-
Tricyclic Antidepressants Intoxication
100.10.18
History & Epidemiology
First TCA for depression in the late 1950s: Imipramine1960-1980:
TCAs were the major pharmacologic treatment for
depression1980-1990: newer CAs (maprotiline) due to serious
toxicity of older TCAsLast 10 years: SSRI
History & Epidemiology
1993-1997 in England and Wales: 95% of poisoning death, esp.
amitriptyline and dothiepin.Leading cause of poisoning fatalities
in US until 1993.12-13% all CA exposures during the last 10 years
< 6 y/o; second most commonly usedMost lethal unintentional drug
ingestions in younger children
Pharmacology & Pharmacokinetics
CAs inhibit presynaptic reuptake of NE and/or serotoninChemical
structure classification:
Tertiary Amines Secondary
AminesAmitriptylineClomipramineDoxepinImipramineTrimipramine
DesipramineNortriptylineProtriptylineAmoxapineMaprotiline
More potent inhibitors in NE
More potent inhibitors in serotonin
Pathophysiology & Manifestations
Tri-blockerMuscarinic acetylcholine receptorsPeripheral 1-
adrenergic receptorSodium channel
GABA receptor-chloride-ionophore complex in brainLow toxicity
threshold
10-20 mg/kg: significant manifestations2-4 mg/kg/d: therapeutic
dose> 1 g: life-threatening in adult
Progression is unpredictable and rapid
4CConductionContractilityConfusionConvulsion
-
Pathophysiology & Manifestations
Acute cardiovascular toxicityAcute cardiovascular
toxicityPrimarily responsible for morbidity and mortalityConduction
delay: RBBB; PR, QRS, QTcThe most common dysrhythmia in overdose:
sinus tachycardia (aberrantly conducted)Wide-complex tachy:
potentially life-threateningBlocks are rare Torsades is more likely
in bradycardia; VT/VF only 4% of all cases
Pathophysiology & Manifestations
Acute cardiovascular toxicityAcute cardiovascular toxicityThe
most common cause of death: refractory hypotension prolong
CPRHypotension is multifactorial:
Impairing myocardial contractilityBlunted responses to
catecholaminesPeripheral vasodilationHypoxia, acidosis, volume
depletion, seizure
Pathophysiology & Manifestations
Acute CNS toxicityAcute CNS toxicityAgitation, delirium
anticholinergic effectsSeizure
GABA-chloride complexGeneralized and briefWithin 1-2 hours of
ingestion4% in patients; 13% in fetal casesRisks: HI, history of
seizure, other drug withdrawal
Uncontrolled seizures are uncommonMA, hyperthermia,
rhabdomyolysis, ARF
Pathophysiology & Manifestations
Other complicationsOther complicationsAcute lung injury, ARDS,
aspiration pneumonitisIschemia bowelPancreatitis
Death in the first several hours due toLate deaths (>1-2
days) due to complications
Diagnostic testing
ECGECGMaximal limb lead QRS is a sensitive indicator of toxicity
(dysrhythmia, coma, hypotension, seizure)
QRS>100 msec: 33% seizures; 14% VT/VFQRS>160 msec: 50%
VT/VF
Terminal 40-ms QRS right side deviationMore sensitive than
QRSPPV and NPV for TCA ingestion: 66% & 100%
-
Managements
ABCD, O2-IV-monitorEarly intubationEKG for all patientsLab
tests: CBC, BCS, ABG, drug levelKeep vital signs
Managements
GI decontamination GI decontamination Benefits against risks be
weighedOrogastric lavage up to 12 hrs after ingestionMay intubation
firstMay not performed in young childActivated charcoal for all
cases (1 g/kg)Additional dose after hrs is reasonable (0.5
g/kg)Monitor ileus induced complications
Managements
Conduction delays correctionConduction delays
correctionHypertonic sodium: undefinedHyperventilation: not
effective as single useAlkalinization: most beneficial
Any conduction delay (QRS>100 msec; R aVR3 msec; new
RBBB)Keep pH: 7.50-7.55No evidence for prophylactic useContinuous
use until clinically and EKG improvement, not necessarily
normalizationWatch for complications-fluid, sodium, chloride
Managements
AntidysrhythmicAntidysrhythmicContraindication:
Class IA (quinidine, procainamide, disopyramide)Class IC
(flecainide, propafenone)Class III (amiodarone, bretylium)
[unstudied]
Lidocaine: most commonly usedMagnesium sulfate: not
routinePhysostigmine: not routinePhenytoin: not recommended
used
Managements
