Embed Size (px)
Citation preview

Journal of Microencapsulation, 2010; 27(6): 471–478
RESEARCH ARTICLE
Insulin-S.O (sodium oleate) complex-loaded PLGAnanoparticles: Formulation, characterization andin vivo evaluation
Shaoping Sun1,2,3, Na Liang1, Hongze Piao1, Hiromitsu Yamamoto3, Yoshiaki Kawashima3
and Fude Cui1
1School of Pharmacy, Shenyang Pharmaceutical University, Shenyang , PR China, 2School of Chemistry andMaterial Science, Heilongjiang University, Harbin, PR China, and 3School of Pharmaceutical Science, Aichi GakuinUniversity, Nissin, Japan
AbstractS.O (sodium oleate) is an anionic surfactant, which is able to forman ionic complex with positively chargedinsulin at suitable pH. In a previous study, the insulin-S.O (Ins-S.O) complex was prepared by a hydro-phobic ion pairing (HIP) method to improve the apparent liposolubility of insulin. The formation of thecomplex was further confirmed by Zeta potential and X-ray method. Based on the preliminary study,poly(lactide-co-glycolide) (PLGA) nanoparticles harbouring Ins-S.O complex was prepared via an emulsionsolvent diffusion method. The effects of key parameters such as concentration of PVA, concentration ofPLGA and initial-loaded drug on the properties of the nanoparticles were investigated. The insulinencapsulation efficiency (EE(%)) reached up to 91.2% and mean diameter of the nanoparticles wassized �160 nm under optimal conditions. The pharmacological effects of the nanoparticles made ofPLGA (75/25, Av Mw 15 000) were further evaluated to confirm their potential suitability for oral delivery.In order to evaluate hyperglycaemic effect of the nanoparticles for oral administration, Ins-S.Ocomplex-loaded PLGA nanoparticles (20 IU/Kg) were administered orally by force-feeding to diabeticrats. In the case of the nanoparticles, the plasma glucose level reduced to 23.85% from the initial one12 h post-administration and this continued for 24 h. The results showed that the use of Ins-S.Ocomplex-loaded PLGA nanoparticles is an effective method of reducing plasma glucose levels. The insulinnanoparticles also improved the glycaemic response to an oral glucose challenge.
Key words: Insulin complex; sodium oleate; PLGA; nanoparticles; bioavailability
Introduction
Oral delivery of insulin is one of the greatest challenges
for drug delivery in modern pharmaceutical technology
because of various obstacles (Damge et al. 1990). These
obstacles include: (1) insulin is too hydrophilic to readily
cross the intestinal mucosa; (2) it is hard for insulin to be
absorbed from the intestinal lumen due to the tight junc-
tions in the epithelial lining (Carino and Mathiowitz 1999;
Kondoh and Yagi 2007); (3) insulin molecules will be
degraded in the gastrointestinal tract by the digestive
enzymes and acidity (Owens et al. 2003; Jintapattanakit
et al. 2007). Due to these barriers, the bioavailability of
insulin administered orally is very low. However, the oral
administration is the most preferable for its convenience
and good patient acceptability. In addition, orally deliv-
ered insulin undergoes a hepatic first pass before entering
the circulation, so it has the potential to mimic the effects
of pancreas-secreted insulin in terms of inhibition of hepa-
tic gluconeogenesis (Eaton et al. 1980; Lewis et al. 1996;
Clement et al. 2002; Damge et al. 2007). In order to over-
come the above obstacles for oral administration,
Address for correspondence: Fude Cui, School of Pharmacy, Shenyang Pharmaceutical University, No. 103, Wenhua Road, Shenyang 110016, PR China.Tel: þ86 24 23986355. Fax: þ86 24 23986355. E-mail: [email protected]
(Received 27 Jun 2009; accepted 29 Nov 2009)
ISSN 0265-2048 print/ISSN 1464-5246 online � 2010 Informa UK LtdDOI: 10.3109/02652040903515490 http://www.informahealthcare.com/mnc
(Received 27 Jun 2009; accepted 29 Nov 2009)
ISSN 0265-2048 print/ISSN 1464-5246 online � 2010 Informa UK LtdDOI: 10.3109/02652040903515490 http://www.informahealthcare.com/mnc
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

nanoparticles of biodegradable polymeric materials such
as poly(lactic acid), poly(glycolic acid) and their copoly-
mers poly(lactide-co-glycolide) (PLGA) have been widely
studied by our group (Cui et al. 2006, 2007). In spite of the
encouraging potential of oral applications of biodegrad-
able polymeric nanoparticles, there is a serious problem
with the particulate system that it is too hard for
water-insoluble polymers to encapsulate hydrophilic insu-
lin sufficiently.
