Embed Size (px)
Citation preview

HURAPRIM
WP7- REPORT
Ahfad University for Women

1
Table of Contents
Abbreviation ……………………………………………………………………………………..…2
Acknowlege …………………………………………………………………………….……...…..3
Chapter 1 Introduction………………………………………………………..………….…….4
Chapter 2 Methodology………………………………………………………………….…...10
Chapter 3 Results………………………………………………………………………………...14
Chapter 4 Discussion……………………………………………………………………….……20
Africa Wide Policy Recommendations……………………………………………….….24
References…………………………………………………………………………………………...26
Tables……………………………………………………………………………………………….….27
(Appendix I………………………………………………………………………………….……….37
(Appendix II…………………………………………………………………………………..…….39
(Appendix III………………………………………………………………………………….…....43
(Appendix IV………………………………………………………………………………….….….46

2
Abbreviation
AHS Academy of Health Sciences
AUW Ahfad University for Women
BHU Basic Health Unit
BSc Bachelor degree of Sciences
CH Credit Hours
CPD Continuous Professional Development
EMRO Eastern Mediterranean Regional Office
FGD Focus Group Discussion
FMOH Federal Ministry of Health
FYS Final Year Students
GP General Practitioner
HC Health Centre
HCW Health Care Workers
HF Health Facility
HP Health Provider
HRH Human Resource for Health
HWF Health Work Force
IDP Internally Displaced People
MHE Ministry of Higher Education
MSc Master Degree of Sciences
NHRHO National Human Resources for Health Observatory
PHC Primary Health Care
RH Rural Hospital
RS Republic of Sudan
RN River Nile
SMOH State Ministry of Health
SPSS Statistical Package of Social Science
WHA World Health Assembly
WHO World Health Organization

3
Acknowledgment
Special thanks and acknowledgment for the following partners who provided timely needed
support before, during and after the data collection process:-
� Federal Ministry of health
� State Ministries of Health in River Nile, Kassala and Sinnar.
� Primary health Care units at SMOH in River Nile, Kassala and Sinnar.
� Academies of health sciences in River Nile, Kassala and Sinnar.
� Registrars and Dean of academies of Health Sciences in River Nile, Kassala and Sinnar.
� School of Health Sciences/AUW
� School of Management/AUW
� Administration and Finance unit/AUW
Also our thanks to the Final Year Students in the three AHS in the three states, health providers
and the users, without their cooperation this study would not have been completed.
The research leading to these results was done in the framework of the HURAPRIM project
which received funding from the European Union’s Seventh Framework Programme (FP7 –
AFRICA-2010) under grant agreement no. 265727.

4
Chapter 1
Introduction
1.1 Introduction:
The Republic of Sudan (RS) covers an area of approximately 1.8 million square km and has a
total population of approximately 33 million. It borders seven countries, Egypt and Libya in the
North, Chad and Central African Republic in the west, Republic of South Sudan in the South and
Ethiopia and Eretria in the East. The capital of the RS is Khartoum, located at the confluence of
the Blue and White Niles. Arabic is the official language of the nation, in addition to other
languages, as well as many dialects.
In 1994 the country was reorganized into 15Wilayaat (states) which are currently 18 states
comprised of 184 localities. Approximately 60% of the population either live in rural areas or are
nomadic. Due to unrest in West Sudan large numbers are now Internally Displaced People (IDP)
which adds to the complexities of internal migration in the RS. On the other hand emigration of
skilled professionals from RS is a significant problem leading to a continuing brain drain
(FMOH, 2005).
1.2. Current health system structure in Sudan:
Since 2005 the health system became a three-tier system having three levels, federal, state and
locality. The federal level is concerned with policy making, planning, supervision, co-
ordination, international relations and partnership. At state level, governments are empowered
for planning, policy making and implementation; while the localities are concerned mostly with
policy implementation and service delivery including health, education, and development
(FMOH, 2008). All states have similar administrative structure as shown in figure 1.

5
Figure (1) The current health system structure. Source: FMOH 2008
1.3Primary health care (PHC) in Sudan:
PHC has been accepted by all WHO member countries as the backbone of efficient health
system and the key to achieving the ambitious goal of health for all. In 2008 the WHO defined
four essential components of PHC (WHR 2008): (i) universal coverage by insuring sufficient
medicines and services; (ii) removing financial barriers to access; (iii) people centered care and
(iv) increasing participation of all stakeholders. PHC was adopted as the key strategy for health
care provision in Sudan since 1978 and re-emphasized in the National Comprehensive Strategy
for Health in 1992-2002 and in the 25-Years Strategic Health Plan 2003-2027.
FMOH Health Facility Description and Renaming Policy defined three components of settings
that provide PHC: Basic Health Unit (BHU), Health Center (HC) and Rural Hospital (RH). The
BHU is structured and staffed to deliver the essential package of PHC services. The HC, headed
by a Family Medicine Specialist, General Practitioner or medical officer, is the first referral level
for the first level facilities. BHU and HC are managed and financed by the localities. Rural
Hospitals serve as secondary referral level health institutions. A 10-year HRH projection plan
was based on the service target approach that aims at provision of a basic health unit for every
5,000 population and a health centre for every 20,000 population in rural area and 50,000 in
urban area and provision of a health facility for population in an area of 5 KM and provision of

6
one rural hospital for every 150,000-250,000 of population by the end of 2027 and maintaining
that ratio.
1.4 Human Resources for Health (HRH) in Sudan:
Although Sudan was a pioneer in Africa in health workforce (HWF) training (the medical
assistants school was established in 1918, midwifery school in 1921, and Khartoum University
School of Medicine in 1924),currentlythe situation of the (HWF) in Sudan is far below the
critical level of 2.5 health care professionals (doctors, nurses, midwives) per 1000 population.
Whether combined for the three professionals or separately, Sudan is still below the critical level,
since the reported rate per 1000 population were 0.22, 0.84, and 0.08 for doctors, nurses and
midwives respectively (WHR, 2006).
In 2008, the total number of health workers in Sudan was 101,453, distributed all over the
country and employed by different sectors beside FMOH. The last years witnessed an increase
number of medical doctors as a result of increasing medical training schools both on the public
and private sectors. In contrast, there is a huge shortage in the paramedic workers with special
regard to the nursing (64000), midwifery staff (17000), and medical assistants and other
paramedics (32000). This has resulted in skill mix mismatch of doctors to nurse ratio of (1.7:1)
in 2006 and is estimated to be 4:1 in 2010 (NHRHO, 2012). Despite the shortage in health
workforce there is progressive migration and specially among physicians to Gulf countries the
United Kingdom and Ireland .
1.5 Intervention Addressing Shortage in HRH: Academy of Health Sciences (AHS):
In order to address this critical HWF shortage, Sudan Declaration 2001 was signed as a joint
initiative between FMOH, MHE and WHO EMRO. The goal was to promote health services
through educational programs and training of the nursing, midwifery and allied health cadres.
Sudan Declaration also called for upgrading the qualification of existing allied health workforce
to Diploma and BSc degrees by the year 2015, by establishing Academies of Health Sciences
(AHS) in all states. The Academy was inaugurated officially on 26th of November 2005. Its
mission is" to scale up production of health personnel including nursing, midwifery and other

