Embed Size (px)
Citation preview
23/03/2006
יישום הנחיות חדשות למניעת פקקת ורידית לאחר לידה בבית
חולים הדסה
Implementation of New Guidelines for Prophylaxis
of Postpartum Venous Thromboembolism at
Hadassah University Hospital – Surveillance of
Adherence to Guidelines and Adverse Events
עבודת הגמר של התלמידה רבקה ויינשטיין
ס לרפואה של האוניברסיטה "כמילוי חלק מהדרישות לשם קבלת תואר דוקטור לרפואה מטעם ביה
.ירושלים, העברית והדסה
:בהדרכתם של
מחלקת , ר אייל ענתבי"ד
-הדסה הר, נשים ויולדות
הצופים
המחלקה , דוד ורון' פרופ
כרם-הדסה עין, להמטולוגיה
מרכז , מאיר ברזיס' פרופ
, לאיכות ובטיחות קלינית
ח הדסה"בי
INTRODUCTION
The increase in risk of thromboembolic events during pregnancy is well-established,
and pregnancy is recognized as a significant risk factor for development of deep-vein
thrombosis and pulmonary embolus. In accordance with this, prophylaxis protocols
are practiced worldwide for pregnant women at risk. However, recent studies have
shown that the risk of venous thromboembolism (VTE) is even greater postpartum
than it is antepartum1,2, and VTE has been found to be one of the major causes of
morbidity and mortality associated with labor, delivery and Caesarean section3. The
Royal College of Obstetrics and Gynecology (RCOG) has recognized this, and has
published guidelines for VTE prophylaxis for women at risk of developing such
complications3. The guidelines are based on assessing the risk in every mother, based
on personal variables, and they outline cases where prophylaxis is indicated.
Low-molecular-weight heparin (LMWH) is considered effective for VTE
prophylaxis4, with a higher cost-effectiveness profile than unfractioned heparin5, and
is safe for use in pregnancy and delivery6,7. Therefore, LMWH is the drug of choice
for VTE prophylaxis in these women.
The obstetrics & gynecology departments at Hadassah hospitals have adapted and
adopted the RCOG guidelines, and beginning March, 2004 have started to implement
them on their patients8. These guidelines substantially broaden the indications for use
of LMWH compared to those previously practiced, and so their implementation was
expected to increase the use of LMWH on the maternity wards. This increase in use of
medication, especially in young, and for the most part healthy, women, raises the
3
question of the cost of implementation of this protocol in the way of side-effects and
complications.
Previous studies monitoring the obstetric use of LMWH have concentrated primarily
on pregnancy, not delivery. In conjunction with the new guidelines focusing on the
time of delivery, we aimed to examine the safety of its use at that time.
The aim of this study was to monitor the adherence to the guidelines in the obstetrics
wards at the Mt. Scopus campus of Hadassah hospital, and see what, if any,
complications arise from the increase in use of LMWH. We found no studies
monitoring the implementation of these or similar guidelines. We found a single
study9 examining the use of peripartum prophylactic LMWH. In this study the
regimen appeared to be both safe and effective. In accordance with this, the
hypothesis this study was based on was that there would be no significant increase in
complications in women receiving low-dose LMWH, and as its effectiveness in
preventing VTE has been established, it will prove to be an effective prophylactic
measure.
4
METHODS
This study was a descriptive, observational prospective matched case-control study.
Data was gathered as patients were treated, and complication rates were compared to
those of obstetrically-matched controls (i.e women with the same number birth, same
method of delivery, and similar age range).
Subjects
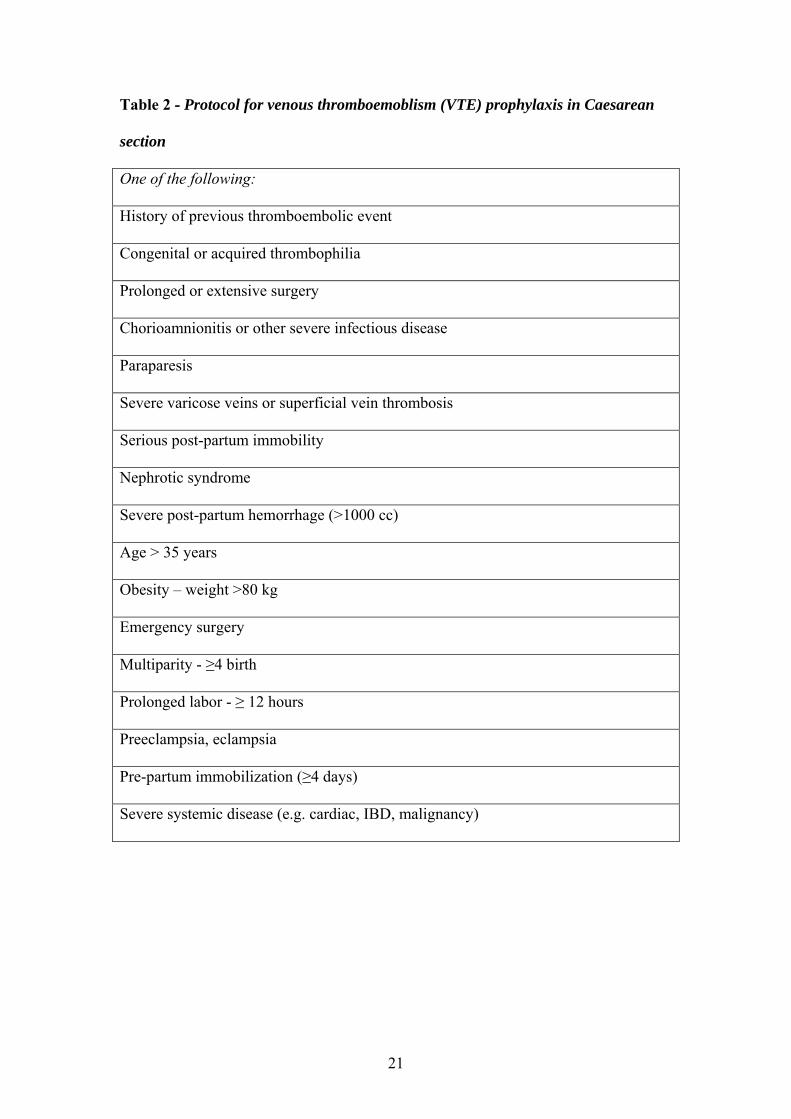
All women delivering a baby at both campuses of Hadassah hospital, if identified by
the treating physician as fulfilling the criteria specified in the protocol (see tables 1 &
2), received LMWH thromboprophylaxis with enoxaparin (Clexane™) 40 mg once
daily. The first 108 women receiving thromboprophylaxis that were identified by the
researcher were monitored for hemorrhagic complications throughout the duration of
their hospital stay (while LMWH was being administered) by filling out a
questionnaire, and by a telephone follow-up a few weeks post-partum.
