Embed Size (px)
Citation preview

1
HYPERTHERMIC INTRAPERITONEA CHEMOTHERAPY (HIPEC) AND CYTOREDUCTIVE
SURGERY (CRS) IN THE PERITONEAL CARCINOMATOSIS
อาจารยทปรกษา: ผศ.นพ.วรวทย วาณชยสวรรณ
ผเรยบเรยง: นพ.อนวตร พลานสนธ $
Peritoneal carcinomatosis(PC) เปนอาการทางคลนกระยะสดทายของผปวยทมการกระจายตวของมะเรงใน
ชองทอง ซงมการพยากรณโรคทแย ผปวยมกเสยชวตภายใน 6 เดอน(1-2) และการรกษา peritoneal carcinomatosis
ยงไมแนนอน และยงม morbidity และ mortality ทสง การผาตดเพอรกษาน Jนเปนสาเหตการตายของผปวยทม
peritoneal carcinomatosis
ในชวงทผานมาการรกษา peritoneal carcinomatosis ไดรบความสนใจเปนอยางมากโดยเฉพาะการใหยาเคม
บาบดเขาไปในชองทองเรมมมาต Jงแต ปค.ศ.1980(3) และมการผาตดเอาเยอหมผนงหนาทองออก (peritoneal) ในป
ค.ศ. 1995 ใชในการรกษา peritoneal carcinomatosis ทมาจากมะเรงทางสตนรเวชและทไมใชทางสตนรเวช การ
รกษาไดมความกาวหนามากขJนท Jงในชองทองและองเชงกราน แมวาจะม morbidity ทสงหลงการผาตดแตกสามารถ
กาจดมะเรงทอยในชองทองและองเชงกรานไดและรกษาชวตไดยนยาวขJน
โดยหลกการของ HIPEC คอการใชยาเคมบาบดรวมกบอณหภมทสงตอสกบเซลลมะเรง ทาใหเกดการเพม
ฤทธ $ของยาเคมบาบดโดยการใหผานทางชองทอง เปนการรกษาวธใหม อาจยงตองมการศกษาเพมเตมเพอยนยนผลท
ดของวธนJ(4)
EPIDERMIOLOGY
Primary peritoneal malignant disorders (เชน peritoneal mesothelioma) เปนภาวะทพบไดนอยมาก มกจะ
พบเปนการกระจายตวมะเรงของอวยวะในชองทอง โดยเฉพาะมะเรงของไสตง ลาไสใหญ รงไข และกระเพาะอาหาร
อาจพบพรอมกบมะเรงต Jงตน (primary tumor) หรอการกลบมาเปนซJาในระยะแพรกระจาย(1)
สวนใน Secondary peritoneal malignant disorder ของมะเรงแตละชนดจะแตกตางกน เชน ในColorectal
cancer พบ isolated PC ได 15-20% และเพมเปน 20-30% หากม metastasis ทอวยวะอนรวมดวย ใน Gastric
cancer หากเปนการวนจฉยคร Jงแรก (first diagnosis) พบ PC ได 10-20% และหากเปนการกลบเปนซJา (recurrence)
พบ PC ได 40-50% ใน Ovarian cancer หากเปน first diagnosis พบ PC ได 60-80% และหากเปน recurrence พบ
PC ได 55-75% เปนตน(5)
PATHOPHYSIOLOGY
กลไกการเกด peritoneal carcinomatosis มหลายปจจย ซงเปนการแพรกระจายของเซลลมะเรงในหลายแบบ
เชนการแพรกระจายโดยตรง แพรกระจายผานทางเดนนJาเหลองหรอทางหลอดเลอดดา หรอจากการผาตด(4)

2
Peritoneal carcinomatosis เกดจากแพรกระจายของเซลลมะเรงผานวธทเรยกวา “neoplastic redistribution”
โดยกลไกเกดจากการควบคมการแพรกระจายทขJนกบ ปจจยทางกายภาพและชวภาพของมะเรงทจดกาเนด ขนาดของ
มะเรงทจดกาเนด นJาในชองทองหรอ mucus โดยเซลมะเรงจะเคลอนทไดอยางอสระในชองทอง มกจะไปตามแรงโนม
ถวงของโลกและ บรเวณทมการดดกลบของนJาในชองทอง บรเวณทมการดดกลบเกดขJนท greater and lesser
omentum กระบงลมโดยเฉพาะดานขวา เปนผลทาใหพบกระจายตวของมะเรงในชองทองทองเชงกราน subphrenic
space, the pericolic grooves และ Morrisom’s pouch
RATIONALE
มการศกษาเกยวกบยาเคมบาบด(4,6-7)ทนามาใชในชองทองวามความเขมขนมากกวาทใหทางกระแสเลอด
เนองจากในชองทองม peritoneal plasma barrier ดงน Jน HIPEC จงเปนการออกฤทธ $ของยาเคมบาบดแบบ
locoregional กบอณหภมสงตอสกบเซลลมะเรง โดยอณหภมทสงออกฤทธ $โดยตรงตอ cytotoxic ในอณหภมและเวลาท
ใช ความรอนทใชมผลตอการเพมขJนของการกระจายตวของยาเขาสเซลลมะเรงและลดความดนภายในเซลลมะเรง
(interstitial fluid pressure)
HIPEC มประสทธภาพทเหนอกวาการใหยาเคมบาบดในชองทองอยางเดยวและการใหความรอนในชองทอง
อยางเดยวในการรกษา peritoneal carcinomatosis ในการศกษาแบบสม(8) การใหยาเคมบาบดในชองทองอยางเดยว
ทาใหยาเคมบาบดซมผานเขาเซลลมะเรงระหวาง 1-3 มลลเมตร(9) แตถาใหความรอนควบคดวยจะทาใหยาเคมบาบด
ผานเขาเซลลมะเรงไดมากขJนเปน 3-6 มลลเมตร(10) ถาการผาตดแบบ cytoreductive หรอการลดขนาดของมะเรงได
นอยกวา 2.5 มลลเมตรกยงทาให HIPEC ไดผลดยงขJน(1) โดยสรปการผาตดแบบ cytoreductive เปนการรกษาแบบ
macroscopic และ HIPEC เปนการรกษาใน microscopic ทชวยการรกษาใหไดผลดยงขJน เนองจาก peritoneal
carcinomatosis เปน locoregional cancer ไมมการแพรกระจายทางกระแสโลหตหรอไปสวนตางๆของรางกาย การ
ผาตดแบบ cytoreductive และ HIPEC จงมความหวงทจะรกษาใหหายขาดได
หลกการใชยาเคมบาบดในชองทองของ HIPEC ขJนกบ pharmacokinetic ของยาทอยชองทอง อณหภมทใช
ในชองทองอยทประมาณ 42-43˚C มผลตอการกาจดเซลลมะเรงโดยเฉพาะ oxaliplatin mitomycin doxorubicin
cisplatin paclitaxel irinotecan แตยงไมขนาดยาเคมบาบดทใชเปนมาตรฐานในการรกษา ในปจจบนการใชยาเคม
บาบดขJนกบเนJองอกแตละชนดดงตาราง(58)

