Embed Size (px)
Citation preview

Histological and Histomorphometrical Comparative Studyof the Degradation and Osteoconductive Characteristicsof a- and b-Tricalcium Phosphate in Block Grafts
Masahiro Yamada,1 Makoto Shiota,1 Yasuo Yamashita,2 Shohei Kasugai1
1 Oral Implantology and Regenerative Dental Medicine, Tokyo Medical and Dental University,1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8549, Japan
2 Maxillofacial Anatomy, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8549, Japan
Received 31 January 2006; revised 7 July 2006; accepted 22 August 2006Published online 14 November 2006 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.b.30715
Abstract: The purpose of the present study was to compare a- and b-tricalcium phosphate
(TCP) as bone graft material for augmenting highly resorbed alveolar ridges. The cranial
bones of 15 rabbits were used. Three titanium chambers filled with porous blocks of a-TCP, b-
TCP, or blood clots were placed in each slit. The two TCP blocks had similar inner/outer
structures and purities. Animals were sacrificed after 2, 4, and 8 weeks. Specimens were
embedded in polyester resin as nondecalcified specimens, and evaluated both histologically
and histomorphometrically. In both TCP groups, blocks had hardly degraded at 2 weeks while
in the a-TCP group, the block had notably started degrading after 4 weeks. In the b-TCP
group, degradation began at 4 weeks and this degradation had increased just slightly after 8
weeks. The a-TCP block degraded significantly more than the b-TCP block. Residual a-TCP
particles surrounded by newly formed bone decreased over time, and both particles and newly
formed bone were simultaneously absorbed by osteoclast-like cells. These observations suggest
that residual a-TCP particles surrounded by newly formed bone may disappear progressively
from bone and could be incorporated into the bone remodeling cycle in combination with
newly formed bone. ' 2006 Wiley Periodicals, Inc. J Biomed Mater Res Part B: Appl Biomater 82B: 139–
148, 2007
Keywords: animal model; osteogenesis; calcium phosphate(s); bone remodeling; biodegra-
dation
INTRODUCTION
Alveolar ridge augmentation is fundamental for implant
dentistry. Although autogenous bone is considered to be
the best material for augmentation, it requires harvesting
surgery with notable associated risks,1,2 such as swelling at
the donor site or devitalization of teeth, abnormal sensa-
tion, etc. A wide variety of graft materials has therefore
been developed. Despite their clinical efficacy, allografts
and xenografts are subject to tight restrictions because of
religious sensibilities, value judgments or state regulations,
which arise mainly from anxiety about infection transmis-
sion from graft materials to recipients.3,4
As a result, alloplasts comprised of calcium phosphate
ceramics and bioactive glass have been studied.5–7 In par-
ticular, synthetic hydroxyapatite (HA), a calcium phosphate
ceramic, has a similar composition to hard tissues such as
teeth and bones8 and has been applied in the medical and
dental fields because of its high biocompatibility and osteo-
conductive properties.9,10
However, because of its high crystallinity and chemical
stability, HA is poorly absorbed or dissolved by multinu-
clear cells or tissue fluids and is poorly displaced by new
bone tissue.11–14 Furthermore, HA has the potential to be
easily adsorbed by bacteria and epithelial cells due to its
high surface energy,15 and may be easily infected and
encapsulated.16,17 Therefore, it is necessary to carefully
consider the application of HA.
Recently, studies have shown that tricalcium phosphate
(TCP) materials are biodegradable ceramics. In particular,
b-TCP has been advanced by both in vitro and in vivostudies.18–26 Because of its favorable osteoconduction and
biodegradation, b-TCP has been applied as a bone substi-
tute material for alveolar ridge augmentation at implanta-
tion sites.27–29
Although a-TCP has a different crystal structure from b-TCP, it has also been reported to show similar favorable
osteoconduction and biodegradation.30,31 Moreover, because
Correspondence to: M. Yamada (e-mail: [email protected])
' 2006 Wiley Periodicals, Inc.
139

of its greater solubility than HA and b-TCP,32 a-TCP easily
allows dissolution of the calcium and phosphate ions that
might otherwise advance osteogenesis.33–35 However, there
are very few in vivo studies comparing a-TCP with b-TCPand their reported differences may not reflect their crystal-
lographic discrepancy due to the extreme differences in
inner or outer shape and porosity36–39 of the tested materi-
als. Recently, Kihara et al.40 reported that osteogenesis
showed good progress following the application of a-TCPand that the residual a-TCP particles were degraded with-
out decreasing the volume of the transplantation region.
These findings suggested the possibility of using a-TCP as
a material for block grafts for the alveolar ridge.
In the present study, we compared the use of a- and b-TCP for augmentation of highly resorbed alveolar ridges
both histologically and histomorphometrically using com-
bined titanium chambers (Ti-chambers).
