Embed Size (px)
Citation preview

1
Natural Resources in Indigenous Medicine
Danister L. Perera
Indigenous system of medicine (ISM) in Sri Lanka culturally renowned heritage of the country and it
historically played a key role in traditional healthcare from the past. According to the written sources
ISM was the sole healthcare system in the country until the European invasion and it could serve at
optimum level under the royal patronage. As historical chronicles and archeological remains provide
supportive evidences ISM had established an island-wide service with well-organized human
resources and infrastructure. The ISM is a knowledge system which inevitably has a connection with
natural environment and uses natural resources for providing an effective healthcare service.
Formally it engages in manufacturing medicine by using natural resources and for the manufacturing
process it uses implements that are made out of natural resources. Also for the treatments and
allied services ISM prescribes objects, articles, apparatus and instruments are fashioned out of
natural resources as traditionally prescribed for the health and wellbeing through curative,
preventive and promotive activities as well. The scope of this monograph will only be limited to the
natural resource utilization involved in formal medicinal manufacturing process. According to WHO
information 80% of world rural population relies on traditional medicine for their day to day health
problems while 35% of Sri Lankan population is primarily depend on ISM for healthcare needs.
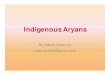
Jayaweera (1981–1982) provides detailed descriptions of 625 MP species used in ayurveda in Sri
Lanka. Approximately 200 MP species are in common use, and of these 50 are heavily used in
ayurvedic and traditional health care systems. While 68% of national demand for medicinal plants
(MPs) is currently met by local supply, stocks of various species are increasingly scarce
(Abeywardana and Hettiaratchi, 2001).
Forest degradation has occurred particularly rapidly in the biodiversity rich, densely populated Wet
Zone of the country’s south-west, where less than 10% of the original forest cover remains, and 40%
of primary forest cover was lost in the period 1956–1983 (Anon., 1986; Gunatilleke and Gunatilleke,
1991). About 80% of locally supplied MPs are collected from the wild. Nearly 80 major MP species
are now considered threatened (Abeywardana and Hettiaratchi, 2001).
Ayurveda as the north Indian medical system had a long term influence on ISM and current Sri
Lankan traditional system of medicine demonstrates a synergetic model of the both. Other than
Ayurveda, ISM had been interacting with Siddha, Unani and other systems of Asian systems of
medicine including Chinese and Tibetan throughout the history. The knowledge system remained in
ISM is coexisted and enriched with all compatible knowledge sources from neighboring countries by
indigenizing the harmonious elements of them.
In Sri Lanka also the astrological book named “Purāna Paladāvaliya” describes astrological
recommendations for farming system and the other book called Daivagna Kāmadhenuva written in
13th century AD also has similar contents. This is very important to understand the ancient wisdom
that inculcated the indispensable nexus between the cosmological dynamics of universe and the
biophysical fluctuations in natural environment.
In the manufacturing process of medicine, ISM uses three kind of natural resources viz; botanical
(udbhidaja), mineral (khanija) and animal (satvaja). In Ayurveda according to the source of origin,
the substances in the Universe are classified as ‘Jangama’ i.e. animal source e.g. milk, meat, blood,

2
urine etc, ‘Audbhida’ i.e. plant sourced e.g. leaves, root, stem etc., and ‘Paarthiva’ or ‘Khanija’ i.e.
mineral sourced e.g. gold, silver, copper, sulphur etc. (Susruta Sutra 1/32 and Caraka Sutra 1/68).
Caraka divided medicines into 50 groups according to their supposed action on different organs or
on symptoms. Susruta also gave another classification of 400 drugs under 37 groups according to
their action against diseases. These resources are coming from any natural habitat like forests,
mountains, desserts, marine and freshwater etc.
