofahealth literateorganisation included:havingleadershiptoallowhealthliteracytobeintegraltoitscorevalues;integrateshealthliteracy into planning, evaluation, patients safety and quality improvement; workforcepreparedness;allowsandintegratespopulationinput;meetstheneedsofthepopulation;useshealthliteracystrategiesincommunicationandconfirmation;provideseasyaccesstonavigate health information and services; utilises easy to understand design anddistributionofmaterials;prioridentificationofhighrisksituationsforhealthliteracy;and,communicatesclearlyaboutcosts(Brachetal2012).
Despitetheintentiontoviewhealthliteracyinterventionsthroughalensofanassetmodel,noarticlesmeasuredinformationflowthroughatwo‐wayprocess(EuropeanHealthPolicyForum 2005). There was a lack of interventions measuring the way in which healthinformationwasdeliveredapartfromtheusabilityofmaterialsprovided.Strategiesweremeasuredbasedonreadabilityornumeracyoronhealthliteracylevelsinindividuals.Theconveyingofhealthmessagesrequiresskillonthepartofthehealthprofessional.Itislikely

95
thatmoreworkneedstooccurinassessingthedeliveryofinterventionsnotonlyintermsofproductsandtime.
Indrawingonthefindingsofthisreview,itwasevidentthatthedomainofhealthliteracyisstill in its infancy inNewZealand. The understanding of how to improve health literacyfromahealthservicesperspectivehasbeenidentifiedinpracticalstepsforimprovement.Further studies are required to engage health professionals and health organisations indevelopingskillstobuildhealthliteracy(basedonadultlearningprinciples)andassessingtheoutcomesoftheseeffortstobuildhealthliteracy.
96
Appendix Two: List of resources analysed
AguideforcarersbookletA5(2ndEdition)
HospiceNewZealand
Aboutus...pamphletDLE
HospiceNorthShore
www.hospicenorthshore.org.nz/site/nshospice/files//ABOUT%20US%20Pamphlet%20FINAL%20PRINT.pdf
InformationpamphletDLE
NorthShoreHospiceTrust
Information&CareCommunicationBookA5
NorthShoreHospiceTrust
FamilySupportInformationPamphlet
NorthShoreHospiceTrust
KaitakawaengaKaiawhinapamphletDLE
NorthShoreHospiceTrust
YourintroductiontoPatientandFamilyServicesbookletA5
HibiscusHospice
HospiceCarespamphletDLE
HibiscusHospice
www.hibiscushospice.org.nz/site/hibiscushospice/files/Hospice%20Cares%20(2).pdf
WelcometoHospiceWestAucklandletterA4
HospiceWestAuckland
97
InformationforPatientsandFamiliespamphletDLE
HospiceWestAuckland
Anappreciationofhospicecare:howyoucanhelppamphletDLE
MercyHospiceAuckland
OtherpamphletDLEsfromMercyHospiceAucklandinclude:
Educationforfamiliesascarers2012
Openingdoors
PreventionofPressureInjuriesintheHome
Endoflifechanges(athome):Adviceforfamilymembers,friendsandcarersofpatientswhoaredyingathome
Morphine–informationforfirsttimeusers
Givethegiftofsight:EyeDonationforTransplantationpamphletDLE
TheNewZealandNationalEyeBank,DepartmentofOphthalmology,SchoolofMedicine,UniversityofAuckland