It was reported that a hydrophobic ion pairing (HIP)
method had been used to enhance the hydrophobicity
of protein/peptides (Adjei et al. 1993; Matsuura et al.
1993; Meyer and Manning 1998). In order to encapsulate
more insulin in the hydrophobic copolymer, the hydro-
phobic ion pairing (HIP) technique has been applied to
prepare Ins-S.O complex to enhance the hydrophobicity of
insulin in our previous work (Sun et al. 2008). The tech-
nique of HIP is simply performed by the interaction
between ionic protein at suitable pH and the opposite
ionic head group of fatty acid, surface-active agents or
other amphiphilic molecules. In this study, Ins-S.O com-
plex was prepared in order to increase insulin EE(%) in
PLGA nanoparticles and oral bioavailability. Initially, a
more liposoluble Ins-S.O complex was prepared by com-
plexing insulin with S.O via the HIP method. The lyophi-
lized complex was then introduced into the organic
solvent containing polymer and subsequently loaded
into nanoparticles by an emulsion solvent diffusion
method. Following this, the physicochemical characteris-
tics of the nanoparticles, hypoglycaemic effect of
orally-administered Ins-S.O complex-loaded nanoparti-
cles and glycaemic response to an oral glucose challenge
were investigated in diabetic rats.
Materials and animals
Materials
Porcine insulin (27.7 IU/mg) was purchased from Xuzhou
Wanbang Biochemical Pharmaceutical Co., Ltd (China).
Sodium oleate was purchased from China National
Pharmaceutical Group Co. (Shanghai Reagent Branch).
PLGA (75 : 25, Av Mw 15 000) was obtained from the
Chengdu Institute of Organic Chemistry, Chinese
Academy of Sciences. Polyvinyl alcohol (PVA, Av Mw 30–
70 kDa, 88% hydrolysis) was supplied by Shin-Etsu
Chemical Co., Ltd. (Japan). Streptozotocin (STZ) was
obtained from Sigma-Aldrich (St. Louis, MO). A glucose
GOD-PAD kit was purchased from Beijing BHKT Clinical
Reagent Co., Ltd. (Beijing, China). All other reagents were
of chemical grade.
Animals
Male Wistar rats weighing 180–220 g, 12–13 weeks’ old,
were provided by the pharmacological laboratory of
Shenyang Pharmaceutical University of PR China.
Induction of diabetes
Wistar rats (body weight 180–220 g) were induced into dia-
betes by an injection of STZ (65 mg/kg body weight) in a
10 mM citrate buffer at pH 4.5, as previously described
(Damge et al. 1988). The concentration of the STZ was
13 mg/ml. Rats were considered diabetic when glycaemia
was higher than 16.67 mmol/dL 7 days after streptozotocin
treatment. The study protocol was reviewed and approved
by the Institutional Animal Care and Use Committee,
Shenyang Pharmaceutical University, PR China.
Methods
Preparation and characterization of Ins-S.O complex
Ins-S.O complex was prepared by a hydrophobic ion pair-
ing method (Sun et al. 2008). Briefly, various amounts
of sodium oleate (S.O) were dissolved in 1 ml of HCl solu-
tion (pH¼ 4.0), then the solution was slowly added in a
dropwise manner into 4 ml of 1.0 mg/ml insulin solution
(pH¼ 4.0) under magnetic stirring. The cloudy mixture
was then centrifugated at 14 000 rpm for 15 min to get
the precipitate. The precipitate was washed three times
with distilled water and then was freeze-dried overnight
at a condenser temperature of �53.7�C and under a
vacuum of 7.3 Pa to get the complex. The insulin com-
plexation efficiency (CE%) was calculated according to
the following formula:
CEð%Þ ¼Mi �Mf
Mi� 100 ð1Þ
where, Mi and Mf represent the amount of initial added
insulin and the amount of free insulin in supernatant,
respectively. The amount of insulin was measured by an
HPLC method. Briefly, the HPLC system was equipped
with a Hitachi pump L-7110, a Hitachi UV-Vis Detector
L-7420, an ODS C18 column (5mm, 150 mm� 4.6 mm)
and a thermostated column compartment. The mobile
phase was composed of 0.1 mol/L NaH2PO4 aqueous solu-
tion, 0.05 mol/l Na2SO4 aqueous solution and acetonitrile
at a ratio of 35 : 35 : 30 and the final pH was adjusted to
3.0 with H3PO4 solution. The detector wavelength, the
column temperature and the flow rate of the mobile
phase was set at 214 nm, 35�C and 1 ml/min, respectively,
the inject volume of the test samples was 20ml and the
472 S. Sun et al.
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

retention time was 7.22 min. The zeta potentials of Ins-S.O
complexes in distilled water medium were evaluated in
order to assess the optimal molar ratio of S.O to insulin
for the charge–charge interaction, using a Zetasizer
Nano-ZS90 (Malvern Instruments, UK) at 25�C. The
X-ray was used to confirm the formation of the Ins-S.O
complex using X-ray Diffractometer (D/max-r A, Rigaku
Denki, Japan).