MATERIALS AND METHODS
Experimental Device
Turned chambers of commercially pure titanium (Node
Iron Works, Tokyo, Japan) with an inner diameter of 8 mm
and an inner height of 4.5 mm were used for standardizing
the experimental spaces and eliminating soft tissue (GBR
efficacy) (Figure 1).
a-TCP and b-TCP Blocks
a-TCP and b-TCP porous blocks (Figure 1) were provided
by BrainBase Corporation (Tokyo, Japan). Prebaked TCPs
(a-TCP, 11358C; b-TCP, 960–10008C) were crushed into
small particles (particle size under 0.85 mm in diameter),
molded with a binder, and sintered (a-TCP, 1150–12008C;
b-TCP, 960–10008C) into porous blocks with almost identi-
cal inner/outer structures (Table I). However, because of
processing difficulties the blocks could not be adjusted for
pore size or inner continuous conditions. The high purity of
the blocks were confirmed by X-ray diffractometry (Mini-
Flex, Rigaku, Tokyo, Japan) in powdering conditions to
crush again a sintered block sample. Just before use, both
TCP blocks were impregnated with rabbit blood using a
vibrator.
Surgery
A total of 15 male adult (6-months-old) Japanese white
rabbits, weighing 3–4 kg, were used in this study. All
experiments were approved by The Committee for Animal
Studies at Tokyo Medical and Dental University. After the
vertex cranium had been shaved and disinfected, general
anesthesia was induced by intramuscular injection of veteri-
nary ketamine hydrochloride (50 mg/mL; Ketalar1; San-
kyo, Tokyo, Japan) and thiopental sodium (25 mg/mL;
Ravonal1; Tanabe, Osaka, Japan). In addition, a local an-
esthetic (20 mg/mL; Xylocaine1; Astra, Sodertalje, Swe-
den) was subcutaneously injected around the operative
field. A full-thickness flap was raised to expose the cra-
nium. Using a trephine (7 mm in diameter), three 0.5-mm
deep circular slits, that crossed the cranial sutures and were
evenly spaced, were prepared at the parietal and frontal
bones. Within these slits, the cortical bone plate on both
sites was perforated with 9 evenly distributed holes using a
small round bur. Fixing screws were placed around the slits
at even spaced intervals.
Three Ti-chambers were filled with the test materials
were placed in each slit and attached to the bone with a
dental adhesive resin cement (Super-Bond C & B1 Clear;
Sun Medical, Shiga, Japan) and fixing screws. The bottom
of each chamber and the material it contained were in
direct contact with the bone without interposition of resin
cement (Figure 2). Each rabbit received 3 chambers: 1 neg-
ative control, 1 positive control, and 1 test chamber.
Negative Control Group: Autologous blood clots only,
that consisted of rabbit’s autologous venous blood þ throm-
Figure 1. Commercial pure titanium chamber (left) and tricalcium-
phosphate porous block used in this study.
TABLE I. Conformation of a-TCP and b-TCP Porous Blocksa
a-TCP b-TCP
Diameter (mm) 6.8 6.7
Thickness (mm) 3.2 3.1
Density (g/mm2) 0.16 0.17
Relative density (%) 53 56
a Both blocks have almost identical inner/outer structure and purity.
Figure 2. Ti-chambers (TC) were placed and attached to the bonewith dental adhesive resin cement involving fixing screws.
140 YAMADA ET AL.
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb

bin (Mitsubishi Pharma Corporation, Osaka, Japan) þ liquid
calcium chloride.
Positive Control Group: b-TCP block containing blood
clots.
Test Group: a-TCP block containing blood clots.
The position of the chambers was randomly chosen for
each rabbit. The skin flaps were sutured with 3-0 surgical
silk. No attempt was made to cover the cylinders with the
periosteum.
Specimen Preparation
The animals were sacrificed after a healing period of 2, 4,
and 8 weeks by excessive intravascular administration of
pentobarbital sodium (50 mg/mL; Nembutal1; Dainippon
Pharmaceutical, Osaka, Japan). The soft tissue of the exper-
imental area was removed and biopsy specimens of the pa-
rietal-frontal bones comprising the three Ti-chambers were
taken en bloc and fixed by immersion in 10% formalin.
The specimens were dehydrated through a graded series of
acetone, embedded in polyester resin (Rigolac1; Showa
Highpolymer, Tokyo, Japan) and sectioned vertically
through the center of each chamber using a sawing and
grinding system (Exakt System; Exakt Apparatebau, Nor-
derstedt, Germany). A total of 7 sections/specimen were
prepared. Each section was ground to a thickness of about
30 mm and stained with 4% toluidine blue.
Analyses
Histological and histomorphometrical analysis were per-
formed using a light microscope digital camera (Olympus1
DP12; Olympus, Tokyo, Japan) and digital image editing
software (Adobe Photoshop CS; Adobe, San Jose, CA).
Morphometric measurements were made on 3 vertical sec-
tions/specimen closest to the center of the specimen. The
following measurements were made (Figure 3).
Area of Residual Implant: Area of residual TCP in the
block (%).
Area of Noninvaded Implant: Area of residual TCP not
invaded by new bone tissue into the block (%).
Each measurement indicated accounted for a certain per-
centage of the area of the original block.
Statistical Analyses
Nonparametric analyses were used because blocks were
grafted on the same individual and because the experimen-
tal groups were not large enough to apply parametric analy-
sis. The Wilcoxon t test was run for intergroup analyses (avs. b) of the measurements. The Kruskal–Wallis H test was
used for comparisons within groups and the Mann–Whitney
U test with the Bonferroni correction was used post hoc to
determine the location of significant differences. The funda-
mental significance for the analyses was set to p < 0.05.
RESULTS
Histological Analysis
Control (Blood Clots Only)
2 Weeks. Connective tissue and a small quantity of
newly formed bone with a high staining intensity were
observed on the surface of the existing bone within the Ti-
chamber (Figure 4).