Plants are divided into three categories in Rigveda viz; Vrksha (tree), Ōshadhi (herbs useful to
humans) and Virudha (creepers). These are subdivided into: Visākha (shrubs), Saka (herbs), Vratati
(climbers), Pratānavati (creepers) and Alasala (spreading on the ground). All grasses are separately
classified as Trna, flowering plants are as Puspavati, the fruit bearing ones are as Phalavati and
leafless plants are placed under the group, Karira. The Atharvaveda divides plants into eight classes
viz; Visākha (spreading branches), Manjari (leaves with long clusters), Sthambini (bushy plants),
Prastanavati (which expands), Ekasrnga (those with monopodial growth), Pratānavati (creeping
plants), Amsumati (with many stalks) and Kandini (plants with knotty joints). In another Vedic
sources, Taittiriya Samhita and Vajasenayi Samhita texts the plant kingdom is classified into vrksa,
vana and druma (trees), visakha (shrubs with spreading branches), sasa (herbs), amsumali
(spreading or deliquescent plants), vratati (climbers), stambini (bushy plants), pratanavati
(creepers), and alasala (those spreading on the ground). In the words of Brahma, the Manu classifies
plants as Osadhi (plants bearing abundant flowers and fruits), but withering away after fructification,
Vanaspati (plants bearing fruits without evident flowers), Vrksa (trees bearing both flowers and
fruits), Guccha (bushy herbs), Gulma (succulent shrubs), Trna (grasses), Pratana (creepers which
spread their stems on the ground) and Valli (climbers and entwines).
The famous Ayurvedic textbooks Caraka Samhitā and Sushruta Samhitā classify plants into
Vanaspati, Vrksa or vanaspatya, Virudha and Osadhi. Susruta again subdivides Virudha into
pratanavatya (creepers with spreading stem on the grounds) and gulminya (succulent herbs),
whereas Caraka subdivides Virudhs into lata (creeper), gulma and osadhis into annuals or perennials
bearing fruits and grasses which go without fruits. These are further divided into 50 groups in
Charaka Samhita based on their physiological actions and diseases they cure. Flowering plants are
divided into sukadhanya (cereals), samidhanya (pulses), saka varga (pot herbs), phala varga (fruits),
harita varga (vegetable), ahayogi varga (oils), and iksu varga (sugarcane). The Vaisesika school of
philosophy classifies plants under seven categories, viz; Vrksa, Trna, Osadhi, Gulma, Lata, Avatana
and Vanaspati. Parasara, the author of Vrksayurveda, classifies plants into Dvimatrka (Dicotyledons)
and Ekamatrka (Monocotyledons). These are further classified into families like Samiganiya,
Puplikagalniya, Svastikaganiya, Tripuspaganiya, Mallikaganiya, Kurcapuspaganiya.
The mineral and metallic substances used ISM are classified in different ways. Although there is a
variation in pattern of classification as well as inclusion of a particular mineral or metal in a particular
class, a common theme of classification emerges out from the classics. Generally these drugs are
classified in to four distinct classes named as Rasa (metallic), Dhātu (minerals), Ratna (gems) and
Visha (poisons). The ancient chemists classified the other metals, minerals and gems into dhātu,
upadhātu, ratna, upratna, mahārasa, uprasa, sadharana rasa and sudha varga. Metals like gold,
silver, copper, lead, tin, and iron, sand, lime and minerals like red arsenic (manassila), gems
(manayah), salts (lavana), and red chalk (gairika) are indicated as drugs pertaining to earth
(bhauma). In ancient metallurgy, the term lōha is often used for metals like gold and silver and

3
minerals containing metals (ores) are called dhatus. There are seven dhātus: suvarna (gold), rajata
(silver), tāmra (copper), trapa (tin), tiksna or ayas (iron), sisa or naga (lead), and vaikrintaka. Salts or
lavanas are mentioned under the pārthiva or geogenic substances. According to Charaka, there are
five salts: sauvarcala, saindhava, vida, audbhida, and samudra. Mani and ratna, being synonyms for
each other stand for gemstones which are also having many varieties.
Substances, which are used in medicine and are derived from animals, are grouped under the head
of Jangama dravya. There are hundreds of such formulations in Ayurveda, which utilize a variety of
animal products. These animal products are much diverse in their habitat of origin and comprise
from marine, aquatic, terrestrial or avian species. In terrestrial animals, the products from wild as
well as from domestic animals are used in medicine. Among a wide variety of products derived from
animals and used in medicine, commonly utilized substances are honey, milk and its derivatives, bile,
fat, bone marrow, blood, flesh, feces, urine, skin, semen, ligaments, bones, shell, horn and feathers.
Along with many usages of animal substances as medicine, Ayurveda also have developed certain
ways of involving animals in human health care without causing harm to them. These approaches
are unique to Ayurveda and require their revalidation in view of current science to establish the
concept of sustainable medicine where the resources are not exploited for their usage to the extent
leading to their extinction.