Preparation and characterization of Ins-S.O
complex-loaded PLGA nanoparticles
PLGA nanoparticles loaded with Ins-S.O complex were
prepared using an emulsion solvent diffusion method.
More specifically, a determined amount of PLGA polymer
and Ins-S.O complex was dissolved in the organic phase
of acetone including a slight of 0.01 M HCl (to solutize
(accelerate the dissolution rate). Ins-S.O complex in
organic phase). Then the oil phase was poured into mag-
netically stirred (500 rpm) aqueous solution containing a
different amount of PVA. The organic phase was then
removed under reduced pressure, leaving behind a colloi-
dal suspension of PLGA nanoparticles in water. Unless
otherwise mentioned, all the experiments were conducted
by varying one of the parameters while keeping all the
other process parameters unchanged: 1 mg insulin-
equivalent Ins-S.O complex and 20 mg of PLGA was dis-
solved in 1 ml of acetone with a slight of 0.01 M HCl as the
organic phase and 20 ml of 1% PVA solution as the aque-
ous phase. The solidified nanoparticles were recovered by
ultracentrifugation at 20 000 rpm for 10 min, washed and
dispersed with distilled water under vortex three times,
followed by lyophilization. The concentration of insulin
in the supernatant was analysed by the HPLC method
mentioned above and the entrapped insulin fraction was
calculated based on the initial amount of insulin added.
The particle size distribution, expressed as mean diameter
and polydispersity index (PDI), was determined by photon
correlation spectroscopy (PCS) using Zetasizer Nano-ZS90
(Malvern Instruments, UK). The lyophilized nanoparticle
samples were suspended in distilled water before mea-
surement. Morphology of the formulated nanoparticles
was observed by SEM, Jeol JSM 5600LV, which requires
an ion coating with platinum by a sputter coater
(JFC-1300, Jeol, Tokyo) for 40 s in a vacuum at a current
intensity of 40 mA after preparing the sample on metallic
studs with double-sided conductive tape.
In vivo bioactivity evaluation
The in vivo bioactivity of insulin in the complex and
PLGA nanoparticles was evaluated in normal rats.
Eighteen normal rats (200� 20 g) were divided into three
groups randomly (six rats in each group) and were fasted
overnight but had free access to water. Test solutions were
prepared as follows: for group 1, the theoretical amount of
insulin in supernatant (TAIS) was measured by the fol-
lowing method: 100 mg of freeze-dried nanoparticles (for-
mulation C, particle size �160 nm) was dissolved in 10 ml
of acetonitrile to solubilize the polymer and precipitate
the insulin, the samples were centrifuged at 20 000 rpm
for 15 min and the pellet was dissolved in a slight of
DMSO and then was diluted by phosphate buffer saline
(pH¼ 7.4). The amount of insulin in pellet (AIP) was mea-
sured by the HPLC method as mentioned above. The the-
oretical amount of insulin in supernatant (PBS 7.4)
(TAIS) was calculated by the following formula, where
TAP represents total amount of insulin in 100 mg of
PLGA nanoparticles.
TAIS ¼ ðTAP� AIPÞ ð2Þ
For group 2, Ins-S.O complex was first dissolved in a
slight of DMSO, then was introduced in phosphate buffer
saline (pH¼ 7.4). The theoretical amount of insulin in the
complex (TAIC) was calculated by the following formula,
where TAI and TAS represent total amount of initial insu-
lin and total amount of insulin in supernatant (TAS)
during preparation of the complex, respectively.
TAIC ¼ ðTAI� TASÞ ð3Þ
For group 3 (control group), insulin was dissolved in
phosphate buffer saline (pH¼ 7.4). All of the three solu-
tions were diluted to an insulin-equivalent concentration
of 1 IU/ml (theoretically) by phosphate buffer saline
(pH¼ 7.4) before administration. Blood samples were
collected from the retro-orbital plexus of the rats at 0 h
and 1 h after they were administered subcutaneously at
1 IU/kg. Plasma was separated by centrifugation at
4000 rpm for 5 min and the glucose level was determined
by the glucose oxidase method (GOD kit, Beijing BHKT
clinical Reagent Co. Ltd, China). The hypoglycaemic
response to insulin was characterized as follows: The ini-
tial plasma glucose (0 h) was taken as 100% level and the
plasma glucose at 1 h was calculated as percentage of the
initial one.
