-
8/11/2019 jop.2012.110716
1/8
Clinical Efficacy of SubgingivallyDelivered 1.2-mg
Simvastatin
in the Treatment of IndividualsWith Class II Furcation Defects:A
Randomized Controlled Clinical TrialA.R. Pradeep,* N. Priyanka,*
Nitish Kalra,* Savitha B. Naik, Sonender P. Singh,*and Santosh
Martande*
Background:Simvastatin (SMV) assists in bone regenera-tion and
has an anti-inflammatory effect when delivered or
applied locally. The present clinical trial is designed
toinvestigate the effectiveness of 1.2-mg SMV as a local
drugdelivery system as an adjunct to scaling and root planing(SRP)
for the treatment of Class II furcation defects.
Methods: Seventy-two patients with mandibular buccalClass II
furcation defects were randomized and categorizedinto two treatment
groups: SRP plus placebo (group 1) andSRP plus 1.2-mg SMV (group
2). Clinical parameters wererecorded at baseline before SRP and at
3 and 6 months; theyincluded modified sulcus bleeding index (mSBI),
probing depth(PD), and relative vertical (RVAL) and horizontal
(RHAL) at-tachment levels. At baseline and after 6 months,
radiologic as-
sessment of bone defect fill was performed.Results: Both
therapies resulted in significant improve-ments. The decrease in
mSBI score at 6 months was greaterin group 2 (2.02 0.23) compared
with group 1 (1.80 0.22). The mean decrease in PD at 6 months was
1.30 1.0and 4.05 1.31 mm in groups 1 and 2, respectively. A
signif-icantly greater gain in mean RVAL and RHAL was found ingroup
2 than in group 1 (P
-
8/11/2019 jop.2012.110716
2/8
detected even after open-flap surgery,4 and there isclinically
significant loss of attachment within thefurcation area during at
least the first 2 years ofmaintenance care.5 Bone deficiencies are
of majorconcern andaffect therapiesin all dental andmedicalfields.
Because of the limitations of current bone
grafting methods, alternative methods for repairingbone defects
are needed.
Statins are specific inhibitors of 3-hydroxy-3-methylglutaryl
coenzyme A reductase, a rate-limit-ing enzyme of the cholesterol
synthesis pathway.6
Statins are widely used to lower blood cholesterollevels. A
recent study suggests that statins canstimulate bone formation by
stimulating the pro-duction of bone morphogenetic protein-2
(BMP-2).7
Simvastatin (SMV) is a chemical modification oflovastatin, which
is obtained by the replacementof 2-methyl-butyryl side chain of
lovastatin with
a 2,2-dimethyl-butyryl group. Various animal studiesshowed that
SMV assists in bone regeneration as wellas the anti-inflammatory
effect when delivered or ap-plied locally.8-10 SMV enhances
alkaline phosphataseactivity and mineralization and increases the
expressionof bone sialoprotein, osteocalcin, and type I
collagen,and it is shown to have an anti-inflammatory effectby
decreasing the production of interleukin-6 andinterleukin-8.11 SMV
is reported to stimulate vascularendothelial growth factor (VEGF)
release in a dose-dependent manner, and the authors of a
previousstudy12 suggested that statins may promote osteo-
blast differentiation and bone nodule formation bystimulating
VEGF expression in bone tissue.Recently, a study by the authors of
the present
study13 showed that locally delivered 1.2-mg SMVstimulated
significant increase in probing depth (PD)reduction, clinical
attachment level (CAL) gain, andimproved bone fill compared with
placebo gel as anadjunct to SRP in the treatment of intrabony
defects(IBDs) in patients with chronic periodontitis (CP).
Various vehicles have been used for local drugdelivery (LDD) in
patients with periodontitis. Vehiclesused are biocompatible, have
predictable biodeg-radation kinetics and ease of fabrication, and
haveregulatoryapproval; thus,theyhavewide applicationsin controlled
drug delivery systems.14 Methylcelluloseis widely used in a variety
of oral and topical phar-maceutical formulations, such as
ophthalmic con-trolled-release in situ gelling systems for
ciprofloxacinand nimesulide-loaded methylcellulose nanoparticlesand
microparticles for oral delivery.15,16 It is usedextensively in
cosmetic and food products. Methyl-cellulose is generally regarded
as a non-toxic, non-allergic, and non-irritating material and is
used asa sustained-release vehicle for therapeutic drugs.17
To the best of our knowledge, there are no pub-
lished data on the use of in situ gel using SMV with
methylcellulose (as a vehicle) for direct placementin patients
with Class II furcation defects. Keepingthe above facts in mind,
the present study was per-formed as a single-center, randomized
controlledclinical trial to investigate the clinical and
radiologic(bone fill) efficacy of 1.2-mg SMV as an adjunct to
SRP in the treatment of mandibular buccal Class IIfurcation
defects.
