Embed Size (px)
Citation preview
Influenza Pandemic Preparedness: Evaluating Modes of Influenza Transmission
Don Milton, MD, DrPHUniversity of MarylandSchool of Public Health
We don’t know how influenza is transmitted!
• “Our understanding of the transmission of influenza is woefully inadequate,” – Institute of Medicine, National Academy of Sciences, USA,
September, 2007– “It is still unclear what proportion of the spread of
influenza virus occurs through each of the potential routes of transmission (contact, droplet spray, and airborne)…”– Institute of Medicine, National Academy of Sciences, USA,
September, 2009
Three Modes of Transmission• Contact
– Inoculation of nasopharynx from direct and indirect mucosal contact, hands, or fomites (objects)
– Close proximity in space (and time if direct, but some delay possible for indirect)
• Large droplet spray – Direct hit with ballistic droplet on mucosal
surfaces
– Close proximity in space and time required
• Aerosol Transmission (Airborne)– Inhale small droplets and droplet residua
(“droplet nuclei”)
– Deposited in posterior nasopharynx, or airways below the larynx
– Close proximity in space and time High risk
– Longer distance in space and time possible dependent on environmental conditions
Why care about mode?
• Airborne transmission implies changes in public health recommendations– Healthcare worker protection:
• Need to be and feel safe• Are handwashing and covering coughs enough?• Respirators? Engineering controls?
– Patient protection: Nosocomial infection can be fatal• Respirators? Engineering controls?
– Pandemic and severe epidemic response:• Vaccines often available only after peak of second wave• Mismatched vaccines in some epidemic years• Resistant viruses are transmissible
– (e.g. season H1N1 prior to 2009 was 99% resistant to oseltamivir)
High Efficiency Human Respiratory Droplet Collector
• Subject breathes into a truncated cone, otherwise is unrestricted (no mouthpiece or mask)
• Pump draws air into the cone and through an impactor which collects particles greater than 5.0 μm onto Teflon surface
• Grow the particles by condensation
• Collect liquid particles with 1.0 μm impactor into buffer McDevitt J et al Aerosol Sci Tech 2013
Initial screening at Student Health Services or research
site
Exhaled particles collected wearing ear-loop surgical mask, with forced cough 10x every 10 min for 30 min
collection
Exhaled particles collected without mask, with forced cough 10x
every 10 min for 30 min collection
2nd np swab
Concentration of liquid fine particle
sample
Advertisement by email, school newspaper, electronic bulletin
boards, flyers
Rapid test positive OR fever >100F plus
cough?
Yes
No further participation
No
Health questionnaire
RTqPCR:Np swab
Coarse particlesFine particles
Culture on MDCK cells:
Fine Particles
Study Design 2009 Campaign
Milton DK et al. (2013) PLoS Pathog 9(3): e1003205.
Results 2009• Recruited patients January –
March, 2009• 41 cases tested• 38 cases with confirmed
influenza infection by RTqPCR of nasal swab
• Exhaled breath data collected successfully from 37 cases
Milton DK et al. (2013) PLoS Pathog 9(3): e1003205.