MoWaiTeOra:Māori HealthServicespamphletDLE
MoWaiTeOra:MāoriHealthServices,WaitemataDistrictHealthBoard
www.healthpoint.co.nz/specialists/other/waitemata‐dhb‐Māori‐health‐services‐mo‐wai/important‐information/
MoWaiTeOra:MāoriHealthServicesPatientSatisfactionSurveyleafletA5oronline
MoWaiTeOra:MāoriHealthServices,WaitemataDistrictHealthBoard
www.surveymonkey.com/s/Mo_Wai_Te_Ora_Patient_Satisfaction_Survey
KaitiakiNursingservice: WhatweofferpamphletDLE
KaitiakiNursingservice,WesternBayofPlentyPHO
98
Whānau OraNavigationCancerCareService,comprisedof:
a. CommunityHealthNavigatorBackgroundbooklet
b. PatientandWhānauCommunicationJournal
WaitemataDistrictHealthBoardandTeWhānauoWaipareiraTrust
HowtoClaimCarerSupportpamphletDLE
MinistryofHealth
www.health.govt.nz/yourhealth‐topics/disability‐services/respite‐and‐carer‐support/carer‐support
CodeofHealthandDisabilityServices:Consumers’Rightspamphlet+booklet
Health&DisabilityCommissioner
www.hdc.org.nz/media/24833/leaflet%20code%20of%20rights.pdf
ThereisalsoaneasyreadbookletfoundontheHDCwebsitehere:www.hdc.org.nz/media/52437/you%20have%20rights%20‐%20easy%20read%20version.pdf
Makingthemostofyourfinalyears:PracticalandspiritualthingstothinkaboutandplanforendoflifepamphletDLE
AdvanceCarePlanningCooperative(ACP)
www.advancecareplanning.org.nz/Portals/0/Documents/Making%20the%20most%20of%20your%20final%20years%20leaflet.pdf
FormsintheHospiceNorthShoreInformationPack
NorthShoreHospiceTrust
WelcometotheCommunityPalliativeCareServiceofMercyHospiceAuckland
MercyHospiceAuckland
Becausegriefhappensandsupportmatters:Supporttohelpchildren,youngpeopleandadultspickupthepieces
Skylight
99
FamilySupportTeam
MercyHospiceAuckland
CloudWorkshop:Artworkshopsforbereavedchildrenandthosewithlifethreateningillnessintheirfamily
SponsoredbyMercyHospiceAuckland
Supportingchildrenandyoungpeoplethroughlossandgrief:aguideforparentsandcaregivers
MercyHospiceAuckland
Listofspeciallychosenbooksforchildrenwithgriefintheirlives
TheWomen’sBookshop
AgreementforCareletterA4
MercyHospiceAuckland
BeingHonestwithyourChildrenpamphletDLE
WaipunaHospice
CaregiverEducationProgrammeinformationsheetA4
WaipunaHospice
Complaints/FeedbackleafletA5
WaipunaHospice
FamilySupportServicespamphletDLE
WaipunaHospice
100
LoanEquipmentinformationsheet2xA4
WaipunaHospice
MethadonepamphletDLE
WaipunaHospice
PatientCommunicationBooknotebook
WaipunaHospice
PlanningforaFuneralpamphletDLE
WaipunaHospice
UnderstandingwhatishappeningpamphletDLE
WaipunaHospice
WaipunaHospiceServicespamphletDLE
WaipunaHospice
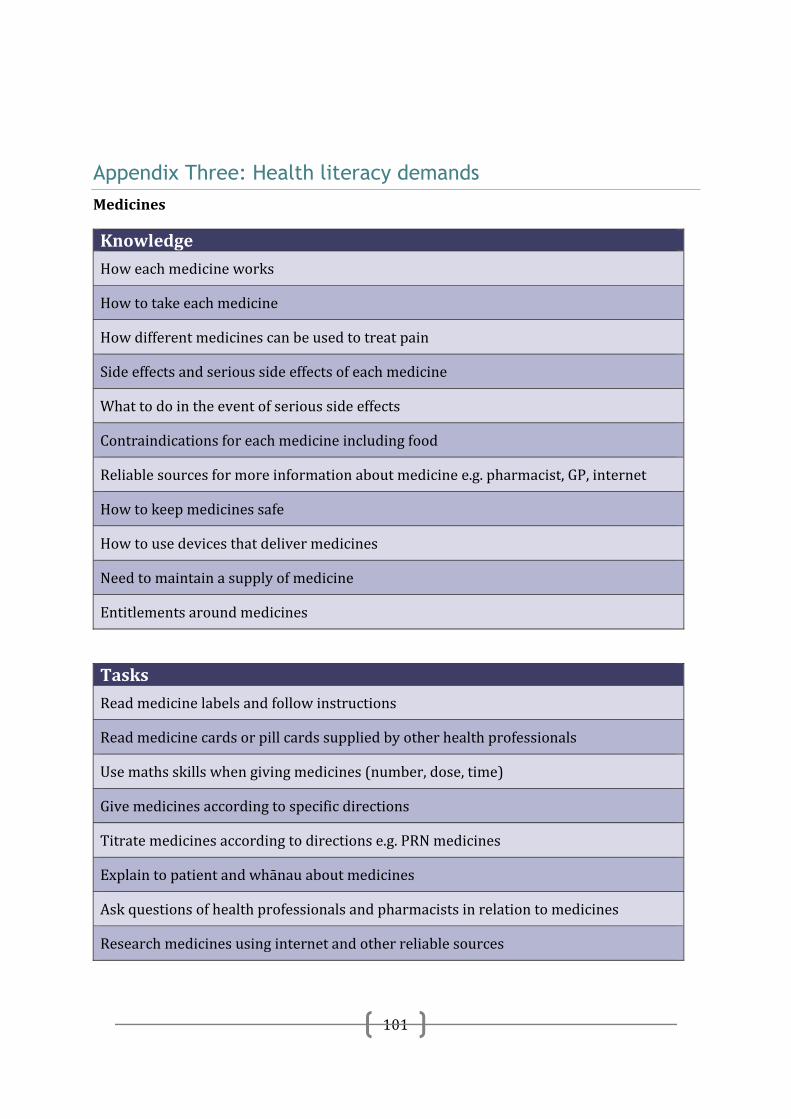
101
Appendix Three: Health literacy demands Medicines
Knowledge
Howeachmedicineworks
Howtotakeeachmedicine
Howdifferentmedicinescanbeusedtotreatpain
Sideeffectsandserioussideeffectsofeachmedicine