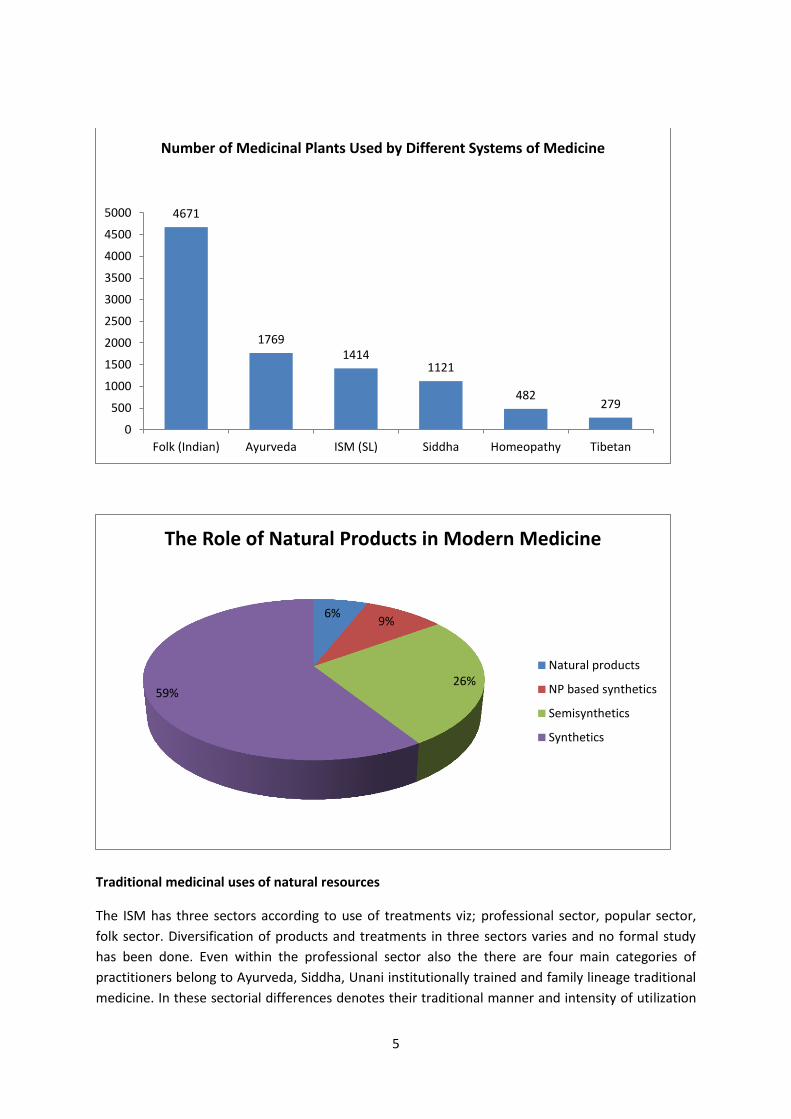
Natural products still play a very important role in the traditional medicine of developing countries
rural population and become more popular among developed countries also. Not only in traditional
medicine but also in other systems medicine like homeopathy and modern medicine use plants as
their medicinal sources. Between 1983 and 1994 41% of new approved drugs had natural products
as they are rich in structurally diverse bioactive molecules that quite often become potential
candidates for new drugs. 120 therapeutic agents in the USA, 25% of all prescriptions dispensed
from community pharmacies from 1959 to 1980 contained plant extracts or active principles
prepared from 90 different higher plant species. About 121 (45 tropical and 76 subtropical)
compounds of defined structure, obtained from only 94 species of plants have been identified for
which no synthetic one is currently available. As a more recent study revealed, of the top 150
proprietary drugs used in the USA in 1993, that 57% of all prescriptions contained at least one major
active compound currently or once derived from (or patterned after) compounds derived from
biological sources. Additionally, the 20 best-selling drugs worth about six billion a year currently
come from natural sources. In fact, in 1996, six out of the top 20 pharmaceutical prescription drugs
dispensed were based on derivatives of natural products. The bioactive ingredients or phytochemical
compounds which are used as drugs and demonstrate that 80% of these have had an ethnomedical
origin identical or related to the current use of the active elements of the plant.