All patients should be monitored for 6 hrsAdmission
criteriaAdmission criteria
QRS > 100msec, cardiac dysrhythmias, altered mental status,
seizures, respiratory depression, hypotension within 6 hrs of
ingestion100% sensitive in identifying significant toxicityHR >
120 + QTc > 480 msec: major toxicity
ICU admission criteria is dependantSinus tachycardia may persist
for 1 week
TCA Treatment SummaryConduction DelaysQRS>100 msecRaVR3
mmT40-ms axis >130
NaHCO3:1-2 meq/kg IV bolus at 3-5 min intervals to reverse the
abnormality or to a target serum pH no greater than 7.55
Controlled ventilation (if clinically indicated for
hypoventilation)
DysrhythmiasSinus tachycardiaWide QRS Tachycardia/VT
Torsades de pointes
No treatmentNaHCO3: 1-2 meq/kg IV bolus at 3-5 min intervals to
reverse the
abnormality or to a target serum pH no greater than 7.55Correct
hypoxia, acidosis, hypotensionConsider lidocaine: 1mg/kg IV bolus
followed by infusion of 20-50
g/kg/minConsider hypertonic saline(3% NaCl)Consider magnesium
sulfate 25-50 mg/kg (Max 2g) IV for 2 minControlled ventilation (if
clinically indicated for hypoventilation)Magnesium sulfateOverdrive
pacing
-
TCA Treatment SummaryHypotension Isotonic saline (0.9% NaCl)
boluses (up to 30 mL/kg)
Correct hypoxia, acidosisNaHCO3: 1-2 meq/kg IV bolus at 3-5 min
intervals to reverse the
abnormality or to a target serum pH no greater than 7.50-
7.55NorepinephrineConsider extracorporeal mechanical circulation
(ECMO,
cardiopulmonary bypass)
Seizures Benzodiazepines, propofolSecure airway with intubation
if necessaryCorrect hypoxia, acidosisBarbituratesContinuous
infusion of midazolam or propofol if barbiturates failConsider
neuromuscular paralysis/general anesthesia if all other
measures fail
Sedative-Hypnotics
History
Bromide, the first available sedative-hypnotics agent in 1853The
barbiturates were introduced in 1903Chlordiazepoxide, the first
commercially available benzodiazepines was synthesized in 1955 and
marketed in 1960.Zolpidem, zaleplon and eszoplicone have replaced
BZDs recently
Pharmacokinetics
Most sedative-hypnotics are rapidly absorbed in GI tractMost
drugs are eliminated by hepatic metabolismBut phenobarbital can be
eliminated increased from kidney by urine alkalization
Sedative-hypnotics
Targets of Toxicity
Body Componets Primary Targets
Airway
Breathing X
Cardiovascular
Disability (nervous system) X
Elimination (Liver &kindney)
Sedative-hypnotics Toxidrome
Coma with normal vital signs
Vital Signs Pupil
Bow
elA
ctivity
SkinBP P R T Mental Status
/ Depressed
-
Clinical clue for Sedative-hypnotics overdose
Clinical signs Sedative-HypnoticsHypothermia Barbiturates,
bromides, ethchlorvynolUnique odors Chloral hydrate,
ethchlorvynolCardiac dysrhythmias Meprobamatebradycardia
GHBtachydysrhythmias Chloral hydrate
Muscular twitching GHB, methaqualone, propofol,
etomidateAcneiform rash BromidesFluctuation coma Glutethimide,
meprobamateGI bleeding Chloral hydrate, methaqualoneDiscolored
urine Propofol (green/pink)Anticholinergic signs Glutethimide
Diagnostic Evaluation
Not all BZDs are detected by screen test
Poisoning Treatment Paradigm
A=Alter absorptionGastric lavageActivated charcoal
A=AntidoteFlumazenil for BZD
B=BasicsContinually reassess the patients ABC and treat
accordingly
Poisoning Treatment Paradigm
B=BasicsSupplemental oxygen, respiratory support, and prevention
of aspiration are the cornerstonesVolume expansion 1st and
vasopressor 2nd for hemodynamic instability
C=Change metabolism D=Distribute DifferentlyE=Enhance
Elimination
Not applicable
Antidotes in Detail:Flumazenil
Flumazenil
IndicationsPure BZD overdose in a nontolerant individual who
has
CNS depressionNormal vital signs, including SaO2Normal
ECGOtherwise normal neurologic exam
-
Flumazenil
ContraindicationsPrior seizure history or current treatment of
seizuresHistory of ingestion of a xenobiotic capable of provoking
seizures or cardiac dysrhythmiasLong term use of benzodiazepinesECG
evidence of cyclic antidepressantsAbnormal vital signs; hypoxia
Flumazenil
DosageSlow IV titration (0.1 mg/min ) to a total dose 1mg.