Investigation of hyperglycaemic effect and oral glucose
tolerance test
In order to display the biological efficacy of Ins-S.O
complex-loaded nanoparticles after oral administration,
two sets of experiments were performed. Thirty-six
STZ-induced male diabetic rats were divided into six
groups randomly (six rats in each group) and fasted
Insulin-S.O complex-loaded PLGA nanoparticles 473
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

overnight but had free access to water for both of the two
sets of experiment. In the first set, aqueous-free insulin
(1 IU/kg) was administered subcutaneously (S.C.) to the
first group of diabetic rats. Ins-S.O complex-loaded nano-
particles (20 IU/kg, formulation C, particle size �160 nm),
free insulin (20 IU/kg) and saline (control) were adminis-
tered orally to the second, third and fourth group, respec-
tively. In the second set, an oral glucose tolerance test
(OGTT) was performed: saline (control group) and
Ins-S.O complex nanoparticles (20 IU/kg, formulation C,
particle size�160 nm) were orally administered to the fifth
and sixth groups, respectively 1 h before they received an
oral dose of glucose (2 g/kg). For the two sets of experi-
ments, blood samples were collected from the inferior
ophthalmic vein at different time points. The methods
for plasma separation and glucose level determination
were as above. The hypoglycaemic response to insulin
was characterized as follows: the initial plasma glucose
was taken as 100% level and all following concentration–
time data was given accordingly as a percentage of the
baseline. The areas above the plasma glucose levels time
curves (AAC) were calculated using the trapezoidal rule
(Ritschel et al. 1988). The specific value of AAC of different
groups to the AAC of subcutaneous injection group was
used to calculate the pharmacological bioavailability. The
relative pharmacological bioavailability (PB%) was calcu-
lated using the following equation:
PB% ¼ ðAACoral=AACS:CÞ � ðDoseS:C=DoseoralÞ ð4Þ
Results and discussion
Preparation and characterization of Ins-S.O complex
The interaction of insulin and S.O in aqueous solution
was verified via measurements of the zeta potential.
Figure 1 indicated that the zeta potential of the Ins-S.O
complex passed from þ25.4� 6.55 mV through 0 and
reached a level of �62� 9.74 mV as the molar ratio of
S.O to insulin changed from 1.85 to 9.23. The net surface
charge on the Ins-S.O complex nearly became 0 as the
result of the complete complexation when the molar
ratio of S.O to insulin got to 6 : 1. When the molar ratio
of S.O to insulin was higher than 6 : 1, the zeta potential
remained negative, owing to increased S.O content.
As a polypeptide, insulin is composed of 51 amino acidic
residues and it has a net positive charge of 6 (due to two
histidine, one lysine, one arginine and two N-terminal
amino acid residues) at pH¼ 4.0 which was lower
than its IP (5.35–5.45), so it can be efficiently
complexed with anionic S.O at stoichiometic molar ratio
(S.O : insulin¼ 6 : 1). The complex efficiency was 96.6�
0.41% at this optimal condition. Figure 2 showed the
powder X-ray diffraction patterns of insulin, S.O, their
physical mixture and the complex. The insulin powder
and S.O powder diffraction pattern shown in Figures 2(a)
and (c) displayed partial sharp crystalline peaks. From
Figure 2(d) it can be observed that the crystalline peaks
had disappeared in the complex. However, some crystal-
line drug signal was still detectable in the physical mix-
tures of insulin and S.O in Figure 2(b). This suggested the
formation of the Ins-S.O complex and the complex was
amorphous form.
Preparation and characterization of Ins-S.O
complex-loaded nanoparticles
Due to the formation of Ins-S.O complex, the apparent
solubility of insulin in organic phase evidently increased
(Sun et al. 2008). So it was much easier to prepare the
nanoparticles via an emulsion solvent diffusion method.
On this basis, the effect of three major preparation vari-
ables on the mean diameter and EE(%) of Ins-S.O complex
nanoparticles were investigated in this study. The results
are shown in Table 1. Ideal particle properties were
obtained under the following conditions: 20 mg of PLGA
and 1 mg insulin-equivalent Ins-S.O complex in 1 ml of
acetone with a slight of HCl as the organic phase, 20 ml
of 1% PVA solution as the aqueous phase. The free insulin
loaded PLGA nanoparticles were prepared as control
under the same optimal conditions. EE(%) of Ins-S.O com-
plex in nanoparticles was 91.2% under this optimal condi-
tion, which was about twice of that of free insulin
(EE(%)¼ 42.5%). It illustrated that the HIP method was
an effective one to increase EE(%) of lipophobic insulin
into lipophilic PLGA nanoparticles. The SEM images of the
drug-loaded nanoparticles revealed their regular spherical
–80
–60
–40
–20
0
20
40
9.23:1
Molar ratio of S.O to insulin
mV
1.85:1 3.69:1 5.54:1 6.00:1 6.46:1 7.38:1
Figure 1. Changes in the zeta potential of the complex at different ratios
of S.O to insulin. Results are expressed as mean� SD, n¼ 3.