MATERIALS AND METHODS
Source of DataThe participants for this study were selected from
theoutpatient section of the Department of Periodontics,Government
Dental College and Research Institute,Bangalore, India, from March
2011 to August 2011.Seventy-two patients (38 males and 34 females,
aged30 to 50 years), diagnosed with CP with mandibularbuccal Class
II furcation defects,18 were enrolled in thisstudy.It wasmadeclear
to thepotentialparticipantsthatparticipation was voluntary. Written
informed consentwasobtained from allpatients,andethical clearance
forthe study was received from the Institutional EthicalCommittee
and Review Board, Government DentalCollege and Research Institute
of Bangalore, India.
Selection CriteriaThe inclusion criteria for the study was: 1)
the pres-ence of buccal Class II furcation defects in
end-odontically vital, asymptomatic mandibular first andsecond
molars with a radiolucency in the furcation
area on an intraoral periapical radiograph with PD
5 mm and horizontal PD 3 mm after Phase I therapy(SRP) and 2) no
history of antibiotic or periodontaltherapy in the preceding 6
months. Exclusion criteriawere: 1) known systemic disease; 2) known
or sus-pected allergy to the SMV group; 3) systemic statintherapy;
4) aggressive periodontitis; 5) use of to-bacco in any form; 6)
alcoholism; 7) diabetes; 8)immunocompromised patients; and 9)
pregnantor lactating females. In addition, teeth with
gingivalrecession, endodontic (pulpal) involvement, Class
IIIfurcation involvement,18 and/or tooth mobility of atleast grade
II19 were also excluded.
Eighty individuals were initially analyzed forthe study. Eight
individuals were excluded becausethey did not meet the inclusion
criteria. After par-ticipant selection (by ARP), 36 participants
wererandomly assigned to each treatment group (usinga
computer-generated system), and one site perparticipant was treated
with SRP plus placebo gel(group 1) or SRP plus SMV (1.2 mg/0.1 mL)
in situgel (group 2). SRP was performed at baseline untilthe root
surface was considered smooth and cleanby the operator (NP). No
antibiotics or antiplaqueand anti-inflammatory agents were
prescribed after
treatment.
J Periodontol December 2012 Pradeep, Priyanka, Karla, Naik,
Singh, Martande
1473
-
8/11/2019 jop.2012.110716
3/8
Clinical parameters, including modified sulcusbleeding index
(mSBI)20 and full-mouth and site-specific plaque index (PI)
score,21 were consideredbefore SRP, and PD, relative vertical
attachmentlevel (RVAL), and relative horizontal attachment
level(RHAL) were recorded at baseline (after SRP) and at
3 and 6 months. A custom-made acrylic stent and acolor-coded
periodontal probe were used to stan-dardize the measurement of PD
and RVAL. RVAL wascalculated by measuring the distance from the
stent(apical extent) to the base of the pocket minusthe distance
from the stent to the cemento-enameljunction. RHAL was measured
using a periodontalprobe from the stent to the deepest horizontal
pointof the periodontal pocket.
A single clinician (NP) provided treatment to bothgroups, and
all pretreatment and post-treatmentclinical parameters were
recorded by another exam-
iner (NK) who was masked to the type of treatmentreceived by the
participants.
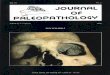
Radiographic Evaluation of Furcation DefectsBone fill was
evaluated at baseline and after 6 monthsusing an image analyzer.i
The radiographic bone fillwas measured with a computer-aided
program ac-cording to the method used by Francetti et al.22
In-dividually customized bite blocks and a parallel-angletechnique
were used to obtain films that were as re-producible as possible.
All radiographs were reviewedin a single reference center by a
masked evaluator(ARP). For evaluation, radiographs were scanned
at
800 dots per inch with a scanner, and the bone defectwas
evaluated using computer-aided software. Thebone defect was
measured on the radiograph bymeasuring the distance from the
furcation fornix tothe base of the defect (Figs. 1 and 2).
Intra-Examiner Calibration
Intra-examiner calibration was achieved by exami-nation of 20
patients two times (24 hours apart) beforebeginning the study.
Calibration was accepted ifmeasurements at baseline and 24 hours
were similarwithin 1 mm at the 95% level.