Onset 1-2 min
Half life53 min
Mechanism of ActionA competitive benzodiazepine receptor
antagonist
Serotonin Reuptake Inhibitors Intoxication
History & Epidemiology
Serotonin reuptake inhibitors:Citalopram, escitalopram,
fluoxetine, luvoxamine, paroxetine, sertraline-lopramine;
-xetine
Atypical antidepressant:Venlafaxine, Reboxetine,bupropion,
trazodone
1980s, first-line therapy for depressionOCD, panic disorder,
alcoholism, obesity, migraine headache, chronic painSafer than
TCAs, MAOIs when overdose
Acute Overdose
Nausea, vomiting, dizziness, blurred vision, depression and
sinus tachycardiaSeizure, QRS complex prolongation,
life-threatening effects
Rarely occur even after large overdosesCitaloparam/escitalopram:
QTc widening and seizure in dose-related; >600 mg
-
Managements
Largely supportiveOrogastric lavage is not generally indicated
due to rarely lifethreateningOral activated charcoal
(1g/kg)Citalopram or escitalopram: 24hrs monitorSmall ingestion can
be observed at home
Libby Zion Law
Serotonin SyndromeSerotonin Syndrome
Syndrome v.s. ToxicityClinical triad
Mental-status changesAutonomic hyperactivityNeuromuscular
abnormalities
Combined serotonergic drug overdose (SSRI and MAOI)Single
serotonergic drug overdose (Ecstasy)
Drugs that Can Produce SSDrugs that Can Produce SSNEUROLOGIC
EMERGENCY
Mechanism of Action Related Drugs
Increased serotonin synthesis L-tryptophan
Decreased serotonin breakdown MAOIs(including linezolide),
ritonavir
Increased serotonin release Amphetamines, MDMA, cocaine,
Fenfluramine
Decreased serotonin reuptake SSRIs, TCAs, dextromethorphan,
meperidine, fentanyl, tramadol
Serotonin receptor agonists Lithium, sumitriptan, buspirone,
LSD
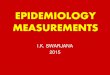
PathophysiologyPathophysiologyNEUROLOGIC EMERGENCY
Boyer, N Engl J Med 2005
-
Boyer, NEJM 2005
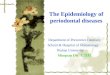
Clinical Findings of SSClinical Findings of SS
Boyer, N Engl J Med 2005
Spectrum of FindingsSpectrum of Findings
Boyer, N Engl J Med 2005
Algorithm for SS DiagnosisAlgorithm for SS Diagnosis
Boyer, NEJM 2005
ManagementManagement
Removal of the precipitating drugsThe provision of supportive
care
IVF and correct vital signs The control of agitation
Give BZD, avoid physical strainThe administration of 5-HT2A
antagonistsThe control of autonomic instability
Use NE, Epi, avoid dopamine for hypotensionShort-acting agents
(nitroprusside/esmolol) for HTN
The control of hyperthermiaUse NDMBs, avoid succinylcholine
ManagementManagement
Administration of 5-HT2A antagonistsCyproheptadine
Oral form onlyInitial dose 12mg, followed by 2mg q2hMaintenance
dose 8mg q6h
-
ManagementManagement
Severity Clinical Presentation Supportive care Interventions
Mild Hyperreflexia and tremor but no feverABCs, removal of the
precipitating drugs Benzodiazepines
Moderate ABCs, removal of the precipitating
drugsBenzodiazepines5-HT2A antagonists
Severe BT>41C ABCs, removal of the precipitating drugs
Benzodiazepines5-HT2A antagonistsNeuromuscular
paralysisIntubation
Antipsychotics
History & Epidemiology
AntipsychoticsMajor tranquilizersNeuroleptics
Introduction of chlorpromazine in 1950, dramatically reduced the
symptoms of schizophrenia.Atypical antipsychotic
ClozapineSynthesized in 1959, but be used until early 1970sFree
of EPS, improvement of negative symptoms of
schizophreniaArgaulocytosis
Clinical Manifestations
AntipsychoticsAcute Overdose
Targets of Toxicity
Body Componets Primary Targets
Airway
Breathing
Cardiovascular X
Disability (nervous system) X
Elimination (Liver &kindney)
-
Antipsychotics OverdoseToxidromes
CNSSomnolence to frank coma
CVTachycardia, hypotension
Anticholinergic manifestations
Diagnostic Evaluation
Hx+PEEKG
Similar to TCA toxicityWide ES, rightward deflection of terminal
40 msec of the QRS in aVR, QTc prolongation
Poisoning Treatment Paradigm
A=Alter absorptionActivated charcoal
A=AntidoteNone
B=BasicsContinually reassess the patients ABC and treat
accordinglyHypotension
NSPreferred NE or phenylephrine over dopamine
Poisoning Treatment Paradigm
B=BasicsVentricular dysrhythmias or QRS >0.12 sec
1st line Sod. Bicarbonate 1-2 mEq/kg, avoid hypoK2nd line
lidocaineIV MgSO4 for TdP
SeizureIV BZD
Central antimuscarinic syndromephysostigmine
C=Change metabolism D=Distribute DifferentlyE=Enhance
Elimination
Not applicable
NeurolepticNeuroleptic Malignant SyndromeMalignant Syndrome
NMS is a rare idiosyncratic reactionTypically occurring in
persons taking neurolepticsor after the sudden withdrawal of
dopamine agonists.