Whattodointheeventofserioussideeffects
Contraindicationsforeachmedicineincludingfood
Reliablesourcesformoreinformationaboutmedicinee.g.pharmacist,GP,internet
Howtokeepmedicinessafe
Howtousedevicesthatdelivermedicines
Needtomaintainasupplyofmedicine
Entitlementsaroundmedicines
Tasks
Readmedicinelabelsandfollowinstructions
Readmedicinecardsorpillcardssuppliedbyotherhealthprofessionals
Usemathsskillswhengivingmedicines(number,dose,time)
Givemedicinesaccordingtospecificdirections
Titratemedicinesaccordingtodirectionse.g.PRNmedicines
Explaintopatientandwhānauaboutmedicines
Askquestionsofhealthprofessionalsandpharmacistsinrelationtomedicines
Researchmedicinesusinginternetandotherreliablesources
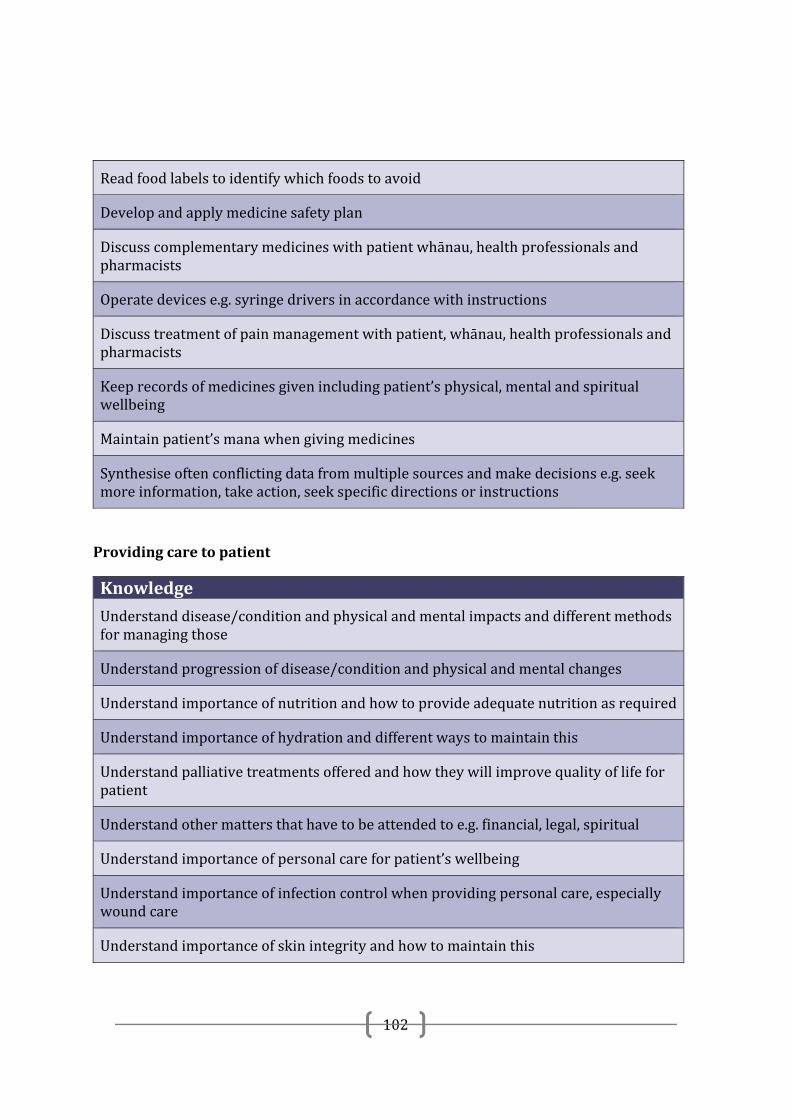
102
Readfoodlabelstoidentifywhichfoodstoavoid
Developandapplymedicinesafetyplan
Discusscomplementarymedicineswithpatientwhānau,healthprofessionalsandpharmacists
Operatedevicese.g.syringedriversinaccordancewithinstructions
Discusstreatmentofpainmanagementwithpatient,whānau,healthprofessionalsandpharmacists
Keeprecordsofmedicinesgivenincludingpatient’sphysical,mentalandspiritualwellbeing
Maintainpatient’smanawhengivingmedicines
Synthesiseoftenconflictingdatafrommultiplesourcesandmakedecisionse.g.seekmoreinformation,takeaction,seekspecificdirectionsorinstructions
Providingcaretopatient
Knowledge
Understanddisease/conditionandphysicalandmentalimpactsanddifferentmethodsformanagingthose
Understandprogressionofdisease/conditionandphysicalandmentalchanges
Understandimportanceofnutritionandhowtoprovideadequatenutritionasrequired
Understandimportanceofhydrationanddifferentwaystomaintainthis
Understandpalliativetreatmentsofferedandhowtheywillimprovequalityoflifeforpatient
Understandothermattersthathavetobeattendedtoe.g.financial,legal,spiritual
Understandimportanceofpersonalcareforpatient’swellbeing
Understandimportanceofinfectioncontrolwhenprovidingpersonalcare,especiallywoundcare
Understandimportanceofskinintegrityandhowtomaintainthis
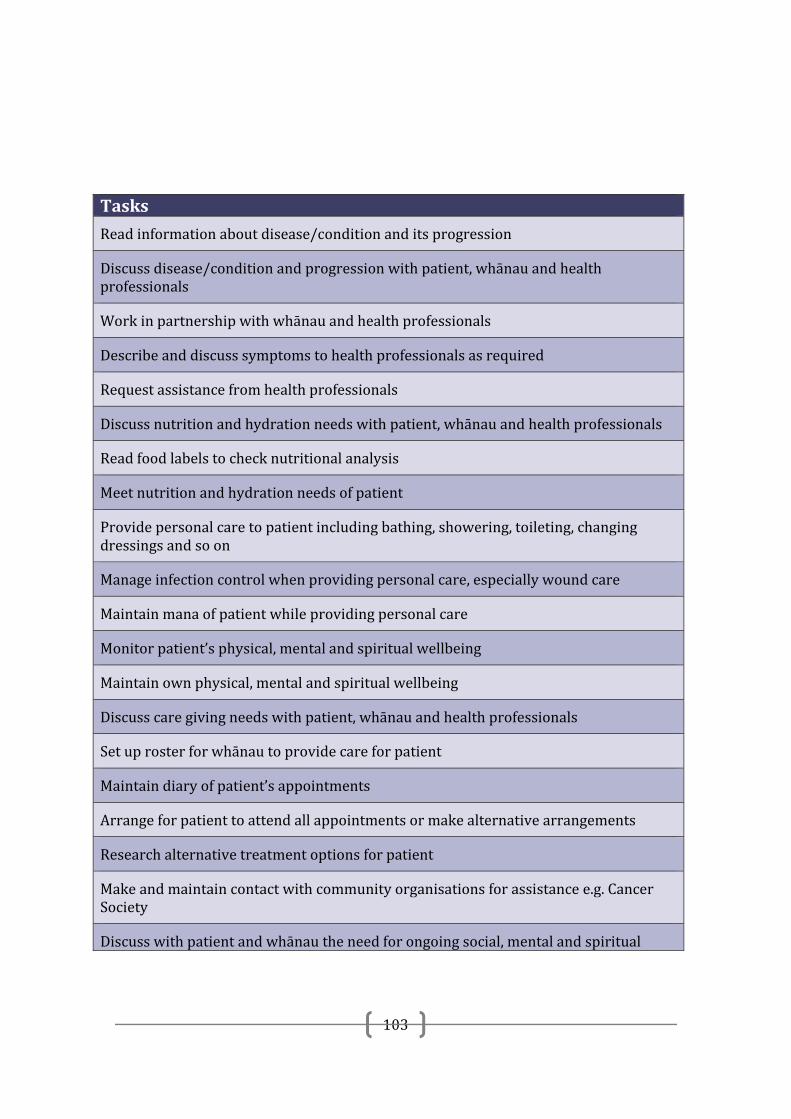
103
Tasks
Readinformationaboutdisease/conditionanditsprogression
Discussdisease/conditionandprogressionwithpatient,whānauandhealthprofessionals
Workinpartnershipwithwhānauandhealthprofessionals
Describeanddiscusssymptomstohealthprofessionalsasrequired
Requestassistancefromhealthprofessionals
Discussnutritionandhydrationneedswithpatient,whānauandhealthprofessionals
Readfoodlabelstochecknutritionalanalysis
Meetnutritionandhydrationneedsofpatient
Providepersonalcaretopatientincludingbathing,showering,toileting,changingdressingsandsoon
Manageinfectioncontrolwhenprovidingpersonalcare,especiallywoundcare
Maintainmanaofpatientwhileprovidingpersonalcare
Monitorpatient’sphysical,mentalandspiritualwellbeing
Maintainownphysical,mentalandspiritualwellbeing
Discusscaregivingneedswithpatient,whānauandhealthprofessionals
