Embed Size (px)
Citation preview

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
348
LICHTENSTEIN HERNIOPLASTY USING
POLYPROPYLENE-POLIGLECAPRONE 25 COMPOSITE
MESH IN BILATERAL INGUINAL HERNIA
IBRAHIM ABDEL GHAFFAR
Department Of General Surgery, Faculty of Medicine, Al-Azhar University
ـــــــــــــــــــــــــــــــــــــ ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ABSTRACT
Objective: To evaluate the lightweight composite mesh of polypropylene-
poliglecaprone (Ultrapro®) mesh in bilateral inguinal hernia repair
(Lichtenstein technique) as regard outcome and complications. Study design: A
prospective, interventional study conducted on 27 patients in Al-Azhar
University Hospitals from 2009 to 2012. Materials and Methods: During study
period, male patients with primary non complicated bilateral inguinal hernia,
between 20 and 65 years of age, and fit for surgery, were selected. Bilateral
Lichtenstein procedure using Ultrapro® mesh was done. Patients were followed
up for twelve months, on weekly basis for one month then every three months.
Intraoperative findings, postoperative complications including pain, recurrence,
and patients' satisfaction, were thoroughly assessed. Results: All patients were
males with mean age of 57.6 years and median duration of symptoms of 7.4
years. The majority of hernias were of funicular and complete scrotal types and
of type III according to the Nyhus classification. Mean operative time was
ninety minutes, without significant intraoperative complications. Mean hospital
stay was 1.5 days. Postoperative pain was easily controlled with analgesics.
Postoperative complications were; urine retention (two patients, 7.4%), mild
scrotal edema (four patients, 14.81%), superficial ecchymosis of the wound (two
patient, 7.4%), unilateral seroma (three patient, 11.11%), numbness at the
upper medial side of the thigh (two patients, 7.4%), and feeling of foreign body
(one patient, 3.7%). As regards to postoperative pain; twenty three patients

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
349
(85.18%) were pain free after 1 month post operatively, additional two patients
(92.95%) were pain free after 3 months, one patient (3.7%) had intermittent
pain for six months and one (3.7%) for nine months (not interfering with
activities in both). Mean period for return to normal activity was three weeks. In
all patients postoperative complications were disappeared at the end of follow
up period with no recurrence. Conclusion: Bilateral inguinal hernioplasty
using Ultrapro® lightweight mesh is effective and successful with encouraging
results and minimal complications.
Key words: Bilateral inguinal hernia, Lichtenstein hernioplasty, polypropylene-
poliglecaprone (Ultrapro®) mesh.
INTRODUCTION
Inguinal hernia is among the most common problems encountered by
general surgeons and may have significant complications.(1) Globally, inguinal
hernia is the most common type of hernia, comprising of approximately 75% of
all abdominal wall hernias.(1-3) Surgery is indicated to prevent complications. (4)
Fortunately, most inguinal hernias are repaired electively. (5,6) Inguinal hernia
repair accounting for 10 to 15% of all surgical procedures and is the second
most common surgical procedure after appendicectomy. (3,7) It has been
estimated that worldwide over 20 million repairs of inguinal hernia are carried
out each year, the specific operation rates varying between countries from
around 100–300 per 100 000 population per year .(8)
Several methods of inguinal hernia repair have been developed over the
years to improve the outcome, the most important being the Lichtenstein mesh
repair (9,10) and laparoscopic mesh repair. (10,11) Better results are obtained with
Lichtenstein (mesh) repair including rapid return to normal activities (12) and low
recurrence rate (less than 1%). (12,13)
Today, some strong recommendations exist in favor of Lichtenstein repair.
American College of Surgeons choose this technique as "gold standard" (9),