Most NMS cases begin to appear 24 to 72 hours after the onset of
drug therapy, almost are apparent in the first 2 weeks of drug
therapy.The prevalence of NMS is between 0.02% and 2.44% for
patients taking neuroleptics
Drugs Implicated in NMSDrugs Implicated in NMS
Ongoing Drug intake
Antipsychotic agentButyrophenones (eg, Haloperidol),
phenothiazines, clozapine, olanzapine, respiradone
Antiemetic agent Metoclopramide, droperidol,
prochlorperazine
Discontinued Drug Intake
Dopaminergic drug Amantidine, bromocriptine, levodopa
-
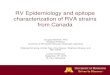
NMS NMS PathophysiologyPathophysiology
Strawn, Am J Psychiatry 2007
NMS Clinical FeaturesNMS Clinical Features
4 clinical syndromeHyperthermia
The key diagnostic featuresAltered mental status
Delirium, somnolence, coma, and mutismSkeletal muscle
rigidity
Lead-pipe rigidityAutonomic dysfunction
Tachycardia, hyper- or hypotension, and diaphoresis
NMS Laboratory StudyNMS Laboratory Study
CPK level should be higher than 1000 U/LLeukocytosis with left
shiftLow serum iron
NMS DSMNMS DSM--IV CriteriaIV Criteria
A. The development of severe muscle rigidity and elevated
temperature associated with the use of neuroleptic medication.
B. Two (or more) of the
following:DiaphoresisDysphagiaTremorIncontinenceChanges in level of
consciousness ranging from confusion to
comaMutismTachycardiaElevated or labile blood
pressureLeucocytosislaboratory evidence of muscle injury (e.g.,
elevated CPK)
C. The symptoms in Criteria A and B are not due to another
substance (e.g., phencyclidine) or a neurological or other general
medicalcondition (e.g., viral encephalitis).
D. The symptoms in Criteria A and B are not better accounted for
by a mental disorder (e.g., Mood Disorder With Catatonic
Features).
NMS ManagementNMS Management
Immediate removal of the offending drug.Supportive therapy is
the key of treatment. BenzodiazepinesDopaminergic
AgentsDantrolene
NMS ManagementNMS Management
Dopaminergic AgentsBromocriptine
Oral form5 to 20 mg q6hSide effects: hypotension, dyskinesia,
erythematous, tender lower extremitiesOther agents:
carbidopa/levodopa, L-dopa, amantadine
-
NMS ManagementNMS Management
DantroleneSingle dose of 2-3mg/kg/day, increases to a total dose
of 10 mg/kg/day IVOral dantrolene 50 to 200 mg daily in divided
dosed every 6 to 8 hoursSide effects: hepatic toxicity
Features differentiating SS and NMSFeatures differentiating SS
and NMS
Serotonin syndrome NMS
Etiology Serotonergic drugs Neuroleptics
Pathophysiology Serotonin excess (toxicity) Idiosyncratic
reaction
Onset Rapid onset and progression Slow onset and
progression
Prominent symptoms
Hyperkinesia and hyperreflexia / clonus Bradykinesia
Rigidity Pyramidal rigidity, terminal development
Extrapyramidalrigidity, a prodromal
symptom
Whyte, Medical Toxicology, 3rd ed.