3
ตาราง1 Standardized Orders for Heated Intraoperative Intraperitoneal Chemotherapy
A. For pseudomyxoma peritonei, adenocarcinoma from appendiccal, colonic, and rectal cancer
1. Add mitomycin C _______ mg to 2 liters of 1.5% dextrose peritoneal dialysis solution.
2. Add doxorubicin _______ mg to the same 2 liters of 1.5% dextrose peritoneal dialysis solution.
3. Dose of mitomycin C and for doxorubicin is 15 mg/m2 for each chemotherapy agent.
4. Use 33% dose reduction for heavy prior chemotherapy, marginal renal function, age greater than 60, extensive
intraoperative trauma to small bowel surfaces, or prior radiotherapy.
5. Add _______ mg 5-flurouracil (400 mg/m2) and leucovorin _______ mg (20 mg/m2) to separate bags of 250 ml normal
saline. Begin IV infusion of both drugs simultaneously with IP chemotherapy in fusion.
6. Send the above to the operating room _______ at ________ o’clock for 90-minute irrigation.
B. for gastric and ovarian cancer, mesothelioma and sarcoma
1. Add cisplatin _________ mg to 1 liter of 1.5 % dextrose peritoneal dialysis solution. Dose of cisplatin 50 mg/m2
2. Add doxorubicin _______ mg to same 1 liter of 1.5 % dextrose peritoneal dialysis solution. Dose of cisplatin 15 mg/m2
3. Use 33% dose reduction for heavy prior chemotherapy, marginal renal function, age greater than 60, extensive
intraoperative trauma to small bowel surfaces, or prior radiotherapy.
4. Add _______ mg 5-fluorouracil (400 mg/m2) leucovorin _______ mg (20 mg/m2) to separate bags of 250 ml normal
saline. Begin IV infusion of both drugs simultaneously with IP chemotherapy infusion.
5. Send the above to operating room ______ at o’clock for 90-minute irrigation.
C. Oxaliplatin and Intravenous 5-Fluoracil and Leucovorin Orders
1. Add oxaliplatin _______ mg (130 mg/m2)to 2 liters 5% dextrose and water for intraperitoneal Administration.
2. Add_______ mg 5-flurouracil (400 mg/m2) and leucovorin _______mg (20mg/m2) to separate bags of 250 ml normal
saline. Begin IV infusion of both drugs simultaneously with IP chemotherapy infusion.
3. Send the above to operating room ______ at o’clock for 60-minute irrigation.

4
TECHNIQUE
ในปจจบนไดมวธการผาตดและการทา HIPEC หลายวธ ซงมความแตกตางของอณหภมทใชใน HIPEC
ปรมาณของยาเคมบาบด หรอการเปดหรอปดทองในชวงทใหยาเคมบาบด
Cytoreductive Surgery
การลงแผลผาตดต Jงแต xiphoid ถง pubis โดยเรมจากสารวจในชองทองประเมนการแพรกระจายของเนJองอก
ในชองทอง อาจมการสงตรวจทาง cytology หรอ pathology การตดกอนเนJอออกใหหมดเทาทเหนดวยตาเปลาหรออาจ
เหลอเนJองอกขนาดเลกทไมเกน 2.5 มลลเมตร ซงจะใหประโยชนในการรกษาดวย HIPEC สวนการผาตดเนJองอกตน
กาเนดใหผาตดแบบ oncologic principle โดยการผาตดตองเอาเนJองอกมะเรงออกใหหมดโดยคานงถงการดแลหลง
ผาตดและคณภาพชวตหลงการผาตด
การผาตด peritonectomy ในบรเวณทมมะเรงอยแบงออกเปน parietal และ visceral peritonectomy การทา
visceral peritonectomy จะตดอวยวะในชองทองหรอ mesentery บางสวนทมเนJองอก สวน falciform ligament ถง
นJาด ไสตง และ omentum ท Jงหมดจะถกตดออกเสมอ สวนการทา parietal peritonectomy ทาในบรเวณทมมะเรงอย
เทาน Jนในทกดานของเยอหมทอง สวนมะเรงขนาดเลกสามารถตดออกไดดวยวธ electroevaporation โดยสรปวธการ
ผาตดไดดงนJ(4)
1. Midline laparotomy.
2. Complete omentectomy with en bloc splecnectomy (if involved).
3. สารวจลาไสเลกจาก ligament of treitz to ileocecal valce และลาไสใหญจนถงไสตรง หลงจากน Jนจงตด
สาไสและ mesentery ทมมะเรง
4. Right hemicolectomy และ parietal peritonectomy (if involved).
5. Pelvic peritonectomy และ hyaterectomy with bilateral salpingo-oophorectomy (if involved หรอเปน
มะเรงรงไข)
6. Left hemicolectomy หรอ sigmoidectomy และ parietal peritonectomy (if involved).
7. Gastric resection (if involved), cholecystectomy, lesser omentectomy, duodenal-hepatic and
gastro-hepatic ligament dissection.
8. Upper quadrant peritonectomy and Glisson capsule (if involved).
9. Resection of disease to left of retrohepatic cava และ strip port hepatic.
HIPEC procedure
HIPEC เปนหตถการททาหลงจาก CRS เสรจสJน โดยการใสยาเคมบาบดเขาไปในชองทอง (intraperitoneal route) โดยตรง รวมกบการใชอณหภมสง (hyperthermia) หวงผลเพอกาจด microscopic tumor โดยการให IP chemotherapy จะทาใหยาเคมบาบดสมผสกบ peritoneal surface โดยตรง local concentration เพมขJน ในขณะท

5
systemic toxicity ลดลง นอกจากนJ blood drainage จาก peritoneal surface จะผานทาง portal vein ไปยงตบ จงชวยกาจด hepatic micrometastasis ไดอกดวย(11)
นอกจาก HIPEC ซงเปนการใหยาเคมบาบดในอณหภมสงแลว ยงมการให IP chemotherapy ในอณหภม
ปกต ไดแก early postoperative intraperitoneal chemotherapy (EPIC) ในวนท 4–6 หลงผาตด และ sequential
intraperitoneal chemotherapy (SIPC) เปน repetitive treatment ใน 6 เดอนหลงผาตดอกดวย
ความรอนทถกใชเพอฆาเซลลมะเรงอยท 42.5 C ในการทดลอง(1) ซงตองรกษาอณหภมในชองทองอยท
41.5-42.5 C ถงมประสทธภาพในการฆาเซลลมะเรงรวมกบยาเคมบาบด ปรมาณยาเคมบาบดทใชใสในชองทองขJนกบ
พJนทผวกายอยทประมาณ 3-5 ลตรซงยาเคมบาบดทใหขJนกบมะเรงตนกาเนด โดยใชระยะเวลาประมาณ 30-120 นาท
แตยงไมมเกณฑทแนนอนโดยสวนใหญจะใชเวลาประมาณ 60-90 นาท(4) และเมอใสยาเคมบาบดลงในชองทองจนครบ
ตามเวลาแลว ไดปลอยยาเคมบาบดออกท JงหมดและลางดวยสารนJาในชองทองตาม
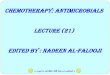
ในปจจบนไดมอปกรณพเศษเพอชวยในการทา hyperthermia perfusion แบบระบบปดปลอดเชJอ โดย
Schematic(1,12) มระบบทประกอบดวย extracorporeal dual-filter system และมทอซลโคนตอในชองทองกบเครอง
Schematic โดยทอซลโคน 2 อนจะถกวางไวท Subphrenic cavity ดานขวาและ deep pelvic เปนขาเขาของยาเคม
บาบด และอก 2 อนวางไวท subphrenic cavity ดานซายและ superficial pelvic เปนขาออกของยาเคมบาบด และมตว
อณหภมท Jงขาเขาและขาออกของยาเคมบาบดเพอรกษาอณหภมใหคงทตลอดและวดอณหภมกายโดยผานทางหลอด
อาหาร
รป 1 แสดง HIPEC circuit and Schematic device