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
350
while National Institute of Clinical Excellence [NICE] from UK (14) and The
National Agency for Accreditation and Evaluation in Health [ANAES] from
France (15) recommended it for inguinal hernia repair. It is easy to learn and
perform. (16) The Lichtenstein Hernia Institute and the British Hernia Centre
reported very low recurrence rates in thousands of cases. (17,18)
Bilateral hernias are another specific issue. The European Hernia Society
(EHS) recommends Lichtenstein and endoscopic repairs. (19) It is widely
believed that the surgical trauma of a one-stage bilateral inguinal hernia repair
results in a greater degree of postoperative pain and an increase in wound
infection, when compared with sequential unilateral repairs. Several authorities
favor sequential repair, and in the past this has been accepted practice.
However, retrospective reviews have indicated that simultaneous repair may be
performed with no greater morbidity than sequential repair. There is no
difference in the long-term recurrence rates after bilateral simultaneous and
unilateral repair. The main advantage of simultaneous over sequential bilateral
hernia repairs is that only one admission, one anaesthesia, one operation and one
period of convalescence are required. This enables a more efficient use of
hospital beds, and as a result there is an economic saving to both the patient and
the hospital. In addition the risk of strangulation on the unoperated side is
eliminated. (20)
Usher first introduced polypropylene prosthetics for inguinal hernia in the
late 1950s, however, the wide acceptance of them took place in 80's following
Lichtenstein's report of very successful results. Meshes have decreased the rate
of recurrence significantly, but some problems related to meshes have been
reported. A hernia mesh has certain features like material, strength, elasticity,
density, pore size. Standard polypropylene (PP) mesh is the most frequently
used one. It is cheap, available in most institutions, non-absorbable, and strong
enough to avoid recurrence. Nevertheless, some actual problems with mesh use

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
351
like foreign body sensation and chronic postoperative pain have created a
conflict about standard polypropylene mesh. Polyester mesh might be an
alternative, but it could not gain popularity. Polyester meshes can degrade by
time especially in infected areas. (21) Newer lighter meshes have been produced
to overcome those problems. (22)
Partially absorbable meshes have two components. Polypropylene non
absorbable part does not lose its strength at all. The other half is absorbed within
12 weeks. (23) Eventually less foreign material is left in situ, while the remaining
mesh can still provide a sufficient mechanical barrier against recurrence. (24)
The use of partially absorbable light weight meshes could be associated with
reduced feeling of a foreign body. (25)
Lightweight meshes are designed to mimic the physiology of the
abdominal wall and the inguinal region. (26,27) Meshes in this group are produced
with small polymer fibers, large pores (>1 mm) and a high flexibility. The
tensile strength is adapted to that of local tissues and the surface area in contact
with the host tissues is low. A welcome and major side effect of the sensitive
mechanical adoption of these meshes to the abdominal wall is a significant
reduction of scar tissue formation resulting in a long-term flexible repair. (27,28)
Flexible lightweight mesh constructions with similar elasticity to the anterior
abdominal wall demonstrate their superiority with respect to a physiologic
abdominal wall repair. (29)
Monocryl (poliglecaprone 25) is a monofilament derived from a segmented
copolymer of caprolactone and glycolide. This complex polymeric system
contains soft segments of polyglycolide that provide high strength. Both hard
and soft segments are combined in the same polymeric chain. Evaluating the
toxicity potential of Monocryl suture, no genotoxic, cytotoxic, teratogenic,
irritating or allergic effects were found. As suture material it was introduced in
1995 and since then it demonstrated many preferable qualities including a