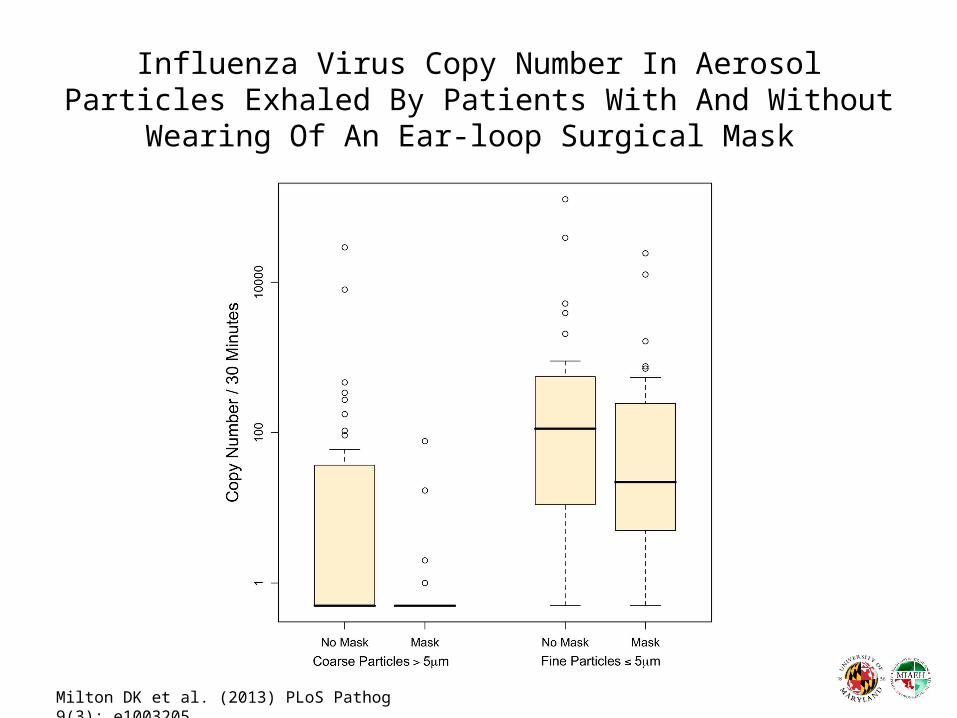
Influenza Virus Copy Number In Aerosol Particles Exhaled By Patients With And Without Wearing Of An
Ear-loop Surgical Mask
Milton DK et al. (2013) PLoS Pathog 9(3): e1003205.
EMIT: Evaluating Modes of Influenza Transmission (using a human challenge model)
• Influenza transmission challenge studies– Determine the contribution of aerosol particles to
transmission– Face shield intervention
• Characterize the exhaled particles in naturally infected and experimentally infected subjects

UMD Population Studied 2012-13
• Subjects: Students, staff, and neighbors of the University of Maryland at College Park, MD
• Recruitment: December 4, 2012 – March 15, 2013• Selection Criteria:
• Positive QuickVue Influenza A/B test OR fever 37.8°C plus a cough or sore throat
• AND within the first 3 days of onset of symptoms.• Questionnaire: age, gender, clinical illness symptoms, medical use,
medical and smoking history.• Data Management
– Paper collection of questionnaire– Entered into REDCap forms and reviewed by study physician