Controls were matched to cases for age (<20, 20-24, 25-29, 30-34, 35-39 or 40+),
parity (1, 2, 3, 4, 5 or 6+) and method of delivery (vaginal vs. Caesarean section). No
other matching was done as these are primarily normal, healthy women, and women
with other medical conditions were usually by definition in the high-risk, prophylaxis-
indicated group. For every case accumulated a matched control was sought and, if
found, she received the same questionnaire and the same follow-up phone call.
5
Every woman receiving thromboprophylaxis who had a matched control entered the
study, with her control, as a couple. For every parameter followed, the answers given
by the case were compared with those of the control.
The study was conducted between March 2004 and June 2005. During this period 81
women after vaginal delivery and 27 women after Caesarean delivery who received
prophylactic enoxaparin injections participated in the study. Of these, matched
controls were found for 71 vaginal-delivery women and 18 Caesarean-delivery
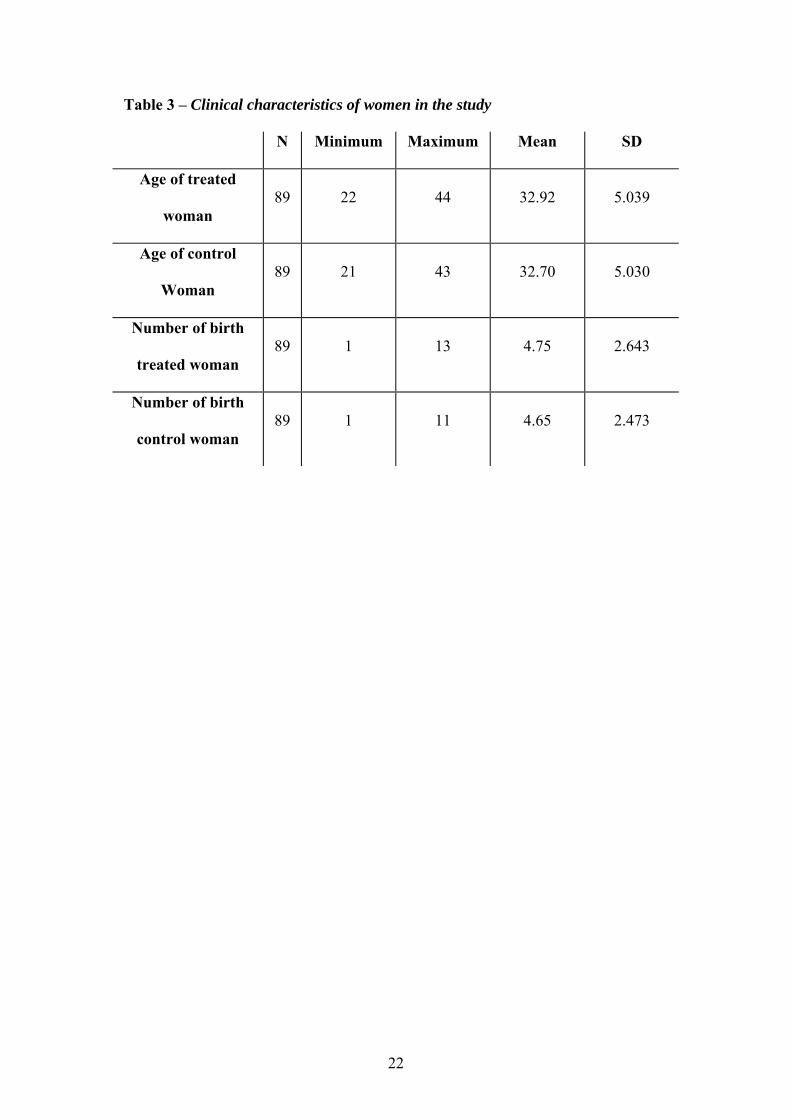
women, for a total of 89 case-control pairs entering the statistical analysis. Clinical
characteristics of the women are shown in table 3. There was no statistically
significant difference of age or parity between the two groups. Of note, there were
women in both groups who were given a questionnaire and never returned it. We have
no record of these women.
Methods
Adherence to guidelines was assessed by evaluating the women in both groups for an
indication for thromboprophylaxis and calculating the percentage of control group
with a known indication on the one hand, and the treated women for a proper
indication on the other hand.
Questionnaires were composed for the purpose of this study (one for vaginal delivery,
one slightly different for Caesarean delivery). The questionnaires collected general
demographic information and relevant information about the delivery, the reason for
enoxaparin administration in cases, hemoglobin levels at admission and lowest
documented post-partum, and questions about various hemorrhagic manifestations
6
during the time of hospitalization. English translation of the questionnaires appears in
the appendix.
The questionnaires were distributed to the women along with an explanation about the
questionnaire and the study. According to the woman’s wishes, the questionnaire was
either completed it with her daily or left for her to complete herself and return at the
time of hospital discharge. When necessary, a translator was used for women who
spoke only Arabic.
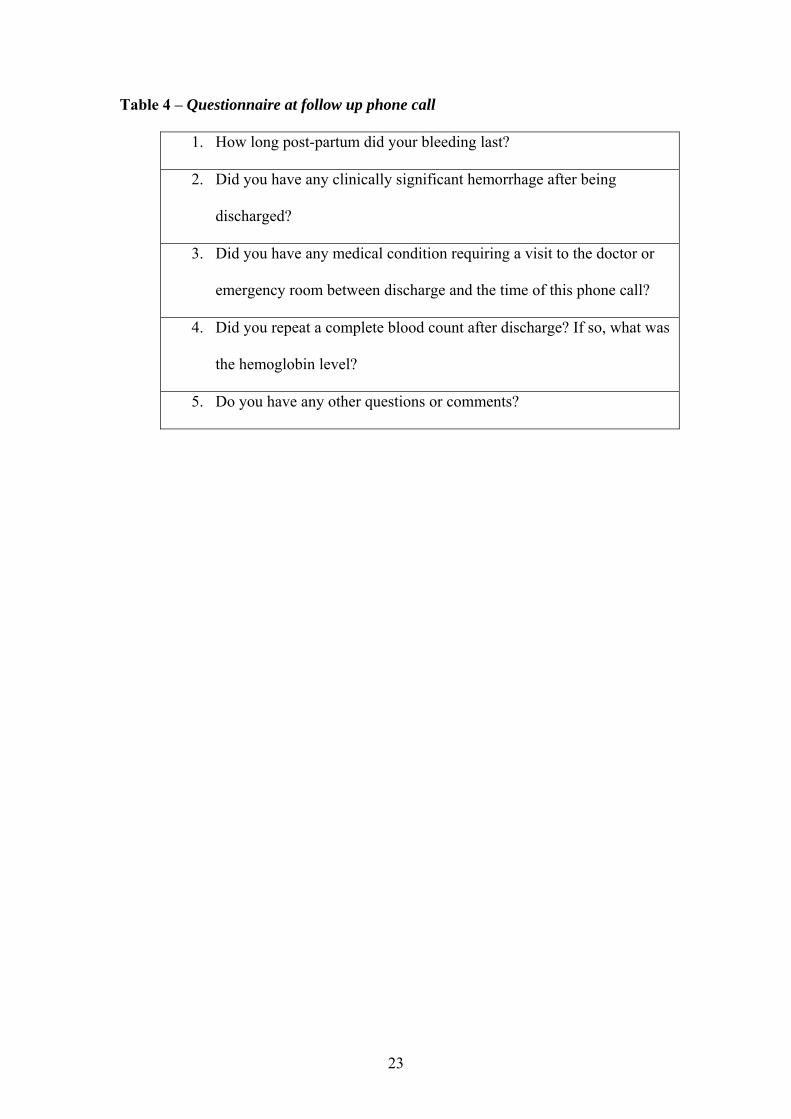
At least 6 weeks post-partum, each woman received a follow-up phone call (see table
4). The purpose of the phone call was to determine if there were any hemorrhagic
complications immediately after discharge that would have been missed on the
questionnaire, if post-partum bleeding was prolonged in women receiving enoxaparin,
if there was a significantly lower hemoglobin level at follow-up blood count in
women receiving enoxaparin, and if there were any puerperial thromboembolic
complications in any of the women.
