Embed Size (px)
Citation preview

H+ homeostasis
The mechanisms by which the body keeps the plasma [H+]
constant

.
.
.
.

.
.
. .

.
.
. .

.
.
.
.

6
The Body and pH
Homeostasis of pH is tightly controlled
Extracellular fluid = 7.4 Blood = 7.35 – 7.45 < 6.8 or > 8.0 death occurs Acidosis (acidemia) below 7.35 Alkalosis (alkalemia) above 7.45

7

Three Major Mechanisms
Buffering Expulsion or retention of CO2
Generation / reclamation of HCO3
–/excretion of H+

Body buffers (I)
Extracellular HCO3
-/H2CO3
HPO42-/H2PO4
-
Plasma proteins

Body buffers (II)
Intracellular HCO3
-/H2CO3
HPO42-/H2PO4
-
Proteins & Amino-acids

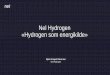
Buffering H++ HCO3
-⇄H2CO3 ⇄CO2+H2O H+ is buffered Bicarbonate is consumed To stop the backward reaction which
will lead to production of H+ ions, CO2
must be expelled To generate base from the backward
reaction H+ must be excreted

Respiratory mechanisms Hyperventilation
H2CO3 ⇌ H2O + CO2
Carbon dioxide diffuses through the CNS to the respiratory centre and stimulates hyperventilation
Hypoventilationless than normal PCO2 results in hypoventilation

.
.

.
.

Metabolic/Renal mechanisms
Excretion of H+
Bicarbonate generation
Bicarbonate reabsorption / reclamation

.
.

.
.

.
.

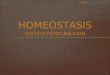
The proton pump
.
The proton pump
The proton pump excretes H+ and generates bicarbonate

Parameters used in assessing acid-base balance
Plasma pH
Arterial PCO2
Plasma [bicarbonate]
Anion gap (AG)

Parameters used in assessing acid-base balance: Reference ranges
Plasma pH: 7.35-7.45 corresponding to [H+] of 43-36 nmol/L (7.4) av
Arterial PCO2 : 4.8-5.8 kPa (5.3) av
Plasma [bicarbonate]: 21-28 mmol/L (25) av
Anion gap: 13-18 mmol/L (15.5) av

What is an ABG? The Components
pH / PaCO2 / PaO2 / HCO3 / O2sat / BE Desired Ranges
pH - 7.35 - 7.45 PaCO2 - 35-45 mmHg (4.8-5.8 Kpa) PaO2 - 80-100 mmHg (> 11 mmol/L) HCO3 - 21-27 O2sat - 95-100% Base Excess - +/-2 mEq/L

Why Order an ABG? Aids in establishing a diagnosis Helps guide treatment plan Aids in ventilator management Improvement in acid/base management
allows for optimal function of medications
Acid/base status may alter electrolyte levels critical to patient status/care

Parameters used in assessing acid-base balance
Others: Actual bicarbonate Standard bicarbonate Base excess PO2

Definitions
Standard bicarbonate: The concentration of bicarbonate
in plasma of a blood specimen that has, following collection, been equilibrated with O2 and CO2 mixtures at 37C. Conditions: fully oxygenated and PCO2 5.3 kPa or 40 mm Hg

Definitions
Base excess: The amount of strong acid that
would be required to titrate one litre of fully oxygenated blood to a pH of 7.4 ([H+]= 40 nm/L) at 37C under conditions where PCO2 is 5.3 kPa or 40 mm Hg

pH / Henderson-Hasselbalch Equation using the dynamics of the bicarbonate buffer
pH = pK + 1ogl0 [HCO3-]
[H2CO3]
pH = 6.10 + 1ogl0 [HCO3 -]
S.PCO2
pH = ~ [base] [acid ]
S=solubility coefficient of CO2= 0.23 mmol/J if PCO2 is expressed in kPa and 0.03 mmol/J if PCO2 is expressed in mmHg

Anion gap Based on the electroneutrality of
plasma [total cations] = [total anions]
([Na+] + [K+] +[Ca+]) = ([Cl-]+[HCO3-]+
[pyruvate]+[acetoacetate]+[lactate]+[urate] +[citrate] )
([Na+] + [K+]) -([Cl-]+[HCO3-]) = Anion
Gap (AG).