4 Weeks. Newly formed bone on the surface of the host
bone was increased compared with 2 weeks and proceeded
along the inner walls of the Ti-chamber. Furthermore,
staining intensity was generally decreased compared with 2
weeks (Figure 5).
8 Weeks. Newly formed bone had progressed along the
inner wall of the tectorium of the Ti-chamber along the
inner walls and was observed up to one-third of the height
Figure 3. The digital image by editing software used for histmorphometric analysis. Area of theremained block parts (Area of Residual Implant) is represented as black and checked. Area of the
nonintruded block parts (Area of Noninvaded Implant) is represented as black. [Color figure can be
viewed in the online issue, which is available at www.interscience.wiley.com.]
141CHARACTERISTICS OF a- AND b-TCP POROUS BLOCKS
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb

of the Ti-chamber at the central area, which showed the
least bone formation [Figure 6(a)].
The staining intensity of the newly formed trabeculae
along the inner walls of the Ti-chamber was decreased
compared with 4 weeks, and the thickness was increased.
However, on the upper side of the Ti-chamber, densely
stained bone was observed [Figure 6(b)].
b-TCP
2 Weeks. The surface of the b-TCP block showed a
smooth circumference. Between the host bone and the block,
newly formed immature bone was present that had a high
staining intensity and was continuous with the host bone
(Figure 7).
4 Weeks. Concavities were observed on the bottom sur-
face of the block. Newly formed bone continuing to the
host bone was increased slightly compared to 2 weeks
[Figure 8(a)].
At high magnification, new bone formation was ob-
served that corresponded to the concavities on the bottom
surface of the block. Although the newly formed bone was
partially in contact with the surface of the b-TCP block, it
never invaded the concavities. The trabeculae ran parallel
to the surface of the block [Figure 8(b)].
Figure 6. (a) Blood clots only group at 8 weeks. Newly formed bone
(NB) is visible up to one-third of the height of the titanium chamber at thecentral area. (Original magnification 35). (b) Blood clots only group at 8
week in moderate magnification. Low stainable newly formed bone (NB)
existed along the inner walls of TC. High stainable NB existed on the
upper side of TC. (Original magnification310). [Color figure can be viewedin the online issue, which is available at www.interscience.wiley.com.]
Figure 7. Toluidine blue staining of b-TCP group in nondecalcified
specimens at 2 weeks. The surface of b-TCP block is circumferentially
smooth (Original magnification 35). [Color figure can be viewed in theonline issue, which is available at www.interscience.wiley.com.]
Figure 4. Toluidine blue staining of blood clots only group in nonde-
calcified specimens at 2 weeks. There is no much newly formedbone (NB) visible. (Original magnification 35) HB, host bone; TC, ti-
tanium chamber. [Color figure can be viewed in the online issue,
which is available at www.interscience.wiley.com.]
Figure 5. Blood clots only group at 4 weeks. Newly formed bone
(NB) has progressed along with the inner wall of titanium chamber
(TC). (Original magnification 35). [Color figure can be viewed in theonline issue, which is available at www.interscience.wiley.com.]
142 YAMADA ET AL.
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb

8 Weeks. The concavities on the bottom surface of the
block had progressed slightly compared with 4 weeks. The
amount of newly formed bone between the block and the
host bone and along the inner walls of the Ti-chamber was
increased compared with 4 weeks [Figure 9(a)].
The newly formed trabeculae between the block and the
host bone were thicker and showed a slightly lower stain-
ing intensity than at 4 weeks. Newly formed immature
bone with a high staining intensity was found on relatively
larger concavities of the block [Figure 9(b)].
a-TCP
2 Weeks. The surface of the a-TCP block showed a
smooth circumference, similar to b-TCP. Between the
block and the host bone, newly formed immature bone
with a high staining intensity was observed. It continued to
the host bone and was partly in contact with the smooth
surface of the block (Figure 10).
4 Weeks. Unlike b-TCP, many inner cavities of the bot-
tom angles were observed, as well as concavities on the
bottom surface of the block. These inner cavities proceeded
to deep parts of the block. Slight concavities were also
observed around the surface of the block that was in con-
tact with the connective tissue. The quantity and maturity
of the newly formed bone were increased compared with 2
weeks [Figure 11(a)].
Newly formed bone invaded in the region of concavities
and cavities. In this region, degraded and fractionated a-TCP particles were frequently surrounded by newly formed
bone [Figure 11(b)].
Some multinuclear giant cells containing phagocytosed
a-TCP particles were observed as well [Figure 11(c)].
8 Weeks. The inner concavities of the a-TCP block had
proceeded remarkably not only in the region of the angles
Figure 9. (a) b-TCP group at 8 weeks (original magnification 35).
Concavities (triangle) on the bottom surface of the block are slightlyincreased compared to 4 weeks. (b) b-TCP group at 8 weeks in
moderate magnification (original magnification 310). Newly formed
bone (NB) (double arrow) is found on the relatively larger concavities
(triangle) of the block. [Color figure can be viewed in the onlineissue, which is available at www.interscience.wiley.com.]
Figure 8. (a) b-TCP group at 4 weeks (original magnification 35).
Concavities (triangle) are observed on the bottom surface of theblock. (b) b-TCP group at 4 weeks (original magnification 310).
