Embed Size (px)
Citation preview

Inhibidores de CDK 4/6 en cáncer de
mama
Prof. Miguel Martín
Instituto de Investigación Sanitaria
Hospital Gregorio Marañón
Universidad Complutense
Madrid

Hanahan & Weinberg, Cell 2011
Cell Cycle deregulation: a Hallmark of cancer

Cell Cyle regulation
Malumbres M, CNIO 2014

Regulation of the G1/S Checkpoint in Breast Cancer
Lange et al. Endocrine-Related Cancer 2011;18:C19–C24; 1Caldon CE, et al. J Cell Biochem 2006;97:261–274; 2Buckley MF, et al. Oncogene 1993;8:2127–2133; 3Dickson C, et al. Cancer Lett 1995;90:43–50; 4Finn RS, et al. Breast Cancer Res 2009;11:R77
G2 S
M
G1
G0
D-type cyclins regulated in
response to mitogenic stimuli,
including activation of RTKs and
steroid hormone receptors1
• Cyclin D1 is amplified in
15–20% of breast
cancers2,3
• Human ER+ breast
cancer cell lines (including
those with HER2
amplification) sensitive to
G0/G1 arrest4

Regulation of the G1/S Checkpoint in Breast Cancer
Lange et al. Endocrine-Related Cancer 2011;18:C19–C24; 1Caldon CE, et al. J Cell Biochem 2006;97:261–274; 2Buckley MF, et al. Oncogene 1993;8:2127–2133; 3Dickson C, et al. Cancer Lett 1995;90:43–50; 4Finn RS, et al. Breast Cancer Res 2009;11:R77
RB
RB
Gene
transcription G2 S
M
G1
G0
P P P
P
Inactive
Active tumor
suppressor
E2F
E2F
R
D-type cyclins regulated in
response to mitogenic stimuli,
including activation of RTKs and
steroid hormone receptors1
• Cyclin D1 is amplified in
15–20% of breast
cancers2,3
• Human ER+ breast
cancer cell lines (including
those with HER2
amplification) sensitive to
G0/G1 arrest4

Regulation of the G1/S Checkpoint in Breast Cancer
Lange et al. Endocrine-Related Cancer 2011;18:C19–C24; 1Caldon CE, et al. J Cell Biochem 2006;97:261–274; 2Buckley MF, et al. Oncogene 1993;8:2127–2133; 3Dickson C, et al. Cancer Lett 1995;90:43–50; 4Finn RS, et al. Breast Cancer Res 2009;11:R77
RB
RB
Gene
transcription G2 S
M
G1
G0
P P P
P
Inactive
Active tumor
suppressor
E2F
E2F
R
CDK4/6 Cyclin D
D-type cyclins regulated in
response to mitogenic stimuli,
including activation of RTKs and
steroid hormone receptors1
• Cyclin D1 is amplified in
15–20% of breast
cancers2,3
• Human ER+ breast
cancer cell lines (including
those with HER2
amplification) sensitive to
G0/G1 arrest4

Regulation of the G1/S Checkpoint in Breast Cancer
Lange et al. Endocrine-Related Cancer 2011;18:C19–C24; 1Caldon CE, et al. J Cell Biochem 2006;97:261–274; 2Buckley MF, et al. Oncogene 1993;8:2127–2133; 3Dickson C, et al. Cancer Lett 1995;90:43–50; 4Finn RS, et al. Breast Cancer Res 2009;11:R77
RB
RB
Gene
transcription G2 S
M
G1
G0
P P P
P
Inactive
Active tumor
suppressor
E2F
E2F
R
CDK4/6 Cyclin D
Pl3K/Akt
STATs MAPKs
ER/PR/AR Wnt/β-catenin
NF-κB D-type cyclins regulated in
response to mitogenic stimuli,
including activation of RTKs and
steroid hormone receptors1
• Cyclin D1 is amplified in
15–20% of breast
cancers2,3
• Human ER+ breast
cancer cell lines (including
those with HER2
amplification) sensitive to
G0/G1 arrest4