Setuprosterforwhānautoprovidecareforpatient
Maintaindiaryofpatient’sappointments
Arrangeforpatienttoattendallappointmentsormakealternativearrangements
Researchalternativetreatmentoptionsforpatient
Makeandmaintaincontactwithcommunityorganisationsforassistancee.g.CancerSociety
Discusswithpatientandwhānautheneedforongoingsocial,mentalandspiritual
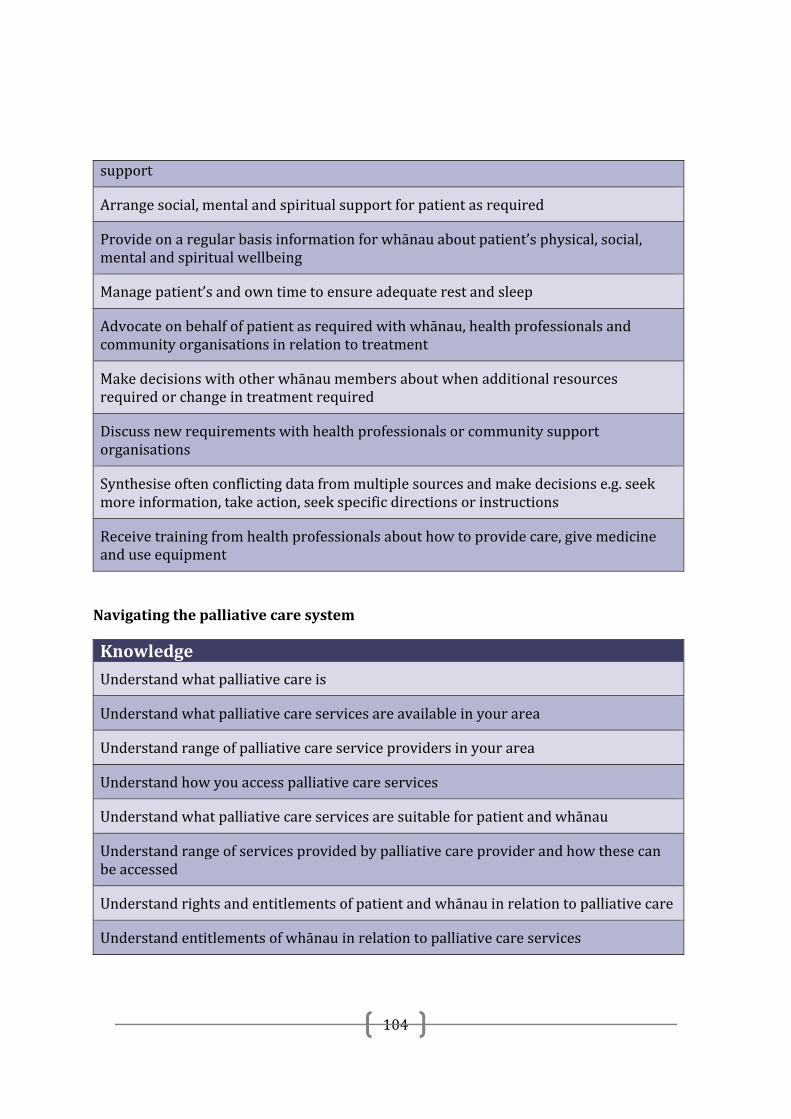
104
support
Arrangesocial,mentalandspiritualsupportforpatientasrequired
Provideonaregularbasisinformationforwhānauaboutpatient’sphysical,social,mentalandspiritualwellbeing
Managepatient’sandowntimetoensureadequaterestandsleep
Advocateonbehalfofpatientasrequiredwithwhānau,healthprofessionalsandcommunityorganisationsinrelationtotreatment
Makedecisionswithotherwhānaumembersaboutwhenadditionalresourcesrequiredorchangeintreatmentrequired
Discussnewrequirementswithhealthprofessionalsorcommunitysupportorganisations
Synthesiseoftenconflictingdatafrommultiplesourcesandmakedecisionse.g.seekmoreinformation,takeaction,seekspecificdirectionsorinstructions
Receivetrainingfromhealthprofessionalsabouthowtoprovidecare,givemedicineanduseequipment
Navigatingthepalliativecaresystem
Knowledge
Understandwhatpalliativecareis
Understandwhatpalliativecareservicesareavailableinyourarea
Understandrangeofpalliativecareserviceprovidersinyourarea
Understandhowyouaccesspalliativecareservices
Understandwhatpalliativecareservicesaresuitableforpatientandwhānau
Understandrangeofservicesprovidedbypalliativecareproviderandhowthesecanbeaccessed
Understandrightsandentitlementsofpatientandwhānauinrelationtopalliativecare
Understandentitlementsofwhānauinrelationtopalliativecareservices
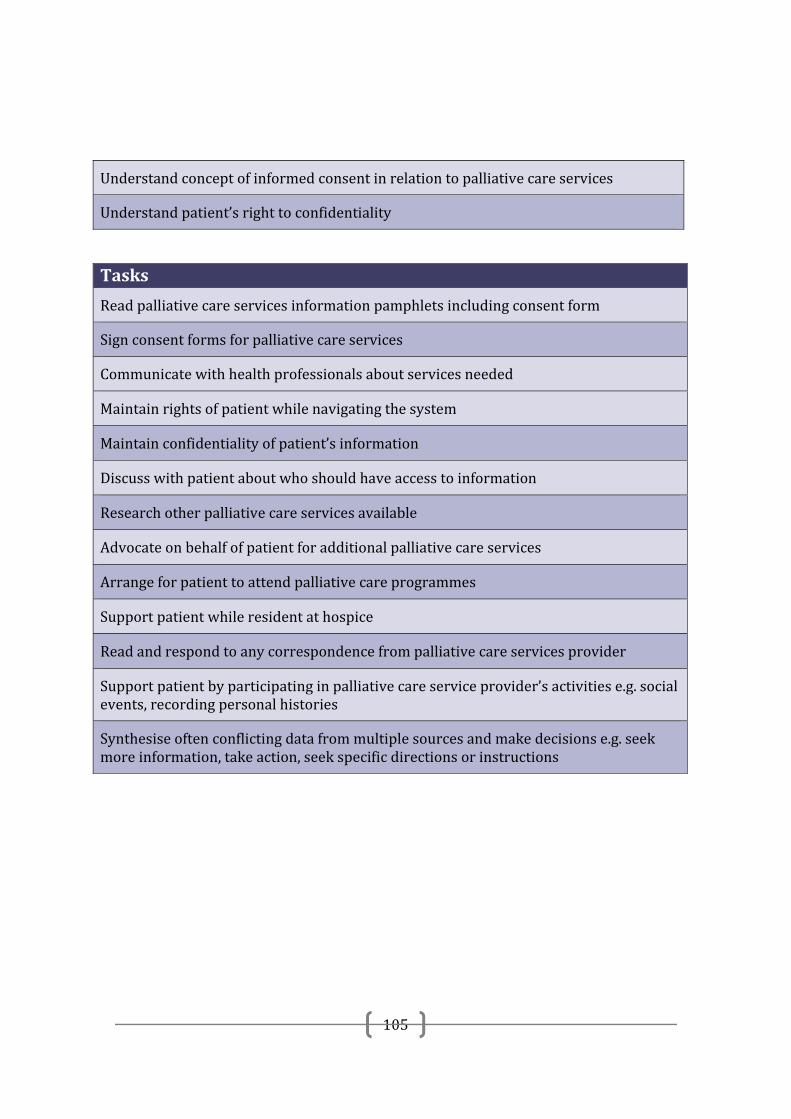
105
Understandconceptofinformedconsentinrelationtopalliativecareservices
Understandpatient’srighttoconfidentiality
Tasks
Readpalliativecareservicesinformationpamphletsincludingconsentform
Signconsentformsforpalliativecareservices
Communicatewithhealthprofessionalsaboutservicesneeded
Maintainrightsofpatientwhilenavigatingthesystem
Maintainconfidentialityofpatient’sinformation
Discusswithpatientaboutwhoshouldhaveaccesstoinformation
Researchotherpalliativecareservicesavailable
Advocateonbehalfofpatientforadditionalpalliativecareservices
Arrangeforpatienttoattendpalliativecareprogrammes
Supportpatientwhileresidentathospice
Readandrespondtoanycorrespondencefrompalliativecareservicesprovider
Supportpatientbyparticipatinginpalliativecareserviceprovider’sactivitiese.g.socialevents,recordingpersonalhistories
Synthesiseoftenconflictingdatafrommultiplesourcesandmakedecisionse.g.seekmoreinformation,takeaction,seekspecificdirectionsorinstructions
106
Appendix Four: Patient Whānau Information Letter, Consent Form & Interview Schedule
Kiaora
Weareaskingyoutotakepartinaresearchproject.