7
allied health personnel; through provision of wide-base relevant and quality education to address
the need in Sudan and beyond".
Academic Objectives:
To graduate health personnel who can contribute effectively to the delivery and improvement of
health services; to equip candidates with the necessary knowledge, skills and attitude needed for
standard professional competency and to provide in-service training and CPD activities
necessary to keep health workers abreast of development in health services (DPQ/AHS 2008).
Academic Degrees awarded by AHS:
• Technical Diploma after studying six semesters totaling 90 credit hours(CH) at least,
including theoretical (40%) and practical training ( 60%).
• BSc after studying eight semesters totaling 120 CH; including theoretical and practical training,
40% to 60% respectively.
• Up-grading (Bridging) Old System graduates: Studying four semesters totaling 60 CH
theoretical (40%) and practical training (60%).
Accordingly, all the old training schools and institutes that were affiliated to the FMOH are now
under the umbrella of the AHS, including all the nursing schools, midwifery schools, paramedics
training institutes. Now the AHS has 18 main branches, one in each state with some states having
some other training sites at main cities. The states have the authority to start training programs
according to their identified needs, following the AHS systems. The AHS provide different
programs: Nursing Diploma; General Medical Assistants; Health Inspectors; Public Health
Assistants; Pharmacy Assistants; Laboratory Assistants; Dentist Assistants; Operation Theatre
Attendants;as well as Upgrading (Bridging) Programs in Nursing; Nurse Teachers; Pharmacy;
Anesthesia;Laboratory and Dentistry(DPQ/AHS 2008).

8
1.6Rationale:
According to data available nurses make up the largest group of HWF involved in providing
services at the PHC levels and represents more than 90% of students enrolled in the AHS. In
2008 out of 4960 students enrolled at the Central AHS in Khartoum of whom 3843 (77%) were
registered in The Nursing Diploma Program, while 513(10%) were in the Nurse Bridging
Program and 208(4%) were registered for Nurse Teachers upgrading Program. Among the 2698
students registered in the State Academies 1907(71%) were enrolled in The Nursing Diploma
Program and 87(3.2%) were in the Nurse Bridging Program (DPQ/AHS 2000).This would
hopefully contribute to staff retention in those states.
Sudan Declaration 2001 is a policy measure to enhance and improve training specially nurses
and medical assistants as well as other paramedical needed cadre to overcome the shortage of
HWF and to provide high quality PHC services acceptable and accessible to the community.
Thus WP7aims to explore to what extent this policy measure has been successful. Evaluating the
impact of policy interventions has witnessed progress in methods used but evaluating the impact
of human resources is more difficult. Huicho and coworkers (2010), argue that evaluating the
impact by improvement in health status is complex. The complexity arises because health status
can be influenced by socioeconomic, cultural and health system factorsMoreover such evaluation
need a baseline against which one assesses the results.
However in this study we did not develop, plan and implement the intervention but we
intervened at a point in time to attempt evaluating the Policy Initiative and Measure that took
place in the different states.
1.7Conceptual Framework:
In this study the conceptual framework is comprised of four steps: Policy Initiative and
implementation; Outputs; Outcomes and Impact.The evaluation of the Policy Initiative will
identify to what extent the establishment of AHS and its branches was relevant to the needs and
expectations in context of the health system by conducting a situation analysis. As for
implementation the evaluation will look into the education and training and choices of Final Year
undergraduate students to work in PHC settings (Specific Objective one -SO1). The evaluation

9
of outputs will look at the direct effect on HCW such as engagement, duration of service and stay
and stability in the locality as well as satisfaction with their functions and responsibilities.
(Specific Objective Two-SO2). It will also look into their performance covering the following
dimensions such as availability, competence, responsiveness and productivity.The evaluation of
outcome will also look at coverage and utilization as well as users satisfaction (Specific
Objective Three-SO3).
1.8 Goal:-
To measure the impact of recent policy initiative (establishment of AHS 2005) in promoting
PHC in Sudan
1.9 Specific Objectives:-
1-To identify choices of AHS final year nurse and medical assistant students
2-To measure satisfaction of nurse and medical assistantgraduates with their functions and
responsibilities
3-To measure the satisfaction of users of skill mix at the different health units.

10
Chapter 2
Methodology
2.1 Study Design:-
This study is a descriptive comparative study between Academies of Health Sciences in three
states in Sudan during the period of April 2013 to October 2014. The methodology includes both
quantitative and qualitative tools.
2.2 Study Settings:-
The 18 states of Sudan were divided into six regions in the first stage: Northern region (Northern
and River Nile states); Eastern region (Gedaref, Kassala and Red Sea States); Central region
(Gezira, Sinnar, Blue Nile and Whit Nile States); Kordofan region (North, South and West
Kordofan states); Darfur region (West, South, North, Central and East Darfur) and Khartoum
region. The Kordofan and Darfur regions were excluded for logistic reasons and Khartoum was
also excluded because it is the capital of the country (where the AHS has different settings and
will not be represented. Thus three regions (Northern, Central and Eastern) were included in the
second stage and from each region one state was selected for convenience and logistic reason;
River Nile representing Northern region; Kassala representing Eastern region; and Sinnar
representing Central region. Each state is divided into localities i.e. River Nile and Sinnar have 7
localities each while Kassala has 11 localities. The locality which houses the AHS was selected
for the study, Atbara, Kassala and Singa representing River Nile, Kassala and Sinnar States
respectively. In each locality any public PHC facility (basic health units, health centres and rural
hospitals) functioning for at least one year with defined catchment areas was selected in the
study.
2.3 Instruments:-
2.3.1 Quantitative: - For each of the specific objectives 1-3 a questionnaire was developed.The
first questionnaire targeted the final year students’ of nursing and medical assistants at Academy
of health sciences in selected localities in order to identify the choices available for those