Regulation of the G1/S Checkpoint in Breast Cancer
Lange et al. Endocrine-Related Cancer 2011;18:C19–C24; 1Caldon CE, et al. J Cell Biochem 2006;97:261–274; 2Buckley MF, et al. Oncogene 1993;8:2127–2133; 3Dickson C, et al. Cancer Lett 1995;90:43–50; 4Finn RS, et al. Breast Cancer Res 2009;11:R77
RB
RB
Gene
transcription G2 S
M
G1
G0
P P P
P
Inactive
Active tumor
suppressor
E2F
E2F
R
CDK4/6 Cyclin D
Pl3K/Akt
STATs MAPKs
ER/PR/AR Wnt/β-catenin
NF-κB
p16
p21
p53 D-type cyclins regulated in
response to mitogenic stimuli,
including activation of RTKs and
steroid hormone receptors1
• Cyclin D1 is amplified in
15–20% of breast
cancers2,3
• Human ER+ breast
cancer cell lines (including
those with HER2
amplification) sensitive to
G0/G1 arrest4

Paloma 1/TRIO 018: Phase 2 Design
N = 66
1:1
Part 1
ER+, HER2–
BC
R
A
N
D
O
M
I
Z
A
T
I
O
N
PD 0332991
125 mg QDa +
Letrozole
2.5 mg QD
Letrozole
2.5 mg QD
Part 2
N = 99
1:1
ER+, HER2–
BC with
CCND1 amp
and/or
loss of p16
R
A
N
D
O
M
I
Z
A
T
I
O
N
PD 0332991
125 mg QDa +
Letrozole
2.5 mg QD
Letrozole
2.5 mg QD
Stratification Factors
• Disease Site (Visceral vs Bone only vs Other)
• Disease-Free Interval (>12 vs ≤12 mo from end of
adjuvant to recurrence or de novo advanced disease) a Schedule 3/1.
• Post-menopausal women, ER+/Her2 negative, RECIST measureable or bone only
• Primary endpoint: PFS (powered for 50% improvement; 9 > 13.5 months
• Analyses presented: IMPAKT 2012, SABCS 2012, AACR 2014 (Final)
Clintrial.gov; Finn RS, et al SABCS 2012, Abstract S1-6

PALOMA 1-TRIO 018. Results: Final Analysis. PFS (ITT)
Finn et al AACR 2014

PALOMA 1-TRIO 018. Results: Final Analysis. OS (ITT)
Finn et al AACR 2014

Most Common Treatment-Related AEs ≥10% (AT)
PD 991 + LET (n = 83)
LET (n = 77)
Grade 1/2 Grade 3 Grade 4 Grade 1/2 Grade 3 Grade 4
Neutropenia 19 46 5 1 1 0
Leukopenia 24 14 0 0 0 0
Anemia 19 4 1 0 0 0
Fatigue 17 2 0 13 0 0
Alopecia 18 0 0 3 0 0
Hot flush 17 0 0 10 0 0
Arthralgia 16 0 0 10 0 0
Nausea 12 2 0 1 0 0
Thrombocytopenia 11 1 0 0 0 0

CDK4/6 inhibitors currently in development
Agent Company Development
Status
Palbociclib
(PD0332991)
Pfizer Phase III
Ribociclib (LEE011) Novartis Phase III
Abemaciclib
(LY28335219)
Lilly Phase III

Palbociclib in HR+/HER2– BC: Phase 3 Studies
Metastatic breast cancer Post-
neoadjuvant
Study 1008 (PALOMA-2) 1023 (PALOMA-3) PEARL PENELOPE
Setting Endocrine
sensitive
Endocrine
resistant
Endocrine
resistant High risk
Menopausal status Post-menopausal Pre-menopausal +
post-menopausal Post-menopausal
Pre-menopausal +
post-menopausal
No. patients 650 521 348 800
Treatment arms
Palbociclib +
letrozole
vs. placebo +
letrozole
Palbociclib +
fulvestrant
vs. placebo +
fulvestrant
Palbociclib +
exemestane
vs. capecitabine
Palbociclib
vs. placebo
Primary endpoint PFS PFS PFS iDFS
FFPV, first patient first visit; iDFS, invasive disease-free survival; PFS, progression-free survival