Whatistheprojectabout?Theprojectisaboutpalliativecarewhichiscaringforpeoplewhohaveillnessessuchascancerorheartdisease,andtheirwhānau,whentreatmentdoesn’tworkanymore.PartoftheresearchprojectisfindingoutaboutMāoripeople’sexperienceofpalliativecare.WealsowanttohearwhatMāoripatientsandwhānausayabout
o theinformationtheyneededtotakecareofthemselvesortheirwhānaumembero howhealthservicesandhealthworkerscommunicatedwithpatientsandwhānauo and if patients and whānau have suggestions about how services and
communicationbyhealthworkerscouldbeimproved.Whoisdoingtheresearch?MynameisDrJacquieKidd(Ngāpuhi).TheothermembersoftheresearchteamareDrPeterWoolford(Pākehā),MsSusanReid(TeRarawa),MrsNicolaCollins(Pākehā),MsStellaBlack(NgaiTūhoe),RawiriBlundell(NgātiPorou).
WhatdoIneedtodo?Weareaskingyoutotakepartinaninterview.Theinterviewwilltakeaboutonehour.Youcanbringotherwhānautotheinterview.Youcanchoosewheretheinterviewwilltakeplace–yourhomeoranotherplacethatyouchoose.Youcanalsochoosethedayandtimefortheinterviewwithyouandyourwhānau.Theinterviewwillbeundertakenbyoneormoreofthefollowingpeople:
RawiriBlundell StellaBlack SusanReid
Peter Rothwell Academic Centre Waikato Hospital Pembroke St Hamilton, New Zealand Telephone 64 7 839 8750 Facsimile 64 7 839 8712 Email: [email protected]
The University of Auckland Peter Rothwell Academic Centre Waikato Hospital Private Bag 3200 Hamilton New Zealand
107
WillIbepaidfortakingpart?Akohaofa$100voucherwillbemadeinrecognitionofthecontributionyouandyourwhānauhavemadetotheproject.Youwillnothavetopayanythingtotakepartintheproject.
Whyareyouaskingmetotakepart?Weareaskingyoutotakepartbecauseyouandyourwhānauareinvolvedwithpalliativecareatthemoment,oryourwhānauhavebeeninvolvedwithpalliativecareinthepast.TakingpartinthisprojectwillhelpustounderstandhowMāoripatientsandwhānauexperiencepalliativecareatthemoment,andhowpalliativecarecanbeimprovedforMāoripatientsandwhānau.
Theinformationfromtheprojectwillbeusedbypalliativecareservicesandhealthworkers,peopleinvolvedinplanningandfundingpalliativecareservices,andotherresearcherstoimprovepalliativecareservicesforMāoripatientsandwhānau.
Whatwillhappenintheinterview?Iwilltalkwithyouabout
o yourexperiencesofpalliativecare
o theinformationyouweregiven
o howhealthservicesandhealthworkerscommunicatedwithpatientsandwhānau
o and if you and your whānau have suggestions about how services andcommunicationbyhealthworkerscouldbeimproved.
Ifyouagreewewouldliketorecordtheinterview.Youdonothavetoagreetotherecording.
Whatwillhappenaftertheinterview?Iftheinterviewisrecordedwewillsendyoutypednotesofyourinterviewsoyoucanreadthem.Wewillinviteyoutoahuitotalkabouttheresultsofthestudy.Youdonothavetoreadthenotesorcometothehuiifyoudonotwantto.
DoIhavetotakepart?Youdon’thavetotakepartifyoudon’twantto.Ifyouchoosenottotakepartthiswillnotaffectanyfuturecareortreatment.Ifyoudotakepartyoucanstoptheinterviewatanytimeandyoudon’thavetoexplainwhy.Beforetheinterviewwewillexplaintheprojectagainandaskyouifyouagreetotakepart.Wewillaskyoutosignaformifyouagreetotakepart.
Howlongwilltheprojecttake?Theprojectwilltakeabout7monthstocomplete(endofMarch2013).Areportforthewholeresearchprojectwillbewritten.Youwillnotbeidentifiedinthisreport.Ifyouwouldliketogetacopyofthefullreportwewillsendyouone.Thefullreportwillbeavailableattheendof2013.
Howdoyoumakesuremyinformationiskeptprivate?Youwillnotbeidentifiedinthenotesfromtheintervieworinthereportabouttheproject.AftertheprojectisfinishedtheconsentformandinterviewnoteswillbestoredinalockedfilingcabinetoronasecurecomputerattheUniversityofAucklandfortenyearsandthenwillbedestroyed.
108
I(DrJacquieKidd)willbetheonlypersonwhocanaccessthenotesandcomputerfiles.Theconsentformwithyournameonwillbestoredinadifferentplacefromthenotes.
WhatifIneedmoreinformationabouttheproject?Ifyouhaveanyquestionsyoucangetmoreinformationaboutthestudyfromme.PleasefeelfreetocontactStellaBlack,ResearchAssistantifyouneedanymoreinformationorhaveanyquestionsaboutthisresearchproject.
MsStellaBlackPhone:021415441
Email:[email protected]
Ifyouhaveanyquestionsorconcernsaboutyourrightsasaparticipantinthisstudy,youmaywanttocontactanindependenthealthanddisabilityadvocate:
Freephone:0800555050
Freefax:08002SUPPORT(080027877678)
Email:[email protected]
ThisstudyhasreceivedethicalapprovalfromtheMulti‐regionEthicsCommittee,ethicsreferencenumberMEC/12/EXP/050,from13April2012until31March2013.