The primary endpoints of the study were to determine whether guidelines were being
adhered to and whether there were more peri-partum hemorrhagic complications in
the treated women compared to their matched controls. Secondary endpoints included
differences in late post-partum hemorrhages and prevention of venous
thromboembolic events.
7
Statistical analysis
Sample size estimation was based on differences between cases and controls in
percentage of hemorrhagic complications. Assuming that only a difference of 10% or
higher between the two groups is clinically significant (anticipating 5% in controls vs.
15% in cases), with α = 5% and power = 80%, a sample size of 52 pairs of case-
control women was calculated as necessary to prove that such a difference is
statistically significant. Any difference of less than 10% was considered to be
clinically insignificant.
Data was analyzed with SPSS statistical software .When referring to binary
parameters, the McNemar test for matched samples was applied to test whether the
difference between the cases and controls was statistically significant. A one-tail p
value was used, as it is not likely to assume that enoxaparin injections will decrease
rates of hemorrhage. When referring to parameters with continuous values, e.g.
decrease in hemoglobin or duration of post partum bleeding, data was analyzed by the
means of the t-test. The t-test was further used for evaluation of the appropriateness of
the age and parity matching performed. This was done with the aid of Microsoft Excel
software.
8
RESULTS
Of the 89 women receiving prophylactic enoxaparin, we have record of the indication
for it in 84 women (94%), indicating 6% of apparent overtreatment. Of these, 66
(78%) had varicose veins, 11 (13%) had known or suspected thrombophilia, and 12
(14%) had other risk factors, including advanced age, multiparity, obesity,
preeclampsia, chorioamnionitis, prolonged immobilization, Behcet disease and
emergency Caesarean section.
Of the 89 women not receiving prophylactic enoxaparin, we have record of an
indication for it by our guidelines in 6 (7%) of women, indicating 93% adherence to
guidelines. In all of these cases, the indication is a combination of age and parity.
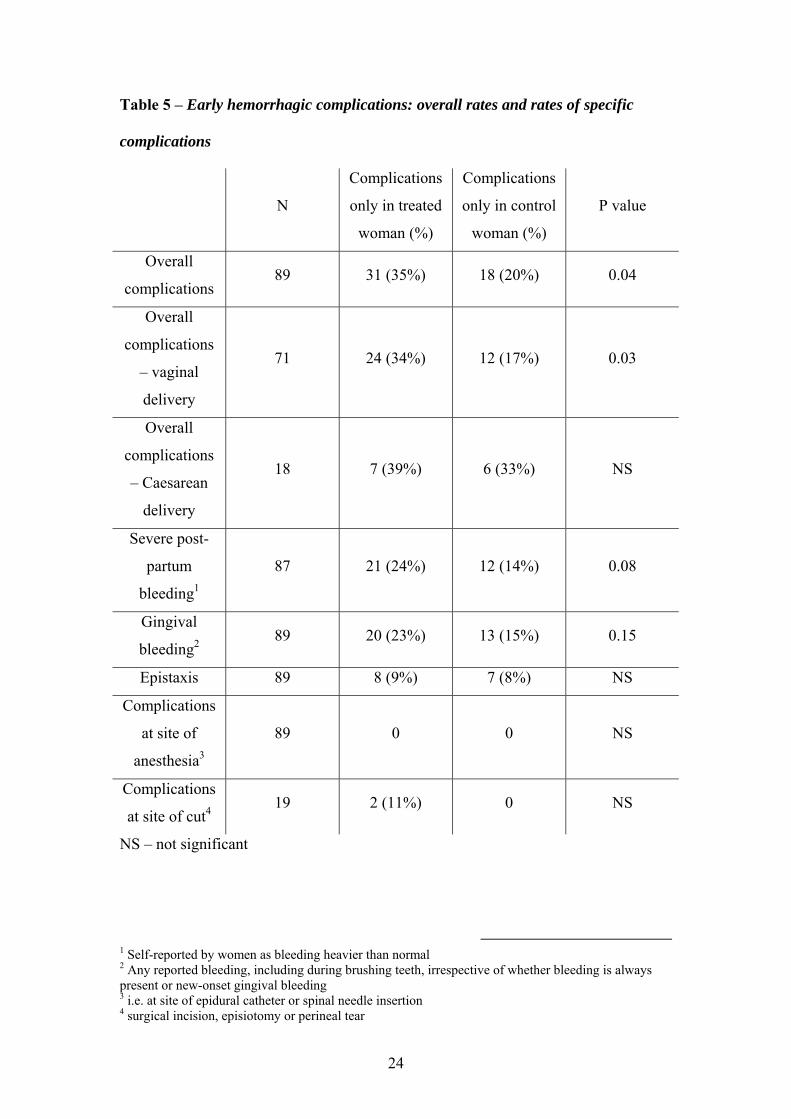
Early hemorrhagic complications are represented in table 5. As to complications in
the cut (surgical incision, episiotomy site or perineal tear) – of 71 pairs of women who
delivered vaginally, there was only one pair in which both women had either an
episiotomy or a perineal tear, and so the sample size for this category is extremely
small – 18 pairs who had a Caesarean plus the above-mentioned single pair. This
sample size is too small for statistical analysis, but we can report that there were no
controls with any reported complications, whereas there were 2 women (11%) who
were getting enoxaparin injections after Caesarean delivery who had reported
complications – one with incomplete closure of the wound with minor bleeding from
the site of the incision, and one with wound infection.
9
The decrease in hemoglobin around delivery, i.e. hemoglobin levels at the time of
admission minus the lowest measured hemoglobin level during hospitalization, was
measured and compared between cases and controls. In women receiving enoxaparin
injections the mean hemoglobin decrease (and standard deviation) was 1.1 g% (0.87),
and in the control women the mean decrease was 1.1 g% (0.81) as well. The mean
difference between the decrease in treated women and the decrease in controls was
-0.03 (1.02) (non-significant p value).