coordinator for data quality
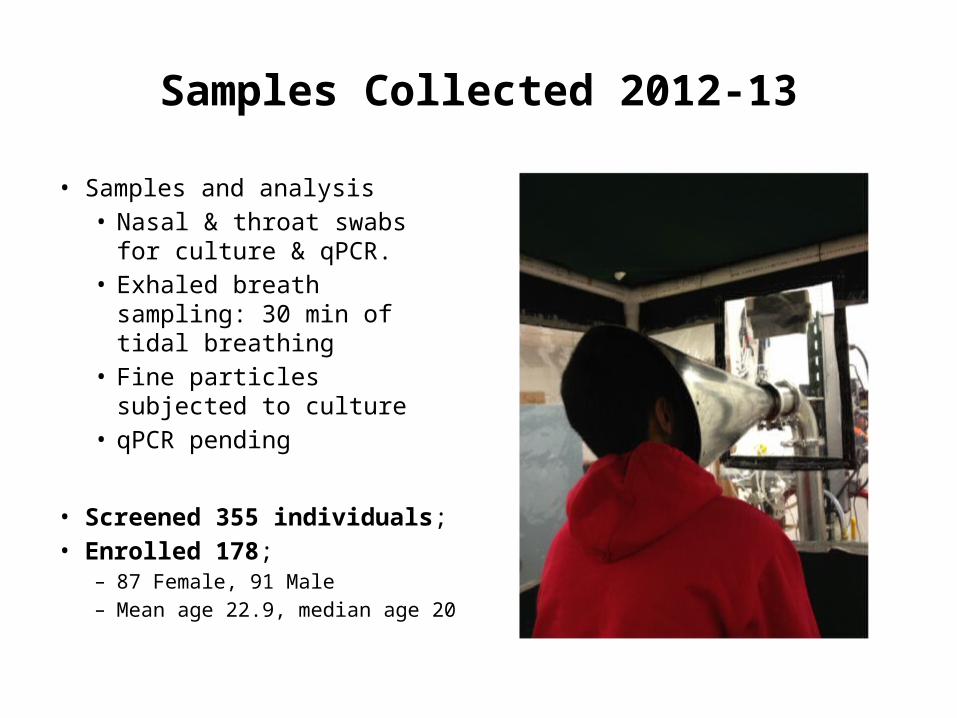
Samples Collected 2012-13
• Samples and analysis• Nasal & throat swabs for
culture & qPCR.• Exhaled breath sampling: 30
min of tidal breathing• Fine particles subjected to
culture• qPCR pending
• Screened 355 individuals; • Enrolled 178;
– 87 Female, 91 Male– Mean age 22.9, median age 20
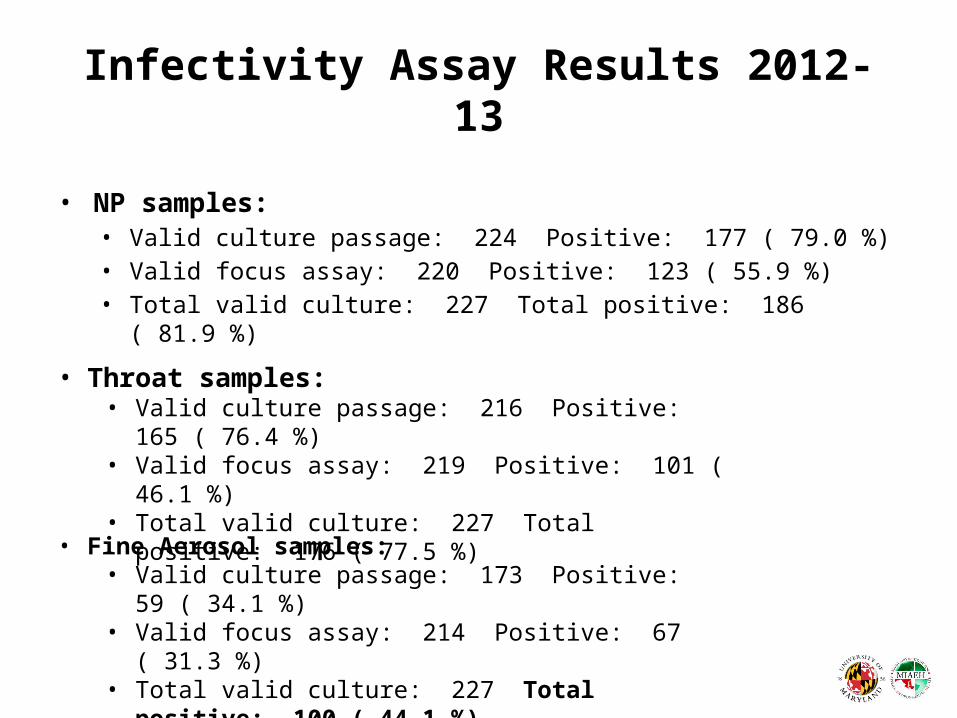
Infectivity Assay Results 2012-13
• NP samples: • Valid culture passage: 224 Positive: 177 ( 79.0 %)• Valid focus assay: 220 Positive: 123 ( 55.9 %)• Total valid culture: 227 Total positive: 186 ( 81.9 %)
• Throat samples: • Valid culture passage: 216 Positive: 165 ( 76.4 %)• Valid focus assay: 219 Positive: 101 ( 46.1 %)• Total valid culture: 227 Total positive: 176 ( 77.5 %)
• Fine Aerosol samples: • Valid culture passage: 173 Positive: 59 ( 34.1 %)• Valid focus assay: 214 Positive: 67 ( 31.3 %)• Total valid culture: 227 Total positive: 100 ( 44.1 %)
Fine particle aerosol only. Zeros are coded as 0.1 for presentation on the log scale.