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
352
significantly lowered tissue reaction in the early phases of wound healing
compared with polyglactine 910 (vicryl). Monocryl is essentially absorbed
without increased cellularity, inflammatory and fibrotic reaction within 84-140
days. (30)
The monocryl poylpropylene composite mesh is currently the member of
the lightweight large porous mesh family with the lowest foreign body reaction
and optimized handling. The clinical studies produced encouraging results to
move forward with this mesh concept. (31)
MATERIALS AND METHODS
Population
This was a prospective, interventional study performed at the department
of surgery, Al-Azhar university hospitals from 2009 to 2012. Twenty seven
patients with bilateral inguinal hernias were eligible for the study. All patients
were males with mean age of 57.6 years.
Inclusion criteria: Clinical diagnosis of bilateral inguinal hernia, any
grade, both types (direct, indirect), primary, not complicated in fit males, age
between 20 and 65 years.
Exclusion criteria: Abnormal laboratory tests; increased intra-abdominal
pressure, patients declared unfit for general or spinal anesthesia and surgery due
to other co-morbid factors.
Study protocol
All patients were interviewed with a standardized questionnaire, and had a
physical examination. The questionnaire inquired about the hernia history as
regard causes, onset, previous complications or repair and history of diseases
that cause increased intra-abdominal pressure.
Complete physical examination (general and local) including PR
examination was done to all patients. Complete laboratory tests, ECG, chest X
ray and abdominopelvic ultrasound were done for all patients.

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
353
Lichtenstein hernioplasty using monocryl polypropylene composite mesh
for bilateral inguinal hernia was planned for all cases. Patients were completely
counseled regarding the procedure, outcome and possible complications. A
written consent was taken.
The procedure
Patients were admitted a day prior to surgery. Assessment for
general/spinal anesthesia was done. Preoperative preparations as (shaving of
pubic hair, fasting 8 hours before surgery) were done. Intravenous Antibiotic
(third generation cephalosporin) was given at the induction of anesthesia as
prophylaxis. The operations were carried out under general/spinal anesthesia.
Standard 6x11cm mesh was inserted on both sides. Fixation of the mesh was
done by prolene 2/0. Drain was inserted on demand (according to size of the
hernia, dissection and hemostasis).
During surgery the procedure followed was meticulous and precise. It was
ensured that all the recommended precautions are taken. Effective postoperative
analgesia was ensured. Scrotal elevator was prescribed for one week to decrease
scrotal oedema. After their discharge from hospital, patients were followed up
on weekly basis for four weeks, then every three months for one year. They
were also advised to avoid any predisposing factors that increase intra-
abdominal pressure; straining (cough, constipation), lifting heavy objects and
hard working for at least three months. Mild laxative and systemic antibiotic
were prescribed.
At follow-up, patients were interviewed with the same standardized
questionnaire used before, which included additional items related to surgery
satisfaction and complications. During every visit the patients were physically
examined for the outcome of the procedure including early, late complications,
pain assessment (based on Inguinal Pain Questionnaire, IPQ) (32) and recurrence.
RESULTS

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
354
A total of 27 consecutive patients scheduled for Lichtenstein hernioplasty
using monocryl polypropylene composite mesh for bilateral inguinal hernia.
They were between 20 and 65 years of age with a mean age of 57.6 years. The
commonest age group in this study was from 50 to 60 years [16 patients
(59.25%)]. All patients were males with symptomatic hernias. The median
duration of symptoms was 7.4 years. The majority of hernias were of funicular
and complete scrotal types and of type III according to the Nyhus classification.
Seven patients (25.9%) presented with scrotal type on both sides, six patients
(22.22%) with scrotal type on one side and funicular on the contralateral side,
six patients (22.22%) with funicular type on both sides, four patients (14.81%)
with scrotal type on one side and bubonocele on the contralateral side, two
patients (7.4%) with funicular type on one side and bubonocele on the
contralateral side and two patients (7.4%) with bubonocele bilaterally. Three
patients (11.11%) presented with associated unilateral vaginal hydrocele and
two patients (7.4%) with bilateral vaginal hydrocele (Table 1).
Table (1): Patient demographics
No. (%) Parameter
57.6 years Mean age
16 patients (59.25%) Commonest age group (50-60 Y)
7.4 years Median duration of symptoms
Seven patients (25.9%)
Six patients (22.22%)
Four patients (14.81%)
Six patients (22.22%
Two patients (7.4%)
Two patients (7.4%)
Type of hernia;
Bilateral Scrotal
Scrotal- funicular
Scrotal-bubonocele
Bilateral Funicular
Funicular-bubonocele
Bilateral bubonocele
Two patients (7.4%)
Three patients (11.11%)
Associated vaginal hydrocele;
Bilateral
Unilateral