During the Global Synthesis Workshop on Biodiversity loss and species extinction: managing risk in a
changing world” held at the IUCN World Conservation Congress in Bangkok, Thailand in 2004 and
recognizes the importance of medicinal plants and other components of biodiversity to human
welfare. Plants synthesize a wide variety of chemical compounds or phytochemicals many of which
have beneficial effects on long-term health and can also be used as effective treatments for human
diseases. Estimated percentages of "green" products produced by some major pharmaceutical firms
are high in number and their drugs, as listed in PDR were evaluated to see what percentage still
contained natural products as one of the major ingredients. A generous scoring, allowing all vitamins
and amino-acids, acetic acid, lactose, as major or minor ingredients or excipients would give at least

4
50% "green" and in addition to pharmaceuticals there are nutraceuticals, functional foods and
cosmaseuticals based on natural plant derivatives share the market widely. Thus, the final
percentage of plants or plant-derived extracts in modern pharmaceuticals will ultimately depend
upon your definition of phytomedicinal compounds. With increasing demand of natural product
medicines and augmented on the other hand, as a consequence of new drug developments from
plants, phytopharmaceuticals are projected to increase their market share. Modern drugs
discovered from natural products.
5
Traditional medicinal uses of natural resources
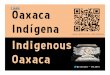
The ISM has three sectors according to use of treatments viz; professional sector, popular sector,
folk sector. Diversification of products and treatments in three sectors varies and no formal study
has been done. Even within the professional sector also the there are four main categories of
practitioners belong to Ayurveda, Siddha, Unani institutionally trained and family lineage traditional
medicine. In these sectorial differences denotes their traditional manner and intensity of utilization
4671
1769 1414
1121
482 279
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Folk (Indian) Ayurveda ISM (SL) Siddha Homeopathy Tibetan
Number of Medicinal Plants Used by Different Systems of Medicine
6% 9%
26% 59%
The Role of Natural Products in Modern Medicine
Natural products
NP based synthetics
Semisynthetics
Synthetics

6
of natural resources for medicinal products. The professional sector mainly relies on formal
pharmacopeia and products manufactured by local Ayurvedic pharmaceutical companies or
imported products by agents of overseas companies. Major portion of these products are classical
products which have been manufactured through pharmacopeial standards or as recommended by
textbooks. Other portion is proprietary ethical products based on research and development of such
company.
Ayurveda pharmacopeia was compiled by an expert committee composed by eminent Ayurvedic
scholars and has contributed a historically valuable source to the nation. Subsequently Siddha iand
Unani pharmacopeias also are initiated at the same time with expert committees composed of
similar disciplines. First Part contains measures, terminology, textual references, collection practices,
applied pharmacy, manufacturing practices, tinctures, liquid extracts, decoctions, distilleries,
fermented wines, purification of metallic and minerals, detoxification of poisonous and toxic
substances, appendices etc. The main part is formulary which contains 22 categories of medicines,
771 recipes with mode of preparation, indications and dosage.
The formulas available in Ayurveda pharmacopeia of Sri Lanka
No: Category Description No.
01 Anupana aqueous extract made of fresh juice of tender leaves 17
02 Kalka paste made out of wet grinding of powders 15
03 Kwatha decoctions made of dried compound of plant materials 188
04 Choorna powders made out of dried plant materials 61
05 Lauha iron-based herbo-mineral preparations 14
06 Parpatee Sulfur-mercury based metallic preparations 07
07 Vatee Pills made out of herbal compounds 25
08 Guggulu Guggulu (specific gum resin) based preparations 16
09 Modaka Sweet-based large bolus 16
10 Guda Khanda Sweet-based semisolid preparations 09
11 Rasa Metallic compounds 93
12 Avaleha Linctus or sweet preparations to be licked 09
13 Asava fermented preparations made out of fresh materials 25
14 Arista fermented preparations made out of decoctions 34
15 Basna medicated dietary supplements used in convalesce 05
16 Taila medicated oils prepared out of compounds of raw materials 102
17 Grita medicated ghee prepared out of compounds of raw materials 27
18 Alepa external applications 18
19 Netra Bindu eye drops 05
20 Drava Sara tinctures (alcoholic preparations) 13
21 Taralasara liquid extracts (alcoholic preparations) 32
22 Kwatasara aqua (alcoholic preparations) 40
Second Part of the Volume I contains single drug profiles which are representing 400 plants, 67
minerals and 37 animal sources. Third Part is more or less an extension of the part two and focused
on systemic pharmacology of each single drug described in previous part. After several decades,
Department of Ayurveda has deliberately considered to revise and update the pharmacopeia in line