Abstract LBA502
A Double Blind Phase 3 Trial of Fulvestrant With or Without
Palbociclib in Pre- and Post-menopausal Women With
Hormone Receptor-positive, HER2-negative Advanced Breast
Cancer That Progressed on Prior Endocrine Therapy
(PALOMA3 Study)
Nicholas Turner,1 Jungsil Ro,2 Fabrice André,3 Sherene Loi,4 Sunil Verma,5 Hiroji Iwata,6 Nadia Harbeck,7 Sibylle Loibl,8 Cynthia Huang Bartlett,9 Ke Zhang,10
Carla Giorgetti,11 Sophia Randolph,10 Maria Koehler,9 Massimo Cristofanilli12
1Royal Marsden Hospital, London, UK; 2National Cancer Center, Goyang-si, Korea; 3Institut Gustave Roussy, Villejuif, France; 4Peter MacCallum Cancer Centre, East Melbourne, Victoria, Australia; 5Sunnybrook Odette Cancer Centre,
Toronto, Canada; 6Aichi Cancer Center Hospital, Nagoya, Japan; 7Brustzentrum der Universität München, München, Germany; 8German Breast Group Forschungs GmbH, Neu-Isenburg, Germany; 9Pfizer Inc, New York City, USA; 10 Pfizer
La Jolla, USA; 11Pfizer Milan, Italy, 12Thomas Jefferson University, Philadelphia, PA, USA
Presented at ASCO 2015; June 1, 2015; Chicago, IL, USA

PALOMA3 Study Design
Placebo
(3 wks on/ 1wk off)
+
Fulvestrant†
(500 mg IM q4w)
Palbociclib
(125 mg QD;
3 wks on/1 wk off)
+
Fulvestrant† (500 mg IM q4w)
†administered on Days 1 and 15 of Cycle 1.
● Visceral metastases
● Sensitivity to prior
hormonal therapy
● Pre-/peri- vs Post-
menopausal
Clinicaltrials.gov NCT01942135
2:1 Randomization
N=521
Stratification:
• Post-menopausal patients must have progressed on prior aromatase inhibitor therapy.
n=347
n=174
• HR+, HER2– ABC
• Pre-/peri-* or post-menopausal
• Progressed on prior endocrine
therapy:
– On or within 12 mo adjuvant
– On therapy for ABC
• ≤1 prior chemotherapy regimen
for advanced cancer
*All received goserelin.

Study Endpoints
● Primary Endpoint
– Progression-free survival (PFS) by investigator assessment
● Secondary Endpoints
– Objective response and clinical benefit rate
– Overall survival
– Safety
– Biomarkers
– Patient-reported outcomes

Statistical Design
● PFS by investigator assessment
– Median PFS from 6 to 9.38 months (HR: 0.64; 90% power, 1-sided =2.5%)*
– Planned 417 patients randomized and 238 PFS events
● Interim Analysis (IA) for PFS
– Planned after approximately 60% (143) of PFS events
– Pre-specified Haybittle-Peto efficacy boundary (1-sided =0.00135)
● Blinded independent central review (BICR)1
– Randomly selected subgroup (approximately 40%)
1. Zhang JJ et al. Clin Cancer Res. 2013;19:2637-45. *2-sided P values are presented.

Demographics and Baseline Tumor Characteristics
Characteristic Palbociclib +
Fulvestrant
(n=347)
Placebo +
Fulvestrant
(n=174)
Median age (range), years 57 (30−88) 56 (29−80)
Receptor status, %
ER+ PR+ 69 64
ER+ PR– 26 28
ECOG performance status, %
0 60 66
1 40 34
Menopausal status,a %
Pre-/peri 21 21
Post 79 79
Visceral metastases,b % 59 60
Number of disease sites, %
1 32 35
2 29 29
3 39 36 aBased on randomization; blung, liver, brain, pleural, and peritoneal involvement.

Tumor Characteristics and Prior Treatment
Characteristic
Palbociclib +
Fulvestrant
(n=347)
Placebo +
Fulvestrant
(n=174)
Documented sensitivity to prior hormonal
therapy,a %
Yes 79 78
No 21 22
Prior aromatase inhibitor +/- GnRH,b % 85 87
Prior tamoxifen +/- GnRH,b % 61 60
Prior chemotherapy in advanced setting,
% 31 36
Prior lines of therapy in advanced setting,
%
0 24 26
1 38 40
2 26 25
≥3 12 9 aRelapsed after 24 months of adjuvant endocrine therapy or had clinical benefit to prior therapy in the advanced setting. bAny prior endocrine therapy anytime before study entry.
GnRH=gonatotropin-releasing hormone.