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
355
The analysis of the results was based on:
1- The operative and early postoperative finding.
The median duration of surgery was 90 minutes (range, 80–100 minutes).
Intraoperative hernias were of direct, indirect and combined types. In nine
patients (33.33%) the hernia was direct on both sides, In eight patients (29.62%)
it was indirect on both sides, In three patients (11.11%) it was direct on one side
and indirect on the contralateral side, In three patients (11.11%) it was
combined on one side and indirect on the contralateral side, In two patients
(7.4%) it was combined on one side and direct on the contralateral side, In two
patients (7.4%) it was combined on both sides. Postoperative pain was mild in
ten patients (37.03%), moderate in fifteen (55.55%), severe in two patients
(7.4%) and was controlled in all patients by non-steroidal anti-inflammatory
drugs (diclofenac sodium 75 mg i. m. injection). The mean hospital stay after
surgery was 1.5 days (Table 2).
Table (2): Operative findings and outcome
Mean time / No. (%) Parameter
90 minutes Operative time
1.5 days Hospital stay
Nine patients (33.33%)
Eight patients (29.62%)
Two patients (7.4%)
Three patients (11.11%)
Two patients (7.4%)
Three patients (11.11%)
Type of hernia;
Bilateral direct
Bilateral indirect
Bilateral combined
Direct-indirect
Direct-combined
Indirect-combined
Three weeks Return to normal activity
There was no mortality, intraoperative or postoperative significant
bleeding, two patients (7.4%) developed urine retention and treated with
catheterization, two patients (7.4%) developed superficial ecchymosis in the
wound and were treated conservatively and four patients (14.81%) developed
mild scrotal edema (resolved spontaneously).

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
356
2- The development of complications.
The average time for return to normal daily activity was three weeks.
Complications like hematoma, secondary hydrocele, ischemic orchitis, testicular
atrophy, dysejaculation syndrome, wound sepsis, mesh migration, rejection,
erosion and fistula formation were not observed. Three patients (11.11%)
developed unilateral seroma. Two patients (7.4%) developed numbness at the
upper medial side of the thigh. One patient (3.7%) experienced a feeling of
foreign body by the third month (Table 3).
Table (3): Complications of the procedure
No. (%) Parameter
2 (7.4%) Urine retention
4 (14.81%) Mild scrotal edema
2 (7.4%) Superficial ecchymosis of the wound
3 (11.11%) Unilateral seroma
2 (7.4%) Numbness at the upper medial side of the thigh
1 (3.7) Feeling of foreign body
0 (0%)
Hematoma, secondary hydrocele, ischemic
orchitis, testicular atrophy, dysejaculation
syndrome, wound sepsis and Mesh migration,
rejection, erosion and fistula formation.
0 (0%) Recurrence
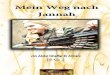
As regards to post-operative pain; twenty three patients (85.18%) were
pain free at 1 month post operatively, additional two patients (92.95%) were
pain free at 3 months, one patient (3.7%) had intermittent pain that lasted for six
months (not interfering with activities) and one patient (3.7%) experienced pain
for up to nine months (not interfering with activities) (Figure 1).
Figure (1): Resolution of pain post operatively