As to post-partum bleeding duration, the mean duration in treated women was 4.9
weeks (standard deviation 2.42) versus 5.2 weeks (SD 3.05) in control women. The
mean difference between bleeding duration in treated women and control women was
-0.24 weeks (SD 3.85) (non-significant p value).
As to the long-term hemorrhagic complications, the results are anecdotal and not
statistically significant. In the treated group we had one woman report prolonged mild
epistaxis, one woman reported slow wound healing and one woman (mentioned above
with wound infection) who was re-admitted for an additional month and had to have
the wound re-opened and surgically drained. In the control women, there were 3
women who reported prolonged post-partum bleeding, and one woman who reported
wound hemorrhage and infection one week post-partum. She was treated in the
emergency room and discharged to her home.
As to thromboembolic complications, we had one treated woman who reported
saphenous vein thrombosis after stopping the prophylactic enoxaparin, and one
control woman who reported a pulmonary embolus.

10
As to hemoglobin levels 6 weeks post partum, there were very few women who went
to have it measured, and so we only have 6 case-control pairs where this value is
available for both women. Of these 6 pairs, there were 4 pairs in which the
hemoglobin level was normal (≥11 g%) in both women, and two pairs in which the
hemoglobin was normal in the treated woman and low (<11 g%) in the control
woman.
11
DISCUSSION
The results of this study show high rates (93%) of adherence to guidelines. The study
further shows higher rates of hemorrhagic complications in women receiving
enoxaparin injections as compared to matched controls not receiving those same
injections, especially in women who delivered vaginally. This is contrary to what we
expected, due to the known low rates of complications for the use of LMWH in
general. However, looking more closely at the complications that arose and
comparing them to the possible severity of deep vein thrombosis and pulmonary
embolus, which the LMWH is there to prevent, we believe that the clinical
significance of these complications is quite low.
Broken down to specific complications, we found no single complication that was
significantly more common in women receiving LMWH. The most significant
complication reported in the women who were getting prophylactic LMWH was the
degree of post partum bleeding. This was a very subjective parameter, determined by
the woman’s interpretation of the degree of her bleeding. While it is reasonable to
assume that in a large cohort women’s overall subjective interpretations shouldn’t
vary from (case) group to (control) group, in this case the women were not blinded to
the treatment, and so treated women all knew they were on blood-thinning injections,
a point which may bias their view.
As to gingival bleeding, there was perhaps a tendency towards more bleeding in
treated women. However, this was not statistically significant, and furthermore, this is
12
not a clinically significant complication, certainly if weighed against deep vein
thrombosis or pulmonary embolus.
As to epistaxis, there was practically no difference between the groups.
As to complications at the site of surgical incision, episiotomy or perineal tear, the
overall prevalence of these complications is too low for this study to have reached any
statistically significant results, but we have one case of a treated woman with severe
wound hemorrhage and infection and one woman with mild hemorrhage from the
surgical incision, and on the other hand a control woman with intermediate-severity
wound infection that necessitated a visit to the emergency room. Based on this data,
there is no evidence that LMWH injections increase the risk of local complications,
although larger studies are necessary to further investigate this point.
As to complications at the site of anesthesia (spinal or epidural catheter), we were
pleased to see there was not a single complication reported. We attribute this to the
great care that was taken during introduction of our treatment protocol to the exact
manner in which spinal cord puncture can be combined with LMWH injections. The
obstetricians, hematologists and anesthesiologists at our institution agreed on
acceptable guidelines which were strictly adhered to, including a 12-hour window
between any injection of LMWH and insertion or removal of needle or catheter, and
6-8 hour window between any insertion or removal of needle or catheter and any
injection of LMWH.
13
As to our only completely objective parameter for degree of hemorrhage, the decrease
in hemoglobin levels, there was no clinically or statistically significant difference
between cases and controls, further indicating that there is no evidence that LMWH
prophylaxis for VTE increases rates of peri-partum hemorrhage.
The long-term follow-up of the women didn’t demonstrate an increase in late
complications due to use of enoxaparin. The bleeding duration was no longer in
treated women than in controls. If anything, it was a mean of 0.24 weeks (which is 1.6
days) longer in the control women, although this was not statistically significant and
the standard deviation was high. Furthermore, as the half-life of enoxaparin is
approximately 4.5 hours10, it is highly unlikely that prolonged post-partum bleeding,
lasting about 5 weeks or longer, can be attributed to the LMWH injections.
As to thromboembolic events, the endpoint the enoxaparin came to prevent, we did
not intend to achieve any data on its efficacy in our study, due to the low prevalence
of these events in the general population and thus the large sample size necessary to
attain significant results. However, we did have a control woman who reported a
pulmonary embolus after her discharge, and we did have a treated woman who
developed saphenous vein thrombosis after stopping LMWH injections. Both of these
findings may indicate the efficiency and the importance of the use of LMWH for
prophylaxis of venous thromboembolic events.
The study design left room for certain bias. Subject selection was unbiased, but
finding matched controls for certain women was difficult. For example, older women
or multiparas, especially if undergoing Caesarean section, fall into the category of
14
LMWH-indicated very easily, and while we matched these parameters, we had to
group the exteremes (i.e. age 40+, parity 6+), and it is posssible the controls were at
the lower end of the spectrum, and the subjects – at the higher end. Furthermore, as
only the women with a matched control ended up entering the study, we have 19
treated women who did not have a matched control. These women did not enter
statistical analysis and their rates of complications were not measured. Another
possible confounder is measurement bias, as the reports of complications were given
subjectively by the women, while the treated women knew they were on blood
thinners.
Based on the results of our study, we recommend the use of enoxaparin 40 mg once
daily for peripartum thromboprophylaxis in women who are at high risk of
thromboembolic events, especially in women who delivered by Caesarean section.
Those women are considered at higher risk for VTE and our study suggests increased
safety of the prophylxis in them. However, further studies are necessary to ascertain
the efficacy of LMWH in prophylaxis of VTE and the safety of this regimen.
15
SUMMARY
The increase in risk of thromboembolic events during pregnancy is well-established,
and pregnancy is recognized as a significant risk factor for development of deep-vein
thrombosis and pulmonary embolus. As part of safety and quality control measures
being taken to improve the quality of care at Hadassah obstetrics wards, the
obstetricians, hematologists and quality control center collaborated to determine
guidelines for prophylaxis of peri-partum thromboembolic events. Prophylaxis was
achieved by injections of low-molecular weight heparin (enoxaparin, Clexane™), 40
mg once daily, to women in the maternity wards at Hadassah hospital who were
considered to be at high risk for thromboembolic events (as determined by advanced
age, advanced parity, obesity, immobility and Caesarean delivery). The aim of our
study was to monitor the physicians’ adherence to the new guidelines and the rates of
complications brought on by this additional treatment.