6
รป 2 แสดง Open technique of HIPEC(13)
รป 3 แสดง close technique of HIPEC (14)
วธการใหยาเคมบาบดในชองทองใน HIPEC มหลายวธ เชน open abdominal technique (coliseum) closed abdominal technique peritoneal cavity expander และ semi-opened abdominal technique ในวธตางๆยงไมมการศกษาทยนยนวาวธการใดดทสด
Open/Coliseum technique หลงจากการผาตด CRS แลว จะดงผวหนงขJนมาร Jงไวกบ self-retaining retractor ใส smoke evacuator แลวคลมดวย plastic sheet ซงเจาะรตรงกลางไว เพอใหศลยแพทยสามารถใสมอลงไปได ขอดคอ การกระจายของยาและความรอนเปนไปอยางท วถง ขอเสยคอ การทาใหอณหภมสงถงระดบทตองการทาไดยากและเสยงตอการสมผสกบยาเคมบาบด จากการศกษาของ Stuart และคณะ(15) เพอดเรองความปลอดภยของบคลากรในหองผาตดในการใช open technique โดยการตรวจระดบยาเคมบาบดในปสสาวะ ระดบยาเคมบาบดเหนอ/ใต plastic sheet รวมท Jง permeability ของ sterile glove ตอยาเคมบาบด พบวาผลท Jงหมดเปน negative แสดงถงความปลอดภยของทเพยงพอของ open technique
Close technique หลงจากการผาตด CRS และใส catheter & temperature probe แลว จะเยบปดผนงหนาทอง แลวจงทา HIPEC ขอดคอ การทาใหอณหภมสงถงระดบทตองการทาไดงาย ลดโอกาสสมผสกบยาเคมบาบด เพม abdominal pressure ทาใหการ penetration ของยาดขJน ขอเสยคอ ไมสามารถบอกไดวาการกระจายของยาและความรอนท วถงหรอไม
Chemotherapeutic agent จากคณสมบตของ peritoneal-plasma barrier ซงเปน semi-permeable membrane ยาเคมบาบดทเหมาะสม ควรมลกษณะเปน high molecular weight, hydrophilic และ highly charged ซงผาน peritoneal-plasma barrier ไดไมด จงออกฤทธ $ภายในชองทองไดนาน ชนดของยาทใชจะแตกตางกนตาม primary tumor เชน mitomycin C (MMC) และ oxaliplatin นยมใชใน pseudomyxoma peritonei มะเรงลาไสใหญ กระเพาะอาหาร cisplatin นยมใชในมะเรงรงไข เปนตน โดยขนาดยาจะคดตาม body surface area และลดขนาดยาลง 33% ในกลมดงนJ(16)
- อายมากกวา 60 ป - มประวตไดรบ multiple lines of systemic CMT - มประวตไดรบ GM-CSF จากภาวะ febrile neutropenia ในขณะทได systemic CMT - มประวตไดรบ radiation therapy ในบรเวณทม bone marrow
INDICATIONS
ใน Peritoneal disease ทสามารถรกษาดวยวธ HIPEC ตองมตวโรคทจากดอยในชองทองและสามารถทจะทาการ
ผาตดออกไดท Jงหมด ไมวาจะเปนมากจากมะเรงกระเพาะอาหาร มะเรงลาไสใหญและไสตรง มะเรงไสตง มะเรงรงไข

7
หรอแมมะเรงของเยอบชองทองเองกตาม ซงผปวยตองไดรบการประเมนทกคร Jงทนาผาตดและ HIPEC เสมอถงขอบงชJ
ในผปวยแตละราย โดยท วไปขอหามทไมนาผปวยมาผาตดมดงนJ(4)
1. อายมากกวา 70 ป
2. มโรคประจาตวหรอโรคอนทมผลตอรางกาย
3. ตวโรคแยลงแมไดรบยาเคมบาบดมาแลว
4. ภาวะขาดสารอาหาร
5. มการกระจายตวโรคออกไปนอกชองทอง
6. กระจายตวไปทตบและไมสามรถผาตดได
7. เนJองอกแพรกระจายไปท retroperitoneum และมการกระจายตวไปตอมนJาเหลอง
อาจมขอหามอนเชน tumor marker ไมลดลงหลงจากไดยาเคม ภาวะอวน เคยไดรบการฉายรงสในชองทอง เคย
ไดรบการผาตดมากกวา 4 คร Jง เปนตน แตทกลาวมายงไมมการศกษาทยนแนนอนถงขอหามหรอขอบงชJในการทา
HIPEC
PROGNOSTIC INDICATOR
ในปจจบนไดมแบบคดกรองผปวยทเหมาะสมกบการทา HIPEC หลายแบบ เพอหาผปวยทสามรถนามาทา
แลวไดประโยชนมากทสด แตยงไมมรปแบบทแนนอนทนามาใชในการคดเลอก การทา CT scan และ MRI เปนตวชวย
ในการวางแผนการผาตดแตไมสามรถทจะยนยนไดวาสามารถทจะทาการผาตดไดสาเรจเนองจากมขอจากดของ CT
scan และ MRI ทม sensitivity ทตาในการประเมนโรค(17)
ปจจบนการผาตดเปนการประเมนทดทสดไมวาจะเปนการผาตดเปดทองหรอการผาตดแบบสองกลอง และ
การประเมนระยะของมะเรงในชองทองน Jนยงไมมระบบทแนนอน ในป 1994 Gilly(18) ไดต Jงระบบมาประเมนโดย
จดแบงตามขนาดและการกระจายตวของมะเรงในชองทอง ดงตาราง วธนJใชไดงายและสะดวก แตไมสามารถทจะ
นาไปใชรวมกบการผาตดได(4)
ตาราง 2 แสดง Gilly staging of peritoneal carcinomatosis
Stage Description
0 No macroscopic disease
1 Malignant granulation less than 5 mm in diameter. Localized in one part of abdomen.
2 Malignant granulation less than 5 mm in diameter. Diffuse to the whole abdomen.
3 Localized or diffuse malignant granulations 5-20 mm in diameter.
4 Localised or diffuse large malignant masses (more than 2 cm in diameter).

8
The Peritoneal Cancer Index (PCI) ไดถกต JงขJนโดย Jacquet และ Sugarbaker(19) เปนระบบทถกใชอยาง
แพรหลายกวาของ Gilly เนองจากสามารถประเมนมะเรงไดท Jงเชงปรมาณและการกระจายตวทดกวา โดยแบงชองทอง
ออกเปน 13 สวนและ ใหคะแนนของขนาดมะเรงทแตกตางกน ดงรป 4 ซงมประโยชนท Jงในการพยากรณโรคและ
ประเมนการผาตดได
รป 4 แสดง Peritoneal Cancer Index staging system for peritoneal carcinomatosis
Sugarbaker ไดแนะนาในผปวยทม carcinomatosis ในมะเรงลาไสทมคา PCI ทมากกวา 20คะแนน(20)
แนะนาใหรกษาตามอาการ การใช HIPEC จะไมเหมาะสม
ปจจบนยงมเครองมอทใชชวยในการพยากรณโรคหลงการผาตดซงมอย 2 แบบ เพอประเมนหลงผาตด โดย
lyon ไดแบงออกเปน complete และ incomplete โดย Complete แบงออกเปน R0 (ไมมกอนมะเรงเหลออย) และ R1
(มะเรงยงเหลออยในระดบ microscopic) cytoreduction และ incomplete เปน R2 cytoreduction ซง R0/R1
cytoreduction มประโยชนในการรอดชวตมากกวา R2 cytoreduction
Jacquet และ Sugarbaker ไดเสนอ completeness of cytoreduction (CCR) score เพอประเมนหลงการ
ผาตด แบงตามตาราง (19,21)