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
357
At the end of the follow up period all patients showed complete cure, no
residual pain, were satisfied by surgery and no recurrence was reported.
DISCUSSION
Inguinal hernia repairs consume an important part of health care resources
because of the high incidence of the problem. (33) Every recurrence after a
primary repair will add an extra cost to health care economics. Moreover,
secondary or tertiary operations after previous repairs carry higher risk of re-
recurrence and specific complications like testicular atrophy. Therefore, every
surgeon should know and perform a current repair method successfully in his
daily practice. (24)
Since Bassini published his original description of inguinal hernia repair in
1887, many techniques for hernia repair such as Shouldice, Darning, modified
Bassini, Lichtenstein and laparoscopic repair have been published. (5,7,8,34-36)
Laparoscopic and Lichtenstein mesh repair are becoming popular in recent days
(36) as they are associated with rapid return to normal activities with low
recurrence rates. (12)
Most studies of postoperative complications after bilateral hernia repair
have been retrospective. These are likely to be inaccurate because of incomplete
recording. Only a prospective comparison can answer the question whether
there is greater morbidity after simultaneous or sequential repair. The study of
Jarrett et al. (20) is the first to describe such a prospective assessment. They have
compared bilateral simultaneous repair with bilateral sequential repairs, and also
with unilateral repair. They conclude that patients undergoing bilateral
simultaneous inguinal hernia repair are not subject to an increased postoperative
morbidity as a consequence of the bilateral repair.
Miller and colleagues (37) demonstrated that the simultaneous repair of
bilateral inguinal hernias is safe and does not result in an increased recurrence
rate. In the present study neither significant increase in operative time (median

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
358
90 minutes), hospital stay (median 1.5 days) nor increased intraoperative and
postoperative morbidity related to the simultaneous repair were recorded.
Postoperative pain and recovery period of the bilateral open tension-free
hernioplasty are equally comparable with those of laparoscopic repair. (38) In
patients presenting with large chronic or recurrent hernias, laparoscopy is often
technically challenging because the difficulties associated with reduction of the
hernia or adhesions. Prior abdominal interventions (e.g. appendectomy) often
complicate laparoscopic dissection. (39)
Additionally, the long-term recurrence rate of 0.1% for tension-free repair
is significantly lower than the 1% to 4% short-term recurrence rate of the
laparoscopic technique. (40-42) More importantly, the tension-free procedure is not
associated with the reported complications of laparoscopic hernia repair, such as
massive bleeding, intestinal perforation, bladder perforation, small bowel
obstruction, trocar site herniation, seroma formation, nerve injuries (as high as
15%), and even death. (42) These complications, which are continuously reported
in the literature, are extremely rare, or even unheard of, with the open hernia
repair. (38) In the present study postoperative pain was tolerable and easily
controlled by simple analgesics, no major intraoperative complication such
related to laparoscopic repair were reported.
The lightweight large porous meshes have less surface area than the
heavyweight group, consequently, the foreign body reaction (FBR) in
lightweight mesh is significantly reduced. In addition to this significantly
decrease typical chronic inflammatory reaction, the fibrotic reaction around the
mesh in total as well as around each mesh fiber is greatly reduced. The fibrotic
reaction as a result of the inflammatory response, however, considerably
influences the long term quality of the hernia repair. (30)
Ultrapro® represents a new member of the lightweight large porous mesh
group. The mesh is constructed of a monofilament lightweight large porous PP

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
359
mesh with pores of more than 3 mm. An absorbable monocryl (poliglecaprone
25) component is added to improve handling characteristics and to optimize
implantation and increased tensile strength in the first week of repair.
Interestingly, the supplement of PP with Monocryl leads to significantly
decreased FBR compared with simple lightweight large porous PP meshes with
identical textile structure; an effect still under investigation. (30)
Two randomized studies (43,44) reported that use of a partially absorbable
lightweight mesh was associated with less chronic pain than a nonabsorbable
heavy mesh after 1 and 3 years. The frequency of recurrence was similar for the
two meshes. Mike and his colleagues (45) concluded that patients with inguinal
hernia who undergo Ultrpro repair have fewer recurrence and less chronic
inguinal pain than those who undergo conventional open repair by conventional
polypropylene mesh.
In the present study a technique of Lichtenstein hernioplasty using ultrapro
mesh was done for 27 patients with bilateral inguinal hernia. Intra-operative
finding, early postoperative and late complications were evaluated over a follow
up period of one year.
As regard operative time, intra-operative complications, hospital stay and
return to normal activity all were satisfactory. Postoperative complications
were insignificant; urine retention (two patients), mild scrotal oedema (four
patients), superficial ecchymosis in the wound (two patients), unilateral seroma
(three patients), numbness at the upper medial side of the thigh (two patients)
and feeling of foreign body (one patient). Postoperative pain was mild to
moderate except in two patients (severe pain). The resolution of postoperative
pain was encouraging; twenty three patients were pain free at one month, twenty
five patients at 3 months, one of the remaining two patients was free from pain
by the sixth month, the other by the ninth month and in both the pain was not
interfering with activities.