Nohooramai,raDr.JacquieKidd,RN,PhDSeniorLecturerSchoolOfNursingFacultyofMedicalandHealthSciences
109
ConsentForm(patientsandwhānau)
Study: Palliativecare,healthliteracy,Māoricommunitiesandhealthservices
Requestforinterpreter
English Iwishtohaveaninterpreter Yes No
Deaf IwishtohaveaNZsignlanguageinterpreter Yes No
Māori EhiahiaanaahaukitetahikaiwhakaMāori/kaiwhakapakehakorero Ae Kao
CookIslandMāori
Kainangaroauitetaitangataurireo Ae Kare
Fijian Augadrevameduaevakadewavosaveiau Io Sega
Niuean Fiamanakoaukefakaaogaetahatagatafakahokohokokupu E Nakai
Sāmoan Outemana’oiaiaisefa’amatalaupu Ioe Leai
Tokelaun KoauefofoukihetinokefakaliliutegaganaPeletaniakinagaganaonamotuotePahefika
Ioe Leai
Tongan Okuoufiema’uhafakatonulea Io Ikai
Otherlanguagestobeaddedfollowingconsultationwithrelevantcommunities.
Ihavereadandunderstoodtheinformationsheetdated2ndJuly2012forvolunteerstakingpartinthestudydesignedtounderstandhowMāoripatientsandwhānauexperiencepalliativecareatthemoment,andhowpalliativecarecanbeimprovedforMāoripatientsandwhānau.
Ihavehadtheopportunitytodiscussthisstudy.IamsatisfiedwiththeanswersIhavebeengiven.
Ihavehadtheopportunitytousewhānausupportorafriendtohelpmeaskquestionsandunderstandthestudy.
Peter Rothwell Academic Centre Waikato Hospital Pembroke St Hamilton, New Zealand Telephone 64 7 839 8750 Facsimile 64 7 839 8712 Email: [email protected]
The University of Auckland Peter Rothwell Academic Centre Waikato Hospital Private Bag 3200 H ilt
110
Iunderstandthattakingpartinthisstudyisvoluntary(mychoice),andthatImaywithdrawfromthestudyatanytime,andthiswillinnowayaffectmycontinuinghealthcare.
Iunderstandthatmyparticipationinthisstudyisconfidentialandthatnomaterialthatcouldidentifymewillbeusedinanyreportsonthisstudy.
Ihavehadtimetoconsiderwhethertotakepartinthestudy.
IknowwhotocontactifIhaveanyquestionsaboutthestudy.
Iconsenttomyinterviewbeingaudiotaped Yes No
Iwouldlikemyaudiotapesenttomeafterthenoteshavebeenprepared
Yes No
Iwishtoreceiveacopyoftheresults Yes No
ThisstudyhasreceivedethicalapprovalfromtheMulti‐regionEthicsCommittee,ethicsreferencenumberMEC/12/EXP/050,from13April2012until31March2013.
I__________________________________(fullname)herebyconsenttotakepartinthisstudy.
Date: Signature:
Fullnamesofresearchers: DrJacquieKiddMsSusanReidMrsNicolaCollinsMsStellaBlack
Contactphonenumberforresearchers:
DrJacquieKidd078398750MsSusanReid093613800MrsNicolaCollins0212422530MsStellaBlack021415441
Projectexplainedby:Projectrole: Signature:Date:Note:Acopyoftheconsentformistoberetainedbyeachparticipantand(inthecaseofpatients)acopyistobeplacedinthemedicalfile
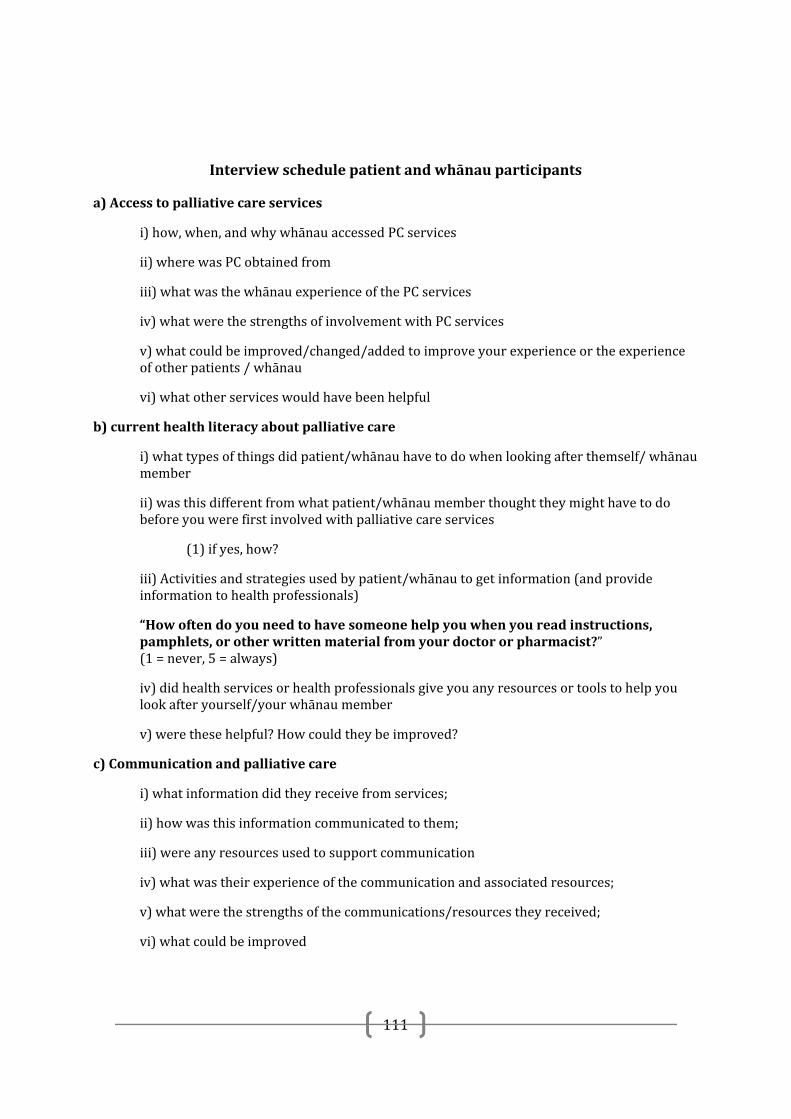
111
Interviewschedulepatientandwhānauparticipants
a)Accesstopalliativecareservices
i)how,when,andwhywhānauaccessedPCservices
ii)wherewasPCobtainedfrom
iii)whatwasthewhānauexperienceofthePCservices
iv)whatwerethestrengthsofinvolvementwithPCservices
v)whatcouldbeimproved/changed/addedtoimproveyourexperienceortheexperienceofotherpatients/whānau
vi)whatotherserviceswouldhavebeenhelpful
b)currenthealthliteracyaboutpalliativecare
i)whattypesofthingsdidpatient/whānauhavetodowhenlookingafterthemself/whānaumember
ii)wasthisdifferentfromwhatpatient/whānaumemberthoughttheymighthavetodobeforeyouwerefirstinvolvedwithpalliativecareservices
(1)ifyes,how?