474 S. Sun et al.
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

shape (Figure 3). The zeta potential was measured as
�33.4 mV.
Effect of preparation variables on formulation
characteristics
Effect of PVA concentration in the external water
phase. PVA concentration in the external water phase
is known to be a key factor affecting the size of nanopar-
ticles and drugs EE(%). In the present work, 0.5%, 1% and
2% PVA solutions were used as the aqueous phase to study
the effect of PVA concentration on the characteristics of
the nanoparticles, as seen in Table 1. The results were
summarized in Table 2 (formulations A, B and C).
Evidently, a significant decrease in particle size and
EE(%) can be achieved by increasing the concentration
of PVA in the aqueous phase. The reasons for particle
size decreasing may be as follows. First, at high concen-
tration, more PVA can be oriented at the interface of
organic and aqueous phases to reduce the interfacial ten-
sion (Galindo-Rodriguez et al. 2004), which can lead to a
decrease of the net shear stress at a constant energy den-
sity (Nandi et al. 2001) during emulsification. Thus, the
mean diameter of nanoparticles decreased (from 744 nm
to 153 nm) as the PVA concentration increased. Secondly,
during the evaporation of organic solvent, the increase of
PVA concentration can inhibit the coalescence of droplets
and the aggregation of nanoparticles. This was a major
reason for decrease of the mean diameters. As far as
EE(%) is concerned, a significant decrease in insulin
EE(%) from 94.58% to 84.89% occurred as the concentra-
tion of PVA increased in aqueous phase. The decrease in
particle size may be a major reason for it. In addition, due
to the increase of PVA concentration, interfacial tension
decreased, which led to more Ins-S.O complex partition-
ing out more rapidly into the aqueous phase during the
emulsification procedure, hence decreasing the EE(%) of
the nanoparticles.
Effect of concentration of PLGA. As seen from Table 2
(formulations C, D and E), the mean diameter and
EE(%) of the nanoparticles increased (from 139 nm to
Figure 2. X-ray diffraction patterns of insulin, S.O, the physical mixture
and Ins-S.O complex.
Figure 3. Scanning electron micrograph of Ins-S.O complex-loaded
nanoparticles prepared under optimized conditions.
Table 1. Preparation parameters for Ins-S.O complex-loaded
nanoparticles.
Formulation
ID
Polymer
Con
(mg/ml)
PVA Con
(m/v)
Volume
of oil
phase
(ml)
Volume of
aqueous
phase
(ml)
Theoretical
loading
(m/m)
A 20 2% 1 20 5.00%
B 20 0.50% 1 20 5.00%
C 20 1% 1 20 5.00%
D 10 1% 1 20 5.00%
E 30 1% 1 20 5.00%
F 20 1% 1 20 6.10%
G 20 1% 1 20 3.60%
Table 2. Characteristics of Ins-S.O complex-loaded nanoparticles.
Formulation
ID
A B C D E F G
Particle
size (nm)
153 744 161 139 438 165 168
PDI 0.091 0.257 0.082 0.162 0.268 0.101 0.089
E (%) 84.89 94.58 91.21 76.73 93.58 81.16 92.57
Insulin-S.O complex-loaded PLGA nanoparticles 475
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

438 nm and from 76.73% to 93.58%, respectively) simulta-
neously with the increase of the PLGA concentration (from
10 mg/ml to 30 mg/ml) in the oil phase. As PLGA concen-
tration increased, the viscosity of the organic phase
increased, which makes the dispersion rate decreased
leading to the increased size of the nanoparticles. Also,
the increased size of nanoparticles and viscosity of organic
phase resulted in the increase of EE(%). In addition, the
increase of nanoparticles size and EE(%) may be due to
short PVA as PLGA concentration increased. As PLGA con-
centration increased, PVA was probably not enough to
cover the surface of droplets completely, which caused
the coalescence of particles during the evaporation of
organic solvent (Song et al. 2008).