Primary and Secondary Outcome MeasuresThe primary outcome of the
study was bone fill. Thesecondary outcomes included RVAL, RHAL, PD,
PI,and mSBI.
Formulation of 1.2-mg SMV In Situ GelThe SMV gel (1.2 mg) was
prepared as described ina previous study.13 The release profile of
SMV from gelhas been studied previously using
high-performanceliquid chromatography.13 Based on its
sufficientlyprolonged release in gingival crevicular fluid
afterLDD,13 1.2 mg SMV was delivered locally in
furcationareas.Briefly, methylcellulose in situ gelwas prepared
by adding the required amount of biocompatible
solvent to an accurately weighed amount of methyl-cellulose. The
vial was heated to 50C to 60C andagitated using a mechanical shaker
to obtain a clearsolution.23 A weighed amount of SMV was added
tothe above solution and dissolved completely to ob-tain a
homogeneous phase of polymer, solvent, anddrug. Thus, the SMV in
situ gel was prepared with aconcentration of1.2 mg.
LDDFor standardization, 0.1 mL prepared SMV gel(1.2 mg/0.1 mL)
was injected into the furcationdefect using a syringe with a blunt
cannula. After
placement of the in situ gel, patients were instructedto refrain
from chewing hard or sticky foods, brushingnear the treated areas,
or using any interdental aidsfor 1 week. Adverse effects were noted
at recall visits,and any supragingival deposits were removed.
Statistical AnalysesPoweranalysiscalculationswereperformedbefore
thestudy was initiated. To achieve 90% power and detectmean
differences of the clinical parameters between
Figure 1.Furcation defect was measured on the baseline
radiograph by measuringthe distance from the furcation fornix to
the base of the defect (3.8 mm).
UNC-15 periodontal probe, Hu-Friedy, Chicago, IL. Nabers
periodontal probe, Hu-Friedy.i Scion Image Analyzer, Scion
Corporation, Frederick, MD. HP Scanjet 3c/I, Hewlett-Packard,
Singapore.
Simvastatin As Local Drug Delivery for Treatment of Class II
Furcation Defects Volume 83 Number 12
1474
-
8/11/2019 jop.2012.110716
4/8
groups, 30 sites in each group were required. Cate-gorical
variable (site-specific PI) was expressed aspercentage and
continuous variable (full-mouth PI,mSBI, PD, RVAL, RHAL, and bone
fill) as mean SD.Site-specific PI was compared by using the x2
testor a Fisher exact test when the expected frequencywas
-
8/11/2019 jop.2012.110716
5/8
mSBI
A statistically significant decrease in mSBI scoresfrom baseline
was found in both groups. The decreasein mSBI score was greater in
group 2 (2.02 0.23)compared with group 1 (1.80 0.22) at 6 months;
it
was significant in both groups at the 5% level of sig-nificance
(P
-
8/11/2019 jop.2012.110716
6/8
minimized by clearance by the liver,34 and systemicside effects
of high doses are significant.
A significant mean bone fill in Class II furcationinvolvement
from baseline (1.54%) to 6 months(25.16%) in group 2 suggests a
role for SMV in
bone formation. This may be because of increased
BMP-2 expression during bone regeneration,35 anti-inflammatory
effects,36 and angiogenesis duringwound healing.
Local delivery of statins in healing sites or defectshas been
shown effective in new bone formation.
Morris et al.9 studied the effect of injectable SMV
Table 4.
Full-Mouth Plaque Scores and Gingival Index (GI) for SMV and
Placebo Groupsat Different Time Intervals
PI GI
Group Mean SD Mean Difference P value Mean SD Mean Difference P
value
1
Baseline 1.90 0.20 2.51 0.42
3 months 0.83 0.15 1.07 0.16 NS 1.42 0.44 1.09 0.17 0.001*
6 months 0.66 0.18 1.24 0.13 NS 1.61 0.43 0.89 0.27 0.001*
2
Baseline 1.88 0.22 2.83 0.27
3 months 0.97 0.18 0.91 0.14 NS 1.03 0.18 1.80 0.22 0.001*6
months 0.68 0.18 1.20 0.13 NS 0.80 0.18 2.02 0.23 0.001*
NS = not significant.* Statistically significant at 5% level of
significance ( P
-
8/11/2019 jop.2012.110716
7/8
in three-wall periodontal IBDs, Class II furcations de-fects,
and edentulous alveolar ridges in beagle dogsby histomorphometric
analysis; 29% greater ridgethickness was found with SMV, but bone
height losswas detected in the interproximal IBDs and
furcationdefects. The greater degree of bone loss in the IBDs
and furcation defects found in this studywas the resultof flap
surgeries involving manipulation of bone withrotary instruments.