iii)Activitiesandstrategiesusedbypatient/whānautogetinformation(andprovideinformationtohealthprofessionals)
“Howoftendoyouneedtohavesomeonehelpyouwhenyoureadinstructions,pamphlets,orotherwrittenmaterialfromyourdoctororpharmacist?”(1=never,5=always)
iv)didhealthservicesorhealthprofessionalsgiveyouanyresourcesortoolstohelpyoulookafteryourself/yourwhānaumember
v)werethesehelpful?Howcouldtheybeimproved?
c)Communicationandpalliativecare
i)whatinformationdidtheyreceivefromservices;
ii)howwasthisinformationcommunicatedtothem;
iii)wereanyresourcesusedtosupportcommunication
iv)whatwastheirexperienceofthecommunicationandassociatedresources;
v)whatwerethestrengthsofthecommunications/resourcestheyreceived;
vi)whatcouldbeimproved
112
Appendix Five: Health Professional Information Letter, Consent Form & Focus Group Interview Schedule, Key Informant Interview Schedule
Tenakoe
MynameisDrJacquieKidd.IamtheleaderofaresearchteamfundedbytheHealthResearchCouncilandMinistryofHealththatisundertakingaresearchprojectcalled‘Palliativecare,healthliteracy,Māoricommunitiesandhealthservices’.OthermembersoftheresearchteamareMrsNicolaCollins,MsSusanReidandMsStellaBlack.
Onepartoftheprojectinvolvesinterviewswithhealthprofessionalswhoprovidepalliativecareservices.WeareinterestedintheirperspectivesandunderstandingsaboutMāoriaccesstopalliativecareservices.Wearealsointerestedinhealthprofessionals’perspectivesonhealthliteracyandpalliativecareforMāoripatientsandwhānau,whatthehealthliteracydemandsofpalliativecareare,andhowservicesandhealthprofessionalstakeintoaccountpatient/whānauhealthliteracyskillsandservicehealthliteracydemandswhentheyareworkingwithMāoripatientsandwhānau.WearealsointerestedinthetoolsandresourcesthathealthservicesandprofessionalsusetohelpthemcommunicatewithMāoripatientsandwhānau.
WearetalkingwithhealthprofessionalsworkinginpalliativecareservicesinAucklandandtheBayofPlenty.Wewouldliketohaveafocusgroupwithstaff,andareinvitingyoutoparticipateinthisfocusgroup.
YourparticipationinthestudywillcontributetounderstandingMāoriaccesstopalliativecareservices,thehealthliteracydemandsplacedonMāoripatients/whānaubyhealthservicesandhealthprofessionals,andwhetherandhowtheseneedsanddemandsaremet.Thisinformationwillbeusefulforpalliativecarehealthworkers,palliativecareservices,peopleinvolvedinplanningandfundingservices,andforotherresearchers.
Peter Rothwell Academic Centre Waikato Hospital Pembroke St Hamilton, New Zealand Telephone 64 7 839 8750 Facsimile 64 7 839 8712 Email: [email protected]
The University of Auckland Peter Rothwell Academic Centre Waikato Hospital
Private Bag 3200 Hamilton New Zealand
113
Yourparticipationisentirelyvoluntary.Ifyoudoagreetotakepartinthestudy,youarefreetowithdrawfromthestudyatanytime,withouthavingtogiveareason.Beforethefocusgroupwewillexplainthestudyagainandaskyouifyouconsenttotakepart.Wewillaskyoutosignaconsentform.
Therewillbeonefocusgroupthatwilltakeaboutonehour.Thefocusgroupswillbeheldatyourworkplace.Duringthefocusgroupyoudonothavetojoininallofthediscussion,andyoumayleavethefocusgroupifyouwishwithouthavingtogiveareason.Wewillalsorecordthefocusgroupusingadigitalrecorder.
Takingpartinthestudywillnotcostyouanythingandyouwillnotbepaidfortakingpartinthestudy.
Theinformationfromyourinterviewwillnotincludeanydetailthatidentifiesyouoryourorganisation.
TheresearchwillbecompletedattheendofMarch2013.Areportforthewholeresearchprojectwillbewritten.Neitheryounoryourorganisationwillbeidentifiedinthisreport.Ifyouwouldliketogetacopyofthefullreportwewillsendyouone.Thefullreportwillbeavailableaboutthemiddleof2013.
Afterthestudyisfinishedthenotes,transcriptsandrecordingfilesfromthefocusgroupwillbestoredinalockedfilingcabinetorsecureelectronicfilesattheUniversityofAucklandfortenyearsandthenwillbedestroyed.Theconsentformswillbestoredinadifferentplacetothetranscripts,notesandrecordingfilesfortenyearsandthendestroyed.
YoucangetmoreinformationaboutthestudyfromNicolaCollins.Pleasefeelfreetocontactherifyouneedanymoreinformationorhaveanyquestionsaboutthisresearchproject.
MrsNicolaCollins,ResearchManager Phone:0212422530
Email:[email protected]
Ifyouhaveanyquestionsorconcernsaboutyourrightsasaparticipantinthisstudy,youmaywanttocontactanindependenthealthanddisabilityadvocate:
Freephone:0800555050 Freefax:08002SUPPORT(080027877678)
Email:[email protected]
ThisstudyhasreceivedethicalapprovalfromtheMulti‐regionEthicsCommittee,ethicsreferencenumberMEC/12/EXP/050,from13April2012until31March2013.