Adherence to guidelines was assessed by monitoring 178 women who delivered
during 2004-2005 and comparing the existence of an indication for
thromboprophylaxis with the receipt of thromboprophylaxis. These women were
further questioned about the severity of uterine bleeding post partum, as well as other
bleeding complications, both immediately after delivery (while still in the hospital)
and a couple of months post partum. The rate of the reported complications was
compared in 89 women receiving thromboprophylaxis with that in 89 controls, not
receiving thromboprophylaxis and matched to the treated women for age, parity and
method of delivery. The statistical analysis was performed by the McNemar test for
matched controls.
16
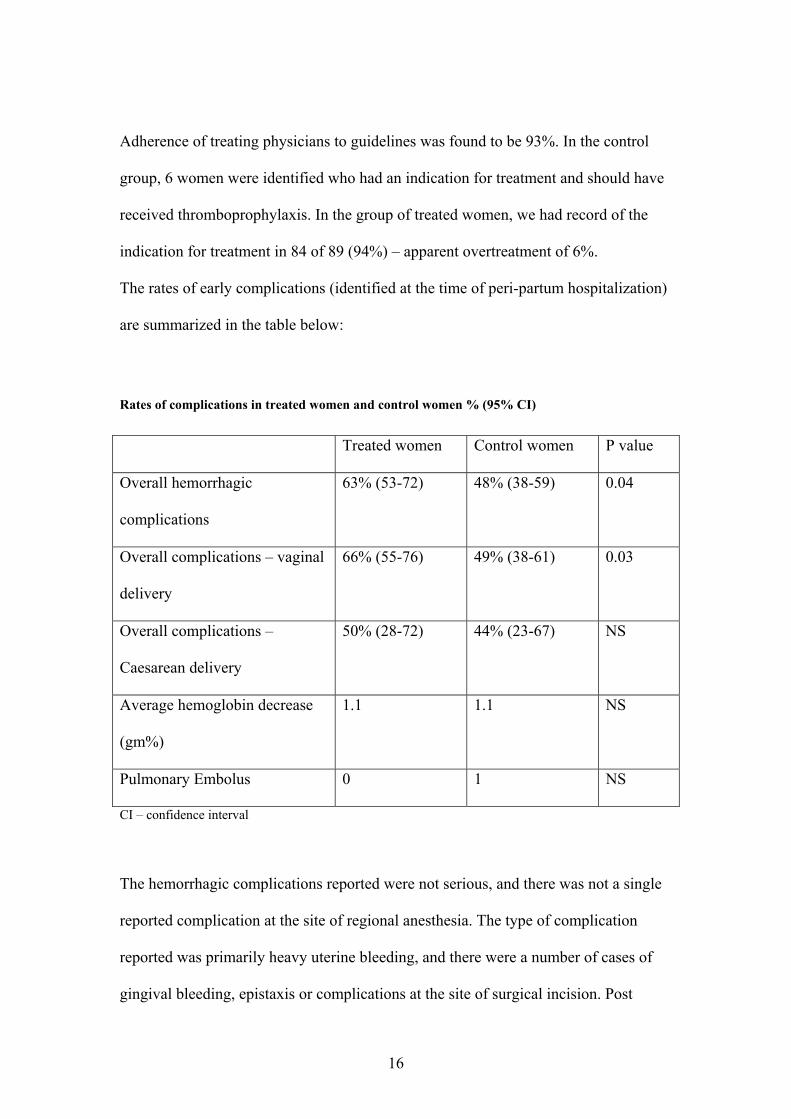
Adherence of treating physicians to guidelines was found to be 93%. In the control
group, 6 women were identified who had an indication for treatment and should have
received thromboprophylaxis. In the group of treated women, we had record of the
indication for treatment in 84 of 89 (94%) – apparent overtreatment of 6%.
The rates of early complications (identified at the time of peri-partum hospitalization)
are summarized in the table below:
Rates of complications in treated women and control women % (95% CI)
Treated women Control women P value
Overall hemorrhagic
complications
63% (53-72) 48% (38-59) 0.04
Overall complications – vaginal
delivery
66% (55-76) 49% (38-61) 0.03
Overall complications –
Caesarean delivery
50% (28-72) 44% (23-67) NS
Average hemoglobin decrease
(gm%)
1.1 1.1 NS
Pulmonary Embolus 0 1 NS
CI – confidence interval
The hemorrhagic complications reported were not serious, and there was not a single
reported complication at the site of regional anesthesia. The type of complication
reported was primarily heavy uterine bleeding, and there were a number of cases of
gingival bleeding, epistaxis or complications at the site of surgical incision. Post

17
partum bleeding duration was similar in both groups (approximately 5 weeks). There
was no significant difference between the two groups in the incidence of other
complications. One woman in the control group suffered a pulmonary embolus, and
one woman suffered from superficial vein thrombosis despite thromboprophylaxis.
In summary, we found high rates of adherence to the new guidelines for peri-partum
thromboprophylaxis. This was associated with slightly higher rates of various
hemorrhages, but these were clinically insignificant. We propose that application of
peri-partum thromboprophylxis is feasible and appears to be safe. However, larger
studies are necessary to further evaluate the safety of this treatment.