9
Stage Description
CCR 0 No residual tumor No peritoeneal seeding esposed during the complete exploration
(complete cytoreduction)
CCR 1 < 2.5 mm Diameter of tumor nodules persisting after cytoreduction (complete
cytoreduction)
CCR 2 >2.5 mm ,
< 2.5 cm
Diameter of tumor nodules persisting after cytoreduction (incomplete
cytoreduction, moderate residual tumor)
CCR 3 >2.5 cm Diameter or a confluence of unresectable tumor nodules at any site within
abdomen (incomplete cytoreductive, gross residual tumor)
ในปจจบน optimal cytoreductive ยงมถกเถยงกนอยมากมายและหลายๆการศกษายงแนะนาแตกตางกน ซง
สวนใหญ optimal cytoreductive จะเหลอมะเรงไมเกน 2.5 มลลเมตรซงใหผลการรกษาทดและการใหยาเคมบาบดผาน
ทางชองจะไดในมะเรงทขนาด 0.5-2 มลลเมตร(22)
MORBIDITY AND MORTALITY
ใน HIPEC และ cytoreductive surgery (CRS) เปนหตถการททาทายและยงมความหลายหลาย ในทผาน
มากการผาตดแบบนJยงไมไดแพรหลายและมอตราการเสยชวตทสง โดยเฉพาะในหลายๆรพ.ทมประสบการณในการ
รกษาและดแลหลงผาตดทแตกตางกน ทาใหยงไมมการศกษาถงปจจยเสยงททาใหเกดภาวะแทรกซอนจากการผาตด
ได โดยรวมแลว morbidity และ mortality อยท 12-66% และ 0-12% ตามลาดบ(4) ซงเปนการวมรวมจากศกษาเลกๆ
แตไดม systematic review รวบรวมขอมลและวเคราะหจากรพ.ตตยภม ม mortality และ morbidityอยท 0.9-5.8%
และ 12-52% ตามลาดบ(4) ท JงนJ morbidity และ mortality ขJนกบประสบการณในการทา HIPEC และ cytoreductive
surgery
สาเหตของ mortality ทพบบอย(2)คอ ภาวะการตดเชJอหลงผาตดรวมกบมภาวะลมเหลวของอวยวะตางๆ
ภาวะแทรกซอนอนๆทมการรายงานในหลายๆการศกษา เชน anastamosis leakage (0-9%) fistula (0-23%)
intestinal perforation (0-10%) intraperitoneal sepsis (0-14%) abscess (0-37%) และ ileus (0-86%) ในบาง
การศกษากลาวถงการนาไปผาตดซJา (reoperative) ถง 0-23% ซง ภาวะแทรกซอนเหลานJสมพนธกบชนดของการ
ผาตดแบบ cytoreductive
สวนภาวะแทรกซอนทเกดกบการทา HIPEC น Jนพบไดนอย แตมรายงานในบางการศกษาทนาจะเกดท Jง
HIPEC และ CRS เชน deep vein thrombosis/Pulmonary embolism (0-9%) pancreatitis pneumonia cardiac
insufficiency และ cerebral infarcts เปนตน ดงน Jนการทา CRS และ HIPEC ตองมการเตรยมผปวยกอนผาตดให
เหมาะสม เพอลดโอกาสในการเกดภาวะแทรกซอนกอนและหลงผาตดได อกท Jงประสบการณในการผาตด CRS จะชวย
ลดภาวะแทรกซอนไดเชนกน แตอยางไรกตามการเลอกผปวยมาทาการผาตดและ HIPEC จะชวยเพมการรอดชวตได

10
MESOTHELIOMA
Malignant mesentheloma เปน primary neoplasm ของเยอบผวของชองทอง เยอหมปอด เยอหมหวใจทม
aggressive สวนใหญมกจะอยในชองทองและไมคอยพบการกระจายตวไปทสวนตางๆ การรกษามกเปนการผาตด ให
ยาเคมบาบดทางกระแสเลอด หรอการฉายแสง จากรายงานพบวาผปวยมชวตไดไมเกน 12 เดอน หลงไดรบการรกษา
(4) ในปจจบนไดมการรกษาแบบ CRS และ HIPEC พบวาสามารถเพมอตราการรอดชวตของผปวยได โดยท median-
survivalอยท 60 เดอน และ 5-year survival อยท 50%
จากการศกษาของ Tristan D. และคณะ(59) เปนการเกบรวบรวมขอมลผปวยทเปน DMPM ท Jงหมด 405 คน
ในป 1989-2009 แบบ Multi-Institutional Experience พบวา Multi-Institutional พบวา Overall median survival อยท
53 เดอน และ 3- and 5-year survival rates อยท 60% และ 47%ตามลาดบ และยงพบอกวาปจจยทมผลตอ
prognosis และชวยเพมอตราการรอดชวตคอ epithelial subtype (P < .001) absence of lymph node metastasis
(P <.001) completeness of cytoreduction scores of CC-0 or CC-1 (P <.001) และ HIPEC (P .002)
และการศกษาของ Dario Baratti และคณะ(60) ไดทาการเกบรวบรวมขอมลแบบ prospective ผปวยทเปน
DMPM จานวน 108 คน ไดรบการทา CRS และ HIPEC (cisplatin 45mg/L + doxorubicin 15mg/L or Mitomycin-C
3.3mg/m2/L, 42.5oC; 90 mim) พบวา Median OS และ
progressive-free survival อยท 63.2 และ 25.1 เดอน (95%CI
5.1–45.1) และ survival curve reached a plateau หลงจาก 7
ป และไดมการศกษาทาง immunostaining พบวา epithelial
histological subtype, negative lymph-nodes, 610% Ki67-
positive cells สมพนธกบการเพมขJนของ OS and PFS.
Positive podoplanin สมพนธกบการเพมขJนของ PFS.
PSEUDOMYXOMA PERITONEI
Pseudomyxoma peritonei (PMP) เปนภาวะทพบไดนอยทมการกระจายตวของ mucinous tumor ในเยอบชองทองและมลกษณะของ ascites แบบ mucin เกดจาก perforated appendiceal epithelial tumor สามารถแบงตาม histopathologic subtype ได 3 ชนด ไดแก dissaminated peritoneal adenomucinosis (DPAM), hybrid และ peritoneal mucinous carcinomatosis (PMCA) โดยท DPAM และ hybrid จดเปน low grade tumor สวน PMCA จดเปน high grade tumor ในอดตรกษาโดย serial debulking with IP chemotherapy เพอลดอาการของ mucinous ascites โดยม 5 และ 10 ป survival เปน 50 และ 30%(33)
การใช CRS รวมกบ HIPEC เปนการรกษาอกทางเลอกหนงของ PMP มาต Jงแตป 1980 โดย Spratt และคณะ โดยใช IP thiothepa พบวาใหผลการรกษาทด และมภาวะแทรกซอนเพยง minor pulmonary atelectasis และมการศกษาแบบ prospective ทยนยนวาการใช CRS with HIPEC เปนการรกษาแบบมาตาฐานของ PMP(34) แตยงขาดการทดลองแบบสม โดยใน phase 1 และ phase 2 มอตราการรอดชวตอยท 66% และ 97% ตามลาดบ(17)

11
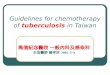
รป 6 แสดงการเปรยบเทยบระหวาง CRS with HIPEC with
systemic CMT กบ systemic CMT alone
สาหรบการเปรยบเทยบระหวาง CRS with HIPEC (study group) กบ debulking with IP chemotherapy (control group) มการศกษาแบบ retrospective ของ Andreasson และคณะ(35) ในป 1993-2008 จานวน 150 คน แบงเปน study group [IP MMC 30-35 mg/m2, 42oC, 90 min] และ control group พบวา study group ม 5-year survival ดกวา control group เทากบ 74% และ 40% ตามลาดบ (P < 0.001)
นอกจากนJ ยงมอกหลายการศกษาทเปน multicentric study เชน จากการศกษาแบบ prospective ของ Elias และคณะ(36) ในป 1993-2007 จานวน 301 คน โดยใหเปน MMC หรอ oxaliplatin พบ DFS 6.5 ป 10 year survival rate 54.8% และจากการศกษาแบบ retrospective ของ Chua และคณะ(37) ในป 1993-2011 จานวน 2,298 คน โดยใหเปน MMC พบ OS 16.3 ป DFS 8.2 ป 10 year survival rate เปน 63% เปนตน
สาหรบ prognostic factor นอกจาก PCI และ
residual tumor เชนเดยวกบ colorectal PC แลว อกปจจย
ทสาคญ คอ histopathologic subtype จากการศกษาของ
Chua และคณะ(37) พบวา 10 year survival ของ DPAM,
hybrid และ PMCA เปน 70, 63 และ 49% ตามลาดบ
COLORECTAL CANCER
PC เปนสาเหตการตายอนดบ 2 ในผปวย colorectal cancer รองจาก liver metastasis หากไมไดรบการรกษา จะม overall survival (OS) ประมาณ 6 เดอน และไมพบอตรารอดใน 5 ป กอนป 2000 การรกษาดวยยาเคมบาบดเชน fluorouracil (5-FU), leucovorin (LV), folinic acid ชวยเพม OS เปน 12.6 เดอน และ 5 ป survival เปน 1% ได(23) ตอมาเมอมการพฒนายาเคมบาบดกลมใหม เชน oxaliplatin, irinotecan รวมท Jง molecular agent เชน bevacizumab, cetuximab, panitumumab พบวาชวยเพม OS เปน 23 เดอน และ 5 ป survival เปน 20-25% ได ปจจบนมกใชเปน combination drug เชน FOLFOX (5-FU + leucovorin + oxaliplatin), FOLFIRI (folinic acid + 5-FU + irinotecan) เปนตน
สาหรบการเปรยบเทยบระหวาง CRS with HIPEC with systemic CMT (study group) กบ systemic CMT alone (control group) จากการศกษาแบบ RCT ของ Verwaal และคณะ(24,25) ในป 1998-2001 จานวน 105 คน แบงเปน study group 54 คน [IP MMC 25 mg/m2, 41-42oC, 90 min] และ control group 51 คน [IV 5-FU + LV x 26 weeks] พบวา study group ใหผลการรกษาทดกวา control group (OS 22.3 vs 12.6 mo; P = 0.032
และ DFS 12.6 vs 7.7 mo) และพบ mortality rate 8% (รป 5) นอกจากนJยงมอกหลายการศกษาทเปน retrospective matched pair study เชน จากการศกษาของ Elias และคณะ(26) ในป 1998-2003 จานวน 96 คน พบวา study group [IP oxaliplatin 460 mg/m2, 43oC, 30 min] ใหผลการรกษาทดกวา control group (OS 62.7 vs