with international standards. In the Ayurvedic Formulary of India (AFI) Part I and Part II there are 635
Formulations (AFI Part I (1978) - 444 formulations and AFI Part II (2000)- 191 formulations). Three
Volumes of Ayurvedic Pharmacopoeia Part II, have been published consisting of 101 monographs on

7
formulations and seven Volumes of Ayurvedic Pharmacopoeia Part I, have been published consisting
of 540monographs on single drugs. Already Government of India has agreed to incorporate all the
418 monographs published in Ayurvedic Pharmacopeia India to proposed updates of Sri Lankan ISM
pharmacopeia. BMARI has expedited developing protocols of standards for endemic plant sources
which is to be included in revised pharmacopeia. But the real ISM formulary is not included into
existing document due to various constrains. No proper intensive study has been conducted to
exploit real wealth of hidden recipes of ISM knowledgebase. For an example a well-known ISM book
called Vatika Prakaranaya which is composed of 5393 Sinhalese verses containing 658 recipes. The
book called Taila Pancha Sataka contains 500 recipes of medicinal oils. Similar number of recipes
could be traced in each and every book which is already published. In addition to that there are
thousands of recipes embedded in other literary sources which are not published. All these recipes
are time-tested and traditionally trialed.
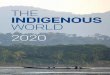
The majority of natural resources accounts of plant-based resources which are basically estimated
that approximately 1000 herbal formulations prepared from around 750 plants are in regular use at
the present time. In Sri Lanka around 1500 plant species are medicinally used out of 3360 of
flowering plant species. WHO has published many technical reports related to consumer
information, worldwide regulations, quality standards, research methodologies and four volumes of
selected medicinal plants totaling 116 monographs.
28%
36%
21%
3% 5%
7%
Medicinal Plants Distribution by Habit
Herbs
Trees
Shrubs
Lianas
Climber H
Climber W

8
Conservational practices and ethics of prudent exploitation
The historical review of ancient culture gives the contextual framework of conservational practices
and ethics of prudent exploitation that supported by cultural belief system and social value system
of traditional societies. Also the value of such best practices and need for validation should also be
highlighted and propagated within the present society for substantial results of sustainable use of
medicinal resources of natural habitats. Home gardens and their plant diversity was one of the key
supportive factors in conservation which was a common feature of ancient societies. Also the
traditional zoning system of resource utilization had been based on commonly agreeable terms as
well as culturally accepted values and norms among the villages. Ethnologically speaking our
ancestors used natural resources with a "proper permission granted by the nature" according the
norms set up by society. In this context ISM practices traditionally respected the nature’s
governance and it’s blessing for healing process which promote the sustainable use of natural
sources.
There are various rituals and taboos prevailing for centuries with coded ethics to preserve ecological
and biological diversity of local habitat. Cultural heritage and vernacular communication system
strongly supported to dictate a self-disciplined community guide in sustainable use of natural
resources. Our ancestors were the key holders of this knowledgebase which had been transmitted
from generation to generation before mainstream knowledge system is overrun by colonial
imperialism. Sri Lankan Indigenous medical knowledge system is therefore regarded as a highly
skilled-based and widely practice-oriented ethno-science that promotes nature-friendly lifestyle to
gain health. This knowledge was considered as sacred and to be learned only by selected persons
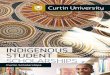
who had inborn and inherited talent in accordance with ancient pedagogics. Learned traditional
medical practitioners were not only really good therapists but also ecologists who took care of
419
214 214 214 208
168 141 129 118
0
50
100
150
200
250
300
350
400
450
Number of Taxa in Importnat Medicinal Plants

9
environment. In this context norms and ethics were culturally established within the professional
behavior to ensure prudent utilization and sustainable use of natural resources. Habitats for
medicinal resources are recommended while different seasons for harvesting and collecting are also
prescribed. Describing different parts of the plant with different properties is also another strategy
of conservation. Most important practice which supports the conservation is diversity of therapeutic
materials and versatile use of procedures must also be highlighted. On the other hand depending on
localized systems or subsystems is more ecofriendly practice which has a minimum impact on the
resource exploitation. The use of natural bioresource for treatments as a living device, leeches are
very important where the natural resources are used in a sustainable manner.