Newly formed bone (NB) is never observed to intrude into the con-
cavities (triangle). [Color figure can be viewed in the online issue,
which is available at www.interscience.wiley.com.]
143CHARACTERISTICS OF a- AND b-TCP POROUS BLOCKS
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb

of the block bottom, but also in the upper part of the side
of the block and deep parts of the inner block. The block
had almost completely lost its original shape. The inner
concavities of the block had approximately progressed to
half the block height [Figure 12(a)].
Newly formed bone had invaded almost the entire
region of the inner concavities. The newly formed trabecu-
lae were thicker and showed a lower staining intensity than
at 4 weeks. Less residual a-TCP particles were surrounded
by the new bone in the same region at 4 weeks as is shown
in Figure 12(b).
Osteoblasts were observed on the surface of the newly
formed bone surrounding the a-TCP particles, as well as
osteocytes [Figure 12(c)]. In addition, both newly formed
bone and a-TCP particles were uniquely absorbed by osteo-
clast-like cells [Figure 12(d)].
Histomorphometrical Analysis (Figure 13 and 14)
Intragroup Comparisons. Area of Residual Implant
and Area of Noninvaded Implant showed notable signifi-
cant differences (p < 0.01) for 2 weeks/8 weeks in the b-TCP group, and 2 weeks/4 weeks and 2 weeks/8 weeks in
the a-TCP group. No other significant differences were
found.
a-TCP vs. b-TCP. Area of Residual Implant and Area
of Noninvaded Implant showed significant differences (p ¼0.044) at 4 weeks and 8 weeks. At 2 weeks, there was no
significant difference.
DISCUSSION
Bone graft materials are categorized as autografts, allo-
grafts, xenografts, and alloplasts. Their fundamental use in
clinical practice is considered to be as scaffolds for osseous
regeneration.41,42 TCPs are recognized as alloplastic materi-
als that have no associated hazards of infecting the recipi-
ents with unknown viruses and are gradually displaced by
new bone in vivo.In the present study, Ti-chambers were used to standard-
ize experimental conditions and borders with the host bone
were sealed circumferentially with dental resin cement. The
biotolerance and border seal-ability of the dental resin
cement were confirmed in previous studies43 and our pilot
study (data not shown). In earlier studies,19,44,45 bone forma-
tion in the chamber was reported to be facilitated by border
sealing around the chamber, similar to guided bone regener-
ation. In the negative control (blood clots only), connective
tissue and newly formed bone originating in the host sutures
and bone marrow were mainly observed along the Ti-cham-
ber side walls and the height of the new bone increased pro-
gressively. At 8 weeks, new bone grew at the lowest point
to one-third of the Ti-chamber height at the central area.
This observation further confirmed previous studies.
In the present study, direct contact and invasion into the
blocks of newly formed bone was observed, corresponding
to concavities on the block surface and to cavities in the
block for both TCP groups. In particular, newly formed
bone surrounded the residual particles in the a-TCP group.
These observations demonstrate the biocompatibility and
biodegradation of the TCPs, which were absorbed and
replaced by new bone. In both groups, the surface of the
blocks showed a smooth circumference and degradation of
the blocks was hardly observed at 2 weeks. However, in
the a-TCP group, many inner cavities in parts of the bot-
tom angles near the host bone were observed at 4 weeks.
At 8 weeks, these regions of inner cavities had proceeded
into the deeper parts of the blocks and to half the block
height at their lowest point. In the b-TCP group, some
minor concavities were found on the bottom surface of the
block at 4 weeks and their number and size had only
increased slightly at 8 weeks. The degradation of b-TCPwas generally lower than a-TCP, where almost no original
block remained at 8 weeks. In the histomorphometrical
analysis, both Area of Residual Implant and Area of Nonin-
vaded Implant differed significantly between the two TCP
groups at 4 weeks and 8 weeks.
Absorption of alloplasts in vivo has been recognized to
occur through two processes, namely cellular absorption by
multinuclear giant cells and dissolution by tissue fluids.26,32
The most different feature between a-TCP and b-TCP is the
solubility in liquid solution. Eggli et al.44 suggested that
absorption of TCPs is initiated via phagocytosis by multinu-
clear giant cells. On the other hand, Schliephake et al.45 and
Fujita et al.24 suggested that their absorption begins with dis-
solution by tissue fluids, and is then followed by cellular
absorption. Furthermore, Zerbo et al.29 and Lu et al.26 sug-
gested that the initial absorption of TCPs is influenced not
only by cellular absorption but also by dissolution. In the
present study, multinuclear giant cells did not contact the a-TCP blocks directly. Instead, the blocks crumbled and
released particles that were phagocytosed at 4 weeks. On the
other hand, there was no direct contact of multinuclear giant
cells with the blocks and phagocytosis of particles was not
Figure 10. Toluidine blue staining of the a-TCP porous block (AB)
group in nondecalcified specimens at 2 weeks. The surface of thea-TCP block is circumferentially smooth (original magnification 35).
[Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
144 YAMADA ET AL.
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb
observed in the b-TCP group. Accordingly, it is suggested
that the differences in degradation observed in vivo between
the a-TCP and b-TCP porous blocks reflect a higher solubil-
ity of a-TCP in liquid solution, as was shown in a previous
in vitro study32 (dominant dissolution by tissue fluids), and
these differences in degradation are hardly influenced by cel-
lular absorption.