12
รป 7 แสดงการเปรยบเทยบระหวาง CRS with HIPEC กบ
CRS alone ตามดวย systemic CMT regimen เดยวกน
23.9 mo; P < 0.05) และจากการศกษาของ Franko และคณะ(27) ในป 2001-2007 จานวน 105 คน พบวา study group [IP MMC 40 mg/m2] ใหผลการรกษาทดกวา control group (OS 33.7 vs 16.8 mo; P < 0.001) เชนกน
สาหรบการเปรยบเทยบระหวาง CRS with
HIPEC (study group) กบ CRS alone (control group)
ตามดวย systemic CMT regimen เดยวกน จากการศกษา
แบบ case-control study ของ Huang และคณะ(28) ในป
2004-2013 จานวน 62 คน แบงเปน study group 33 คน
[IP MMC 30 mg/m2 + cisplatin 120 mg/m2, 43oC, 90
min] และ control group 29 คน [IV FOLFOX or FOLFIRI]
พบวา survival พบวา study group ใหผลการรกษาทดกวา
control group (OS 13.7 vs 8.5 mo; P = 0.02) และอตรา
การเกดภาวะแทรกซอนใน 2 กลมไมแตกตางกน (P = 0.11) และเมอเปรยบเทยบดาน แสดงใหเหนวาการใช HIPEC
มผลตอ survival ทเพมขJน
นอกจากนJ ยงมอกหลายการศกษาทเปน multicentric study เชน จากการศกษาของ Glehen และคณะ(29)
ในป 1987-2002 จานวน 506 คน พบ median OS เปน 19.2 เดอน และการศกษาของ Elias และคณะ(30) ในป
1990-2007 จานวน 523 คน พบ median OS เปน 30.1 เดอน เปนตน จากการศกษาขางตน แสดงใหเหนวาการรกษา
colorectal peritoneal carcinomatosis ดวย CRS with HIPEC with systemic CMT สามารถเพม survival ไดอยางม
นยสาคญ
HIPEC regimen for colorectal PC
เนองจาก HIPEC ประกอบดวย method, inflow temperature, volume of perfusate, drug, dosage, timing of drug delivery และ total perfusion time ทาใหในแตละสถาบนม HIPEC regimen ทแตกตางกน โดยในPC ทมาจาก gastrointestinal origin นยมใชยาเคมบาบดเปน MMC และ oxaliplatin
สาหรบการเปรยบเทยบระหวาง MMC และ oxaliplatin จากการศกษาแบบ retrospective ของ Prada-Villaverde และคณะ(31) ในป 2000-2012 จานวน 539 คน เปรยบเทยบการใช IP MMC และ oxaliplatin พบวา survival ไมแตกตางกน (OS 32.7 vs 31.4 mo; P = 0.925) แตในกลม PSDSS I/II พบวา MMC ใหผลการรกษาทดกวา (OS 54.3 vs 28.2 mo; P = 0.012) ดงน Jนในผปวยทม low burden of disease (PSDSS I/II) จงแนะนาใหใชเปน MMC based regimen
เนองจากในแตละสถาบนม HIPEC regimen ทแตกตางกน ทาใหการเปรยบเทยบผลการรกษาระหวางสถาบนเปนไปไดยาก ดงน Jนในป 2013 จงไดมการประชมของ The American society of peritoneal surface malignancies (ASPSM)(32) กาหนดเปน Consensus guidelines for colorectal PC โดยใช HIPEC close technique, อณหภม 42oC, volume of perfusate 3 L, mitomycin C 40 mg โดยให 30 mg ท 0 นาท และ 10 mg ท 60 นาท รวม total perfusion time 90 นาท

13
GASTRIC CANCER
Gastric cancer เปนโรคทมการดาเนนโรครนแรง โดยม survival ประมาณ 9-10 เดอน ในกรณทม PC รวมดวย survival จะเหลอเพยง 3-4 เดอน หากรกษาดวย systemic CMT survival จะเพมเปน 3-9 เดอน และไมพบอตรารอดใน 5 ป(38) ในปจจบนยงไมม standard treatment ในการรกษา PC จาก gastric cancer โดยท วไปใชเปน combine systemic CMT เชน FOLFOXIRI (oxaliplatin + irinotecan + 5-FU), ECF (epirubicin + cisplatin + 5-FU) เปนตน
สาหรบการเปรยบเทยบระหวาง CRS with HIPEC with systemic CMT (study group) กบ systemic CMT alone (control group) จากการศกษาแบบ RCT ของ Rudloff และคณะ(39) ในป 2009-2012 จานวน 17 คน แบงเปน study group [IP oxaliplatin 460 mg/m2, 41oC, 30 min] และ control group IV FOLFOXIRI] พบวา study group ใหผลการรกษาทดกวา control group โดยม OS 11.3 เดอนและ 4.3 เดอน ตามลาดบ และพบ mortality rate 11% โดยใน study group พบวาผปวย 4 คน มชวตรอดเกน 12 เดอน ในขณะท control groupไมพบผปวยทมชวตรอดเกน 11 เดอน
สาหรบการเปรยบเทยบระหวาง CRS with HIPEC
with systemic CMT (study group) กบ CRS with systemic
CMT (control group) จากการศกษาแบบ RCT ของ Yang
และคณะ(40) ในป 2011 จานวน 68 คน แบงเปน study
group 34 [IP MMC 30 mg/m2 + cisplatin 120 mg/m2]
และ control group พบวา overall survival ของ study
group มผลการรกษาทดกวา control group เทากบ 11เดอน
และ 6.5 เดอนตามลาดบmo; P = 0.046) และการเกดภาวะแทรกซอนใน 2 กลมไมแตกตางกน (P = 0.839) แสดงให
เหนวาการใช HIPEC มผลตอ survival ทเพมขJน
นอกจากนJ ยงมการศกษาแบบ retrospective ของ Glehen และคณะ(41) ในป 1989-2007 โดยใหเปน MMC
หรอ oxaliplatin พบ OS 9.2 เดอน 1-, 3-, 5- year survival rate เปน 43, 18, 13% ตามลาดบ และการศกษาของ
Yonemura และคณะ(42) ในผปวย 85 คนทไดรบ CRS and HIPEC โดยใหเปน MMC, etopside หรอ cisplatin พบวา
มอตราการรอดชวตใน 1 ปและ 5 ปเทากบ 43% และ 11% ตามลาดบ เปนตน
การรกษา PC จาก gastric cancer ดวย CRS with HIPEC ยงไมไดผลสาเรจทดนก จงไดพฒนาแนวทางการรกษาแบบ multi-modal therapy โดยเรมจาก neoadjuvant intraperitoneal systemic chemotherapy (NIPS) ซงเปนการให neoadjuvant CMT ท Jงทาง IP และ IV ตามดวย cytoreductive surgery, HIPEC และ EPIC โดยการให NIPS น Jน มจดประสงคเพอกาจด peritoneal free cancer cells, ลด staging และเพมโอกาสในการผาตดใหได complete cytoreduction โดยในผปวยทม positive peritoneal lavage หลงการรกษาดวย NIPS พบวา 63% ผลกลายเปน negative peritoneal lavage(43) จากการศกษาแบบ prospective ของ Canbay และคณะ ในป 2005-2012 จานวน