18
סיכום
. לידתית-הריון מהווה גורם סיכון ליצירת קרישים ותסחיפים הגורמים לעיתים אף לתמותה סב
על סמך הספרות נוסחו הנחיות , במסגרת פעילות של שיפור איכות ובטיחות במיילדות בהדסה
) ג ביום" מ40, קלקסן תת עורי(הוחל בטיפול מניעתי נוגד קרישה : למניעת קרישי דם לאחר לידה
). חוסר ניידות ולידה בניתוח קיסרי, ולדנות גדולה, השמנה, גיל מבוגר(ולדות עם סיכון מוגבר לי
מטרת המחקר היתה לבדוק את היענות הרופאים בביצוע ההנחיות החדשות ואת שיעור
.ההיארעות של סיבוכי הטיפול
ובדיקת 2004-2005 יולדות בשנים 178- י בחינה של הטיפול שניתן ל"ההיענות להנחיות נבדקה ע
ודימומים היולדות נשאלו אודות חומרת הדימום הרחמי. קיום התוויה לטיפול מונע קרישה
יולדות שקיבלו 89שיעור הסיבוכים הושווה בין . מהלידה ועד כחודשיים לאחר מכן, נוספים
ולדות י( יולדות שלא קיבלו טיפול זה ושהיוו את קבוצת הביקורת 89-טיפול מניעתי נוגד קרישה ל
.McNemar בעזרת מבחן ) מספר וצורת הלידה , מותאמות לגיל
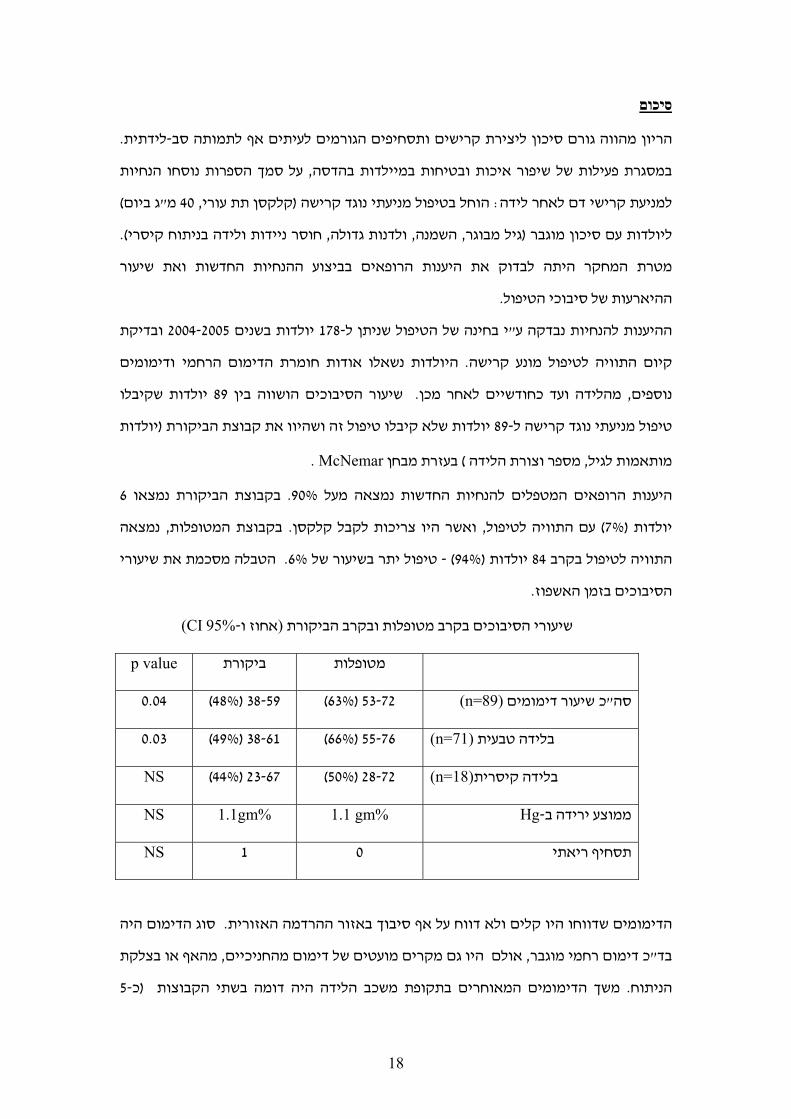
6בקבוצת הביקורת נמצאו . 90%היענות הרופאים המטפלים להנחיות החדשות נמצאה מעל
נמצאה ,המטופלות בקבוצת .ואשר היו צריכות לקבל קלקסן ,עם התוויה לטיפול) 7%(יולדות
הטבלה מסכמת את שיעורי . 6%פול יתר בשיעור של טי-) 94%( יולדות 84התוויה לטיפול בקרב
.הסיבוכים בזמן האשפוז
CI) 95%-אחוז ו(שיעורי הסיבוכים בקרב מטופלות ובקרב הביקורת
p value ביקורת מטופלות
53-72) 63%( 38-59) 48%( 0.04 (n=89)שיעור דימומים כ"סה
55-76) 66%( 38-61) 49%( 0.03(n=71)בלידה טבעית
28-72) 50%( 23-67) 44%( NS (n=18)בלידה קיסרית
Hg 1.1 gm% 1.1gm% NS-ממוצע ירידה ב
NS 1 0 תסחיף ריאתי
סוג הדימום היה . הדימומים שדווחו היו קלים ולא דווח על אף סיבוך באזור ההרדמה האזורית
מהאף או בצלקת , אולם היו גם מקרים מועטים של דימום מהחניכיים, כ דימום רחמי מוגבר"בד
5-כ(משך הדימומים המאוחרים בתקופת משכב הלידה היה דומה בשתי הקבוצות . הניתוח
19
לא נמצא הבדל מהותי בין שתי הקבוצות בשיעור היארעותם של ). שבועות בשתי הקבוצות
ויולדת אחרת סבלה , יולדת אחת בקבוצת הביקורת סבלה מתסחיף ריאתי. סיבוכים אחרים
.י הרגל השטחיים למרות הטיפול המניעתימקריש בוריד
טיפול זה . נמצאה היענות גבוהה להנחיות החדשות למתן טיפול מונע קרישי דם לאחר לידה: דיון
אולם לא היתה לכך משמעות , בעליה בשיעור הדימומים הקלים שלאחר לידה אמנם היה כרוך
.קלינית
דרוש מחקר גדול . ת בסיכון הינו בר ביצועיישום ההנחיות לטיפול נוגד הקרישה ליולדו ,לסיכום
.להוכחת בטיחותו של הטיפול, יותר
20
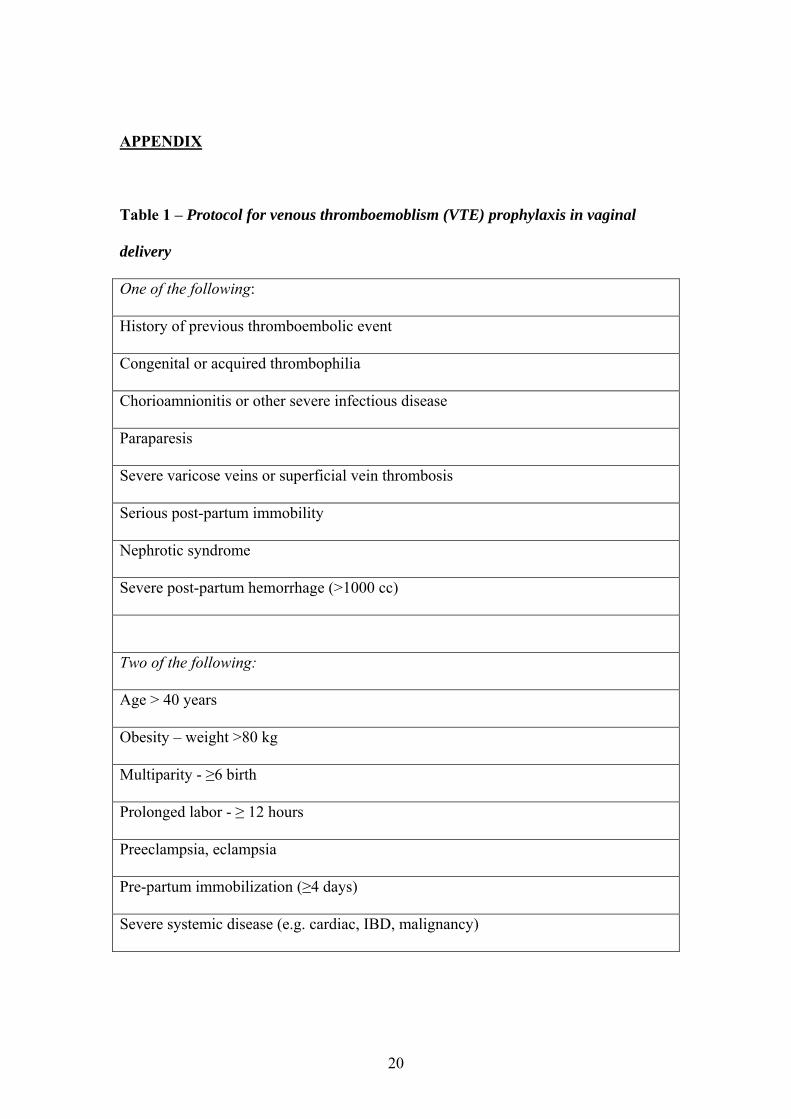
APPENDIX
Table 1 – Protocol for venous thromboemoblism (VTE) prophylaxis in vaginal
delivery
One of the following:
History of previous thromboembolic event
Congenital or acquired thrombophilia
Chorioamnionitis or other severe infectious disease
Paraparesis
Severe varicose veins or superficial vein thrombosis
Serious post-partum immobility
Nephrotic syndrome
Severe post-partum hemorrhage (>1000 cc)
Two of the following:
Age > 40 years
Obesity – weight >80 kg
Multiparity - ≥6 birth
Prolonged labor - ≥ 12 hours
Preeclampsia, eclampsia
Pre-partum immobilization (≥4 days)
Severe systemic disease (e.g. cardiac, IBD, malignancy)
21
Table 2 - Protocol for venous thromboemoblism (VTE) prophylaxis in Caesarean