11
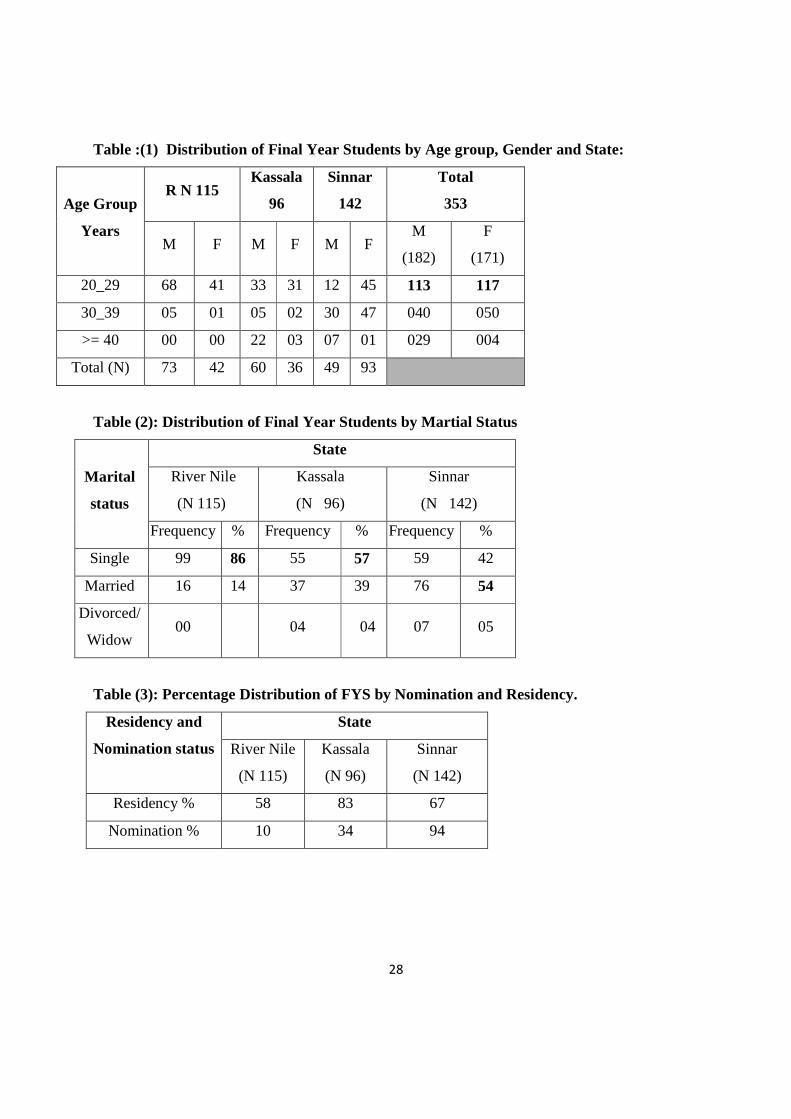
graduate (SO1)(Appendix I). The second questionnaire addressed (SO2)(Appendix II) the health
providers in the public PHC settings to measure their satisfaction with their functions and
responsibilities and to describe the performance of nurses and medical assistants. The third
questionnaire targeted the users of the services in the selected localities to measure their
satisfaction of the skill mix at the different health settings (SO3). The questionnaire covered the
demographic data of users and asked about the number of visits, reasons for visiting and the
provider. There were nine questions (Q11-19) that addressed satisfaction directly. Two questions
asked about waiting and consultation time, five questions were related to management asking the
user if he/she was treated with respect, managed appropriately, participated in decisions and
given satisfactory explanation and if he/she was satisfied with the provider efficiency. There was
a final question about the overall satisfaction (AppendixIII). All three questionnaires were
previously validated, translatedinto Arabic and tested in a pilot trial at Umbada locality in
Khartoum State. Modifications following the pilot trial were introduced as required.
2.3.2 Qualitative: - Three Focus Group Discussions (FGD) was conducted in each state. Two
FGD targeted separately women and men users in addition to a FGD that was held with
community leaders. There were guidelines for the discussion, which covered 13 areas (Appendix
IV).Structured interviews were conducted with registrars or/and directors in the three selected
AHS.
2.4 Study Population:-
All final year students of Nursing and Medical Assistant programs in each of the three AHS were
included in the study. All health providers (HP) ,nurses and medical assistants, working for at
least 6 months in the public PHC facilities in the locality were included. Any user of public PHC
facilities aged 20 years and above and who visited the PHC facilities at least two times during
the last 6 months and was living in the same catchment area and present at the PHC setting
during the study period was eligible for inclusion.
For FGD eight users aged 20 - 60 years old from different educational and social backgrounds
were selected and included in the discussion. There was one group of women users and one
group of men users in each state. The FGD for community leaders was mixed and members of
both sexes were included.

12
2.5 Data Collection:-
The data collection team was composed of graduates of Ahfad University for Women (AUW) as
follows; one team leader (MSc. Holder) and field supervisor (MSc. Holder) in addition to four
members (BSc. Holders). The data collectors participated in three days training workshop for
data collection of each specific objective, focus group discussion and team work. To maintain the
quality of data the six members of the team took part in data collection in two states (River Nile
and Kassala), while four took part in data collection in Sinnar and new two members (after
training) were added to the team.
2.6. Ethical consideration:-
The research proposal and tools were approved by the AUW Institutional Review Board and also
approved by the National Directorate of the AHS, the administration of AHS in the three states
and Directors of the PHC in each state and locality. A statement in Arabic was read by the
interviewer before administering the questionnaire. It explained the aim and objectives of the
research and emphasized confidentiality of all information as well as the right to refuse or
withdraw without any after effects. Witnessed verbal consent was granted from the FYS, the
health providers and users before administering the questionnaire. Also witnessed verbal consent
was obtained from all members who attended the FGD at the different states.
2.7 Data Management:-
2.7.1 Quantitative: - The team leader and field supervisor prepared the data coding sheets for
each specific objective’ tools while the rest of the group completed the data entry. Afterword the
data cleaning was carried out by the statistical team under supervision of a statistician. Moreover
the statistician took a random sample of 10% and rechecked it. Finally the statistical analysis was
conducted using SPSS version 16.0.
2.7.2 Qualitative:-
For each FGD there was a leader who conducted the discussion, one member recorded the
discussion and one member took hand written notes. The discussions were held in Arabic. The
structured interviews of registrars and/or directors were conducted by the team leader in Arabic.

13
All records and notes were transcribed into Arabic revised by the three researchers and then
translated into English.
2.8 Challenges and Constrains: -
1. There was great delay in response in writing from stakeholders and the Research Team
has to arrange for personal visits and meetings to discuss pertinent issues. This resulted in
untimely delay.
2. All members of the team were females and from outside the states, arrangements for
travel, lodging etc. were rigorously undertaken but still sometimes they have to travel
long distances to reach the different PHC settings.
3. In the middle of the study, there was the fasting month (Ramadan) and we have to stop all
activities and restart after Ramadan and the festivities.
4. During July and August the rainy season was very heavy which added to the delay in data
collection in one state (Sinnar).
5. FGD in Kassala for community leaders was not held. Kassala state has 11 localities , one
of them is Kassala city which houses the AHS. The key person had difficulty in
identifying the community leaders due to different political and tribal issues.Also the
period of data collection was fixed and the team has to return to Khartoum.

14
Chapter 3
Results
The study was conducted in three periods: - the River Nile was covered during the period (1-10
June 2014); Kassala during the period (11-18 June 2014) and Sinnar during the period (18-23
August) due to delay arising from the rainy season and fasting month (Ramadan).
3.1 Education, training and choices of FYS, Nurses and Medical Assistants (SO1):-
In total there were 389 FYS in the 3 AHS: 132 in RN, 102 in Kassala and 155 in Sinnar.Of these
353 students were administered the questionnaire i.e. a response rate (RR) of 91%. In River Nile
115 students responded (RR of 87%) while 94 students responded in Kassala (RR 94%) and 142
in Sinnar (RR 92%). The 46 students who did not participate in the questionnaire were absent
from AHS at the time of the survey.
3.1.1 Demographic characteristics of the participants:-
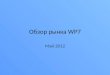
Males represented 52% of the 353 total of students but they represented 63%, 62% and 35% in
RN, Kassala and Sinnar respectively (Table 1). Among the males 62% were aged (20-29 years)
as compared to 68% among the females but it represented 93% ,55% and 24% among males in
RN, Kassala and Sinnar respectively as compared to 97%, 86% and 48% among females in RN,
Kassala and Sinnar respectively. The cohort of graduates in RN was younger and this might be
due to the fact that only 10% were nominated by the local government or other governmental
institutions. The majority of students in RN were single (86%) as compared to 57%in Kassala
and 42% in Sinnar(Table 2).
In Kassala 83% of students were from the same locality as compared to 67% and 58% in Sinnar
and RN respectively. The nominated students represented 94% of the FYS in Sinnar as compared
to 34% in Kassala and only 10% in RN(Table 3).
3.1.2 Choices of FYS, Nurses and Medical Assistants to work in PHC settings
The majority of the FYS (95%) in Kassala preferred to work in PHC settings after graduation as
compared to 79% and 72% in Sinnar and RN respectively(Table 4).
3.1.3Structured Interviews: Three registrars and two directors were interviewed on the basis of
set criteria addressing admission, curriculum, methods of teaching and assessment.