Absorption by osteoclast-like cells of the residual a-TCPparticles surrounded by newly formed bone was observed
at 8 weeks. Additionally, in the same region there were
less residual a-TCP particles surrounded by newly formed
bone at 8 weeks than at 4 weeks. These observations sug-
gest that the residual a-TCP particles surrounded by newly
formed bone might disappear progressively from new bone,
at least in part by cellular absorption.
The Area of Noninvaded Implant, which represents the
area of the block not invaded by regenerating tissue, includ-
ing newly formed bone, was significantly lower for a-TCPthan b-TCP at both 4 weeks and 8 weeks. These findings
indicate that a large amount of new bone formation invaded
the a-TCP block with notable degradation. An earlier study
reported that intrusion of osteoblasts or osteoclasts required
spaces of more than 50 mm, while new bone formation
required spaces of more than 100 mm.12 Consequently, the
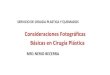
Figure 11. (a) a-TCP group at 4 weeks (original magnification 35). Many inner cavities of the bot-
tom angles are visible. (b) a-TCP group at 4 weeks (original magnification 310). Newly formed
bone (NB) intrudes into the inner cavities of the block. Degraded and fractionated a-TCP particles
(asterisk) are surrounded by NB. (c) a-TCP group at 4 weeks at high magnification (original magnifi-cation 340). Multinuclear giant cell (double arrow) phagocytose a-TCP particles. [Color figure can
be viewed in the online issue, which is available at www.interscience.wiley.com.]
145CHARACTERISTICS OF a- AND b-TCP POROUS BLOCKS
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb
formation of different spaces in the two types of blocks fol-
lowing degradation may cause the discrepancy in the ranges
of newly formed bone invasion into the blocks.
In an earlier study, it was reported that increases in the
local Ca and P ion concentrations as a consequence of deg-
radation of TCPs stimulated new bone formation. Sugimoto
et al.46 and Honda et al.47 showed that high concentrations
of Ca ions in vivo accelerated the activation and differen-
tiation of osteoblasts. Aoki et al. speculated that the local
pH showed a trend toward the basic side due to the release
of Ca ions and that this chemical change proved that the
circumjacent bone undergoes some kind of activation. Fur-
thermore, recent studies21,30,33–35 have shown that dissolu-
tion of Ca and P ions around TCPs accelerates new bone
formation via reseparation and the formation of amorphous
apatite layers around the residual particles. In particular,
Fusimi et al.30 observed by transmission electron micros-
copy that a collagen-free layer created from hydroxyapatite
was present around a-TCP particles surrounded by newly
formed bone and that new bone was formed circumferen-
tially on this apatite layer. Furthermore, Habibovic et al.35
concluded in a goat study that biomaterials containing Ca
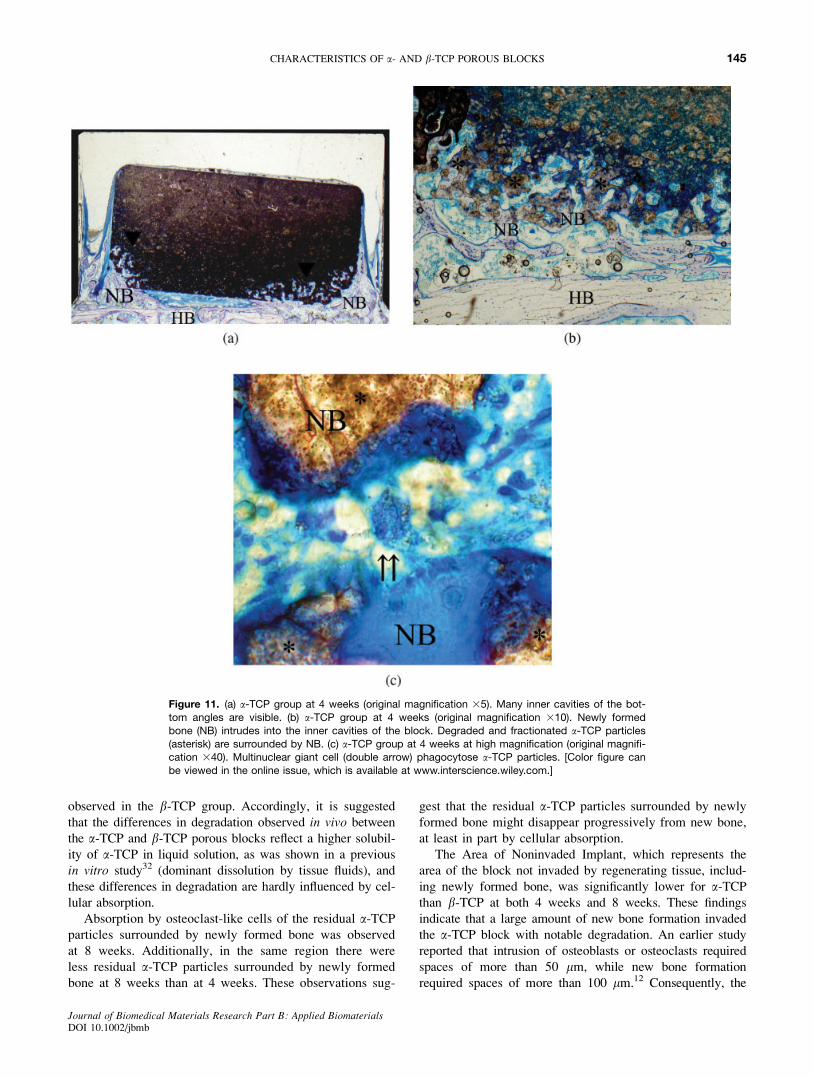
Figure 12. (a) a-TCP group at 8 weeks (original magnification 35). The inner cavities of the blockprogress to one-third of the Ti-chamber height at the lowest point. Asterisk show a-TCP particles
surrounded by newly formed bone. (b) a-TCP group at 8 weeks (original magnification 310). Newly
formed bone (NB) intrudes almost the entire inner cavities of the blocks. Less residual a-TCP par-
ticles (asterisk) are surrounded by the new bone in the same region at 4 weeks. (c) a-TCP group at8 weeks at high magnification (original magnification 350). Osteoblasts (double arrow) are visible
on the surface of newly formed bone (NB) surrounding TCP particles (asterisk). Arrow shows multi-
nuclear giant cell. (d) a-TCP group at 8 weeks at high magnification (original magnification 350).