Causes of metabolic acidosis and increased anion gap (increased production of fixed or organic acids)
Lactic acid (shock, infection, hypoxia)
Urate (renal failure) Ketones (diabetes mellitus, alcohol) Drugs and toxins (salicylates,
biguanides, ethylene glycol, methanol)

Causes of metabolic acidosis and normal anion gap (loss of HCO-
3 or ingestion of H+ ions)
Proximal renal tubular acidosis
Diarrhoea Drugs
(acetazolamide) Addison’s disease
Pancreatic fistulae
Ammonium chloride ingestion

Key to solving acid-base problems:
Look at the plasma pH Is there acidaemia or alkalaemia?
Find the primary cause (parameters with a change consistent with or supporting the change in pH)
Find the secondary or compensatory changes (parameters with a change not consistent with or opposing the change in pH)

Simple acid-base disturbances
pH< 7.35 PCO2 AG HCO3
pH >7.45 PCO2 AG HCO3

Simple acid-base disturbances
pH< 7.35 PCO2 AG HCO3
Acute respiratory acidosis
Chronic respiratory acidosis
Metabolic acidosis Mixed acidosis pH >7.45 PCO2 AG HCO3
Acute respiratory alkalosis
Chronic respiratory alkalosis
Metabolic alkalosis Mixed alkalosis

.
.

Metabolic Acidosis
Processes: Increased acids (endogenous/
exogenous) Increased H+
Decreased excretion of H+
Bicarbonate depletion / loss

Mechanisms of acid-base disturbances:Metabolic acidosis
Addition of hydrogen ions to body fluids in excess of the excretory capacity
(Processes that add hydrogen ions to body fluids faster than the body can excrete)
Starvation ketosis Diabetic ketoacidosis Lactic acidosis Ingestion of substances that are acidic or
yield acidic metabolites e.g. NH4Cl, methanol, paraldehyde, salicylates
(here , there is nothing
wrong with the kidneys)

Mechanisms of acid-base disturbances:Metabolic acidosis
Failure to excrete hydrogen ions at the normal rate (here , there is something wrong with the kidneys)
Inadequate production of ammonia by the kidney e.g. chronic renal failure
Inability to maintain the blood-urine H+ concentration gradient (pH 7.4 : 6) DRTA, Oliguria /Anuria: e.g. acute renal failure

Mechanisms of acid-base disturbances:Metabolic acidosis
Loss of bicarbonate from the body From the GIT e.g. severe diarrhoea,
fistulous drainage, uretero-sigmoidostomy
Proximal renal tubular acidosis (PRTA; failure to generate or reclaim bicarbonate) e.g. Fanconi syndrome, carbonate dehydratase inhibitors; e.g. acetazolamide)

Respiratory acidosis
Processes involved: Mechanical blockage of airway Respiratory depression.Structures involved: Brain, meninges, nerves,
respiratory muscles, lung tissue

Mechanisms of acid-base disturbances:Respiratory acidosis
Increased alveolar PCO2 leading to increased arterial PCO2
Lung disease e.g. chronic airways obstruction, respiratory distress syndrome
Weakness of respiratory muscles e.g. poliomyelitis
CNS disease e.g. encephalitis, meningitis Drug overdose e.g. hypnotics,
anaesthetics

Metabolic alkalosis
Processes involved: Loss of H+
Gain of base

Mechanisms of acid-base disturbances:Metabolic alkalosis
Metabolic Alkalosis Loss of hydrogen ions from the body Loss of H+ in vomit Diuretics (potassium non-sparing diuretics) Na+
, K + increased excretion of H+ ([H+])
Mineralocorticoid excess Na+ , K + increased excretion of H+ [H+]
Glucocorticoid excess Na+ , K + increased excretion of H+ [H+]
K+ depletion if severe increased excretion of H+
[H+]

Mechanisms of acid-base disturbances:Metabolic alkalosis
Addition of base to body fluids in excess of the excretory capacity
NaHCO3 infusions Ingestion of alkali e.g. NaHCO3,
MgO, CaCO3
Milk-alkali syndrome (treatment of peptic ulcer).

Respiratory alkalosis
Loss of carbon dioxide

Mechanisms of acid-base disturbances:Respiratory alkalosis
Respiratory alkalosis Lowered alveolar PCO2
Voluntary overbreathing, hysteria Artificial ventilation Drug overdose e.g. salicylate
poisoning sometimes

Salicylate toxicity: blood [salicylate]> 30mg dL
Usually: Accidental in children Deliberate in young adultsIn the treatment of: Rheumatoid arthritis Dermatosis

Salicylate toxicity
Initially there is stimulation of the respiratory centre ⇒ low PCO2, low HCO-
3, and respiratory alkalosis Salicylates alter peripheral
metabolism ⇒ production of various organic acids e.g. lactic acid ⇒metabolic acidosis with anion gap

Salicylate toxicity
Adults: Mixed respiratory alkalosis and
metabolic acidosisChildren: Metabolic acidosis

Salicylate toxicity: other features
Sweating Vomiting Dehydration A metabolic alkalosis can occur as
a result of vomiting

Salicylate toxicity: useful laboratory measurements
Total body K+ : () Plasma total CO2 : () Plasma [urea]: ()

Salicylate toxicity: Management
Initially and in case of spasm of pyloric
sphincter: Gastric lavageAfter significant absorption of
salicylate: Forced alkaline diuresis