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
360
At the end of follow up time all operated patients were satisfied and
showed complete improvement with no recurrence reported.
CONCLUSION
Bilateral inguinal hernioplasty using Ultrapro® lightweight mesh is
effective and successful with encouraging results and minimal complications.

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
361
REFERENCES
1. Garba ES (2000). The patterns of adult external abdominal hernias in Zaria.
Nig J Surg Res. 5(1):12–5.
2. Williams NS, Bulstrode CJK, O’Connell PR (2008). Bailey & Love’s Short
Practice of Surgery. 25. London: Hodder Arnold.
3. Primatesta P, Golacre MJ (1996). Inguinal hernia repair, incidence of
elective and emergency surgery. Int J Epidemol. 5:835–9.
4. Mann CV, Russel RCG, William NS. (eds) (2004). Hernia in Bailey and
Love, Short practice of surgery, 24th edition, London Champion Hall (ch:
73).
5. Watkin D Kirk R (2000). Abdominal wall and groin. In: General Surgical
Operations RM Kirk; 4thed. New York: Churchill Living Stone; 117-40.
6. Gallegos NC, Dawsen J, Jarvis M (1991). Risk of strangulation in groin
hernia. Br J. 78:1171-3.
7. Schools IG, Van Dijkman B, Butzelaar RM, Van Geldere D, Simons MP
(2001). Inguinal hernia repair in Amsterdam region. Hernia. 5(1):37–40.
8. Kingsnorth AN, LeBlanc KA (2003). Management of abdominal hernias. 3.
New York: Edward Arnold, London; pp. 4047.
9. Amid PK (2004). Pioneers in Hernia Surgery. Lichtenstein tension free
hernioplasty: Its inception, evolution, and principles. Hernia. 8: 1-7.
10. Cervantes J (2004). Inguinal Hernia in the New Millennium. World J
Surg. 28: 343-7.
11. Seid AS, Amos E (1994). Entrapment neuropathy in laparoscopic
herniorrhaphy. Surg Endosc. 8: 1050-3.
12. EU Hernia Trialists Collaboration (2002). Repair of groin hernia with
synthetic mesh: meta-analysis of randomized controlled trials. Ann Surg.
325(3):322–32.

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
362
13. Gourgiotis S, Germanos S, Stratopoulos C, Moustafellos P, Panteli A
(2006). Lichtenstein tension-free repair of inguinal hernia. Chirurgia
(Bucur). 101:509-12.
14. National Institute of Clinical Excellence (NICE) (2004). Final appraisal
determination, laparoscopic surgery for inguinal hernia repair. London.
15. The National Agency for Accreditation and Evaluation in Health (ANAES)
(2000). Clinical and economic evaluation of laparoscopic surgery in the
context of inguinal hernia repair. Paris.
16. Paajanen H, Varjo R (2010). Ten-year audit of Lichtenstein hernioplasty
under local anaesthesia performed by surgical residents. BMC Surg. 10:24.
17. Amid PK, Shulman AG, Lichtenstein IL (1996). Open "tension-free" repair
of inguinal hernias: the Lichtenstein technique. Eur J Surg. 162:447–53.
18. Kurzer M, Belsham PA, Kark AE (2003). The Lichtenstein repair for
groin hernias. Surg Clin North Am. 83:1099–117.
19. Simons MP, Aufenacker T, Bay-Nielsen M, Bouillot JL, Campanelli G,
Conze J (2009). European Hernia Society guidelines on the treatment of
inguinal hernia in adult patients. Hernia. 13:343–403.
20. Jarrett PE, Serpell JW, Johnson CD (1990). A prospective study of bilateral
inguinal hernia repair. Annals of the Royal College of Surgeons of England.
vol. 72, 299-303.
21. Earle DB, Mark LA (2008). Prosthetic material in inguinal hernia repair:
how do I choose? Surg Clin North Am. 179–201.
22. Shah BC, Goede MR, Bayer R, Buettner SL, Putney SJ, McBride CL
(2009). Does type of mesh used have an impact on outcomes in laparoscopic
inguinal hernia? Am J Surg. 198:759–64.
23. Rosch R, Junge K, Quester R, Klinge U, Klosterhalfen B, Schumpelick V
(2003). Vypro II mesh in hernia repair: impact of polyglactin on long-term
incorporation in rats. Eur Surg Res. 35:445–50.