However, the present study, inwhich only a non-surgical approach
(SRP) was usedin conjunction with locally delivered 1.2-mg
SMV,effective bone fill and a greater decrease in PD andRVAL and
RHAL gain was found in the treatment ofmandibular buccal Class II
furcation involvement.Therefore, this study confirms that locally
deliveredSMV enhances bone growth in furcation areas whenused as an
adjunct to SRP.
In the present study, there is decreased gingival
bleeding index from baseline to 6 months, suggestingan
anti-inflammatory effect of SMV. A similar anti-inflammatory effect
of SMV was observed in our pre-vious study13 in patients with
periodontal IBD. Withregard to the dose of SMV used, 1.2 mg/0.1 mL
persite is injected in the present study. It has beenshown that
local application of 70 mg/kg causesinflammation.23 Stein et al.8
demonstrated that, byreducing the SMV dose from2.2 to 0.5 mg, there
wasa decrease in the inflammation to a more clinicallyacceptable
level without sacrificing bone growth po-tential. A 45% increase in
bone area was reported
with 0.5-mg SMV versus the gel control (similar toa 2.2-mg
dose), and clinical swelling was significantlyreduced compared with
the high SMV dose. Becauseit was difficult to achieve proper
viscosity with a low-er concentration, a 1.2% SMV concentration was
usedto prepare a flowable gel that could easily passthrough the
syringe. A decrease in the viscosity of gelwas also studied in
vitro when exposed to 37C(mouth temperature). The use of smaller
(25-gauge)needles with little extrusion of drug solution and
betterdispersion of the drug at the site of injection madeit easier
to inject the SMV gel at the diseased site.
A decrease in PD and gain in CAL are the majorclinical outcomes
measured to determine the suc-cess of any periodontal treatment. A
significantdecrease in PD and gain in RVAL and RHAL werefound
within both groups compared with baseline atall time intervals.
When comparing the two groups,the decrease in PD and RVAL and RHAL
gain werestatistically significant at each period, even after
6months (P
-
8/11/2019 jop.2012.110716
8/8
6. Jadhav SB, Jain GK. Statins and osteoporosis: Newrole for old
drugs. J Pharm Pharmacol2006;58:3-18.
7. Mundy G, Garrett R, Harris S, et al. Stimulation of
boneformation in vitro and in rodents by statins.
Science1999;286:1946-1949.
8. Stein D, Lee Y, Schmid MJ, et al. Local simvastatineffects on
mandibular bone growth and inflamma-
tion.J Periodontol2005;76:1861-1870.9. Morris MS, LeeY, Lavin
MT, et al. Injectable simvastatin
in periodontal defects and alveolar ridges: Pilot studies.J
Periodontol2008;79:1465-1473.
10. Nyan M, Sato D, Oda M, et al. Bone formation with
thecombination of simvastatin and calcium sulfate incritical-sized
rat calvarial defect. J Pharmacol Sci2007;104:384-386.
11. Sakoda K, Yamamoto M, Negishi Y, Liao JK, Node K,Izumi Y.
Simvastatin decreases IL-6 and IL-8 produc-tion in epithelial
cells. J Dent Res2006;85:520-523.
12. Takenaka M, Hirade K, Tanabe K, et al. Simvastatinstimulates
VEGF release via p44/p42 MAP kinase invascular smooth muscle cells.
Biochem Biophys ResCommun2003;301:198-203.
13. Pradeep AR, Thorat MS. Clinical effect of
subgingivallydelivered simvastatin in the treatment of patientswith
chronic periodontitis: a randomized clinical trial.J
Periodontol2010;81:214-222.
14. Gilding DK, Reed AM. Biodegradable polymers for usein
surgery polyglycolic/polylactic acid homo- and co-polymers
1.Polymer1979;2:1459-1484.
15. Al-Kassas RS, El-Khatib MM. Ophthalmic controlledrelease in
situ gelling systems for ciprofloxacin basedon polymeric
carriers.Drug Deliv2009;16:145-152.
16. Ravikumara NR, Madhusudhan B, Nagaraj TS, HirematSR, Raina
G. Preparation and evaluation of nimesulide-loaded ethylcellulose
and methylcellulose nanopar-ticles and microparticles for oral
delivery. J Biomater
Appl2009;24:47-64.17. Final report on the safety assessment of
hydroxye-thylcellulose, hydroxypropylcellulose, methylcellu-lose,
hydroxypropyl methylcellulose and cellulosegum. Int J
Toxicol1986;5:1-59.