Tumor Characteristics and Prior Treatment
Characteristic Palbociclib +
Fulvestrant
(n=347)
Placebo +
Fulvestrant
(n=174)
Documented sensitivity to prior hormonal
therapy,a %
Yes 79 78
No 21 22
Prior aromatase inhibitor +/- GnRH,b % 85 87
Prior tamoxifen +/- GnRH,b % 61 60
Prior chemotherapy in advanced setting,
% 31 36
Prior lines of therapy in advanced setting,
%
0 24 26
1 38 40
2 26 25
≥3 12 9 aRelapsed after 24 months of adjuvant endocrine therapy or had clinical benefit to prior therapy in the advanced setting. bAny prior endocrine therapy anytime before study entry.
GnRH=gonatotropin-releasing hormone.

● Neutropenia was the most common AE leading to dose reductions (21%) and interruptions (45%)
Treatment Summary
*ITT population.
AE=adverse event; AT=as treated.
Treatment Summary (AT population)
Palbociclib
+
Fulvestrant
(n=345)
Placebo +
Fulvestrant
(n=172)
Relative fulvestrant dose intensity (%),
median 99.7 100
Relative palbociclib/placebo dose
intensity (%), median 91.7 100
Dose interruptions due to AEs, % 54 4
Cycle delays due to AEs, % 22 1
Dose reductions due to AEs, % 32 2
Discontinuations due to AEs, %* 2.6 1.7

Adverse Events—All Cause
AE, % Palbociclib + Fulvestrant
(n=345)
Placebo + Fulvestrant
(n=172)
Any Grade Grade 3 Grade 4 Any Grade Grade 3 Grade 4
Any AE 98 59 11 89 16 2
Neutropenia 79 53 9 3 0 1
Leukopenia 46 25 1 4 0 1
Anemia 26 3 0 10 2 0
Thrombocytopenia 19 2 1 0 0 0
Fatigue 38 2 0 27 1 0
Nausea 29 0 0 26 1 0
Headache 21 <1 0 17 0 0
Upper respiratory infectiona 19 <1 0 16 0 0
Diarrhea 19 0 0 17 1 0
Constipation 17 0 0 14 0 0
Alopecia 15 0 0 6 0 0
AE=adverse event. AEs with ≥15% incidence in the palbociclib + fulvestrant group reported. aUpper respiratory infection includes influenza, influenza-like illness, laryngitis, nasopharyngitis or pharyngitis, rhinitis, sinusitis, and upper respiratory tract infection.

Summary of Adverse Events
● In patients receiving palbociclib + fulvestrant vs placebo + fulvestrant:
– Overall incidence of SAEs was similar (9.6% vs 14.0%)
– Incidence of febrile neutropenia was the same (0.6% vs 0.6%)
– Infections (any grade) were more common (34.2% vs 24.4%)
• The vast majority were of grade 1 or 2 (32.5% vs 22.7%)
● There were no deaths due to AEs/toxicity
AE=adverse event; SAE=serious adverse event.

0 2 4 6 8 10 12
Time (Month)
0
10
20
30
40
50
60
70
80
90
100
PF
S P
rob
ab
ilit
y (
%)
347 279 132 59 16 6 PAL+FUL
174 109 42 16 6 1 PCB+FUL
Number of patients at risk
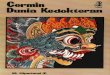
Primary Endpoint: PFS (ITT Population)
CI=confidence interval; HR=hazard ratio; ITT=intent-to-treat; NE=not estimable; PFS=progression-free survival.
Palbociclib
+
Fulvestrant
n=347
Placebo +
Fulvestrant
n=174
Median PFS,
months
(95% CI)
9.2
(7.5, NE)
3.8
(3.5, 5.5)
HR (95% CI) 0.422 (0.318, 0.560)
2-sided P value <0.000001

PAL+FUL
147
118 53 24 7 2
PCB+FUL 64 37 12 4 1 1
12
PF
S P
rob
ab
ilit
y (
%)
0 2
Number of patients at risk
4 6
Time (Month)
8 10
CI=confidence interval; NE=not estimable; PFS=progression-free survival.
PFS: Central Blinded Review Audit (n=211)
Palbociclib
+
Fulvestrant
n=147
Placebo +
Fulvestrant
n=64
Median PFS,
months
(95% CI)
NE 3.7
(3.4, 7.2)
HR (95% CI) 0.268 (0.158, 0.455)
2-sided P value <0.000001
0
10
20
30
40
50
60
70
80
90
100