15
a)Duration of study: All three AHS offered 3 years (6 semesters) program granting Diploma in
Nursing and General Medical Assistant Diploma.
b)Admission requirements:The admissionrequirements were similar in all three states (Birth
certificate, Sudanese secondary school certificate, National identity number, completed
application form)supported by nomination from the locality or direct application. Applicant must
pass either written or oral examination in general knowledge.
c)Core competences:The main core competences for nurses that were mentioned by AHS’
registrars in the three states were ability to providenursing care: in emergency room, for
different internal diseases, for different paediatric diseases, in different specialized units and for
obstetrics and gynecology cases.
d)Teaching and learning methods: The three AHS use variable methods of teaching and
evaluationincluding visualized lectures, power point presentations, group discussions and
tutorials. Supervised practical and clinical training is offered in all three AHS.
e)Student Assessment:Continuous evaluation (mainly periodic tests) as well as formative is
applied in the three academies.
3.2 Satisfactions and Performance of Nurses and Medical Assistants as Health Providers
(SO2):
3.2.1 Characteristics of HP:
There were 82 (HP) in the three states, 27 in RN, 39 in Kassala and 16 in Sinnar. Of these 51
were nurses and 31 were medical assistants.Among the 82 HP there were 31 graduates of AHS
comprised of 18 nurses and 13 MA.(Table 5)
There were 39PHC settings in the three statescomprisedof three rural hospitals, one in each state,
and 36 health centers twelve in R, nineteen in Kassala and five in Sinnar. The 31 AHS graduates
were distributed among the three rural hospitals, and 17 HCs( Table 5).
Approximately all 82HP were living adjacent to the health settings, 100% in RN and Sinnar and
79% in Kassala(Table 6).Out of the total 82 HP 51(62%) were working for four years and more
but represented 81%, 70% and 49% in Sinnar, RN and Kassala respectively (Table 7).

16
3.2.2 Satisfaction of Health Providers:
There were seven questions (Q31-37) that aimed to measure satisfaction of HP with their roles
and responsibilities (Appendix II). Of these questions (Q31)addressedworkload and functions
and (Q37) asked about assigned responsibilities. Two questions (Q32, Q33) asked about
methods of supervision and communication with supervisor , while (Q34) addressed payment
and benefits .Question 35 asked about satisfaction with relationship with colleagues and (Q36)
asked about satisfaction with relationship with patients.
Satisfaction rate of HP with their workload and functions was 85% in RN as compared to 90%
in Kassala and 94% in Sinnar. Their satisfaction rate bout their roles and responsibilities was
82% in RN and 92% and 100% in Kassala and Sinnar respectively (Table 8). The satisfaction
rate about methods of supervision was 89% in R.N , 95% in Kassala and 100% in Sinnar. HP
were highly satisfied about the communication with supervisors ranging from 95% in Kassala,
to 96% in R.N and 100% in Sinnar. But when asked about payment and benefits the response
rate varied, since only 59% in Kassala were satisfied, as compared to 63% in RN and 94% in
Sinnar. However when asked about their relationship with colleagues they were highly satisfied
in the three states and the rate of satisfaction was 97% in Kassala and 100% in both RN and
Sinnar. They were very highly satisfied with their relationship with patients since the
satisfaction rate was 100% in all three states (Table 8).When asked if they will continue in their
current jobs 100%, 92% and 89% in Sinnar, Kassala and RN respectively said yes (Table 9).
Unavailability of working materials and unavailability of water and electricity were the most
reported factors that negatively affected the performance of the health providers across the states.
Other factors were lack of transportation, shortage of staff and the deteriorating physical
condition of the working setting (Table 10). Also a number of suggestions were proposed to
improve work such as educational courses and structured training, improving the physical
working environment and providing psychological and financial support.
3.3 UsersSatisfaction(SO3) :-
3.3.1 Characteristics of the Participants:
A total of 336 users were interviewed, 152 in RN, 122 in Kassala and 62 in Sinnar. Of these 295
(88%) were visiting HC, 37 (11%) visiting RH and 4 (1%) visiting BHU (Table 11). The
majority of users 215 (64%) were in the age group20-39 years old and the remainder 121(36%)

17
were aged 40 years and above. Predominantly they were females 242 (72%) and the overall were
married 272 (81%). As for education levels 184 users (55%) had primary and secondary
education, while 84 (25%) were illiterate and 68 (20%) were university graduates. But there were
differences between states since university graduates represented 37% in RN as compared to
11% and 4% in Sinnar and Kassala respectively. Illiteracy among users was highest in Kassala
(44%) as compared to 18% and 13% in Sinnar and RN respectively (Table 12). The majority of
overall users were housewives 186 (55%), as compared to 42% in RN, 45% in Sinnar and 77%
in Kassala(Table 13)
Among the overall users 44% visited the health facility five times and more, while 22% visited
3-4 times and 35% visited less than three times. The numbers of visits were comparable in the
three states (Table 14). The reasons for visiting the PHC facilities were almost the same across
the three states, the majority(47%) visit as patients or co-patients(37%) while 5% come for
antenatal follow up and the remainder (11%) come for other reasons such as vaccination
renewing prescription and regular medical checkup.
3.3.2 User Satisfaction:
There were nine questions (Q11-19) (Appendix III) that addressed satisfaction of users directly.
Those users who considered waiting time was very short or short or enough were considered
satisfied and the rate of satisfaction was 68%,67% and 50% in RN, Kassala and Sinnar
respectively(Table 15). There was high rate of satisfaction with consultation time, 93% in
RN,97% in Sinnar and 100% in Kassala. The rate of satisfaction of users with management,
treatment with respect, participation in decision and with provider efficiency was very high
ranging from 91% to 100% in the three states. The rate of overall satisfaction with services
provided was 96% in RN and 98% in both Kassala and Sinnar (Table 15)
When the gender and educational level of users were cross-tabulated with satisfaction level, there
was no significant difference between males and females. However all illiterate users in the three
states were 100% satisfied, while among the other three educational levels the satisfaction was
very high ranging from 90% to 100% (Table 16). It seems that the educational level did not
affect the user’s satisfaction.

18
3.3.3 Focus Group Discussions with users:-
Six FGD were conducted for users, two in each state of which one was attended by women and
the other by men. Each group was comprised of eight members selected from the catchment area
of PHC setting adjacent to the PHC setting and were regular users. The discussion focused on the
following ten areas: frequency of visits to HC, reasons for visiting, satisfaction with accessibility,
number and reasons of visiting the HC; and satisfaction with services provided by nurses and
medical assistants such as receiving appropriate management, explanation and support as well as
their competence. Issues related to waiting and consultation time were also raised.The groups
confirmed that they regularly visit the HC: the number of visits varied from three to six visits and
peaked in certain seasons such as harvest season in Kassala.
Malaria and respiratory infections were the most common reasons for visiting followed by
hypertension and diabetes. In RN state kidney diseases, urinary tract infection and immunization
were mentioned, and in Sinnar fever and diarrheas and in Kassala tuberculosis and typhoid were
mentioned.
All groups in the three states agreed that HP , nurses and medical assistants treat patients with
respect and decency, and the women groups in RN and Kassala added that the Academy
graduates have a sense of humanity. Women and men groups in RN and Kassala agreed that the
HP do not explain sufficiently but they only write the disease and medication except in case of
diabetes and other chronic diseases they offer some explanation. While in Sinnar both groups
agreed that the HP provide the required information. Both groups in Sinnar and Kassala agreed
that the HP is qualified and efficient but sometimes they requested the wrong investigations.
Women groups in RN and Kassala as well as men groups in Sinnar and Kassala agreed that the
HP provided emotional support to patients. Waiting time to meet the HP was between 10 to 15
minutes for women in RN and Sinnar and about three hours in Kassala. All male members in the
FGD in River Nile were satisfied with the waiting time, while the males of FGD groups in Sinnar
and Kassala said that the waiting time was too long.

