Embed Size (px)
Citation preview


Pancreas exocrin
› Pancreatite acute
› Pancreatite cronice
› Afectiuni ereditare ale pancreasului
› Tumori pancreatice
Pancreas endocrin
› Diabetul zaharat
› Tumorile neuroendocrine PET-NET

Pancreas exocrin
› Pancreatite acute
› Pancreatite cronice
› Afectiuni ereditare ale pancreasului
› Tumori pancreatice
Pancreas endocrin
› Diabetul zaharat
› Tumorile neuroendocrine PET-NET

4
Pancreatita acuta
urgenta
garda UPU
Chirurg sau
Internist
Pancreatita cronica
durere abdominala trenanta
Medic de familie !
Eventual internist din policlinica
Tumori pancreatice
Nutritionist, medic de familie, endocrinolog, psihiatru, gastroenterolog

5
Necesita explorari
Uneori sofisticate
Necesara internare
De obicei
gastroenterolog

Incidenta 4,9-35 %ooo /an
In crestere in tarile europene
Cauza majora de spitalizare in SUA
Cauza = crester consum de alcool
Mortalitate 5- 17%
Vege SS et al Gastrointestinal epidmiology 2007

Incidence of AP increased between 2000 and 2005 from 13.2 to 14.7
Incidence of AP for males increased from 13.8 to 15.2, for females from 12.7 to 14.2
Mortality for AP fluctuated between 6.9 and 11.7 per million
persons/ year and was almost similar for males and females. Incidence and mortality of AP and CP increased markedly with age. CONCLUSION: Incidence of AP steadily increased. Mortality for AP remained fairly stable. Patient burden and health care costs probably will increase
because of an ageing
BW Ml Spanier et alWorld J Gastroenterol 2013 May 28; 19(20): 3018-3026

European studies increase in the incidence rate of acute pancreatitis
922 patients with confirmed diagnosis of AP ( (2000–2009)in 1 hospital incidence rate varied from 24 to 35/100 000 inhabitants annually. Mean age was 60 ± 16 years. 53% men and 47% women etiologies of AP were biliary stones in 60% and alcohol abuse in 19%
of patients. severe in 50% and 43 Davor Stimac et al - Gastroenterology Research and Practice
Volume 2013, Article ID 956149,

Cauza › Pancreatita cronica
› Fibroza chistica
› Chirurgia pancreatica
Prevalenta 3,9/100.000 EU › 3,3/100.000 Franta
› 4,2 /100000 Germania
› 2,9/100000 Italia
› 3.0/100000 Spania
› 5,5/100000 UK
Mattson,Jakc Report 2005- Pancreatic exocrine insuffiency epidemiology

› Loss of functioning parenchyma Chronic pancreatitis Cystic Fibrosis Tumours Resections
› ↓secretion despite intact parenchyma Obstruction ↓endogenous stimulation (coeliac, Crohns, DM)
› Asynchrony Gastric resections Short bowel syndrome Crohns, DM
› Enzyme inactivation Zollinger-Ellison syndrome

Prevalenta
› Creste cu varsta
› Mai mare la barbati
Distributia pe sex si varsta difera f de etiologie
› Alcoolica mai frecv la Barbati
› Idiopatica si hiperlipemica la femei
› Fiborza chistica egala femei barbati
› Fibroza chistica mai frecv in primul an de viata
› Pancreatita cronica si chirurgie la varstnic Rothenbacher D, etal Scand J Gast 2005;40(6)

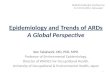
Insuficienta pancreatica exocrina
Pancreatectomie
Rezectie
gastrica
Pancreatita
cronica
Pancreatita
acuta
Fibroza
chistica
“Pancreatita
senila”
Plenitudine Meteorism
Intoleranta
alimentelor
Steatoree
Pierdere in
greutate
Dispepsie
Malabsortie
Durere
abdominala
Greata / varsaturi Pierderea apetitului
PEI
Cauze
Indicatie
Semne
simptome