PFS: Patient Subgroup Analysis
ER=estrogen receptor; PgR=progesterone receptor. aRace was unspecified in 2 patients (1 in each treatment group).
Subgroup Hazard Ratio and 95% CI
All randomized patients (ITT) Age
Racea
Menopausal status at study entry
<65 Years 65 Years
White Asian Black and other
Pre/Peri Post
Site of metastatic disease Visceral Non visceral
Sensitivity to prior hormonal therapy Yes No
Receptor status ER+/PgR+ ER+/PgR-
Disease-free interval 24 months
>24 months Prior chemotherapy
(Neo)adjuvant only Metastatic +/- (neo)adjuvant No prior chemotherapy
Prior lines of therapy in advanced setting 0 1 2 3+
In favor of Placebo + Fulvestrant In favor of Palbociclib + Fulvestrant
n (%)
521 (100) 392 (75.2) 129 (24.8) 385 (73.9) 105 (20.2)
29 (5.6) 108 (20.7) 413 (79.3) 311 (59.7) 210 (40.3) 410 (78.7) 111 (21.3) 349 (67.0) 139 (26.7)
65 (12.5) 281(53.9) 219 (42.0) 170 (32.6) 132 (25.3) 129 (24.8) 202 (38.8) 133 (25.5) 57 (10.9)
P value for Interaction
0.480
0.412
0.940
0.624
0.302
0.883
0.149
0.427
0.684
0.125 0.25 0.5 1 2 8

PFS: Patient Subgroup Analysis
ER=estrogen receptor; PgR=progesterone receptor. aRace was unspecified in 2 patients (1 in each treatment group).
Subgroup Hazard Ratio and 95% CI
All randomized patients (ITT) Age
Racea
Menopausal status at study entry
<65 Years 65 Years
White Asian Black and other
Pre/Peri Post
Site of metastatic disease Visceral Non visceral
Sensitivity to prior hormonal therapy Yes No
Receptor status ER+/PgR+ ER+/PgR-
Disease-free interval 24 months
>24 months Prior chemotherapy
(Neo)adjuvant only Metastatic +/- (neo)adjuvant No prior chemotherapy
Prior lines of therapy in advanced setting 0 1 2 3+
In favor of Placebo + Fulvestrant In favor of Palbociclib + Fulvestrant
n (%)
521 (100) 392 (75.2) 129 (24.8) 385 (73.9) 105 (20.2)
29 (5.6) 108 (20.7) 413 (79.3) 311 (59.7) 210 (40.3) 410 (78.7) 111 (21.3) 349 (67.0) 139 (26.7)
65 (12.5) 281(53.9) 219 (42.0) 170 (32.6) 132 (25.3) 129 (24.8) 202 (38.8) 133 (25.5) 57 (10.9)
P value for Interaction
0.480
0.412
0.940
0.624
0.302
0.883
0.149
0.427
0.684
0.125 0.25 0.5 1 2 8

Summary of Key Secondary Efficacy Endpoints
CBR=clinical benefit rate (CR+PR+SD ≥24 wk); CR=complete response; ORR=objective response (CR+PR); OS=overall survival; PR=partial response;
SD=stable disease.
* CBR is underestimated.
36% of palbociclib and 24% of placebo pts remain on study treatment with <24 weeks of follow up.
At the time of the interim analysis, OS data was immature with 28 deaths.
Palbociclib +
Fulvestrant
(n=347),
% of patients
Placebo +
Fulvestrant
(n=174),
% of patients
P value
ORR 10.4 6.3 0.1582
CBR* 34.0 19.0 0.0004

Conclusions
● Palbociclib combined with fulvestrant improved PFS compared to
placebo and fulvestrant in women with HR+/HER2– advanced breast
cancer whose disease had progressed on prior endocrine therapy.
– HR = 0.422 (95% CI, 0.318 to 0.560; P<0.000001)
● Benefit from palbociclib was also demonstrated across pre-specified
subgroups.
● Palbociclib was well tolerated.
● Palbociclib in combination with fulvestrant is an effective treatment
option for women whose cancer progressed on prior endocrine
therapy.