Nohooramai,ra
Dr.JacquieKidd,RN,PhDSeniorLecturerSchoolOfNursingFacultyofMedicalandHealthScience
114
ConsentForm(healthcareprofessionals)
Study:Palliativecare,healthliteracy,Māoricommunitiesandhealthservices
Requestforinterpreter:
English Iwishtohaveaninterpreter Yes No
Deaf IwishtohaveaNZsignlanguageinterpreter Yes No
Māori EhiahiaanaahaukitetahikaiwhakaMāori/kaiwhakapakehakorero Ae Kao
CookIslandMāori
Kainangaroauitetaitangataurireo Ae Kare
Fijian Augadrevameduaevakadewavosaveiau Io Sega
Niuean Fiamanakoaukefakaaogaetahatagatafakahokohokokupu E Nakai
Sāmoan Outemana’oiaiaisefa’amatalaupu Ioe Leai
Tokelaun KoauefofoukihetinokefakaliliutegaganaPeletaniakinagaganaonamotuotePahefika
Ioe Leai
Tongan Okuoufiema’uhafakatonulea Io Ikai
Otherlanguagestobeaddedfollowingconsultationwithrelevantcommunities.
IhavereadandIunderstandtheinformationsheetdated19thSeptember2012forvolunteerstakingpartinthestudydesignedtounderstandhealthprofessional’sknowledgeabouthealthliteracy,thehealthliteracydemandsassociatedwithpalliativecare,andhowthesedemandsaremanagedforMāoripatientsandwhānauinvolvedwithpalliativecareservices.
Ihavehadtheopportunitytodiscussthisstudy.IamsatisfiedwiththeanswersIhavebeengiven.
Peter Rothwell Academic Centre Waikato Hospital Pembroke St Hamilton, New Zealand Telephone 64 7 839 8750 Facsimile 64 7 839 8712 Email: [email protected]
The University of Auckland Peter Rothwell Academic Centre Waikato Hospital Private Bag 3200 Hamilton New Zealand
115
Ihavehadtheopportunitytousewhānausupportorafriendtohelpmeaskquestionsandunderstandthestudy.
Iunderstandthattakingpartinthisstudyisvoluntary(mychoice),andthatImaywithdrawfromthestudyatanytime,andthiswillinnowayaffectmyemployment.
Iunderstandthatmyparticipationinthisstudyisconfidentialandthatnomaterialthatcouldidentifymewillbeusedinanyreportsonthisstudy.
Ihavehadtimetoconsiderwhethertotakepartinthestudy.
IknowwhotocontactifIhaveanyquestionsaboutthestudy.
Iwishtoreceiveacopyoftheresults Yes No
ThisstudyhasreceivedethicalapprovalfromtheMulti‐regionEthicsCommittee,ethicsreferencenumberMEC/12/EXP/050,from13April2012until31March2013.
I__________________________________(fullname)herebyconsenttotakepartinthisstudy.
Date: Signature:
Note:
Acopyoftheconsentformistoberetainedbyeachparticipantand(inthecaseofpatients)acopyistobeplacedinthemedicalfile.
Fullnamesofresearchers: DrJacquieKiddMsSusanReidMrsNicolaCollinsMsStellaBlack
Contactphonenumberforresearchers: DrJacquieKidd078398750MsSusanReid093613800MrsNicolaCollins0212422530MsStellaBlack021415441
Projectexplainedby:
Projectrole:
Signature:
Date:
116
Interviewschedulehealthprofessionals
1) Māoriaccesstopalliativecareservices
a) Healthprofessionals(HP)experienceofMāoriaccesstopalliativecareservices(under/overaccess,quality)
b) DoyouthinkthatMāoriaccessdiffersbetweengeneralist(e.g.GPbased)orspecialistPCservices?i) Ifso,why?
2) HealthliteracyforMāoriinpalliativecarea) HPsunderstandingofthetermHLb) Whathealthliteracydemandsdoespalliativecare/theservicemakeonpatients/
familiesHL?c) DoestheservicetaketheseHLdemandsintoaccountinprovisionofservicesand
resources?i) ifso,how?ii) HowdoesHPknowthis?iii) CanHPgiveexamples?
d) Generallyspeaking,dopatients/whānaulevelofHLdifferbetweenMāoriandnon‐Māoripatients/whānau?i) Ifso,how?ii) HowdoesHPknowthis?iii) CanHPgiveexamples?
e) DoestheserviceuseanystrategiestohelpaddressthedifferentHLlevelsseenwithMāoripatients/whānau?i) Ifyes,whatarethestrategies?ii) Howweretheydeveloped?iii) Howeffectivearethesestrategies?iv) Couldtheybeimproved?v) Ifso,how?
3) Communicationwithpatientsandwhānaua) Ingeneral,howdoesHPcommunicatewithpatients/whānauinitially?
i) Andovertime?b) Aredifferentcommunicationstrategies/techniques/approaches/resourcesused
withMāoripatients/whānau?i) Ifso,canyoudescribetheseii) Howweretheydeveloped?iii) Whatarethestrengthsoftheseapproaches?iv) Howdoyouknowthesearestrengths?
c) WhatarethebarrierstoeffectivecommunicationwithMāoripatientsandwhānau?i) Whatiscurrentlybeingdonetoaddressthesebarriers?ii) Whatelsecouldbedone?
117
Key informant interview schedule
Healthliteracy(HL)demandsarethereading,writing,speaking,listening,andnumeracy(maths)patientsandwhānauhavetodotoengagewithyourservices.
1. Couldyoupleasetellmewhattheprocessiswhenapatientandwhānaufirstcomesintocontactwithyourorganisation?
ii) Whodotheyfirsthavecontactwith?
iii) Whatdopatientsandwhānauhavetodoatthatfirstcontact?Whatinformationdoyoucollectformthemandhow
(a) Oralinteractiononly
(b) Fillinforms
(c) Readdocuments
(d) Signdocuments
1. Astheprocessprogresses,whoelsedothepatientandwhānauhavecontactwith?
2. Whatotherthingsdopatientsandwhānauhavetoread,write,calculate,speakabout,listento?
3. Whatdoyounoticepatientsandwhānaudoing–takingnotes,askingyoutoexplainmore,checkingthingsonthecomputerorotherinformationsources
4. Whatdoyouaskpatientsandwhānautodoaboutdecisionmaking?Howdoyouinvolvepatientsandwhānauindecisionmaking?
5. (whererelevant)Aboutequipment–howdoyouinstructpatientsandwhānauhowtousethis?
6. (whererelevant)Aboutgivingandusingmedications–howdoyouinstructpatientsandwhānauhowtousethis?Whatdoyouaskpatientsandwhānautodoaboutthis(e.g.keepnotes,ringGP,ringpharmacist)
7. (whererelevant)Aboutsymptommanagementsuchaslevelofpain,levelofdiscomfort,howthepatient’ssymptomshavebeen,newsymptoms,‐whatdoyouaskpatientsandwhānautodoaboutthesethings?