Pancreatita cronica
Incidenta PC este de 3,5 - 4 /
100 000 locuitori.
Prevalenta/Predominanta de
vârsta si sex: pancreatita
cronica afecteaza
preponderent barbatii în vârsta
de 35 - 45 ani (de 3 ori mai
frecventa decât la femei).
Forma usoara Forma severa Pseudochist
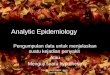
Recidiva
Restitutio ad integrum
PA
PC
PA Pancreatita acuta
PC Pancreatita cronica
Klöppel & Maillet, Hepatogastroenterol 38:408, 1991

14
INCIDENTA = 3-10 %ooo loc
PREVALENTA = 5.5-30 %ooo loc
!!Este in crestere
Variaza geografic
Tara Incidenta
/100 000 loc
Sursa
Japonia 5.7 JGastroenterol
38(4):315-26, 2003
Elvetia 1.6 Eur J Gastroenterol
Hepatol.13(6):749-
50, 2001
Finlanda
23 Pancreatology.2(5):
469-77, 2002
Cehia 7.9 idem

Inciența este de 6-7 /100.000 locuitori în vest
80% sex masculin.
Vârsta medie depinde de etiologie,
› ~ 40-45 ani la PC alcoolică,
› ~ 25-30 la PC idiopatică,
› ~ 15-20 la cei PC ereditară,
› ~ 10 ani la copii cu PC tropicală.
Incidența este crescută la negri față de albi.
James Jupp a,1, David Fine b,2, ColinD.Johnson c,*Best
Practice&ResearchClinicalGastroenterology24(2010)219e231

Etiologie.
Consumul excesiv de alcool 70-85%
Fumatul, l factor de risc extern cancerului pancreatic.
Alte cauze rare de PC:
hipercalcemia peste 12mg/dl (3mmol/l (1% din PC sunt datorate hiperPTH, 7% din hiperPTH au și PC).
PC tropicală.
PC genetică.
PC autoimună
PC obstructivă.
PC idiopatică. 10% din cazurile de PC
James Jupp a,1, David Fine b,2, ColinD.Johnson c,*Best
Practice&ResearchClinicalGastroenterology24(2010)219e231

Benigne
Maligne
Epiteliale
Nonepiteliale
Exocrine
Endocrine

Epithelial tumours Benign Serous cystadenoma 8441/01 Mucinous cystadenoma 8470/0 Intraductal papillary-mucinous adenoma 8453/0 Mature teratoma 9080/0 Borderline (uncertain malignant potential) Mucinous cystic neoplasm with moderate dysplasia 8470/1 Intraductal papillary-mucinous neoplasm with moderate dysplasia Solid-pseudopapillary neoplasm 8452/1 Malignant Ductal adenocarcinoma 8500/3 Mucinous noncystic carcinoma 8480/3
Signet ring cell carcinoma 8490/3 Adenosquamous carcinoma 8560/3 Undifferentiated (anaplastic) carcinoma 8020/3 Undifferentiated carcinoma with osteoclast-like giant cells 8035/3 Mixed ductal-endocrine carcinoma 8154/3 Serous cystadenocarcinoma 8441/3 Mucinous cystadenocarcinoma 8470/3 – non-invasive 8470/2
– invasive 8470/3 Intraductal papillary-mucinous carcinoma 8453/3 – non-invasive 8453/2 – invasive (papillary-mucinous carcinoma) 8453/3
Acinar cell carcinoma 8550/3 Acinar cell cystadenocarcinoma 8551/3 Mixed acinar-endocrine carcinoma 8154/3 Pancreatoblastoma 8971/3
Solid-pseudopapillary carcinoma 8452/3
Others
Non-epithelial tumours
Secondary tumours

Primary Tumour (T) TX Primary tumour cannot be assessed T0 No evidence of primary tumour Tis Carcinoma in situ T1 Tumour limited to the pancreas, 2 cm or less in greatest
dimension T2 Tumour limited to the pancreas, more than 2 cm in
greatest dimension T3 Tumour extends directly into any of the following:
duodenum, bile duct, peripancreatic tissues3 T4 Tumour extends directly into any of the following:
stomach, spleen, colon, adjacent large vessels4 Regional Lymph Nodes (N) NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Regional lymph node metastasis N1a Metastasis in a single regional lymph node N1b Metastasis in multiple regional lymph nodes Distant Metastasis (M) MX Distant metastasis cannot be assessed M0 No distant metastasis MI Distant metastasis
Stage grouping Stage 0 Tis N0 M0
Stage I T1 N0 M0
T2 N0 M0
Stage II T3 N0 M0
Stage III T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4 Any N M0
Stage IVB Any T Any N M1