section
One of the following:
History of previous thromboembolic event
Congenital or acquired thrombophilia
Prolonged or extensive surgery
Chorioamnionitis or other severe infectious disease
Paraparesis
Severe varicose veins or superficial vein thrombosis
Serious post-partum immobility
Nephrotic syndrome
Severe post-partum hemorrhage (>1000 cc)
Age > 35 years
Obesity – weight >80 kg
Emergency surgery
Multiparity - ≥4 birth
Prolonged labor - ≥ 12 hours
Preeclampsia, eclampsia
Pre-partum immobilization (≥4 days)
Severe systemic disease (e.g. cardiac, IBD, malignancy)
22
Table 3 – Clinical characteristics of women in the study
N Minimum Maximum Mean SD
Age of treated
woman 89 22 44 32.92 5.039
Age of control
Woman 89 21 43 32.70 5.030
Number of birth
treated woman 89 1 13 4.75 2.643
Number of birth
control woman 89 1 11 4.65 2.473
23
Table 4 – Questionnaire at follow up phone call
1. How long post-partum did your bleeding last?
2. Did you have any clinically significant hemorrhage after being
discharged?
3. Did you have any medical condition requiring a visit to the doctor or
emergency room between discharge and the time of this phone call?
4. Did you repeat a complete blood count after discharge? If so, what was
the hemoglobin level?
5. Do you have any other questions or comments?
24
Table 5 – Early hemorrhagic complications: overall rates and rates of specific
complications
N
Complications
only in treated
woman (%)
Complications
only in control
woman (%)
P value
Overall
complications 89 31 (35%) 18 (20%) 0.04
Overall
complications
– vaginal
delivery
71 24 (34%) 12 (17%) 0.03
Overall
complications
– Caesarean
delivery
18 7 (39%) 6 (33%) NS
Severe post-
partum
bleeding1
87 21 (24%) 12 (14%) 0.08
Gingival
bleeding2 89 20 (23%) 13 (15%) 0.15
Epistaxis 89 8 (9%) 7 (8%) NS
Complications
at site of
anesthesia3
89 0 0 NS
Complications
at site of cut4 19 2 (11%) 0 NS
NS – not significant
1 Self-reported by women as bleeding heavier than normal 2 Any reported bleeding, including during brushing teeth, irrespective of whether bleeding is always present or new-onset gingival bleeding 3 i.e. at site of epidural catheter or spinal needle insertion 4 surgical incision, episiotomy or perineal tear
25
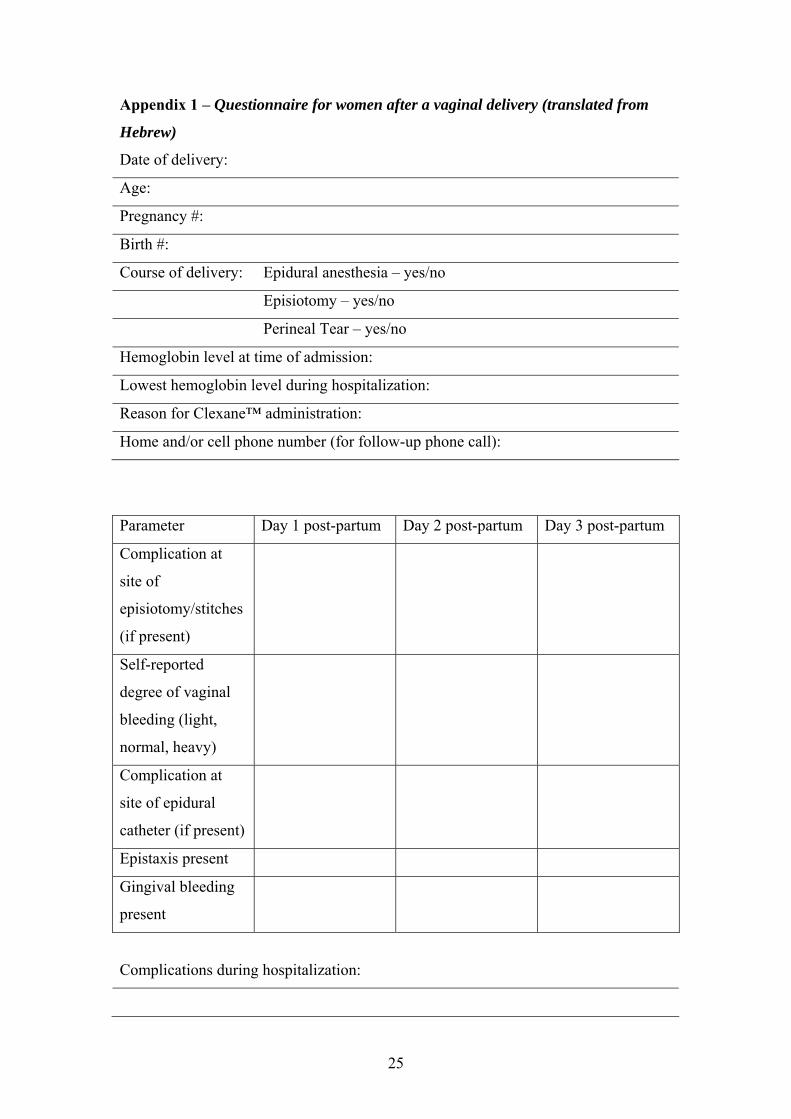
Appendix 1 – Questionnaire for women after a vaginal delivery (translated from
Hebrew)
Date of delivery:
Age:
Pregnancy #:
Birth #:
Course of delivery: Epidural anesthesia – yes/no
Episiotomy – yes/no
Perineal Tear – yes/no
Hemoglobin level at time of admission:
Lowest hemoglobin level during hospitalization:
Reason for Clexane™ administration:
Home and/or cell phone number (for follow-up phone call):
Parameter Day 1 post-partum Day 2 post-partum Day 3 post-partum
Complication at
site of
episiotomy/stitches
(if present)
Self-reported
degree of vaginal
bleeding (light,
normal, heavy)
Complication at
site of epidural
catheter (if present)