Effect of initial-loaded drug. Table 2 (formulations C, F
and G) shows the effect of the initial-loaded drug on the
characteristics of nanoparticles. As seen in Table 2, with
the amount of Ins-S.O complex increased, the EE(%)
decreased (from 92.57% to 81.16%). However, the
amount of Ins-S.O complex has little effect on the particle
size. It was clear that increasing the Ins-S.O complex con-
centration in the oil phase could increase the concentra-
tion gradient of insulin between the oil phase and
the external water phase, and the drug diffusion from
the oil phase into the aqueous phase was promoted
(Li et al. 2004).
In vivo bioactivity evaluation
In order to verify whether insulin retained its bioactivity
during the complexation process and encapsulation pro-
cess, we evaluated the hypoglycaemic effect of free insulin,
insulin in the complex and in the PLGA nanoparticles by
subcutaneous method. Because the noticeable insulin
response to blood sugar appears 45–90 min after subcuta-
neous (S.C.) administration of insulin (Eneroth and
Ahlund 1968), the plasma glucose levels of rats after sub-
cutaneous administration of various samples were deter-
mined at 60 min.
It was found that subcutaneous administration in rats
reduced the plasma glucose level to almost the same per-
centage for free insulin, insulin in the complex and in the
complex loaded in PLGA nanoparticles. The plasma glu-
cose level for free insulin, insulin in the complex and in the
complex loaded PLGA nanoparticles were decreased to
59.0� 8.19%, 56.0� 6.28% and 57.8� 5.42%, respectively.
However, there was no significant difference. This result
clearly indicated that the insulin also retained its bioactiv-
ity in vivo during the preparation of the complex and the
PLGA nanoparticles. However, it was interesting that the
hypoglycaemic activity of insulin in the form of the com-
plex and the complex loaded PLGA nanoparticles was
slightly higher than that of free insulin. This could be
explained as follows: Usually, insulin exists as a hexamer
and it is required to disassociate into the dimer or further
monomer before being absorbed. The HIP method could
avoid the formation of a insulin hexamer (Polaschegg
1998).
Investigation of hyperglycaemic effect and oral
glucose tolerance test
Investigation of hyperglycaemic effect. In order to con-
firm the potential use of Ins-S.O complex-loaded PLGA
nanoparticles for oral delivery, the pharmacological effects
were evaluated in diabetic rats. From Figure 4, it was
observed that oral administration of the saline (control
group) and free insulin group (20 IU/kg) did not appreci-
ably lower the blood glucose levels of the animals.
Conversely, oral administration of Ins-S.O complex-
loaded nanoparticles (20 IU/kg) produced significant
plasma glucose reduction. Oral administration of Ins-S.O
complex-loaded PLGA nanoparticles reduced the fasting
plasma glucose level to 23.85% within the first 12 h and this
continued for 24 h. The pharmacological relative bioactiv-
ity to the S.C. was �11.5%. This phenomenon illustrated
that the Ins-S.O complex PLGA nanoparticles was an
effective candidate for decreasing blood glucose com-
pared with free insulin. The increased absorption of
Ins-S.O complex PLGA nanoparticles could be due to sev-
eral factors. First, when existing as Ins-S.O complex, insu-
lin can be absorbed through mucosal membrane present
in the oral route more easily because the apparent liposo-
lubility increased. Secondly, when encapsulated in PLGA
nanoparticles, insulin can partly avoid degradation by acid
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
Time (h)
Blo
od G
luco
se (
% o
f ini
tial)
0 2 4 6 8 10 12 14 16 18 20 22 24
Figure 4. Plasma glucose level after administration of various insulin
samples: Data represents the mean� SD, n¼ 6 per group (˙) SC injec-
tion of 1 IU/kg insulin solution, oral administration of (#) Ins-S.O com-
plex loaded PLGA nanoparticles (20 IU/kg), (�) free insulin (20 IU/kg)
and (m) saline.
476 S. Sun et al.
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.
and enzyme in the gastrointestinal tract. Furthermore, the
particle size of the complex was �160 nm. So the complex
may be taken up via the Peyer’s patches located in the
mucosa of the small intestine before insulin was degraded
(Desai et al. 1996). The absorption mechanism will be fur-
ther studied in our future works.