Sex Cancer Recorded deaths 2007 Predicted number of deaths 2012
Men
Stomach 37424 33926
colon and rectum 85244 89117
Pancreas 35022 39088
Lung 183019 183592
Prostate 68282 69960
Leukemias 21553 22320
All cancers (malignant and benign) 706619 717398
Women
Stomach 25060 21138
Colon and rectum 75294 73989
Pancreas 34965 38443
Lung 69115 78658
Breast 89012 88101
Uterus (cervix and corpus) 27393 26720
Leukemias 17884 18605
All cancers (malignant and benign)554515 565703
Malvezi M et al - Annals of Oncology 28 feb 2012


10th most frequent cancer
the 8th leading cause of cancer-related
death
Incidence
men: 7,3 – 8,7 per 100.000
women: 4,5 – 5,7 per 100.000
>95% of patients are dying of their disease
No survival increases have been observed
in the last years
S. Cascinu et al. Annals of Oncology 21 (Supplement 5): v55–v58,
2010

Demographic factors Old age (most reliable and important predictor) Sex (more common in males than in females) Ethnic origin (mortality highest in black populations)
Genetic factors and medical conditions Family history (one first degree → 2,3 fold increased risk) Hereditary pancreatitis Hereditary non-polyposis colorectal cancer Ataxia-telangiectasia Peutz-Jeghers syndrome (132 fold increased risk) Familial breast cancer (BRCA2 mutations) Familial atypical multiple mole melanoma (germline mutations in p16) Chronic pancreatitis (2% per decade) Diabetic mellitus Gastrectomy
Deficiency in carcinogen metabolism and DNA repair Environmental and lifestyle factors Cigarette smoking Occupational exposures Low dietary intake of fruits and vegetables Food preparation and cooking methods (grilling or charring confers the highest risk)
James L Abbruzzese et al. Lancet 2004; 363: 1049–57

Enviromental factors
cigarette smoking* RR = at least 1,5
especially in smokers with GSTT1 (homozygous deletions of
gene glutathione S-transferase T1)
risk level returns to baseline by 15 years after cessation
dietary** excessive fat or meat
diabetes mellitus*** diagnosed within the preceding two years
associated with obesity
*Ghadirian P. Cancer 1991; 67:2664-70
**Farrow DC. Am J Epidemiol 1990; 132:423-31
***Gullo L. N Engl J Med 1994; 331:81-4

Normal pancreas has 3 types of epithelial cells Acinar cells – 80%
Ductal cells – 10-15%
Endocrine cells - <5%
95% of neoplasms arise from the exocrine elements - ductal and acinar cells
Ductal adenocarcinoma = 85% to 90% of pancreatic tumors
Localization: 60-70% head, 5-10% body,10-15%
tail

Benign Serous cystadenoma Mucinous cystadenoma Intraductal papillary mucinous adenoma Mature cystic teratoma
Borderline (uncertain malignant potential) Mucinous cystic tumor with moderate dysplasia Intraductal papillary mucinous tumor with moderate dysplasia Solid-pseudopapillary tumor
Malignant Ductal adenocarcinoma Osteoclast-like giant cell tumor Serous cystadenocarcinoma Mucinous cystadenocarcinoma (noninvasive or invasive) Intraductal papillary mucinous carcinoma (noninvasive or
invasive) Acinar cell carcinoma Pancreatoblastoma Solid-pseudopapillary carcinoma Miscellaneous carcinomas
Hamilton SR, Aaltonen LA. World Health Organization Classification of Tumours.
Pathology and Genetics of Tumours of the Digestive System. Lyon, France: IARC
Press; 2000

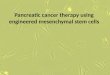
successive accumulation of gene mutations
3 precursor lesions*:
› Primary histologic precursor of pancreatic cancer =
pancreatic intraductal neoplasia (PanIN)
PanIN 1a,b (minimally dysplastic epithelium)
** activation of the KRAS2 oncogene,
inactivation of the tumor-suppressor gene CDKN2A
inactivation of the tumor-suppressor genes TP53 and deleted in
pancreatic
cancer 4 (DPC4, also known as the SMAD4
PanIN 2,3 (severe dysplasia)
› Mucinous cystic neoplasm (MCN)
› intraductal pancreatic mucinous neoplasm (IPMN)
* Jason Klapman. Cancer Control October 2008, Vol. 15, No. 4 ** Feldmann G. J Hepatobiliary Pancreat Surg 2007;14:224-32