14
194 คน โดยการให NIPS ดวย oral S-1 และ IP cisplatin and docetaxel ตามดวย CRS with HIPEC พบวาสามารถเพม OS เปน 15.8 เดอนได
เนองจาก gastric cancer เปนมะเรงทมการดาเนนโรครนแรง พยากรณโรคไมด การกลบเปนซJาสวนใหญสามารถพบ PC ไดถง 40-50% รวมกบการรกษาดวย CRS with HIPEC เมอตรวจพบ PC แลวไดผลไมดนก ดงน Jนการศกษาในชวงหลงจงมงเนนไปทการใช HIPEC เพอปองกนการเกด PC ซงจากหลาย retrospective study รายงานวาการทา HIPEC สามารถเพมอตราการรอดชวต และลดอตราการกลบเปนซJาไดอยางมนยสาคญ นอกจากนJในป 2014 ไดม study protocol ของการศกษาแบบ RCT ในผปวย locally advanced gastric cancer with serosal invasion ออกมา โดยแบงเปนกลมทรกษาดวย D2 resection with HIPEC และ D2 resection without HIPEC โดยท primary outcome ไดแก overall survival และ secondary outcome ไดแก 3-, 5- year recurrence free survival, localization of recurrence, morbidity และ quality of life ท JงนJเพอพสจนวาการทา HIPEC น Jน สามารถเพมอตราการรอดชวตไดจรงหรอไม OVARIAN CANCER
Epithelial ovarian cancer (EOC) เปนมะเรงทตอบสนองตอการรกษาดวย CMT ไดด ปจจบน standard
treatment คอ CRS with platinum-based systemic CMT ไดแก carboplastin, cisplatin 6 cycle โดยม 5 year
survival rate เปน 39% แตหลงจากรกษาดวย first line แลว พบวา 60% จะม recurrence ใน 12-18 เดอน(44) แบง
ออกเปน 2 กลม คอ platinum-sensitive (DFS > 6 เดอน) และกลม platinum-resistance (DFS < 6 เดอน) ซงม
survival เปน 30 และ 12 เดอน ตามลาดบ(45) โดยสวนมากจะเปน locoregional recurrence และพฒนากลายเปน
กลม platinum-resistance ซงตอบสนองตอ systemic CMT ไมด
สาหรบการเปรยบเทยบระหวาง IP chemotherapy (study group) กบ IV chemotherapy (control group) จากการศกษาแบบ RCT ของ Armstrong และคณะ(46) ในป 1998-2001 ในผปวย optimally debulked stage III ovarian cancer จานวน 415 คน แบงเปน study group [IP cisplatin + paclitaxel] และ control group [IV cisplatin + paclitaxel] พบวา study group ใหผลการรกษาทดกวา control group (OS 65.6 vs 49.7 mo; P = 0.03)
สาหรบการเปรยบเทยบระหวาง CRS with HIPEC with systemic CMT (study group) กบ CRS with systemic CMT (control group) จากการศกษาแบบ RCT ของ Spiliotis และคณะ(47) ในป 2006-2013 ในผปวย recurrence EOC จานวน 120 คน แบงเปน study group 60 คน [IP cisplatin + paclitaxel, 42.5oc, 60 min in platinum-sensitive และ doxorubicin + paclitaxel, 42.5oc, 60 min in platinum-resistant] และ control group 60 คน พบวา study group ใหผลการรกษาทดกวา control group (OS 26.7 vs 13.4 mo; P < 0.006)
สาหรบการเปรยบเทยบระหวาง platinum-sensitive กบ platinum-resistance โดยการรกษาดวย HIPEC จากการศกษาแบบ prospective ของ Bakrin และคณะ(48) จานวน 246 คน พบวาไมมความแตกตางระหวาง 2 กลม (OS 52 vs 48 mo; P = 0.568) และจากการศกษาแบบ retrospective ของ Bakrin และคณะ(45)จานวน 566 คน กไมพบความแตกตางระหวาง 2 กลมเชนกน (OS 51.6 vs 47.2 mo; P = 0.799) โดยเชอวาเปนผลมาจาก HIPEC สามารถออกฤทธ $ไดดกวา systemic CMT

15
แม EOC จะตอบสนองตอ systemic CMT ไดด แตเนองจากม recurrence rate ประมาณ 60% ใน 12-18 เดอน จงมแนวคดทจะใช CRS with HIPEC เปน first line therapy จากการศกษาของ Gonzalez และคณะ(49) ในป 2002-2010 จานวน 42 คน โดยเมอรกษาดวย CRS with HIPEC ในชวงทเปน upfront, first recurrence และ second or subsequent recurrence พบวา OS เปน 77.8, 62.8 และ 35.7 เดอน ตามลาดบ DFS เปน 21.1, 18 และ 5.7 เดอน ตามลาดบ ซงพบวา OS ไมแตกตางกนระหวางกลม upfront และ first recurrence (P = 0.89) แตลดลงอยางมนยสาคญในกลม second or subsequent recurrence (P = 0.02) ดงน Jนในปจจบน CRS with platinum-based systemic CMT ยงคงเปน standard treatment ใน advanced EOC สวน CRS with HIPEC จะเปน secondary procedure หลงการรกษาดวย platinum based systemic CMT ลมเหลว
นอกจากนJ ยงมรายงานการรกษา PC ดวย CRS with HIPEC โดยไมไดแยกตามชนดของ primary tumor อกมากมาย เชน จากการศกษาแบบ retrospective ของ Glehen และคณะ(50) ในป 1989-2007 จานวน 1,290 คน พบ OS 34 เดอน 5 ป survival rate 37% เมอแยกตามชนดของ primary tumor พบวา OS ของ pseudomyxoma peritonei, mesothelioma, colorectal cancer และ gastric cancer เปน 77, 41, 30 และ 9 เดอน ตามลาดบ และจากการศกษาแบบ prospective single center ของ Leviene และคณะ(51) ในป 1991-2013 จานวน 1,000 คน พบ OS 29.4 เดอน 5 ป survival rate เปน 31.5% โดยสรปแลว ในปจจบน CRS with HIPEC เปนอกทางเลอกในการรกษาผปวย peritoneal carcinomatosis จากมะเรงหลากหลายชนด ซงพบวาสามารถเพม survival rate ไดอยางมนยสาคญ โดยม morbidity และ mortality rate ทยอมรบได PROGNOSIS
นอกจาก Completeness of cytoreduction score (CC score) และ PCI ซงเปน prognostic indicator ทสาคญในมะเรงทกชนดดงทกลาวไปขางตนแลว ยงพบวามอกหลายปจจยทสงผลตอ survival outcome ดงนJ(50-52)
- Primary tumor แตกตางกนตามความรนแรงของโรค โดย pseudomyxoma peritonei ม prognosis ดทสด รองลงมาคอ mesothelioma, appendiceal neoplasm, colorectal cancer และ gastric cancer ตามลาดบ
- Learning curve และ institutional experience ยงประสบการณมาก กมโอกาสทจะผาตดใหได complete CRS มาก และโอกาสเกด complication นอย ทาใหได survival outcome ทดตามมา
- Time period of procedure เนองจากมการพฒนาเทคนคในการเลอกผปวยทเหมาะสม และวธการผาตดทดขJน
- Poor prognostic indicator อนๆ ไดแก poor performance status, malignant ascites, bowel obstruction, synchronous peritoneal carcinomatosis, synchronous/previously resected liver metastasis และ unfavorable peritoneal sites เชน small bowel, porta hepatis, diaphragm, retroperitoneal region POST-OPERATIVE MANAGEMENT
การดแลผปวยหลงการผาตด Cytoreductive surgery with HIPEC น Jน ไมแตกตางกบการดแลผปวยหลงการผาตด major surgery อนๆ โดยมแนวทางในการดแล ดงนJ(53-55)
- Monitor การทางานของอวยวะตางๆ