Epistaxis present
Gingival bleeding
present
Complications during hospitalization:
26
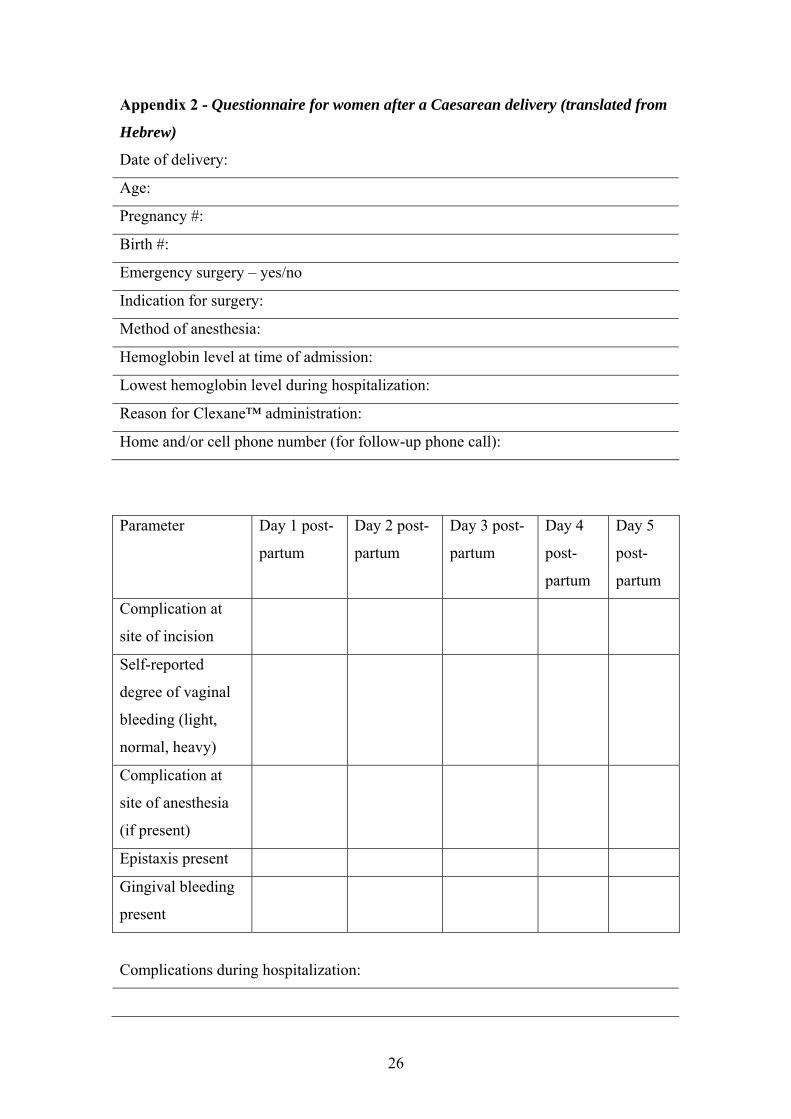
Appendix 2 - Questionnaire for women after a Caesarean delivery (translated from
Hebrew)
Date of delivery:
Age:
Pregnancy #:
Birth #:
Emergency surgery – yes/no
Indication for surgery:
Method of anesthesia:
Hemoglobin level at time of admission:
Lowest hemoglobin level during hospitalization:
Reason for Clexane™ administration:
Home and/or cell phone number (for follow-up phone call):
Parameter Day 1 post-
partum
Day 2 post-
partum
Day 3 post-
partum
Day 4
post-
partum
Day 5
post-
partum
Complication at
site of incision
Self-reported
degree of vaginal
bleeding (light,
normal, heavy)
Complication at
site of anesthesia
(if present)
Epistaxis present
Gingival bleeding
present
Complications during hospitalization:
27
REFERENCES
1 Simpson EL, Lawrenson RA, Nightingale AL, Farmer RD. Venous
thromboembolism in pregnancy and the puerperium: incidence and additional risk
factors from a London perinatal database. BJOG 2001 Jan; 108(1):56-60.
2 Martinelli I, De Stefano V, Taioli E, Paciaroni K, Rossi E, Mannucci PM. Inherited
thrombophilia and first venous thromboembolism during pregnancy and puerperium.
Thromb Haemostat. 2003 Apr;89(4):769-70.
3 Drife J, Lewis G, editors. Why Mothers Die 1997-99: Fifth Report of the
Confidential Enquiries into Maternal Deaths in the United Kingdom. London: RCOG
press; 2001.
4 Ellison J, Walker ID, Greer IA. Antenatal use of enoxaparin for prevention and
treatment of thromboembolism in pregnancy. BJOG 2000 Sep;107(9):1116-21.
5 Potdar N, Jabbar B, Burrell SJ. Thromboprophylaxis after vaginal delivery: a district
general hospital experience. J Obstet Gynaecol. 2006 Jan;26(1):24-6.
6 Dulitzky M, Pauzner R, Langevitz P, Pras M, Many A, Schiff E. Low-molecualr-
weight heparin during pregnancy and delivery: preliminary experience with 41
pregnancies. Obstet Gynecol. 1996 Mar;87(3):380-3.
7 Bonnar J, Norris LA, Greene R. Low molecular weight heparin for
thromboprophylaxis during Caesarean section. Thromb Res. 1999 Nov 15;96(4):317-
22.
28
8 Ben-Meir A, Varon D, Gielchinsky Y, Rojansky N. Prevention of Venous Thrombo-
embolism in Obstetrics and Gynecology – An Update. Harefuah 2005 Dec;
144(12):859-64.
9 Florjanski J, Zalewski J, Tomialowicz M, Heimrath J, Pajak J, Fuchs T, Klosek A,
Klyszcz B. Przebieg ciazy, porodu i pologu u kobiet z zylakami lub zakrzepowym
zapaleniem zyl konczyn dolnych, u ktorych stosowano heparyny drobnoczasteczkowe
[The course of pregnancy, delivery and puerperium in women with varices and
thrombphlebitis of lower extremities, after application of low molecular weight
heparins].Ginekol Pol. 2001 Dec;72(12A):1291-5.
10 Buckley, MM, Sorkin EM. Enoxaparin. A review of its pharmacology and clinical
applications in the prevention and treatment of thromboembolic disorders. Drugs
1992 Sep;44(3): p. 465-97.