19
3.3.4 FGD with Community Leaders:
Only two FGD were held , one in RN and one in Sinnar. Due to logistics and time it was not
possible to hold a FGD in Kassala. The groups were mixed comprised of eight persons ,five
males and three females.
In RN the group said they visit the HC periodically and mainly for diabetes and hypertension,
while in Sinnar they visit regularly and the number of visits is six and more and for different
reasons. Both groups agreed that HP provide required information in specific problems but in
general they lack experience, since they only prescribe treatment to relieve pain but not to treat
the condition. Waiting time was considered satisfactory for the two groups.Consultation time
ranged from 5 to 10 minutes and the community leaders in Sinnar were satisfied with the time
and they think it is enough to get answers for all of patient’ questions.

20
Chapter 4
Discussion:
4.1 Human Resources in African PHC:
Africa has 24% of the global health burden but only 3% of health workers (2.3 health workers
per 1000 population vs. 9.3 per 1000 population globally) commanding less than 1% of world
health expenditure(WHO,2006).Training of health workers is elitist, hospital-focused and not
appropriately equipping health workers for PHC. Shortages are exacerbated by high migration
due to poor salaries, poor working conditions, poor professional development, and unclear career
pathway. The First Global Forum on HR for Health in 2008 recognised the global shortage and
recommended that governments determine appropriate health workforce skills mix and to
institute coordinated policies, (WHO,2008)
The sixty-second WHA in 2009 urged countries “to train and retain adequate numbers of health
workers, with appropriate skill mix, including PHC nurses, midwives, allied health professionals
and family physicians, able to work in a multidisciplinary context, in cooperation with non-
professional community health workers in order to respond effectively to peoples health needs.
Unfortunately the pace of training is such that it would take 36 years for physicians and 29 years
for nurses and midwives to reach WHO’s target of 2.28 professionals per 1000 population for
African countries (Kinfu, 2009).
A systematic review of the effectiveness of PC nursing(Keleher H. et.al.,2009)reviewed 31
relevant studies in an attempt to answer the research question:"What is the impact of the primary
and community care nurse on patient care outcomes compared with usual doctor-led care in PC
settings". It was found that nurses in PC settings can provide effective care and achieve positive
health outcomes similar to that provided by doctors. Nurses are also effective in a more diverse
range of roles including chronic diseases management, illness prevention and health promotion.
4.2 Policy Initiative (Sudan Declaration 2001):
In Sudan there is huge shortage in HRH especially in nursing, midwifery, medical assistants and
other allied health cadres. To overcome this shortage a policy initiative known as Sudan

21
Declaration 2001 was signed ant it was put into effect in November 2005.It aimed at promotion
of health services through educational programs and training of nurses, medical assistants,
midwives and other allied health cadres as well as upgrading(bridging) the existing qualifications
to diploma and B Sc degrees. To achieve this AHS was established with branches in all states.
The intervention was implemented in November 2005 and this study attempted to evaluate this
policy intervention.
4.3 Evaluation:
The objectives of this limited study were achieved. The study covered three AHS out of the
existing 15 AHS and they were representative of the different AHS. There were 389 FYS in the
three AHS i.e an average 130 FYS in each AHS, which if the same number is found in the 15
AHS, there will be a total of 1950 FYS in the 15 states and since the programs are three years
programs it is estimated that a total of 5850 students will be enrolled at any time, which will be
a good addition to the HRH pool.
The first objective was to identify choices of final year students.The response rate among the
FYS was high (91%) which strengthens the validityof the results. Overall 81% of FYS preferred
to work in PHC settings in their states after graduation which is a very positive indicator if they
will be incited to remain.This means if extrapolated that 1580 PHC cadre will be added to PHC
facilities. This will also encourage authorities to reevaluate the curricula and training to achieve
the appropriate skill mix as recommended by the Sixty TwoWHA (WHA, 2009).
The second objective was to measure the satisfaction of graduates with their functions and
responsibilities. The study found that the overall majority of HP , nurses and medical assistants,
were highly satisfied with their functions and responsibilities,100% in Sinnar,92% in Kassala
and 89% in RN. They stated that theywill continue in their current jobs. However ,although they
were satisfied with their current functions and responsibilities, a significant proportion ,44% in
Sinnar, 41% in Kassala and 11% in RN, said that their current functions and responsibilities
were not up to their expectations as students . This is an area that needs to be addressed by the
policy makers.

22
The third objective was to measure the satisfaction of users of skill mix at the different health
units. The study found an overall high rate of userssatisfaction with the performance of HP in the
three states 96% in RN and 98% in both Kassala and Sinnar. This was also confirmed by the
FGD with users and all groups, males and female, stated that HP treat their patients with respect
and decency which is greatly needed in PC practice. The Focus Groups in RN and Kassala also
stated that the AHS graduates have a sense of humanity.
4.4 Conclusions:
This policy initiative was successful on the basis of this evaluation of three AHS. The estimated
numbers of FYS and their preference to work in PHC settings after graduation ,fulfills one of the
objectives of the initiative to graduate HCW who can contribute effectively to HC services and
delivery.
4.5 Recommendations:
1-To conduct similar studies in the other 12 AHS which had already graduated students.
2-To compare between formal regular graduates and those who did bridging.
3-To review the curriculum with a view to develop the 60% component of the practicum to attain
competencies and skills that will achieve the needed and recommended skill mix and should
address the curative, preventive and promotive aspects.
4-To develop a system of regular evaluation of community oriented comprehensive practice.
5-To develop a clear framework and career pathway for the HP based on performance and
continuous professional development.

23
4.6 Limitations:
1-Thisevaluation was based on an already implemented intervention. Accordingly certain
indicators were not inbuilt from the start.
2-The study, due to logistics, did not evaluate the curriculum in depth and did not monitor the
delivery of its contents.
3-The study did not conduct an observational evaluation of performance of HP based on a
checklist due to logistics and limitation of funding.
4-The study could not evaluate or estimate the cost of this policy initiative due to many factors
that were out of our reach.