Both newly formed bone (NB) and a-TCP particles (asterisk) are absorbed by osteoclast-likecell (double arrow). [Color figure can be viewed in the online issue, which is available at www.
interscience.wiley.com.]
146 YAMADA ET AL.
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb

and P accelerated the differentiation of osteoblasts and the
formation of new bone via biological apatite layers formed
by redeposition of Ca and P and coprecipitated endogenous
proteins such as BMPs.
No apatite layers were observed around the residual a-TCP particles in the present study. It is possible that the
newly formed bone surrounding the residual particles at 4
weeks and 8 weeks could be generated by Ca and P ions,
as observed in previous studies. However, some studies
have suggested that excessive local concentrations of Ca
interrupt new bone formation.11,37,39,48 Although good bone
formation was observed in the a-TCP porous blocks used
in the present study, the same results may not be observed
for a-TCP porous blocks that have a higher solubility and
therefore elevate the local Ca and P concentrations.37,39
In previous studies,25,48 it has been suggested that TCP
particles embedded in newly formed bone are subject to
cellular absorption and become incorporated into the bone
remodeling process. In the present study, these findings
were never observed in the b-TCP group because there was
little new bone formation inside the blocks. However, in
the a-TCP group, bone formation by osteoblasts, and the
resorption of both the residual particles and newly formed
bone by osteoclast-like cells were observed at 8 weeks.
These observations may indicate that the newly formed
bone around a-TCP shows features and homeostasis that
are similar to normal bone, such as the bone remodeling
cycle for functional loading.
CONCLUSIONS
a-TCP porous blocks showed higher initial solubility invivo than b-TCP blocks. Additionally, the residual a-TCPparticles surrounded by newly formed bone appeared to be
dissolved by tissue fluids and absorbed by osteoclast-like
cells. Furthermore, the degradation of a-TCP seemed to be
aligned with bone formation, while the newly formed bone
surrounding a-TCP became incorporated into the bone
remodeling cycle with the residual particles.
REFERENCES
1. Clavero J, Lundgren S. Ramus or chin grafts for maxillarysinus inlay and local onlay augmentation: Comparison of do-nor site morbidity and complications. Clin Implant Dent RelatRes 2003;5:154–160.
2. Raghoebar GM, Louwerse C, Kalk WW, Vissink A. Morbid-ity of chin bone harvesting. Clin Oral Implants Res 2001;12:503–507.
3. Li CM, Ho YR, Liu YC. Transmission of human immunodefi-ciency virus through bone transplantation: A case report. JFormos Med Assoc 2001;100:350,351.
4. Honig JF, Merten HA, Heinemann DE. Risk of transmissionof agents associated with Creutzfeldt-Jakob disease and bo-vine spongiform encephalopathy. Plast Reconstr Surg 2000;105:2273–2275.
5. Hollinger JO, Brekke J, Gruskin E, Lee D. Role of bone sub-stitutes. Clin Orthopaed Relat Res 1996;324:55–65.
6. Cancian DC, Hochuli-Vieira E, Marcantonio RA, Garcia Jun-ior IR. Utilization of autogenous bone, bioactive glasses, andcalcium phosphate cement in surgical mandibular bone de-fects in Cebus apella monkeys. Int J Oral Maxillofac Implants2004;19:73–79.
7. Al Ruhaimi KA. Bone graft substitutes: A comparative quali-tative histologic review of current osteoconductive graftingmaterials. Int J Oral Maxillofac Implants 2001;16:105–114.
8. Ishikawa K. Lies and truth of apatite (Japanese). J OralImplants 2002;12:34–50, 2003;13:53–67, 14:49–65, 15:31–50.
9. Velich N, Nemeth Z, Hrabak K, Suba Z, Szabo G. Repair ofbony defect with combination biomaterials. J Craniofac Surg 2004;15:11–15.
10. Goto T, Kojima T, Iijima T, Yokokura S, Kawano H, Yama-moto A, Matsuda K. Resorption of synthetic porous hydroxy-apatite and replacement by newly formed bone. J OrthopaedSci 2001;6:444–447.
11. Yamada K, Umeda M, Komori T, Kawai T. Influence of hy-droxyapatite (HA) chemical composition on solubility behav-ior and bone formation. Jpn Stomatol Soc 2001;5090–5097.