Impacts of ecological footprints of ancestral societies were easily renewable and reversible in a
sustainable manner. Their consuming pattern was environmental-friendly and economically viable to
their livelihood. Therefore they were affected by less or no mental stress and psychologically
frustrated because of their simple and middle-path oriented lifestyle. Family relationships, culture,
communication and community were highly conducive for enabling a supportive atmosphere to
cope up with any stressful condition. Beyond all those individually each person had a strong belief in
supra-humane blessings coming from their faithful deeds extended with good conducts in the past. If
the result is good they are happy. If not it is something to go through and compensate. This
philosophy helped them to make their minds and keep negotiating with outer world. Ecological
wellbeing was a very vital and obligatory factor which could heal their whole life. Sometimes they
had a ritualistic practice to tell their illness to a selected tree in a respectful way and keep hopes only
on that natural object. Positive thinking was practiced in deep sense as a life custom which expels all
negative effects through reciting blissful invocations.
Indigenous medical knowledge is always utilizing natural resources enriched with healing properties
but in a sustainable manner. One formula contains multi-ingredients and has pluralistic applications
which support customized therapeutic interventions and situational adaptations. Personalized
therapy is also one of the effective ways of promoting eco-friendly resource use patterns that had
been practiced widely in traditional medicine as a theory. In Other way indigenous medicine is a
localized system which utilizes only limited number of species found in particular natural habitat.
This does not encourage over-exploitation or outside persons to harvest resources by any means.
Also another very important practice in indigenous medicine to avoid unnecessary exposure of
natural medicinal resources is to decoding the names. In addition to that there are many norms and
ethics to follow before collect medicinal plant or part of a plant. All these restrictions, taboos and
proscriptions were well-established cultural practices to protect environment and it’s natural
treasure trove protected from unethical exploitations, inhumane destructions and irrational
manipulations.
Policies, Strategies and Issues
Sri Lanka, with as a biodiversity hotspot, has 7106 plant species including microscopic flora and of
which around 1500 species are used for medicinal purposes. It is estimated about 1414 plant species
recorded in medicinal uses and approximately 208 of those are reported to be in frequent use. Out
of these 50 are heavily used in Ayurvedic and traditional health care systems while nearly 80
medicinal plant species are now considered threatened. These species include several endemic
species which are becoming increasingly rare and under threat of extinction. It is seen that 104

10
manufacturers produced 655 herbal formulas utilizing 740 varieties of plants, but the trade is still
dependent on mass scale imports. The pharmaceutical industry of ISM totally relies on continuous
supply of natural resources and their quality which creates the dilemma of conservation and
utilization. Over 70% of the plant collections involve destructive harvesting because of the use of
parts like roots, bark, wood, stem and the whole plant in case of herbs.
The intensive harvesting of wild medicinal plants due to the increasing use has in many places
resulted in overexploitation, and forms a serious threat to biodiversity in the country. Several studies
attest to a trend of increasing harvesting pressures on traditional supply areas linked to a growing
shortage in supply of popular medicinal plant species. The current demand for certain taxa exceeds
supply, with traders reporting acute shortages and price increases of these. As a result, several plant
species have been exploited to such an extent that they are seldom found in unprotected areas. As
the global strategy and plan of action referenced in the Beijing Declaration notes, it is important that
research on traditional medicine be improved in the quality of services and products which is mainly
depended on the GMP. Since the medicinal properties in plants are mainly due to the presence of
secondary metabolites which the plants need in their natural environments under particular
conditions of stress and competition and which perhaps stimulates the demand for wild collections.
While it can be presumed that cultivated plants are likely to be somewhat different in their
properties from those gathered from their natural habitats, it is also clear that certain values in
plants can be deliberately enhanced under controlled conditions of cultivation. The large-scale
commercial cultivation has a number of socio-economic impacts on rural people as an income
regeneration which is sometimes potentially harmful to farmers when the market is not organized in
a proper supply-chain.