Human Challenge Studies
• Series of 3 quarantine studies (planned 45 volunteers per cohort): Feb to June 2013
• Initiation of infection in healthy seronegative adults (Donors) using GMP A/Wisconsin/H3N2/67/2005
• Exposure of seronegative Recipients to Donors
• Intervention arm – face shield and hand hygiene to allow transmission by droplet nuclei only
• In effect 2AR (full Tmx) vs. 2AR (droplet nuclei only)

Exposure Events
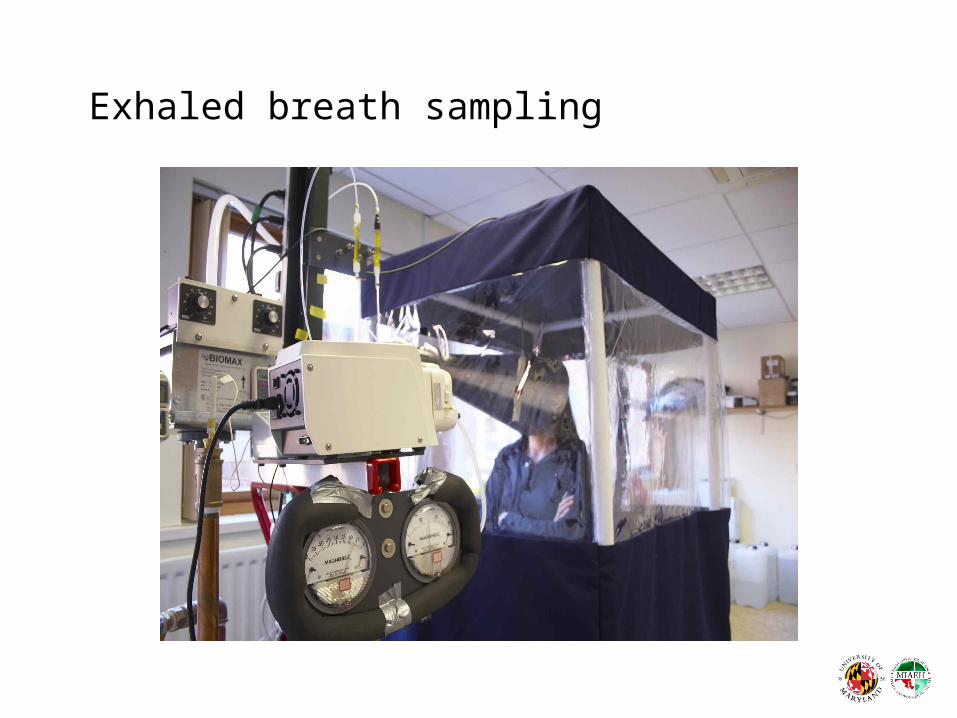
Exhaled breath sampling
Initial G-II Donor results Q3 (vs. wild type influenza A)
Cough Community & Donor Cases
Mechanism of Breath Aerosol Formation
Johnson & Morawska, 2009
New Technology
• G-III Design– Three stages (> 10 µm, 10-1 µm, < 1 µm)– All stages collect in liquid medium– Fine particles collected in 0.10 to 1.0 mL regardless of sampling time
• 100 to 1000 fold increase in concentration• No losses during concentration step
– Integrated particle counter– Integrated microfluidic sensor systems
• Two versions: – High flow with cone for unrestricted sampling– Lower flow with mouthpiece for physiologic studies
• IARPA – BIC Project
Same Debate?
• High concentration in some fluids – but not known for respiratory fluids at level of fine particle generation
• Much longer tubular forms may inhibit aerosolization
• Need data
The Aerobiological Pathway for Transmission of Communicable
Respiratory Disease
A: Source, B: Transport and Dispersion, C: DepositionRoy C and Milton DK, New Engl J Med, 2004
The UMD EMIT TeamFaculty, Postdocs, Grad Students and Staff• Sheryl Ehrman, PhD• Michael Grantham, PhD• Larissa May, MD• Barbara Albert, MD• Min Qi Wang, PhD• Jovan Panetlic, PhD• Fengjie Liu, PhD• Jing Yan• Maurice Rocque• Aneeqa Chowdhury• Emma Claye• Emily Chimiak• Ryan Grove• Jake Guag
Undergraduate Students
• Joey Avizad• Sam Choi• Naomi Cole• Michelle Ehiriodo• Somayah Eltoweissy• Lindsey Ferry• Alexandra Hudson• Ashley Kang• Shea Kozak• Katherine Leppart• Domonique Parkes• Paren Patel• Audrey Ready• Roberto Rosario• Dana Silverstein• John Sittmann• Mariah Smith• Makeda Warde (HS Student)