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
363
24. Kulacoglu H (2011). Current options in inguinal hernia repair in adult
patients. Hippokratia Med J. 15(3): 223–31.
25. Gao M, Han J, Tian J, Yang K (2010). Vypro II mesh for inguinal hernia
repair: a meta-analysis of randomized controlled trials. Ann Surg. 251:838–
42.
26. Klinge U. Klosterhalfen B, Conze J (1998). A modified mesh for hernia
repair adapted to abdominal wall physiology. Eur. J. Surg. 164, 951-60.
27. Klinge U, ConzeJ, Klosterhalfen B (1996). Alteration of abdominal wall
mechanics after mesh implantation. Experimental alteration of mesh
stability. Langenbecks Archly Fur hirwgle; 381, 323—32.
28. Klosterhalfen B, Klinge U, Ienze U (1997). Morphological correlation of
the functional mechanics of the abdominal wall after mesh implantation.
Langenbecks Archly Fur Chirurgie; 382, 87—94.
29. Klinge U, Muller M, Brucker C, Schumpelick V (1998). Application of
three dimensional stereography to assess abdominal wall motility. Hernia 2,
11-4.
30. Klosterhalfen B, Junge K, Klinge U (2005). The lightweight and large
porous mesh concept for hernia repair. J. Invest, Surg. 15, 319-28.
31. Holzheimer RG (2004). First results of Lichtenstein hernia repair with
Ultrapro mesh as cost saving procedure-quality control combined with a
modified quality of life questionnaire (SF-36) in a series of ambulatory
operated patients. Eur. J. Med. Res. 9, 323–7.
32. Franneby U (2008). ―Validation of an Inguinal Pain Questionnaire for
Assessment of Chronic Pain after Groin Hernia Repair,‖ British Journal of
Surgery, Vol. 95, No. 4, pp. 488-93.
33. Fitzgibbons RJ, Richards AT, Quinn TH (2002). Open hernia repair. In:
Souba WS, Mitchell P, Fink MP, Jurkovich GJ, Kaiser LR, Pearce WH,