Normal duct
Normal duct
PanIN Ia PanIN Ib PanIN II PanIN III
MCN low grade
IPMN low grade
Intermediate grade
High grade
Cancer
Jason Klapman. Cancer Control October 2008, Vol. 15, No. 4

Gene/ chromosomal region
(oncogenes and tumor supression)
% of tumors with genetic mutation
K-ras (12p) >90%
p16 CDKN2A (9p) >95%
PK53 (17p) 50%-70%
SMAD4/DPC4 (18q) 55%
AKT2 (19q) 10%-20%
MYB (6q) 10%
AIB1 (20q) 10%
BRCA2 (13q) 7%-10%
LKB1/STK11 (19p) <5%
MKK4 (17p) <5%
TGF-β-R1 (9q) or TGF-β-R2 (3p) <5%
RB1 (13q) <5%
Modified from Hruban RH, Wilentz RE. The pancreas. In: Kumar V, Abbas AK, Fausto N, editors. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia: Elsevier; 2005

Oncogenes – K-ras present in 90% of cancers
frequency of mutations = extent of dysplasia
Can be detected in chronic pancreatitis without neoplasia
Tumor suppressor genes TP53 mutations → chromosomal instability → cancer
P16 mutation
associated with FAMMM syndrome (melanoma and pancreatic cancer)
associated with decreased survival
DPC4 = effect on cell cycle regulation and cell differentiation
Other: up-regulation of EGF, telomere shortening


Cancer Incidence
Oesophagus 578
Stomach 2650
Colorectum 4554
Liver 1279
Gallbladder 293
Pancreas 1682
Lung 8387
Prostate 3620

Cancer Incidence Oesophagus 103
Stomach 1351 Colorectum 4142 Liver 692
Gallbladder 355 Pancreas 1184 Breast 7929 Cervix uteri 3402 Corpus uteri 1208 Ovary 1686

Male Female both
Lung Breast Lung
Colorectum Colorectum Colorectum
Prostate Cervix uteri Breast
Stomach Lung Stomach
Bladder Ovary Prostate
Romania GLOBOCAN 2008

Statisitica MS – PCR in 2011 – 975 cazuri = 4,8 %ooo locuitori
Studii › Diculescu et al –Romanian J gastroenterol 2005 –
studiu de cohorta PAC – 62 pacienti sp Elias
› Hajjar N et al – Chirurgia 2012 – 81 pacienti Chirurgie 3 Cluj
› Hecser L et al – Rom J Legal Med2009 – case reports PAC
› Diaconu B – J Gastrointest Liver Disease 2009 –SPINK 1 mutatie in 94 pac cu PCR

Cauze
› Raportarea in functie de ICM/DRG modifica
formularea diagnostica
› Raportarea in teritoriu deficitara
› Patologie complexa ce implica multe
esaloane medicale ( primara, secundara
tertiare) fiecare cu raportari diferite

Dezavantaje
› Simptomatologia in patologia pancreatica apare de f multe ori f tardiv in stadii avansate
› Diagnosticul se bazeaza pe explorari imagistice sofisticate inabordabila pt metode de screening
“Avantaje”
› Pancreatitele acute se interneaza doar in spitalele de urgenta
› Rata incidentei in tumorile maligne pancreatica este practic egala cu cea a mortalitatii
› Putine cazuri de Pancreatite cronice

Abord multidiscliplinar
Standardizarea diagnosticelor
APPR => registre pe domenii restranse
de cazuri
› Pancreatite ereditare
› Tumori pancreatice rare
› Tumori neuroendocrine (PET-NET)

Incidenta pancreatitelor acute este in
crestere in tarile occidentale ( si la noi?)
Cunoasterea corecta a abordarii PAC poate
salva vieti
Pancreatitele cronice sunt subdiagnosticate si
subestimate
Tumorile pancreatice sunt in crestere si nu
sunt metode de screening eficient actual