Sri Lanka Conservation and Sustainable Use of Medicinal Plants project was implemented in 1999 in
five Medicinal Plant Conservation Areas (Bibile, Rajawaka, Naula, Kanneliya and Ritigala) under
ministry of indigenous medicine with GEF / World Bank funds. The project was planned to reach
goals by mobilizing the cooperation of local populations in areas in or near villages known for active
collection of medicinal plants from the wild. These Areas, called Medical Plant Conservation Areas
associated with other conservation such as forestry, strictly reserved nature sanctuaries, and other
forest categories that contain significant medicinal plant populations). Through this structure,
villagers were encouraged to, modify their traditional harvesting and use practices, adopt the
cultivation of medical plants as a substitute for harvesting from the wild and offer the opportunities
to develop new sources of income from value added enterprises. The project shared for
operationalizing this implementation strategy were grouped in three components viz; Expansion of
conservation and sustainable use of medicinal plants in situ, through activities covering socio-
economic and ethnobotanical data collection to establish baseline information and inventories,
growth and yield studies (sustainability studies) of various species, in education and extension of
ayurvedic medicine practices, development and implementation of conservation strategies, and the
development of action plans for harvesting, processing, and producing medicinal plants in a
sustainable Manner at the village level. ii) Expansion of ex situ cultivation and conservation of
medicinal plant materials and genotypes through the establishment and improvement of national
nurseries, conduct of propagation research and technical field planting for further extension to end
users, and development of extension and dissemination channels; iii) Provision of information
services and supporting institutional Focused on the development and promoting of an adequate
legal and regulatory framework covering access to and management of indigenous medicinal plant

11
knowledge and related information (intellectual property rights), the compilation and preservation
of knowledge about medicinal plants and has network for managing this information, training and
awareness building, monitoring and assessment.
Herbal Farmer Village (Osu Govi Gammana) project of the Ministry of Indigenous Medicine started in
March 2005 and it was expected by this project to minimize the cost increased annually for the
foreign countries for the import of dried herbs. A survey conducted in 2000 revealed that nearly a
sum of Rs 125 Million is annually spent for the dried herbal raw materials of which some of them can
be cultivated in Sri Lanka. The major expectation of this project was to identify herbs which are
locally cultivatable and turn out a new farmer community for the cultivation of herbs to popularize
this cultivation as a source of income generation. Furthering the activities of this project was aimed
to establishment and maintenance of commercial scale herbal cultivation among farmer
communities, encouragement and development of herbal gardens, expansion of herb cultivation in
association with Divi Neguma among low –income families. The Department of Ayurveda have been
established 5 herbal Gardens in Sri Lanka They are at Haldummulla (65 acres), Girandurukotte (165
aces) in Uva province, Pattipola (25 acres), Pallekele (5 acres) in Central parts and Navinna Garden
(12 acres) in Western province at Colombo which provides information, education and research
services as well as conservation base of genetic resources.
The main focus of state policy with regard to ISM will ensure positive outcomes of future trends,
potentials and ways forward to use plant resources in ISM in an economically and environmentally
viable manner. Therefore the institutional support will be granted for increasing the availability of
economically potential natural resources for the industry which needs a critical attention with multi-
stakeholder partnership. Agrotechnology and financial support for the commercial scale and
research level cultivations will be assured as the most critical strategic solution for the issue of
conservation and sustainable use. To achieve better quality and sustainability of the industry the
need of national level integrated program for cultivation of medicinal plants will be emphasized. The
national policies on ISM industry should be revisited and totally revised in accordance with current
socio-economical and ecological requirements. The supply of resources for ISM industry is not
properly researched and analyzed with it’s market potentials which should be estimated carefully
and systematically to envisage the economic output of the sector.
The National Science and Technology Commission (NASTEC) has published an elaborative document
on 'A National Programme for Herbal Health Care Products' with the collective deliberation by a
group of experts representing several relevant fields. The report has identified significant thrust
areas to be researched and prioritized in a timely manner which are also related to medicinal plant
resources like economic mapping of autogenic flora, selection of plant species and verification,
incorporation of Ethnomedical and Ethnobotanical data, trial propagation for developing high yield
varieties, medium scale plant propagation, phytochemical studies on herbal ingredients, quantitative
and analytical studies on main ingredients etc. One of the most significant recommendations in this
report is to establish a Knowledge Based on herbal medicines and their uses. This is a very important
step to be taken in order to drive the industry towards a productive goal, and to coalesce with
mainstream industrial interventions. This will support an information network and data system
programmed to be accessible to relevant stakeholders involved in the herbal healthcare product
sector. Especially the ayurveda sector will be benefitted through such a knowledge base by crossing
over international market constraints and improvement of the quality of products.