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
364
Pemberton JH, Soper NJ, editors. ACS Surgery: Principles and Practice. 6th
ed. Philadelphia, U.S.A: Decker Publishing Inc; pp. 828–49.
34. Gulzar MR, Iqbal J, Ulhaq MI, Afzal M (2007). Darning versus Bassini
repair for inguinal hernia; a prospective comparative study. Professional
Med J. 5(1):128–33.
35. Maggiore D, Muller G, Hafanki J (2001). Bassini versus Lichtenstein two
basic techniques for inguinal hernia repair. Hernia. 5(1):21–24.
36. Lal P, Kajla RK (2003). Laparoscopic total extra-peritoneal versus open
Lichtenstein inguinal hernia repair. J Surg Enosc. 5:850–6.
37. Miller AR, van Heerden JA, Naessens JM, O’Brien PC (1991).
Simultaneous bilateral hernia repair. A case against conventional wisdom.
Ann Surg. 213:272-6.
38. Amid PK, Shulman AG, Lichtenstein IL (1996). Simultaneous Repair of
Bilateral Inguinal Hernias under Local Anesthesia. Ann of Surg. Vol. 223,
No. 3, 249-52.
39. Maghsoudi H, Pourzand A (2005). Giant prosthetic reinforcement of the
visceral sac: the Stoppa groin hernia repair in 234 patients. Ann Saudi Med.
25(3):228–32.
40. Arregui ME, Navarrete J, Davis CJ (1993). Laparoscopic inguinal
herniorrhaphy; techniques and controversies. Surg Clin North Am. 73:513-
27.
41. Kavic MS (1996). Laparoscopic hernia repair. Surg Endosc. 7:163-7.
42. Fitzgibbons RJ, Camps J, Cornet DA (1995). Laparoscopic inguinal
herniorrhaphy. Results of a multicenter trial. Ann Surg. 221: 3-13.
43. Bringman S, Wollert 5, Osterberg J, Smedberg 5, Granlund H, Heikkinen T
(2006). Three years results of a randomized clinical trial of lightweight or
standard polypropylene mesh in Lichtenstein repair of primary inguinal
hernia. Br Surg 96:1056—59.

AAMJ, VOL10, NO4, OCT 2013
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
365
44. O’Dwyer PJ, Kings north AN, Molloy RG, Small PK, Lammer B,
Horeyseck G (2005). Randomized clinical trial assessing impact of a
lightweight or heavy weight mesh on chronic pain after inguinal hernia
repair. Br J Surg 92, 166—70.
45. Mike SL, Eino B, Yolanda G, Theo JM (2003). Recurrences after
conventional anterior and laparoscopic inguinal hernia repair. Ann Surg.
237(1): 136–41.

IBRAHIM ABDEL GHAFFAR
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
366
25بوليجليكابرون –بين باستخدام شبكة بوليبروبيلين اصالح الفتق االربى على الجان
ابراهين عبد الغفار
جايعت االسز -كهيت انطب -قسى انجزاحت انعايت
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
يعذ انفخق االرب ي أ كزز انعهياث انجزاحيت شيعا حيذ يجز سيا حان عشزي يهي
يا يؤد ان اسخالك كبيز ف انارد يشداد ذا . جزاحت الصالح انفخق االرب عه يسخ انعانى
ة نهشبك انخ حعذ اكزز يا ف األسخالك بحذد انضاعفاث ي ذ انضاعفاث يا يحذد خيج
.انشبك رقيهت انس عا ف انشبكت خفيفت انس
( 65-20) 57.6يعذل اعارى -قذ اجزيج ذ انذراست عه سبعت عشزي يزيضا ي انذكر
ة نيخخيشخاي باسخخذاو شبكت حى اصالح انفخق بطزيق -يعا ي انفخق االرب عه انجابي -عاو
.انزكبت خفيفت انس 25بنيجهيكابز –بنيبزبيهي
حى حقييى انجزاحت خالل س حبي حذد ححس كايم نهزض يع ححس حذريج ف سبت
حذد األنى بعذ انجزاح حيذ اخخف األنى ي رالد عشزي حان بعذ شز ي حانخي بعذ رالرت شر
حى رصذ اربعت حاالث ي انخرو . حان بعذ سخت شر ي انحان األخيز بعذ حسعت شري
انخفيف بكيس انصف رالد حاالث ي انخجع انصه عه احي احذ حانخي ي انخيم بأعه
.نفخقانفخذ حان احذ ي عذو االرحياح ف انطقت االربيت نى يخى رصذ حذد حاالث ارحجاع ل
انزكبت خفيفت انس فعانت اجحت ف اصالح انفخق 25بنيجهيكابز –ا شبكت بنيبزبيهي
االرب عه اناحيخي كا ا يضاعفاحا قهيه غيز يؤرز