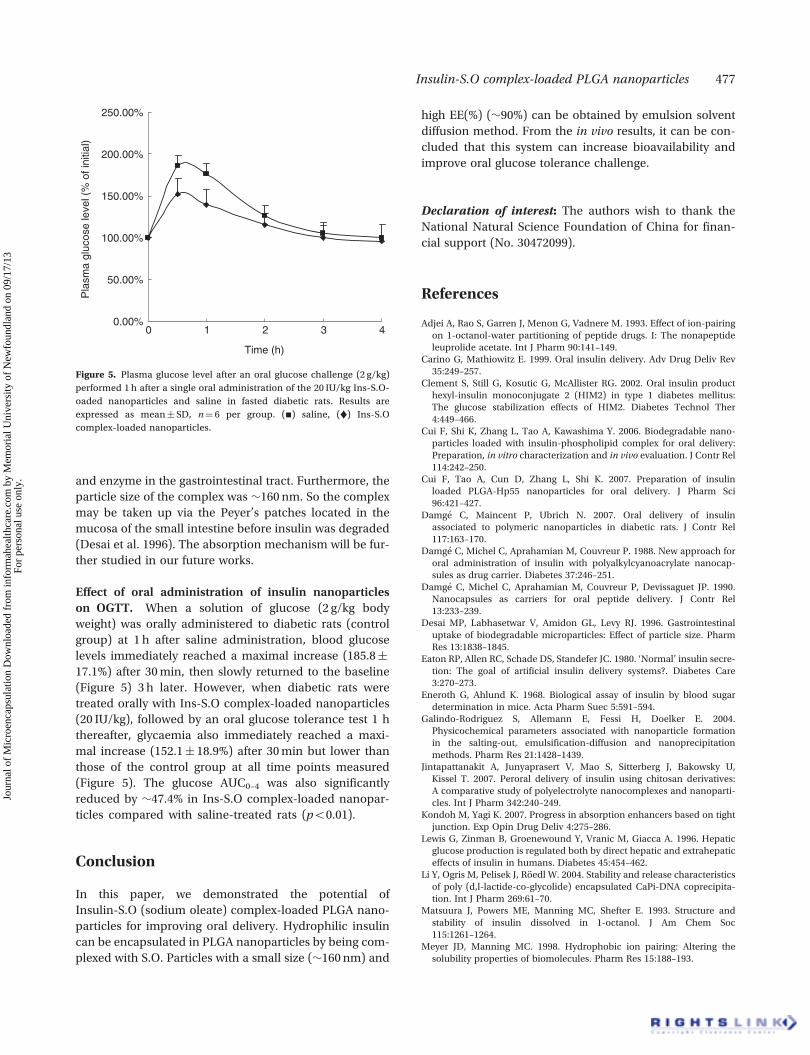
Effect of oral administration of insulin nanoparticles
on OGTT. When a solution of glucose (2 g/kg body
weight) was orally administered to diabetic rats (control
group) at 1 h after saline administration, blood glucose
levels immediately reached a maximal increase (185.8�
17.1%) after 30 min, then slowly returned to the baseline
(Figure 5) 3 h later. However, when diabetic rats were
treated orally with Ins-S.O complex-loaded nanoparticles
(20 IU/kg), followed by an oral glucose tolerance test 1 h
thereafter, glycaemia also immediately reached a maxi-
mal increase (152.1� 18.9%) after 30 min but lower than
those of the control group at all time points measured
(Figure 5). The glucose AUC0–4 was also significantly
reduced by �47.4% in Ins-S.O complex-loaded nanopar-
ticles compared with saline-treated rats (p50.01).
Conclusion
In this paper, we demonstrated the potential of
Insulin-S.O (sodium oleate) complex-loaded PLGA nano-
particles for improving oral delivery. Hydrophilic insulin
can be encapsulated in PLGA nanoparticles by being com-
plexed with S.O. Particles with a small size (�160 nm) and
high EE(%) (�90%) can be obtained by emulsion solvent
diffusion method. From the in vivo results, it can be con-
cluded that this system can increase bioavailability and
improve oral glucose tolerance challenge.
Declaration of interest: The authors wish to thank the
National Natural Science Foundation of China for finan-
cial support (No. 30472099).
References
Adjei A, Rao S, Garren J, Menon G, Vadnere M. 1993. Effect of ion-pairingon 1-octanol-water partitioning of peptide drugs. I: The nonapeptideleuprolide acetate. Int J Pharm 90:141–149.
Carino G, Mathiowitz E. 1999. Oral insulin delivery. Adv Drug Deliv Rev35:249–257.
Clement S, Still G, Kosutic G, McAllister RG. 2002. Oral insulin producthexyl-insulin monoconjugate 2 (HIM2) in type 1 diabetes mellitus:The glucose stabilization effects of HIM2. Diabetes Technol Ther4:449–466.
Cui F, Shi K, Zhang L, Tao A, Kawashima Y. 2006. Biodegradable nano-particles loaded with insulin-phospholipid complex for oral delivery:Preparation, in vitro characterization and in vivo evaluation. J Contr Rel114:242–250.
Cui F, Tao A, Cun D, Zhang L, Shi K. 2007. Preparation of insulinloaded PLGA-Hp55 nanoparticles for oral delivery. J Pharm Sci96:421–427.