12
Conclusions and Recommendations
The trade in traditional medicines forms part of a multimillion-rupee ‘hidden economy’ in Sri Lanka
which is stimulated by high dependency rates on natural remedies, ongoing R & D process of ISM
industry and also with the export market demand. Therefore the supply of quality medicinal plant
products throughout the island is not only critical for the health of millions of consumers, but also
for the welfare of the people collect, store and transport them to maintain the market supply. With
the same reason the environmental impact of overexploitation is becoming a critical threat because
demand for natural resources the ISM pharmaceutical industries is now greater than at any time in
the past. The international conventions like CITES and national laws on protected species will
monitor in more restrictive manner utilization of biological resources in trade which can have a
negative impact on the industry. Hence there is a timely need for reviewing current status of
resource density and harvesting intensity manipulated by ISM industry in Sri Lanka for furthering
remedial measures.
One of the major problems related to natural resources used in ISM is lack of information
management system and integrated policy planning for resource management. National records are
rarely kept on local collections and accessibility to resource-bases and availability of resources are
not properly mapped. The present medicinal plant market is essentially a “suppliers’ market” where
supply is decreasing while the demand is increasing with a significant growth rate. However, the
monetary returns for the raw materials are not equally divided amongst the “suppliers”. The local
level collectors receive the least while the middlemen—wholesale dealers, vendors, traders, and
exporters get increasingly more. However, the increasing global demand for many medicinal plant
products offers the industry an opportunity to conduct research and development for “added-value”
with innovations. Preparation of some medicinal products and extracts and conversion into dosage
forms can be carried out with hitech for local, regional and international markets which has not been
supported in a proper manner and not recognized in mainstreamed trade system. Therefore
commercial level cultivations should be promoted with proper evidence-based agronomic
technologies and well-established market networks for ensuring the sustainability of farmer’s
income. The Cultivation of medicinal plants is broadly viewed not only as a resources for meeting
current and future demands for large volume production of plant-based drugs and herbal
preparations, but also as a means for relieving harvest pressure on wild populations.
The government should adopt WHO Guidelines on good agricultural and collection practices (GACP)
for medicinal plants, which provide general technical guidance on obtaining medicinal plant
materials of good quality for the sustainable production of herbal products classified as medicines.
These guidelines are also related to WHO's work on the conservation of medicinal plant resources,
promotion of sustainable use and cultivation of medicinal plants. The main objectives of these
guidelines are to contribute to the quality assurance of medicinal plant materials used as the source
for herbal medicines to improve the quality, safety and efficacy of finished herbal products, guide
the formulation of national and/or regional GACP guidelines and GACP monographs for medicinal
plants and related standard operating procedures; and encourage and support the sustainable
cultivation and collection of medicinal plants of good quality in ways that respect and support the
conservation of medicinal plants and the environment in general. These guidelines also concern the
cultivation and field collection of medicinal plants and include certain post-harvest operations which
can have impact on quality.

13
Countries with a strong history of practicing traditional medicine with significant utilization of
natural resources have a common interest in protecting against misappropriation and securing IPR
that would allow them to derive economic benefits from their own traditional medicine-related
resources. In 2005, the World Health Assembly concluded that member states should take measures
to protect, preserve and to improve if necessary traditional medical knowledge and medicinal plant
resources for sustainable development of traditional medicine, depending on the circumstances in
each country; such measures might include, where appropriate, the IPR of traditional practitioners
over traditional medicine formulas and texts, as provided for under national legislation consistent
with international obligations. Therefore IPR should be taken as the most burdened issue related to
traditional medical knowledge of natural resources and their bioactive ingredients which need to be
addressed nationally. The Beijing Declaration states that “traditional medicine should be further
developed based on research and innovation in line with the Global Strategy and Plan of Action on
Public Health, Innovation and Intellectual Property. Also adds “Governments, international
organizations and other stakeholders should collaborate in implementing the global strategy and
plan of action.” The referenced resolution contains a number of provisions related to the protection
of traditional medicine and intellectual property rights, and promotion and improvement of research
on traditional medicine. However, several developed countries were unwilling to endorse what they
saw as further intellectual property protection for traditional medicine where genetic resources,
cultural expressions and traditional knowledge integral parts of healing process in ISM.