24
4.7:Africa Wide Policy Recommendation:
Health workforce needs-based shortages and skill mix imbalance are significant HCW
challenges. Task shifting ,defined as delegating tasks to existing or new HWFwith either less
training or specifically tailored training is a potential strategy to address these challenges.
Moreover when the skill mix and activities and tasks of each member of the HWF at the PC
settings are not well matched to the local health care needs of the communities being served ,
then health care services become less accessible and when they become accessible they
become less affordable.
The primary objective of task shifting and skill mix is to increase productive efficiency which
results in enhancing and increasing the number and quality of health care services provided
and can lead to increased patient access to better quality services. But it was observed by
(Gupta et .al,2003) that productive skill mix will vary across and within countries because of the
different health care services being provided and because of different contextual factors such
as the health system, payment scheme, workforce training and management culture.
Two case studies from Pakistan and Ethiopia warrant discussion to illustrate the importance of
contextual and enabling factors that can play a role in the skill mix. A review of the Pakistan
Lady Health Worker Program suggests that contextual factors are important in determining the
success or failure of a skill mix policy change (Lehman U. et.al, 2007). There was a high level
political support for the program. The lady health worker had to be a resident of the
community in which she works.She was attached to a government health facility which will
provide her with training, allowance and medical supplies. Those selected have to be
nominated by the community and should have at least eight years of education.
On the other hand the community- based health extension workers within The Health
Extension Program in Ethiopia offers a different experience of the services offered by the health
extension workers in remote areas and the importance of contextual factors (Teklehaimanot A.
et.al.2007).Some of the factors identified include leadership and training, workplace
infrastructure, living conditions and relationship with the community. Although it has a limited
budget it is successful.
The case study of the establishment of the Academy of Health Sciences in all states of Sudan to
train candidates who are nominated by their localities or communities and will go back to work
in PHC settings in the localities that they are residents of, can be a good model to address the
shortage of HCWF in Sub-sahara Africa. It should be recommended.

25
The problems in health policy in developing countries are not "what to do" but rather of
implementation "how to do it".
The implementation depends on contextual factors both across and within countries.
WHO(2008) recommended a series of questions to be addressed:
1-What are the country -specific factors that will guide decision making in the implementation
of task shifting and skill mix?
2-What preconditions should be met for the safe, efficient and effective implementation of task
shifting and skill mix?
3-How can countries create enabling conditions for task shifting through an appropriate
regulatory framework?
4-What measures must be taken to ensure quality of care under task shifting and skill mix
approach?
These questions suggest that skill mix and task allocation and shifting can work.
In conclusion the case study of the AHS as introduced in 2005 and if implemented in other
countries in Africa but in the contextual needs and factors prevailing in each country it can be
productively efficient.

26
References:-
• AHS, Academy of Health Sciences. 2008. The Academy of Health Sciences; Present and
Future Prospects. Vol. 3, 3.
• Directorate of Planning and Quality-Academy of Health Sciences 2008.The Academy of
Health Sciences: Present Situation and Future Prospects. Sudan Journal of Public
Health:3(3);136-139.
• FMOH, Federal ministry of health. 2010. Annual Health Statistical Report. Khartoum: National Health Information Center, 2010.
• FMOH, Federal ministry of health. 2008. Annual Health Statistical Report 2007.Khartoum: National Health Information Center, 2008.
• Gupta N, Diallo K ,Zurn P, DalPoz MR.2003. Assessing human resources for health:What can be learned from labour force surveys? HR for Health, 1(5):
• Kinfu Y,2009. The Health Worker Shortage in Africa. Are enough physicians and nurses being trained. Bul.WHO,87(3):225-230.
• Keleher H, Parker R, Abdulwadus O, Francis K (2009) Systematic Review of the effectiveness of Primary Care Nursing. Int.J. Nurs.Pract.;15(1):16-24.
• Lehmann U, Sanders D.2007.Community Health Workers: what do we know about them The state of Evidence on Programs, Activities, Costs and Impacts on Health Outcomes using Community Health Workers, Geneva, WHO.
• NHRHO, National Human Resources for Health. 2012. National Human Resources for Health Strategy 2012-2016. Directorate General of Human Resources for Health Development. Khartoum: FMOH, NHRHO and WHO, 2012. pp. 1-2.
• Omar, Maya. 2008. Comprehensive training needs assessment in Sudan: Executive action • document. Khartoum. January 2008, Vol. 3, 1. • Sixty Second WHA,2009. Primary Health Care ,Including Health System Strengthening.
Bull. WHO,91(11),892-4. • Teklehaimanot A, Kitaw Y, Yohannes AG et.al. 2007.Study of the Working Conditions
of Health Extension Workers in Ethiopia. Ethiop. J. of H. Develop.,21(3);246-259. • WHO, 2006.Working Together for Health. WHR,2006, Geneva. • WHO ,2008. The Kampala Declaration and Agenda for Global Action. • WHO, 2008. Task Shifting :Global Recommendations and Guidelines. Geneva. • WHO, 2011. http://www.who.int/gho/countries/sdn.pdf. [Online] WHO, April 4, 2011.
[Cited: December 19, 2013.]

27
Tables
28
Table :(1) Distribution of Final Year Students by Age group, Gender and State:
Age Group
Years
R N 115 Kassala
96
Sinnar
142
Total
353
M F M F M F M
(182)
F
(171)
20_29 68 41 33 31 12 45 113 117
30_39 05 01 05 02 30 47 040 050
>= 40 00 00 22 03 07 01 029 004
Total (N) 73 42 60 36 49 93
Table (2): Distribution of Final Year Students by Martial Status
Marital
status
State
River Nile
(N 115)
Kassala
(N 96)
Sinnar
(N 142)
Frequency % Frequency % Frequency %
Single 99 86 55 57 59 42
Married 16 14 37 39 76 54
Divorced/
Widow 00 04 04 07 05
Table (3): Percentage Distribution of FYS by Nomination and Residency.
Residency and
Nomination status
State
River Nile
(N 115)
Kassala
(N 96)
Sinnar
(N 142)
Residency % 58 83 67
Nomination % 10 34 94

29
Table (4) Distribution of FYS by Workplace Preference after Graduation:
Work setting RN (N 115)
%
Kassala (N
96)
%
Sinnar (N
142)
%
Total (N353)
N %
Basic Health Unit 19 15 12 053 15
Health center 19 33 32 100 28
Rural Hospital 34 47 35 133 38
Other 28 5 21 067 20
Table (5): Distribution of Health Providers in the three states:
State
Health providers
Total No
of H.
Facilities
Health
Facilities
with AHS
graduates
All AHS Graduates
Subtotal Nurse M.A RH HC RH HC
River Nile
27
12 7 5 1
12 1
6
Kassala
39 9 2 7
1
19 1
7
Sinnar
16
10
9
1
1
05
1
4
Total
82
31 18 13 3 36 3 17

30
Table (6): Distribution of Health Providers by Residency in the Same Locality
State Residents in the same state
N %
River Nile 27 100
Kassala 31 079
Sinnar 16 100
Table (7): Distribution of 82 Health Providers by Work Experience:
Working period < 1 year
N %
1-3 years
N %
4-5 years
N %
+5 years
N %
River Nile 2 7 6 22 6 22 13 48
Kassala 5 13 15 38 5 13 14 36
Sinnar 0 0 3 19 13 81 - -
Total 7 9 24 29 24 29 27 33

31
Table (8): Percentage Distribution of satisfaction of Health Providers
Table (9): Distribution of H. Providers by willingness to continue in same job:
State Yes
N %
River Nile 24 89
Kassala 36 92
Sinnar 16 100
Table (10): Distribution of HP by Negative Factors that affect their work
State
Unavailability of
working materials
N %
Unavailability of water &
electricity
N %
River Nile 9 33 7 26
Kassala 6 15 10 26
Sinnar 0 0 0 0
State HP
No
Percentage Satisfaction rate
Functions Roles & Responsibilities
Method of supervision
Communication with supervisor
Payment and Benefits
Relationship with
Colleagues
Relationship with Patients
River Nile
27
85
82
89
96
63
100
100
Kassala
39
90
92
95
95
59
97
100
Sinnar
16
94
100
100
100
94
100
100