18. Hamp SE, Nyman S, Lindhe J. Periodontal treatment
ofmultirooted teeth. Results after 5 years. J Clin
Perio-dontol1975;2:126-135.
19. Miller SC. Textbook of Periodontia. Philadelphia: Bla-kiston
Company; 1938:91.
20. Mombelli A, van Oosten MA, Schurch E, Lang NP. Themicrobiota
associated with successful or failing os-seointegrated titanium
implants. Oral Microbiol Immu-nol1987;2:145-151.
21. Silness J, Loe H. Periodontal disease in pregnancy. II.
Correlation between oral hygiene and periodontalcondition.Acta
Odontol Scand1964;22:121-135.
22. Francetti L, Trombelli L, Lombardo G, et al. Eval-uation of
efficacy of enamel matrix derivative inthe treatment of intrabony
defects: A 24-month mul-ticenter study. Int J Periodontics
Restorative Dent2005;25:461-473.
23. Thylin MR, McConnell JC, Schmid MJ, et al. Effects
ofsimvastatin gels on murine calvarial bone.J
Periodon-tol2002;73:1141-1148.
24. Goodson JM, Hogan PE, Dunham SL. Clinical re-sponses
following periodontal treatment by local drugdelivery.J
Periodontol1985;56(Suppl. 11):81-87.
25. Needleman IG, Pandya NV, Smith SR, Foyle DM. Therole of
antibiotics in the treatment of periodontitis (Part2 Controlled
drug delivery). Eur J Prosthodont RestorDent1995;3:111-117.
26. Sotiriou CG, Cheng JW. Beneficial effects of statins
incoronary artery disease Beyond lowering choles-terol.Ann
Pharmacother2000;34:1432-1439.
27. Garlet GP, Martins W Jr, Fonseca BA,Ferreira BR, SilvaJS.
Matrix metalloproteinases, their physiological in-hibitors and
osteoclast factors are differentially regu-lated by the cytokine
profile in human periodontaldisease.J Clin
Periodontol2004;31:671-679.
28. Tobert JA. New developments in lipid-lowering ther-apy: The
role of inhibitors of hydroxymethylglutaryl-coenzyme A
reductase.Circulation1987;76:534-538.
29. Song C, Guo Z, Ma Q, et al. Simvastatin inducesosteoblastic
differentiation and inhibits adipocyticdifferentiation in mouse
bone marrow stromalcells. Biochem Biophys Res Commun 2003;308:
458-462.30. Baek KH, Lee WY, Oh KW, et al. The effect of
simvastatin on the proliferation and differentiation ofhuman
bone marrow stromal cells. J Korean Med Sci2005;20:438-444.
31. Junqueira JC, Mancini MN, Carvalho YR, Anbinder AL,Balducci
I, Rocha RF. Effects of simvastatin on boneregeneration in the
mandibles of ovariectomized ratsand on blood cholesterol levels. J
Oral Sci2002;44:117-124.
32. Pytlik M, Janiec W, Misiarz-Myrta M, Guba1a I. Effects
ofsimvastatin on the development of osteopenia causedby ovariectomy
in rats. Pol J Pharmacol2003;55:63-71.
33. Tikiz C, Tikiz H, Taneli F, Gumusx
er G, Tuzun C. Effectsof simvastatin on bone mineral density and
remodelingparameters in postmenopausal osteopenic subjects: 1-year
follow-up study. Clin Rheumatol 2005;24:447-452.
34. Todd PA, Goa KL. Simvastatin. A review of its
phar-macological properties and therapeutic potential
inhypercholesterolaemia.Drugs1990;40:583-607.
35. Alam S, Ueki K, Nakagawa K, et al. Statin-inducedbone
morphogenetic protein (BMP) 2 expression dur-ing bone regeneration:
An immunohistochemicalstudy. Oral Surg Oral Med Oral Pathol Oral
RadiolEndod2009;107:22-29.
36. Borg E, Grondahl K, Persson LG, Grondahl HG.Marginal bone
level around implants assessed in
digital and film radiographs: In vivo study in the dog.Clin
Implant Dent Relat Res2000;2:10-17.
Correspondence: Dr. A. R. Pradeep, Department of Peri-odontics,
Government Dental College and Research In-stitute, Bangalore
560002, Karnataka, India. E-mail:[email protected].
Submitted December 05, 2011; accepted for publicationJanuary 26,
2012.
J Periodontol December 2012 Pradeep, Priyanka, Karla, Naik,
Singh, Martande
1479
mailto:[email protected]:[email protected]