12. Takagi T. Experimental study of the subperiosteal onlay graftof synthetic hydroxyapatite. J Tohoku Univ Dent Soc 1985;4:135–151.
13. Yonehara Y, Takato T, Susami T, Hurumori T, Mori Y, Hikiti N,Nakatsuka T. Investigation of the biocompatibility and osteo-inductive ability of a high-porosity hydroxyapatite and tricalciumphosphate composite. Jpn J Plast Reconstr Surg 1997;40:717–723.
Figure 13. No mark, p > 0.05. The a-TCP group is significantly
lower than the b-TCP group at 4 weeks and 8 weeks. There are sig-
nificant differences at 2 weeks/8 weeks in the b-TCP group, and 2weeks/4 weeks and 2 weeks/8 weeks in the a-TCP group. Compari-
son between two groups – Wilcoxon t test, *p ¼ 0.044; comparison
within each group – Kruskal–Wallis H test and Mann–Whitney U test
with Bonferroni correction, #1p ¼ 0.007, #2p ¼ 0.008.
Figure 14. No mark, p > 0.05. The a-TCP group is significantly
lower than the b-TCP group at 4 weeks and 8 weeks. There are sig-nificant differences for 2 weeks/8 weeks in the b-TCP group, and 2
weeks/4 weeks and 2 weeks/8 weeks in the a-TCP group. Compari-
son between two groups – Wilcoxon t test, *p ¼ 0.044; comparison
within each group – Kruskal–Wallis H test and Mann–Whitney U testwith Bonferroni correction, #3p ¼ 0.006, #4p ¼ 0.009.
147CHARACTERISTICS OF a- AND b-TCP POROUS BLOCKS
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb
14. Schmid J, Hammerle CH, Fluckiger L, Winkler JR, Olah AJ,Gogolewski S, Lang NP. Blood-filled spaces with and withoutfiller materials in guided bone regeneration. A comparativeexperimental study in the rabbit using bioresorbable mem-branes. Clin Oral Implants Res 1997;8:75–81.
15. Yamashita K. CEPRO (Japanese), Tokyo, Japan; 2000.16. Rosen HM. The response of porous hydroxyapatite to contigu-
ous tissue infection. Plast Reconstr Surg 1991;88:1076–1080.17. Chidyllo SA, Marschall MA. Porous hydroxyapatite and tissue
infection. Plast Reconstr Surg 1992;90:146–147.18. Bhaskar SN, Brady JM, Getter L, Grower MF, Driskell T.
Biodegradable ceramic implants in bone. Electron and lightmicroscopic analysis. Oral Surg Oral Med Oral Pathol 1971;32:336–346.
19. Takaoka K. Effects of b-tricalcium phosphate on bone aug-mentation within a titanium cap in rabbit parietal bone. J JpnSoc Conserv Dent 2001;44:115–123.
20. Yamada Y, Boo JS, Ozawa R, Nagasaka T, Okazaki Y, HataK, Ueda M. Bone regeneration following injection of mesen-chymal stem cells and fibrin glue with a biodegradable scaf-fold. J Craniomaxillofac Surg 2003;31:27–33.
21. Le Huec JC, Clement D, Brouillaud B, Barthe N, Dupuy B, Foli-guet B, Basse-Cathalinat B. Evolution of the local calcium con-tent around irradiated b-tricalcium phosphate ceramic implants:In vivo study in the rabbit. Biomaterials 1988;19: 733–738.
22. Koepp HE, Schorlemmer S, Kessler S, Brenner RE, Claes L,Gunther KP, Ignatius AA. Biocompatibility and osseointegra-tion of b-TCP: Histomorphological and biomechanical studiesin a weight-bearing sheep model. J Biomed Mater Res BAppl Biomater 2004;70:209–217.
23. Fujita R, Yokoyama A, Kawasaki T, Kohgo T. Bone augmenta-tion osteogenesis using hydroxyapatite and b-tricalcium phos-phate blocks. J Oral Maxillofac Surg 2003;61:1045–1053.
24. Fujita R, Wakasa R, Yokoyama A, Komatsubara H, TakeishiA, Kawasaki T, Kohgo T. Onlay graft of hydroxyapatite andb-tricalcium phosphate blocks on the bone. Hokkaido J DentSci 2000;21:118–129.
25. Morikawa S. Comparative study on b-tricalcium phosphateand hydroxyapatite as bioactive artificial bone fillers. JikeikaiMed J 2000;115:193–207.
26. Lu JX, Gallur A, Flautre B, Anselme K, Descamps M, ThierryB, Hardouin P. Comparative study of tissue reactions to calciumphosphate ceramics among cancellous, cortical, and medullarbone sites in rabbits. J Biomed Mater Res 1998;42:357–367.
27. Szabo G, Suba Z, Hrabak K, Barabas J, Nemeth Z. Autogenousbone versus b-tricalcium phosphate graft alone for bilateralsinus elevations (2- and 3-dimensional computed tomographic,histologic, and histomorphometric evaluations): Preliminaryresults. Int J Oral Maxillofac Implants 2001;16:681–692.
28. Zijderveld SA, Zerbo IR, van den Bergh JP, Schulten EA, tenBruggenkate CM. Maxillary sinus floor augmentation using ab-tricalcium phosphate (Cerasorb) alone compared to autogenousbone grafts. Int J Oral Maxillofac Implants 2005;20:432–440.