32
Table (11): Distribution of Users by Type of Health Facility:
Health Facility
State
RN (N152)
N (%)
Kassala (N 122)
N (%)
Sinnar (N 62)
N (%)
Total (N 336)
N (%)
Primary Health
Unit 1 1 0 0 3 5 4 1
Health Center 145 95 104 85 46 74 295 88
Rural Hospital 6 4 18 15 13 21 37 11
Table (12): Distribution of Users by Educational level
Educational
Level
State
River Nile ( N 152)
No %
Kassala ( N 122)
No %
Sinnar ( N 62)
No %
Illiterate 19 13 54 44 11 18
Primary/Elementary 30 20 46 38 29 47
Secondary 47 31 17 14 15 24
University & Higher
Education 56 37 05 04 07 11

33
Table (13): Distribution of Users by Occupation:
Occupation
State
River Nile (N 152)
N (%)
Kassala (N 122)
N (%)
Sinnar (N 62)
N (%)
Total (N 336)
N (%)
Housewife 64 42 94 77 28 45 186 55
Professional/ Semi
professional 35 23 9 7 8 13 52 15
Skilled/ Semi skilled 30 20 7 6 11 18 48 14
Others 23 15 12 10 15 24 50 15
Table (14): Distribution of Users by Number of Visits to Health Facility in 2013:
Number of visits
State
River Nile (N 152)
N (%)
Kassala (N 122)
N (%)
Sinnar (N 62)
N (%)
<3 44 29 52 43 20 32
3-4 35 23 22 18 16 26
>4 73 48 48 39 26 42

34
Table (15): Distribution of Users satisfaction to Specific Indicators:
Indicator
State
River Nile ( 152)
N (%)
Kassala (122)
N (%)
Sinnar ( 62)
N (%)
Waiting Time 103 68 082 67 31 50
Consultation
Time 141 93 122 100 60 97
Treatment with
Respect 151 99 122 100 62 100
Appropriate
Management 139 91 119 98 59 95
Participation in
Decision 145 95 117 96 59 95
Explanation of
Medical
Condition
140 92 118 97 61 98
Provider
efficiency 145 95 121 99 60 97
Receiving
Professional
Advice
148 97 119 98 59 95
Overall
satisfaction with
Services
146 96 120 98 61 98

35
Table (16): Distribution of Overall Users Satisfaction by Gender/ Education Level / State
Education Level
River Nile Kassala Sinnar M (N 56) F (N 96) M (N 17) F (N 105) M (N 21) F (N 41) No % No % No % No % No % No %
Illiterate 06 100
13 100 5 100 49 100 2 100 09 100
Primary (Elementary)
10 90 20 95 4 100 42 98 9 100 20 95
Secondary 17 94
30 100 5 100 12 92 8 100 07 100
University/ Above 23 96
33 94 3 100 02 100 2 100 05 100
Total Satisfied Users
56 95 96 97 17 100 105 98 21 100 41 98

36
Appendices

37
(Appendix I)
Ahfad University for Women
Project: Human Resources for Primary Health Care in Africa - Sudan
SO 1:- To identify choices of AHS final year nurse and medical assistant students
Date ....................................................... Data collectors name: -
..............................................
State .................................................. Locality: .
Type of health facility:-
1- Basic Health Unit.
2- Health Center
3- Rural hospital
Name of the health Facility:-
.........................................
My name is ……………………………., I am from Ahfad University for Women, and one of the
team members to collect data about the human resources for primary health care. The main
objective of this interview is to identify the choices of AHS final year nurse and medical
assistant students. Duration for filling this questionnaire about 10 minutes, all information will
be confidential and for academic use only, the participation is voluntary. Do you want to
participate? 1- Yes 2- No
Section (1) Demographic information:-
1- Sex:- 1- Male 2- Female
2- Age:- How old are you?..............................................................
3- Marital Status:- 1- Single 2- Married
3- Divorced 4- Widow 5- Others …………
4- Education level:- 1- Secondary 2- Diploma
3- University 4- Others ………..
5- Do you have children? 1- Yes 2- No
6- Are you originally from this area? 1- Yes 2- No
Section (2): History for study and work
7- When had you enrolled at the AHS?.............................................
8- Are you nominated to join the AHS? 1- Yes 2- No

38
9- If yes; by whom?
………………………………………………….…………………………………………
10- If no; how did you register at AHS?
……………………………………………………………………………………………
11- Why did you join the AHS?
………………………………………………..…………………………..……………
12- Did you work in any health facilities before joining the AHS? 1- Yes 2- No
13- If yes; where did you work?
1. Rural hospital
2. Health Center
3. Basic Health Unit
4. Other specify …………………………………………………………..
14- Do you know your job discretion? 1- Yes 2- No
15- If yes specify ..........................................................................................................
………………………………………………………………………………………………
……………………………………………………………………………
16. Where are you planning to work after graduation?
1. Rural hospital
2. Health Center
3. Basic Health Unit
4. Other specify …………………………………………………………..
17.Why?……………………………………………………………………………………………
………………………………………………………………………………………
18. Do you prefer to work in other health facilities?
1. Yes 2. No
19. If yes specify ……………………………………………………………………………..
20. Why
………………………………………………………………………………………………………
………………………………………………………………………………………
39
(Appendix II)
Ahfad University for Women
Project: Human Resources for Primary Health Care in Africa - Sudan
SO 2:- (a)To measure satisfaction of graduate with their functions and responsibilities
(b) To evaluate the performance of nurse graduates at PHC settings
Date .................................. ..................... Data collectors name: - ..............................................
State.................................................. Locality:................................................... Type of health facility:-
4- Basic Health Unit. 5- Health Center 6- Rural hospital
Name of the health Facility:-.........................................
My name is ……………………………. I am from Ahfad University for Women, and one of the team members to collect data about the human resources for primary health care. The main objective of this interview is measure the satisfaction of the AHS graduates (nurses and medical assistances) with their functions and responsibility as well as to evaluate their performance at health facility level. Duration for filling this questionnaire is about 25 minutes, all information will be confidential and for academic use only, the participation is voluntary. Do you want to participate? 1- Yes 2- No Section (1) Demographic information:-
1-Sex:- 1- Male 2- Female 2- Age:- How old are you?.............................................................. 3- Civil Status:- 1- Single 2- Married
3- Divorced 4- Widow 5- Others ………… 4-Do you have children? 1- Yes 2- No 5-Education level:- 1- Secondary 2- Diploma
3- University 4- Others ……….. 6Are you originally from this area? 1- Yes 2- No 7-Year of graduation from AHS:- 1- 2010 2- 2011
3- 2012 4- 2013 5- Others …………. Section (2): History of enrollment at the AHS
8-Have you been nominated to join the AHS? 1- Yes 2- No 9-If yes; by whom? ………………………………………………….………………………………………… 10-If no; how did you register at AHS? ………………………………………………………………………………………………… 11-Which AHS you graduated from?