16
- Correct coagulopathy ในกรณทมปญหา - Control pain - IV proton pump inhibitor prophylaxis - Total parenteral nutrition (TPN) - Early nasojejunal enteral nutrition - ปองกน venous thrombosis โดยให low MW heparin และ compression devices - Antibiotics ใหเฉพาะในกรณทมปญหาเรอง post-operative infection
QUALITY OF LIFE (QOL)
เนองจาก CRS with HIPEC เปน extensive surgery จงมโอกาสเกดภาวะแทรกซอนตามมาสง นอกจากนJ ยงมผลตอคณภาพการใชชวตอกดวย จากการประเมนโดยใช Gastrointestinal quality of life index questionnaire (GIQLI) ในชวงกอนผาตด และหลงผาตดท 1, 3, 6 และ 12 เดอน พบวา QOL ลดลงอยางมนยสาคญในชวง 6 เดอนแรก และกลบส baseline ในชวง 12 เดอน โดยปจจยททาให QOL ลดลงในชวง 3, 6 และ 12 เดอน คอ origin of PC, presence of stoma และ recurrence ตามลาดบ(56) นอกจากนJยงมการศกษา QOL หลงจากไดรบการรกษาดวย CRS with HIPEC มาแลว 6-18 เดอน เทยบกบ ผปวยมะเรงทไดรบการรกษาดวยวธอนและอยในชวงของ disease free พบวา QOL ไมแตกตางกน(57)
โดยสรปการทา Cytoreductive surgery (CRS) and Heated Intraperitoneal Chemotherapy มประโยชน
สามารถใชในการรกษาในโรค Pseudomyxoma Peritonei, Peritoneal Mesothelioma, appendiceal
adenocarcinoma Colorectal Peritoneal metastasis สวน Peritoneal metastasis จากอวยวะอน น Jนยงไมมหลกฐาน
เพยงพอวาจะมประโยชนจากการทา CRS รวมกบ HIPEC อยางไรกตามการผาตดเชนนJถอเปนหตถการใหญและม
ความเสยงตอผปวยอยางมากเชนนJ จาเปนตองเลอกผปวยใหเหมาะสม ยงคงตองอาศยขอมลการศกษาเพมเตมตอไป
อกเชนกน

17
REFERENCES.
[1] Glehen O, Mohamed F, Gilly FN. Peritoneal carcinomatosis from digestive tract cancer: new management
by cytoreductive surgery and intraperitoneal chemohyperthermia. Lancet Oncol 2004;5:219e28.
[2] Chua TC, Yan TD, Saxena A, Morris DL. Should the treatment of peritoneal carcinomatosis by
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy still be regarded as a highly morbid
procedure?: a systematic review of morbidity and mortality. Ann Surg 2009;249:900e7
[3] Spratt JS, Adcock RA, Muskovin M, Sherrill W, McKeown J. Clinical delivery system for intraperitoneal
hyperthermic chemotherapy. Cancer Res 1980;40:256e60.
[4] Franco Raviello, Stefano Caruso, Daniele Marelli, et.al. Treatment of peritoneal carcinomatosis with
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: State of the art and future
developments. Surgical oncology 2011; e38-e54.
[5] Piso P, et al. Multimodal treatment approaches for peritoneal carcinosis in colorectal cancer. Deutsches
Arzteblatt international. 2011;108(47):802-8.
[6] Sugarbaker PH. Observations concerning cancer spread within the peritoneal cavity and concepts
supporting an ordered pathophysiology, Peritoneal carcinomatosis: principles and management. Boston:
Kluwer Academic Publishers; 1996. 79e100.
[7] Van der Speeten K, Stuart OA, Sugarbaker PH. Pharmacokinetics and pharmacodynamics of
perioperative cancer chemotherapy in peritoneal surface malignancy. Cancer J 2009;15:216e24.
[8] ] Elias D, Bonnay M, Puizillou JM, Antoun S, Demirdjian S, El Otmany A, et al. Heated intra-operative
intraperitoneal oxaliplatin after complete resection of peritoneal carcinomatosis: pharmacokinetics and tissue
distribution. Ann Oncol 2002;13:267e72.
[9] Koga S, Hamazoe R, Maeta M. Treatment of implanted peritoneal cancer in rats by continuous
hyperthermic peritoneal perfusion in combination with anticancer drugs. Cancer Res 1984;44:1840e2.
[10] Beaujard AC, Glehen O, Caillot JL, Francois Y, Bienvenu J, Panteix G, et al. Intraperitoneal
chemohyperthermia with mitomycin C for digestive tract cancer patients with peritoneal carcinomatosis.
Cancer 2000;88:2512e9.
[11] Macri A, Fortugno A, Saladino E. Rationale and techniques of cytoreductive surgery and peritoneal
chemohyperthermia. World journal of gastrointestinal oncology. 2011;3(12):169-74.
[12] Ceelen WP, Hesse U, Hemptinne B, Pattyn P. Hyperthermic intraperitoneal chemoperfusion in the treatment of locally advanced intra-abdominal cancer. Br J Surg 2000;87:1006e15.

18
[13] Gonzalez-Moreno S, Gonzalez-Bayon LA, Ortega-Perez G. Hyperthermic intraperitoneal chemotherapy:
Rationale and technique. World journal of gastrointestinal oncology. 2010;2(2):68-75.
[14] Boutros et al. World Journal of Surgical Oncology 2010 8:72 doi:10.1186/1477-7819-8-72
[15] Stuart OA, Stephens AD, Welch L, Sugarbaker PH. Safety monitoring of the coliseum technique for
heated intraoperative intraperitoneal chemotherapy with mitomycin C. Annals of surgical oncology.
2002;9(2):186-91.
[16] Al-Quteimat OM, Al-Badaineh MA. Intraperitoneal chemotherapy: Rationale, applications, and limitations. Journal of
oncology pharmacy practice : official publication of the International Society of Oncology Pharmacy Practitioners. 2013.
[17] Stewart 4th JH, Shen P, Levine EA. Intraperitoneal hyperthermic chemotherapy for peritoneal surface malignancy: current status and future directions. Ann Surg Oncol 2005;12:765e77. [18] Gilly FN, Carry PY, Sayag AC. Regional chemotherapy with mitomycin C and intraoperative hyperthermia for digestive cancers with peritoneal carcinomatosis. Hepatogastroenterology 1994;41:124e9. [19] Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. In: Sugarbaker PH, editor. Peritoneal carcinomatosis: principles of management. Boston, USA: Kluwer Academic Publishers; 1996. p. 359e74. [20] Sugarbaker PH. Intraperitoneal chemotherapy and cytoreductive surgery for the prevention and treatment of peritoneal carcinomatosis and sarcomatosis. Semin Surg Oncol 1998;14:254e61. [21] Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res 1996; 82:359e74. [22] Bijelic L, Jonson A, Sugarbaker PH. Systematic review of cytoreductivesurgery and heated intraoperative intraperitoneal chemotherapy for treatment of peritoneal carcinomatosis in primary and recurrent ovarian cancer. Ann Oncol 2007;18:1943e50. [23] Macri A, Saladino E, Bartolo V, Adamo V, Altavilla G, Mondello E, et al. Peritoneal carcinomatosis of colorectal origin. World journal of gastrointestinal oncology. 2010;2(2):98-101. [24]Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van Tinteren H, Boot H, et al. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2003;21(20):3737-43. [25] Verwaal VJ, Bruin S, Boot H, van Slooten G, et al. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Annals of surgical oncology. 2008;15(9):2426-32. [26] Elias D, Lefevre JH, Chevalier J, Brouquet A, Marchal F, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2009;27(5):681-5. [27] Franko J, Ibrahim Z, Gusani NJ, Holtzman MP, Bartlett DL, Zeh HJ, 3rd. Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion versus systemic chemotherapy alone for colorectal peritoneal carcinomatosis. Cancer. 2010;116(16):3756-62