Damge C, Maincent P, Ubrich N. 2007. Oral delivery of insulinassociated to polymeric nanoparticles in diabetic rats. J Contr Rel117:163–170.
Damge C, Michel C, Aprahamian M, Couvreur P. 1988. New approach fororal administration of insulin with polyalkylcyanoacrylate nanocap-sules as drug carrier. Diabetes 37:246–251.
Damge C, Michel C, Aprahamian M, Couvreur P, Devissaguet JP. 1990.Nanocapsules as carriers for oral peptide delivery. J Contr Rel13:233–239.
Desai MP, Labhasetwar V, Amidon GL, Levy RJ. 1996. Gastrointestinaluptake of biodegradable microparticles: Effect of particle size. PharmRes 13:1838–1845.
Eaton RP, Allen RC, Schade DS, Standefer JC. 1980. ‘Normal’ insulin secre-tion: The goal of artificial insulin delivery systems?. Diabetes Care3:270–273.
Eneroth G, Ahlund K. 1968. Biological assay of insulin by blood sugardetermination in mice. Acta Pharm Suec 5:591–594.
Galindo-Rodriguez S, Allemann E, Fessi H, Doelker E. 2004.Physicochemical parameters associated with nanoparticle formationin the salting-out, emulsification-diffusion and nanoprecipitationmethods. Pharm Res 21:1428–1439.
Jintapattanakit A, Junyaprasert V, Mao S, Sitterberg J, Bakowsky U,Kissel T. 2007. Peroral delivery of insulin using chitosan derivatives:A comparative study of polyelectrolyte nanocomplexes and nanoparti-cles. Int J Pharm 342:240–249.
Kondoh M, Yagi K. 2007. Progress in absorption enhancers based on tightjunction. Exp Opin Drug Deliv 4:275–286.
Lewis G, Zinman B, Groenewound Y, Vranic M, Giacca A. 1996. Hepaticglucose production is regulated both by direct hepatic and extrahepaticeffects of insulin in humans. Diabetes 45:454–462.
Li Y, Ogris M, Pelisek J, Roedl W. 2004. Stability and release characteristicsof poly (d,l-lactide-co-glycolide) encapsulated CaPi-DNA coprecipita-tion. Int J Pharm 269:61–70.
Matsuura J, Powers ME, Manning MC, Shefter E. 1993. Structure andstability of insulin dissolved in 1-octanol. J Am Chem Soc115:1261–1264.
Meyer JD, Manning MC. 1998. Hydrophobic ion pairing: Altering thesolubility properties of biomolecules. Pharm Res 15:188–193.
0.00%
50.00%
100.00%
150.00%
200.00%
250.00%
4
Time (h)
Pla
sma
gluc
ose
leve
l (%
of i
nitia
l)
0 1 2 3
Figure 5. Plasma glucose level after an oral glucose challenge (2 g/kg)
performed 1 h after a single oral administration of the 20 IU/kg Ins-S.O-
oaded nanoparticles and saline in fasted diabetic rats. Results are
expressed as mean� SD, n¼ 6 per group. (#) saline, (˙) Ins-S.O
complex-loaded nanoparticles.
Insulin-S.O complex-loaded PLGA nanoparticles 477
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

Nandi A, Khakhar DV, Mehra A. 2001. Coalescence in surfactant-sta-bilized emulsions subjected to shear flow. Langmuir 17:2647–2655.
Owens DR, Zinman B, Bolli G. 2003. Alternative routes of insulin delivery.Diab Med 20:886–898.
Polaschegg E. 1998. Effect of physicochemical variables of regular insulinformulations on their absorption from the subcutaneous tissue.Diabetes Res Clin Pract 40:39–44.
Ritschel WA, Ritschel GB, Ritschel BEC, Lucker PW. 1988. Rectal deliverysystem for insulin. Methods Find Exp Clin Pharmacol 10:645–656.
Song X, Zhao Y, Wu W, Bi Y, Cai Z, Chen Q, Li Y, Hou S. 2008. PLGAnanoparticles simultaneously loaded with vincristine sulfate and vera-pamil hydrochloride: Systematic study of particle size and drug. Int JPharm 350:320–329.
Sun S, Cui F, Kawashima Y, Liang N, Zhang L, Shi K, Yu Y. 2008. A novelinsulin-sodium oleate complex for oral administration: Preparation,characterization and in vivo evaluation. J Drug Deliv Sci Tec18:239–243.
478 S. Sun et al.
Jour
nal o
f M
icro
enca
psul
atio
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.





