40
………………………………………………..…………………………..……………… 12-How long have you been working in this health facility?
…………………………………………………………………………………………… 13-Since graduation; did you work in any health facilities? 1- Yes 2- No 14-If yes; please specify where?..................................................................................... Section (3) Satisfaction: (A)Working Experience:-
15-How long it takes you to reach your work place?
………………………………………….…………………………………………… 16- What is your working hours per day?
……………………………………………………………….……………………… 17- Do you know your job discretion? 1- Yes 2- No
18- What are your main duties at this health facility ?
……………………………………………………………………………………………………………………………………………………………………………
19- Do you submit regular reports ? 1- Yes 2- No
20- If yes; to whom?.....................................................................................................
21- Is there is any support from the SMOH to facilitate your work? 1- Yes 2- No
22- If yes; what kind of support? ………………………………………………………………………………………
23- Is there is full health team in this health facility? 1- Yes 2- No
24- If yes; how many members?..........................................................................
25- If yes; are you an active member of the team? 1- Yes 2- No
26- If yes; how?………………………………………………………………………..
27- If no; why?..................................................................................................
28- Do you face any difficulties at work? 1- Yes 2- No
29- If yes, what kind of difficulties? ……………………………………………………………………………..……………
30- If Yes how do you handle it?.....................................................................................

41
B) Satisfaction with Roles and Responsibilities:
Please explain to what extend are you satisfied with the following:-
Satisfied Not satisfied If not satisfied; why?
31- Your work loads
32- The way you ar supervised
33- Communication with your supervisor
34- Financial issues
35- Your relation with colleagues
36- Your relation with patients
37- Your responsibilities
38- Do you have equal rights in work promotion? 1- Yes 2- No
39- Do the working environment and work supplies enable you to perform your duties?
1- Yes 2- No
40- Have you been provided with any training or academic courses?
1-Yes 2- No
41- If yes; how many per year?........................................................................................
42- Are your current work duties similar to your expectations when you were a student?
1- Yes 2- No
43- If no, please explain what were your expectations? ……………………………………………………………………………………
44- If you have a second chance to decide; would you choose your current job?
1- Yes 2- No
45- Will you advice your friends and relatives to choose this job?
1- Yes 2- No
46- Do you have an interest to continue in this career? 1- Yes 2- No
47- If yes; why?................................................................................................................
48- If no; why?..............................................................................................................
49- If no, what are your future plans?
..................................................................................................................................

42
Section (4): Professional Practice:
50- How many nurses/medical assistant work with you ...................................................
51Do you work shifts? 1- Yes 2- No
52If yes; how long you stay per shift?.....................................................................
53If no; what are your working hours day?..................................................................
54: How many days off you have per month?5
55-If you stayed extra hours do you get overtime?..................................................................
56 Who is the person in-charge to evaluate your work?...........................................................
57-How often this evaluation happens?...........................................................................
58What kind of workshops and trainings that you were nominated to attend? ………………………………………………………………………………………
59Is there a fair process of nomination between health staff? 1- Yes 2- No
60To what extend you benefits from theses workshops and trainings? ………………………………………………………………………………………
61 Is there is/are any (unfair) regulation/s in your work guidelines? If yes, specify?............................................................................................................
62What were your main achievements up to now? 63 What interventions you think if implemented will improve your performance? ……………………………………………………………………… 64 Have you any suggestions for improvement of your performance? ......................................................................................................... 65What is/are your personal skills that helped you to improve your work?
………………………………………………………………………………… 66-What are the factors that negatively affect your work performance? ……………………………………………………………………………………
67-Is there a system for accountability in your work? 1- Yes 2- No 68 If yes; specify?...................................................................................................

43
( Appendix III)
Ahfad University for Women
Human Resources for Primary Health Care in Africa - Sudan
SO:3 To measure the satisfaction of users of skill mix at the different health settings. Date .................................. ..................... Data collectors name: -
.............................................. State.................................................. Locality: ................................................... Type of health facility:-
7- Basic Health Unit. 8- Health Center 9- Rural hospital
Name of the health Facility:-.........................................
My name is ……………………………., I am from Ahfad University for Women, and one of the team members to collect data about the human resources for primary health care. The main objective of this interview is measure the satisfaction of the AHS graduates (nurses and medical assistances) with their functions and responsibility as well as to evaluate their performance at health facility level. Duration for filling this questionnaire about 25 minutes, all information will be confidential and for academic use only, the participation is voluntary. Do you want to participate? 1- Yes 2- No Section (1) Demographic information:-
1. Gender
a. Female b. Male
2. Age ………………………………………………………………..
3. Civil Status: a. Single b. Married c. Divorced d. Widow
4. Educational Level:
a. Illiterate b. Primary c. Secondary d. University & Higher
5. Type of occupation : --------------------------------------------
Section (2): Visit’ Information
6-How many times did you visit during the last 6 months?
a. Less than 3 b.3 visits c. 4 visits d. 5 visits and more
7-When was your last visit? ---------------------------- 1-
8What is the reason for coming this time?
a. antenatal care visit b. feeling sick c. for communication d. co-patient

44
9-Who often provide you with the services?
a. Doctor b. Medical assistant c. Nurse d. Community health worker
e. Other, please specify………..
Section 3: Satisfaction with the skill mix
10. How long do you wait to meet the nurse/ Medical assistant?
a. 5minutes- 10minutes b. 15-30 minutes c. Hour d. More than hour
11-In your opinion is the waiting time to meet the nurse/ Medical assistant?
a. Very short b. Short c. Enough d. Long e. Very long
12-. Consultation time?
a. Very short b. Short c. Enough d. Long e. Very long
Please indicate to what extend are you satisfied or dissatisfied with the following
conditions:
Very
Satisfied
Satisfied Very
Dissatisfied
Dissatisfied
13- Received in a positive manner and treated with
respect by the nurse/ Medical assistant?
14-Receiving any emotional support from the nurse/
Medical assistant?
15- Receiving a beneficial treatment provided by the
nurse/ Medical assistant?
16-Being involved by the nurse/ medical assistant in
decision making for your treatment.
17- The nurse/ Medical assistant explains clearly all
relevant issues to you
18-The nurse/ Medical assistant has appropriate
competence to help you with your health problems?
19-Receiving the advice you need from the nurse/
Medical assistant?
20-Satisfied with the services provided by the
nurse/medical assistant?

45
21-If not satisfied why?----------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------
22. Does the nurse/ medical assistant provide any other services eg. Family Panning advice?
a. Yes b. No
23-if yes what are these services?
---------------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------
24--Does the center provide the services supposed to be provided?
a. Yes b. No

46
(Appendix IV)
Human Resources for primary Heath Care in Africa
HURAPRIM - Work Package 7 Ahfad University for Women - Sudan
Guidance for group to measure the satisfaction of users of skill mix at the different health settings.
Structure of the group:
- Both gender will be represented in separate groups - Age : different age category 20-60 - Different social status - Different educational qualifications. - Patient and co patient- key persons and community leaders (separately)
Areas to be discussed 1. How often they visit the health facility?
2. Reasons for visiting the health facility?
3. Who often provide the services?
4. Receiving the needed advice from the nurse/ medical assistant?
5. Competence of nurse/ medical assistant to help with the health problems? Why?
6. Receiving emotional support from the nurse/ medical assistant?
7. Treated with respect from the nurse/ medical assistant?
8. Clearly the nurse/ medical assistant explain things to you.
9. Waiting time to meet the nurse/ medical assistant?
10. Satisfaction with the waiting time?
11. Satisfaction with the consultation time?