19
[28] Huang CQ, Feng JP, Yang XJ, Li Y. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from colorectal cancer: a case-control study from a Chinese center. Journal of surgical oncology. 2014;109(7):730-9. [29] Glehen O, Kwiatkowski F, Sugarbaker PH, Elias D, Levine EA, De Simone M, et al. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2004;22(16):3284-92. [30] Elias D, Gilly F, Boutitie F, Quenet F, Bereder JM, Mansvelt B, et al. Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2010;28(1):63-8. [31] Prada-Villaverde A, Esquivel J, Lowy AM, et al. The American Society of Peritoneal Surface Malignancies evaluation of HIPEC with Mitomycin C versus Oxaliplatin in 539 patients with colon cancer undergoing a complete cytoreductive surgery. Journal of surgical oncology. 2014;110(7):779-85. [32] Turaga K, Levine E, Barone R, et al. Consensus guidelines from The American Society of Peritoneal Surface Malignancies on standardizing the delivery of hyperthermic intraperitoneal chemotherapy (HIPEC) in colorectal cancer patients in the United States. Annals of surgical oncology. 2014;21(5):1501-5. [33] Bevan KE, Mohamed F, Moran BJ. Pseudomyxoma peritonei. World journal of gastrointestinal oncology. 2010;2(1):44-50. [34] Moran B, Baratti D, Yan TD, Kusamura S, Deraco M. Consensus statement on the loco-regional treatment of appendiceal mucinous neoplasms with peritoneal dissemination (pseudomyxoma peritonei). J Surg Oncol 2008;98:277e82. [35] Andreasson H, Graf W, Nygren P, Glimelius B, Mahteme H. Outcome differences between debulking surgery and cytoreductive surgery in patients with Pseudomyxoma peritonei. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2012;38(10):962-8. [36] Elias D, Gilly F, Quenet F, Bereder JM, Sideris L, Mansvelt B, et al. Pseudomyxoma peritonei: a French multicentric study of 301 patients treated with cytoreductive surgery and intraperitoneal chemotherapy. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2010;36(5):456-62. [37] Chua TC, Moran BJ, Sugarbaker PH, Levine EA, Glehen O, Gilly FN, et al. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2012;30(20):2449-56. [38] Canbay E, Mizumoto A, Ichinose M, Ishibashi H, Sako S, Hirano M, et al. Outcome data of patients with peritoneal carcinomatosis from gastric origin treated by a strategy of bidirectional chemotherapy prior to cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in a single specialized center in Japan. Annals of surgical oncology. 2014;21(4):1147-52.

20
[39] Rudloff U, Langan RC, Mullinax JE, Beane JD, Steinberg SM, Beresnev T, et al. Impact of maximal cytoreductive surgery plus regional heated intraperitoneal chemotherapy (HIPEC) on outcome of patients with peritoneal carcinomatosis of gastric origin: results of the GYMSSA trial. Journal of surgical oncology. 2014;110(3):275-84. [40] Yang XJ, Huang CQ, Suo T, Mei LJ, Yang GL, Cheng FL, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: final results of a phase III randomized clinical trial. Annals of surgical oncology. 2011;18(6):1575-81. [41] Glehen O, Gilly FN, Arvieux C, Cotte E, Boutitie F, Mansvelt B, et al. Peritoneal carcinomatosis from gastric cancer: a multi-institutional study of 159 patients treated by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Annals of surgical oncology. 2010;17(9):2370-7. [42] Yonemura Y, Fujimura T, Nishimura G, FallaR Sawa T, Katayama K, Tsugawa K, et al. Effects of intraoperative chemohyperthermia in patients with gastric cancer with peritoneal dissemination. Surgery 1996;119:437e44. [43] Yonemura Y, Elnemr A, Endou Y, Hirano M, Mizumoto A, Takao N, et al. Multidisciplinary therapy for treatment of patients with peritoneal carcinomatosis from gastric cancer. World journal of gastrointestinal oncology. 2010;2(2):85-97. [44] Fagotti A, Gallotta V, Romano F, Fanfani F, Rossitto C, Naldini A, et al. Peritoneal carcinosis of ovarian origin. World journal of gastrointestinal oncology. 2010;2(2):102-8. [45] Bakrin N, Bereder JM, Decullier E, Classe JM, et al. Peritoneal carcinomatosis treated with cytoreductive surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for advanced ovarian carcinoma: a French multicentre retrospective cohort study of 566 patients. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2013;39(12):1435-43. [46] Armstrong DK, Bundy B, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. The New England journal of medicine. 2006;354(1):34-43. [47] Spiliotis J, Halkia E, Lianos E, Kalantzi N, Grivas A, Efstathiou E, et al. Cytoreductive Surgery and HIPEC in Recurrent Epithelial Ovarian Cancer: A Prospective Randomized Phase III Study. Annals of surgical oncology. 2014. [48] Bakrin N, Cotte E, Golfier F, Gilly FN, Freyer G, Helm W, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for persistent and recurrent advanced ovarian carcinoma: a multicenter, prospective study of 246 patients. Annals of surgical oncology. 2012;19(13):4052-8. [49] Gonzalez Bayon L, Steiner MA, Vasquez Jimenez W, Asencio JM, Alvarez de Sierra P, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for the treatment of advanced epithelial ovarian carcinoma: upfront therapy, at first recurrence, or later? European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2013;39(10):1109-15. [50] Glehen O, Gilly FN, Boutitie F, Bereder JM, et al. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy: a multi-institutional study of 1,290 patients. Cancer. 2010;116(24):5608-18.

21
[51] Levine EA, Stewart JHt, Shen P, Russell GB, Loggie BL, Votanopoulos KI. Intraperitoneal chemotherapy for peritoneal surface malignancy: experience with 1,000 patients. Journal of the American College of Surgeons. 2014;218(4):573-85. [52] Cavaliere F, De Simone M, Virzi S, Deraco M, et al. Prognostic factors and oncologic outcome in 146 patients with colorectal peritoneal carcinomatosis treated with cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy: Italian multicenter study S.I.T.I.L.O. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2011;37(2):148-54. [53] Cooksley TJ, Haji-Michael P. Post-operative critical care management of patients undergoing cytoreductive surgery and heated intraperitoneal chemotherapy (HIPEC). World journal of surgical oncology. 2011;9:169. [54] Webb CA, Weyker PD, Moitra VK, Raker RK. An overview of cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion for the anesthesiologist. Anesthesia and analgesia. 2013;116(4):924-31. [55] Saxena A, Yan TD, Morris DL. A critical evaluation of risk factors for complications after cytoreductive surgery and perioperative intraperitoneal chemotherapy for colorectal peritoneal carcinomatosis. World journal of surgery. 2010;34(1):70-8. [56] Passot G, Bakrin N, Roux AS, Vaudoyer D, Gilly FN, Glehen O, et al. Quality of life after cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy: a prospective study of 216 patients. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2014;40(5):529-35. [57] Tan WJ, Wong JF, Chia CS, Tan GH, Soo KC, Teo MC. Quality of life after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: an Asian perspective. Annals of surgical oncology. 2013;20(13):4219-23. [58]Van Leeuwen B, Graf W, Påhlman L, Mahteme H. Swedish experience with Peritonectomy and HIPEC.
HIPEC in peritoneal carcinomatosis. Ann Surg Oncol. 2007; 15: 745-753.