29. Zerbo IR, Bronckers AL, de Lange G, Burger EH. Localisa-tion of osteogenic and osteoclastic cells in porous b-trical-cium phosphate particles used for human maxillary sinus floorelevation. Biomaterials 2005;26:1445–1451.
30. Fushimi M. Solubilities and bone interfaces in sintered a-tri-calcium phosphate and hydroxyapatite. J Jpn Soc Biomater1995;13:224–235 (in Japanese).
31. Nagase M, Chen RB, Asada Y, Nakajima T. Radiographicand microscopic evaluation of subperiosteally implanted
blocks of hydrated and hardened a-tricalcium phosphate inrabbits. J Oral Maxillofac Surg 1989;47:582–586.
32. Doi Y. Bioceramics. J Gifu Dent Soc 2002;28:281–290 (inJapanese).
33. Geesink RG, de Groot K, Klein CP. Bonding of bone to apa-tite-coated implants. J Bone Joint Surg Br Vol 1988;70:17–22.
34. Hanawa T, Kamiura Y, Yamamoto S, Kohgo T, Amemiya A,Ukai H, Murakami K, Asaoka K. Early bone formationaround calcium-ion-implanted titanium inserted into rat tibia.J Biomed Mater Res 1997;36:131–136.
35. Habibovic P, Yuan H, van der Valk CM, Meijer G, van Blit-terswijk CA, de Groot K. 3D microenvironment as essentialelement for osteoinduction by biomaterials. Biomaterials 2005;26:3565–3575.
36. Merten HA, Wiltfang J, Grohmann U, Hoenig JF. Intraindi-vidual comparative animal study of a and b-tricalcium phos-phate degradation in conjunction with simultaneous insertionof dental implants. J Craniofac Surg 2001;12:59–68.
37. Yuan H, De Bruijn JD, Li Y, Feng J, Yang Z, De Groot K, ZhangX. Bone formation induced by calcium phosphate ceramics in softtissue of dogs: A comparative study between porous a-TCP andb-TCP. J Mater Sci Mater Med 2001;12:7–13.
38. Wiltfang J, Merten HA, Schlegel KA, Schultze-Mosgau S,Kloss FR, Rupprecht S, Kessler P. Degradation characteristicsof a and b-tricalcium phosphate (TCP) in minipigs. J BiomedMater Res 2002;63:115–121.
39. Yuan H, Yang Z, De Bruij JD, De Groot K, Zhang X. Mate-rial-dependent bone induction by calcium phosphate ceramics:A 2.5-year study in dog. Biomaterials 2001;22:2617–2623.
40. Kihara H, Shiota M, Yamashita Y, Kasugai S. Biodegaradationprocess of a-TCP particles and new bone formation in a rabbitcranial defect model. J Biomed Mater Res. Forthcoming.
41. Donos N, Kostopoulos L, Tonetti M, Karring T. Long-termstability of autogenous bone grafts following combined appli-cation with guided bone regeneration. Clin Oral Implants Res2005;16:133–139.
42. Slotte C, Lundgren D, Burgos PM. Placement of autogeneicbone chips or bovine bone mineral in guided bone augmenta-tion: A rabbit skull study. Int J Oral Maxillofac Implants 2003;18:795–806.
43. Inoue T, Matsuzaka K, Murakami S. An experimental studyon the osteogenesis of bmp-containing 4-meta/mma-tbb adhe-sive resin. Engl Jpn J Conserv Dent 2002;45:434–440.
44. Eggli PS, Muller W, Schenk RK. Porous hydroxyapatite andtricalcium phosphate cylinders with two different pore sizeranges implanted in the cancellous bone of rabbits. A compara-tive histomorphometric and histologic study of bony ingrowthand implant substitution. Clin Orthopaed Relat Res 1988; 232:127–138.
45. Schliephake H, Kage T. Enhancement of bone regenerationusing resorbable ceramics and a polymer-ceramic compositematerial. J Biomed Mater Res 2001;56:128–136.
46. Sugimoto T, Kanatani M, Kano J, Kaji H, Tsukamoto T,Yamaguchi T, Fukase M, Chihara K. Effects of high calciumconcentration on the functions and interactions of osteoblasticcells and monocytes and on the formation of osteoclast-likecells. J Bone Miner Res 1993;8:1445–1452.
47. Honda Y, Fitzsimmons RJ, Baylink DJ, Mohan S. Effects ofextracellular calcium on insulin-like growth factor II inhuman bone cells. J Bone Miner Res 1995;10:1660–1665.
48. Aoki H, Kato K, Ogiso M, Tabata T. Osteocompatibility ofapatite ceramics in mandibles. Sikarikozassi 1977;18:86–89(in Japanese).
148 YAMADA ET AL.
Journal of Biomedical Materials Research Part B: Applied BiomaterialsDOI 10.1002/jbmb





![XXX V I. K e0,$, E / $'Ï, N APOK[4] B.I. Whittington (1997) Tricalcium aluminat heaxahidrate (TCA) filter aid in the Bayer industry: factors affecting TCA pr eparation and morphology](https://img.pdfslide.tips/doc/110x75/5fe3599a46775b517d017a1a/xxx-v-i-k-e0-e-n-apok-4-bi-whittington-1997-tricalcium-aluminat.jpg)